
To fluid restrict or not..that is the question!
38
Dr. Shiva Mongolu Consultant Physician & Endocrinologist Hull & East Yorkshire Hospitals NHS Trust To fluid restrict or not..that is the question! A practical approach to the management of hyponatraemia
Transcript of To fluid restrict or not..that is the question!

Dr. Shiva Mongolu
Consultant Physician & Endocrinologist
Hull & East Yorkshire Hospitals NHS Trust
To fluid restrict or
not..that is the question! A practical approach to the management of
hyponatraemia

Aims
⦿ Understand the physiology of Na regulation
⦿ How to identify the cause
⦿ How to diagnose SIADH
⦿ Efficacy of treatment options ● Fluid restriction
● 1.8% Saline/3% Saline
● Demeclocycline
● Tolvaptan

Questions
• How is the patient?
• Is it acute or chronic ?
• Is it SIADH or volume depletion ?
• Do I need to intervene ?

More questions • Fluid restrict or Saline ?
• How much fluid to restrict ? Does it work ?
• Do slow sodium tablets work ?
• When should I use Demeclocycline ?
• What about the expensive drug Tolvaptan ?
• When should I use hypertonic saline ? Is it 1.8% or 3% ?

Background ⦿ Most common endocrine abnormality
⦿ Incidence 15-30% of hospitalised patients
(Na<135 mEq/L)
⦿ Associated with increased mortality (twice likely to
die during their hospital stay [RR 1.95])
⦿ Gait instability and falls
⦿ Overly rapid correction can cause severe
neurological deficits and death (osmotic
demyelination syndrome or central pontine
myelinolysis)

Physiology
Sodium is therefore regulated by 3 mechanisms: 1) RAAS
2) ADH release
3) Thirst mechanism

Osmoregulation Volume regulation
What is sensed ? Plasma osmolality Effective circulating volume
How clinically
assessed?
Plasma[Na⁺], P osm History, Physical exam, urine
[Na⁺]
Sensors Hypothalamic
osmoreceptors
Carotid sinus
Atria
Afferent arteriole (glomerulus)
Effectors ADH
Thirst mechanism
Sympathetic nervous system
Renin-angiotensin-aldo
system
Natriuretic peptides
ADH
What is effected ? Water excretion (ADH)
Water intake (thirst)
Sodium excretion

Acute vs. Chronic
● Hyponatraemia > 48hours duration is chronic
● Assume hyponatraemia chronic unless definite history (marathon
runners, psychotic patients, ecstasy users)
● Suggested rate of correction
● no more than 0.5-1mmol/hr
● Less than 8-10 mmol/L in 24 hours
● Less than 18 mmol/L in 48 hours
● Danger of rapid correction
● Central Pontine Myelinolysis (osmotic demyelination syndrome)
Asymptomatic patients with chronic hyponatraemia have a low risk of
serious neurologic sequelae but a well-described risk of osmotic
demyelination with rapid correction

Do I need to intervene ?

Do I need to intervene ?
Rx Rapid correction Risk of ODS
No Rx Risk of cerebral edema Seizures Death

ACUTE HYPONATRAEMIA
brain edema marked, minimal
brain volume regulation
CHRONIC ASYMPTOMATIC
HYPONATRAEMIA
complete brain volume
regulation
minimal brain edema
CHRONIC SYMPTOMATIC
HYPONATRAEMIA
some brain edema, partial
brain volume regulation
Endocrine Cases – Case 1
⦿ 62 yr old lady referred with acute confusion, unsteadiness, falls; preceeded by vomiting & diarrhoea a week before
⦿ On Bendrofluazide for HTN
⦿ Clinically euvolemic, GCS 14, AMT 8/10
⦿ Na 103 K 4.5 Cortisol 982 TFT normal
⦿ Serum Osm 230 Urine Osm 630 Urine Na 18
⦿ Diagnosis = Volume depletion+BFZ+ ?SIADH

Treatment
⦿ 0.9% Saline 8-12 hrly + Slow Sodium
tablets
⦿ Na improved to 109 in 24 hrs, 118 in 48
hrs
⦿ Saline and Slow Na stopped
⦿ Na continued to improve and was 126
on day3
⦿ Discharged with OP fu

Case 1 – follow-up
⦿ Represented 1 week later with agitation,
emotional lability, unable to care for
herself and her husband
⦿ Quite tearful, drooling of saliva, slow
speech and agitation
⦿ Na 135
⦿ MRI Brain

‘Increased signal in basal ganglia bilaterally, including head of caudate nuclei and the putamina as well as pons consistent with central pontine myelinolysis’

Risk factors for ODS
⦿ Serum Sodium at presentation
⦿ Duration of hyponatremia
⦿ Rate of correction
More common in :
○ Alcoholism
○ Malnutrition
○ Advanced liver disease

How quickly should I correct?
• Rule 1 : Correct hyponatraemia at the rate at which it occurred
• Rule 2 : If duration of hyponatraemia unclear, always safer to assume chronic onset
• Rule 3 : If hyponatraemia of chronic duration (onset over weeks rather than days) – : – Maximum Na rise of 8-10mmol/L over 24 hours (max 2 mmols/hr)
– Preferably much slower if not significantly symptomatic
– Be more cautious with severe hyponatraemia (Na < 110)
• Once Na at safe level (i.e. 115-120) aim for gradual correction

What is the cause ?
• Hypertonic – Significant hyperglycaemia
• High glucose concentration draws fluid from intracellular to extracellular space
• Normotonic
– Severe hyperlipidaemia • High lipid levels result in reduced plasma fraction, therefore falsely low sodium concentration
• Hypotonic
Correction for hyperglycaemia 1.6 mmol Na for every 5 mmol increase in glucose. E.g. Patient with Na of 127, Glucose of 30mmol/L. After correction –> Na = 135

Hypotonic hyponatraemia
⦿ Hypovolemic hypotonic hyponatraemia
● Solute loss
● Cerebral salt wasting
● Salt wasting nephropathy
● diuretics
⦿ Hypervolemic
● Liver cirrhosis, heart failure, nephrotic
syndrome
⦿ Euvolemic hyponatraemia (SIADH)

Is this SIADH ?
⦿ Exclude hypovolemia
⦿ Adrenal insufficiency and
hypothyroidism excluded
⦿ Drug related
⦿ Reset osmostat
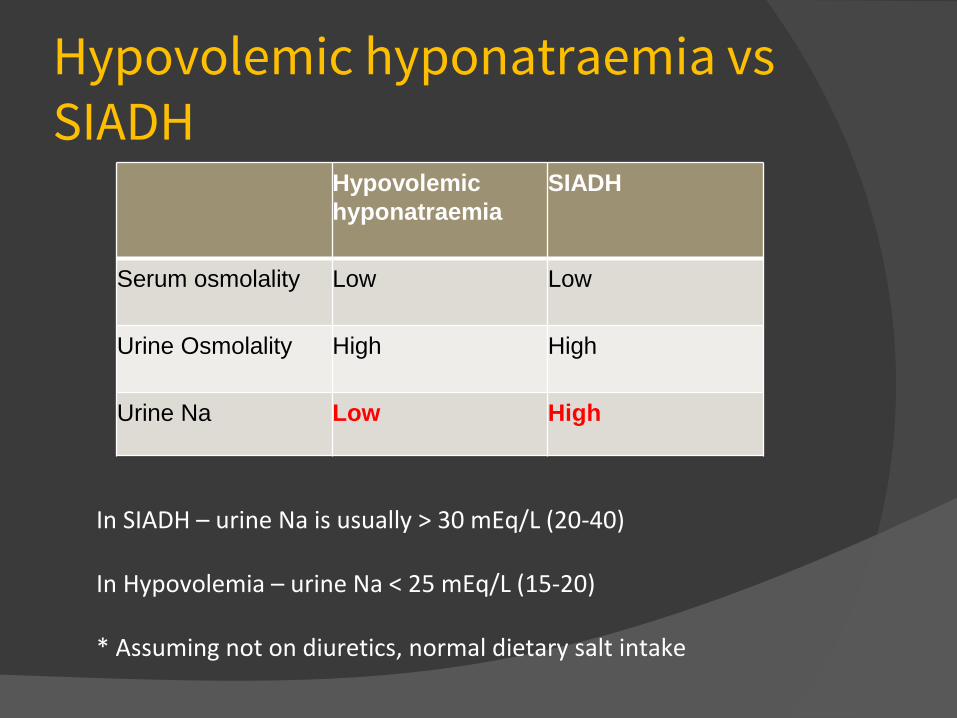
Hypovolemic hyponatraemia vs SIADH
Hypovolemic
hyponatraemia
SIADH
Serum osmolality
Low Low
Urine Osmolality
High High
Urine Na Low High
In SIADH – urine Na is usually > 30 mEq/L (20-40) In Hypovolemia – urine Na < 25 mEq/L (15-20) * Assuming not on diuretics, normal dietary salt intake

Hypovolemic hyponatraemia vs SIADH ⦿ Urine osmolality > 100 indicates impaired ability to
dilute urine
⦿ Usually secondary to raised ADH level
⦿ Note – raised ADH can be both appropriate or inappropriate
⦿ If in doubt, treat with 0.9% Saline 1000 mls over 10 hours
⦿ If Na improves, it indicates hypovolemia. If doesn’t change/falls, it is SIADH

Case 2
● 76 yr old male
● 4 day history of confusion and falls
● Fit and well
● Started on Citalopram and Zopiclone 2 weeks ago due to low mood and memory problems
● Examination unremarkable
● Na 112 K 3.2 normal renal function
● Serum osmo 230 Urine osm 283 urine Na 31
● TSH 1.3 SST normal
● CT Head – no acute infarction/haemorrage

Diagnosis ?
⦿ ? Drug-induced SIADH ? Volume depletion ⦿ Citalopram and Zopiclone stopped ⦿ Given 0.9% Saline slowly ⦿ Repeat Na 109 ⦿ Diagnosis ? What next ? ⦿ No improvement with fluid restriction
800mls/24hr ⦿ Confusion worsening , GCS 14/15 ⦿ Treated with 1.8% Saline 500 mls 50ml/hr ⦿ Na gradually improved to 124 and 132 at
discharge

Treatment options - SIADH
⦿ Treat the cause
⦿ Fluid restriction ( 800 – 1000 mls/day )
⦿ Slow Sodium tablets
⦿ Hypertonic Saline ○ 1.8% Saline 500mls, 50mls/hr
○ 3% Saline – only in ITU setting
⦿ Demeclocycline (600 – 1200 mg daily )
⦿ Tolvaptan (15-30 mg daily )

Fluid restrict or saline?
● Volume status unclear from clinical assessment ● 1000mls of 0.9% saline over 10hrs, measure urine and serum
sodium pre / post
● Severe hyponatraemia with acute neurological compromise ● Consider hypertonic saline (usually Na < 110 mmol/L)
● Dual diagnosis ● i.e. SIADH + depleted intravascular volume, e.g. in septic shock,
high-volume diarrhoea
● Initial treatment with 0.9% saline, may require intermittent hypertonic saline (1.8%) if large volumes of IV fluids required

Will fluid restriction work? General guidelines
⦿ restrict all intake consumed by drinking,not just water
⦿ aim for fluid restriction that is 500ml/d below the 24-hr urine output
⦿ do not restrict sodium intake Predictors of failure of fluid restriction*
⦿ high urine osmolality (>500 mOsm/kg H2O) ⦿ urine Na+K greater than serum [Na] ⦿ 24 hr urine output < 1500 ml/day ⦿ Increase in serum[Na] < 2mmol/day
*The urine/plasma electrolyte ratio: a predictive guide to water restriction. Furst H et al; Am J Med Sci 2000

Do slow sodium tablets work? ● SIADH vs salt wasting?
● Oral sodium tablets favored in neurosurgical units ● Role in transient aldosterone resistance?
● Does it help in SIADH? ● Excess sodium excreted in urine together with water ● Effect can be estimated from urine osmolality ● May be effective in mild SIADH (Na > 125, urine
osmolality < 500) ● Is not practical in patients with moderate to severe
SIADH as amount of oral sodium required is excessive

Effect of Slow Na in SIADH
⦿ Eg : patient with a urine osmolality of 400, taking
2 tablets QDS
⦿ 1 tablet of slow Na contains = 10mmol Na +
10mmol Cl (20 mmol solute)
⦿ 8 tablets = 160 mmol
⦿ Urine volume = 𝑠𝑜𝑙𝑢𝑡𝑒 𝑙𝑜𝑎𝑑
𝑢𝑟𝑖𝑛𝑒 𝑜𝑠𝑚𝑜=
160
400 = 0.4L = 400ml
⦿ Excess water excretion = 400 mls (160 mmol of
solute diluted in 400 ml of water gives osmolality
of 400)

Effect of Saline in SIADH

When to use Demclocycline?
⦿ Induces reversible nephrogenic diabetes
insipidus
⦿ Doses used in studies 600-1200mg daily
⦿ Effect takes atleast 72 hrs
⦿ Significant rise in 5-7 days
⦿ Risk of hypernatraemia and renal
impairment
⦿ Can be used in chronic SIADH

What about Tolvaptan?
Can be considered in the following situations ●Confimed SIADH, alternative diagnosis excluded AND
●Symptomatic Hyponatremia with Na < 125 not responding to fluid restriction (1000mls/24h) OR ●Na <125 despite fluid restriction (1000mls/24h) and discharge would be expedited with correction of hyponatremia
OR ●Definite acute onset significant hyponatremia with acute symptoms ( may consider direct treatment with tolvaptan rather than fluid restriction in select cases ) with history and findings in keeping with SIADH

How does Tolvaptan work? ⦿ Competitive ADH receptor antagonist (V2
receptor)
⦿ Causes selective water diuresis
⦿ Licensed for use in SIADH
⦿ Dose 15-30mg
⦿ Concern about possibility of too rapid correction
⦿ 1.8% of patients in SALT trials had Na rise >12 mmol in first 24 hrs
⦿ No report of CPM with Tolvaptan
* For inpatient use only after review by Endocrine Consultant

Tolvaptan
Tolvaptan not to be used in the following
circumstances: 1.Serum Na < 110 mmol/L*
2.GCS < 14 ( unless chronically low GCS )*
3.Concurrent septic shock or hypovolemic shock in addition to
pre-existing SIADH
4.Patient unable to take oral or NG fluids ( on parenteral
nutrition/IV fluids only )
* 3% Hypertonic Saline should be used cautiously in ITU in
these patients

Hypertonic saline
⦿ Indicated in patients where there is :-
● EITHER urgent need to correct symptomatic
hyponatraemia
● OR other measures unavailable/have failed
● OR dual diagnosis (hypovolaemia + SIADH) requiring
high volume / continuous IV fluid replacement therapy
⦿ Will correct hyponatraemia regardless of
underlying aetiology (however if SIADH, Na will
drop back down on stopping hypertonic saline if no
other intervention)

Hypertonic saline
Option of 1.8% saline and 3% saline 1.8% saline (308mmol of Na/L) ⦿ 500ml bags readily available (ITU/NeuroITU/pharmacy if not kept on ward)
⦿ Can be safely given via peripheral cannula on ward (only via slow infusion through a pump)
⦿ For treatment on ward - 500mls at 50mls/hr with repeat measurement of Na at the end of infusion to assess response in serum Na.
⦿ E.g. to get Na from 120 to 128, may require 1000mls of 1.8% saline/24hrs for total of 48hrs

Summary ⦿ Two main causes of hypotonic hyponatraemia in
inpatients are : hypovolemia and SIADH
⦿ Assume hyponatraemia chronic unless there is clear evidence
⦿ When treating hyponatraemia, consider the risks of cerebral edema vs risks of rapid Rx
⦿ If severe hyponatraemia (Na<110mmol/L) or neurological compromise, urgent correction with 3% Saline (irrespective of the cause) in ITU setting
⦿ Contact Endocrine team for advice

Thank you Questions ?


















