
THE TWILIGHT SERIES trauma Dandenong 2012.pdf · Permanent Teeth 2004 4. ... Epidemiology of dental...
28
21/03/12 1 THE TWILIGHT SERIES www.zimendo.com.au Phillippe O Zimet Associate Professor in Endodontics School of Dentistry and Oral Health La Trobe University 77 Stud Rd Dandenong www.zimendo.com.au [email protected] At the end of this lecture participants will be able to : 1.describe the aim and objective of trauma management. 2.discuss the aetiology of dental trauma. 3.classify dental injuries. 4.understand the effect of trauma on the pulp. 5.understand the effect of trauma on the periodontium. 6.examine a patient with dental trauma. 7.undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.Pursue endodontic management of traumatized teeth. Treatment guidelines are from: 1. Guidelines for the evaluation and management of traumatic dental injuries. International Association of Dental Trauma Updated February 2012 Part 1 Anthony J. DiAngelis, Jens O. Andreasen, Kurt A. Ebeleseder, David J. Kenny, Martin Trope, Asgeir Sigurdsson, Lars Andersson, Cecilia Bourguignon, Marie Therese Flores, Morris Lamar Hicks, Antonio R. Lenzi, Barbro Malmgren, Alex J. Moule, Yango Pohl, Mitsuhiro Tsukiboshi
Transcript of THE TWILIGHT SERIES trauma Dandenong 2012.pdf · Permanent Teeth 2004 4. ... Epidemiology of dental...

21/03/12!
1!
THE TWILIGHT SERIES
www.zimendo.com.au
Phillippe O Zimet Associate Professor
in Endodontics School of Dentistry
and Oral Health La Trobe University
77 Stud Rd Dandenong
www.zimendo.com.au
!
!
!
!
!
!
!
! !
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!
Treatment guidelines are from:
1. Guidelines for the evaluation and management of
traumatic dental injuries.
International Association of Dental Trauma
Updated February 2012 Part 1 Anthony J. DiAngelis,
Jens O. Andreasen, Kurt A. Ebeleseder, David J. Kenny, Martin Trope, Asgeir Sigurdsson, Lars Andersson, Cecilia
Bourguignon, Marie Therese Flores, Morris Lamar Hicks,
Antonio R. Lenzi, Barbro Malmgren, Alex J. Moule, Yango
Pohl, Mitsuhiro Tsukiboshi

21/03/12!
2!
Definition and Diagnosis are from: 2. AAPD Trauma Guide 2007
3. AAPD Guideline on Pulp Therapy for Primary and Young
Permanent Teeth 2004
4. The Dental trauma Guide http://www.dentaltraumaguide.org
5. Traumatic Dental Injuries – A
Manual
Highly recommended text
Andreasen et al 2011
!
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!
AIM of Trauma Management:
•!Maintain, preserve or reinstate the
original dentition
Objective of Trauma Management:
•!Preserve the pulp
•!Preserve the periodontal ligament
•!Maintain aesthetics of the dentition
•!Maintain function of the dentition
•!Ensure comfort of the dentition

21/03/12!
3!
Want to avoid treatable pathology that may result in loss of tooth (such as inflammatory resorption) or patient symptoms
such as pulp necrosis or pulpitis.
A parent’s nightmare
Pathology may not be evident early or provide confusing signs and symptoms. May get necrosis
with infection late such as after calcification.
How do we assess and manage?
Sitra yusuf!
18 09 08 Nov 2010
Every effort is made to preserve the pulp of the immature permanent tooth, or induce
revascularization or regeneration of pulp tissue.
March 2007! June 2009!
mccartney!
05 09 07!130807! 210808!
160710!
•!avulsed teeth 32, 31 and 42 some 5 days ago. Teeth placed in milk soon after for 2 hr
•!note from the referring practitioner
regarding an alveolar fracture
•!Clinical examination revealed imbrucation
of the lower anterior dentition with a lingual splint
•!43, 42, 41, 32 and 31 to be non responsive
to pulp testing.
•!Treatment?
!

21/03/12!
4!
Gray 300610!
The response
of the teeth
to trauma
is variable
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!
Remember dental trauma can happen any time and any place. The first course of treatment is
prevention.!
EPIDEMIOLOGY - Relation to
prevention
•!Importance of mouthguard and face
shields
•!Use of seatbelts
•!Use of safe toys eg swings
Ref: Monash University Accident
Research Centre, Newsome
(mouthguards) IJPD 2001, Shahim
ADJ 2006, Bastone ADJ 2000) !

21/03/12!
5!
Should football players wear custom fitted mouthguards? Results from a group randomised controlled trial
C Finch, R Braham, A McIntosh, P McCrory and R Wolfe
Injury Prevention 2005;11:242-246
• This is the first randomized controlled trail of the
effectiveness of protective equipment in community level
Australian football, and one of a few worldwide in any sport.
• Players who were allocated to the
custom fitted mouthguard study arm had
a significantly lower rate of head and
orofacial injuries than all other players.
Mouthguards in sport activities : history, physical properties and injury prevention effectiveness. Knapik JJ, Marshall SW, Lee RB, Darakjy SS, Jones SB, Mitchener TA,
delaCruz GG, Jones BH. Sports Med. 2007;37(2):117-44
Studies that have examined injuries among mouthguard
users and nonusers are of highly variable methodological quality. However, published research consistently shows that
mouthguards offer significant protection against orofacial
injuries.
Meta-analysis indicates that the overall risk of an orofacial injury is 1.6–1.9 times higher when a mouthguard is not worn,
relative to wearing a mouthguard.
Epidemiology of dental trauma; a review of the literature
Bastone, Freer and McNamara
ADJ 2000
•!Accidents within and around the home were the major sources of injury to the primary dentition
•!Accidents at home and school accounted for most of the
injuries to the permanent dentition.
SO BE READY TO TREAT TRAUMA AT ANY TIME!!
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!

21/03/12!
6!
WHO CLASSIFICATION (1992) -DENTAL INJURIES!
TREAT IN ASSOCIATION WITH HARD! !TISSUE/PULP!
1. PERIODONTAL TISSUES!1.1. Concussion!1.2. Subluxation!1.3. Extrusive Luxation(peripheral dislocation,partial avulsion)!1.4. Lateral luxation!1.5. Intrusive luxation(Central dislocation)!1.6. Avulsion (exarticulation)!
2. INJURIES TO SUPPORTING BONE!2.1. Comminution (splintering) of the mandibular or maxillary alveolar socket!2.2. Fracture of the mandibular or maxillary socket wall!2.3. Fracture of the mandibular or maxillary alveolar process!2.4. Fracture of the mandible or maxilla!
3. GINGIVAE OR ORAL MUCOSA!3.1. Laceration of gingivae or oral mucosa (includes tear and degloving)!3.2. Contusion of gingivae or oral mucosa (sub mucosal haemorrhage)!3.3. Abrasion of gingivae or oral mucosa (superficial)!
WHO CLASSIFICATION (1992) -DENTAL INJURIES!
!4. HARD DENTAL TISSUES AND PULP!
1.! Enamel infraction!
2.! Enamel fracture (uncomplicated crown! !fracture)!
3.! Enamel/dentine fracture (uncomplicated! !crown ! fracture)!
4.! Complicated crown fracture!
5.! Uncomplicated crown/root fracture!
6.! Complicated crown /root fracture!
7.! Root fracture!
The common theme following trauma to the dentition is that following dental
trauma there may injury to the:
•! Pulp
•! Tooth
•! Separation or crushing of supporting tissues (gingivae, PDL, bone)
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!

21/03/12!
7!
RESULTS OF TRAUMA-MANY TISSUES
AFFECTED BY TRAUMA!
"
"
"!
•"
•!
!
Nothing/Physiologic surface resorption"Pulp healing
•!Internal Resorption!
•!External Resorption (Infection "Induced / Inflammatory)!
•!
External Resorption (Replacement)"Ankylosis"
!•!Pulpal Canal Obliteration"!•! Invasive Cervical Resorption "•! Pulpal ischaemia - Necrosis or infection"
•! Transient apical internal resorption"
•! Transient apical breakdown"
•! Transient/permanent marginal breakdown"
•!Following dental trauma there may injury to the:
•! Pulp
•! Tooth
•! Separation or crushing of supporting
tissues (gingivae, PDL, bone)
Yusuf 1711 08
Consequences:
What does this picture
represent?
•! haemolysis vital
pulp •! haemolysis with
ischaemia
•! neuropraxia
•! neurotmesis
•! pulp necrosis •! pulp necrosis with
infection!
Yusuf 1711 08
121109 220210 180908
Consequences:
At what point is
treatment required?

21/03/12!
8!
tigas!
Pulp necrosis and infection:
19 01 10 19 07 10
Perera presurgical 220811!
Perera
220811!
Pulp necrosis and infection:
22 08 11
Battle open
apex and pulp
necrosis
280907!
Pulp necrosis – tooth fails to develop. Treat when signs or symptoms of infection occur:
280907
21 09 04 18 10 04
22 12 04 14 11 05
04 09 08
Prevalence of outcome following trauma
to 899 injured teeth (Hecova Dent Trauma 2010):
Follow up: In children, pulp necrosis was usually
diagnosed within 6 months after the injury
(91.9% of all injured teeth) and in virtually all
teeth within one year.
In patients older than 15 years, pulp necrosis
was predominantly diagnosed later than 6
months (61.7% of all cases) or even later than
12 months (40%) after the trauma

21/03/12!
9!
trzcinski!
Calcific Metamorphosis (Pulpal Calcific Obliteration)
Aetiology
•!Impact injury that did not result in necrosis
•!Vital pulp
•!Process of calcification- Temporary disruption in blood supply leads to deposition of tertiary dentine (irregular
secondary) dentine. Can occur with all injury types.
19 07 07 29 04 08
16 07 11
Sandra Ennor 21 yellow from
calcified pulp 03 05 10!
70% of teeth with PCO discolour. The colour may be yellow or even grey!
!
Robertson A etal Incidence of pulp necrosis subsequent
to pulpcanal obliteration from trauma of permanent
incisors. J Endod 1996:22:557-560
Root development
!!
Crown fracture
Prognosis: !
Adeleke O Oginni and Comfort A Adekoya-Sofowora
2007
Pulp caclification can result in coronal discolouration which can occur some years
later siderus calcification
and pap
170709
280808 021008 170709
•!1% annual risk of pulp necrosis and signs of infection

21/03/12!
10!
Prevalence of outcome following trauma
to 899 injured teeth (Hecova Dent Trauma 2010):
!
Pulp canal obliteration
extrusive luxations, 62.5% with open apices
and in 8.6% teeth with closed apices.
lateral luxation, 34.8% in teeth with
incomplete root formation and in 5.7% teeth
with complete root development.
Following dental there may injury to the: •! Pulp
•! Tooth
•! Separation or crushing of supporting
tissues (gingivae, PDL, bone)
Perera presurgical
220811 fracture
130112
130112 290410
Following dental trauma there may injury to the:
•! Pulp
•! Tooth
•! Separation or crushing of supporting
tissues (gingivae, PDL, bone) •! Separation cause collagen to cleave
and some cell damage

21/03/12!
11!
Following dental there may injury to the: •! Pulp
•! Tooth
•! Separation or crushing of supporting tissues
(gingivae, PDL, bone)
•! Crushing damages the cellular and intercellular systems.
•! Damaged tissue is removed by macrophages and
osteoclasts before traumatized tissue is repaired
McCarthy!
Bony healing!
!
•!impaction stage (clot – gelatinous coagulum) •!inflammation stage 7 days
•!primary soft callus formation stage 2 weeks
•!callus mineralisation stage 4th week to 10th week
•!callus remodellation stage
Soft Tissue
Collagen at margins 3 days
Granulation tissue fills defect 7 days
Scarring with Collagen and decreasing Vascularity 2 weeks Connective tissue with Epidermis 1 month
!Can I still reposition teeth at 5 days? !
McCarthy!
PDL!
!
•!By 2 weeks 2/3 of the mechanical strength of the PDL is restored
PULP
If vascular supply is severed, ingrowth of new vessels begins
at 4 days
!
Can I still reposition teeth at 5 days? !
Following dental there may injury to the: •! Pulp
•! Tooth
•! Separation or crushing of supporting tissues (gingivae,
PDL, bone)
•! In complicated luxation, intrusion or avulsion injuries the loss of protecting cementoblast layer and epithelial rests
of Malassez allows osteoclasts and macrphages to
remove damaged PDL and cementum on root surface.

21/03/12!
12!
Definition of resorption
•! Loss of hard tissue by
physiologic or pathologic means
due to activation of clastic cells
130807 300409
1. Alveolar changes - Transient marginal breakdown
Following injury to the supporting bone, remodelling
occurs with fabrication of granulation tissue.
This is seen as a widened PDL space. After 2-3 months the periodontium usually reforms
This can also be seen at the apex as transient apical
breakdown (a transient apical radiolucency)
cril
ly!
02 04 07! 28 05 07!
1. Alveolar changes -Permanent marginal breakdown
Following injury to the supporting bone,
remodelling occurs with fabrication of
granulation tissue.
This is seen as a widened PDL space.
In some instances the healing of the bone
does not occur.
This may be due to the degree of trauma,
or presence of infection.
Bony sequestrum may even occur.
May be seen after lateral luxations,
avulsion, intrusion, alveolar fracture or jaw
fracture
130807
300409
2. Tooth resorption:
Andreasen’s Classification of
resorption:
1.! Internal
inflammatory
2.! External:
•! Surface
•! Inflammatory
•! Replacement

21/03/12!
13!
2. Tooth resorption
Linsdkog/Heithersay’s
Classification:
This classification is clinically
based subdividing resorptions into
three broad groups:
(1) trauma induced tooth
resorption;
(2) infection induced tooth
resorption;
(3) hyperplastic invasive tooth
resorptions.
Linsdkog/Heithersay’s
Classification (Heithersay ADJ
2007): "
!This classification is clinically based
subdividing resorptions into three broad
groups:
(1) ! trauma induced tooth resorption;
•! Surface resorption
•! Transient apical internal resorption
•! Pressure resorption and orthodontic
resorption
•! Replacement resorption
•! Ankylosis
Linsdkog/Heithersay’s
Classification (Heithersay ADJ
2007): "
!This classification is clinically based
subdividing resorptions into three broad
groups:
(1) ! trauma induced tooth resorption;
•! Surface resorption
•! Transient apical internal resorption
•! Pressure resorption and orthodontic
resorption
•! Replacement resorption
•! Ankylosis
maclean not properly repositioned 161211!
Minimize surface resorption and
maximize pulpal healing
by ensuring teeth are
repositioned correctly
!
Maclean!

21/03/12!
14!
Linsdkog/Heithersay’s
Classification (Heithersay ADJ
2007): "
!This classification is clinically based
subdividing resorptions into three broad
groups:
(1) ! trauma induced tooth resorption;
•! Surface resorption
•! Transient apical internal resorption
•! Pressure resorption and orthodontic
resorption
•! Replacement resorption
•! Ankylosis
Jacob peters!
Transient apical internal
resorption
•!TAIR may be associated with colour change
•!Problem is that resolution of colour change
does not always occur and a more invasive
approach (commencement of RCT) may still be
warranted (Heithersay 2007).
•!When I see colour change I am now less
inclined to watch.!
Deege
n!
01 02 07! 22 03 07! 10 05 07
Transient apical internal resorption may be associated with transient
apical breakdown
Linsdkog/Heithersay’s
Classification (Heithersay ADJ
2007): "
!This classification is clinically based
subdividing resorptions into three broad
groups:
(1) ! trauma induced tooth resorption;
•! Surface resorption
•! Transient apical internal resorption
•! Pressure resorption and orthodontic
resorption
•! Replacement resorption
•! Ankylosis

21/03/12!
15!
Compare Inflammatory Resoprtion to Replacement
Resorption
RR is affected by the status of
the periodontal ligament.
There is minimal impact from
endodontic treatment. Most
influence is from
•!apical diameter for intrusion
•!initial management in order to
maintain vitality of the periodontal ligament fibers
after avulsion!
Tooth survival improves with proper management. Either replace or store: 11 and 21 were placed in milk
after 5 minutes for about 1 hour. 11 was passively
managed.
As 21 showed signs of resorption, active management.
Is this inflammatory or replacement resorption?!
30.05.04!
peppler!
09 10 09 11 is positive to
EPT. Bizarre!
Prevalence of outcome following trauma
to 899 injured teeth (Hecova Dent Trauma 2010):
!
Root resorption:
prevalence of replacement resorption was
2.9% in laterally luxated teeth immature teeth
and of mature teeth
42.9% of avulsed and replanted teeth (9 of 17
immature teeth and 12 of 32 mature teeth).
21/03/12!
16!
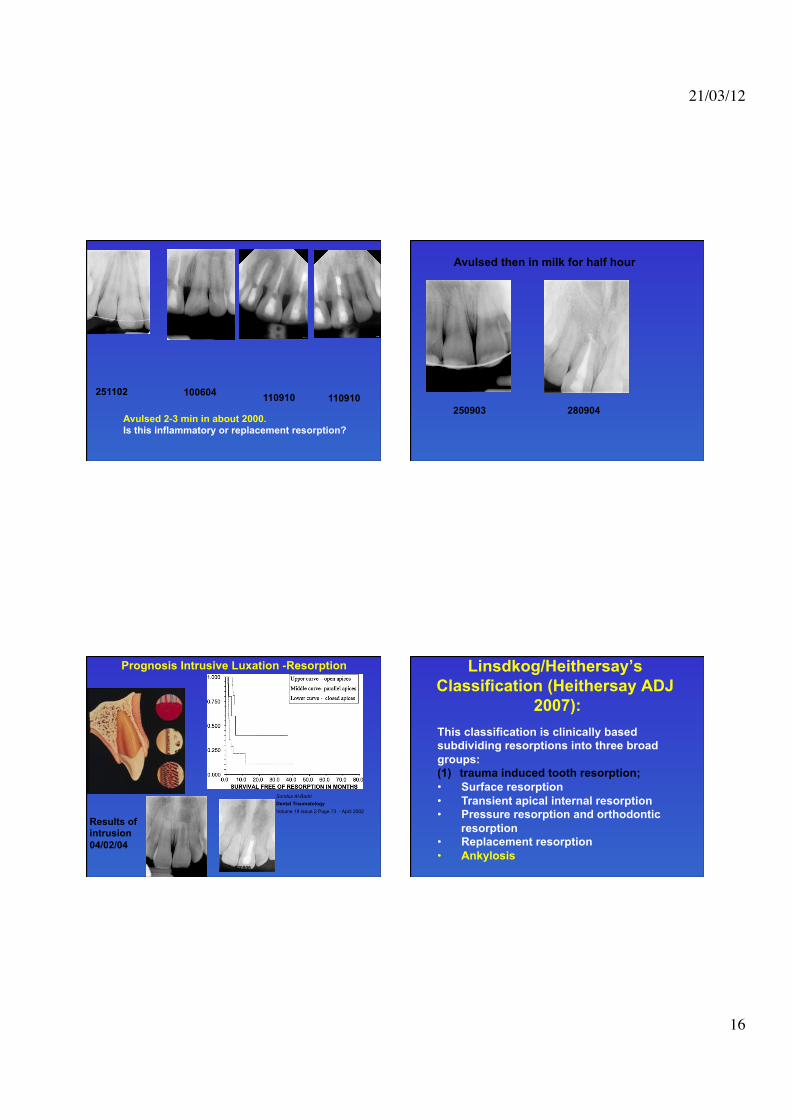
Bsmith 100604avulse
2-3 min in
about 2000
100604 110910
110910
Avulsed 2-3 min in about 2000. Is this inflammatory or replacement resorption?
251102
James Avulsed Milk
half hour 280904!
280904 250903
Avulsed then in milk for half hour
collis!
Prognosis Intrusive Luxation -Resorption
Results of intrusion
04/02/04!
Sondos Al-Badri
Dental Traumatology
Volume 18 Issue 2 Page 73 - April 2002
120506!
Linsdkog/Heithersay’s
Classification (Heithersay ADJ
2007): "
!This classification is clinically based
subdividing resorptions into three broad
groups:
(1) ! trauma induced tooth resorption;
•! Surface resorption
•! Transient apical internal resorption
•! Pressure resorption and orthodontic
resorption
•! Replacement resorption
•! Ankylosis

21/03/12!
17!
•!Results in interface and fusion between bone and
tooth
Ankylosis!
Linsdkog/Heithersay’s
Classification:"
!This classification is clinically based
subdividing resorptions into three broad
groups:
(1) trauma induced tooth resorption;
(2) infection induced tooth resorption;
Associated with pulpal necrosis and
infection which may or may not be of
traumatic origin
Linsdkog/Heithersay’s
Classification:
This classification is clinically
based subdividing resorptions into
three broad groups:
(2) infection induced tooth
resorption;
•!Internal inflammatory (infective)
root resorption
•!External inflammatory root
resorption
Linsdkog/Heithersay’s
Classification:
This classification is clinically
based subdividing resorptions into
three broad groups:
(2) infection induced tooth
resorption;
•!Internal inflammatory (infective)
root resorption
•!External inflammatory root
resorption

21/03/12!
18!
Jacob peterson!
071008!
09 02 09!09 12 08!
21 08 08!
23 06 08!
23 06 08!
Subluxation
Linsdkog/Heithersay’s
Classification:
This classification is clinically
based subdividing resorptions into
three broad groups:
(2) infection induced tooth
resorption;
•!Internal inflammatory (infective)
root resorption
•!External inflammatory root
resorption
If you don!t follow up correctly this can happen: Prevalence of outcome following trauma
to 899 injured teeth (Hecova Dent Trauma 2010):
!
Root resorption:
inflammatory resorptions were observed in
33.3% of intruded teeth with immature teeth
and 33.3% mature teeth.

21/03/12!
19!
Prevalence of outcome following trauma
to 899 injured teeth (Hecova Dent Trauma 2010):
!
Root resorption:
external resorptions of the root substances in
16.2% of all teeth.
inflammatory resorptions were observed in
4.5% of laterally luxated immature teeth and
of 14.9% of mature teeth.
Linsdkog/Heithersay’s
Classification:
This classification is clinically based
subdividing resorptions into three broad
groups:
(1) ! trauma induced tooth resorption;
(2) infection induced tooth resorption;
(3) hyperplastic invasive tooth
resorptions.
•!Internal replacement (invasive)
resorption
•!Invasive coronal resorption
•!Invasive cervical resorption
•!Invasive radicular resorption
tigas!
What do the statistics mean clinically:
Tooth 32 was avulsed while the adjacent teeth were
luxated. Patient replanted the tooth back into the
socket himself within about 15-20min.
10 03 11 19 01 10 19 07 10 21 11 11
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!

21/03/12!
20!
MATTHEW YOUSSEF email 21
march 2012!
Intra-oral examination for
all trauma
Clinical • Tooth colour
• Millimetre
Dislocation (Vertical/Horizontal) • Loosening/moblity
• Tenderness to palpation
• Tenderness to percussion • Thermal sensibility test; CO2, EPT Thermal sensitivity test; hot, cold
• Mucosal laceration • Locate missing segments Note craze lines (infractures), fracture
Occlusal interference Radiographic (hard and soft tissue): May need to take multiple vertical and
horizontal angles
• •!
•
•
!At the end of this lecture participants will be able to : 1.!describe the aim and objective of trauma management. 2.!discuss the aetiology of dental trauma.
3.!classify dental injuries.
4.!understand the effect of trauma on the pulp.
5.!understand the effect of trauma on the periodontium.
6.!examine a patient with dental trauma.
7.!undertake acute management of traumatized teeth (including diagnosis and treatment planning). 8.!Pursue endodontic management of traumatized teeth.
"
!!
!
!
!
" !
!
Summary of Dental Trauma Triage
Table 1. The Dental Trauma Algorithm for
medics and corpsmen (translated from
Hebrew)
Yehuda Zadik
Dental Traumatology 2008; 24: 698–701;

21/03/12!
21!
1. Loss of consciousness or confusion?
Nausea or vomiting?
Facial or jaw deformation? Haematoma
in the face or in the floor of the mouth? Yes. Immediately refer to
Emergency Department
2. Avulsion ("knock-out!) of a tooth? Yes. Find the tooth. Hold it by the crown and
wash under gentle running saline or water
(Do not scrub!). Replant the tooth into the
Socket.
Success in replantation?
Yes. Refer to a
dentist within
24 h. Continue to #
3
No. Place the tooth in
milk, saline or inside
the patient!s mouth.
Refer immediately to a
dentist or ED
3. Tooth displacement (other than
avulsion)?
No
No
Yes. Refer to a dentist
within 24 h
No
If can!t see the tooth confirm is it intruded, avulsed
or coronal fracture. Try to account for tooth or
segments (?avulsion, embed in lip, inhaled)
4. Tooth mobility (other than
avulsion)?
Yes More than 2 mm
mobility?
Yes. Refer to a dentist within
24 h. Continue to # 5 No
5. Tooth fracture? Yes. Tooth fracture with pulp
exposure, intra-coronal
bleeding or pain?
Yes. Refer to a dentist
within 24 h. Continue to # 6
No
Is restoration needed?
Yes. Refer to a dentist within
48 h
No
No
5. Tooth fracture? Yes. Tooth fracture with pulp
exposure, intra-coronal
bleeding or pain?
Yes. Refer to a dentist
within 24 h. Continue to # 6
The tooth is
fractured but
no pulp
exposure. Is restoration needed?
Yes. Refer to a dentist within
48 h. Continue to #6
No
No
6. Soft tissue laceration?
No Yes. Through-and-through
laceration
Yes. Superficial
laceration
A suspected foreign body
embedded in the soft tissue and/or
infection
Yes. Refer to a dentist
or Emergency Department
within several hours
Root development !!
Prognosis – Pulp healing: !

21/03/12!
22!
FOLLOW UP
3 weeks
6 weeks
3 months
6 months (equals one year)
12 months (equals two years)
24 months (equals four years)!
!
General Patient instructions •!Soft diet for up to two weeks.
•!Brush teeth with a soft toothbrush after
each meal.
•!Use a chlorhexidine (0.1%) mouth rinse twice a day for 1 week.
!
Follow up as for all trauma:
Any symptoms
Clinical signs
•! Sinus tract stoma or swelling
•! Gingivitis
•! Pocket depth
•! Recession
•! Tooth Colour
•! Loosening
•! Tenderness to palpation
•! Tenderness to percussion
•! Thermal test (sensibility, sensitivity)
•!Radiograph-mm dislocation, pulp calcification, continued root
development, marginal bone loss, periradicular radiolucency, resorption.!
In Summary when do I perform endodontic treatment? IADT 2011 suggest 2 signs and symptoms are required to
suggest pulpal infection.
When I think the pulp is infected (not just necrotic)
1.!Radiographic: •!Periapical lesion not resolve or increasing
•!Size of pulp chamber (internal resorption)
•!Sign of external inflammatory resorption
•!Pulp calcification is a sign of pulp vitality
•!Continued root development
2 !Clinical:
•!Response to pulp testing: calcification vs necrosis (but is
it infected?) vs vascular intact •!Colour (calcification vs necrosis vs transient hyperaemia)
•!Sinus tract stoma
•!Prolonged TTP
3. Tenderness to percussion
Andreasen found that the only sign significantly
related to pulp necrosis was tenderness to
pecussion following tooth luxation. (Andreasen et al;
Textbook and colour Atlas of Traumatic Injuries to the teeth – 4th Edition p 378 from Andreasen FM,
Endod Dent Traumatol 1989;5:111-31)
"!

21/03/12!
23!
4. Coronal discolouration
Andreasen states that grey colour changes can be
seen in the crown even 2 to 3 weeks after trauma.
This may be accompanied by radiographic periapical
radiolucency. (Andreasen et al; Textbook and colour Atlas of Traumatic Injuries to the teeth – 4th Edition p
378 from Andreasen FM, Endod Dent Traumatol
1989;5:111-31).
But even colour changes may be transitory and as with apical radiolucency may resolve and reverse
within 1 year. (Andreasen et al; Textbook and colour
Atlas of Traumatic Injuries to the teeth – 4th Edition p
378 from Andreasen FM, Endod Dent Traumatol 1989;5:199 and 201).
"!
4. Coronal discolouration
Grey coronal colour change is often, not always,
related to pulpal haemorrhage or pulp necrosis.
Yellow coronal colour change is related to pulpal calcification.
Clinically Heithersay feels that if discoloration begins
it rarely reverses (ADJ 2007). If there is no change in
3 months I begin RCT.
"!
When do I Splint teeth?""
Reason for splinting:"1.! Aid repair"
2.! Comfort-loose, TTP"
!
!
•!The prognosis for the healing outcome is more dependent on the type of injury rather
than the effect of the splinting.
•!the use of cap splints and orthodontic
bands were associated with a greater frequency of pulp necrosis (31, 38) and pulp
canal obliteration (45) when compared with
acid etch resin splints and no splinting.
•!the majority of the selected studies suggested that an extended fixation period is
not an indicator for a poor healing outcome.
Review by Kahler and Heithersay. Dental Traumatology 2008

21/03/12!
24!
This is not correct position
James
McCartney!
Original badly placed
Corrected with orthodontics and associated resorption
What does
treatment delay
mean?
Arnes Muhic 090909
fracture trauma palatal 12!
Andreasen, J.O., Andreasen, F.M., Skeie, A., Hjørting-Hansen, E. &
Schwartz, O.Effect of treatment delay upon pulp and periodontal
healing of traumatic dental injuries – a review article.Dental
Traumatology 18 (3), 116-128.2002
Fig. 18. Effect of treatment delay upon healing of 98 luxated teeth with
dislocation. From Eklund et al., 1976 (22).

21/03/12!
25!
Kinga Wojciechowska
Trauma displaced 11
041208!
1.3 Extrusive Luxation!
21 02 08.! 15 01 09.!
Cayla 190208!
21 02 08!
17 03 08!17 03 08!
24 06 09!
patients archibald
donahue
intrusion!
1.5 Intrusive Luxation
2 weeks!

21/03/12!
26!
IADT 2011 Guidelines for intrusion:
Incomplete root formation:
•! Allow eruption without intervention
•! If no movement in 3 weeks initiate orthodontic
repositioning •! If tooth is intruded more than 7mm, reposition surgically or
orthodontically.
Teeth with complete root formation:
Allow eruption without intervention if intruded less that 3mm.
If no movement in 3 weeks initiate orthodontic or surgical repositioning to limit chance of ankylosis.
If tooth is intruded more than 7mm, reposition surgically or
orthodontically.
Teeth with closed apices will require RCT – commence 2 to 3 weeks after repositioning.
Once an intruded tooth has been repositioned surgically or
orthodontically – stabilize for 4 to 6 weeks.
Summary of the three methods are only partly evidence based. (From www.dentaltraumaguide.org)
Spontaneous eruption
This is the treatment of choice for deciduous/primary teeth
and for permanent teeth with incomplete root formation.
This treatment has been shown to lead to significantly fewer healing complications than orthodontic and surgical
repositioning. If no movement is noted within 3 weeks,
recommend rapid orthodontic repositioning.
Orthodontic repositioning
This treatment may be preferred for patients with delayed treatment. This allows repair of marginal bone in the socket
along with the slow repositioning of the tooth.
Surgical repositioning
This treatment technique is preferable in acute phase. Intrusion with major dislocation of the tooth (approximately
more than half a crown length) may be an indication for
surgical repositioning.
!
Root canal treatment should be considered in all cases with completed root formation where the
chance of pulp revascularization is unlikely.
Endodontic therapy should preferably be initiated
within 3-4 weeks post-trauma.
!
Andreasen, J.O., Andreasen, F.M., Skeie, A., Hjørting-Hansen, E. &
Schwartz, O.Effect of treatment delay upon pulp and periodontal healing
of traumatic dental injuries – a review article.Dental
Traumatology 18 (3), 116-128.2002!
Fig. 6. Effect of treatment delay upon pulp
healing of 38 complicated crown fractures treated by pulp capping. From Fuks et al., 1982

21/03/12!
27!
Andreasen, J.O., Andreasen, F.M., Skeie, A., Hjørting-Hansen, E.
& Schwartz, O.Effect of treatment delay upon pulp and
periodontal healing of traumatic dental injuries – a review
article.Dental Traumatology 18 (3), 116-128.2002
Fig. 12. Effect of treatment delay upon pulp
healing of 345 root fractures. From Cvek et al., 2002 (34).
taliscott!
12 11 08!180808! 22 06 09!
If pulp capping is not successful try
revascularization rather
than calcium hyrdoxide
or MTA apexification.
This is different to Follow-up procedures for avulsed permanent teeth:
•!If root canal treatment is indicated (teeth with closed apex),
the ideal time to begin treatment is 7- 10 days postreplant.
•!Calcium hydroxide is recommended for intra canal medication for up to one month followed by root canal filling
with an acceptable material.
•!An exception is a tooth that has been dry for more than 60
minutes before replantation – in such cases the root canal treatment may be done prior to replantation.
•!In teeth with open apices, that have been replanted
immediately or kept in appropriate storage media, pulp revascularization is possible. Root canal treatment should be
avoided unless there is clinical and radiographic evidence of
pulp necrosis.

21/03/12!
28!
•!In cases of replanted teeth where endodontic treatment is not yet indicated teeth should be
monitored by frequent controls during the first year
(once a week during the first month, 3, 6, and 12
months) and then yearly thereafter.
•!Clinical and radiographic examination will provide
information to determine outcome.
SUMMARY: My preference is to give teeth and pulps the benefit of the doubt and treat as necessary as we can induce
periapical lesions to heal:
Arnes Muhic 090909
fracture trauma palatal 12!
What to do with this case?


















