
Clinical management of severe external root resorption to external root resorption in either the...
6
Case Report Chin Dent J 2005‧Vol 24‧No 1 59 Received: November 23, 2004 Accepted: February 19, 2005 Reprint requests to: Dr. Chun-Pin Lin, School of Dentistry, College of Medicine, National Taiwan University and National Taiiwan University Hospital, No. 1, Chang Te Street, Taipei, Taiwan 10048, ROC. Clinical management of severe external root resorption TIEN-CHUN KUO 1,2,3 YA-AN CHENG 1 CHUN-PIN LIN 1,2 1 Graduate Institute of Clinical Dentistry, National Taiwan University, Taipe, Taiwan, ROC. 2 Department of Dentistry, National Taiwan University Hospital, Taipei, Taiwan, ROC. 3 Department of Dentistry, Taiwan Adventist Hospital, Taipei, Taiwan, ROC. This case demonstrates external root resorption arrest and formation of an apical barrier by conventional endodontic therapy combined with calcium hydroxide dressing and a mineral trioxide aggregate (MTA) apical plug. The upper left central incisor exhibited severe external root resorption, and a periapical radiolucent lesion received root canal treatment combined with calcium hydroxide dressing for over 4 years. The dressing was renewed every 3 months, and the coronal portion was sealed with composite resin. After detection of the apical barrier, a MTA apical plug backfilled with gutta-percha was performed and the access carity was restored with composite resin. The patient has been regularly recalled every 6 months, and no symptoms or signs hare been noted. Radiography showed the apical lesion healed and the external root resorption had been arrested after 1 year.(Chin Dent J, 24(1):59-63, 2005) Key words: external root resorption, calcium hydroxide, apexification. External root resorption occurs on the outer surface of the root, and the causes for this may vary. There are several types of external root resorption with the most common being external inflammatory root resorption. It may arise as a sequela of traumatic injuy, orthodontic tooth movement, or chronic infection of the pulp or periodontal structures 1 . External inflammatory root resorption is considered a major resorptive condition without symptoms. The treatment of external inflammatory resorption is dependent on the etiology; nonsurgical root canal treatment combined with a calcium hydroxide dressing was recommended by Andreasen 2 . Mineral trioxide aggregate (MTA), well known for its great biocompatibility, has demonstrated excellent sealing ability in studies of dye penetration and bacterial leakage even under blood contamination conditions 3-5 . MTA is widely applied in root-end filling, perforation repair, and pulp capping. It can induce regeneration of periradicular tissues, such as bone and cementum. The following case report demonstrated nonsurgical root canal treatment of severe external root resorption and the use of MTA as an apical plug to promote periapical healing of an open apex. CASE PRESENTATION A 19-year-old female patient was referred from the orthodontic department for evaluation and treatment of the upper left central incisor. The tooth had suffered previously from a traumatic injury for several years central. The patient mentioned that the tooth had been treated in a local dental clinic nearly a year ago and no symptoms had been noted since then. Her medical history was noncontributory. Clinical examinations revealed no mobility of the upper left central incisor 6 , and the pocket depths around the tooth were within a normal range. Palpation and percussion tests induced no discomfort or pain. The access cavity had been sealed with cotton and Caviton ® . The periapical radiographic film showed several resorpted bowl-shaped lesions on the external surface of the root combined with a radiolucent lesion around the root apex, and the root
Transcript of Clinical management of severe external root resorption to external root resorption in either the...
Case Report
Chin Dent J 2005‧Vol 24‧No 1 59
Received: November 23, 2004 Accepted: February 19, 2005 Reprint requests to: Dr. Chun-Pin Lin, School of Dentistry, College of
Medicine, National Taiwan University and National Taiiwan University Hospital, No. 1, Chang Te Street, Taipei, Taiwan 10048, ROC.
Clinical management of severe external root resorption
TIEN-CHUN KUO 1,2,3 YA-AN CHENG 1 CHUN-PIN LIN 1,2
1 Graduate Institute of Clinical Dentistry, National Taiwan University, Taipe, Taiwan, ROC. 2 Department of Dentistry, National Taiwan University Hospital, Taipei, Taiwan, ROC. 3 Department of Dentistry, Taiwan Adventist Hospital, Taipei, Taiwan, ROC.
This case demonstrates external root resorption arrest and formation of an apical barrier by conventional endodontic therapy combined with calcium hydroxide dressing and a mineral trioxide aggregate (MTA) apical plug. The upper left central incisor exhibited severe external root resorption, and a periapical radiolucent lesion received root canal treatment combined with calcium hydroxide dressing for over 4 years. The dressing was renewed every 3 months, and the coronal portion was sealed with composite resin. After detection of the apical barrier, a MTA apical plug backfilled with gutta-percha was performed and the access carity was restored with composite resin. The patient has been regularly recalled every 6 months, and no symptoms or signs hare been noted. Radiography showed the apical lesion healed and the external root resorption had been arrested after 1 year.(Chin Dent J, 24(1):59-63, 2005)
Key words: external root resorption, calcium hydroxide, apexification.
External root resorption occurs on the outer
surface of the root, and the causes for this may vary. There are several types of external root resorption with the most common being external inflammatory root resorption. It may arise as a sequela of traumatic injuy, orthodontic tooth movement, or chronic infection of the pulp or periodontal structures 1. External inflammatory root resorption is considered a major resorptive condition without symptoms. The treatment of external inflammatory resorption is dependent on the etiology; nonsurgical root canal treatment combined with a calcium hydroxide dressing was recommended by Andreasen 2.
Mineral trioxide aggregate (MTA), well known for its great biocompatibility, has demonstrated excellent sealing ability in studies of dye penetration and bacterial leakage even under blood contamination conditions 3-5. MTA is widely applied in root-end filling, perforation repair, and pulp capping. It can
induce regeneration of periradicular tissues, such as bone and cementum. The following case report demonstrated nonsurgical root canal treatment of severe external root resorption and the use of MTA as an apical plug to promote periapical healing of an open apex.
CASE PRESENTATION
A 19-year-old female patient was referred from the orthodontic department for evaluation and treatment of the upper left central incisor. The tooth had suffered previously from a traumatic injury for several years central. The patient mentioned that the tooth had been treated in a local dental clinic nearly a year ago and no symptoms had been noted since then. Her medical history was noncontributory.
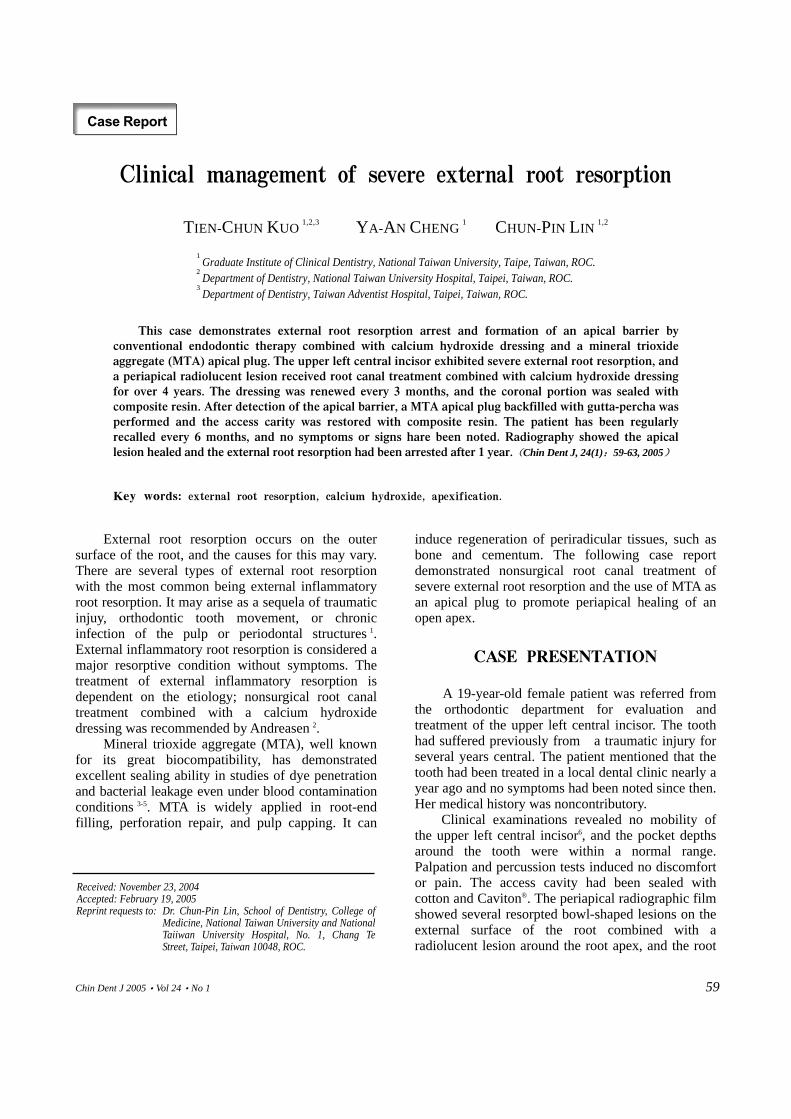
Clinical examinations revealed no mobility of the upper left central incisor6, and the pocket depths around the tooth were within a normal range. Palpation and percussion tests induced no discomfort or pain. The access cavity had been sealed with cotton and Caviton®. The periapical radiographic film showed several resorpted bowl-shaped lesions on the external surface of the root combined with a radiolucent lesion around the root apex, and the root
T.C. Kuo, Y.A. Cheng and C.P. Lin.
Chin Dent J 2005‧Vol 24‧No 1 60
Figure 1. Initial x-ray film showing multiple bowl-shaped external root resorption with periapical radiolucent lesions.
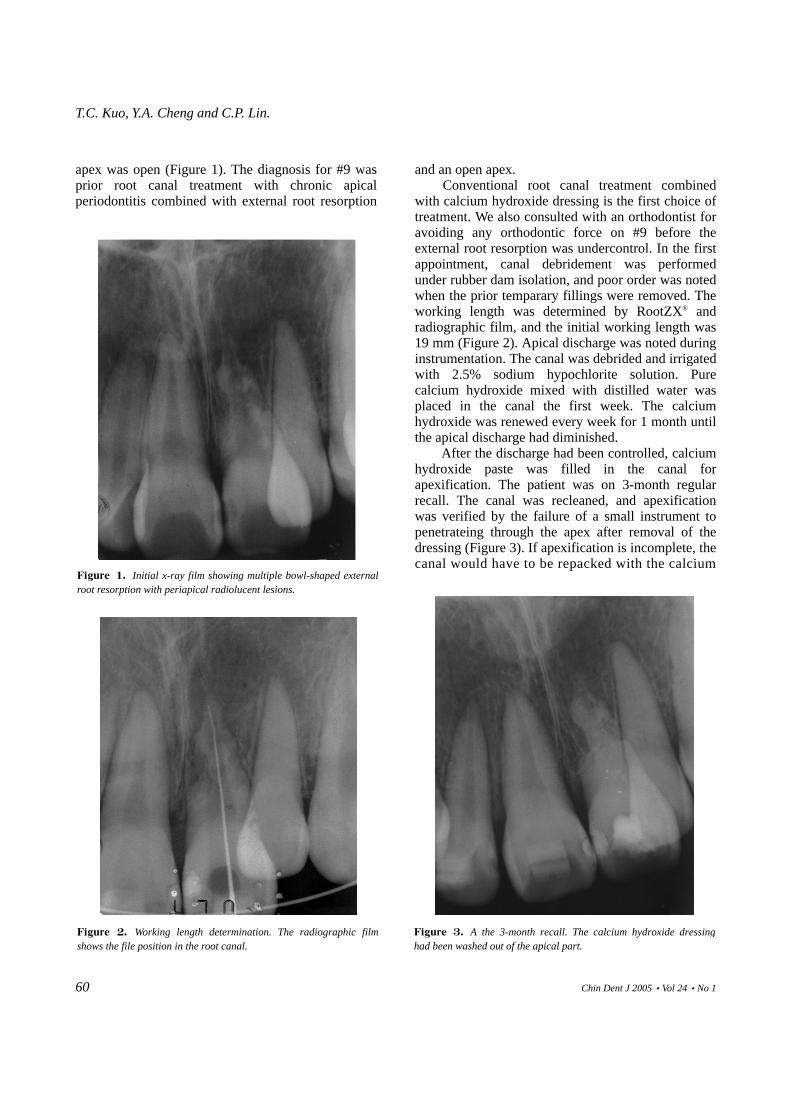
Figure 2. Working length determination. The radiographic film shows the file position in the root canal.
apex was open (Figure 1). The diagnosis for #9 was prior root canal treatment with chronic apical periodontitis combined with external root resorption
and an open apex. Conventional root canal treatment combined
with calcium hydroxide dressing is the first choice of treatment. We also consulted with an orthodontist for avoiding any orthodontic force on #9 before the external root resorption was undercontrol. In the first appointment, canal debridement was performed under rubber dam isolation, and poor order was noted when the prior temparary fillings were removed. The working length was determined by RootZX® and radiographic film, and the initial working length was 19 mm (Figure 2). Apical discharge was noted during instrumentation. The canal was debrided and irrigated with 2.5% sodium hypochlorite solution. Pure calcium hydroxide mixed with distilled water was placed in the canal the first week. The calcium hydroxide was renewed every week for 1 month until the apical discharge had diminished.
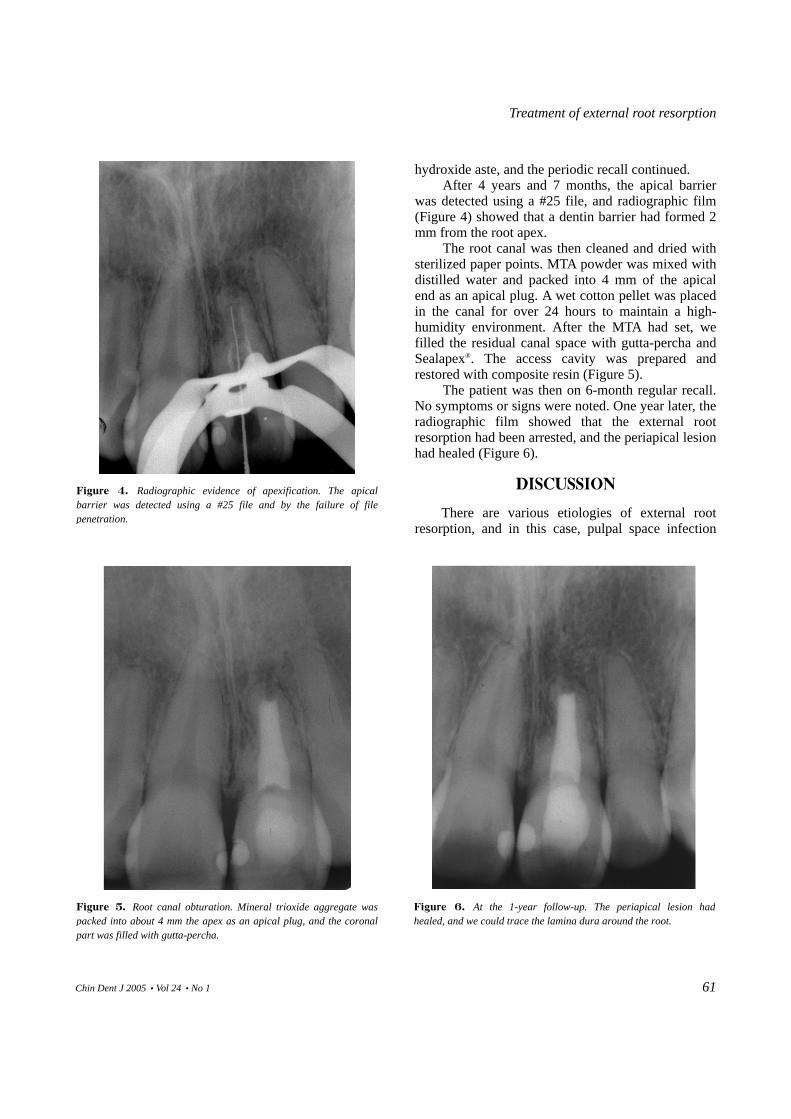
After the discharge had been controlled, calcium hydroxide paste was filled in the canal for apexification. The patient was on 3-month regular recall. The canal was recleaned, and apexification was verified by the failure of a small instrument to penetrateing through the apex after removal of the dressing (Figure 3). If apexification is incomplete, the canal would have to be repacked with the calcium
Figure 3. A the 3-month recall. The calcium hydroxide dressing had been washed out of the apical part.
Treatment of external root resorption
Chin Dent J 2005‧Vol 24‧No 1 61
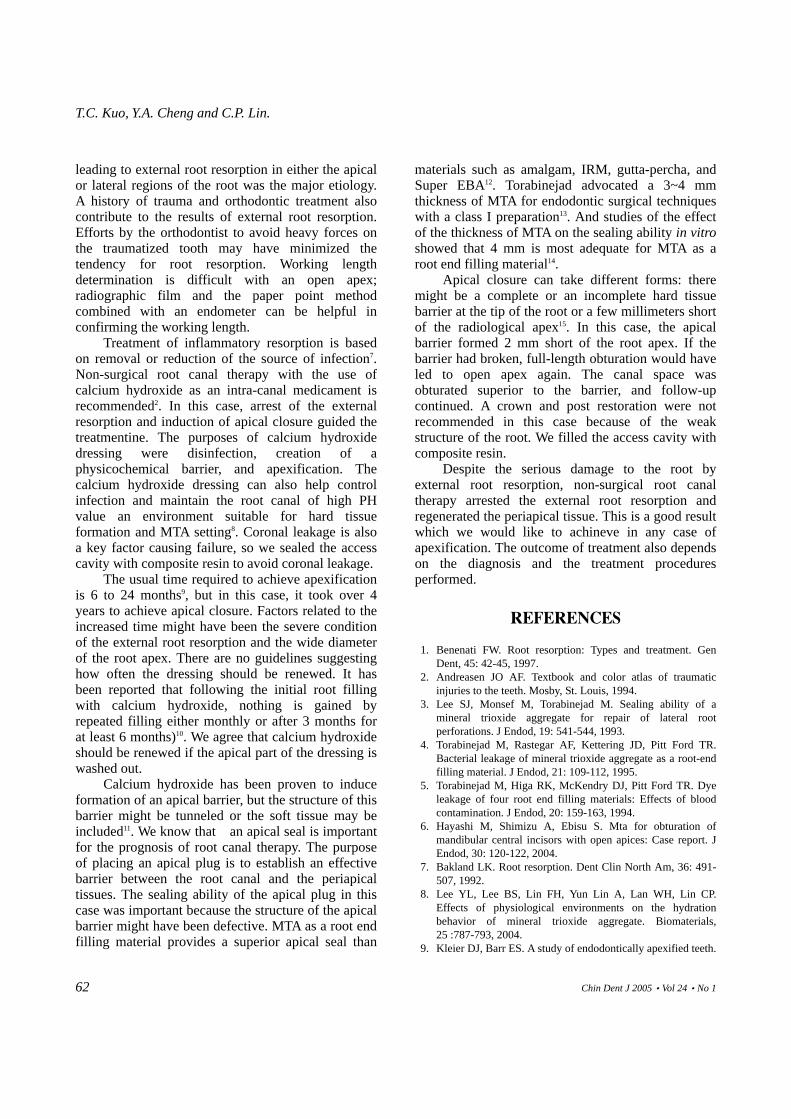
hydroxide aste, and the periodic recall continued. After 4 years and 7 months, the apical barrier
was detected using a #25 file, and radiographic film (Figure 4) showed that a dentin barrier had formed 2 mm from the root apex.
The root canal was then cleaned and dried with sterilized paper points. MTA powder was mixed with distilled water and packed into 4 mm of the apical end as an apical plug. A wet cotton pellet was placed in the canal for over 24 hours to maintain a high-humidity environment. After the MTA had set, we filled the residual canal space with gutta-percha and Sealapex®. The access cavity was prepared and restored with composite resin (Figure 5).
The patient was then on 6-month regular recall. No symptoms or signs were noted. One year later, the radiographic film showed that the external root resorption had been arrested, and the periapical lesion had healed (Figure 6).
DISCUSSION
There are various etiologies of external root resorption, and in this case, pulpal space infection
Figure 4. Radiographic evidence of apexification. The apical barrier was detected using a #25 file and by the failure of file penetration.
Figure 5. Root canal obturation. Mineral trioxide aggregate was packed into about 4 mm the apex as an apical plug, and the coronal part was filled with gutta-percha.
Figure 6. At the 1-year follow-up. The periapical lesion had healed, and we could trace the lamina dura around the root.
T.C. Kuo, Y.A. Cheng and C.P. Lin.
Chin Dent J 2005‧Vol 24‧No 1 62
leading to external root resorption in either the apical or lateral regions of the root was the major etiology. A history of trauma and orthodontic treatment also contribute to the results of external root resorption. Efforts by the orthodontist to avoid heavy forces on the traumatized tooth may have minimized the tendency for root resorption. Working length determination is difficult with an open apex; radiographic film and the paper point method combined with an endometer can be helpful in confirming the working length.
Treatment of inflammatory resorption is based on removal or reduction of the source of infection7. Non-surgical root canal therapy with the use of calcium hydroxide as an intra-canal medicament is recommended2. In this case, arrest of the external resorption and induction of apical closure guided the treatmentine. The purposes of calcium hydroxide dressing were disinfection, creation of a physicochemical barrier, and apexification. The calcium hydroxide dressing can also help control infection and maintain the root canal of high PH value an environment suitable for hard tissue formation and MTA setting8. Coronal leakage is also a key factor causing failure, so we sealed the access cavity with composite resin to avoid coronal leakage.
The usual time required to achieve apexification is 6 to 24 months9, but in this case, it took over 4 years to achieve apical closure. Factors related to the increased time might have been the severe condition of the external root resorption and the wide diameter of the root apex. There are no guidelines suggesting how often the dressing should be renewed. It has been reported that following the initial root filling with calcium hydroxide, nothing is gained by repeated filling either monthly or after 3 months for at least 6 months)10. We agree that calcium hydroxide should be renewed if the apical part of the dressing is washed out.
Calcium hydroxide has been proven to induce formation of an apical barrier, but the structure of this barrier might be tunneled or the soft tissue may be included11. We know that an apical seal is important for the prognosis of root canal therapy. The purpose of placing an apical plug is to establish an effective barrier between the root canal and the periapical tissues. The sealing ability of the apical plug in this case was important because the structure of the apical barrier might have been defective. MTA as a root end filling material provides a superior apical seal than
materials such as amalgam, IRM, gutta-percha, and Super EBA12. Torabinejad advocated a 3~4 mm thickness of MTA for endodontic surgical techniques with a class I preparation13. And studies of the effect of the thickness of MTA on the sealing ability in vitro showed that 4 mm is most adequate for MTA as a root end filling material14.
Apical closure can take different forms: there might be a complete or an incomplete hard tissue barrier at the tip of the root or a few millimeters short of the radiological apex15. In this case, the apical barrier formed 2 mm short of the root apex. If the barrier had broken, full-length obturation would have led to open apex again. The canal space was obturated superior to the barrier, and follow-up continued. A crown and post restoration were not recommended in this case because of the weak structure of the root. We filled the access cavity with composite resin.
Despite the serious damage to the root by external root resorption, non-surgical root canal therapy arrested the external root resorption and regenerated the periapical tissue. This is a good result which we would like to achineve in any case of apexification. The outcome of treatment also depends on the diagnosis and the treatment procedures performed.
REFERENCES
1. Benenati FW. Root resorption: Types and treatment. Gen Dent, 45: 42-45, 1997.
2. Andreasen JO AF. Textbook and color atlas of traumatic injuries to the teeth. Mosby, St. Louis, 1994.
3. Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod, 19: 541-544, 1993.
4. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR. Bacterial leakage of mineral trioxide aggregate as a root-end filling material. J Endod, 21: 109-112, 1995.
5. Torabinejad M, Higa RK, McKendry DJ, Pitt Ford TR. Dye leakage of four root end filling materials: Effects of blood contamination. J Endod, 20: 159-163, 1994.
6. Hayashi M, Shimizu A, Ebisu S. Mta for obturation of mandibular central incisors with open apices: Case report. J Endod, 30: 120-122, 2004.
7. Bakland LK. Root resorption. Dent Clin North Am, 36: 491-507, 1992.
8. Lee YL, Lee BS, Lin FH, Yun Lin A, Lan WH, Lin CP. Effects of physiological environments on the hydration behavior of mineral trioxide aggregate. Biomaterials, 25 :787-793, 2004.
9. Kleier DJ, Barr ES. A study of endodontically apexified teeth.

Treatment of external root resorption
Chin Dent J 2005‧Vol 24‧No 1 63
Endod Dent Traumatol, 7: 112-117, 1991. 10. Chosack A, Sela J, Cleaton-Jones P. A histological and
quantitative istomorphometric study of apexification of nonvital permanent incisors of vervet monkeys after repeated root filling with a calcium hydroxide paste. Endod Dent Traumatol, 13: 211-217, 1997.
11. Cox CF, Subay RK, Ostro E, Suzuki S, Suzuki SH. Tunnel defects in dentin bridges: Their formation following direct pulp capping. Oper Dent, 21: 4-11, 1996.
12. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling
material. J Endod, 19: 591-595, 1993. 13. Torabinejad M, Chivian N. Clinical applications of mineral
trioxide aggregate. J Endod, 25: 197-205, 1999. 14. Valois CR, Costa ED, Jr. Influence of the thickness of
mineral trioxide aggregate on sealing ability of root-end fillings in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 97: 108-111, 2004.
15. Morabito A, Defabianis P. Apexification in the endodontic treatment of pulpless immature teeth: Indications and requirements. J Clin Pediatr Dent, 20: 197-203, 1996.

W.P. Chen, B.S. Lee and C.P. Lin.
Chin Dent J 2005‧Vol 24‧No 1 64











![Surgical Endodontic Management of External Root Resorption ... · Complete destruction of Hertwig’s epithelial root sheath results in cessation of normal root development [6]. Inducing](https://static.fdocuments.net/doc/165x107/60f91b476d59a55ab268f1a6/surgical-endodontic-management-of-external-root-resorption-complete-destruction.jpg)


![Review Article Apical External Root Resorption and Repair ...external root resorption increases with the magnitude of the applied orthodontic force [ , , , ] and with continuous forces](https://static.fdocuments.net/doc/165x107/612422b33a54d70bce7d8287/review-article-apical-external-root-resorption-and-repair-external-root-resorption.jpg)



