The Threat and the Challenge of MDR-TB
59
The Threat and the Challenge of The Threat and the Challenge of MDR-TB MDR-TB . . A Curable Disease with a Proper Clinical and A Curable Disease with a Proper Clinical and Operational Management Operational Management Prof. José A. Prof. José A. Caminero Caminero Luna Luna Department of Pneumonology Department of Pneumonology University Hospital of Gran Canaria “Dr. University Hospital of Gran Canaria “Dr. Negrín” Negrín” Las Palmas de G.C. SPAIN Las Palmas de G.C. SPAIN (The Union) 43rd Union World Conference Malaysia, November 14, 2012
-
Upload
national-press-foundation -
Category
Documents
-
view
32 -
download
0
description
A curable disease with a proper clinical and operational management.By Prof. Jose A. Caminero Luna
Transcript of The Threat and the Challenge of MDR-TB

The Threat and the Challenge of MDR-TBThe Threat and the Challenge of MDR-TB..A Curable Disease with a Proper Clinical and Operational A Curable Disease with a Proper Clinical and Operational
ManagementManagement
Prof. José A. Prof. José A. CamineroCaminero Luna Luna
Department of PneumonologyDepartment of PneumonologyUniversity Hospital of Gran Canaria “Dr. Negrín”University Hospital of Gran Canaria “Dr. Negrín”
Las Palmas de G.C. SPAINLas Palmas de G.C. SPAIN
(The Union)(The Union)
43rd Union World ConferenceMalaysia, November 14, 2012

Tuberculosis is certainly the disease that has provoked the most damage (diseases
and deaths) to mankind throughout history. It has caused death and disease for perhaps more than 3
million years and, as a rule, has affected the poorest
strata of society
J.A. Caminero. Eur Respir J 2004, 25: 895J.A. Caminero. Eur Respir J 2004, 25: 895

Amenophis IVAmenophis IV
andand
NefertitiNefertiti
(Deceased TB) (Deceased TB)
1360 b. c.1360 b. c.
Simón Bolívar (1783-1830)Simón Bolívar (1783-1830)Liberator of the Americas. Died of TB after a long illnessLiberator of the Americas. Died of TB after a long illness

Mycobacterium tuberculosisMycobacterium tuberculosis
It is probably the infectious agent that has It is probably the infectious agent that has caused the greatest number of Deaths in caused the greatest number of Deaths in
the History of Humanitythe History of Humanity
Today it is still considered as the 2nd Greatest Murderer, out of all single
Pathogens
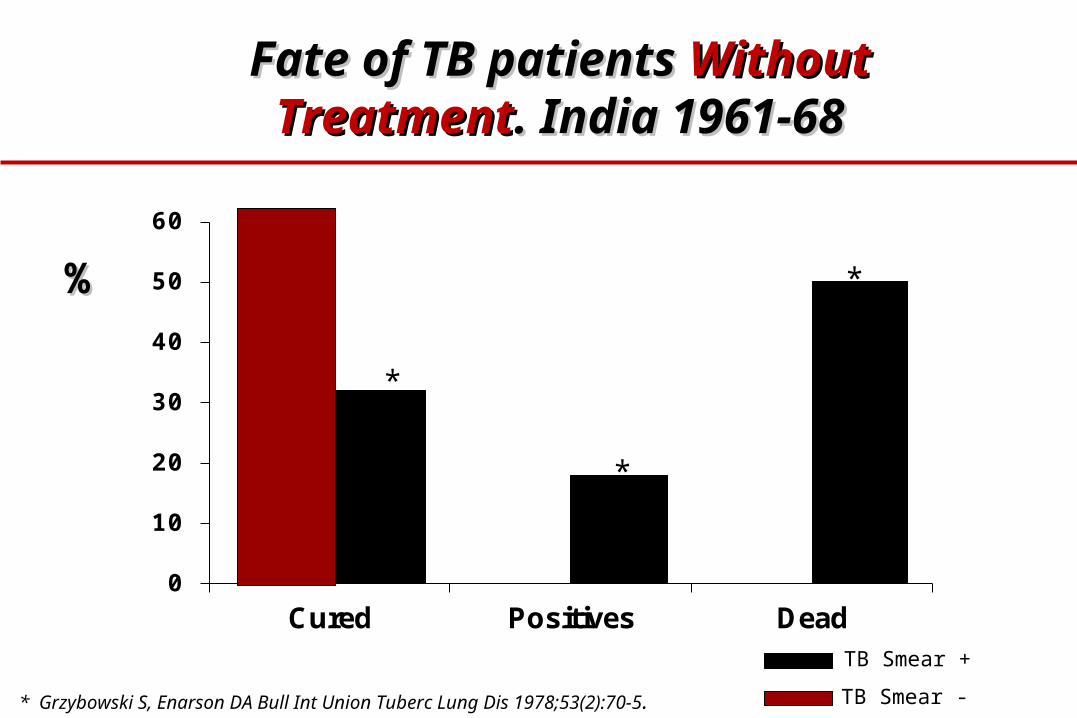
Fate of TB patients Fate of TB patients Without Without TreatmentTreatment. India 1961-68. India 1961-68
0
10
20
30
40
50
60
Cured Positives Dead
* Grzybowski S, Enarson DA Bull Int Union Tuberc Lung Dis 1978;53(2):70-5.
%%
TB Smear +
TB Smear -
*
*
*

Two Genius of the Medicine: Waskman and FlemingTwo Genius of the Medicine: Waskman and Fleming

Dr. Selman A. WaksmanDr. Selman A. Waksman
- Discovered STREPTOMYCIN in 1943- Discovered STREPTOMYCIN in 1943- Together with his laboratory assistant A. Schatz - Together with his laboratory assistant A. Schatz
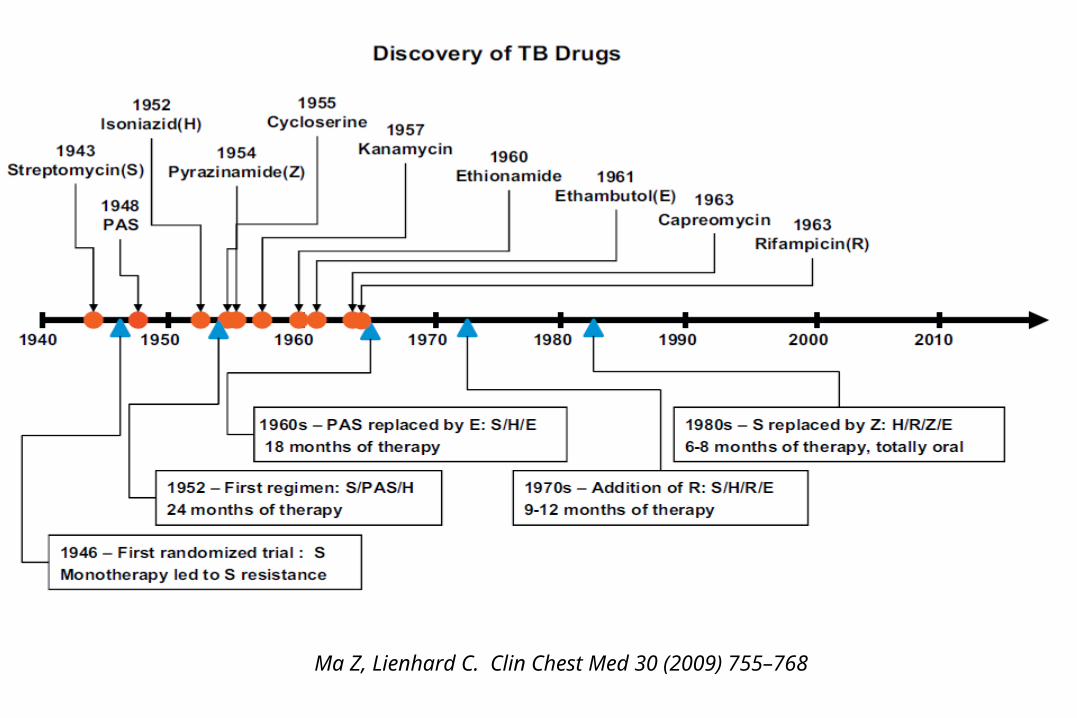
Ma Z, Lienhard C. Clin Chest Med 30 (2009) 755–768

INH-PAS-SM INH-PAS-SM

ANTIMYCOBACTERIAL DRUGSANTIMYCOBACTERIAL DRUGS
1. ISONIAZID1. ISONIAZID 2. RIFAMPICIN2. RIFAMPICIN3. PYRAZINAMIDE3. PYRAZINAMIDE 4. ETHAMBUTOL4. ETHAMBUTOL5. STREPTOMYCIN5. STREPTOMYCIN 6. CAPREOMYCINE6. CAPREOMYCINE7. KANAMYCIN7. KANAMYCIN 8. AMIKACIN8. AMIKACIN9. ETHION. – PROTHIONAMIDE9. ETHION. – PROTHIONAMIDE 10. CYCLOSERINE-TERIZ.10. CYCLOSERINE-TERIZ.11. P.A.S.11. P.A.S. 12. THIACETAZONE12. THIACETAZONE
13. QUINOLONES:13. QUINOLONES: 14. CLOFAZIMIDE14. CLOFAZIMIDE - OFLOXACIN- OFLOXACIN 15. Others:15. Others: - LEVOFLOX. - GATIFLOXACIN - MOXIFLOX- LEVOFLOX. - GATIFLOXACIN - MOXIFLOX - MACROLIDES, CLAVULANATE - MACROLIDES, CLAVULANATE., Etc., Etc
AT LEAST AT LEAST 44 FOR GOOD RETREATMENT! FOR GOOD RETREATMENT!

TB TB An An INCURABLEINCURABLE disease ?disease ?
The The ThreatThreat and the and the Fear Fear of of MDR/XDR- TBMDR/XDR- TB
“It may affect over 10 million people world-wide…” JAMA (2000)
“MDR Tuberculosis … A global pandemic” BMJ (1998)
“MDR … a time bomb” Am Rev Respir Dis (1985)
The Threat of MDR-TB?
“Once liberated, it will be impossible to control...” WHO publicity (1997)
“More fatal than AIDS” Washington Post (1998)
“It may destabilise Russian society” NDCF (2000)

Consequences of MDR/XDR-TB
Poor response to standardised treatment
Long duration of contagiousness
High risk of morbidity and mortality
Individualised treatment more costly
Difficult management --> requires specialized Difficult management --> requires specialized TrainingTraining

The global TB situation, 2011 The global TB situation, 2011
Estimated number of cases, 2011
Estimated number of deaths, 2011
990,000*(840,000–1.1 million)
8.7 million(8.3–9.0 million)
630,000 (460,000–790,000)
[of 12m prevalent cases]
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 million (1.0–1.2 million)
430,000(400,000–460,000)
Source: WHO Global Tuberculosis Report 2012
* Excluding deaths attributed to HIV/TB

% of MDR among new TB cases (1994-2011 data)
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2012. All rights reserved
Global average 3.7% (2.1 – 5.2%)

% of MDR among previously treated TB cases (1994-2011 data)
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2012. All rights reserved
Global average 20% (13 – 26%)

- Between November 2009 and December 2010, 156 consecutively diagnosed new and 68 previously treated TB
- MDR-TB was found in 35.3% (95% CI 27.7–42.8) of new patients and 76.5% (95% CI 66.1–86.8) of those previously treated.
- Overall, nearly one in two patients enrolled had MDR-TB.
- Extensively drug-resistant TB was reported in 15 of the 107 MDR-TB patients (14.0%, 95% CI 7.3–20.7).

High prevalence of childhood multi-drug resistant tuberculosis in Johannesburg, South Africa: a cross sectional study
Lee Fairlie,Natalie C Beylis, Gary Reubenson, David P Moore,and Shabir A Madhi
BMC Infect Dis. 2011; 11: 28.
-1317 children were treated for TB in 20081317 children were treated for TB in 2008
- DST was performed in 148 (72.5%) of the - DST was performed in 148 (72.5%) of the 204 children who had culture-204 children who had culture-confirmed confirmed tuberculosis.tuberculosis.
- The prevalence of isoniazid-resistance was 14.2% (n = 21) and the prevalence of The prevalence of isoniazid-resistance was 14.2% (n = 21) and the prevalence of MDR-TB MDR-TB 8.8%8.8% (n = 13) (95%CI, 4.8-14.6%). (n = 13) (95%CI, 4.8-14.6%).
- The prevalence of HIV co-infection was The prevalence of HIV co-infection was 52.1%52.1% in children with drug in children with drugsusceptible-TB and 53.9% in children with MDR-TB.susceptible-TB and 53.9% in children with MDR-TB.
- Ten (76.9%) of the 13 children with MDR-TB received appropriate treatment and Ten (76.9%) of the 13 children with MDR-TB received appropriate treatment and four (30.8%) died at a median of 2.8 months (range 0.1-4.0 months) after four (30.8%) died at a median of 2.8 months (range 0.1-4.0 months) after the date of tuberculosis investigation.the date of tuberculosis investigation.

Countries (84) reporting ≥1 XDR-TB case by Oct 2012

TB TB An An INCURABLEINCURABLE disease ?disease ?
The The ThreatThreat and the and the Fear Fear of of MDR/XDR- TBMDR/XDR- TB

The ResistantThe Resistant
M. tuberculosisM. tuberculosis
day by day is moreday by day is more
RESISTANTRESISTANT

M tuberculosis M tuberculosis vs vs Human SpecieHuman Specie
The Millennial Fight The Millennial Fight between between 22 SpeciesSpecies

Dr. Selman A. WaksmanDr. Selman A. Waksman
- Discovered STREPTOMYCIN in 1943- Discovered STREPTOMYCIN in 1943- Together with his laboratory assistant A. Schatz - Together with his laboratory assistant A. Schatz
Mono Mono - Resistance - Resistance

INH-PAS-SM INH-PAS-SM
Poly Poly - Resistance - Resistance
M. TB Resistant to2 or more Drugs

RIFAMPICINARIFAMPICINA
Discovered in 1963 by Discovered in 1963 by Lepetit LaboratoriesLepetit Laboratories
MultiMulti–Drug-Resistance –Drug-Resistance ((MDRMDR) )
M. TB Resistant to, at least, H+R

CONCLUSSIONSCONCLUSSIONS::
1.1. Only ciprofloxacin, ofloxacin, levofloxacin, sparfloxacin and Only ciprofloxacin, ofloxacin, levofloxacin, sparfloxacin and moxifloxacin have been tested in randomized controlled trials for moxifloxacin have been tested in randomized controlled trials for treating tuberculosis.treating tuberculosis.
2.2. We cannot recommend ciprofloxacin in treating tuberculosis.We cannot recommend ciprofloxacin in treating tuberculosis.3.3. Trials of newer fluoroquinolones for treating tuberculosis are needed Trials of newer fluoroquinolones for treating tuberculosis are needed
and are on-going.and are on-going.4.4. No difference has been demonstrated between sparfloxacin and No difference has been demonstrated between sparfloxacin and
ofloxacin in drug-resistant tuberculosis.ofloxacin in drug-resistant tuberculosis.
ExtensivelyExtensively–Drug-Resistance –Drug-Resistance ((XDRXDR) )
MDR-TB plus Resistance to FQ and 1 SLDI (Kn, Ak, Cm)

Ma Z, Lienhard C. Clin Chest Med 30 (2009) 755–768
Already there are TB Cases with Resistance to all these DrugsAlready there are TB Cases with Resistance to all these Drugs
Totally-Drug Resistant (TDR-TB)?Totally-Drug Resistant (TDR-TB)?

- In 2007, two patients with strains having resistance to all first and second-line anti-TB drugs which were tested were reported from Italy (1)
- In 2009, 15 TB patients in Iran were reported to be resistant to all anti-TB drugs tested (2)
- In December 2011, clinicians in Mumbai, India, described four patients with “TDR-TB” (3). A few weeks later, the Times of India reported another eight cases in Mumbai.
Totally Drug Resistant (Totally Drug Resistant (T.D.R.T.D.R. – TB) – TB)
1) Migliori GB, et al. Euro Surveill. 2007 May;12(5):E070517.12) Velayati AA, et al. Chest. 2009 Aug;136(2):420–5.3) Udwadia ZF, et al. Clin. Infect. Dis. 2012 Feb 15;54(4):579–81.

1.1. Mono-Resistance Mono-Resistance 2.2. Poly-ResistancePoly-Resistance3.3. M.D.R.M.D.R.4.4. X.D.R.X.D.R.5.5. T.D.R.T.D.R. (Totally Resistant TB) (Totally Resistant TB)
The The BattleBattle between the Human Species and M. tuberculosis between the Human Species and M. tuberculosis
Is DR –TB an Incurable Epidemic ?
NotNot always!! With adequate Management it is curable, always!! With adequate Management it is curable, although the possibility of success can decrease although the possibility of success can decrease
notablynotably

Ma Z, et al. Lancet 2010; 375: 2100–09

Patients with an Patients with an ExtensiveExtensive pattern of pattern of ResistanceResistance has always has always
existed , but with an existed , but with an Adequate Adequate Clinical ManagementClinical Management and and
EnoughEnough ResourcesResources a good Rate a good Rate of of SuccessSuccess is Possible is Possible

Possibilities to Possibilities to CureCure MDR/XDR-TB MDR/XDR-TBAvailable EvidenceAvailable Evidence
1.1. HistoricHistoric Evidence (Pre-Rifamp. period) Evidence (Pre-Rifamp. period)
2.2. CurrentCurrent Evidence Evidence
1.1. MDR-TB Patients (2 Meta-analysis)MDR-TB Patients (2 Meta-analysis)2.2. XDR-TB Patients (1 Systematic Rev. and 1 Meta-analysis) XDR-TB Patients (1 Systematic Rev. and 1 Meta-analysis)
The MDR/XDR-TB patients of The MDR/XDR-TB patients of 1950-70s1950-70s were those with were those with
Resistance to H+S+PAS (then Resistance to H+S+PAS (then there was not Rif nor Fq)there was not Rif nor Fq)
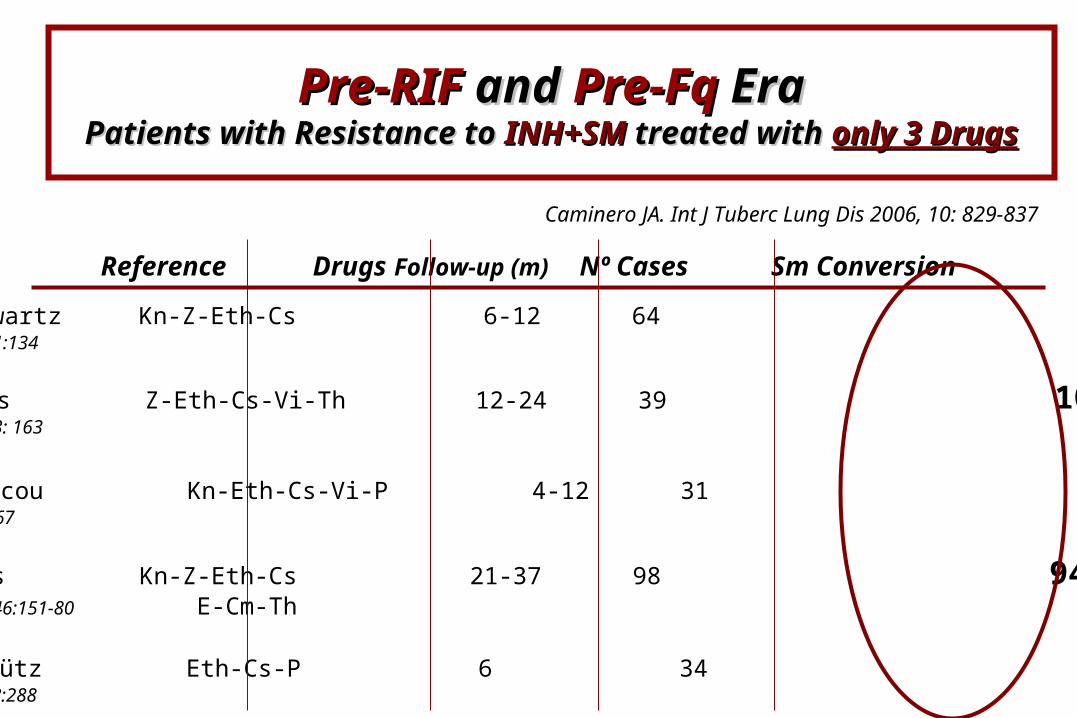
USA. Schwartz Kn-Z-Eth-Cs 6-12 64 57 %JAMA 1962; 181:134
UK. Pines Z-Eth-Cs-Vi-Th 12-24 39 100 %Chest 1962; 53: 163
Morocco. Chicou Kn-Eth-Cs-Vi-P 4-12 31 67,7 %RevTuberc1962;26:867
USA. Kass Kn-Z-Eth-Cs 21-37 98 94,8 %Tubercle1965;46:151-80 E-Cm-Th
Germany. Schütz Eth-Cs-P 6 34 85 %PraxisPneum1964;18:288
Reference Drugs Follow-up (m) Nº Cases Sm Conversion
Pre-RIFPre-RIF and and Pre-Fq Pre-Fq EraEraPatients with Resistance to Patients with Resistance to INH+SMINH+SM treated with treated with only 3 Drugsonly 3 Drugs
Caminero JA. Int J Tuberc Lung Dis 2006, 10: 829-837

Hungary. Böszörmenyi Z-Eth-Cs 3 31 51,6 %Tubercle 1965;46:143
USA. Lester Kn-Z-Eth-Cs- 6-60 146 83.5 %AmRevRespirDis1968;97:392-8
Poland. Zierski Z-Eth-Cs 3-9 65 92,4 %Tubercle 1964;45:96
Czechosl. Tousek Z-Eth-Cs 60-84 55 96 %Tubercle 1967;48:27
Spain. March Z-Eth-Cs-Vi-E 6-18 33 93,4 %RevClinEsp1968;109:117
Reference Drugs Follow-up (m) Nº Cases Sm Conversion
Pre-RIFPre-RIF and and Pre-Fq Pre-Fq EraEraPatients with Resistance to Patients with Resistance to INH+SMINH+SM treated with treated with only 3 Drugsonly 3 Drugs
Caminero JA. Int J Tuberc Lung Dis 2006, 10: 829-837

Possibilities to Possibilities to CureCure MDR/XDR-TB MDR/XDR-TBAvailable EvidenceAvailable Evidence
1.1. Historic Evidence (Pre-Rifamp. period)Historic Evidence (Pre-Rifamp. period)
2.2. CurrentCurrent Evidence Evidence
1.1. MDR-TB Patients (2 Meta-analysis)MDR-TB Patients (2 Meta-analysis)2.2. XDR-TB Patients (1 Systematic Rev. and 1 Meta-analysis) XDR-TB Patients (1 Systematic Rev. and 1 Meta-analysis)

- Systematic search (to December 2008) - Systematic search (to December 2008) 36 met inclusion 36 met inclusion criteria, representing 31 treatment programmes from criteria, representing 31 treatment programmes from
21 Countries21 Countries
- 62% [95% CI 57–67] successful outcomes62% [95% CI 57–67] successful outcomes- 13% [9–17] defaulted13% [9–17] defaulted- 11% [9–13] died11% [9–13] died- 2% [1–4] were transferred out2% [1–4] were transferred out
September 2009

- 34 clinical reports (mean 250 patients) met the inclusion criteria.- 34 clinical reports (mean 250 patients) met the inclusion criteria.
- The proportion of patients treated successfully improved when:- The proportion of patients treated successfully improved when:- Treatment duration was - Treatment duration was at least 18 monthsat least 18 months- Patients received - Patients received DOT throughout treatmentDOT throughout treatment
- Studies that combined both factors had significantly higher pooled - Studies that combined both factors had significantly higher pooled success proportions success proportions (69%)(69%) than other studies of treatment than other studies of treatment outcomes outcomes (58%)(58%)
- IndividualizedIndividualized treatment regimens had treatment regimens had higher treatment success (64%)higher treatment success (64%) than than standardized regimens (54%), although the difference was not significantstandardized regimens (54%), although the difference was not significant
- Treatment approaches and study methodologies were heterogeneous across studies.Treatment approaches and study methodologies were heterogeneous across studies.
- Many important variables, including patients’ HIV status, were inconsistently reported - Many important variables, including patients’ HIV status, were inconsistently reported between studies.between studies.

- Systematic review and meta-analysis reviewed treatment outcomes for children with MDR-TB.
- Eight studies, which reported outcomes on 315 patients, contributed to the database.
- Average duration of treatment ranged from 6 months to 34 ms.
- The pooled estimate for treatment success (defined as a composite of cure and completion) was 81.7% with death in 5.9%, and default in 6.2% of patients.
- Adverse reactions occurred in 39.1% of the children, the most common of which were nausea and vomiting followed by hearing loss, psychiatric effects and hypothyroidism.
Ettehad D, Schaaf HS, Seddon JA, Cooke GS, Ford N. Treatment outcomes for children with multidrug-resistant
tuberculosis: a systematic review and meta-analysis. Lancet Infect Dis 2012;12:449-56.
MDR-TB Treatment in Children

- LongerLonger treatment duration and treatment duration and delayed sputum smear conversiondelayed sputum smear conversion were reported in were reported in most studies among XDR-TB patients.most studies among XDR-TB patients.
- Median time to sputum Median time to sputum SmearSmear conversionconversion ranged 41– 56 days in MDR-TB patients, ranged 41– 56 days in MDR-TB patients, while it ranged 88–110 days in XDR-TB cases.while it ranged 88–110 days in XDR-TB cases.
- The median time to The median time to Culture conversionCulture conversion ranged 58–99 days in MDR-TB cases; it ranged 58–99 days in MDR-TB cases; it was substantially different in XDR-TB patients, ranging 60–195 days.was substantially different in XDR-TB patients, ranging 60–195 days.

Sotgiu G. Eur Respir J 2009; 33: 871-881
- Very different Outcomes- Very different Outcomes

- 13 observational studies covering 560 patients:- 13 observational studies covering 560 patients:- - 43.7%43.7% (95% CI, 32.8%–54.5%) favorable outcomes (95% CI, 32.8%–54.5%) favorable outcomes- 20.8% (95% CI, 14.2%–27.3%) Died.- 20.8% (95% CI, 14.2%–27.3%) Died.
- Studies in which a higher proportion of patients received a - Studies in which a higher proportion of patients received a later-generation fluoroquinolonelater-generation fluoroquinolone reported a higher reported a higher
proportion of favorable treatment outcomes (p= .012)proportion of favorable treatment outcomes (p= .012)

With each 10% increase in With each 10% increase in the proportion of patients the proportion of patients
receiving a later-receiving a later-generation generation
fluoroquinolone, there wasfluoroquinolone, there wasa 4% increase in the a 4% increase in the
proportion of patients with proportion of patients with favorable outcomes.favorable outcomes.
Jacobson et al. CID 2010; 51 (July)

Patients with an Patients with an ExtensiveExtensive pattern of pattern of ResistanceResistance has always existed, but with has always existed, but with
Adequate Clinical ManagementAdequate Clinical Management and and Enough Resources Enough Resources a good Rate of a good Rate of
SuccessSuccess is Possible is Possible
The The Clinical ManagementClinical Management of MDR or of MDR or XDR-TB Patients is KeyXDR-TB Patients is Key

- There are There are no Clinical Trialsno Clinical Trials comparing different comparing different Regimen and DrugsRegimen and Drugs
- There areThere are only personal only personal experiences and experiences and publications showing very different resultspublications showing very different results
- The most important The most important Recommendations/ GuidelinesRecommendations/ Guidelines have changed in the last decades and have changed in the last decades and are not in agreementare not in agreement
- Currently there are very Currently there are very controversialcontroversial issues, sometimes issues, sometimes with no agreementwith no agreement
MDR/XDR-TB Clinical ManagementMDR/XDR-TB Clinical ManagementMany Many ControversialControversial Issues to Address Issues to Address
Caminero JA. Int J Tuberc Lung Dis 2006, 10: 829-837

1. How to approach 1. How to approach DiagnosisDiagnosis of MDR? Reliability of DST of MDR? Reliability of DST
2. How 2. How Many DrugsMany Drugs to Treat MDR-TB ? to Treat MDR-TB ?
3. 3. RationalRational Use of the FLD and SLD Use of the FLD and SLD
5. Role of 5. Role of SurgerySurgery in MDR-TB Treatment in MDR-TB Treatment
MDR/XDR-TB Clinical Management.MDR/XDR-TB Clinical Management.ControversialControversial Issues Issues
4. Length of the 4. Length of the InjectableInjectable (Intensive phase) (Intensive phase)
6. Approach to the Ideal Regime in MDR-TB6. Approach to the Ideal Regime in MDR-TBStandardizedStandardized vs vs IndividualizedIndividualized Regimes Regimes
Caminero JA. Int J Tuberc Lung Dis 2006, 10: 829-837

M. tuberculosis Resistance
In TB, drug resistance is always the result of poor case
management of drug sensitive tuberculosis cases
The first priority to fight against
MDR/XDT-TB is to strengthen the
NTP with a good management of
the susceptible TB
- 37 studies were included. Inappropriate treatment regimens were prescribed in 67% of studies.
- The percentage of patients receiving inappropriate regimens varied between 0.4% and 100%.
- In 19 studies the quality of treatment regimen reporting was low

Even for countries with unlimited resources, the time to generate a MDR-TB case is less than the time required to cure it

PRIORITIESPRIORITIES in a National in a National Tuberculosis Programme (NTP)Tuberculosis Programme (NTP)
1. To Avoid 1. To Avoid MDR-TBMDR-TB
4. To Avoid 4. To Avoid XDR-TBXDR-TB

PRIORITIESPRIORITIES in a National in a National Tuberculosis Programme (NTP)Tuberculosis Programme (NTP)
1. To Avoid 1. To Avoid MDR-TBMDR-TB
4. To Avoid XDR-TB4. To Avoid XDR-TB

THE BEST WAY TO THE BEST WAY TO AVOID AVOID MDR-TBMDR-TB (1)(1)
To Give the best To Give the best initial treatment initial treatment when the when the patient presents TB for the first time.patient presents TB for the first time.
2 HRZE / 4 HR2 HRZE / 4 HR- Advisable Advisable DailyDaily, at least in the Intensive Phase, but , at least in the Intensive Phase, but preferable preferable along all along all the treatmentthe treatment
- EMBEMB (or Intensive Phase) along all the treatment if (or Intensive Phase) along all the treatment if Smear +Smear + at the end at the end of the 2º month, or until knowing Susceptibility H+Rof the 2º month, or until knowing Susceptibility H+R

Directly Observed Directly Observed TreatmentTreatment is is
fundamental to fundamental to prevent prevent Resistance Resistance
emergence emergence
THE BEST WAY TO THE BEST WAY TO AVOID AVOID MDR-TBMDR-TB (2)(2)

PRIORITIESPRIORITIES in a National in a National Tuberculosis Programme (NTP)Tuberculosis Programme (NTP)
1. To Avoid MDR-TB1. To Avoid MDR-TB
4. To Avoid 4. To Avoid XDR-TBXDR-TB

THE BEST WAY TO THE BEST WAY TO AVOID AVOID XDR-TBXDR-TB (1)(1)
- Selection of the Selection of the Best SLD Regimen Best SLD Regimen according the according the Classification of the MDR-TB Classification of the MDR-TB (New, never receiving previously (New, never receiving previously SLD and receiving previously SLD)SLD and receiving previously SLD)
- To support in the selection of this Regimen is essential To support in the selection of this Regimen is essential to know the possible to know the possible Resistance to Fq+SLDI Resistance to Fq+SLDI in MDR-TBin MDR-TB
- SurveillanceSurveillance to address the best SLD Regimen to address the best SLD Regimen- Genotype SLD Genotype SLD in all the MDR-TB patients previous to start in all the MDR-TB patients previous to start
the SLD Regimen the SLD Regimen
Directly Observed Directly Observed TreatmentTreatment is is
fundamental to fundamental to prevent prevent Resistance Resistance
emergence emergence
THE BEST WAY TO THE BEST WAY TO AVOID XDR-TB AVOID XDR-TB (2)(2)

Conclusions
1. MDR/XDR-TB is a global threat and a world challenge
2. With adequate clinical and operational management, all the TB
cases has a chance to be cured, even those with very extensive
pattern of resistance
3. The first priority to fight against MDR/XDT-TB is to strengthen
the NTP with a good management of the susceptible TB