The Prevalence and Adverse Associations of Stigmatization in People with Eating Disorders
20
THE PREVALENCE AND ADVERSE ASSOCIATIONS OF STIGMATIZATION IN PEOPLE WITH EATING DISORDERS
-
Upload
scoti-riff -
Category
Health & Medicine
-
view
218 -
download
1
Transcript of The Prevalence and Adverse Associations of Stigmatization in People with Eating Disorders
THE PREVALENCE ANDADVERSE ASSOCIATIONS OFSTIGMATIZATION IN PEOPLEWITH EATING DISORDERS
#1 Perceived as attention-seekers who are
personally responsible for their condition
#2 Current stigma-related interventions target
public perceptions about eating disorders
Eating disorders are stigmatized
#1 Is the stigma most commonly perpetrated by the public the same as that most commonly experienced by sufferers?
#2 Is the most commonly experienced stigma also the most damaging?
#3 Are anti-stigma initiatives targeting the most commonly experienced/damaging public perceptions?
#4 Are males stigmatised more than females? If so, how?
Gaps in the literature

› Young adults (mean age = 24.7 years)
› Predominantly female (95%)
› Residing in USA (33%), Aus (31%) or UK (21%)
› Students (48%) or employed (36%)
› Single (63.4%) or in a relationship (34%)
› Currently receving tx (57%), received treatment in the
past (33%), or never recevied treatment (7%)
Sample
Anorexia nervosa Bulimia nervosa EDNOS
165 66 86
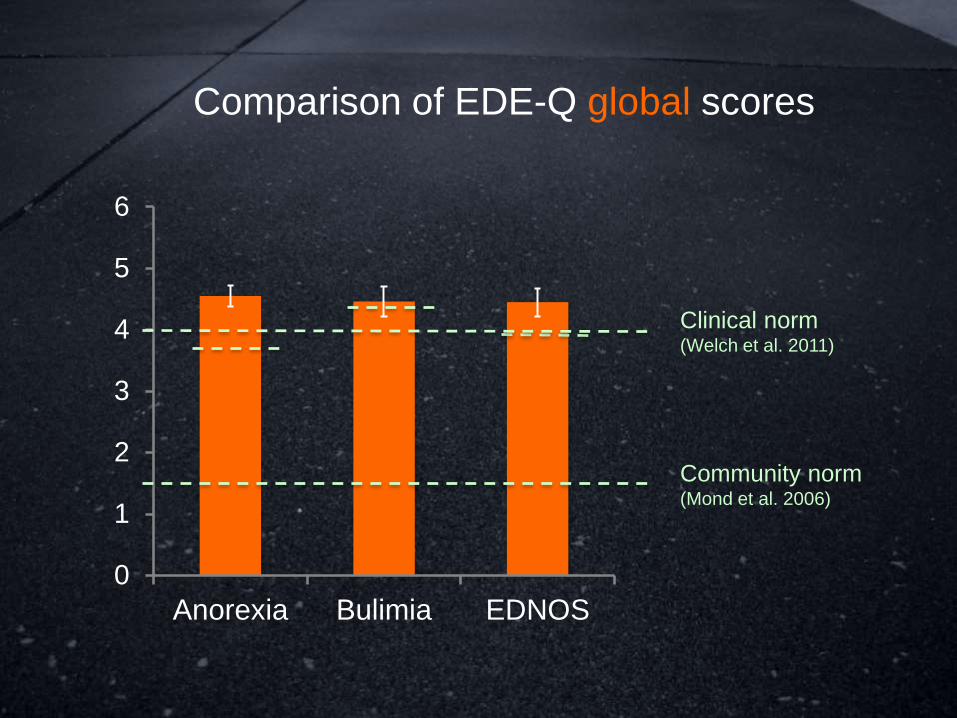
Comparison of EDE-Q global scores
0
1
2
3
4
5
6
Anorexia Bulimia EDNOS
Clinical norm(Welch et al. 2011)
Community norm(Mond et al. 2006)
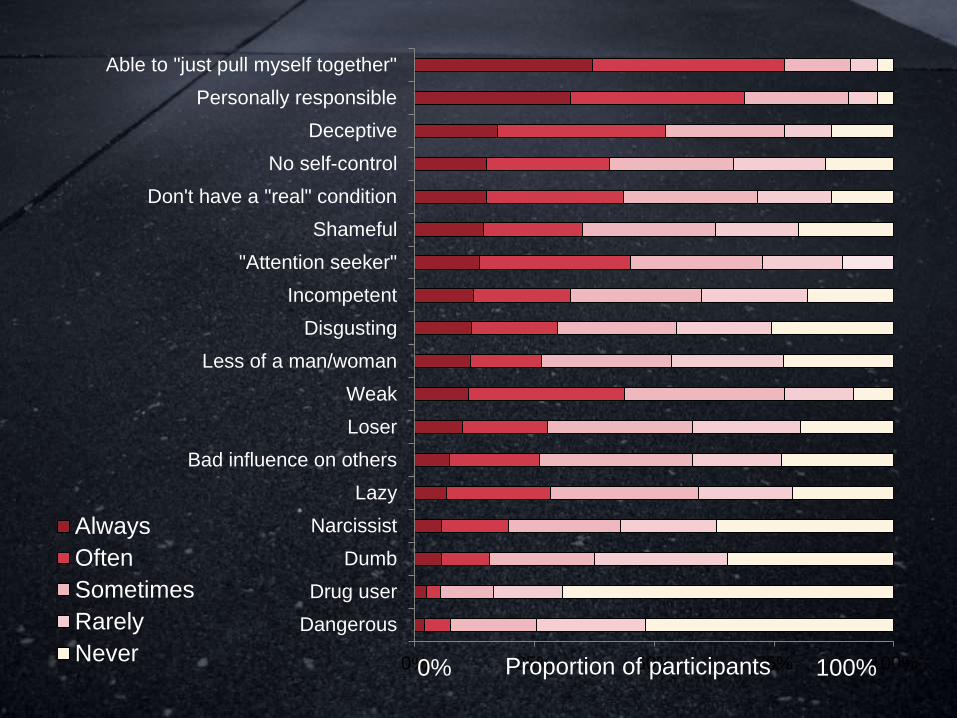
Q. “How frequently have you been subjected
to the following stigmatizing attitudes/beliefs
due to your eating disorder?”
Never
Rarely
Sometimes
Often
Always
Frequency of stigma
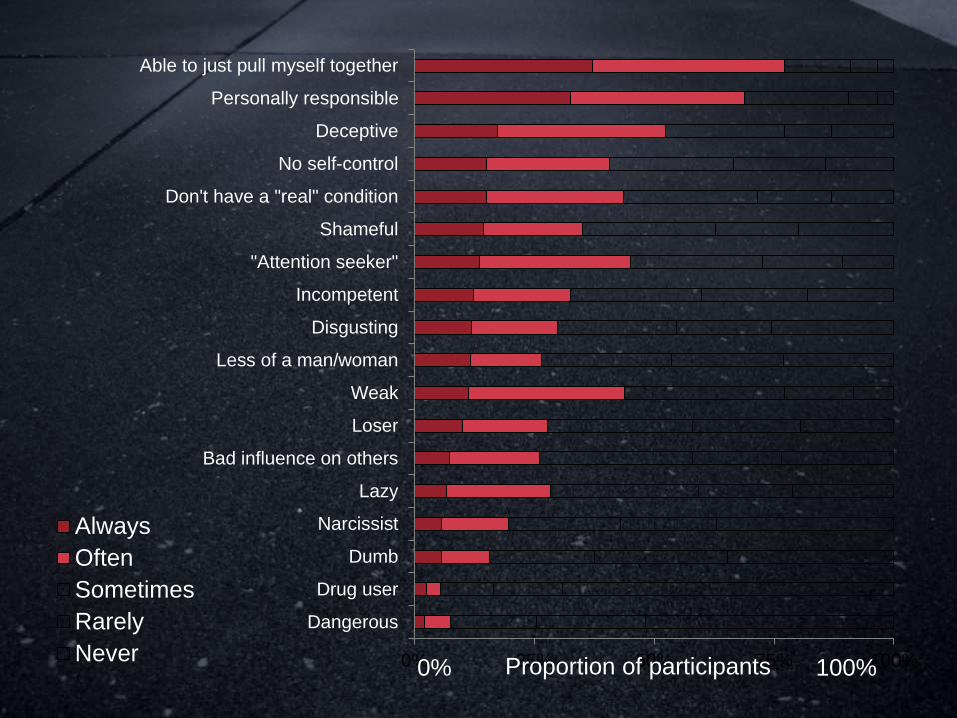
0% 25% 50% 75% 100%
Dangerous
Drug user
Dumb
Narcissist
Lazy
Bad influence on others
Loser
Weak
Less of a man/woman
Disgusting
Incompetent
"Attention seeker"
Shameful
Don't have a "real" condition
No self-control
Deceptive
Personally responsible
Able to just pull myself together
Always
Often
Sometimes
Rarely
NeverProportion of participants 0% 100%
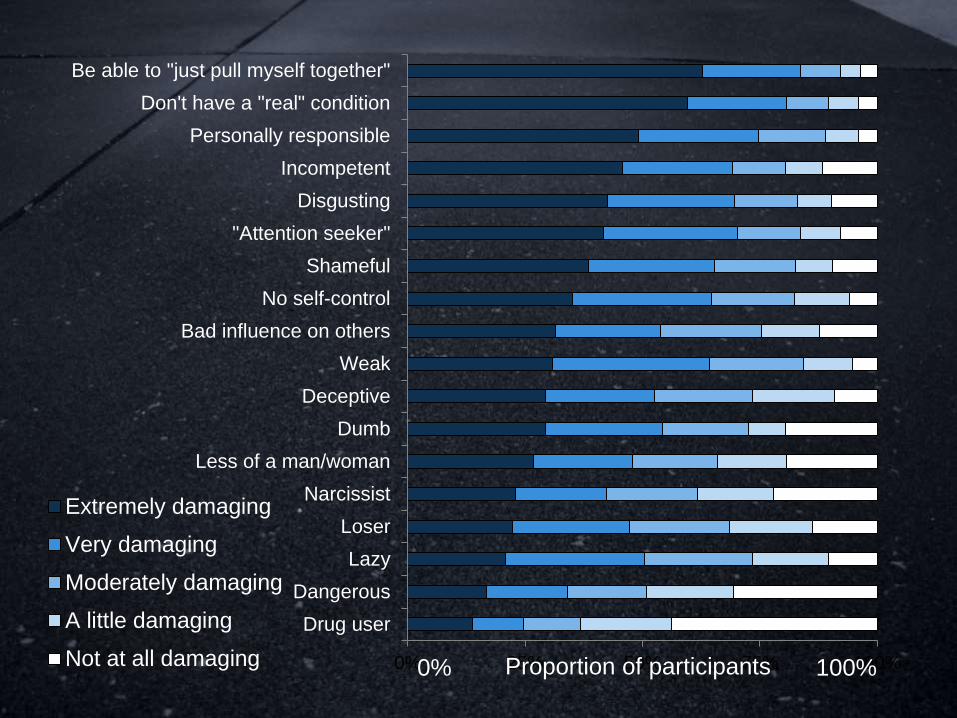
Q. “How damaging have the following
attitudes and beliefs been to your physical or
psychological wellbeing?”
Not at all damaging
A little damaging
Moderately damaging
Very damaging
Extremely damaging
Damage due to stigma

0% 25% 50% 75% 100%
Drug user
Dangerous
Lazy
Loser
Narcissist
Less of a man/woman
Dumb
Deceptive
Weak
Bad influence on others
No self-control
Shameful
"Attention seeker"
Disgusting
Incompetent
Personally responsible
Don't have a "real" condition
Able to just pull myself together
Extremely damaging
Very damaging
Moderately damaging
A little damaging
Not at all damaging Proportion of participants 0% 100%

#1 No self-control
More frequently experienced for bulimia than
for anorexia or EDNOS
Medium/large effect: F(1, 314) = 28.8, p< .001
#2 Less of a man/less of a woman
More frequently experienced for males than
females
Medium effect: F(1 314) = 11.42, p < .001
Notable between-groups differences
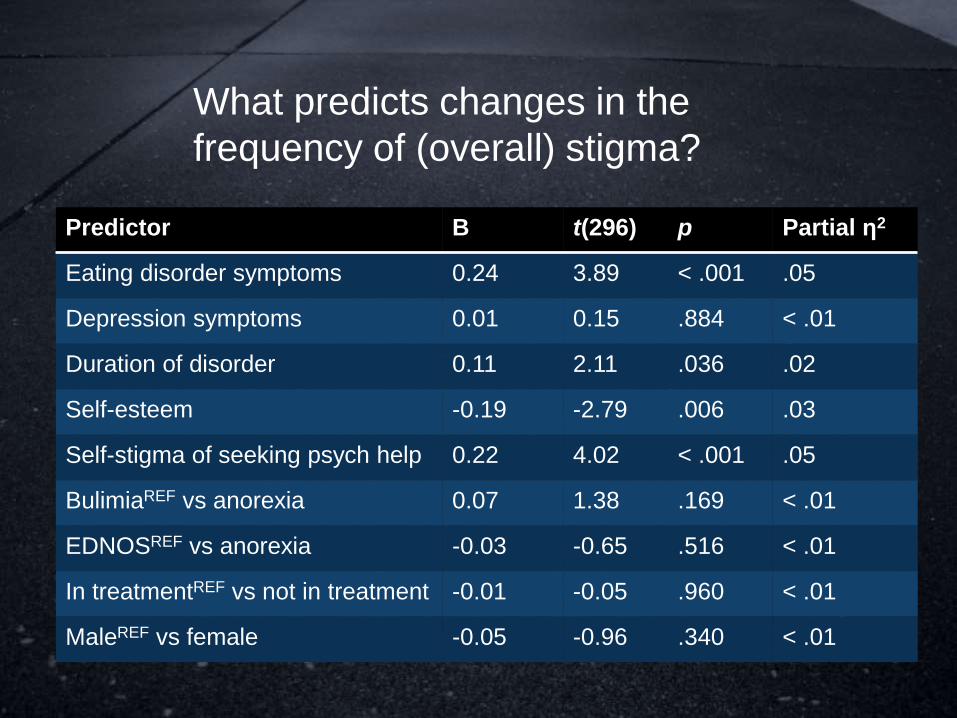
What predicts changes in the
frequency of (overall) stigma?
Predictor B t(296) p Partial η2
Eating disorder symptoms 0.24 3.89 < .001 .05
Depression symptoms 0.01 0.15 .884 < .01
Duration of disorder 0.11 2.11 .036 .02
Self-esteem -0.19 -2.79 .006 .03
Self-stigma of seeking psych help 0.22 4.02 < .001 .05
BulimiaREF vs anorexia 0.07 1.38 .169 < .01
EDNOSREF vs anorexia -0.03 -0.65 .516 < .01
In treatmentREF vs not in treatment -0.01 -0.05 .960 < .01
MaleREF vs female -0.05 -0.96 .340 < .01

#1 Destigmatising eating disorders? Prioritise
the perceptions that eating disorders are trivial
and/or self-inflicted
#2 Destigmatising bulimia? Go after the
perception that sufferers have no self-control
#3 Destigmatising males? Go after the
perception that male sufferers have less
masculinity/manhood
Discussion
#1 Diagnoses were self-reported and not
confirmed through interviews
#2 Cross-sectional design
#3 Few males = limited power to detect sex
differences
#4 Self-stigma may have been a contaminant
Limitations
GRIFFITHS, S., MOND, J. M., MURRAY, S.
B., & TOUYZ, S. (IN PRESS). THE
PREVALENCE AND ADVERSE ASSOCIATIONS
OF STIGMATIZATION IN PEOPLE WITH EATING
DISORDERS. INTERNATIONAL JOURNAL OF
EATING DISORDERS

Comparison of EDE-Q subscale
scores
0
1
2
3
4
5
6
Restraint EatingConcern
ShapeConcern
WeightConcern
Clinical norms(Welch et al. 2011)
Community norms(Mond et al. 2006)
0% 25% 50% 75% 100%
Dangerous
Drug user
Dumb
Narcissist
Lazy
Bad influence on others
Loser
Weak
Less of a man/woman
Disgusting
Incompetent
"Attention seeker"
Shameful
Don't have a "real" condition
No self-control
Deceptive
Personally responsible
Able to "just pull myself together"
Always
Often
Sometimes
Rarely
NeverProportion of participants 0% 100%
0% 25% 50% 75% 100%
Drug user
Dangerous
Lazy
Loser
Narcissist
Less of a man/woman
Dumb
Deceptive
Weak
Bad influence on others
No self-control
Shameful
"Attention seeker"
Disgusting
Incompetent
Personally responsible
Don't have a "real" condition
Be able to "just pull myself together"
Extremely damaging
Very damaging
Moderately damaging
A little damaging
Not at all damaging Proportion of participants 0% 100%
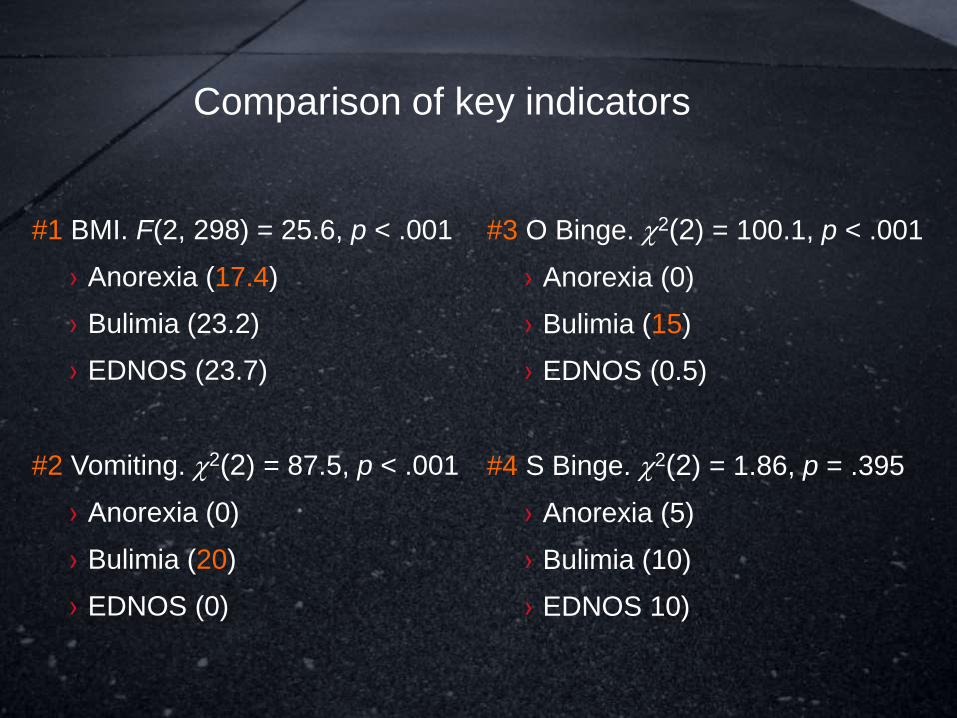
#1 BMI. F(2, 298) = 25.6, p < .001
› Anorexia (17.4)
› Bulimia (23.2)
› EDNOS (23.7)
#2 Vomiting. 2(2) = 87.5, p < .001
› Anorexia (0)
› Bulimia (20)
› EDNOS (0)
Comparison of key indicators
#3 O Binge. 2(2) = 100.1, p < .001
› Anorexia (0)
› Bulimia (15)
› EDNOS (0.5)
#4 S Binge. 2(2) = 1.86, p = .395
› Anorexia (5)
› Bulimia (10)
› EDNOS 10)
#1 Should be able to just ‘pull myself together”
Experienced very often or always: 77.3%
Very damaging or extremely damaging: 83.6%
#2 Personally responsible for my condition
Experienced very often or always: 68.8%
Very damaging or extremely damaging: 74.8%
The two stigma standouts
#4 More stigma is associated with more
marked eating disorder symptoms and a
longer duration of disorder (and vice versa)
#5 More stigma is associated with more self-
stigma of seeking psychological help (and vice
versa)
Discussion