The plain film diagnosis of ischaemic lesions of the colon
6
Clin. Radiol. (1968) 19, 303-308 THE PLAIN FILM DIAGNOSIS OF ISCHAEMIC LESIONS OF THE COLON ERIC SAMUEL and D. J. SINCLAIR* From the Radiodiagnostie Department, Royal Infirmary, Edinburgh (1) The value of plain film findings in ischaemic lesions of the colon has been emphasised. (2) The importance of considering the clinical features in association with the radiological findings in reaching a diagnosis is emphasised. Some of the less common causes have been briefly discussed and illustrated. (3) The similarity of the appearances to those seen in barium enema is noted and the usefulness of the gas content of the bowel as a contrast medium is described. (4) The appearances of vascular changes in association with commoner lesions of the colon are noted and the diagnostic features are recorded. (5) The importance of a combined assessment of the clinical and radiological features is discussed. THE possibility of ischaemic lesions of the colon may first be entertained after inspection of the plain film of the abdomen if certain diagnostic signs are appreciated. These appearances may be typical and will then allow a specific diagnosis, but in the vast majority of cases they are indeter- minate and diagnosis will depend largely on the clinical history together with less positive radio- logical findings. It is the aim of this paper to draw attention to the appearances of ischaemic lesions of the colon as they appear on plain film radio- graphic examination. The radiological features of ischaemic colitis have been described fully by several authors and have been comprehensively reviewed by Schwartz, Boley, Robinson, Krieger, Schultz and Allen (1964). The emphas!s of published reports has, however, largely been placed on contrast examination of the colon and on angiographic studies. The initial diagnostic suspicion must, however, come from the clinical presentation but the features noted on plain film examination of the abdomen may prove valuable corroborative evidence. Schwartz et al. (1964) describe a gas distribution in the bowel which may be normal or similar to that seen in mechanical obstruction or paralytic ileus. Rigler and Pogue (1965) have dealt with the X-ray signs of intestinal necrosis which may follow by recognising the presence of abnormal gas shadows in the bowel wall, abdominal cavity or portal venous system. They also considered the presence of a distended loop with excessive fluid and bowel wall thickening to be evidence of * Present Address: St. Joseph's Hospital, Victoria, B.C., Canada. impending necrosis of the bowel wall. Nelson and Eggleston (1960) described rigid, thick-walled, fixed loops as evidence of mesenteric venous occlusion but these changes are related to small bowel and do not appear in the colon. It is also possible to see in the colon, on the plain film and especially in the supine view, evidence of oedema and submucosal haemorrhage as manifested by thumbprinting and pseudo-tumour formation. These changes are usually well seen in the region of the splenic flexure and transverse colon, the sites of maximum susceptibility to vascular lesions. Many of these patients present as acute abdominal emergencies. The initial film series therefore consists of erect and supine views of the abdomen and an erect view of the chest. The radiological features of importance which are especially looked for in addition to the usual signs of obstruction are:-- (1) The presence of gas in abnormal sites. (2) Segmental bowel distension with oedematous changes in the bowel wall. (3) Evidence of a possible cause of bowel ischaemia. (1) Abnormal Gas.--Vascular injury to the bowel may result in the appearance of gas in abnormal sites, the commonest being within the wall of the bowel, less commonly in the peritoneal cavity after perforation, and still more rarely, within the portal system. The presence of gas in any one of these sites gives a grave prognosis as its appearance indicates necrosis or impending necrosis of the bowel wall. Gas in the portal venous radicles in the liver also indicates necrosis of the bowel wall. It must be 303
-
Upload
eric-samuel -
Category
Documents
-
view
212 -
download
0
Transcript of The plain film diagnosis of ischaemic lesions of the colon

Clin. Radiol. (1968) 19, 303-308
T H E P L A I N F I L M D I A G N O S I S O F I S C H A E M I C L E S I O N S O F T H E C O L O N
ERIC SAMUEL and D. J. SINCLAIR*
From the Radiodiagnostie Department, Royal Infirmary, Edinburgh
(1) The value of plain film findings in ischaemic lesions of the colon has been emphasised. (2) The importance of considering the clinical features in association with the radiological
findings in reaching a diagnosis is emphasised. Some of the less common causes have been briefly discussed and illustrated.
(3) The similarity of the appearances to those seen in barium enema is noted and the usefulness of the gas content of the bowel as a contrast medium is described.
(4) The appearances of vascular changes in association with commoner lesions of the colon are noted and the diagnostic features are recorded.
(5) The importance of a combined assessment of the clinical and radiological features is discussed.
THE possibility of ischaemic lesions of the colon may first be entertained after inspection of the plain film of the abdomen if certain diagnostic signs are appreciated. These appearances may be typical and will then allow a specific diagnosis, but in the vast majority of cases they are indeter- minate and diagnosis will depend largely on the clinical history together with less positive radio- logical findings. It is the aim of this paper to draw attention to the appearances of ischaemic lesions of the colon as they appear on plain film radio- graphic examination.
The radiological features of ischaemic colitis have been described fully by several authors and have been comprehensively reviewed by Schwartz, Boley, Robinson, Krieger, Schultz and Allen (1964). The emphas!s of published reports has, however, largely been placed on contrast examination of the colon and on angiographic studies. The initial diagnostic suspicion must, however, come from the clinical presentation but the features noted on plain film examination of the abdomen may prove valuable corroborative evidence.
Schwartz et al. (1964) describe a gas distribution in the bowel which may be normal or similar to that seen in mechanical obstruction or paralytic ileus. Rigler and Pogue (1965) have dealt with the X-ray signs of intestinal necrosis which may follow by recognising the presence of abnormal gas shadows in the bowel wall, abdominal cavity or portal venous system. They also considered the presence of a distended loop with excessive fluid and bowel wall thickening to be evidence of
* Present Address: St. Joseph's Hospital, Victoria, B.C., Canada.
impending necrosis of the bowel wall. Nelson and Eggleston (1960) described rigid, thick-walled, fixed loops as evidence of mesenteric venous occlusion but these changes are related to small bowel and do not appear in the colon. It is also possible to see in the colon, on the plain film and especially in the supine view, evidence of oedema and submucosal haemorrhage as manifested by thumbprinting and pseudo-tumour formation. These changes are usually well seen in the region of the splenic flexure and transverse colon, the sites of maximum susceptibility to vascular lesions.
Many of these patients present as acute abdominal emergencies. The initial film series therefore consists of erect and supine views of the abdomen and an erect view of the chest. The radiological features of importance which are especially looked for in addition to the usual signs of obstruction a re : - -
(1) The presence of gas in abnormal sites. (2) Segmental bowel distension with oedematous
changes in the bowel wall. (3) Evidence of a possible cause of bowel
ischaemia. (1) Abnormal Gas.--Vascular injury to the
bowel may result in the appearance of gas in abnormal sites, the commonest being within the wall of the bowel, less commonly in the peritoneal cavity after perforation, and still more rarely, within the portal system. The presence of gas in any one of these sites gives a grave prognosis as its appearance indicates necrosis or impending necrosis of the bowel wall.
Gas in the portal venous radicles in the liver also indicates necrosis of the bowel wall. It must be
303
30~ C L I N I C A L R A D I O L O G Y
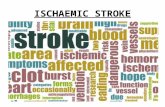
claanges in reg ion o r splenic nexure c o n f i r m e d by b a r i u m e n e m a a n d vascu la r studies. Even tua l ly r e tu rned to no rma l . FIG. I
differentiated from biliary tract gas following an internal biliary fistula and this can be best made by relating the peripheral distribution of gas bubbles in the former condition to gas bubbles more centrally placed when they lie in the biliary tree.
Gas in the bowel wall radiologically presents as linear or curvilinear shadows and these are usually not continuous, but discrete linear shadows lying parallel to the bowel wall and occurring in the infarcted portion of the bowel. Differentiation from pneumatosis coli should not be difficult on clinical grounds and on radiological grounds, as the bubbly appearance of the gas filled cysts is different from the linear shadows of intramural gas. In addition the translucent areas of gas outside the bowel must be differentiated from the normal fat lines in the retroperitoneal tissues (Fig. 1).
(2) Bowel Changes.--When occlusion of the artery supplying the bowel occurs, the first changes are reflected in the mucosa; oedema and haemorrhage occur initially and are later followed by ulceration resulting in the appearance of blood and mucus in the stool. On the plain films the changes in the mucosa of the loop of bowel involved are seen as 'ridging' (or thumbprinting identations) of the gas outline of the bowel. If submucosal haemorrhage has occurred in the affected segment of bowel, then scalloping becomes
more pronounced and 'pseudo-tumour' formation may be seen. The normal sacculations of a partly filled gas loop of colon must be differentiated from this pseudo-turnout appearance and this can best be done by noting the constancy of the appearances and the rounding of the outlines of the imprint defects in vascular lesions as opposed to those caused by incompletely filled gas loops (Fig. 2). In addition there may be evidence of fluid in the mesentery or of free fluid in the peritoneal cavity (Budin and Jacobson, 1967).
The involved loop of bowel may remain fixed in one position and in cases of doubt a repeat examination will confirm the permanence of the changes, enabling differentiation to be made. in one case in our series such appearances were noted for several days (Fig. 3).
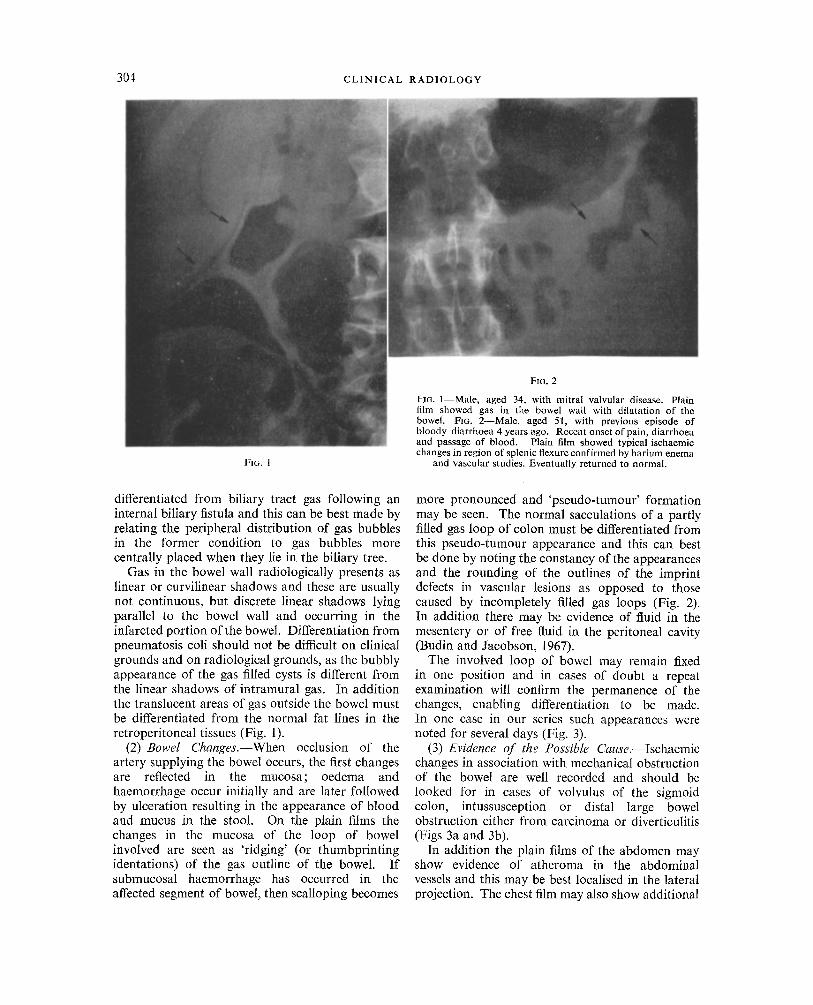
(3) Evidence of the Possible Cause.--Ischaemic changes in association with mechanical obstruction of the bowel are well recorded and should be looked for in cases of volvulus of the sigmoid colon, intussusception or distal large bowel obstruction either from carcinoma or diverticulitis (Figs 3a and 3b).
In addition the plain films of the abdomen may show evidence of atheroma in the abdominal vessels and this may be best localised in the lateral projection. The chest film may also show additional
THE PLAIN FILM DIAGNOSIS OF ISCHAEMIC LESIONS OF THE COLON 305
Fm. 3A
Flo. 3B Female aged 52, with features.of large bowel obstruction. Plain film showed changes in the transverse colon (A) which persisted for six days (B). Changes
confirmed at laparotomy. Obstruction was due to diverticulitis.
evidence by the presence of rheumatic valvular disease or ischaemic ventricular aneurysm as a possible source of the embolus.
Comment.--Most of the common causes of ischaemic changes in the colon have been reported in the literature. They may a r i s e : -
(1) Due to atheroma, embolism, or obstruction from aneurysm formation.
(2) During or following surgery on the lower abdominal aorta.
(3) In association with strangulation due to volvulus, herniation or intussusception.
(4) In association with arterial changes of collagen disorders. Two less widely reported causes have been noted : - - (a) in association with obstruc-
tion due to diverticulitis; (b) following prolonged hypo-
tension or excessive admini- stration of adrenaline or aramine (myamine).
Occlusion may occur in the artery or in the vein independently. The reletive frequency of arterial as opposed to venous occlusion varies with each series reported in the literature and many do not attempt to differentiate. In ad- dition it is well recognised that venous thrombosis occurs as a sequel of arteria~ occlusion. It would also seem equally possible that arterial changes may follow venous occlusion and in this case the progress of events would be slower than when the artery is primarily involved. The following case would seem to illus- trate these features.
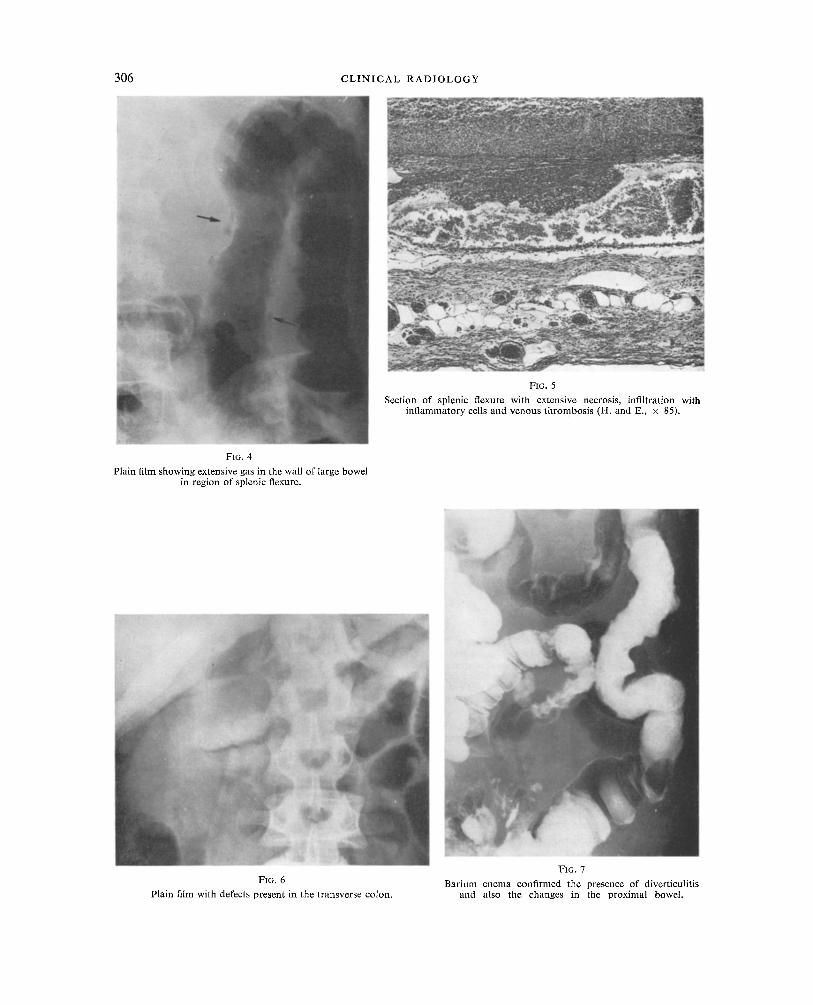
Case W. G.--64-year old diabetic who suffered an episode of loss of consciousness during which he was profoundly hypotensive. This episode was followed by low abdominal pain and profuse diarrhoea (Fig. 4). The patient was treated by left hemicolectomy. The histo- logical studies (Fig. 5) showed extensive venous thrombosis with minimal changes in the arteries in addition to the extensive necrosis.
In this case the profound hypotension may have been a significant factor in the production of the extensive venous thrombosis.
Several cases have been noted recently in the Royal Infirmary of Edinburgh where oedematous changes have been present in the bowel proxi- mal to an area of diverticulitis and the part played by venous occlusion in the production of these radio-
logical and pathological changes has to be evaluated. These changes may follow chronic distension of
the bowel from venous occlusion and the mucosal changes are probably a sequel of infection or thrombophlebitis. The identification of such features, however, is important since the findings may influence the treatment contemplated, between surgical resection or conservative management. Evidence of these changes indicating an oedematous bowel wall would suggest that surgical resection, if undertaken through this area, might lead to difficulties with the suture line.
306 C L I N I C A L R A D I O L O G Y
FIG, 5
Section of splenic flexure with extensive necrosis, infiltration with inflammatory cells and venous thrombosis (H. and E., × 85).
F~G. 4
Plain film showing extensive gas in the wall of large bowel in region of splenic flexure.
FIG. 6
Plain film with defects present in the transverse colon.
FIG. 7
Barium enema confirmed the presence of diverticulitis and also the changes in the proximal bowel.
THE P L A I N F I L M D I A G N O S I S OF I S C H A E M I C L E S I O N S OF THE C O L O N 307
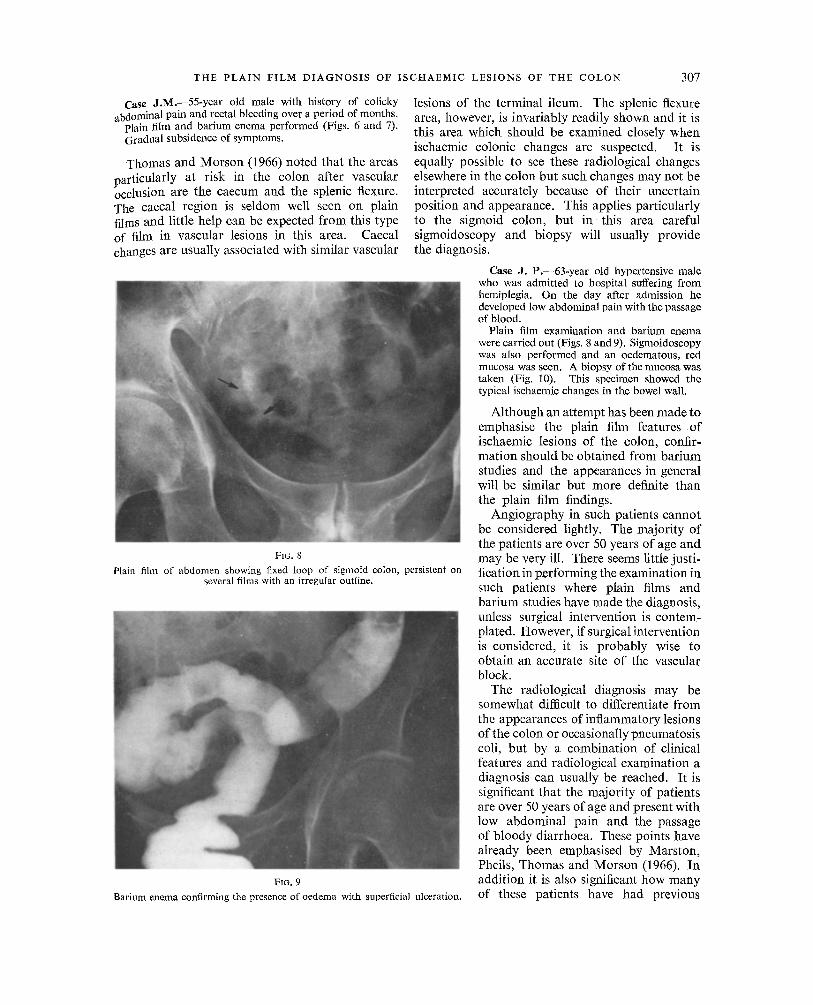
Case J.M.--55-year old male with history of colicky . abdominal pain and rectal bleeding over a period of months.
Plain film and barium enema performed (Figs. 6 and 7). Gradual subsidence of symptoms.
Thomas and Morson (1966) noted that the areas particularly at risk in the colon after vascular occlusion are the caecum and the splenic flexure. The caecal region is seldom well seen on plain films and little help can be expected from this type of film in vascular lesions in this area. Caecal changes are usually associated with similar vascular
FIG. 8
Plain fihn of abdomen showing fixed loop of sigmoid colon, persistent on several films with an irregular outline.
FIG. 9
Barium enema confirming the presence of oedema with staperficial ulceration.
lesions of the terminal ileum. The splenic flexure area, however, is invariably readily shown and it is this area which should be examined closely when ischaemic colonic changes are suspected. It is equally possible to see these radiological changes elsewhere in the colon but such changes may not be interpreted accurately because of their uncertain position and appearance. This applies particularly to the sigmoid colon, but i n this area careful sigmoidoscopy and biopsy will usually provide the diagnosis.
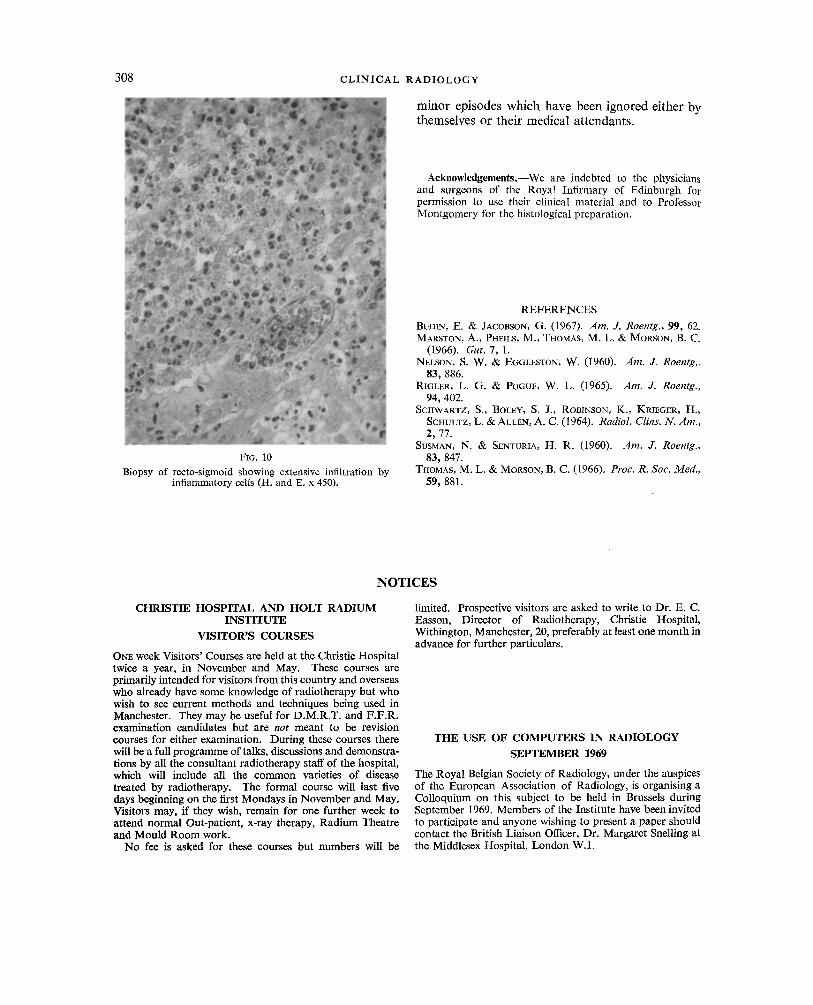
Case J. P.--63-year old hypertensive male who was admitted to hospital suffering from hemiplegia. On the day after admission he developed low abdominal pain with the passage of blood.
Plain film examination and barium enema were carried out (Figs. 8 and 9). Sigmoidoscopy was also performed and an oedematous, red mucosa was seen. A biopsy of the mucosa was taken (Fig. 10). This specimen showed the typical ischaemic changes in the bowel wall.
Although an attempt has been made to emphasise the plain film features of ischaemic lesions of the colon, confir- mation should be obtained from barium studies and the appearances in general will be similar but more definite than the plain film findings.
Angiography in such patients cannot be considered lightly. The majority of the patients are over 50 years of age and may be very ill. There seems little justi- fication in performing the examination in such patients where plain films and barium studies have made the diagnosis, unless surgical intervention is contem- plated. However, if surgical intervention is considered, it is probably wise to obtain an accurate site of the vascular block.
The radiological diagnosis may be somewhat difficult to differentiate f rom the appearances of inflammatory lesions of the colon or occasionally pneumatosis coli, but by a combination of clinical features and radiological examination a diagnosis can usually be reached. It is significant that the majority of patients are over 50 years of age and present with low abdominal pain and the passage of bloody diarrhoea. These points have already been emphasised by Marston, Pheils, Thomas and Morson (1966). In addition it is also significant how many of these patients have had previous
308 C L I N I C A L RADIOLOGY
m i n o r ep i sodes w h i c h h a v e b e e n i g n o r e d e i t h e r by t h e m s e l v e s o r t h e i r m e d i c a l a t t e n d a n t s .
Acknowledgements.--We are indebted to the physicians and surgeons of the Royal Infirmary of Edinburgh for permission to use their clinical material and to Professor Montgomery for the histological preparation.
FIG. 10 Biopsy of recto-sigmoid showing extensive infiltration by
inflammatory cells (H. and E. x 450).
REFERENCES
BUDIN, E. & JACOBSON, G. (1967). Am. J. Roentg., 99, 62. MARSXON, A., PHEmS, M., THOMAS, M. L. & MORSON, B. C.
(1966). Gut, 7, 1. NELSON, S. W. & EG6LESTON, W. (1960). Am. J. Roentg.,
83, 886. R~GLER, L. G. & POGUE, W. L, (1965). Am. J. Roentg.,
94, 402. SCHWARTZ, S., BOLEY, S. J., ROBINSON, K., KRIEGER, H.,
SCHULTZ~ L. &ALLAN, A. C. (1964). Radiol. Clins. N. Am., 2, 77.
SUSMAN, N. & SENTURIA, H. R. (1960). Am. J. Roentg., 83, 847.
THOMAS, M. L. & MORSON, B. C. (1966). Proc. R. Soc. Med., 59, 881.
N O T I C E S
CHRISTIE HOSPITAL AND HOLT RADIUM INSTITUTE
VISITOR'S COURSES
ONE week Visitors' Courses are held at the Christie Hospital twice a year, in November and May. These courses are primarily intended for visitors from this country and overseas who already have some knowledge of radiotherapy but who wish to see current methods and techniques being used in Manchester. They may be useful for D.M.R.T. and F.F.R. examination candidates but are not meant to be revision courses for either examination. During these courses there will be a full programme of talks, discussions and demonstra- tions by all the consultant radiotherapy staff of the hospital, which will include all the common varieties of disease treated by radiotherapy. The formal course will last five days beginning on the first Mondays in November and May. Visitors may, if they wish, remain for one further week to attend normal Out-patient, x-ray therapy, Radium Theatre and Mould Room work.
No fee is asked for these courses but numbers will be
limited. Prospective visitors are asked to write to Dr. E. C. Easson, Director of Radiotherapy, Christie Hospital, Withington, Manchester, 20, preferably at least one month in advance for further particulars.
THE USE OF COMPUTERS IN RADIOLOGY
SEPTEMBER 1969
The Royal Belgian Society of Radiology, under the auspices of the European Association of Radiology, is organising a Colloquium on this subject to be held in Brussels during September 1969. Members of the Institute have been invited to participate and anyone wishing to present a paper should contact the British Liaison Officer, Dr. Margaret Snelling at the Middlesex Hospital, London W.1.

![Neurotoxic dorsal CA1 lesions versus 4 VO ischaemic ... · CA1 field may underlie impairments, which chiefly involve anterograde memory loss [14, 40, 43], and re-semble deficits](https://static.fdocuments.net/doc/165x107/60a2e0f383e52c165e435b5c/neurotoxic-dorsal-ca1-lesions-versus-4-vo-ischaemic-ca1-ield-may-underlie.jpg)