The oral and dental complications associated with the use ...
26
Mohamed Hania
Transcript of The oral and dental complications associated with the use ...
Mohamed Hania

Introduction
Oral & Dental Complications of RPDs
Literature Review
Discussion
Conclusions

Definition :- Removable partial dentures (RPDs) are dental prostheses that replace one or more missing teeth but not all They receive support and retention from underlying tissues and from some, if not all, of the remaining teeth They can be removed by the patient from the oral cavity Must have adequate support, retention, and
stability Used to restore function, occlusion, aesthetics and
phonetics
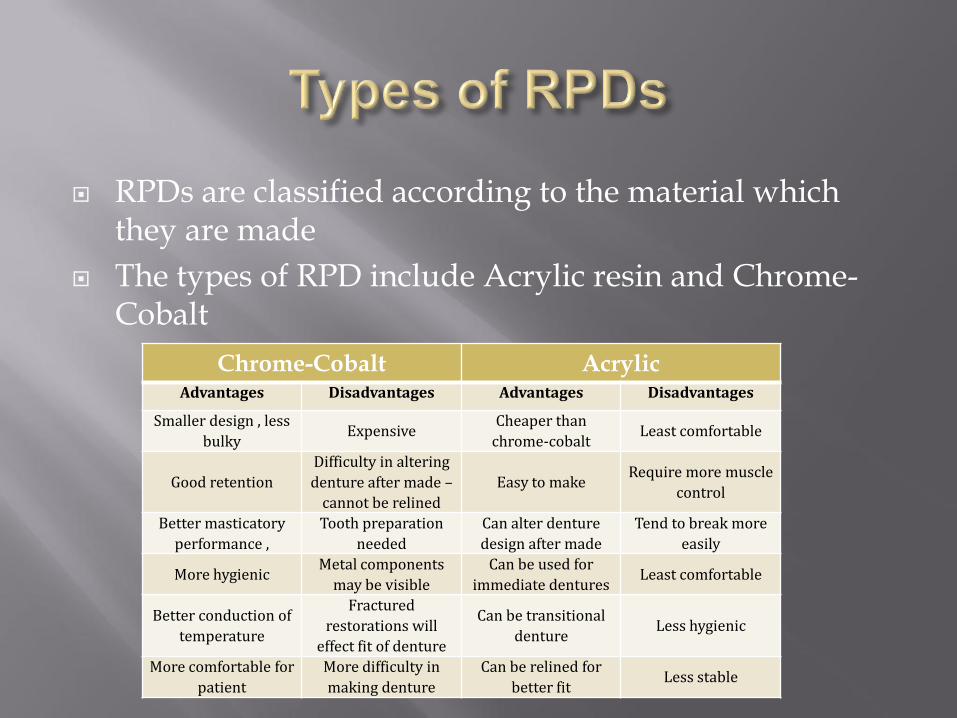
RPDs are classified according to the material which they are made
The types of RPD include Acrylic resin and Chrome-Cobalt
Chrome-Cobalt Acrylic Advantages Disadvantages Advantages Disadvantages
Smaller design , less
bulky Expensive
Cheaper than
chrome-cobalt Least comfortable
Good retention
Difficulty in altering
denture after made –
cannot be relined
Easy to make Require more muscle
control
Better masticatory
performance ,
Tooth preparation
needed
Can alter denture
design after made
Tend to break more
easily
More hygienic Metal components
may be visible
Can be used for
immediate dentures Least comfortable
Better conduction of
temperature
Fractured
restorations will
effect fit of denture
Can be transitional
denture Less hygienic
More comfortable for
patient
More difficulty in
making denture
Can be relined for
better fit Less stable
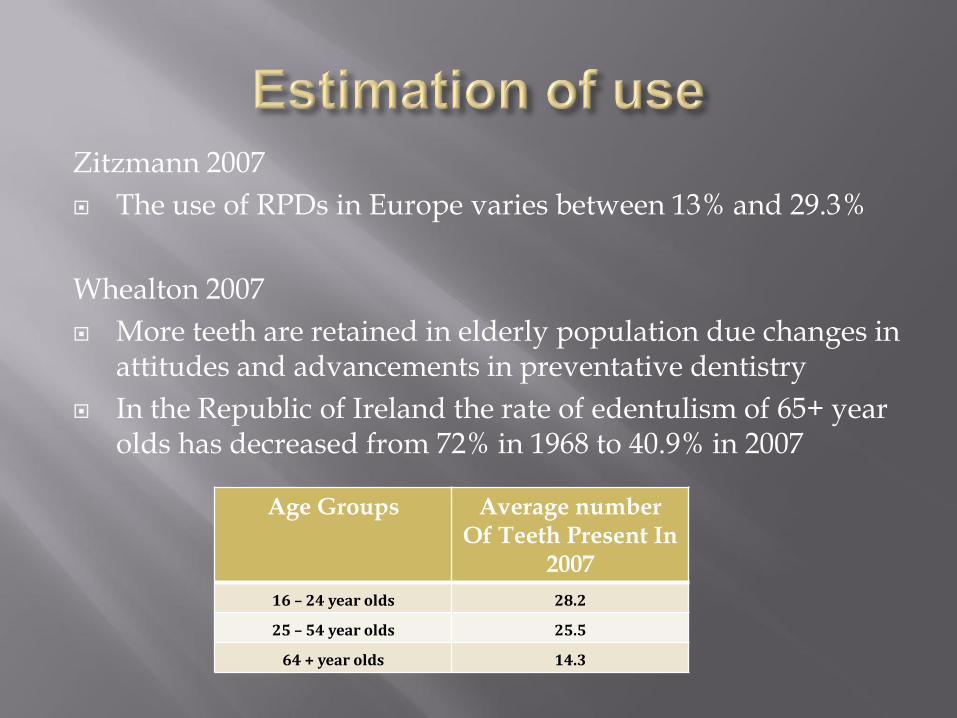
Zitzmann 2007
The use of RPDs in Europe varies between 13% and 29.3%
Whealton 2007
More teeth are retained in elderly population due changes in attitudes and advancements in preventative dentistry
In the Republic of Ireland the rate of edentulism of 65+ year olds has decreased from 72% in 1968 to 40.9% in 2007
Age Groups Average number Of Teeth Present In
2007
16 – 24 year olds 28.2
25 – 54 year olds 25.5
64 + year olds 14.3
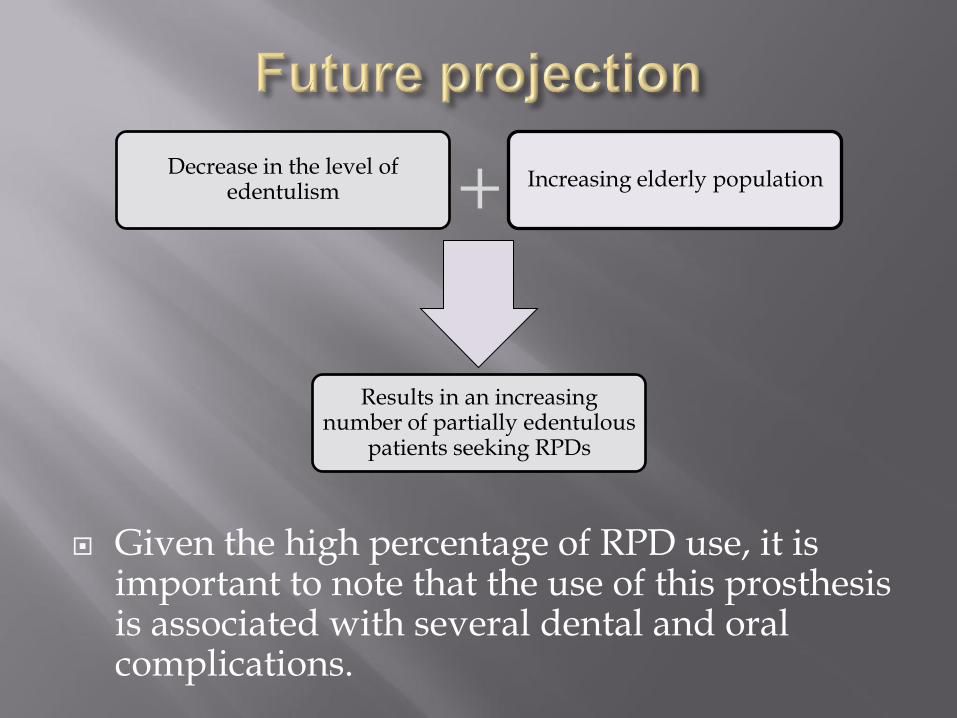
Given the high percentage of RPD use, it is important to note that the use of this prosthesis is associated with several dental and oral complications.
Decrease in the level of edentulism
Increasing elderly population
Results in an increasing number of partially edentulous
patients seeking RPDs
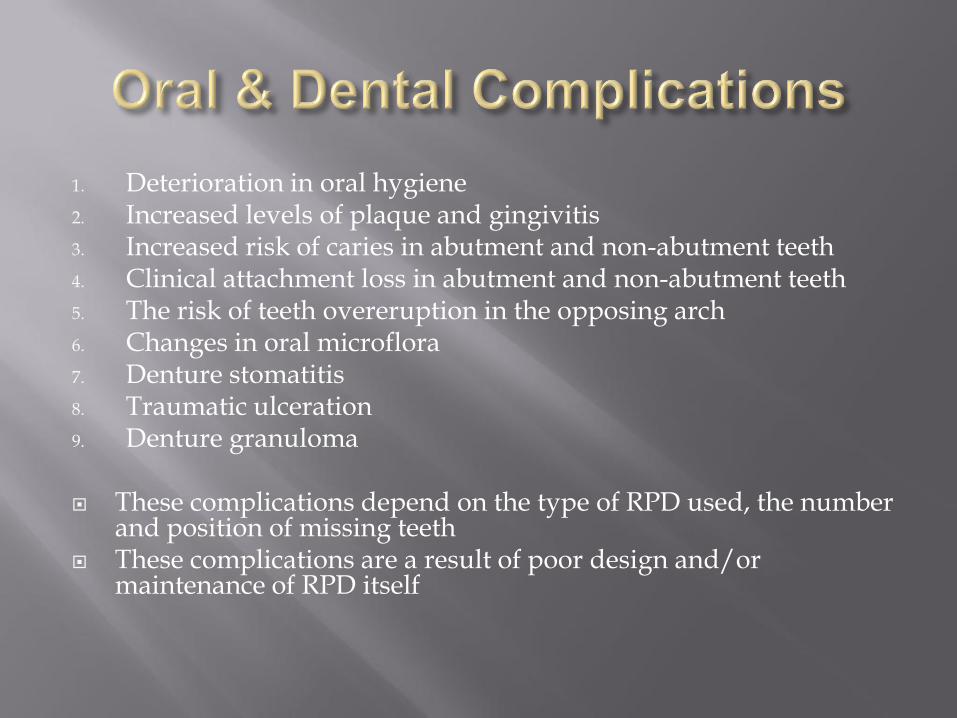
1. Deterioration in oral hygiene 2. Increased levels of plaque and gingivitis 3. Increased risk of caries in abutment and non-abutment teeth 4. Clinical attachment loss in abutment and non-abutment teeth 5. The risk of teeth overeruption in the opposing arch 6. Changes in oral microflora 7. Denture stomatitis 8. Traumatic ulceration 9. Denture granuloma These complications depend on the type of RPD used, the number
and position of missing teeth These complications are a result of poor design and/or
maintenance of RPD itself
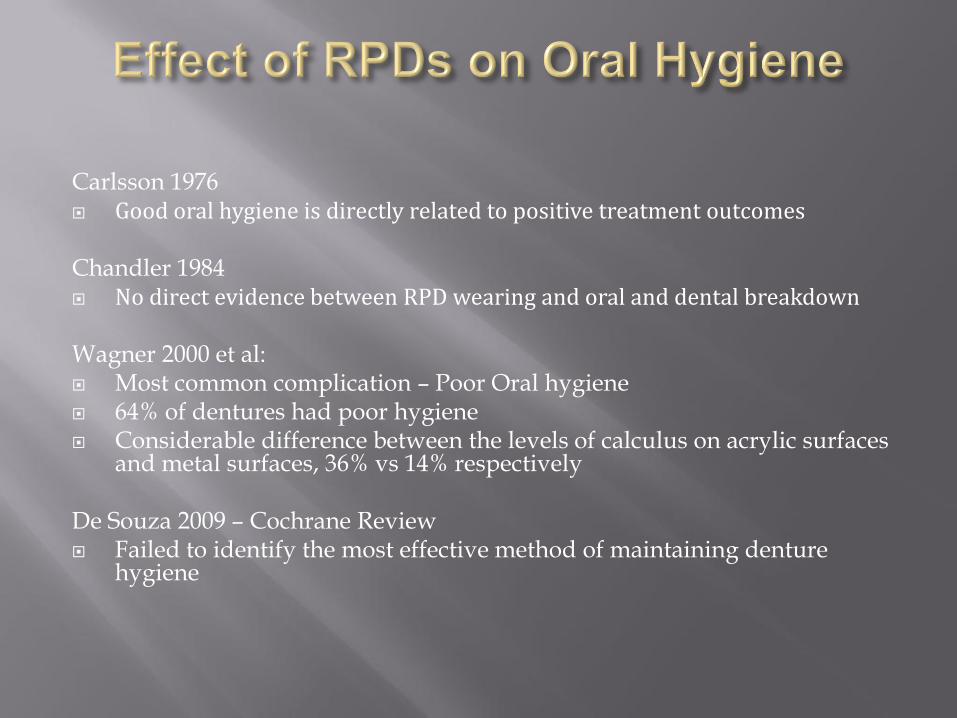
Carlsson 1976 Good oral hygiene is directly related to positive treatment outcomes Chandler 1984 No direct evidence between RPD wearing and oral and dental breakdown Wagner 2000 et al: Most common complication – Poor Oral hygiene 64% of dentures had poor hygiene Considerable difference between the levels of calculus on acrylic surfaces
and metal surfaces, 36% vs 14% respectively De Souza 2009 – Cochrane Review Failed to identify the most effective method of maintaining denture
hygiene

Author(S) , Year Design of Study Sample Size Control Results
Carlsson, GE, 1976 13 year retrospective study 58 patients No control
Majority of patients need
treatment for caries,
periodontitis and other
prosthodontic treatment
Good oral hygiene is directly
related to positive treatment
outcomes
Chandler, JA, 1984 8- to 9-year retrospective
study 38 patients Non-RPD 9wearers
RPD wearing resulted in no
difference in the levels of caries,
probing depths, tooth mobility
and bone loss when compared
to non RPD wearers.
RPDs caused increased levels of
gingival inflammation in areas
that were covered and in the
gingivae apical to clasp arms.
No direct evidence between RPD
wearing and oral and dental
breakdown.
Wagner B, 2000
Retrospective study
10 years after provision of
RPDs
74 patients No control
Several abutment teeth
supporting an RPD had better
success rate
Non – Clasp retained RPDs had a
higher failure rate (66.7%) than
Clasp Retained Partial Denture
(44.8%)
De Souza, RF et al, 2009
Cochrane review
Randomized controlled trials
(RCTs)
N/A N/A
Six RCTs could not be compared
due to wide range of variables
and different interventions.

Bergman et al 1977,1982 RPDs that are carefully designed and accompanied with good oral hygiene and regular
follow ups, caused little deterioration in periodontal health Issues with occlusion, mastication, stability and clasp retention
Yusuf 1989 The frequency and severity of the complications tended to increase with increasing age
of the RPDs Kearn 2001 Disproportionately more number of abutment teeth being lost compared to non-
abutment teeth (26.4% vs 14.2% respectively) Recommended Maintenance regime Zlataric et al 2002 Natural abutment teeth had the highest levels of plaque(PI) and gingivitis(GI) similar
levels to surveyed crowns on abutments Mobility(TM) of abutment teeth was grade one in 50% of cases. Non abutment performed better for levels of PI, GI and TM but had significantly more
gingival recession Recommended Maintenance regime
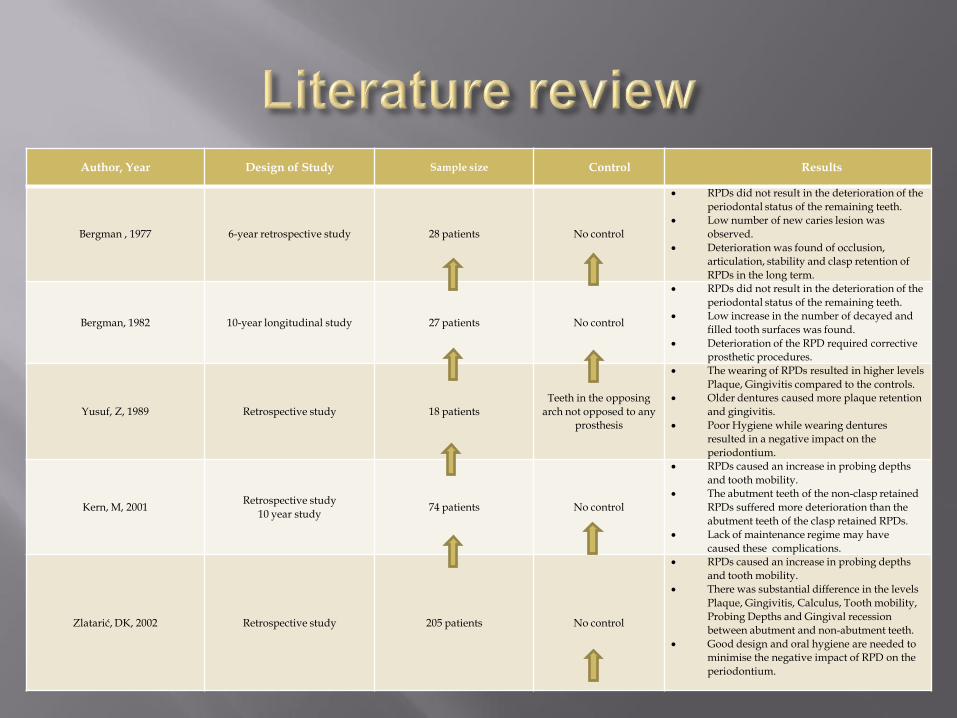
Author, Year Design of Study Sample size Control Results
Bergman , 1977 6-year retrospective study 28 patients No control
RPDs did not result in the deterioration of the
periodontal status of the remaining teeth.
Low number of new caries lesion was
observed.
Deterioration was found of occlusion,
articulation, stability and clasp retention of
RPDs in the long term.
Bergman, 1982 10-year longitudinal study 27 patients No control
RPDs did not result in the deterioration of the
periodontal status of the remaining teeth.
Low increase in the number of decayed and
filled tooth surfaces was found.
Deterioration of the RPD required corrective
prosthetic procedures.
Yusuf, Z, 1989 Retrospective study 18 patients
Teeth in the opposing
arch not opposed to any
prosthesis
The wearing of RPDs resulted in higher levels
Plaque, Gingivitis compared to the controls.
Older dentures caused more plaque retention
and gingivitis.
Poor Hygiene while wearing dentures
resulted in a negative impact on the
periodontium.
Kern, M, 2001 Retrospective study
10 year study 74 patients No control
RPDs caused an increase in probing depths
and tooth mobility.
The abutment teeth of the non-clasp retained
RPDs suffered more deterioration than the
abutment teeth of the clasp retained RPDs.
Lack of maintenance regime may have
caused these complications.
Zlatarić, DK, 2002 Retrospective study 205 patients No control
RPDs caused an increase in probing depths
and tooth mobility.
There was substantial difference in the levels
Plaque, Gingivitis, Calculus, Tooth mobility,
Probing Depths and Gingival recession
between abutment and non-abutment teeth.
Good design and oral hygiene are needed to
minimise the negative impact of RPD on the
periodontium.
Budtz-Jorgensen 1990 Caries detected at six times the frequency in RPD
wearing than patients who were provided with cantilever resin bonded bridges
Jepson (RCT) 2001 RPD wearers had nearly five times more caries
lesions when compared to those with fixed prostheses
Steele 1997 & Nevalainen 2004 Increased susceptibility to root caries

Author, Year Design of Study Sample Size Control Results
Jepson, NJ, 2001 Randomised control trial
2 years 60 patients
Cantilever resin bonded
bridges (RBBs)
Bigger increase in the levels of
new and recurrent caries lesions
in patients wearing RPDs than
patients provided with cantilever
RBBs.
Budtz-jorgensen, 1990 A 5 year longitudinal study 53 patients Fixed partial denture opposing
complete upper denture
Caries was 6 times more likely in
patients with RPD than patients
with FPD.
Occlusion and function
deteriorated in the RPD patients
only.
RPD patients needed more
follow-upprosthodontic
treatment than FPD patients.
Nevalainen, MJ, 2004 5 year follow-up study 113 patients No control
RPD patients had higher levels of
salivary microbes and higher
root caries incidence than those
with natural teeth.
Steele J.G 1997 Cross sectional study 1228 patients Control is previous disease
history
RPDs increased the risk of having
root caries.
RPDs use should precipitate
additional steps to prevent root
caries.
Kiliardis 2000 & Craddock 2004 Overeruption of molars with no opposing dentition
occurred in 82% to 83% of cases
Matsuda 2014 Overeruption can occur in 38.1% of cases in patients
provided with RPDs, 57.1% in unopposed teeth, and 4.1% in teeth opposed by natural dentition
This may be due to wearing of the artificial teeth and/or the displacement of denture by residual ridge resorption
Which can be minimized by having regular relining and/or replacement of artificial teeth i.e. maintenance regimes

John MT 2004 Provision of fixed partial dentures, RPDs, and
complete dentures He found there was an improvement in quality of
life in all patients The provision of fixed partial dentures resulted in
the greatest improvement in the patient’s quality of life
Aleem 2009 & Jepson 1995 Observed that just replacing RPDs will have a
positive effect on patient’s quality of life Patient acceptance and satisfaction with RPDs was
still poor
Baxter 1984 & Krall 1998
Found that there was either little or no relationship between fully dentate patients and patients with RPDs on nutrition
Factors such as financial and socioeconomic status were more likely to be a significant factor on nutrition
Shinkai 2001
RPDs had poorer masticatory performance, compared with fully dentate patients
Nutritional intake did not differ

Nordlund 2009 Streptococcus Mutans and Lactobacilli are the microorganisms
responsible for the caries process Beighton 1990 & Tanka 2009 They are found in higher levels in patients wearing RPDs
than in patients with fixed prostheses & natural dentition Candida Albican was detected to be three times higher in
RPD wearers Mihalow 1998 Levels of Strep Mutans increased within 4-6 months of RPD
wearing Preshaw 2011 Periodontal disease-causing pathogens were found to be in
insignificant levels in RPD wearing patients compared to non-RPD wearing patients
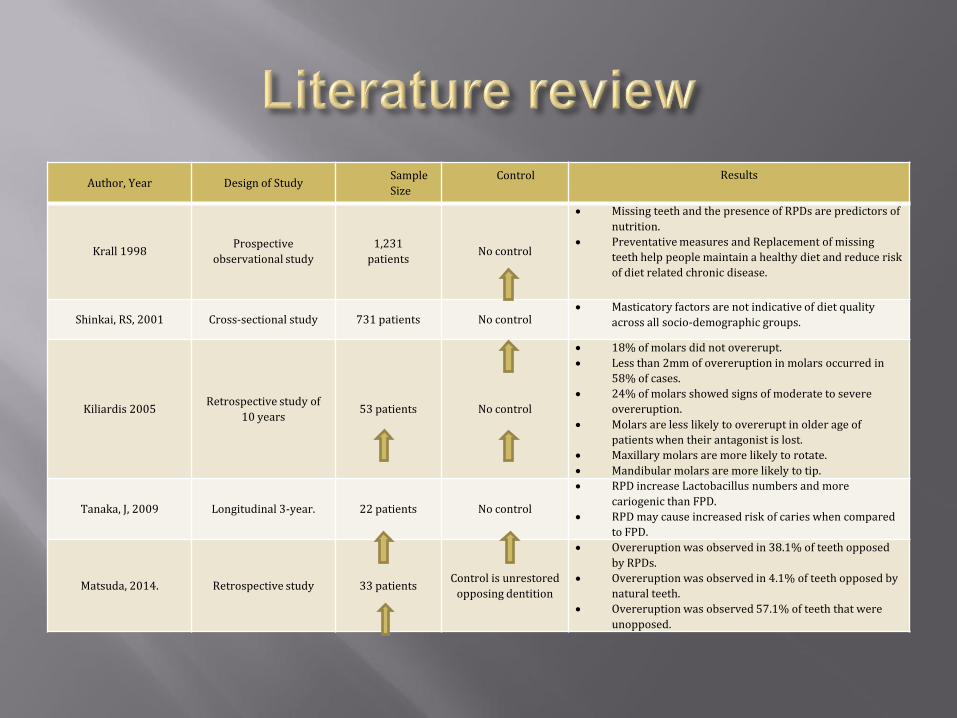
Author, Year Design of Study Sample
Size
Control
Results
Krall 1998 Prospective
observational study
1,231
patients No control
Missing teeth and the presence of RPDs are predictors of
nutrition.
Preventative measures and Replacement of missing
teeth help people maintain a healthy diet and reduce risk
of diet related chronic disease.
Shinkai, RS, 2001 Cross-sectional study 731 patients No control Masticatory factors are not indicative of diet quality
across all socio-demographic groups.
Kiliardis 2005 Retrospective study of
10 years 53 patients No control
18% of molars did not overerupt.
Less than 2mm of overeruption in molars occurred in
58% of cases.
24% of molars showed signs of moderate to severe
overeruption.
Molars are less likely to overerupt in older age of
patients when their antagonist is lost.
Maxillary molars are more likely to rotate.
Mandibular molars are more likely to tip.
Tanaka, J, 2009 Longitudinal 3-year. 22 patients No control
RPD increase Lactobacillus numbers and more
cariogenic than FPD.
RPD may cause increased risk of caries when compared
to FPD.
Matsuda, 2014. Retrospective study 33 patients Control is unrestored
opposing dentition
Overeruption was observed in 38.1% of teeth opposed
by RPDs.
Overeruption was observed in 4.1% of teeth opposed by
natural teeth.
Overeruption was observed 57.1% of teeth that were
unopposed.
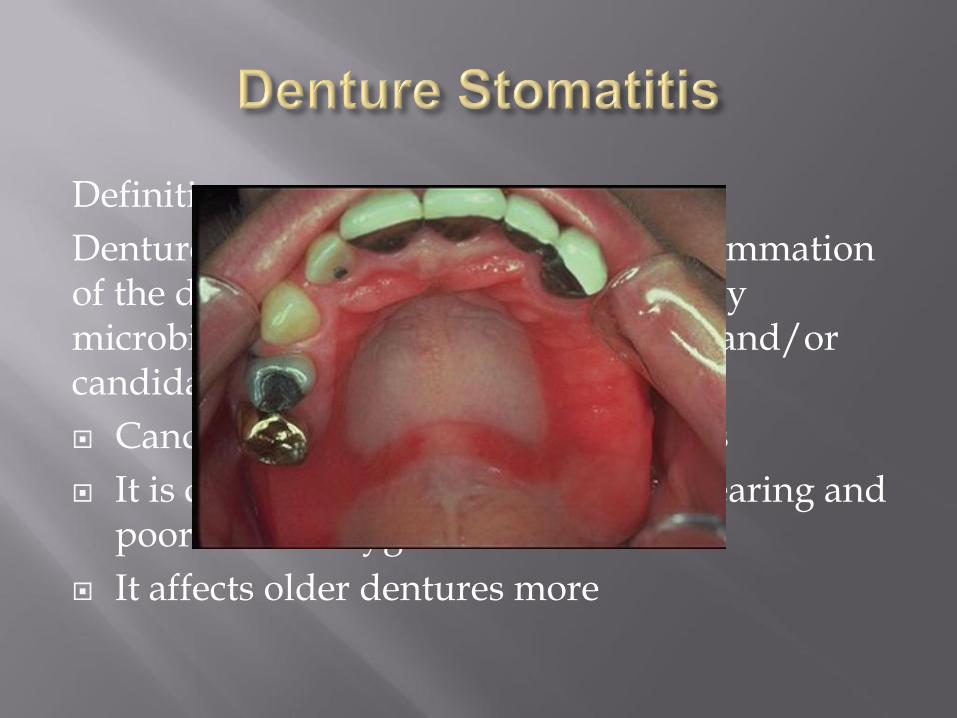
Definition :-
Denture stomatitis is defined as an inflammation of the denture bearing mucosa caused by microbial plaque composed of bacteria and/or candida species
Candida involvement in 90% of cases
It is caused by night-time denture wearing and poor denture hygiene
It affects older dentures more

Traumatic ulcers which are a break in the lining of epithelium caused by mechanical injury to the mucosa by RPDs
Chronic irritation by a denture can result in a condition called denture granuloma
benign hyperplasia of fibrous connective tissue and is most commonly found in the sulci where the denture is overextended

It is clear from the research of the literature that well-designed, randomised controlled studies with large sample size is lacking
It is difficult to extrapolate valuable conclusions regarding RPD complications, as the baselines of the patient’s oral health have not been established and poor level of evidence in the literature
It can be reasonable to assume that some oral and dental complications can be a result of certain risk factors (poor oral hygiene and diet, untreated periodontal disease etc) of patients remaining following prosthodontic treatment
RPDs alone is not a major risk factor

Nonetheless complications of RPDs are extensive and real. The design of the RPD is very critical in maintaining periodontal health
and a need for a maintenance regime Kratochvil, 1963 In distal extensions RPDs – RPI system Kapur (RCT) 1994 I Bars vs Occlusally approaching clasps McHenry 1992 Lingual bars causes significantly less gingival inflammation than lingual
plates Zlataric 2002 RPDs should be located as far away from the gingival margin as possible
to prevent gingival trauma and inflammation. Every effort should be made to retain posterior teeth for the distal extensions The options of implant supported dentures or the use of attachments should be explored

The oral and dental complications of RPDs are extensive and can be severe but that should NOT preclude them as a treatment modality
The complications that are widely known can be minimised if not eliminated with careful design, beginning at mounted study cast stage and a regular maintenance regime following delivery of prosthesis
RPDs are still an effective treatment modality , have a major role in replacing missing teeth which can restore function, occlusion, aesthetics and phonetics

Shinkai, RS, 2001. Oral function and diet quality in a community based sample, Journal of Dental Research 80:1625-1630
Nordlund, A, 2009. Improved ability of biological and previous caries multimarkers to predict caries disease as revealed by multivariate PLS modelling , Biomed Central Oral Health 9,28
Tanaka, J, 2009. Longitudinal research on the oral cavity of elderly wearing fixed or removable prostheses , Journal of Prosthodontic Research 53:83-8
Beighton, D, 1990. Associations between salivary levels of mutans streptococci ,lactobacilli , yeasts and black pigmented bacteroids spp and dental variables in elderly patients, Archives of Oral Biology 35, 173s-175s
Milhalow, DM, 1988. The influence of removable partial dentures on the level of strep mutans in saliva, Journal of Prosthetic Dentistry, 59, 49-51.
Preshaw, P.M, 2011. Association of removable partial denture use with oral and systemic health, Journal of Dentistry, 08, 18
Tanaka, J, 2009. Longitudinal research on the oral cavity of elderly wearing fixed or removable prostheses, Journal of Prosthodontic Research 53:83-8
Jean B, 2003. Reassessing the presence of Candida albicans in denture related stomatitis . Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 95: 1
Scully, C, 2008. Oral and maxillofacial medicine: the basis of diagnosis and treatment. 2nd ed. Edinburgh: Churchill Livingstone.
Tyldesley, AF, 2003. Tyldesleys's Oral Medicine. 5th ed. Oxford: Oxford University Press. Newton, A.V 1962. Denture sore mouth. British Dental Journal 112:357-60, Neville, BW, 2002. Oral &Maxillofacial pathology. 2nd ed. Philadelphia: W.B. Saunders.
Chandler, JA, 1984. Clinical evaluation of patients 8 to 9 years after placement of removable partial denture Journal of Prosthetic Dentistry 51;736-43
Zlatarić, DK, 2002. The effect of removable partial dentures on periodontal health of abutment and non-abutment teeth Journal of Periodontology 73(2): 137-144
Yusuf, Z, 1989. Periodontal status of teeth in contact with denture in removable partial denture wearers Journal of Oral Rehabilitation 16:119-26
Kern, M, 2001. Periodontal findings in patients 10 years after insertion of removable partial dentures Journal of Oral Rehabilitation 28:991-997
Kratochvil, f, 1963. Influence of occlusal rest position and clasp design on movement of abutment teeth Journal of Prosthetic Dentistry 13,114-124
Kratochvil, f, 1963. Influence of occlusal rest position and clasp design on movement of abutment teeth Journal of Prosthetic Dentistry 13,114-124
Kapur, KK, 1994. A randomized clinical trial of two basic removable partial denture designs Part 1 comparisons of five-year success rates and periodontal health Journal of Prosthetic Dentistry 72:268-282
McHenry, 1992. The effect of removable partial denture framework design on gingival inflammation a clinical model Journal of Prosthetic Dentistry 68:799-803
Zlatarić, DK, 2002.The effect of removable partial dentures on periodontal health of abutment and non-abutment teeth Journal of Periodontology 73(2): 137-144
Dinh X. Bui. Removable Partial Denture and its Effects on Periodontal Health. [ONLINE] Available at: http://www.drbui.com/artrpd.html.
Budtz-jorgensen, 1998. Alternate frame work designs for removable partial dentures , Journal of Prosthetic Dentistry 80:58-66
Jepson, NJ, 2001. Caries incidence following restoration of shortened lower dental arch in randomised controlled trial British Dental Journal 191:140-144
Budtz-jorgensen, 1990. A 5 year longitudinal study of cantilevered fixed partial dentures compared with removable partial dentures in a geriatric population, Journal of Prosthetic Dentistry 64:42-47
Nevalainen, MJ, 2004. A 5 year follow-up study on the prosthetic rehabilitation of the elderly in Finland, Journal of Oral Rehabilitation 31;647-653
Steele, JG, 1997. Partial denture as an independent indicator of root caries risk in group of older adults ,Gerodontology 14:67-74
Carlsson, GE, 2005. Tooth movement, British Dental Journal 198:420-421 ,
Kiliaridis, 2000. Vertical position , rotation and tipping of molars without antagonists, International Journal of Prosthodontics 13:480-486
Craddock, HL, A study of the incidence of over eruption and occlusal interferences in unopposed posterior teeth British Dental journal 196:341-348
Matsuda, 2014. Over eruption of teeth opposing removable partial denture : a preliminary study, International Journal of Prosthodontics 27:475-476
John, MT, Oral health-related quality of life in patients treated with fixed , removable and complete dentures , International Journal of Prosthodontics 17:503-511
John, MT, Oral health-related quality of life in patients treated with fixed , removable and complete dentures , International Journal of Prosthodontics 17:503-511
Aleen, PF, 2009. Determining the minimally important difference for the oral health impact profile, European Journal of Oral Science 117:129-34
Jepson, NJ, 1995.The influence of denture design on patient acceptance of partial dentures, British dental journal 178:296-300
Makila, 1969. Effects of complete dentures on dietary intake and serum levels of pantothenic acid , folic acid and iron in edentulous person, Suomen Hammaslaakariseuran Toimitukisia 65:299-311
Baxter, JC, 1984. The nutritional intake of geriatric patients with varied dentitions , Journal of Prosthetic Dentistry 51:164-168
Krall, E, 1998. How dentition status and masticatory function affect nutrient intake , Journal of the American Dental Association 129:1261-1269

Carr, AC, 2005. McCracken’s Removable Partial Prosthodontics. 5th ed. St. Louis, Missouri: Elsevier Mosby
Carr, AC, 2005. McCracken’s Removable Partial Prosthodontics. 5th ed. St. Louis, Missouri: Elsevier Mosby
Zitzmann, NU, 2007. What is the prevalence of various types of prosthetic dental restorations in Europe?, Clinical Oral Implants Research 18:20-33
Preshaw, P.M, 2011. Association of removable partial denture use with oral and systemic health. Journal of Dentistry, 08, 18
Whelton, H. A Ten year longitudinal study: Oral health of Irish adults 2000-02. Department of Health and Children. Brinswick Press LTD. Final report ,April 2007
Whelton, H. A Ten year longitudinal study: Oral health of Irish adults 2000-02. Department of Health and Children. Brinswick Press LTD. Final report ,April 2007
Whelton, H. A Ten year longitudinal study: Oral health of Irish adults 2000-02. Department of Health and Children. Brinswick Press LTD. Final report ,April 2007
Vaupel, JW, 2010. Bio demography of human ageing. Nature, 464
Douglas, CW, 1988. Need and effective demand for prosthodontic treatment. Journal of Prosthetic Dentistry, 59, 94-104
Carr, AC, 2005. McCracken’s Removable Partial Prosthodontics. 5th ed. St. Louis, Missouri: Elsevier Mosby
Carr, AC, 2005. McCracken’s Removable Partial Prosthodontics. 5th ed. St. Louis, Missouri: Elsevier Mosby
Preshaw, P.M, 2011. Association of removable partial denture use with oral and systemic health. Journal of Dentistry, 08, 18
Wagner B, 2000. Clinical evaluation of Removable partial denture 10 years after insertion Clinical Oral Investigations 4:74-80
Wagner B, 2000. Clinical evaluation of Removable partial denture 10 years after insertion Clinical Oral Investigations 4:74-80
De Souza, RF et al, 2009. Intervention for cleaning dentures for adults (Cochrane review) CD007395
Carlsson, GE, 1976. Late results of treatment with removable partial denture Journal of Oral Rehabilitation 3,267-272
Wagner, B, 2000. Clinical evaluation of Removable partial denture 10 years after insertion, Clinical Oral Investigations 4:74-80
Kratochvil, f, 1963. Influence of occlusal rest position and clasp design on movement of abutment teeth, Journal of Prosthetic Dentistry 13,114-124
Chandler, JA, 1984. Clinical evaluation of patients 8 to 9 years after placement of removable partial denture , Journal of Prosthetic Dentistry 51;736-43
Bergman,B ,1982.Caries, periodontal and prosthetic findings in patients with removable partial dentures , Journal of Prosthetic Dentistry 48,506-514
Bergman B, 1977.Caries and periodontal status in patients fitted with removable partial dentures. 4,132-146
Bergman,B ,1982.Caries, periodontal and prosthetic findings in patients with removable partial dentures: a ten-year longitudinal study, Journal of Prosthetic Dentistry 48,506-51