
· The Ministry of Health wishes to sincerely thank the technical advice and assistance provided...
82
Transcript of · The Ministry of Health wishes to sincerely thank the technical advice and assistance provided...


22

1


33

4
P a g e | 5
MESSAGE FROM MINISTER
The development of the Health Emergency and Disaster Management Plan (HEADMAP) paves way for the health staff to effectively respond to emergencies and disasters. This edition of the HEADMAP is committing the Ministry of Health in efforts to build a resilient culture towards disasters and also adopt new ideas such as climate change and an all-hazard approach in disaster management.
Disaster management is about people and the ability for them to plan, prepare and mitigate factors which are within their control. I am confident that with this revised HEADMAP the Ministry and its staff will be able to response much more effectively and efficiently during times of disasters.
Dr. Neil Sharma Minister for Health
4

5
P a g e | 5
MESSAGE FROM MINISTER
The development of the Health Emergency and Disaster Management Plan (HEADMAP) paves way for the health staff to effectively respond to emergencies and disasters. This edition of the HEADMAP is committing the Ministry of Health in efforts to build a resilient culture towards disasters and also adopt new ideas such as climate change and an all-hazard approach in disaster management.
Disaster management is about people and the ability for them to plan, prepare and mitigate factors which are within their control. I am confident that with this revised HEADMAP the Ministry and its staff will be able to response much more effectively and efficiently during times of disasters.
Dr. Neil Sharma Minister for Health
5
6
P a g e | 7
ACKNOWLEDGEMENTS
The Ministry of Health wishes to sincerely thank the technical advice and assistance provided through the partners, organizations and staff in the revision and finalization of this 2nd edition of the Fiji National Health Emergencies and Disaster Management Action Plan.
• Members of the National Health Emergencies and Disaster Management Action Plan Consultation Workshop held in August 2012
• Members of the Review Committee • The Permanent Secretary for Health, Dr. Eloni Tora • The Deputy Secretary for Public Health, Dr. Josefa Koroivueta • The Divisional Medical Officers – Central, Eastern, Western and Northern, Dr. Samuela
Korovou, Dr. Dave Whippy, Dr. Susan Nakalevu and Dr. Pablo Romakin • Chief Health Inspector, Ms. Unaisi Bera • Chief Dietitian, Ms. Anaisi Delai • Acting Manager – National Food and Nutrition Centre, Ms. Ateca Kama • National Advisor Non-Communicable Diseases, Dr. Isimeli Tukana • Acting National Advisor Communicable Disease, Dr. Mike Kama • National Advisor Intensive Care Systems, Dr. Vereniki Rawalui • Director Nursing Services, Sr. Selina Ledua • Chief Pharmacist, Mr. Apolosi Vosanibola • Fiji Health Sector Support Program (FHSSP) Director, Dr. Rosalia Saaga’Bave • Fiji MoH Climate Change Coordinator, Ms. Jyotishma Naicker • World Health Organization (WHO) Acting Environmental Health & Disaster Coordinator, Dr.
Lachlan Mclyer • Fiji Red Cross Society • Strategic Planning Office • Fiji MoH National Health Emergency Coordinator , Mr. Vimal Deo
The Ministry would like to acknowledge the technical assistance rendered by the Fiji Health Sector Support Program (FHSSP) as well as their financial assistance in seeing this edition of HEADMAP to completion. Finally the Ministry also acknowledges all those who have contributed towards this revision of the HEADMAP in any other way.
P a g e | 6
FOREWORD – DEPUTY SECRETARY PUBLIC HEALTH
Cyclones, Floods and Natural Disasters are all too familiar to Fiji and the Pacific. It is estimated that within the last decade there has been an increase in the frequency and severity of natural disasters. Whilst the core business of the Ministry of Health is provision of health care, we must also ensure that our resources, health facilities and staff are in tune with emerging disease control measures, disaster management and climate change adaptation skills. The revision of the Health Emergency and Disaster Management Plan (HEADMAP) is a commitment by the Ministry of Health towards the Disaster Risk Reduction and now requires an integrated comprehensive approach through the wellness concept (prevention), preparedness, response and recovery phases. The Ministry’s Plan takes into consideration the various types of hazards and the action plan provides a means of practical disaster management skills and knowledge. This plan is to be read in conjunction to other Disaster Management plans and Standard Operating Procedures which make the road to disaster management more manageable. The plan requires the whole of government and society support in ensuring that Fiji is ready in times of disasters and that we are prepared at all times. The Ministry of Health is committed to reducing the health impact of disasters and encourages staff, partners, donors, non-governmental organizations to work together in being prepared!
Dr. Josefa Koroivueta Deputy Secretary Public Health
6

7
P a g e | 7
ACKNOWLEDGEMENTS
The Ministry of Health wishes to sincerely thank the technical advice and assistance provided through the partners, organizations and staff in the revision and finalization of this 2nd edition of the Fiji National Health Emergencies and Disaster Management Action Plan.
• Members of the National Health Emergencies and Disaster Management Action Plan Consultation Workshop held in August 2012
• Members of the Review Committee • The Permanent Secretary for Health, Dr. Eloni Tora • The Deputy Secretary for Public Health, Dr. Josefa Koroivueta • The Divisional Medical Officers – Central, Eastern, Western and Northern, Dr. Samuela
Korovou, Dr. Dave Whippy, Dr. Susan Nakalevu and Dr. Pablo Romakin • Chief Health Inspector, Ms. Unaisi Bera • Chief Dietitian, Ms. Anaisi Delai • Acting Manager – National Food and Nutrition Centre, Ms. Ateca Kama • National Advisor Non-Communicable Diseases, Dr. Isimeli Tukana • Acting National Advisor Communicable Disease, Dr. Mike Kama • National Advisor Intensive Care Systems, Dr. Vereniki Rawalui • Director Nursing Services, Sr. Selina Ledua • Chief Pharmacist, Mr. Apolosi Vosanibola • Fiji Health Sector Support Program (FHSSP) Director, Dr. Rosalia Saaga’Bave • Fiji MoH Climate Change Coordinator, Ms. Jyotishma Naicker • World Health Organization (WHO) Acting Environmental Health & Disaster Coordinator, Dr.
Lachlan Mclyer • Fiji Red Cross Society • Strategic Planning Office • Fiji MoH National Health Emergency Coordinator , Mr. Vimal Deo
The Ministry would like to acknowledge the technical assistance rendered by the Fiji Health Sector Support Program (FHSSP) as well as their financial assistance in seeing this edition of HEADMAP to completion. Finally the Ministry also acknowledges all those who have contributed towards this revision of the HEADMAP in any other way.
7

8
P a g e | 8
ACRONYMS
CD Communicable Disease
CHARM Comprehensive Hazard and Risk Management
DD Divisional Dietitian
D-HEADMS Divisional Health Emergency and Disaster Management Structure
DHI Divisional Health Inspector
DHS Divisional Health Sister
DMO Divisional Medical Officer
DSHS Deputy Secretary Hospital Services
DSLO Divisional Service Liaison Officer
DSPH Deputy Secretary Public Health
EMSEC Emergency Services Committee
EOC Emergency Operations Centre
FHSSP Fiji Health Sector Support Program
FINIP Fiji National Influenza Pandemic Plan
FNDRM Fiji National Disaster and Risk Management Plan 2006
FNU Fiji National University
FPS Fiji Pharmaceutical Services
GIS Geographical Information System
HEADMAP Health Emergency and Disaster Management Action Plan
HEADMC Health Emergency and Disaster Management Committee
HERT Health Emergency Response Team
HQ Headquarters (Ministry of Health - Head Office)
MCM Mass Casualty Management
MLO Media Liaison Officer
MoH Ministry of Health
NDMO National Disaster Management Office
NDRMC National Disaster Risk Management Committee
NEC National Health Executive Council
NGO Non-Governmental Organization
P a g e | 9
NHEADRS National Health Emergency and Disaster Response System
NHEC National Health Emergency Coordinator
PH Public Health
PSH Permanent Secretary of Health
RMC Risk Management Committee
SAHI Senior Assistant Health Inspector
SDD Sub-Divisional Dietitian
SDHI Sub-Divisional Health Inspector
SDHS Sub-Divisional Health Sister
SDMO Sub-Divisional Medical Officer
SN Staff Nurse
SOP Standard Operating Procedures
SOPAC Secretariat for the Pacific Islands Applied Geosciences Commission
SPC Secretariat of Pacific Community
UNICEF United Nations Children’s Fund
UNOCHA United Nations Office for the Coordination of Humanitarian Affairs
USP University of the South Pacific
WHO World Health Organization
8

9
P a g e | 8
ACRONYMS
CD Communicable Disease
CHARM Comprehensive Hazard and Risk Management
DD Divisional Dietitian
D-HEADMS Divisional Health Emergency and Disaster Management Structure
DHI Divisional Health Inspector
DHS Divisional Health Sister
DMO Divisional Medical Officer
DSHS Deputy Secretary Hospital Services
DSLO Divisional Service Liaison Officer
DSPH Deputy Secretary Public Health
EMSEC Emergency Services Committee
EOC Emergency Operations Centre
FHSSP Fiji Health Sector Support Program
FINIP Fiji National Influenza Pandemic Plan
FNDRM Fiji National Disaster and Risk Management Plan 2006
FNU Fiji National University
FPS Fiji Pharmaceutical Services
GIS Geographical Information System
HEADMAP Health Emergency and Disaster Management Action Plan
HEADMC Health Emergency and Disaster Management Committee
HERT Health Emergency Response Team
HQ Headquarters (Ministry of Health - Head Office)
MCM Mass Casualty Management
MLO Media Liaison Officer
MoH Ministry of Health
NDMO National Disaster Management Office
NDRMC National Disaster Risk Management Committee
NEC National Health Executive Council
NGO Non-Governmental Organization
P a g e | 9
NHEADRS National Health Emergency and Disaster Response System
NHEC National Health Emergency Coordinator
PH Public Health
PSH Permanent Secretary of Health
RMC Risk Management Committee
SAHI Senior Assistant Health Inspector
SDD Sub-Divisional Dietitian
SDHI Sub-Divisional Health Inspector
SDHS Sub-Divisional Health Sister
SDMO Sub-Divisional Medical Officer
SN Staff Nurse
SOP Standard Operating Procedures
SOPAC Secretariat for the Pacific Islands Applied Geosciences Commission
SPC Secretariat of Pacific Community
UNICEF United Nations Children’s Fund
UNOCHA United Nations Office for the Coordination of Humanitarian Affairs
USP University of the South Pacific
WHO World Health Organization
9


10
P a g e | 10
SECTION A GENERAL – ABOUT THIS PLAN
1.0 Introduction Over the last 10 years, an average of 700 disasters has been reported every year.Annually, an estimated 268 million people are affected by disasters, of whom more than100,000 are killed. In 2010, humanitarian emergencies requiring international assistanceoccurred in 32 countries. The epidemiological profile associated with disasters and conflictsis changing. Although most of the mortality associated with disasters and conflicts continuesto be due to infectious diseases, non-communicable diseases are increasingly among the topfive causes of morbidity and mortality in such settings. Global trends in urbanization areproviding a further impetus for the adaptation of intervention strategies.
[WHO] Fiji is geographically situated in one of the most natural disaster prone areas in the world. Some hazards occur as a consequence of tropical depressions and cyclones or as part of tropical weather condition that normally affects the region.Hazards such as landslides, flash floods, storm surges are most common. There have been 36 recorded natural disasters in Fiji since 1980, with 221 fatalities and over $1 billion dollars worth of economic damage to Fiji’s economy. In 2012, a Tropical Depression (TD17F) caused widespread flooding particularly within the Western Division resulting in 5 casualties and over 200,000 people being directly affected by the disaster.
[MoH Flood Report 2012] The Ministry of Health in 2002 had drafted its National Disaster Management Plan and alignedit to the Fiji National Disaster Management Plan 2005 of the National Disaster Management Council following the review of the National Disaster Management Act (2005). In 2005, the WHO-funded the National Disaster Management Plan was remodelledto become the National Health Emergencies and Disaster Management Plan, commonly referred to as the HEADMAP. Together with this document, the National Influenza Pandemic Plan (FINIP) and the National CD Surveillance and Outbreak Guidelines were drafted. MoH is a member of the Risk Management Committee (RMC), under the Fiji National Disaster Risk Management Council (NDRMC), which is chaired by the National Disaster Management Office (NDMO). Under RMC, the MoH is responsible for the development, implementation and monitoring of all disaster risk reduction initiatives within Government and the wider community. The review of the 2007 – 2011 HEADMAP has seen the addition of standard operating procedures (SOPs) and specific guidelines for various types of hazards faced in Fiji. It must be reiterated that the National Health Emergencies and Disaster Management Plan (HEADMAP) is supported by a number of other plans and documents related to disaster risk reduction and disaster management. At the national level these include Hazard Mitigation, Cyclone Contingency, Other Hazard Contingency, Community Support and Agency Support Plans. The Ministry of Health has prepared the following organisational and operational plan which will allow it to respond effectively and maintain an appropriate level of business continuity during and following disasters.
P a g e | 11
1.1 Objectives The primary objective of the Fiji National Health Emergencies and Disaster Management Plan (HEADMAP) is to serve as a guide for the health sector in the management of public health emergencies and disasters. The specific objectives include:
• Minimise the potential loss of lives and impact of disasters; • Ensure prompt and appropriate disaster responses to affected communities; • Achieve rapid and recovery and rehabilitation following any emergency/disaster. • Ensure provision of adequate resources to support implementation at various levels
1.2 Application and Purpose of the HEADMAP Plan The Fiji National Health Emergencies and Disaster Management Plan (HEADMAP) apply to all health programmes and activities within the National, Divisional and Sub divisional Health Services that are related to Health Emergencies and Disaster Management. These include mitigation, preparedness, emergency responses, relief and rehabilitation. The plan proposes to achieve its listed objectives by:
• outlining the roles and responsibilities of specific bodies with respect to disaster management
• indicate the roles of Ministry of Health Divisions, other agencies and government departments in relation to natural and human generated disasters
• give guidelines for operations and activities in relation to all stages of disaster management • to create a greater understanding of the disaster management arrangements that have
been agreed upon within the Ministry of Health and with other National agencies (such as NDRMC)
1.3 Supporting Plans The HEADMAP plan is derived in response to Fiji’s Disaster Management Act and the need to prepare emergency response guide for disasters and public health emergencies. The chart below outlines links to existing and supporting documents that need to be reads in conjunction with the HEADMAP:
• Fiji National Disaster Management Plan 1995 • Fiji Natural Disaster Management Act 1998 • Fiji National Disaster Risk Management Plan 2006 • Fiji Communicable Diseases Surveillance and Diseases Outbreak Guidelines • Fiji National Influenza Pandemic Plan (FINIP) • Fiji National Dengue Strategic Plan 2010 – 2014 • Fiji Guidelines for Diagnosis and Management of Typhoid Fever 2005 • MoH Standard Operating Procedures (SOP) for MoH Emergency Operation Centre
(2013) • Food Safety Emergency Response Plan 2012
10
11
P a g e | 10
SECTION A GENERAL – ABOUT THIS PLAN
1.0 Introduction Over the last 10 years, an average of 700 disasters has been reported every year.Annually, an estimated 268 million people are affected by disasters, of whom more than100,000 are killed. In 2010, humanitarian emergencies requiring international assistanceoccurred in 32 countries. The epidemiological profile associated with disasters and conflictsis changing. Although most of the mortality associated with disasters and conflicts continuesto be due to infectious diseases, non-communicable diseases are increasingly among the topfive causes of morbidity and mortality in such settings. Global trends in urbanization areproviding a further impetus for the adaptation of intervention strategies.
[WHO] Fiji is geographically situated in one of the most natural disaster prone areas in the world. Some hazards occur as a consequence of tropical depressions and cyclones or as part of tropical weather condition that normally affects the region.Hazards such as landslides, flash floods, storm surges are most common. There have been 36 recorded natural disasters in Fiji since 1980, with 221 fatalities and over $1 billion dollars worth of economic damage to Fiji’s economy. In 2012, a Tropical Depression (TD17F) caused widespread flooding particularly within the Western Division resulting in 5 casualties and over 200,000 people being directly affected by the disaster.
[MoH Flood Report 2012] The Ministry of Health in 2002 had drafted its National Disaster Management Plan and alignedit to the Fiji National Disaster Management Plan 2005 of the National Disaster Management Council following the review of the National Disaster Management Act (2005). In 2005, the WHO-funded the National Disaster Management Plan was remodelledto become the National Health Emergencies and Disaster Management Plan, commonly referred to as the HEADMAP. Together with this document, the National Influenza Pandemic Plan (FINIP) and the National CD Surveillance and Outbreak Guidelines were drafted. MoH is a member of the Risk Management Committee (RMC), under the Fiji National Disaster Risk Management Council (NDRMC), which is chaired by the National Disaster Management Office (NDMO). Under RMC, the MoH is responsible for the development, implementation and monitoring of all disaster risk reduction initiatives within Government and the wider community. The review of the 2007 – 2011 HEADMAP has seen the addition of standard operating procedures (SOPs) and specific guidelines for various types of hazards faced in Fiji. It must be reiterated that the National Health Emergencies and Disaster Management Plan (HEADMAP) is supported by a number of other plans and documents related to disaster risk reduction and disaster management. At the national level these include Hazard Mitigation, Cyclone Contingency, Other Hazard Contingency, Community Support and Agency Support Plans. The Ministry of Health has prepared the following organisational and operational plan which will allow it to respond effectively and maintain an appropriate level of business continuity during and following disasters.
P a g e | 11
1.1 Objectives The primary objective of the Fiji National Health Emergencies and Disaster Management Plan (HEADMAP) is to serve as a guide for the health sector in the management of public health emergencies and disasters. The specific objectives include:
• Minimise the potential loss of lives and impact of disasters; • Ensure prompt and appropriate disaster responses to affected communities; • Achieve rapid and recovery and rehabilitation following any emergency/disaster. • Ensure provision of adequate resources to support implementation at various levels
1.2 Application and Purpose of the HEADMAP Plan The Fiji National Health Emergencies and Disaster Management Plan (HEADMAP) apply to all health programmes and activities within the National, Divisional and Sub divisional Health Services that are related to Health Emergencies and Disaster Management. These include mitigation, preparedness, emergency responses, relief and rehabilitation. The plan proposes to achieve its listed objectives by:
• outlining the roles and responsibilities of specific bodies with respect to disaster management
• indicate the roles of Ministry of Health Divisions, other agencies and government departments in relation to natural and human generated disasters
• give guidelines for operations and activities in relation to all stages of disaster management • to create a greater understanding of the disaster management arrangements that have
been agreed upon within the Ministry of Health and with other National agencies (such as NDRMC)
1.3 Supporting Plans The HEADMAP plan is derived in response to Fiji’s Disaster Management Act and the need to prepare emergency response guide for disasters and public health emergencies. The chart below outlines links to existing and supporting documents that need to be reads in conjunction with the HEADMAP:
• Fiji National Disaster Management Plan 1995 • Fiji Natural Disaster Management Act 1998 • Fiji National Disaster Risk Management Plan 2006 • Fiji Communicable Diseases Surveillance and Diseases Outbreak Guidelines • Fiji National Influenza Pandemic Plan (FINIP) • Fiji National Dengue Strategic Plan 2010 – 2014 • Fiji Guidelines for Diagnosis and Management of Typhoid Fever 2005 • MoH Standard Operating Procedures (SOP) for MoH Emergency Operation Centre
(2013) • Food Safety Emergency Response Plan 2012
11

12
P a g e | 12
1.4 Monitoring and Evaluation Monitoring will be conducted against the action points listed in each phase. Evaluation will consider the plans stated objectives [Section 1.1]. An assessment tool is provided to collect data post-disaster to contribute to the plans evaluation. The Fiji National and Divisional Health Emergencies and Disaster Management Plans must be reviewed and updated in consultation all stakeholders on a periodic basis. It is also recommended that expert independent reviews of these plans be periodically sought.
• Review all the Health Emergencies and Disaster management plans at all levels annually
• Evaluate of the PH emergency response effort according to the following criteria: • Resources • Timeliness • Systems • Data/Reports • Communications • Performance indicators • Recommendations
• Identify and reassess priorities in accordance with the evaluation tools for monitoring the
performance of the plans with the view to identifying flaws and re-assessing priorities whilst also helping to:
• Act as a learning tool for those who took part • Validate decisions made and tactics chosen • Obtaining funding • Post-disaster planning debrief: • Specific clinical, behavioural (word on the street) or PH research can be conducted
in all phases to evaluate the disaster impacts & response
• Submit report of public health crises to the NDMO following each incident.
1.5 Contact List
A Key Contact List is included at the end of this document. This list contains contact information for key people, organizations and agencies which may be involved in an emergency response. The list is designed for ready reference during an emergency and must be kept up to date to be of value.
12


13
P a g e | 12
1.4 Monitoring and Evaluation Monitoring will be conducted against the action points listed in each phase. Evaluation will consider the plans stated objectives [Section 1.1]. An assessment tool is provided to collect data post-disaster to contribute to the plans evaluation. The Fiji National and Divisional Health Emergencies and Disaster Management Plans must be reviewed and updated in consultation all stakeholders on a periodic basis. It is also recommended that expert independent reviews of these plans be periodically sought.
• Review all the Health Emergencies and Disaster management plans at all levels annually
• Evaluate of the PH emergency response effort according to the following criteria: • Resources • Timeliness • Systems • Data/Reports • Communications • Performance indicators • Recommendations
• Identify and reassess priorities in accordance with the evaluation tools for monitoring the
performance of the plans with the view to identifying flaws and re-assessing priorities whilst also helping to:
• Act as a learning tool for those who took part • Validate decisions made and tactics chosen • Obtaining funding • Post-disaster planning debrief: • Specific clinical, behavioural (word on the street) or PH research can be conducted
in all phases to evaluate the disaster impacts & response
• Submit report of public health crises to the NDMO following each incident.
1.5 Contact List
A Key Contact List is included at the end of this document. This list contains contact information for key people, organizations and agencies which may be involved in an emergency response. The list is designed for ready reference during an emergency and must be kept up to date to be of value.
13

14
Tabl
e 1
Show
s the
Pha
ses o
f Disa
ster
Man
agem
ent,
Plan
ning
Issu
es, P
erfo
rman
ce In
dica
tors
and
Res
pons
ibili
ties
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONS
IBIL
ITIE
S
MIT
IGAT
ION
AND
WEL
LNES
S (P
REVE
NTIO
N)
Infra
stru
ctur
e- S
afe
heal
th
facil
ities
(bui
ldin
g, e
quip
men
t, em
erge
ncy
wat
er su
pply
, ge
nera
tor,
ratio
ns, d
ry st
ores
, PP
Es)
Heal
th F
acili
ties w
ell e
quip
ped
and
safe
dur
ing
disa
ster
s Ch
eckl
ist fo
r Mon
itorin
g fo
r Saf
e He
alth
Fac
ilitie
s NH
EC, D
MO,
AM
U, S
DMO,
SD
HI, C
orpo
rate
Ser
vice
s
Wel
lnes
s in
the
com
mun
ity-
com
mun
icatio
ns st
rate
gy (p
ublic
aw
aren
ess)
M
essa
ges D
evel
oped
Allo
cate
d bu
dget
s for
wel
lnes
s of
exis
ting
prog
ram
me,
In
volv
emen
t in
inte
grat
ed
com
mun
ity w
elln
ess
prog
ram
mes
CHI,
NCHP
/Wel
lnes
s Uni
t
Safe
and
Sec
ure
Desig
nate
d Ev
acua
tion
cent
ers
Repo
rt o
n al
l EC
in F
iji (w
ith
reco
mm
enda
tions
)
Cond
uct a
sses
smen
t for
EC
and
mak
e Re
com
men
datio
ns to
ND
MO
CHI,
EH T
eam
, Cor
pora
te
Serv
ices
Colla
bora
tion
with
oth
er
com
mun
ity-b
ased
age
ncie
s Re
gula
r Mee
tings
M
eetin
g w
ith h
ealth
Clu
ster
DS
PH, N
HEC,
Clim
ate
Chan
ge
Offic
er
Clim
ate
chan
ge a
dapt
atio
n Ad
optin
g Cl
imat
e Ch
ange
In
terv
entio
ns in
to D
isast
er
Man
agem
ent P
lans
Links
with
the
Fiji
Join
t Nat
iona
l Ac
tion
Plan
(JNA
P) fo
r Disa
ster
Ri
sk R
educ
tion
and
Clim
ate
Chan
ge A
dapt
atio
n
DSPH
, NHE
C, C
limat
e Ch
ange
Of
ficer
, DM
O, S
DMO,
SDH
I,
Focu
s on
vuln
erab
le p
lace
s and
pe
ople
Stan
dard
Ope
ratin
g Pr
oced
ures
fo
r Vul
nera
ble
Popu
latio
ns in
Pl
ace
Deve
lop
SOP:
Vul
nera
ble
Popu
latio
ns
DSPH
, NHE
C, C
HI
Advo
cacy
of d
isast
er re
leva
nt
stra
tegi
es a
nd p
lans
M
OU/
MOA
with
age
ncie
s M
eetin
g w
ith S
take
hold
ers
PSH,
DSP
H, N
HEC
14

15
Tabl
e 1
Show
s the
Pha
ses o
f Disa
ster
Man
agem
ent,
Plan
ning
Issu
es, P
erfo
rman
ce In
dica
tors
and
Res
pons
ibili
ties
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONS
IBIL
ITIE
S
MIT
IGAT
ION
AND
WEL
LNES
S (P
REVE
NTIO
N)
Infra
stru
ctur
e- S
afe
heal
th
facil
ities
(bui
ldin
g, e
quip
men
t, em
erge
ncy
wat
er su
pply
, ge
nera
tor,
ratio
ns, d
ry st
ores
, PP
Es)
Heal
th F
acili
ties w
ell e
quip
ped
and
safe
dur
ing
disa
ster
s Ch
eckl
ist fo
r Mon
itorin
g fo
r Saf
e He
alth
Fac
ilitie
s NH
EC, D
MO,
AM
U, S
DMO,
SD
HI, C
orpo
rate
Ser
vice
s
Wel
lnes
s in
the
com
mun
ity-
com
mun
icatio
ns st
rate
gy (p
ublic
aw
aren
ess)
M
essa
ges D
evel
oped
Allo
cate
d bu
dget
s for
wel
lnes
s of
exis
ting
prog
ram
me,
In
volv
emen
t in
inte
grat
ed
com
mun
ity w
elln
ess
prog
ram
mes
CHI,
NCHP
/Wel
lnes
s Uni
t
Safe
and
Sec
ure
Desig
nate
d Ev
acua
tion
cent
ers
Repo
rt o
n al
l EC
in F
iji (w
ith
reco
mm
enda
tions
)
Cond
uct a
sses
smen
t for
EC
and
mak
e Re
com
men
datio
ns to
ND
MO
CHI,
EH T
eam
, Cor
pora
te
Serv
ices
Colla
bora
tion
with
oth
er
com
mun
ity-b
ased
age
ncie
s Re
gula
r Mee
tings
M
eetin
g w
ith h
ealth
Clu
ster
DS
PH, N
HEC,
Clim
ate
Chan
ge
Offic
er
Clim
ate
chan
ge a
dapt
atio
n Ad
optin
g Cl
imat
e Ch
ange
In
terv
entio
ns in
to D
isast
er
Man
agem
ent P
lans
Links
with
the
Fiji
Join
t Nat
iona
l Ac
tion
Plan
(JNA
P) fo
r Disa
ster
Ri
sk R
educ
tion
and
Clim
ate
Chan
ge A
dapt
atio
n
DSPH
, NHE
C, C
limat
e Ch
ange
Of
ficer
, DM
O, S
DMO,
SDH
I,
Focu
s on
vuln
erab
le p
lace
s and
pe
ople
Stan
dard
Ope
ratin
g Pr
oced
ures
fo
r Vul
nera
ble
Popu
latio
ns in
Pl
ace
Deve
lop
SOP:
Vul
nera
ble
Popu
latio
ns
DSPH
, NHE
C, C
HI
Advo
cacy
of d
isast
er re
leva
nt
stra
tegi
es a
nd p
lans
M
OU/
MOA
with
age
ncie
s M
eetin
g w
ith S
take
hold
ers
PSH,
DSP
H, N
HEC
15

16
Page
| 16
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONSI
BILI
TIES
PREP
ARED
NESS
Deve
lopm
ent o
f Disa
ster
M
anag
emen
t &Re
spon
se
Stan
dard
Ope
ratin
g Pr
oced
ures
SO
P de
velo
ped
Cons
ulta
tion
with
Hea
lth S
taff,
Fo
rmul
atio
n of
SOP
, Pub
licat
ion
of S
OP
PSH,
DSP
H, N
HEC
Stoc
kpili
ng o
f em
erge
ncy
equi
pmen
t St
ockp
ile/R
esou
rces
ava
ilabl
e De
velo
p an
inve
ntor
y of
stoc
kpile
s for
Disa
ster
s; Pr
ocur
e ne
cess
ary s
tock
s
DSPH
, DSH
S, F
PS, C
HI, E
H Te
am, N
HEC
Deve
lopm
ent o
f IEC
M
ater
ial d
evel
oped
De
sign
and
Pre-
test
Em
erge
ncy/
Disa
ster
Pr
epar
edne
ss M
essa
ges
NHEC
, Wel
lnes
s Tea
m
Trai
ning
of s
taff
and
capa
city
build
ing
Tr
aini
ngs c
ondu
cted
Deve
lop
a Tr
aini
ng P
acka
ge fo
r He
alth
Disa
ster
Man
agem
ent;
Impl
emen
t the
Tra
inin
g w
ithin
Di
visio
ns a
nd su
b-di
visio
ns
Trai
ning
Uni
t, NH
EC
16

17
Page
| 16
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONSI
BILI
TIES
PREP
ARED
NESS
Deve
lopm
ent o
f Disa
ster
M
anag
emen
t &Re
spon
se
Stan
dard
Ope
ratin
g Pr
oced
ures
SO
P de
velo
ped
Cons
ulta
tion
with
Hea
lth S
taff,
Fo
rmul
atio
n of
SOP
, Pub
licat
ion
of S
OP
PSH,
DSP
H, N
HEC
Stoc
kpili
ng o
f em
erge
ncy
equi
pmen
t St
ockp
ile/R
esou
rces
ava
ilabl
e De
velo
p an
inve
ntor
y of
stoc
kpile
s for
Disa
ster
s; Pr
ocur
e ne
cess
ary s
tock
s
DSPH
, DSH
S, F
PS, C
HI, E
H Te
am, N
HEC
Deve
lopm
ent o
f IEC
M
ater
ial d
evel
oped
De
sign
and
Pre-
test
Em
erge
ncy/
Disa
ster
Pr
epar
edne
ss M
essa
ges
NHEC
, Wel
lnes
s Tea
m
Trai
ning
of s
taff
and
capa
city
build
ing
Tr
aini
ngs c
ondu
cted
Deve
lop
a Tr
aini
ng P
acka
ge fo
r He
alth
Disa
ster
Man
agem
ent;
Impl
emen
t the
Tra
inin
g w
ithin
Di
visio
ns a
nd su
b-di
visio
ns
Trai
ning
Uni
t, NH
EC
Page
| 17
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONSI
BILI
TIES
RESP
ONSE
Coor
dina
tion-
To
esta
blish
a
Heal
th E
mer
genc
y Res
pons
e Te
am
HERT
For
med
M
obili
ze a
HER
T in
eac
h su
b-di
visio
n, d
evel
op S
OP fo
r the
te
am
DMO,
SDM
O, D
ivisi
onal
&
Sub-
Divis
iona
l Tea
ms
Defin
e an
d de
term
ine
leve
l of
resp
onse
Ac
tivat
e EO
C as
per
SOP
De
velo
p st
atio
n sp
ecifi
c Disa
ster
M
anag
emen
t Pla
ns
DMO,
SDM
O, D
ivisi
onal
&
Sub-
Divis
iona
l Tea
ms
Mon
itorin
g an
d ev
alua
tion
T
imel
y rep
ortin
g an
d fe
edba
ck
Deve
lop
feed
back
mec
hani
sm,
repo
rtin
g sy
stem
s and
chec
klist
s
NHEC
, DM
O, S
DMO,
Di
visio
nal &
Sub
-Div
ision
al
Team
s Ad
min
istra
tion
- Log
istics
, Tr
ansp
orta
tion,
Hum
an re
sour
ce,
Fina
nces
, Com
mun
icatio
n
Depl
oym
ent P
lan
Desig
ned
Rele
ase
of a
dditi
onal
staf
f to
affe
cted
are
as
PSH,
DSP
H, D
SHS,
DSA
F
Clin
ical S
ervi
ces -
Fac
ilitie
s-
acce
ssib
ility
, Spa
ce- b
eds,
Ambu
lanc
e, P
sych
osoc
ial,
Med
ical a
nd la
bora
tory
supp
lies,
Bloo
d se
rvice
s, M
ortu
ary,
Nu
triti
on
Com
plia
nce
of sa
fe h
ospi
tal
guid
elin
e De
velo
pmen
t of S
afe
Hosp
ital
Guid
elin
e
DSPH
, DSH
S, N
HEC
Com
plia
nce
Emer
genc
y eq
uipm
ent
stan
dard
list
Proc
ure
supp
lies a
nd m
aint
ain
supp
lies i
n or
der
DSHS
, MS,
DM
O, S
DMO
Quar
terly
aud
its o
f co
mpl
ianc
e Co
nduc
ting
of q
uart
erly
m
onito
ring
DS
HS, M
S, D
MO,
SDM
O
SOP
for m
ass b
uria
l De
velo
p in
cons
ulta
tion
the
Mas
s Fat
ality
Man
agem
ent
Guid
elin
es
DSPH
, DSH
S, N
HEC,
MS,
DM
O, O
ther
stak
ehol
ders
(P
olice
, Mili
tary
, NDM
O)
Turn
arou
nd ti
me
(24h
rs)
Tria
ge a
nd e
mer
genc
y m
anag
emen
t sys
tem
in p
lace
M
S, D
MO,
SDM
O, D
ivisi
onal
&
Sub-
Divis
iona
l Tea
ms
Bloo
d ba
nk
Regu
lar c
ondu
ct b
lood
driv
es
Bloo
d Co
ordi
nato
r, DS
HS, M
S,
DMO,
SDM
O
17

18
Pag
e | 1
8 PH
ASES
OF
DISA
STER
M
ANAG
EMEN
T PL
ANNI
NG IS
SUES
PE
RFO
RMAN
CE IN
DICA
TORS
AC
TIVI
TIES
RE
SPO
NSIB
ILIT
IES
RESP
ONS
E
Publ
ic He
alth
- En
viro
nmen
tal
Heal
th, N
utrit
ion,
Was
te
Man
agem
ent,
Pest
Con
trol
, Cl
inica
l Out
reac
h, S
urve
illan
ce,
Infe
ctio
n Co
ntro
l
Repo
rts o
n Si
te In
spec
tions
Co
nduc
t ins
pect
ion
of a
ffect
ed
area
, con
duct
rapi
d as
sess
men
t su
rvey
s
NHEC
, DM
O, S
DMO,
Di
visio
nal &
Sub
-Div
ision
al
Team
s
Supp
ly o
f saf
e w
ater
In
spec
tion
of W
ater
supp
lies;
Prov
ision
of P
urifi
catio
n ta
blet
s CH
I, EH
Tea
m, N
HEC
Redu
ce V
ecto
r Ind
ices
Cond
uct S
ourc
e Re
duct
ion
exer
cise
for m
osqu
ito co
ntro
l CH
I, EH
Tea
m, N
HEC
Prov
ision
of d
ieta
ry su
pple
men
ts
Asse
ssm
ent o
f nut
ritio
nal
requ
irem
ents
, dist
ribut
ion
of
ratio
ns a
nd su
pple
men
ts
SDM
O, S
ub-D
ivisi
onal
Tea
m,
DD a
nd S
DD
Cove
rage
indi
cato
r: no
. cov
ered
/ no
. of e
vacu
atio
n ce
nter
s Da
ily A
sses
smen
ts
SDM
O an
d Su
b-Di
visio
nal
Team
Daily
SitR
ep R
epor
ts
Com
pilin
g of
fiel
d da
ta fo
r re
port
ing
DMO
and
Divi
siona
l Tea
m;
SDM
O an
d Su
b-Di
visio
nal
Team
18

19
Pag
e | 1
8 PH
ASES
OF
DISA
STER
M
ANAG
EMEN
T PL
ANNI
NG IS
SUES
PE
RFO
RMAN
CE IN
DICA
TORS
AC
TIVI
TIES
RE
SPO
NSIB
ILIT
IES
RESP
ONS
E
Publ
ic He
alth
- En
viro
nmen
tal
Heal
th, N
utrit
ion,
Was
te
Man
agem
ent,
Pest
Con
trol
, Cl
inica
l Out
reac
h, S
urve
illan
ce,
Infe
ctio
n Co
ntro
l
Repo
rts o
n Si
te In
spec
tions
Co
nduc
t ins
pect
ion
of a
ffect
ed
area
, con
duct
rapi
d as
sess
men
t su
rvey
s
NHEC
, DM
O, S
DMO,
Di
visio
nal &
Sub
-Div
ision
al
Team
s
Supp
ly o
f saf
e w
ater
In
spec
tion
of W
ater
supp
lies;
Prov
ision
of P
urifi
catio
n ta
blet
s CH
I, EH
Tea
m, N
HEC
Redu
ce V
ecto
r Ind
ices
Cond
uct S
ourc
e Re
duct
ion
exer
cise
for m
osqu
ito co
ntro
l CH
I, EH
Tea
m, N
HEC
Prov
ision
of d
ieta
ry su
pple
men
ts
Asse
ssm
ent o
f nut
ritio
nal
requ
irem
ents
, dist
ribut
ion
of
ratio
ns a
nd su
pple
men
ts
SDM
O, S
ub-D
ivisi
onal
Tea
m,
DD a
nd S
DD
Cove
rage
indi
cato
r: no
. cov
ered
/ no
. of e
vacu
atio
n ce
nter
s Da
ily A
sses
smen
ts
SDM
O an
d Su
b-Di
visio
nal
Team
Daily
SitR
ep R
epor
ts
Com
pilin
g of
fiel
d da
ta fo
r re
port
ing
DMO
and
Divi
siona
l Tea
m;
SDM
O an
d Su
b-Di
visio
nal
Team
Pag
e | 1
9 PH
ASES
OF
DISA
STER
M
ANAG
EMEN
T PL
ANNI
NG IS
SUES
PE
RFO
RMAN
CE IN
DICA
TORS
AC
TIVI
TIES
RE
SPO
NSIB
ILIT
IES
RECO
VERY
Need
s Ass
essm
ent a
nd S
ITRE
PS
Wee
kly
Repo
rts S
ubm
itted
on
prog
ress
Co
mpi
ling
of fi
eld
data
for
repo
rtin
g
DMO
and
Divi
siona
l Tea
m;
SDM
O an
d Su
b-Di
visio
nal
Team
Di
seas
e Su
rvei
llanc
e fo
r No
tifia
ble
& T
ime
Sens
itive
Di
seas
es
Prom
pt R
epor
ting
on C
D's
Utili
zatio
n of
CD
Guid
elin
e fo
r in
vest
igat
ion,
Tra
inin
g of
staf
f an
d re
activ
e re
spon
se st
rate
gies
NACD
, DM
O an
d Di
visio
nal
Team
; SDM
O an
d Su
b-Di
visio
nal T
eam
, He
alth
Ser
vice
s Pro
visio
n,
Seco
ndar
y &
Cur
ativ
e Se
rvice
s, Pr
imar
y He
alth
Car
e Se
rvice
s, Pu
blic
Heal
th In
terv
entio
ns,
Colla
bora
tive
Prog
ram
mes
with
In
tern
atio
nal H
ealth
Par
tner
s, He
alth
Info
rmat
ion
Deliv
ery
Mon
itorin
g an
d Ev
alua
tion
Feed
back
from
Com
mun
ity, V
isits
M
ade,
Rep
orts
Asse
ssm
ent T
empl
ates
, Re
port
ing
Syst
em a
nd
Mon
itorin
g Pr
otoc
ols d
esig
ned
DMO
and
Divi
siona
l Tea
m;
SDM
O an
d Su
b-Di
visio
nal
Team
, NHE
C, M
S, D
SPH,
DSH
S
Reha
bilit
atio
n Of
The
Vict
ims &
Th
e Af
fect
ed P
opul
atio
n
Com
mun
ity B
ased
Wel
lnes
s Ap
proa
ch in
tegr
ated
into
Re
cove
ry
Follo
w U
p Pr
otoc
ols d
esig
ns,
prop
osal
dev
elop
men
ts d
one
Reha
bilit
atio
n of
Eva
cuat
ion
Cent
ers
Subm
issio
n of
Ass
essm
ent R
epor
t to
NDM
O De
velo
pmen
t of A
sses
smen
t Ch
eckl
ist a
nd P
rogr
ess R
epor
ts
M
anag
emen
t Of P
atie
nts
w
ith N
CDs I
n Af
fect
ed A
reas
Re
ferr
al o
f Cas
es a
nd R
epor
ts
Utili
zatio
n of
Exis
ting
Repo
rtin
g Sy
stem
s
Com
mun
ity T
reat
men
t Of
M
inor
Inju
ries
Repo
rts F
iled
Asse
ssm
ent f
orm
s des
igne
d an
d te
sted
Psyc
hoso
cial A
sses
smen
t and
As
sista
nce
Repo
rt S
ubm
itted
, Ass
istan
ce
Rend
ered
Re
port
ing
Tem
plat
e de
signe
d,
awar
enes
s con
duct
ed
19

20
Page
| 20
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONSI
BILI
TIES
RECO
VERY
Reco
nstr
uctio
n an
d Re
habi
litat
ion
of In
frast
ruct
ure,
Ut
ilitie
s Dev
elop
men
t and
Im
prov
emen
t Pro
gram
, Bud
gete
d al
loca
tions
for i
nfra
stru
ctur
es
such
as w
ater
tank
s, ge
nera
tors
an
d fu
el
Asse
ssm
ent R
epor
ts, P
ropo
sals
for R
econ
stru
ctio
n
Fiel
d As
sess
men
t con
duct
ed,
Deve
lopm
ent o
f Che
cklis
ts fo
r Da
mag
e As
sess
men
ts,
Quot
atio
ns a
nd P
ropo
sals
to b
e de
velo
ped
PSH,
DSP
H, D
SHS,
DSA
F,
Corp
orat
e Se
rvice
s, AM
U
Man
agem
ent o
f hea
lth p
erso
nnel
in
disa
ster
are
as, R
einf
orce
men
t of
med
ical p
erso
nnel
dur
ing
prol
onge
d di
sast
ers,
Allo
win
g pe
riods
of R
&R,
Rem
uner
atio
n sc
hedu
les f
or d
isast
er p
erio
ds
and
Psyc
hoso
cial s
uppo
rt fo
r sta
ff
Hum
an R
esou
rce
Plan
s, Pr
opos
al
on R
emun
erat
ion,
Rep
orts
on
staf
f per
form
ance
and
ass
istan
ce
prov
ided
Prop
osal
Dev
elop
men
t on
Staf
f Ro
tatio
n an
d Re
mun
erat
ion
from
Sub
-Div
ision
al le
vel t
o HQ
PSH,
DSP
H, D
SHS,
DSA
F,
Corp
orat
e Se
rvice
s, HR
Post
disa
ster
sym
posiu
m
Cond
uctin
g of
Mee
ting
(Sym
posiu
m) a
nd R
epor
t Or
gani
ze fo
r a P
ost D
isast
er
Mee
ting
and
disc
ussio
ns
PSH,
DSP
H, D
SHS,
DSA
F,
NHEC
20

21
Page
| 20
PHAS
ES O
F DI
SAST
ER
MAN
AGEM
ENT
PLAN
NING
ISSU
ES
PERF
ORM
ANCE
INDI
CATO
RS
ACTI
VITI
ES
RESP
ONSI
BILI
TIES
RECO
VERY
Reco
nstr
uctio
n an
d Re
habi
litat
ion
of In
frast
ruct
ure,
Ut
ilitie
s Dev
elop
men
t and
Im
prov
emen
t Pro
gram
, Bud
gete
d al
loca
tions
for i
nfra
stru
ctur
es
such
as w
ater
tank
s, ge
nera
tors
an
d fu
el
Asse
ssm
ent R
epor
ts, P
ropo
sals
for R
econ
stru
ctio
n
Fiel
d As
sess
men
t con
duct
ed,
Deve
lopm
ent o
f Che
cklis
ts fo
r Da
mag
e As
sess
men
ts,
Quot
atio
ns a
nd P
ropo
sals
to b
e de
velo
ped
PSH,
DSP
H, D
SHS,
DSA
F,
Corp
orat
e Se
rvice
s, AM
U
Man
agem
ent o
f hea
lth p
erso
nnel
in
disa
ster
are
as, R
einf
orce
men
t of
med
ical p
erso
nnel
dur
ing
prol
onge
d di
sast
ers,
Allo
win
g pe
riods
of R
&R,
Rem
uner
atio
n sc
hedu
les f
or d
isast
er p
erio
ds
and
Psyc
hoso
cial s
uppo
rt fo
r sta
ff
Hum
an R
esou
rce
Plan
s, Pr
opos
al
on R
emun
erat
ion,
Rep
orts
on
staf
f per
form
ance
and
ass
istan
ce
prov
ided
Prop
osal
Dev
elop
men
t on
Staf
f Ro
tatio
n an
d Re
mun
erat
ion
from
Sub
-Div
ision
al le
vel t
o HQ
PSH,
DSP
H, D
SHS,
DSA
F,
Corp
orat
e Se
rvice
s, HR
Post
disa
ster
sym
posiu
m
Cond
uctin
g of
Mee
ting
(Sym
posiu
m) a
nd R
epor
t Or
gani
ze fo
r a P
ost D
isast
er
Mee
ting
and
disc
ussio
ns
PSH,
DSP
H, D
SHS,
DSA
F,
NHEC
21

2222

2323

24 P a g e | 25
SECTION C HAZARDS, RISKS AND VULNERABILITIES
3.0 Hazards The ability to manage a disaster response effectively depends in part on the ability of the emergency management system to identify and prepare for a range of predictable hazards. Hazards must be considered in terms of the threat and the threatened community, and mapped accordingly. Hazards must therefore be considered in the context of interactivity. To identify a hazard, the extreme events that could potentially impact on a community must be considered and the vulnerability of the population to the effects of these events can be estimated. The resources required for the community to cope can then be identified. A hazard is a situation or condition with the potential to harm a community or environment, which may be natural, accidental or intentional. Categories of hazards include:
a. Natural Hazards - These include wildfires, storms, floods, cyclones, tsunamis, earthquakes, weather extremes;
b. Technological Hazards - These are caused by the failure of socio-technical systems. These include dam and levee failure and systems failures related to agriculture (e.g. drought), food contamination, industrial sites, infrastructure and transportation;
c. Biological Hazards - These include the spread of disease or pests among plants, animals or people;
d. Civil and Political Hazards - These include terrorism, sabotage, civil unrest, hostage situations and enemy attack; and
e. Organizational Hazards - These include poor organization, workforce disruption, inadequate resources, low levels of training or competence, and/or a lack of awareness of staff responsibilities in an emergency.
The following list of potential hazards (focusing largely on natural hazards) contains the most likely types of foreseeable emergencies or disasters that could affect the delivery of health services within Fiji. For each hazard, the primary damage, area affected and frequency of occurrence is listed.
24

25P a g e | 25
SECTION C HAZARDS, RISKS AND VULNERABILITIES
3.0 Hazards The ability to manage a disaster response effectively depends in part on the ability of the emergency management system to identify and prepare for a range of predictable hazards. Hazards must be considered in terms of the threat and the threatened community, and mapped accordingly. Hazards must therefore be considered in the context of interactivity. To identify a hazard, the extreme events that could potentially impact on a community must be considered and the vulnerability of the population to the effects of these events can be estimated. The resources required for the community to cope can then be identified. A hazard is a situation or condition with the potential to harm a community or environment, which may be natural, accidental or intentional. Categories of hazards include:
a. Natural Hazards - These include wildfires, storms, floods, cyclones, tsunamis, earthquakes, weather extremes;
b. Technological Hazards - These are caused by the failure of socio-technical systems. These include dam and levee failure and systems failures related to agriculture (e.g. drought), food contamination, industrial sites, infrastructure and transportation;
c. Biological Hazards - These include the spread of disease or pests among plants, animals or people;
d. Civil and Political Hazards - These include terrorism, sabotage, civil unrest, hostage situations and enemy attack; and
e. Organizational Hazards - These include poor organization, workforce disruption, inadequate resources, low levels of training or competence, and/or a lack of awareness of staff responsibilities in an emergency.
The following list of potential hazards (focusing largely on natural hazards) contains the most likely types of foreseeable emergencies or disasters that could affect the delivery of health services within Fiji. For each hazard, the primary damage, area affected and frequency of occurrence is listed.
25

26
Page
| 26
TY
PE O
F HAZ
ARDS
AND
THE
IR LI
KELY
IMPA
CTS
Ha
zard
s Pr
imar
y da
mag
es it
can
caus
eAr
eas t
hat c
an b
e af
fect
ed
Freq
uenc
y of t
he
haza
rds
Seco
ndar
y dam
ages
Cy
clone
Co
mpl
etel
y des
troy h
ealth
facil
ities
Affe
cts s
taff
rota
tion
of M
oH
Re
stric
ts m
ovem
ents
of s
taff
and
patie
nts
to a
nd fr
om h
ealth
facil
ities
Disr
upts
hea
lth se
rvice
s del
ivera
nce
De
lay s
urge
ries
Pa
tient
s disc
harg
ed e
arly
Bl
ow a
way
roof
tops
/wal
ls
Blow
aw
ay tr
ee b
ranc
hes
Bl
ow a
way
pow
er lin
es/t
elep
hone
lines
Fly a
way
loos
e de
bris
W
ater
cuts
Dest
roy p
lant
atio
ns
In
jurie
s
Can
kill p
eopl
e
Dest
roy h
ouse
s/ro
ads/
pow
er
lines
/tel
epho
ne lin
es
De
pres
sing
Bl
ocka
ge o
f roa
ds
Di
spla
ce fa
milie
s
Dest
roy v
eget
atio
n an
d kil
l ani
mal
s on-
land
;
Dest
roy m
arin
e lif
e an
d th
eir h
abita
ts;
Da
mag
e w
ater
sour
ces
Di
stur
banc
e of
fam
ilies r
outin
es
Stre
ss
Will
be
advi
sed
by th
e Fi
ji M
eteo
rolo
gica
l Se
rvice
but
the
seas
on is
from
No
vem
ber –
Ap
ril e
very
yea
r in
the
Sout
h Pa
cific
Annu
ally
, mor
e co
mm
on d
urin
g El
Ni
no y
ears
. Clim
ate
proj
ectio
ns sh
ow a
n in
crea
se in
the
occu
rren
ce o
f sev
ere
cyclo
nes (
Abov
e Ca
tego
ry 3
)
Pr
olon
ged
closu
re o
f hea
lth fa
ciliti
es
St
aff r
outin
e af
fect
ed
Re
dire
ctio
n of
fund
s to
suit
prio
ritise
d ne
eds o
f the
MoH
Due
to a
ccom
pany
ing h
eavy
rain
s, ca
n al
so ca
use
flood
, lan
dslid
e an
d st
orm
surg
e
Outb
reak
of d
engu
e du
e to
incr
ease
in m
osqu
ito p
opul
atio
n
Outb
reak
of (
com
mun
icabl
e di
seas
es) e
.g. t
ypho
id, d
iarr
hoea
, le
ptos
pirio
sis, d
ysen
tery
due
to p
ollu
ted
wat
er a
nd a
bsen
ce o
f toi
let
facil
ities
Psyc
holo
gica
lly d
epre
ssed
peo
ple
Se
xual
Rep
rodu
ctive
Hea
lth N
eeds
com
prom
ised
(fam
ily)
W
omen
and
girl
s vul
nera
ble
to Se
xual
Vio
lenc
e
Preg
nant
Mot
hers
at r
isk to
Mat
erna
l mor
bidi
ty a
nd m
orta
lity
Ne
w b
orn
at ri
sk o
f neo
nata
l mor
talit
y and
mor
bidi
ty
Yo
ung
boys
vuln
erab
le to
Sexu
al V
iole
nce
Sh
orta
ge a
nd a
ssoc
iate
d pr
ice ri
se o
f fre
sh fr
uits
and
vege
tabl
e
26

27
Page
| 26
TY
PE O
F HAZ
ARDS
AND
THE
IR LI
KELY
IMPA
CTS
Ha
zard
s Pr
imar
y da
mag
es it
can
caus
eAr
eas t
hat c
an b
e af
fect
ed
Freq
uenc
y of t
he
haza
rds
Seco
ndar
y dam
ages
Cy
clone
Co
mpl
etel
y des
troy h
ealth
facil
ities
Affe
cts s
taff
rota
tion
of M
oH
Re
stric
ts m
ovem
ents
of s
taff
and
patie
nts
to a
nd fr
om h
ealth
facil
ities
Disr
upts
hea
lth se
rvice
s del
ivera
nce
De
lay s
urge
ries
Pa
tient
s disc
harg
ed e
arly
Bl
ow a
way
roof
tops
/wal
ls
Blow
aw
ay tr
ee b
ranc
hes
Bl
ow a
way
pow
er lin
es/t
elep
hone
lines
Fly a
way
loos
e de
bris
W
ater
cuts
Dest
roy p
lant
atio
ns
In
jurie
s
Can
kill p
eopl
e
Dest
roy h
ouse
s/ro
ads/
pow
er
lines
/tel
epho
ne lin
es
De
pres
sing
Bl
ocka
ge o
f roa
ds
Di
spla
ce fa
milie
s
Dest
roy v
eget
atio
n an
d kil
l ani
mal
s on-
land
;
Dest
roy m
arin
e lif
e an
d th
eir h
abita
ts;
Da
mag
e w
ater
sour
ces
Di
stur
banc
e of
fam
ilies r
outin
es
Stre
ss
Will
be
advi
sed
by th
e Fi
ji M
eteo
rolo
gica
l Se
rvice
but
the
seas
on is
from
No
vem
ber –
Ap
ril e
very
yea
r in
the
Sout
h Pa
cific
Annu
ally
, mor
e co
mm
on d
urin
g El
Ni
no y
ears
. Clim
ate
proj
ectio
ns sh
ow a
n in
crea
se in
the
occu
rren
ce o
f sev
ere
cyclo
nes (
Abov
e Ca
tego
ry 3
)
Pr
olon
ged
closu
re o
f hea
lth fa
ciliti
es
St
aff r
outin
e af
fect
ed
Re
dire
ctio
n of
fund
s to
suit
prio
ritise
d ne
eds o
f the
MoH
Due
to a
ccom
pany
ing h
eavy
rain
s, ca
n al
so ca
use
flood
, lan
dslid
e an
d st
orm
surg
e
Outb
reak
of d
engu
e du
e to
incr
ease
in m
osqu
ito p
opul
atio
n
Outb
reak
of (
com
mun
icabl
e di
seas
es) e
.g. t
ypho
id, d
iarr
hoea
, le
ptos
pirio
sis, d
ysen
tery
due
to p
ollu
ted
wat
er a
nd a
bsen
ce o
f toi
let
facil
ities
Psyc
holo
gica
lly d
epre
ssed
peo
ple
Se
xual
Rep
rodu
ctive
Hea
lth N
eeds
com
prom
ised
(fam
ily)
W
omen
and
girl
s vul
nera
ble
to Se
xual
Vio
lenc
e
Preg
nant
Mot
hers
at r
isk to
Mat
erna
l mor
bidi
ty a
nd m
orta
lity
Ne
w b
orn
at ri
sk o
f neo
nata
l mor
talit
y and
mor
bidi
ty
Yo
ung
boys
vuln
erab
le to
Sexu
al V
iole
nce
Sh
orta
ge a
nd a
ssoc
iate
d pr
ice ri
se o
f fre
sh fr
uits
and
vege
tabl
e
Page
| 27
Stor
m su
rge
Se
a w
ater
affe
cts h
ealth
facil
ities
alo
ng
shor
elin
es
Da
mag
es se
a w
all p
rote
ctin
g he
alth
fa
ciliti
es
Re
stric
ts m
ovem
ents
by s
ea
De
lays
hea
lth st
affs
out
reac
h pr
ogra
mm
es
W
ash
away
coas
tline
s
Dest
roy h
ouse
s alo
ng co
astli
nes
Da
mag
e in
frast
ruct
ure
alon
g coa
stlin
es –
ro
ad, b
ridge
s, w
ater
, po
wer
and
te
leph
one
lines
Dist
urbs
mar
ine
ecos
yste
m
De
stro
ys fo
od so
urce
Exte
nds t
he a
reas
of c
omm
uniti
es a
long
se
asho
re in
land
Incr
ease
s int
ensit
y of a
ctivi
ties i
nlan
d
Affe
cts s
hore
line
activ
ities
Coas
tline
Ac
com
pany
cy
clone
s and
st
rong
win
ds
Ad
ded
stre
ss to
pat
ient
s
Stru
ctur
e of
hea
lth fa
ciliti
es d
eter
iora
tes
He
alth
staf
f do
not e
njoy
the
wor
king
envir
onm
ent
Af
fect
s die
t of c
omm
unity
Incr
ease
in ri
sky m
eals
Ps
ycho
logi
cally
dep
ress
ed p
eopl
e
Sexu
al R
epro
duct
ive H
ealth
Nee
ds co
mpr
omise
d (fa
mily
)
Mob
ility t
o th
e ou
ter i
sland
s del
ayed
Heal
th fa
ciliti
es a
t the
out
er is
land
s hav
e to
ope
rate
with
the
min
imal
dru
gs o
r fac
ilitie
s not
affe
cted
Wom
en a
nd g
irls v
ulne
rabl
e to
Sexu
al V
iole
nce
Pr
egna
nt M
othe
rs a
t risk
to M
ater
nal m
orbi
dity
and
mor
talit
y
New
bor
n at
risk
of n
eona
tal m
orta
lity a
nd m
orbi
dity
Stre
ss a
nd cr
eate
s con
ditio
ns co
nduc
ive to
NCD
’s
Youn
g bo
ys vu
lner
able
to Se
xual
Vio
lenc
e
Fl
ood
In
unda
te h
ealth
facil
ities
Dam
age
of st
ruct
ures
Dam
age
of e
quip
men
ts
Fa
ciliti
es cl
ogge
d w
ith m
uddy
wat
er
St
aff a
nd p
atie
nts f
orce
d to
mov
e to
hig
her
loca
tions
Wat
er cu
ts
Ov
erflo
w o
f sep
tic ta
nks
W
ater
seep
age
into
conc
rete
wal
ls
Disr
upts
serv
ices b
y the
hea
lth m
inist
ry
In
unda
te h
ouse
s/sh
ops r
oads
/pla
ntat
ions
/ br
idge
s
Drow
n pe
ople
and
ani
mal
s
Dam
age
hous
es/r
oads
pl
anta
tions
/env
ironm
ent
W
ash
away
brid
ges/
road
s/w
ater
m
ains
/sew
erag
e lin
es
Re
stric
ts m
obilit
y
Stre
ssfu
l
Dist
urba
nce
of fa
milie
s rou
tines
Riv
er p
lain
s L
ow ly
ing
area
s
Annu
ally
, mor
e co
mm
on d
urin
g La
Ni
na y
ears
and
in th
e ho
t and
wet
seas
on
(Nov
embe
r to
April
)
pr
olon
ged
closu
re o
f hea
lth fa
ciliti
es
St
aff r
outin
e af
fect
ed
Re
dire
ctio
n of
fund
s to
suit
prio
ritise
d ne
eds o
f the
MoH
Outb
reak
of d
engu
e du
e to
incr
ease
in m
osqu
ito p
opul
atio
n
Outb
reak
of(c
omm
unica
ble
dise
ases
) typ
hoid
, dia
rrho
ea,
lept
ospi
riosis
, dys
ente
ry, s
cabi
es d
ue to
pol
lute
d w
ater
and
dam
ages
to
toile
t sys
tem
Low
supp
ly of
food
in fo
od sh
ops a
nd ga
rden
s
Psyc
holo
gica
lly d
epre
ssed
peo
ple
Se
xual
Rep
rodu
ctive
Hea
lth N
eeds
com
prom
ised
(fam
ily)
W
omen
and
girl
s vul
nera
ble
to Se
xual
Vio
lenc
e
Preg
nant
Mot
hers
at r
isk to
Mat
erna
l mor
bidi
ty a
nd m
orta
lity
Ne
w b
orn
at ri
sk o
f neo
nata
l mor
talit
y and
mor
bidi
ty
Yo
ung
boys
vuln
erab
le to
Sexu
al V
iole
nce
Sh
orta
ge a
nd a
ssoc
iate
d pr
ice ri
se o
f fre
sh fr
uits
and
vege
tabl
e
27

28
Page
| 28
Drou
ght
Lo
wer
ed w
ater
tabl
es
W
ater
supp
ly to
hea
lth fa
ciliti
es d
isrup
ted
ther
efor
e co
mpr
omise
d pa
tient
care
Wat
er su
pply
to sc
hool
s and
all o
ther
use
rs
disr
upte
d
Clos
ure
of ce
rtain
serv
ices a
t hea
lth
facil
ities
Crop
des
truct
ion
El
ectri
city d
isrup
tion
due
to lo
w d
am le
vels
at M
onas
avu
De
pres
sion,
stre
ss a
mon
g pop
ulat
ion
Part
of t
he co
untr
y or
coun
try
wid
e
Annu
ally
, mor
e pr
onou
nced
dur
ing
El
Nino
yea
rs
Dive
rsio
n of
gov
ernm
ent b
udge
t tow
ards
em
erge
ncy w
ater
su
pply.
Poor
hyg
iene
and
sani
tatio
n
Incr
ease
in co
mm
unica
ble
dise
ases
like
diar
rhoe
a an
d de
ngue
, as
wel
l as s
kin d
iseas
es
Fo
od su
pply
and
secu
rity c
ompr
omise
d, go
vern
men
t bu
dget
ary a
lloca
tions
to e
mer
genc
y foo
d su
pply
M
alnu
tritio
n am
ong c
hild
ren
and
the
poor
Cond
ition
s con
duciv
e to
non
-com
mun
icabl
e di
seas
es
Lo
ss o
f inc
omes
and
livel
ihoo
ds fo
r far
mer
s
Fire
Co
mpl
etel
y des
troy h
ealth
facil
ities
Affe
cts s
taff
rota
tion
of M
oH
Re
stric
ts m
ovem
ents
of s
taff
and
patie
nts
to a
nd fr
om h
ealth
facil
ities
Disr
upts
hea
lth se
rvice
s del
ivera
nce
De
lay s
urge
ries
Pa
tient
s disc
harg
ed e
arly
M
ore
caus
aliti
es tr
ansp
orte
d to
the
heal
th
facil
ities
Heal
th fa
ciliti
es in
chao
tic st
ate
Di
spla
ced
heal
th st
aff a
nd fa
milie
s
Can
kill p
eopl
e
Dest
roy h
ouse
s and
bel
ongi
ngs
De
stro
ys ve
geta
tion
To
tally
des
troy t
erre
stria
l eco
syst
em
All t
ypes
of h
ouse
s an
d be
long
ings
Fr
eque
ntly
In
crea
se in
out
patie
nts
Ri
se in
inpa
tient
Psyc
holo
gica
lly d
epre
ssed
peo
ple
Pe
ople
are
disp
lace
d fro
m th
eir t
errit
orie
s
Incr
ease
in d
isabi
lity
No
hou
ses a
nd to
ilets
for v
ictim
s
No fo
od su
pply
Slo
w d
own
econ
omic
activ
ities
Loss
of e
mpl
oym
ent
Ps
ycho
logi
cally
dep
ress
ed p
eopl
e
No h
ouse
s and
bel
ongi
ng
Re
duce
s pro
perty
valu
es
Af
fect
s far
m fi
nanc
ial o
utpu
t
28
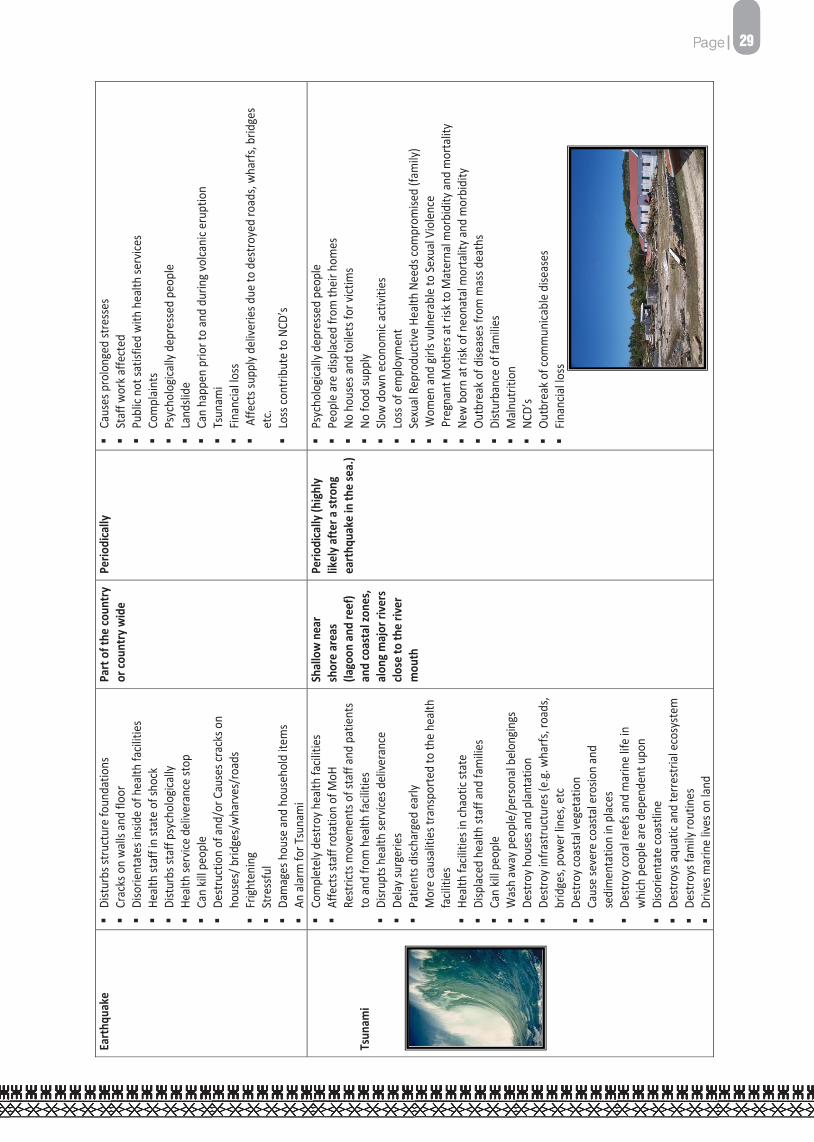
29
Page
| 28
Drou
ght
Lo
wer
ed w
ater
tabl
es
W
ater
supp
ly to
hea
lth fa
ciliti
es d
isrup
ted
ther
efor
e co
mpr
omise
d pa
tient
care
Wat
er su
pply
to sc
hool
s and
all o
ther
use
rs
disr
upte
d
Clos
ure
of ce
rtain
serv
ices a
t hea
lth
facil
ities
Crop
des
truct
ion
El
ectri
city d
isrup
tion
due
to lo
w d
am le
vels
at M
onas
avu
De
pres
sion,
stre
ss a
mon
g pop
ulat
ion
Part
of t
he co
untr
y or
coun
try
wid
e
Annu
ally
, mor
e pr
onou
nced
dur
ing
El
Nino
yea
rs
Dive
rsio
n of
gov
ernm
ent b
udge
t tow
ards
em
erge
ncy w
ater
su
pply.
Poor
hyg
iene
and
sani
tatio
n
Incr
ease
in co
mm
unica
ble
dise
ases
like
diar
rhoe
a an
d de
ngue
, as
wel
l as s
kin d
iseas
es
Fo
od su
pply
and
secu
rity c
ompr
omise
d, go
vern
men
t bu
dget
ary a
lloca
tions
to e
mer
genc
y foo
d su
pply
M
alnu
tritio
n am
ong c
hild
ren
and
the
poor
Cond
ition
s con
duciv
e to
non
-com
mun
icabl
e di
seas
es
Lo
ss o
f inc
omes
and
livel
ihoo
ds fo
r far
mer
s
Fire
Co
mpl
etel
y des
troy h
ealth
facil
ities
Affe
cts s
taff
rota
tion
of M
oH
Re
stric
ts m
ovem
ents
of s
taff
and
patie
nts
to a
nd fr
om h
ealth
facil
ities
Disr
upts
hea
lth se
rvice
s del
ivera
nce
De
lay s
urge
ries
Pa
tient
s disc
harg
ed e
arly
M
ore
caus
aliti
es tr
ansp
orte
d to
the
heal
th
facil
ities
Heal
th fa
ciliti
es in
chao
tic st
ate
Di
spla
ced
heal
th st
aff a
nd fa
milie
s
Can
kill p
eopl
e
Dest
roy h
ouse
s and
bel
ongi
ngs
De
stro
ys ve
geta
tion
To
tally
des
troy t
erre
stria
l eco
syst
em
All t
ypes
of h
ouse
s an
d be
long
ings
Fr
eque
ntly
In
crea
se in
out
patie
nts
Ri
se in
inpa
tient
Psyc
holo
gica
lly d
epre
ssed
peo
ple
Pe
ople
are
disp
lace
d fro
m th
eir t
errit
orie
s
Incr
ease
in d
isabi
lity
No
hou
ses a
nd to
ilets
for v
ictim
s
No fo
od su
pply
Slo
w d
own
econ
omic
activ
ities
Loss
of e
mpl
oym
ent
Ps
ycho
logi
cally
dep
ress
ed p
eopl
e
No h
ouse
s and
bel
ongi
ng
Re
duce
s pro
perty
valu
es
Af
fect
s far
m fi
nanc
ial o
utpu
t
Page
| 29
Ea
rthq
uake
Dist
urbs
stru
ctur
e fo
unda
tions
Cr
acks
on
wal
ls an
d flo
or
Di
sorie
ntat
es in
side
of h
ealth
facil
ities
Heal
th st
aff i
n st
ate
of sh
ock
Di
stur
bs st
aff p
sych
olog
ically
Heal
th se
rvice
del
ivera
nce
stop
Can
kill p
eopl
e
Dest
ruct
ion
of a
nd/o
r Cau
ses c
rack
s on
hous
es/ b
ridge
s/w
harv
es/r
oads
Frig
hten
ing
St
ress
ful
Da
mag
es h
ouse
and
hou
seho
ld it
ems
An
ala
rm fo
r Tsu
nam
i
Part
of t
he co
untr
y or
coun
try w
ide
Perio
dica
lly
Ca
uses
pro
long
ed st
ress
es
Staf
f wor
k affe
cted
Publ
ic no
t sat
isfie
d w
ith h
ealth
serv
ices
Co
mpl
aint
s
Psyc
holo
gical
ly de
pres
sed
peop
le
La
ndsli
de
Ca
n ha
ppen
prio
r to
and
durin
g vol
cani
c eru
ptio
n
Tsun
ami
Fin
ancia
l loss
Affe
cts s
uppl
y del
iverie
s due
to d
estro
yed
road
s, w
harfs
, brid
ges
etc.
Lo
ss co
ntrib
ute
to N
CD’s
Tsun
ami
Co
mpl
etel
y des
troy h
ealth
facil
ities
Af
fect
s sta
ff ro
tatio
n of
MoH
Re
stric
ts m
ovem
ents
of s
taff
and
patie
nts
to a
nd fr
om h
ealth
facil
ities
Disr
upts
hea
lth se
rvice
s del
ivera
nce
De
lay s
urge
ries
Pa
tient
s disc
harg
ed e
arly
Mor
e ca
usal
ities
tran
spor
ted
to th
e he
alth
fa
ciliti
es
He
alth
facil
ities
in ch
aotic
stat
e
Disp
lace
d he
alth
staf
f and
fam
ilies
Ca
n kil
l peo
ple
W
ash
away
peo
ple/
pers
onal
bel
ongin
gs
De
stro
y hou
ses a
nd p
lant
atio
n
Dest
roy i
nfra
stru
ctur
es (e
.g. w
harfs
, roa
ds,
brid
ges,
pow
er lin
es, e
tc
De
stro
y coa
stal
vege
tatio
n
Caus
e se
vere
coas
tal e
rosio
n an
d se
dim
enta
tion
in p
lace
s
Dest
roy c
oral
reef
s and
mar
ine
life
in
whi
ch p
eopl
e ar
e de
pend
ent u
pon
Di
sorie
ntat
e co
astli
ne
De
stro
ys a
quat
ic an
d te
rrest
rial e
cosy
stem
Dest
roys
fam
ily ro
utin
es
Dr
ives m
arin
e liv
es o
n la
nd
Shal
low
nea
r sh
ore
area
s (la
goon
and
reef
) an
d co
asta
l zon
es,
alon
g maj
or ri
vers
clo
se to
the
river
m
outh
Perio
dica
lly (h
ighl
y lik
ely a
fter a
stro
ng
eart
hqua
ke in
the
sea.
)
Ps
ycho
logic
ally
depr
esse
d pe
ople
Pe
ople
are
disp
lace
d fro
m th
eir h
omes
No h
ouse
s and
toile
ts fo
r vict
ims
No
food
supp
ly
Slow
dow
n ec
onom
ic ac
tiviti
es
Lo
ss o
f em
ploy
men
t
Sexu
al R
epro
duct
ive H
ealth
Nee
ds co
mpr
omise
d (fa
mily
)
Wom
en a
nd gi
rls vu
lner
able
to Se
xual
Vio
lenc
e
Preg
nant
Mot
hers
at r
isk to
Mat
erna
l mor
bidi
ty a
nd m
orta
lity
Ne
w b
orn
at ri
sk o
f neo
nata
l mor
talit
y and
mor
bidi
ty
Ou
tbre
ak o
f dise
ases
from
mas
s dea
ths
Di
stur
banc
e of
fam
ilies
M
alnu
tritio
n
NCD’
s
Outb
reak
of c
omm
unica
ble
dise
ases
Finan
cial lo
ss
29

30
3.1 Vulnerabilities Vulnerability describes the relationship between common social and economic characteristics of the population and their ability to cope with hazards. While a disaster will inevitably create challenges, coping ability is still the basic factor in determining the effects of the disaster. The factors that increase vulnerability to extreme events are essentially the same as the determinants of health. Past events and lessons learned from other places may help identify groups at greater risk. The health sector has processes for collecting and assessing this information. It will also be necessary to gather information on the vulnerabilities within specific infrastructures and economies, including looking at the health sector’s own staff, facilities and programs for vulnerabilities. 3.2 Managing Hazards and Vulnerabilities Hazard analysis involves identifying and profiling hazards, assessing vulnerabilities and risk, determining probability scenarios and outcomes, and identifying capabilities and shortfalls. Hazard management involves considering a full range of threats and the implications of their consequences to both the health of the population and the health sector. The Ministry’s focus will be on preparedness, reflecting the concept that successful management of vulnerabilities, resources and the environment will reduce the likelihood of an incident exceeding the disaster threshold. MoH will undertake an ongoing hazard/vulnerability assessment program, in conjunction with health authorities, to maintain appropriate information on vulnerable communities and environments. 3.3 Managing Risk Risk management involves planning and implementing decisions that will minimize the adverse effects of accidental and business losses. Its scope extends to all losses and all entities participating in mitigation, preparedness, response, and recovery. 3.4 Mitigation Mitigation refers to actions intended to eliminate or reduce the risk of future impacts from hazards to vulnerable communities. These actions are prompted by the potential risk of a hazard, rather than an imminent threat. Mitigation may be structural, involving physical measures intended to eliminate or reduce risk, or non-structural, comprising social methods aimed at managing the activities that contribute to the risk. Mitigation measures are particularly important for facilities providing emergency health care, as these facilities will be in high demand following an emergency or disaster. Mitigation is concerned with preventing a harmful interaction between extreme events and a vulnerable community. The decision to mitigate a hazard is reached through the risk management process, and decisions will be influenced by costs, political perspectives, past experiences and other issues that will contribute to risk management.
P a g e | 31
Mitigation will be an established component of the strategic emergency management program within the ministry.The objective is to integrate mitigation activities into all emergency management planning to control costs and reduce hazards. 3.5 Preparedness Emergency preparedness consists of the activities that take place before an incident that increase an organization’s readiness to respond. It consists of activities designed to:
(a) Plan for effective response to and recovery from disasters; (b) Arrange for both internal and external resources to be available when needed; (c) Provide education and training for everyone with a role during a disaster, from first
responders to members of the public, with the education and training needed to respond effectively;
(d) Provide education and public awareness about emergency preparedness; (e) Train, exercise, and evaluate emergency plans; and (f) Revise plans and procedures.
Preparedness reflects the acknowledgement that something can happen, the assignment of a responsibility to respond and a commitment to put the plans, resources and infrastructure in place to ensure the response capability. It is implemented through a continuous cycle of planning, training, equipping, exercising and evaluating. The planning component of preparedness encompasses both emergency response planning and business continuity planning. The two concepts are linked – response planning deals with how the ministry will organize and react to assist affected communities cope with the extraordinary demands of a disaster, The response and recovery aspects of the disaster management are described in the following Section.
30
31
3.1 Vulnerabilities Vulnerability describes the relationship between common social and economic characteristics of the population and their ability to cope with hazards. While a disaster will inevitably create challenges, coping ability is still the basic factor in determining the effects of the disaster. The factors that increase vulnerability to extreme events are essentially the same as the determinants of health. Past events and lessons learned from other places may help identify groups at greater risk. The health sector has processes for collecting and assessing this information. It will also be necessary to gather information on the vulnerabilities within specific infrastructures and economies, including looking at the health sector’s own staff, facilities and programs for vulnerabilities. 3.2 Managing Hazards and Vulnerabilities Hazard analysis involves identifying and profiling hazards, assessing vulnerabilities and risk, determining probability scenarios and outcomes, and identifying capabilities and shortfalls. Hazard management involves considering a full range of threats and the implications of their consequences to both the health of the population and the health sector. The Ministry’s focus will be on preparedness, reflecting the concept that successful management of vulnerabilities, resources and the environment will reduce the likelihood of an incident exceeding the disaster threshold. MoH will undertake an ongoing hazard/vulnerability assessment program, in conjunction with health authorities, to maintain appropriate information on vulnerable communities and environments. 3.3 Managing Risk Risk management involves planning and implementing decisions that will minimize the adverse effects of accidental and business losses. Its scope extends to all losses and all entities participating in mitigation, preparedness, response, and recovery. 3.4 Mitigation Mitigation refers to actions intended to eliminate or reduce the risk of future impacts from hazards to vulnerable communities. These actions are prompted by the potential risk of a hazard, rather than an imminent threat. Mitigation may be structural, involving physical measures intended to eliminate or reduce risk, or non-structural, comprising social methods aimed at managing the activities that contribute to the risk. Mitigation measures are particularly important for facilities providing emergency health care, as these facilities will be in high demand following an emergency or disaster. Mitigation is concerned with preventing a harmful interaction between extreme events and a vulnerable community. The decision to mitigate a hazard is reached through the risk management process, and decisions will be influenced by costs, political perspectives, past experiences and other issues that will contribute to risk management.
P a g e | 31
Mitigation will be an established component of the strategic emergency management program within the ministry.The objective is to integrate mitigation activities into all emergency management planning to control costs and reduce hazards. 3.5 Preparedness Emergency preparedness consists of the activities that take place before an incident that increase an organization’s readiness to respond. It consists of activities designed to:
(a) Plan for effective response to and recovery from disasters; (b) Arrange for both internal and external resources to be available when needed; (c) Provide education and training for everyone with a role during a disaster, from first
responders to members of the public, with the education and training needed to respond effectively;
(d) Provide education and public awareness about emergency preparedness; (e) Train, exercise, and evaluate emergency plans; and (f) Revise plans and procedures.
Preparedness reflects the acknowledgement that something can happen, the assignment of a responsibility to respond and a commitment to put the plans, resources and infrastructure in place to ensure the response capability. It is implemented through a continuous cycle of planning, training, equipping, exercising and evaluating. The planning component of preparedness encompasses both emergency response planning and business continuity planning. The two concepts are linked – response planning deals with how the ministry will organize and react to assist affected communities cope with the extraordinary demands of a disaster, The response and recovery aspects of the disaster management are described in the following Section.
31

32 P a g e | 32
SECTION D OPERATIONAL GUIDELINES - EMERGENCY & DISASTER RESPONSE
Adequate preparedness is necessary to minimise negative health consequences during and after the disaster, and to quickly assess and respond immediately to an emergency. This section represents key operational measures that need to be taken for emergency and disaster response. 4.0 General Country (National), Divisional and Sub-Divisional Profile
• Obtain demographic analysis such as the baseline national, divisional and sub-divisional profile
with identified vulnerable groups and high risk areas • Determine staffing and human resources requirements for disaster response. • Detail and collate status of water supply, power supply, mortuary facilities, transportation,
telecommunication (particularly emergency communications), evacuation centers and health facilities for all locations nationwide (this information may already be available out of the GIS database at the Prime Minister’s Office, or USP or SOPAC)
• Maintain and analyze historical data of previous health related disasters and other relevant statistics
• Ensure other support including community awareness preparedness, NGOs participation and networking and other foreign embassies involvement is done at national & divisional levels
• Establish set criteria for health disaster declarations
4.1 Disaster Preparedness of Technical & Administrative Organisation in Health Sector
• Ensure that Standard Operating Procedures are in place and channels of communications are
identified and stipulated for mandatory compliance at all levels • Ensure that the Chief Pharmacist oversees the procurement, storage, stockpiling and easy
accessibility of medical supplies, consumables, Personal protective Equipment’s, drugs and other emergency related supplies at strategic locations for distribution.
• Ensure the procurement of chemicals, insecticides, chlorine and equipment for emergency water purification.
• Preparation of “requisition clusters” of likely medical supplies, drugs and other resources necessary in case of particular disaster circumstances or outcomes (e.g. water shortage, tainted water supply, mass death etc.)
4.2 Coordination
4.2.1 Intra-sectoral roles • Establish divisional and sub-divisional disaster management committees with linkages to
the National MOH Disaster committee, Divisional and District Disaster Management Committee, the NDMO and National Disaster Management Council
• Delineate, establish and document the roles of each committee within the Divisional plans
P a g e | 33
4.2.2 Inter-sectoral roles
• Identify and understand the roles of Non-Governmental Organisations (NGO’s) and other civil society groups such as Red Cross, St John’s Ambulance Brigade at all levels and establish close working relationships, possibly underwritten by mutual-aid agreements at appropriate levels.
• Understand the roles and capabilities of UN agencies and development partners such as WHO, United Nations Children’s Fund (UNICEF), Secretariat for the Pacific Communities (SPC) and South Pacific Applied Geosciences Commission (SOPAC) at all levels. And establish close working relationships and mutual-aid agreements with these agencies prior to the incidence of any disaster or emergency.
4.3 Technical & Operational Plans • Ensure that disaster contingency plans and other technical health plans (such as those covering
clinical management of specific diseases and protocols, infection control guidelines etc.) are in place for activation whenever appropriate.
• Ensure that Mass Casualty Management (MCM) plans and protocols are drawn up • Detail health requirements of temporary evacuation centres including safe water, sanitation
and hygiene. • Formation of rapid response teams (with details of staff after-hours contacts) within the
divisions and sub divisions 4.4 Routine Operations The day-to-day activities of the ministry are considered to be routine operations. Minor emergencies may occur during routine operations, and will be handled internally within the ministry in conjunction with the Hospital Emergency Systems. Emergencies within the context of routine operations will be handled by the Medical Teams within each sub-divisional hospitals, health facilities or divisional hospitals and will not normally require any special arrangements elsewhere within the ministry. The key focus of emergency management during routine operations will be preparedness, including the regular exercising of emergency procedures, and effective and early response to minor incidents when they occur. 4.5 Emergency Operations The major operational function performed from the national level is to exercise over-all command and coordination so as to provide maximum health service support to the stricken area. When emergency operations are initiated, the PSH for the Ministry of Health will be designated as the National Co-ordinator in command. He/She will take overall command and oversight of all operations from the National Operations centre, which will be at the MOH Headquarters. The National Operations Centre will link up with the NDMO to coordinate activities. At Hospitals and Divisional levels, the Divisional Director is to take control of the emergency operations in conjunction with the Divisional DISMAC.
32

33P a g e | 32
SECTION D OPERATIONAL GUIDELINES - EMERGENCY & DISASTER RESPONSE
Adequate preparedness is necessary to minimise negative health consequences during and after the disaster, and to quickly assess and respond immediately to an emergency. This section represents key operational measures that need to be taken for emergency and disaster response. 4.0 General Country (National), Divisional and Sub-Divisional Profile
• Obtain demographic analysis such as the baseline national, divisional and sub-divisional profile
with identified vulnerable groups and high risk areas • Determine staffing and human resources requirements for disaster response. • Detail and collate status of water supply, power supply, mortuary facilities, transportation,
telecommunication (particularly emergency communications), evacuation centers and health facilities for all locations nationwide (this information may already be available out of the GIS database at the Prime Minister’s Office, or USP or SOPAC)
• Maintain and analyze historical data of previous health related disasters and other relevant statistics
• Ensure other support including community awareness preparedness, NGOs participation and networking and other foreign embassies involvement is done at national & divisional levels
• Establish set criteria for health disaster declarations
4.1 Disaster Preparedness of Technical & Administrative Organisation in Health Sector
• Ensure that Standard Operating Procedures are in place and channels of communications are
identified and stipulated for mandatory compliance at all levels • Ensure that the Chief Pharmacist oversees the procurement, storage, stockpiling and easy
accessibility of medical supplies, consumables, Personal protective Equipment’s, drugs and other emergency related supplies at strategic locations for distribution.
• Ensure the procurement of chemicals, insecticides, chlorine and equipment for emergency water purification.
• Preparation of “requisition clusters” of likely medical supplies, drugs and other resources necessary in case of particular disaster circumstances or outcomes (e.g. water shortage, tainted water supply, mass death etc.)
4.2 Coordination
4.2.1 Intra-sectoral roles • Establish divisional and sub-divisional disaster management committees with linkages to
the National MOH Disaster committee, Divisional and District Disaster Management Committee, the NDMO and National Disaster Management Council
• Delineate, establish and document the roles of each committee within the Divisional plans
P a g e | 33
4.2.2 Inter-sectoral roles
• Identify and understand the roles of Non-Governmental Organisations (NGO’s) and other civil society groups such as Red Cross, St John’s Ambulance Brigade at all levels and establish close working relationships, possibly underwritten by mutual-aid agreements at appropriate levels.
• Understand the roles and capabilities of UN agencies and development partners such as WHO, United Nations Children’s Fund (UNICEF), Secretariat for the Pacific Communities (SPC) and South Pacific Applied Geosciences Commission (SOPAC) at all levels. And establish close working relationships and mutual-aid agreements with these agencies prior to the incidence of any disaster or emergency.
4.3 Technical & Operational Plans • Ensure that disaster contingency plans and other technical health plans (such as those covering
clinical management of specific diseases and protocols, infection control guidelines etc.) are in place for activation whenever appropriate.
• Ensure that Mass Casualty Management (MCM) plans and protocols are drawn up • Detail health requirements of temporary evacuation centres including safe water, sanitation
and hygiene. • Formation of rapid response teams (with details of staff after-hours contacts) within the
divisions and sub divisions 4.4 Routine Operations The day-to-day activities of the ministry are considered to be routine operations. Minor emergencies may occur during routine operations, and will be handled internally within the ministry in conjunction with the Hospital Emergency Systems. Emergencies within the context of routine operations will be handled by the Medical Teams within each sub-divisional hospitals, health facilities or divisional hospitals and will not normally require any special arrangements elsewhere within the ministry. The key focus of emergency management during routine operations will be preparedness, including the regular exercising of emergency procedures, and effective and early response to minor incidents when they occur. 4.5 Emergency Operations The major operational function performed from the national level is to exercise over-all command and coordination so as to provide maximum health service support to the stricken area. When emergency operations are initiated, the PSH for the Ministry of Health will be designated as the National Co-ordinator in command. He/She will take overall command and oversight of all operations from the National Operations centre, which will be at the MOH Headquarters. The National Operations Centre will link up with the NDMO to coordinate activities. At Hospitals and Divisional levels, the Divisional Director is to take control of the emergency operations in conjunction with the Divisional DISMAC.
33
34P a g e | 34
Alternate Operations Centres will be designated if MoH HQ is affected by the disaster. The activities to be conducted within the Emergency Operations centres will be reflected in the Divisional Disaster Management Plans. At Hospitals and Divisional levels, the Divisional Director and the Sub Divisional Medical Officer are in control of the emergency operations respectively. When the alarm is raised, the National and Divisional Operation Centres are activated and assume over-all responsibility for the coordination of disaster management at both levels. When an event or set of circumstances is identified as having the potential to substantively disrupt routine activities, a decision will be made to progress from routine to emergency operations. This decision will be communicated promptly throughout the ministry, normally initiated by the National Health Emergency Unit. Emergency operations have four possible activation levels. In most situations, the levels will be activated sequentially as the emergency or disaster develops. In certain situations, however, levels may be skipped or the highest activation level may be declared at the outset. The notification of alert system shall consist of the following:
• If a health emergency or disaster occurs (or is suspected to have occurred) within an area, the Sub-divisional Medical Officer shall immediately inform the Divisional Director and the MOH Head Office.
• Notify all other agencies through the National Health Emergencies and Disaster Management Committee of the Ministry of Health.
• Notify heads of each department and their subordinates of the Alert and its implications via normal channels
• Notify the Divisions and Subdivisions through the Divisional Directors and SDMOs
P a g e | 35
The following are the emergency activation levels that apply to the ministry. This is an internal emergency management structure and the levels are not directly related to those that may be assigned in other organizations or jurisdictions:
ALERT STATUS
Table 2 Defines the Alert Levels for Health Emergency & Disaster Management
Level Alert Level
MOH EOC Meeting Actions to be taken by MOH EOC members
1 WHITE
White meeting
Meeting is only necessary when coming down from yellow, orange or red level. Otherwise, activities will be: MOH awareness campaigns; MOH planning for evacuation and execution of
simulation exercises.
2 YELLOW
Yellow meeting
Increase MOH staff awareness measures and advisories through the media announcing the immediate need for preparations when
approaching a disaster. Revision and updating of emergency plans and preparations for evacuation. Execution of a simulation exercise if possible. When coming down from Orange or Red levels, analyses the possibility of letting the MOH services go back to almost normal depending
on the situation
3 RED Red meeting
MOH EOC activated. Immediate assessment on all the division and inform the DMO’s (Divisional Medical Officers) and MS’s
(Medical Superintendents). The activation of the Divisional EOC will be under the responsibility of the DMO.
4 GREEN Green meeting MOH EOC activated. Analysis of the situation. Response/recovery
Activities depending on the magnitude and duration of the disaster.
It should also be noted that the MoH Standard Operating Procedure manual on Disaster Management should also be refereed to for specific procedures and operations.
34

35P a g e | 34
Alternate Operations Centres will be designated if MoH HQ is affected by the disaster. The activities to be conducted within the Emergency Operations centres will be reflected in the Divisional Disaster Management Plans. At Hospitals and Divisional levels, the Divisional Director and the Sub Divisional Medical Officer are in control of the emergency operations respectively. When the alarm is raised, the National and Divisional Operation Centres are activated and assume over-all responsibility for the coordination of disaster management at both levels. When an event or set of circumstances is identified as having the potential to substantively disrupt routine activities, a decision will be made to progress from routine to emergency operations. This decision will be communicated promptly throughout the ministry, normally initiated by the National Health Emergency Unit. Emergency operations have four possible activation levels. In most situations, the levels will be activated sequentially as the emergency or disaster develops. In certain situations, however, levels may be skipped or the highest activation level may be declared at the outset. The notification of alert system shall consist of the following:
• If a health emergency or disaster occurs (or is suspected to have occurred) within an area, the Sub-divisional Medical Officer shall immediately inform the Divisional Director and the MOH Head Office.
• Notify all other agencies through the National Health Emergencies and Disaster Management Committee of the Ministry of Health.
• Notify heads of each department and their subordinates of the Alert and its implications via normal channels
• Notify the Divisions and Subdivisions through the Divisional Directors and SDMOs
P a g e | 35
The following are the emergency activation levels that apply to the ministry. This is an internal emergency management structure and the levels are not directly related to those that may be assigned in other organizations or jurisdictions:
ALERT STATUS
Table 2 Defines the Alert Levels for Health Emergency & Disaster Management
Level Alert Level
MOH EOC Meeting Actions to be taken by MOH EOC members
1 WHITE
White meeting
Meeting is only necessary when coming down from yellow, orange or red level. Otherwise, activities will be: MOH awareness campaigns; MOH planning for evacuation and execution of
simulation exercises.
2 YELLOW
Yellow meeting
Increase MOH staff awareness measures and advisories through the media announcing the immediate need for preparations when
approaching a disaster. Revision and updating of emergency plans and preparations for evacuation. Execution of a simulation exercise if possible. When coming down from Orange or Red levels, analyses the possibility of letting the MOH services go back to almost normal depending
on the situation
3 RED Red meeting
MOH EOC activated. Immediate assessment on all the division and inform the DMO’s (Divisional Medical Officers) and MS’s
(Medical Superintendents). The activation of the Divisional EOC will be under the responsibility of the DMO.
4 GREEN Green meeting MOH EOC activated. Analysis of the situation. Response/recovery
Activities depending on the magnitude and duration of the disaster.
It should also be noted that the MoH Standard Operating Procedure manual on Disaster Management should also be refereed to for specific procedures and operations.
35

36 P a g e | 36
4.6 Activation During Level 1 and Level 2 activation, the functions of the ministry are related primarily to maintaining situational awareness, providing advice and coordination to the health authorities and integrating ministry activities with the provincial emergency response structure. At Level 3, particularly if it involves a health emergency such as pandemic influenza or a natural disaster that produces mass casualties, one or more of the regional health authorities and the associated health infrastructure may be overwhelmed. In these circumstances, the role of the ministry must adapt and expand. It is for this reason that a physical EOC is established at Level 3. The ministry must be prepared to exercise a surge response and, in extreme circumstances, to assume a direct command and control function over the health emergency response. 4.7 Integrated Response All actions of the ministry during an emergency will be undertaken within the framework of the integrated response model, involving other Governmental Departments and Ministries. Appropriate health representation will be provided to the District, Divisional and National levels. Although the integrated provincial structure will have the lead in the provincial response to an emergency, a complementary health emergency structure, with health EOCs at each level, will still be required to handle the health-specific aspects of the response and recovery. 4.8 Lines of Communication The diagram shown in Figure 5 (page 23) also describes the communication and chain of command structures. If not managed carefully, this could lead to duplication of effort and misunderstandings; ministry staff must therefore ensure that all essential information is passed along both lines of communication. This is particularly important in the case of decisions and direction to staffs. During an emergency the ministry will maintain liaison and coordination (provided by the NHEC) with outside agencies including other emergency management organizations, and non-governmental organizations and agencies. Internally, the various Sub-Divisions and Divisions will be required to submit an updated situation reports to National MoH EOC at least once daily through the various District Emergency Operations and/or Field Management teams.
P a g e | 37
4.9 Public Affairs (Communication and Media Issues) During major emergencies, demand for information is unrelenting. The media require information to advise the public about the emergency, and media facilities may also be used to distribution of public information. It may be necessary to use the media for the distribution of alerts and warnings under some circumstances. It is essential that all emergency public information activities be coordinated among stakeholders. Every effort must be made to coordinate the release of information with MoH Media Liaison Officer. The National Health Emergency Unit in consultation with relevant stakeholders would also conduct the following:
• Develop a Strategic Communication Plan for National level implementation • Establish a Strategic Communication standing committee, to coordinate the
collection and dissemination of information related to public health emergencies at all levels and informing the general population of the progress and impact on the emergency
• Standardise operating procedures for the formulation of media policies, information exchange, and risk communications
• Identify a Media Liaison Officer’s at various levels • Information management and PR guidelines to be adopted with the designated MLO
at both national and divisional levels • Prepare appropriate IEC materials and messages for the community
4.10 MoH Emergency Operations Centre (EOC) At the onset of an incident, when the switch is made from routine to emergency operations, the DSPH will establish an emergency response committee at the Ministry. This Committee will normally be comprised of HQ Staff, operating on extended hours as necessary. During Level 1 activation, this response committee will be the central point for all matters relating to the response. At Level 2 activation, alert status would be maintained and only the NHEC would handle duties relating to his position (there would be no physical EOC is established).The NHEC would update the DSPH/PSH and Minister on events by email or written reports. At Level 3 activation, a physical EOC will be established. The Ministry EOC will be located in the ministry building at Denim House,Amy Street, Toorak. Headquarters staff would be required to man the EOC on a 24 hour basis.
36

37P a g e | 36
4.6 Activation During Level 1 and Level 2 activation, the functions of the ministry are related primarily to maintaining situational awareness, providing advice and coordination to the health authorities and integrating ministry activities with the provincial emergency response structure. At Level 3, particularly if it involves a health emergency such as pandemic influenza or a natural disaster that produces mass casualties, one or more of the regional health authorities and the associated health infrastructure may be overwhelmed. In these circumstances, the role of the ministry must adapt and expand. It is for this reason that a physical EOC is established at Level 3. The ministry must be prepared to exercise a surge response and, in extreme circumstances, to assume a direct command and control function over the health emergency response. 4.7 Integrated Response All actions of the ministry during an emergency will be undertaken within the framework of the integrated response model, involving other Governmental Departments and Ministries. Appropriate health representation will be provided to the District, Divisional and National levels. Although the integrated provincial structure will have the lead in the provincial response to an emergency, a complementary health emergency structure, with health EOCs at each level, will still be required to handle the health-specific aspects of the response and recovery. 4.8 Lines of Communication The diagram shown in Figure 5 (page 23) also describes the communication and chain of command structures. If not managed carefully, this could lead to duplication of effort and misunderstandings; ministry staff must therefore ensure that all essential information is passed along both lines of communication. This is particularly important in the case of decisions and direction to staffs. During an emergency the ministry will maintain liaison and coordination (provided by the NHEC) with outside agencies including other emergency management organizations, and non-governmental organizations and agencies. Internally, the various Sub-Divisions and Divisions will be required to submit an updated situation reports to National MoH EOC at least once daily through the various District Emergency Operations and/or Field Management teams.
P a g e | 37
4.9 Public Affairs (Communication and Media Issues) During major emergencies, demand for information is unrelenting. The media require information to advise the public about the emergency, and media facilities may also be used to distribution of public information. It may be necessary to use the media for the distribution of alerts and warnings under some circumstances. It is essential that all emergency public information activities be coordinated among stakeholders. Every effort must be made to coordinate the release of information with MoH Media Liaison Officer. The National Health Emergency Unit in consultation with relevant stakeholders would also conduct the following:
• Develop a Strategic Communication Plan for National level implementation • Establish a Strategic Communication standing committee, to coordinate the
collection and dissemination of information related to public health emergencies at all levels and informing the general population of the progress and impact on the emergency
• Standardise operating procedures for the formulation of media policies, information exchange, and risk communications
• Identify a Media Liaison Officer’s at various levels • Information management and PR guidelines to be adopted with the designated MLO
at both national and divisional levels • Prepare appropriate IEC materials and messages for the community
4.10 MoH Emergency Operations Centre (EOC) At the onset of an incident, when the switch is made from routine to emergency operations, the DSPH will establish an emergency response committee at the Ministry. This Committee will normally be comprised of HQ Staff, operating on extended hours as necessary. During Level 1 activation, this response committee will be the central point for all matters relating to the response. At Level 2 activation, alert status would be maintained and only the NHEC would handle duties relating to his position (there would be no physical EOC is established).The NHEC would update the DSPH/PSH and Minister on events by email or written reports. At Level 3 activation, a physical EOC will be established. The Ministry EOC will be located in the ministry building at Denim House,Amy Street, Toorak. Headquarters staff would be required to man the EOC on a 24 hour basis.
37

38P a g e | 38
4.11 Ministry Roles and Tasks The principal roles of the ministry during a major emergency and disasters are:
(a) To resume mission-critical Ministry functions, services, programs and operations within a reasonable time following the onset of the emergency or disaster;
(b) To provide emergency and disaster related direction and advice to the health authorities;
(c) To integrate Ministry resources with those of the integrated response structure as required, including liaison staff at the Emergency Coordination Centre (NDMO)
(d) To facilitate inter-regional cooperation in emergency and disaster related health matters;
Office of the Minister And
Permanent Secretary for Health
The role of the Minister/PSH during an emergency/disaster is to: (a) provide public health measures including epidemic control and immunization programs; (b) provide and coordinate ambulance services and triage, treatment, transportation and care of casualties; (c) provide the continuity of care for persons evacuated from hospitals or other health institutions and for medically dependant persons from other care facilities; (d) provide standard medical units consisting of emergency hospitals, advanced treatment centres and casualty collection units; (e) inspect and monitor potable water supplies; (f) inspect and regulate food quality with the assistance of the Minister of Agriculture and Fisheries; (g) provide critical incident stress debriefing and counselling services; and (h) Provide support and supervision services for physically challenged or medically disabled persons affected by an emergency. The Minister/PSH will provide oversight and direction as required to fulfil this mandate. The ministry will ensure that the minister’s office is kept appraised of the overall emergency situation and that reports of major incidents or events that may be of media interest are transmitted to the minister’s office without delay.
Senior Health Executives
Principal tasks of the Senior Health Executives based at HQ are: (a) provide health-related strategic direction in support of the emergency; (b) frame emergency issues for the Minister/PSH ; (c) provide health-related input (d) review and validate risk/threat assessments and making appropriate recommendations to the Minister/PSH; (e) recommend priorities for the use or allocation of resources in support of the emergency; (f) provide oversight on the application of resources in coordination with other government agencies and other entities; (g) provide broad operational guidance to the HQ EOC; and (h) determine the need for disaster assistance funding
P a g e | 39
National Health Emergency and Disaster
Management Task Force
Health Emergency and Disaster Management Task Force (HEAD MTF) is established to provide prompt, coordinate technical and administrative support to the Divisional Health Emergency and Disaster Management Unit (DHEADMU) and the focal point in supportive agencies such as National Disaster Management Office (NDMO), World Health Organization (WHO) and other United Nations (UN), etc. Taskforce is activated by the Permanent Secretary for Health (PSH) or in his/ her absence the Deputy Secretary for Public Health (DSPH) following the occurrence of a major emergency situation requiring an integrated and inter-programmatic response (Health departmental representation and response). The over-arching responsibilities of the Health Emergency and Disaster Management Task Force • Appoint a Disaster Service Liaison Officer (role done by NHEC) and
Deputy Disaster Service Liaison Officer • Develop and implement MoH Support Plans • Develop and test emergency Standard Operating Procedures • Develop and implement disaster risk reduction initiatives and assist in
public awareness and education in consultation with the NDMO • Apply Comprehensive Hazard & Risk Management (CHARM) principle
/ tool in development planning & budgeting • Appoint and train (in conjunction with NDMO) a MoH Operations
Room Team for National Emergency Operation Centre rostering • Conduct training for MoH training officials in disaster risk managementRoles of the Taskforce are outlined in the annex.
Emergency Operations Centre (EOC)
(All MoH EOC)
The principal tasks of the Ministry EOC’s will be to: a. Maintain situational awareness throughout the emergency; b. Coordinate, in conjunction with the NDMO/Commissioners/
District Office, health aspects of the disaster/emergency response; c. Keep senior ministry officials briefed; d. Monitor and coordinate the health authorities’ activities; e. Provide real time liaison with the NDMO’s Office; f. Coordinate the provision of emergency medical resources which
may be required; g. Provide liaison with key organizations, particularly WHO h. Staff requests for access to national emergency stockpiles and/or
the provision of other support; and i. To provide current information in support of the ministry
communications plan. j. Identify vulnerable groups, i.e. lactating mothers, children under
five (preschool children), the elderly, diabetics etc, and alert emergency teams to their presence
k. Institute preventative and curative measures to check and control occurrence and spread of disease
38
39P a g e | 38
4.11 Ministry Roles and Tasks The principal roles of the ministry during a major emergency and disasters are:
(a) To resume mission-critical Ministry functions, services, programs and operations within a reasonable time following the onset of the emergency or disaster;
(b) To provide emergency and disaster related direction and advice to the health authorities;
(c) To integrate Ministry resources with those of the integrated response structure as required, including liaison staff at the Emergency Coordination Centre (NDMO)
(d) To facilitate inter-regional cooperation in emergency and disaster related health matters;
Office of the Minister And
Permanent Secretary for Health
The role of the Minister/PSH during an emergency/disaster is to: (a) provide public health measures including epidemic control and immunization programs; (b) provide and coordinate ambulance services and triage, treatment, transportation and care of casualties; (c) provide the continuity of care for persons evacuated from hospitals or other health institutions and for medically dependant persons from other care facilities; (d) provide standard medical units consisting of emergency hospitals, advanced treatment centres and casualty collection units; (e) inspect and monitor potable water supplies; (f) inspect and regulate food quality with the assistance of the Minister of Agriculture and Fisheries; (g) provide critical incident stress debriefing and counselling services; and (h) Provide support and supervision services for physically challenged or medically disabled persons affected by an emergency. The Minister/PSH will provide oversight and direction as required to fulfil this mandate. The ministry will ensure that the minister’s office is kept appraised of the overall emergency situation and that reports of major incidents or events that may be of media interest are transmitted to the minister’s office without delay.
Senior Health Executives
Principal tasks of the Senior Health Executives based at HQ are: (a) provide health-related strategic direction in support of the emergency; (b) frame emergency issues for the Minister/PSH ; (c) provide health-related input (d) review and validate risk/threat assessments and making appropriate recommendations to the Minister/PSH; (e) recommend priorities for the use or allocation of resources in support of the emergency; (f) provide oversight on the application of resources in coordination with other government agencies and other entities; (g) provide broad operational guidance to the HQ EOC; and (h) determine the need for disaster assistance funding
P a g e | 39
National Health Emergency and Disaster
Management Task Force
Health Emergency and Disaster Management Task Force (HEAD MTF) is established to provide prompt, coordinate technical and administrative support to the Divisional Health Emergency and Disaster Management Unit (DHEADMU) and the focal point in supportive agencies such as National Disaster Management Office (NDMO), World Health Organization (WHO) and other United Nations (UN), etc. Taskforce is activated by the Permanent Secretary for Health (PSH) or in his/ her absence the Deputy Secretary for Public Health (DSPH) following the occurrence of a major emergency situation requiring an integrated and inter-programmatic response (Health departmental representation and response). The over-arching responsibilities of the Health Emergency and Disaster Management Task Force • Appoint a Disaster Service Liaison Officer (role done by NHEC) and
Deputy Disaster Service Liaison Officer • Develop and implement MoH Support Plans • Develop and test emergency Standard Operating Procedures • Develop and implement disaster risk reduction initiatives and assist in
public awareness and education in consultation with the NDMO • Apply Comprehensive Hazard & Risk Management (CHARM) principle
/ tool in development planning & budgeting • Appoint and train (in conjunction with NDMO) a MoH Operations
Room Team for National Emergency Operation Centre rostering • Conduct training for MoH training officials in disaster risk managementRoles of the Taskforce are outlined in the annex.
Emergency Operations Centre (EOC)
(All MoH EOC)
The principal tasks of the Ministry EOC’s will be to: a. Maintain situational awareness throughout the emergency; b. Coordinate, in conjunction with the NDMO/Commissioners/
District Office, health aspects of the disaster/emergency response; c. Keep senior ministry officials briefed; d. Monitor and coordinate the health authorities’ activities; e. Provide real time liaison with the NDMO’s Office; f. Coordinate the provision of emergency medical resources which
may be required; g. Provide liaison with key organizations, particularly WHO h. Staff requests for access to national emergency stockpiles and/or
the provision of other support; and i. To provide current information in support of the ministry
communications plan. j. Identify vulnerable groups, i.e. lactating mothers, children under
five (preschool children), the elderly, diabetics etc, and alert emergency teams to their presence
k. Institute preventative and curative measures to check and control occurrence and spread of disease
39
40 P a g e | 40
l. Ensure adequate supply of blood is available for transfusion purposes.
m. Provide field hospital and resources at the disaster site if necessaryn. Liaise and coordinate with other health agencies for the non
redundant provision of medical and first-aid assistance in disaster-affected areas.
o. Ensure proper accreditation of health service workers and first aid personnel and stations for information of field personnel and the public.
p. Coordinate arrangements with Transport sub-committee for the use of additional vehicles to augment existing ambulance service where necessary.
q. Verify and procure medical supply, equipment and manpower needs through the relevant departments.
r. Provide full assessment on patient conditions for medical evacuation
s. Monitor sanitary conditions in disaster-affected areas t. Monitor quality of water supplies in disaster-affected areas u. Recommend evacuation as necessary and advise on medical
resources necessary to cover evacuation requirements v. Provide environmental health services at emergency shelters.
Media Liaison Officer
The Ministry public affairs staff is responsible for developing an appropriate communications plan and implementing it in an emergency. They will work closely with the EOC to provide: (a) media liaison to the media; (b) media liaison to the central government communications office; (c) media liaison with regional (health authorities) communications staffs; (d) core content for public communications at the provincial/regional level; (e) advice and support for regional communication initiatives; (f) timely minister’s briefings and media releases emphasizing the nature of the emergency, the scale and scope of casualties and what is being done to mitigate the situation and treat casualties; (g) where emergency medical services are available, how to access them and how to access services which are not available locally; and (h) Advice to the Minister/PSH and ministry executive regarding communications strategies for sensitive or emerging issues.
Human Resources During an emergency it is expected that an appropriate level of day-to-day HR support will be provided to the Ministry.
P a g e | 41
4.12 Health Authorities The health authorities (Divisional and Sub-divisional Offices’) are expected to:
(a) Develop and implement when necessary a comprehensive emergency and disaster management and response plan, in coordination with the Ministry plan;
(b) Integrate the MoH HEADMAP with the divisional and sub-divisional emergency structure;
(c) Cooperate with and provide assistance to other health authorities in the event of an emergency or disaster that requires sharing resources (e.g., evacuation of a facility in an adjacent Health Authority or accommodating casualties from another Health Authority or providing manpower support).
The health authorities need to communicate among themselves at the corporate and senior staff level, and some inter-authority coordination may be done in this way. It is essential, however, that the Ministry of be kept advised/informed of any agreements/decisions between or among or between health authorities during an emergency/disaster. The Ministry will play an important coordination role, ensuring the mobilization of the full array of available health care resources from both the public and private arenas. 4.13 Needs Assessment And Situation Report
The Health authorities should submit a situational assessment report to the Divisional Medical Officer and the MoH EOC as soon as possible in the event of disaster. The following areas to be assessed:
• Health (physical and psychological) • Disease surveillance • Environmental • Socio-economic factors
A Rapid Health Assessment Survey should be completed and submitted to the National Health Emergencies and Disaster Management Committee within seven (7) days of a disaster declaration. The standardized questionnaire should at least include:
• The number and age of residents • description of illnesses and injuries • type of shelter • water supply • food supply(refer to Appendix for Emergency Ration Scale) • medical care
4.14 Ambulance Service The Ambulance Service becomes a first responder in an emergency, and fits into integrated response structure. Personnel throughout the service are trained and services are coordinated with the appropriate level of the EOC. For policy matters and internal communications the project officer at MoH HQ shall take lead in such matters and the SOP for Ambulances should be referred to.
40
41P a g e | 40
l. Ensure adequate supply of blood is available for transfusion purposes.
m. Provide field hospital and resources at the disaster site if necessaryn. Liaise and coordinate with other health agencies for the non
redundant provision of medical and first-aid assistance in disaster-affected areas.
o. Ensure proper accreditation of health service workers and first aid personnel and stations for information of field personnel and the public.
p. Coordinate arrangements with Transport sub-committee for the use of additional vehicles to augment existing ambulance service where necessary.
q. Verify and procure medical supply, equipment and manpower needs through the relevant departments.
r. Provide full assessment on patient conditions for medical evacuation
s. Monitor sanitary conditions in disaster-affected areas t. Monitor quality of water supplies in disaster-affected areas u. Recommend evacuation as necessary and advise on medical
resources necessary to cover evacuation requirements v. Provide environmental health services at emergency shelters.
Media Liaison Officer
The Ministry public affairs staff is responsible for developing an appropriate communications plan and implementing it in an emergency. They will work closely with the EOC to provide: (a) media liaison to the media; (b) media liaison to the central government communications office; (c) media liaison with regional (health authorities) communications staffs; (d) core content for public communications at the provincial/regional level; (e) advice and support for regional communication initiatives; (f) timely minister’s briefings and media releases emphasizing the nature of the emergency, the scale and scope of casualties and what is being done to mitigate the situation and treat casualties; (g) where emergency medical services are available, how to access them and how to access services which are not available locally; and (h) Advice to the Minister/PSH and ministry executive regarding communications strategies for sensitive or emerging issues.
Human Resources During an emergency it is expected that an appropriate level of day-to-day HR support will be provided to the Ministry.
P a g e | 41
4.12 Health Authorities The health authorities (Divisional and Sub-divisional Offices’) are expected to:
(a) Develop and implement when necessary a comprehensive emergency and disaster management and response plan, in coordination with the Ministry plan;
(b) Integrate the MoH HEADMAP with the divisional and sub-divisional emergency structure;
(c) Cooperate with and provide assistance to other health authorities in the event of an emergency or disaster that requires sharing resources (e.g., evacuation of a facility in an adjacent Health Authority or accommodating casualties from another Health Authority or providing manpower support).
The health authorities need to communicate among themselves at the corporate and senior staff level, and some inter-authority coordination may be done in this way. It is essential, however, that the Ministry of be kept advised/informed of any agreements/decisions between or among or between health authorities during an emergency/disaster. The Ministry will play an important coordination role, ensuring the mobilization of the full array of available health care resources from both the public and private arenas. 4.13 Needs Assessment And Situation Report
The Health authorities should submit a situational assessment report to the Divisional Medical Officer and the MoH EOC as soon as possible in the event of disaster. The following areas to be assessed:
• Health (physical and psychological) • Disease surveillance • Environmental • Socio-economic factors
A Rapid Health Assessment Survey should be completed and submitted to the National Health Emergencies and Disaster Management Committee within seven (7) days of a disaster declaration. The standardized questionnaire should at least include:
• The number and age of residents • description of illnesses and injuries • type of shelter • water supply • food supply(refer to Appendix for Emergency Ration Scale) • medical care
4.14 Ambulance Service The Ambulance Service becomes a first responder in an emergency, and fits into integrated response structure. Personnel throughout the service are trained and services are coordinated with the appropriate level of the EOC. For policy matters and internal communications the project officer at MoH HQ shall take lead in such matters and the SOP for Ambulances should be referred to.
41

42
P a g e | 42
4.15 National Health Emergency and Disaster Response System The National Health Emergency and Disaster Response System (NHEADRS) is an all-hazards system involving mitigation, prevention, response and recovery, with a managed interface between the national, divisional and sub-divisional levels. It provides interface between national, divisional and sub-divisional levels at each level of emergency or disaster response management. 4.16 Health Emergency Response Teams Each health facility should have a Health Emergency Response Teams (HERT) which is responsible to providing a health response surge capacity. The teams are made up of local medical support teams and public health support teams. They will assist provinces, sub-divisions and other jurisdictions, in assessments post disaster/emergency, as well in mitigating the medical and health effects of major disasters/emergencies. In the event of a public health emergency, the Sub-Divisional Medical Officer would activate HERTs. HERTs may be structured as follows:
(a) disaster medical response teams
(b) specialized issue-specific teams – infection control, epidemiology teams;
(c) and/or rapid response teams – medical, nursing and other personnel to liaise with provincial/territorial counterparts to assess HERT response and to coordinate HERT resources.
In an emergency, a request may be made for the provision of HERTs with a particular complement of health professionals. This could be for a team that can treat a particular form of trauma, or could be a mixed team to set up a hospital or undertake a range of emergency tasks. An inventory of applicable skills will be maintained at the national level to assist in the coordination of HERT resources. Requests for additional HERT teams should be forwarded to the National Health Emergency & Disaster Unit, from where it will be coordinated with the DSPH and PSH. 4.17 Mass Casualty Management (MCM)
The Ministry shall be responsible in developing a Mass Casualty Management Guideline and this shall be activated by the “on site” Field Management Teams (who will be responsible for Field Organisation, Management of Victims, Transfer Organisation, Hospital Organisation, and updating of Situational Reports). 4.18 Management of the Dead in Disaster Situations
The Ministry shall be responsible in developing a Mass Fatality Management Guideline and implement the appropriate management of the dead in accordance to this Guideline.
P a g e | 43
The NDMO to coordinate with Chief Health Inspectors, the DHIs of the Ministry of Health and other stakeholders whenever necessary for the proper management of the dead in accordance with the Burial and Cremation Act. A coordinated effort with the police will be needed to address disaster death management cases where forensic services are mandated.Furthermore, MoH to coordinate with the Fiji Military Forces to establish additional facilities such as morgues when the need arises. 4.19 Recovery and Reconstruction There are basically two (2) types of recovery:
1. Rehabilitation -Transitional phase (partial) 2. Reconstruction Full restoration
Recovery and Rehabilitation includes physical rehabilitation and material reconstruction,as well as socio-economic and psycho-social interventions. The assumptions involved here are that:
• response committees, processes and procedures have already been set up and have been functioning right from the pre-disaster phase
• there is no clear-cut boundary between the relief and the recovery periods
The post-disaster phase of activities and duties shall include: • enhancing the of surveillance systems • reconstruction and rehabilitation of infrastructures • rehabilitation of affected population • documentation, evaluation, refinement of plan • research
The national, divisional and sub divisional health emergencies disaster management committees will undertake:
• post-disaster assessment • promotion of health education & communication programmes • activities to alleviate psychological effects • re-establishment of health status to pre-disaster state
The respective committees should also have the following in place: • An effective and certified system for surveillance of notifiable and endemic
diseases • A reliable procedure for transporting specimens to laboratories • multi-disciplinary health teams to evaluate the number and type of people
affected • preparation of regular reports
42

43
P a g e | 42
4.15 National Health Emergency and Disaster Response System The National Health Emergency and Disaster Response System (NHEADRS) is an all-hazards system involving mitigation, prevention, response and recovery, with a managed interface between the national, divisional and sub-divisional levels. It provides interface between national, divisional and sub-divisional levels at each level of emergency or disaster response management. 4.16 Health Emergency Response Teams Each health facility should have a Health Emergency Response Teams (HERT) which is responsible to providing a health response surge capacity. The teams are made up of local medical support teams and public health support teams. They will assist provinces, sub-divisions and other jurisdictions, in assessments post disaster/emergency, as well in mitigating the medical and health effects of major disasters/emergencies. In the event of a public health emergency, the Sub-Divisional Medical Officer would activate HERTs. HERTs may be structured as follows:
(a) disaster medical response teams
(b) specialized issue-specific teams – infection control, epidemiology teams;
(c) and/or rapid response teams – medical, nursing and other personnel to liaise with provincial/territorial counterparts to assess HERT response and to coordinate HERT resources.
In an emergency, a request may be made for the provision of HERTs with a particular complement of health professionals. This could be for a team that can treat a particular form of trauma, or could be a mixed team to set up a hospital or undertake a range of emergency tasks. An inventory of applicable skills will be maintained at the national level to assist in the coordination of HERT resources. Requests for additional HERT teams should be forwarded to the National Health Emergency & Disaster Unit, from where it will be coordinated with the DSPH and PSH. 4.17 Mass Casualty Management (MCM)
The Ministry shall be responsible in developing a Mass Casualty Management Guideline and this shall be activated by the “on site” Field Management Teams (who will be responsible for Field Organisation, Management of Victims, Transfer Organisation, Hospital Organisation, and updating of Situational Reports). 4.18 Management of the Dead in Disaster Situations
The Ministry shall be responsible in developing a Mass Fatality Management Guideline and implement the appropriate management of the dead in accordance to this Guideline.
P a g e | 43
The NDMO to coordinate with Chief Health Inspectors, the DHIs of the Ministry of Health and other stakeholders whenever necessary for the proper management of the dead in accordance with the Burial and Cremation Act. A coordinated effort with the police will be needed to address disaster death management cases where forensic services are mandated.Furthermore, MoH to coordinate with the Fiji Military Forces to establish additional facilities such as morgues when the need arises. 4.19 Recovery and Reconstruction There are basically two (2) types of recovery:
1. Rehabilitation -Transitional phase (partial) 2. Reconstruction Full restoration
Recovery and Rehabilitation includes physical rehabilitation and material reconstruction,as well as socio-economic and psycho-social interventions. The assumptions involved here are that:
• response committees, processes and procedures have already been set up and have been functioning right from the pre-disaster phase
• there is no clear-cut boundary between the relief and the recovery periods
The post-disaster phase of activities and duties shall include: • enhancing the of surveillance systems • reconstruction and rehabilitation of infrastructures • rehabilitation of affected population • documentation, evaluation, refinement of plan • research
The national, divisional and sub divisional health emergencies disaster management committees will undertake:
• post-disaster assessment • promotion of health education & communication programmes • activities to alleviate psychological effects • re-establishment of health status to pre-disaster state
The respective committees should also have the following in place: • An effective and certified system for surveillance of notifiable and endemic
diseases • A reliable procedure for transporting specimens to laboratories • multi-disciplinary health teams to evaluate the number and type of people
affected • preparation of regular reports
43
44 P a g e | 44
Within the concept of comprehensive emergency/disaster management, the recovery phase is an essential element of the response. During an emergency it is usually the early response that becomes the focus of attention, and care must be taken to ensure that the long-term impacts of emergencies on individuals and communities are not overlooked or undervalued, particularly in the health sector. The recovery phase can last for long periods of time, and a variety of public health issues may arise after the primary hazard impact has receded. Psychosocial trauma may become more evident with time, and damaged infrastructure, displaced staff and disruptions to external services may hamper a return to normal business. The health sector must therefore expect to be involved with the ongoing consequences of a disaster for longer than many other community agencies. Following a major disaster, recovery will include:
(a) If requested, provision of personnel, facilities and material resources in support of the Recovery and Reconstruction Group;
(b) If requested, provide advice and assistance to local authorities on recovery and reconstruction;
(c) Provide financial administration of recovery and reconstruction operations expenditures;
(d) Choose the best recovery and reconstruction alternatives to restore services and facilities;
(e) Accomplish recovery and reconstruction, to the extent possible, through the existing government organization structure;
(f) Following any catastrophic event, restore normal operating and decision making processes as quickly as possible;
(g) Develop fast track permit review procedures and criteria to facilitate rapid recovery; (h) Plan for the availability of priority equipment and services required for the recovery
and reconstruction process; (i) Develop, implement and maintain mutual aid agreements for recovery and
reconstruction services; (j) Join other government agencies and the private sector to return the government’s
services and facilities to pre-event levels or better; (k) Restore medical facilities as required by the emergency or disaster; and (l) Arrange appropriate government support from NDMO.
P a g e | 45
SECTION E LOGISTICS, FINANCE AND ADMINISTRATION 5.0 General Support services will function normally during emergency and disasters, except that additional administrative and financial resources will be provided to ensure that any special requirements of the emergency response are met, including extended hours for emergency staffs. When the establishment of an EOC is authorized, appropriate resources from program areas within the Ministry will be provided to staff the Logistics and Finance/ Administration sections. The corporate shared services function is responsible for providing infrastructure services to support the operation of the emergency response cell or EOC, providing maintenance of the physical environment of the EOC and providing appropriate support to the emergency operations. 5.1 Logistics By definition, disasters are situations within which resources are overwhelmed. The availability and conditions of physical resources is therefore essential to the response, and must be planned in advance. Financial and resource planning must include methods for obtaining of additional resources needed to respond during an emergency. Resource management will ensure that existing resources are operational and that a practiced system for obtaining additional emergency resources is in place and funded. The direct provision of medical and related support services in an emergency is primarily the responsibility of the health authorities (Divisional and Sub-Divisional Authorities). The Ministry will play an important role in coordinating the emergency resources required by the health authorities and ensuring that allocation, consumption and replenishment of the resources is monitored and controlled efficiently. In the event of a Level 3 activation, the Ministry may be required to assume direct command and control of all emergency-related logistics including resource allocation and delivery, particularly as related to unique or mission-critical pharmaceuticals and medical supplies. The Ministry will conduct liaison with all emergency management staffs to ensure effective control over the provision and delivery of urgent medical supplies throughout the emergency situation. 5.2 National Emergency Services Stockpile& Pharmaceutical Services The Fiji Pharmaceutical Services (FPS) maintains a national emergency stockpile system and is responsible to provide emergency supplies to health facilities when requested. The FPS together with NHEC Unit will develop a stockpile of items which may include items ranging from small backpack trauma kits to complete 200-bed emergency field hospitals. Items are stored and maintained at FPS warehouse located in Suva. The FPS will be required to deliver supplies within 24-48 hours of receiving a request during emergencies.
44


45P a g e | 44
Within the concept of comprehensive emergency/disaster management, the recovery phase is an essential element of the response. During an emergency it is usually the early response that becomes the focus of attention, and care must be taken to ensure that the long-term impacts of emergencies on individuals and communities are not overlooked or undervalued, particularly in the health sector. The recovery phase can last for long periods of time, and a variety of public health issues may arise after the primary hazard impact has receded. Psychosocial trauma may become more evident with time, and damaged infrastructure, displaced staff and disruptions to external services may hamper a return to normal business. The health sector must therefore expect to be involved with the ongoing consequences of a disaster for longer than many other community agencies. Following a major disaster, recovery will include:
(a) If requested, provision of personnel, facilities and material resources in support of the Recovery and Reconstruction Group;
(b) If requested, provide advice and assistance to local authorities on recovery and reconstruction;
(c) Provide financial administration of recovery and reconstruction operations expenditures;
(d) Choose the best recovery and reconstruction alternatives to restore services and facilities;
(e) Accomplish recovery and reconstruction, to the extent possible, through the existing government organization structure;
(f) Following any catastrophic event, restore normal operating and decision making processes as quickly as possible;
(g) Develop fast track permit review procedures and criteria to facilitate rapid recovery; (h) Plan for the availability of priority equipment and services required for the recovery
and reconstruction process; (i) Develop, implement and maintain mutual aid agreements for recovery and
reconstruction services; (j) Join other government agencies and the private sector to return the government’s
services and facilities to pre-event levels or better; (k) Restore medical facilities as required by the emergency or disaster; and (l) Arrange appropriate government support from NDMO.
P a g e | 45
SECTION E LOGISTICS, FINANCE AND ADMINISTRATION 5.0 General Support services will function normally during emergency and disasters, except that additional administrative and financial resources will be provided to ensure that any special requirements of the emergency response are met, including extended hours for emergency staffs. When the establishment of an EOC is authorized, appropriate resources from program areas within the Ministry will be provided to staff the Logistics and Finance/ Administration sections. The corporate shared services function is responsible for providing infrastructure services to support the operation of the emergency response cell or EOC, providing maintenance of the physical environment of the EOC and providing appropriate support to the emergency operations. 5.1 Logistics By definition, disasters are situations within which resources are overwhelmed. The availability and conditions of physical resources is therefore essential to the response, and must be planned in advance. Financial and resource planning must include methods for obtaining of additional resources needed to respond during an emergency. Resource management will ensure that existing resources are operational and that a practiced system for obtaining additional emergency resources is in place and funded. The direct provision of medical and related support services in an emergency is primarily the responsibility of the health authorities (Divisional and Sub-Divisional Authorities). The Ministry will play an important role in coordinating the emergency resources required by the health authorities and ensuring that allocation, consumption and replenishment of the resources is monitored and controlled efficiently. In the event of a Level 3 activation, the Ministry may be required to assume direct command and control of all emergency-related logistics including resource allocation and delivery, particularly as related to unique or mission-critical pharmaceuticals and medical supplies. The Ministry will conduct liaison with all emergency management staffs to ensure effective control over the provision and delivery of urgent medical supplies throughout the emergency situation. 5.2 National Emergency Services Stockpile& Pharmaceutical Services The Fiji Pharmaceutical Services (FPS) maintains a national emergency stockpile system and is responsible to provide emergency supplies to health facilities when requested. The FPS together with NHEC Unit will develop a stockpile of items which may include items ranging from small backpack trauma kits to complete 200-bed emergency field hospitals. Items are stored and maintained at FPS warehouse located in Suva. The FPS will be required to deliver supplies within 24-48 hours of receiving a request during emergencies.
45
46 P a g e | 46
5.3 Finance Financial management and control during an emergency will be governed by the provisions of the Financial Regulations of the Public Service. During emergency/disasters, health authorities may be eligible for financial assistance to offset incremental and extraordinary costs. Details regarding available emergency financial assistance, expenditure controls and other information will be available under the Public Health Program for Public Health matters and with Hospital Services for clinical measures. When the MoH HQ EOC is established, the Finance/Administrationsection of the Ministry shall be responsible for all financial aspects of managing an emergency event. This includes making and/or collecting payments relating to the provision of human resources and all other supplies and services, monitoring emergency-related costs and administering any necessary procurement contracts.
5.4 Administration
Effective administration is an essential component of sound emergency/disaster management – responders and EOC staffs must be provided with timely administrative support in order to focus on managing the response.
Day-to-day events and activities must be recorded from the outset of an emergency situation, using an appropriate log or diary system. Operational forms and other documentation should be prepared in advance and stored with other EOC material, and staffs must be practiced in their use. A comprehensive record of all activities related to an emergency is an essential component of emergency management. To this end, care must be taken to prepare, maintain and safeguard accurate records of all activities and events throughout each phase of the emergency. It is particularly important that a thorough record be kept of all major decisions taken. 5.5 Emergency Communications
The Ministry HQ does not maintain any special emergency communications equipment except for radio telephones andone satellite telephone. Normal landline and cellular (mobile) telephones, facsimile and email facilities will be utilized. Should the circumstances of the emergency reduce or limit communications, the NHEC Unit would have priority and restrictions may be imposed on the non-emergency use of ministry communications equipment and facilities. If demanded by operational circumstances, essential communications can be routed through other Government Departments and Ministries.
P a g e | 47
SECTION F TRAINING AND EXERCISES 6.0 General Training is a key to minimizing the impact of disasters and to ensure an effective response system. The Ministry will ensure that appropriate emergency management training takes place at two levels – individual and collective. Individual training involves personal study and participation in workshops, seminars and courses. Collective training involves emergency exercises and other activities which provide individuals and teams with learning opportunities as well as testing and evaluating emergency plans. Training may be provided by any of the following methods:
(a) In-house – specific to an organization’s plans, equipment and responsibilities; (b) Interagency – joint training with other organizations, often coordinated and
conducted by Government Departments (e.g. NDMO or PSC) and (c) Academic – utilizing the existing network of academic institutions in both the public
and private sectors. Evidence-based information will form the basis for providing emergency management training within the health sector. 6.1 Training Process Effective training must be part of a comprehensive process which includes effective evaluation and validation. In this context:
(a) Evaluation refers to the means to examine and judge effectiveness through a defined methodology. The aim of evaluation is to determine to what extent learners were satisfied, whether new knowledge and skills were obtained and whether training objectives were met. Effective evaluation focuses on the outcomes or results achieved during and after training, and not simply the achievement of stated objectives. It utilizes various monitoring and feedback mechanisms applied to training.
(b) Validation is a confirmation process designed to ensure that the products of training
meet the operational training requirement. It measures the readiness of the organization and is the composite result of:
i Implementing and testing; ii Evaluation; and
iii Recommendations and corrective actions. Validation of emergency management training is the final step in the process and is essential to determine if the training is effective in supporting and enhancing emergency preparedness and planning efforts.
46
47P a g e | 46
5.3 Finance Financial management and control during an emergency will be governed by the provisions of the Financial Regulations of the Public Service. During emergency/disasters, health authorities may be eligible for financial assistance to offset incremental and extraordinary costs. Details regarding available emergency financial assistance, expenditure controls and other information will be available under the Public Health Program for Public Health matters and with Hospital Services for clinical measures. When the MoH HQ EOC is established, the Finance/Administrationsection of the Ministry shall be responsible for all financial aspects of managing an emergency event. This includes making and/or collecting payments relating to the provision of human resources and all other supplies and services, monitoring emergency-related costs and administering any necessary procurement contracts.
5.4 Administration
Effective administration is an essential component of sound emergency/disaster management – responders and EOC staffs must be provided with timely administrative support in order to focus on managing the response.
Day-to-day events and activities must be recorded from the outset of an emergency situation, using an appropriate log or diary system. Operational forms and other documentation should be prepared in advance and stored with other EOC material, and staffs must be practiced in their use. A comprehensive record of all activities related to an emergency is an essential component of emergency management. To this end, care must be taken to prepare, maintain and safeguard accurate records of all activities and events throughout each phase of the emergency. It is particularly important that a thorough record be kept of all major decisions taken. 5.5 Emergency Communications
The Ministry HQ does not maintain any special emergency communications equipment except for radio telephones andone satellite telephone. Normal landline and cellular (mobile) telephones, facsimile and email facilities will be utilized. Should the circumstances of the emergency reduce or limit communications, the NHEC Unit would have priority and restrictions may be imposed on the non-emergency use of ministry communications equipment and facilities. If demanded by operational circumstances, essential communications can be routed through other Government Departments and Ministries.
P a g e | 47
SECTION F TRAINING AND EXERCISES 6.0 General Training is a key to minimizing the impact of disasters and to ensure an effective response system. The Ministry will ensure that appropriate emergency management training takes place at two levels – individual and collective. Individual training involves personal study and participation in workshops, seminars and courses. Collective training involves emergency exercises and other activities which provide individuals and teams with learning opportunities as well as testing and evaluating emergency plans. Training may be provided by any of the following methods:
(a) In-house – specific to an organization’s plans, equipment and responsibilities; (b) Interagency – joint training with other organizations, often coordinated and
conducted by Government Departments (e.g. NDMO or PSC) and (c) Academic – utilizing the existing network of academic institutions in both the public
and private sectors. Evidence-based information will form the basis for providing emergency management training within the health sector. 6.1 Training Process Effective training must be part of a comprehensive process which includes effective evaluation and validation. In this context:
(a) Evaluation refers to the means to examine and judge effectiveness through a defined methodology. The aim of evaluation is to determine to what extent learners were satisfied, whether new knowledge and skills were obtained and whether training objectives were met. Effective evaluation focuses on the outcomes or results achieved during and after training, and not simply the achievement of stated objectives. It utilizes various monitoring and feedback mechanisms applied to training.
(b) Validation is a confirmation process designed to ensure that the products of training
meet the operational training requirement. It measures the readiness of the organization and is the composite result of:
i Implementing and testing; ii Evaluation; and
iii Recommendations and corrective actions. Validation of emergency management training is the final step in the process and is essential to determine if the training is effective in supporting and enhancing emergency preparedness and planning efforts.
47
48
P a g e | 48
Appropriate arrangements for evaluation and validation will be made for all training conducted or sponsored by the ministry or within the provincial health sector. 6.3 Individual Training For Ministry health staffs, individual training will be based upon invitation and sponsorship arrangements with regional partners. Participants will be selected through the MoH Training Committee and may also be based on recommendation from the Minister or PSH. 6.4 Collective Training The Ministry will, as a general rule, conduct or sponsor at least one emergency exercise annually, in conjunction with health authorities. In principle, these exercises should become progressively more complex, however the realities of staff turnover, cost and time may limit them to the orientation or tabletop levels. Functional exercises will be held when cost and other factors permit. When practicable, staff will participate in collective training activities organized or sponsored by other jurisdictions. 6.5 Conduct of Exercises Exercises are an important component of response preparedness and are an essential part of the evaluation and validation processes. When properly designed they bring skills, knowledge, functions and systems together and apply them against realistic event scenarios. A well-designed exercise will test specific aspects of a plan, identify deficiencies and ensure operational functionality. At both the individual and collective levels it will help deliver practical skills, build confidence, and strengthen the network between individuals and agencies. If properly managed, it will also raise interest in emergency preparedness within organizations and the public. There are five general types of exercises, although different organizations may name and divide them differently. Identifying which type of exercise is needed and whether its purpose is for training or evaluation are important decisions in the exercise design process. Exercises have limitations, that is, they may not, for example, predict actual performance in that real emergencies rarely follow predicted patterns. It is also difficult, in an exercise, to effectively test how an organization’s response procedures are initiated, as planned or pre-announced exercises allow too much forewarning to be realistic and no-notice exercises are difficult to simulate properly. The timing and frequency of exercises requires careful consideration. All systems and procedures need to be regularly reviewed, inspected or otherwise tested. However, how this happens often depends on the stability of staff is and whether procedures change over time. The following table describes the various forms of Exercises that may be undertaken.
48

49
P a g e | 48
Appropriate arrangements for evaluation and validation will be made for all training conducted or sponsored by the ministry or within the provincial health sector. 6.3 Individual Training For Ministry health staffs, individual training will be based upon invitation and sponsorship arrangements with regional partners. Participants will be selected through the MoH Training Committee and may also be based on recommendation from the Minister or PSH. 6.4 Collective Training The Ministry will, as a general rule, conduct or sponsor at least one emergency exercise annually, in conjunction with health authorities. In principle, these exercises should become progressively more complex, however the realities of staff turnover, cost and time may limit them to the orientation or tabletop levels. Functional exercises will be held when cost and other factors permit. When practicable, staff will participate in collective training activities organized or sponsored by other jurisdictions. 6.5 Conduct of Exercises Exercises are an important component of response preparedness and are an essential part of the evaluation and validation processes. When properly designed they bring skills, knowledge, functions and systems together and apply them against realistic event scenarios. A well-designed exercise will test specific aspects of a plan, identify deficiencies and ensure operational functionality. At both the individual and collective levels it will help deliver practical skills, build confidence, and strengthen the network between individuals and agencies. If properly managed, it will also raise interest in emergency preparedness within organizations and the public. There are five general types of exercises, although different organizations may name and divide them differently. Identifying which type of exercise is needed and whether its purpose is for training or evaluation are important decisions in the exercise design process. Exercises have limitations, that is, they may not, for example, predict actual performance in that real emergencies rarely follow predicted patterns. It is also difficult, in an exercise, to effectively test how an organization’s response procedures are initiated, as planned or pre-announced exercises allow too much forewarning to be realistic and no-notice exercises are difficult to simulate properly. The timing and frequency of exercises requires careful consideration. All systems and procedures need to be regularly reviewed, inspected or otherwise tested. However, how this happens often depends on the stability of staff is and whether procedures change over time. The following table describes the various forms of Exercises that may be undertaken.
Pag
e | 4
9
Tabl
e 3
Show
s the
Var
ious
Typ
es o
f Tra
inin
g Ex
erci
ses
No
Type
De
scrip
tion
1 O
rient
atio
n
As t
he n
ame
sugg
ests
, th
e or
ient
atio
n ex
erci
se i
s co
nduc
ted
at a
n in
trod
ucto
ry l
evel
. Its
pur
pose
is
to
fam
iliar
ize p
artic
ipan
ts w
ith ro
les,
pla
ns, p
roce
dure
s or
equ
ipm
ent.
It ca
n al
so b
e us
ed to
reso
lve
ques
tions
of
coor
dina
tion
and
assig
nmen
t of
res
pons
ibili
ties.
The
orie
ntat
ion
sem
inar
is
a lo
w-s
tres
s ev
ent,
usua
lly
pres
ente
d as
an
info
rmal
disc
ussio
n in
a g
roup
set
ting.
The
re is
litt
le o
r no
sim
ulat
ion.
A v
arie
ty o
f se
min
ar
form
ats c
an b
e us
ed, i
nclu
ding
: a)
Le
ctur
e;
b) D
iscus
sion;
c)
Sl
ide
or v
ideo
pre
sent
atio
n;
d) C
ompu
ter d
emon
stra
tion;
e)
Pa
nel d
iscus
sion;
and
/or
f) Gu
est l
ectu
rers
Th
e or
ient
atio
n ex
erci
se c
an b
e us
ed fo
r a w
ide
varie
ty o
f pur
pose
s, in
clud
ing:
a)
Di
scus
sing
a to
pic
or p
robl
em in
a g
roup
sett
ing;
b)
Int
rodu
cing
som
ethi
ng n
ew (e
.g.,
polic
ies a
nd p
lans
); c)
Ex
plai
ning
exi
stin
g pl
ans t
o ne
w st
aff;
d) I
ntro
duci
ng a
cyc
le o
f exe
rcise
s or p
repa
ring
part
icip
ants
for s
ucce
ss in
mor
e co
mpl
ex e
xerc
ises;
and
/or
e)
Mot
ivat
ing
peop
le fo
r par
ticip
atio
n in
subs
eque
nt e
xerc
ises.
2 Dr
ill
A dr
ill i
s a
coor
dina
ted,
sup
ervi
sed
exer
cise
act
ivity
nor
mal
ly u
sed
to t
est
a sin
gle
spec
ific
oper
atio
n or
fu
nctio
n. W
ith a
dril
l, th
ere
is no
att
empt
to
coor
dina
te o
rgan
izatio
ns o
r fu
lly a
ctiv
ate
an E
OC.
Its
role
is t
o pr
actic
e an
d pe
rfec
t on
e cl
early
def
ined
par
t of
a r
espo
nse
plan
and
to
help
pre
pare
for
mor
e ex
tens
ive
exer
cise
s. T
he e
ffect
iven
ess
of a
dril
l is
its fo
cus
on a
sin
gle,
rela
tivel
y lim
ited
port
ion
of th
e ov
eral
l em
erge
ncy
man
agem
ent s
yste
m.
Drill
s m
ay a
lso b
e us
ed t
o pr
ovid
e tr
aini
ng o
n ne
w e
quip
men
t, to
dev
elop
new
pol
icie
s or
pro
cedu
res,
or
to
prac
tice
and
mai
ntai
n cu
rren
t ski
lls.
49
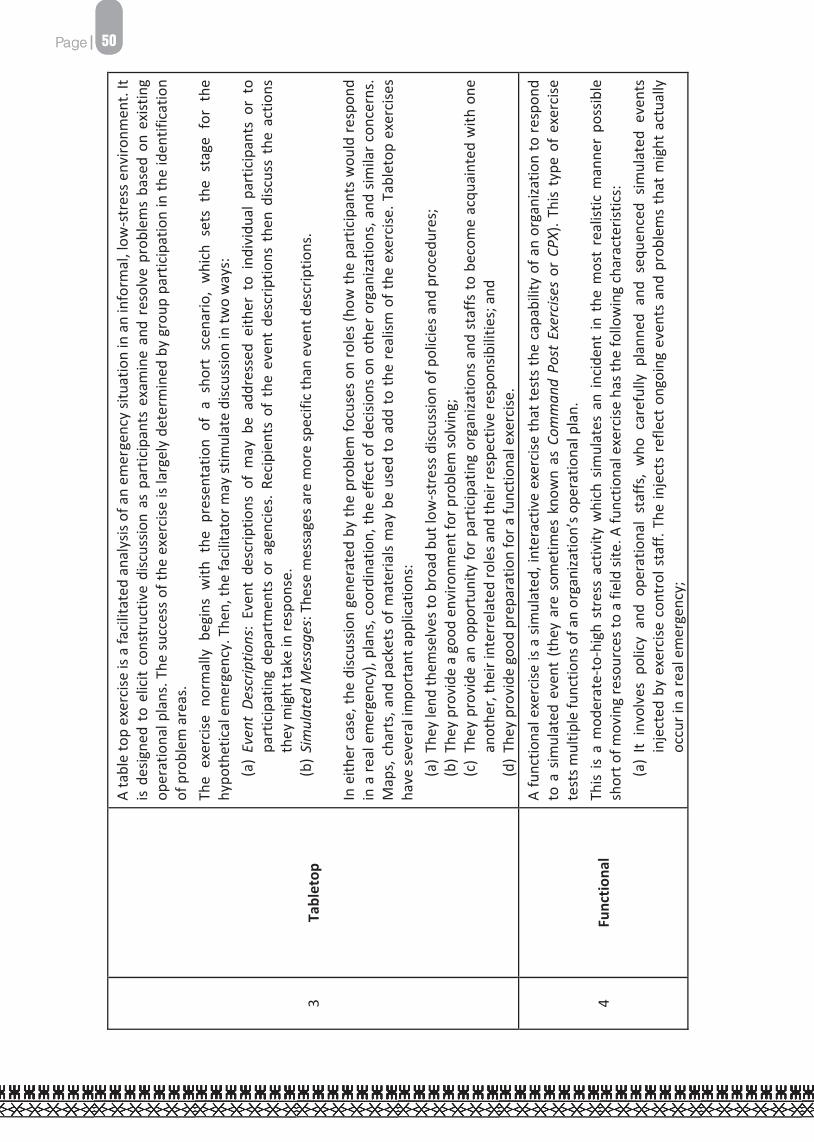
50
Pag
e | 5
0
3 Ta
blet
op
A ta
ble
top
exer
cise
is a
faci
litat
ed a
naly
sis o
f an
emer
genc
y sit
uatio
n in
an
info
rmal
, low
-str
ess e
nviro
nmen
t. It
is de
signe
d to
elic
it co
nstr
uctiv
e di
scus
sion
as p
artic
ipan
ts e
xam
ine
and
reso
lve
prob
lem
s ba
sed
on e
xist
ing
oper
atio
nal p
lans
. The
suc
cess
of t
he e
xerc
ise is
larg
ely
dete
rmin
ed b
y gr
oup
part
icip
atio
n in
the
iden
tific
atio
n of
pro
blem
are
as.
The
exer
cise
nor
mal
ly b
egin
s w
ith t
he p
rese
ntat
ion
of a
sho
rt s
cena
rio,
whi
ch s
ets
the
stag
e fo
r th
e hy
poth
etic
al e
mer
genc
y. T
hen,
the
faci
litat
or m
ay st
imul
ate
disc
ussio
n in
two
way
s:
(a)
Even
t De
scrip
tions
: Ev
ent
desc
riptio
ns o
f m
ay b
e ad
dres
sed
eith
er t
o in
divi
dual
par
ticip
ants
or
to
part
icip
atin
g de
part
men
ts o
r ag
enci
es. R
ecip
ient
s of
the
eve
nt d
escr
iptio
ns t
hen
disc
uss
the
actio
ns
they
mig
ht ta
ke in
resp
onse
. (b
) Sim
ulat
ed M
essa
ges:
The
se m
essa
ges a
re m
ore
spec
ific
than
eve
nt d
escr
iptio
ns.
In e
ither
cas
e, th
e di
scus
sion
gene
rate
d by
the
prob
lem
focu
ses
on ro
les
(how
the
part
icip
ants
wou
ld re
spon
d in
a re
al e
mer
genc
y), p
lans
, coo
rdin
atio
n, th
e ef
fect
of d
ecisi
ons
on o
ther
org
aniza
tions
, and
sim
ilar c
once
rns.
M
aps,
cha
rts,
and
pac
kets
of m
ater
ials
may
be
used
to a
dd to
the
real
ism o
f the
exe
rcise
. Tab
leto
p ex
erci
ses
have
seve
ral i
mpo
rtan
t app
licat
ions
: (a
) Th
ey le
nd th
emse
lves
to b
road
but
low
-str
ess d
iscus
sion
of p
olic
ies a
nd p
roce
dure
s;
(b) T
hey
prov
ide
a go
od e
nviro
nmen
t for
pro
blem
solv
ing;
(c
) Th
ey p
rovi
de a
n op
port
unity
for p
artic
ipat
ing
orga
niza
tions
and
sta
ffs to
bec
ome
acqu
aint
ed w
ith o
ne
anot
her,
thei
r int
erre
late
d ro
les a
nd th
eir r
espe
ctiv
e re
spon
sibili
ties;
and
(d
) The
y pr
ovid
e go
od p
repa
ratio
n fo
r a fu
nctio
nal e
xerc
ise.
4 Fu
nctio
nal
A fu
nctio
nal e
xerc
ise is
a s
imul
ated
, int
erac
tive
exer
cise
that
test
s th
e ca
pabi
lity
of a
n or
gani
zatio
n to
resp
ond
to a
sim
ulat
ed e
vent
(th
ey a
re s
omet
imes
kno
wn
as C
omm
and
Post
Exe
rcise
s or
CPX
). Th
is ty
pe o
f ex
erci
se
test
s mul
tiple
func
tions
of a
n or
gani
zatio
n’s o
pera
tiona
l pla
n.
This
is a
mod
erat
e-to
-hig
h st
ress
act
ivity
whi
ch s
imul
ates
an
inci
dent
in t
he m
ost
real
istic
man
ner
poss
ible
sh
ort o
f mov
ing
reso
urce
s to
a fie
ld si
te. A
func
tiona
l exe
rcise
has
the
follo
win
g ch
arac
teris
tics:
(a
) It
invo
lves
pol
icy
and
oper
atio
nal
staf
fs,
who
car
eful
ly p
lann
ed a
nd s
eque
nced
sim
ulat
ed e
vent
s in
ject
ed b
y ex
erci
se c
ontr
ol s
taff.
The
inje
cts
refle
ct o
ngoi
ng e
vent
s an
d pr
oble
ms
that
mig
ht a
ctua
lly
occu
r in
a re
al e
mer
genc
y;
50
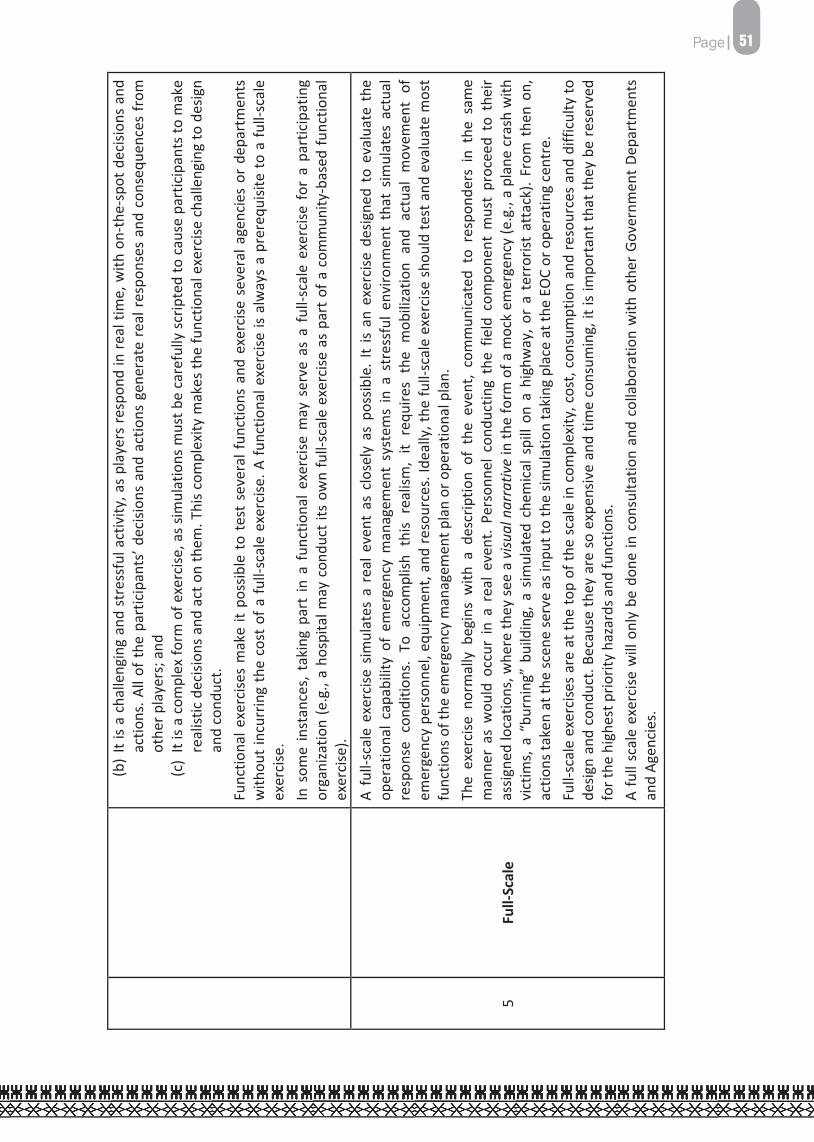
51
Pag
e | 5
0
3 Ta
blet
op
A ta
ble
top
exer
cise
is a
faci
litat
ed a
naly
sis o
f an
emer
genc
y sit
uatio
n in
an
info
rmal
, low
-str
ess e
nviro
nmen
t. It
is de
signe
d to
elic
it co
nstr
uctiv
e di
scus
sion
as p
artic
ipan
ts e
xam
ine
and
reso
lve
prob
lem
s ba
sed
on e
xist
ing
oper
atio
nal p
lans
. The
suc
cess
of t
he e
xerc
ise is
larg
ely
dete
rmin
ed b
y gr
oup
part
icip
atio
n in
the
iden
tific
atio
n of
pro
blem
are
as.
The
exer
cise
nor
mal
ly b
egin
s w
ith t
he p
rese
ntat
ion
of a
sho
rt s
cena
rio,
whi
ch s
ets
the
stag
e fo
r th
e hy
poth
etic
al e
mer
genc
y. T
hen,
the
faci
litat
or m
ay st
imul
ate
disc
ussio
n in
two
way
s:
(a)
Even
t De
scrip
tions
: Ev
ent
desc
riptio
ns o
f m
ay b
e ad
dres
sed
eith
er t
o in
divi
dual
par
ticip
ants
or
to
part
icip
atin
g de
part
men
ts o
r ag
enci
es. R
ecip
ient
s of
the
eve
nt d
escr
iptio
ns t
hen
disc
uss
the
actio
ns
they
mig
ht ta
ke in
resp
onse
. (b
) Sim
ulat
ed M
essa
ges:
The
se m
essa
ges a
re m
ore
spec
ific
than
eve
nt d
escr
iptio
ns.
In e
ither
cas
e, th
e di
scus
sion
gene
rate
d by
the
prob
lem
focu
ses
on ro
les
(how
the
part
icip
ants
wou
ld re
spon
d in
a re
al e
mer
genc
y), p
lans
, coo
rdin
atio
n, th
e ef
fect
of d
ecisi
ons
on o
ther
org
aniza
tions
, and
sim
ilar c
once
rns.
M
aps,
cha
rts,
and
pac
kets
of m
ater
ials
may
be
used
to a
dd to
the
real
ism o
f the
exe
rcise
. Tab
leto
p ex
erci
ses
have
seve
ral i
mpo
rtan
t app
licat
ions
: (a
) Th
ey le
nd th
emse
lves
to b
road
but
low
-str
ess d
iscus
sion
of p
olic
ies a
nd p
roce
dure
s;
(b) T
hey
prov
ide
a go
od e
nviro
nmen
t for
pro
blem
solv
ing;
(c
) Th
ey p
rovi
de a
n op
port
unity
for p
artic
ipat
ing
orga
niza
tions
and
sta
ffs to
bec
ome
acqu
aint
ed w
ith o
ne
anot
her,
thei
r int
erre
late
d ro
les a
nd th
eir r
espe
ctiv
e re
spon
sibili
ties;
and
(d
) The
y pr
ovid
e go
od p
repa
ratio
n fo
r a fu
nctio
nal e
xerc
ise.
4 Fu
nctio
nal
A fu
nctio
nal e
xerc
ise is
a s
imul
ated
, int
erac
tive
exer
cise
that
test
s th
e ca
pabi
lity
of a
n or
gani
zatio
n to
resp
ond
to a
sim
ulat
ed e
vent
(th
ey a
re s
omet
imes
kno
wn
as C
omm
and
Post
Exe
rcise
s or
CPX
). Th
is ty
pe o
f ex
erci
se
test
s mul
tiple
func
tions
of a
n or
gani
zatio
n’s o
pera
tiona
l pla
n.
This
is a
mod
erat
e-to
-hig
h st
ress
act
ivity
whi
ch s
imul
ates
an
inci
dent
in t
he m
ost
real
istic
man
ner
poss
ible
sh
ort o
f mov
ing
reso
urce
s to
a fie
ld si
te. A
func
tiona
l exe
rcise
has
the
follo
win
g ch
arac
teris
tics:
(a
) It
invo
lves
pol
icy
and
oper
atio
nal
staf
fs,
who
car
eful
ly p
lann
ed a
nd s
eque
nced
sim
ulat
ed e
vent
s in
ject
ed b
y ex
erci
se c
ontr
ol s
taff.
The
inje
cts
refle
ct o
ngoi
ng e
vent
s an
d pr
oble
ms
that
mig
ht a
ctua
lly
occu
r in
a re
al e
mer
genc
y;
Pag
e | 5
1
(b) I
t is
a ch
alle
ngin
g an
d st
ress
ful a
ctiv
ity, a
s pl
ayer
s re
spon
d in
real
tim
e, w
ith o
n-th
e-sp
ot d
ecisi
ons
and
actio
ns. A
ll of
the
par
ticip
ants
’ dec
ision
s an
d ac
tions
gen
erat
e re
al r
espo
nses
and
con
sequ
ence
s fr
om
othe
r pla
yers
; and
(c
) It
is a
com
plex
form
of e
xerc
ise, a
s sim
ulat
ions
mus
t be
care
fully
scr
ipte
d to
cau
se p
artic
ipan
ts to
mak
e re
alist
ic d
ecisi
ons
and
act o
n th
em. T
his
com
plex
ity m
akes
the
func
tiona
l exe
rcise
cha
lleng
ing
to d
esig
n an
d co
nduc
t. Fu
nctio
nal e
xerc
ises
mak
e it
poss
ible
to
test
sev
eral
func
tions
and
exe
rcise
sev
eral
age
ncie
s or
dep
artm
ents
w
ithou
t inc
urrin
g th
e co
st o
f a fu
ll-sc
ale
exer
cise
. A fu
nctio
nal e
xerc
ise is
alw
ays
a pr
ereq
uisit
e to
a fu
ll-sc
ale
exer
cise
. In
som
e in
stan
ces,
tak
ing
part
in a
fun
ctio
nal e
xerc
ise m
ay s
erve
as
a fu
ll-sc
ale
exer
cise
for
a p
artic
ipat
ing
orga
niza
tion
(e.g
., a
hosp
ital m
ay c
ondu
ct it
s ow
n fu
ll-sc
ale
exer
cise
as
part
of a
com
mun
ity-b
ased
func
tiona
l ex
erci
se).
5 Fu
ll-Sc
ale
A fu
ll-sc
ale
exer
cise
sim
ulat
es a
rea
l eve
nt a
s cl
osel
y as
pos
sible
. It
is an
exe
rcise
des
igne
d to
eva
luat
e th
e op
erat
iona
l cap
abili
ty o
f em
erge
ncy
man
agem
ent
syst
ems
in a
str
essf
ul e
nviro
nmen
t th
at s
imul
ates
act
ual
resp
onse
con
ditio
ns.
To a
ccom
plish
thi
s re
alism
, it
requ
ires
the
mob
iliza
tion
and
actu
al m
ovem
ent
of
emer
genc
y pe
rson
nel,
equi
pmen
t, an
d re
sour
ces.
Idea
lly, t
he fu
ll-sc
ale
exer
cise
sho
uld
test
and
eva
luat
e m
ost
func
tions
of t
he e
mer
genc
y m
anag
emen
t pla
n or
ope
ratio
nal p
lan.
Th
e ex
erci
se n
orm
ally
beg
ins
with
a d
escr
iptio
n of
the
eve
nt,
com
mun
icat
ed t
o re
spon
ders
in
the
sam
e m
anne
r as
wou
ld o
ccur
in a
rea
l eve
nt.
Pers
onne
l con
duct
ing
the
field
com
pone
nt m
ust
proc
eed
to t
heir
assig
ned
loca
tions
, whe
re th
ey se
e a
visu
al n
arra
tive
in th
e fo
rm o
f a m
ock
emer
genc
y (e
.g.,
a pl
ane
cras
h w
ith
vict
ims,
a “
burn
ing”
bui
ldin
g, a
sim
ulat
ed c
hem
ical
spi
ll on
a h
ighw
ay, o
r a
terr
orist
att
ack)
. Fro
m t
hen
on,
actio
ns ta
ken
at th
e sc
ene
serv
e as
inpu
t to
the
simul
atio
n ta
king
pla
ce a
t the
EO
C or
ope
ratin
g ce
ntre
. Fu
ll-sc
ale
exer
cise
s ar
e at
the
top
of th
e sc
ale
in c
ompl
exity
, cos
t, co
nsum
ptio
n an
d re
sour
ces
and
diffi
culty
to
desig
n an
d co
nduc
t. Be
caus
e th
ey a
re s
o ex
pens
ive
and
time
cons
umin
g, it
is im
port
ant t
hat t
hey
be re
serv
ed
for t
he h
ighe
st p
riorit
y ha
zard
s and
func
tions
. A
full
scal
e ex
erci
se w
ill o
nly
be d
one
in c
onsu
ltatio
n an
d co
llabo
ratio
n w
ith o
ther
Gov
ernm
ent D
epar
tmen
ts
and
Agen
cies
.
51


52 P a g e | 52
SECTION G APPENDICES Glossary Guide to Developing an Emergency & Disaster Management Plan for Divisional & Sub-Divisional Teams Links to Related Plans and Documents Supporting Plan – CD & Pandemic Plan National Health Emergency and Disaster Management Task Force National Health Emergency and Disaster Management Task Force Members Basic Duties Of Health Representatives At An Emergency Operation Centre (EOC) Situation Report Format – Ministry Of Health Rapid Health Assessment Survey Emergency Ration Scale Actions to Ensure Safety of Patients, MoH Staff and Facilities Emergency Contact Numbers
P a g e | 53
GLOSSARY Agency Agencies are Government Ministries, Departments, Organizations, Statutory Authorities, and Public Corporations that have responsibilities in the disaster management organisation. Assessment The process of determining the impact of a disaster or events on a society, the needs for immediate emergency measures to save and sustain the lives of survivors, and the possibilities for expediting recovery and development. Comprehensive Hazard and Risk Management (CHARM) It is a tool that can be used to identify the potential risk that can exacerbate the impact of hazards. This tool is to be widely mainstreamed into planning and budgeting processes by all agencies at national, local and community level. Damage Assessment The preparation of specific, quantified estimates of physical damage resulting from a disaster, recommendations concerning the repair, reconstruction or replacement of structures, equipment, and the restoration of economic (including agricultural) activities. Disaster The occurrence of a sudden or major misfortune which disrupts the basic fabric and normal functioning of a society (or community). An event or series of events which gives rise to casualties and/or damage or loss of property, infrastructure, essential services or means of livelihood on a scale which is beyond the normal capacity of the affected communities to cope with unaided. Disaster Management A collective term encompassing all aspects of planning for and responding to disasters, including both pre- and post-disaster activities. It refers to the management of both the risks and the consequences of disasters. Disaster Mitigation A collective term used to encompass all activities undertaken in anticipation of the occurrence of a potentially disastrous event, including preparedness and long-term risk reduction measures. [Suggested definition: The term used to describe measures, usually specific programmes that are aimed at moderating or reducing the effects of disaster.] Disaster Preparedness Measures that ensure the readiness and ability of a society to: (a) forecast and take precautionary measures in advance of an imminent threat (in cases where advance warnings are possible), and (b) respond to and cope with the effects of a disaster by organising and delivering timely and effective rescue, relief, and other appropriate post-disaster assistance.
52
53P a g e | 52
SECTION G APPENDICES Glossary Guide to Developing an Emergency & Disaster Management Plan for Divisional & Sub-Divisional Teams Links to Related Plans and Documents Supporting Plan – CD & Pandemic Plan National Health Emergency and Disaster Management Task Force National Health Emergency and Disaster Management Task Force Members Basic Duties Of Health Representatives At An Emergency Operation Centre (EOC) Situation Report Format – Ministry Of Health Rapid Health Assessment Survey Emergency Ration Scale Actions to Ensure Safety of Patients, MoH Staff and Facilities Emergency Contact Numbers
P a g e | 53
GLOSSARY Agency Agencies are Government Ministries, Departments, Organizations, Statutory Authorities, and Public Corporations that have responsibilities in the disaster management organisation. Assessment The process of determining the impact of a disaster or events on a society, the needs for immediate emergency measures to save and sustain the lives of survivors, and the possibilities for expediting recovery and development. Comprehensive Hazard and Risk Management (CHARM) It is a tool that can be used to identify the potential risk that can exacerbate the impact of hazards. This tool is to be widely mainstreamed into planning and budgeting processes by all agencies at national, local and community level. Damage Assessment The preparation of specific, quantified estimates of physical damage resulting from a disaster, recommendations concerning the repair, reconstruction or replacement of structures, equipment, and the restoration of economic (including agricultural) activities. Disaster The occurrence of a sudden or major misfortune which disrupts the basic fabric and normal functioning of a society (or community). An event or series of events which gives rise to casualties and/or damage or loss of property, infrastructure, essential services or means of livelihood on a scale which is beyond the normal capacity of the affected communities to cope with unaided. Disaster Management A collective term encompassing all aspects of planning for and responding to disasters, including both pre- and post-disaster activities. It refers to the management of both the risks and the consequences of disasters. Disaster Mitigation A collective term used to encompass all activities undertaken in anticipation of the occurrence of a potentially disastrous event, including preparedness and long-term risk reduction measures. [Suggested definition: The term used to describe measures, usually specific programmes that are aimed at moderating or reducing the effects of disaster.] Disaster Preparedness Measures that ensure the readiness and ability of a society to: (a) forecast and take precautionary measures in advance of an imminent threat (in cases where advance warnings are possible), and (b) respond to and cope with the effects of a disaster by organising and delivering timely and effective rescue, relief, and other appropriate post-disaster assistance.
53
54
P a g e | 54
Disaster Service Liaison Officer (DSLO) An officer, nominated by each of the Agencies that are members of the National Disaster Management Committee, who serves as the primary point of contact for that Agency in matters related to natural disasters. District Disaster Management Council (DDMC) The body at the district level comprising the heads of all Agencies and Non-Governmental Organizations, in the District, chaired by the District Officer and providing assistance to him in coping with disaster mitigation and emergency operations. District DISMAC This acronym encompasses the District Officer’s office, the Emergency Operations Centre (DEOC), and the District Disaster Management Council at the District level and is used in communications to refer to these bodies collectively. Divisional Disaster Management Council The body at the Divisional Level comprising the heads of all Agencies and Non-governmental organisations in the Division, chaired by the Divisional Commissioner, and responsible for providing assistance to the Commissioner in coping with disaster mitigation and emergency operations. Divisional DISMAC This acronym encompasses the Divisional Commissioner’s office, the Emergency Operations Centre (DivEOC), and the Divisional Disaster Management Council at the Division level and is used in communications to refer to these bodies collectively. Emergency An extraordinary situation in which people are unable to meet their basic survival needs, and there are serious and immediate threats to human life and well being. Emergency Operations Centre A suitably equipped and staffed area or room, within which an emergency operation is conducted. Emergency Operations Centres are set up as and when required by the disaster controllers at National, Divisional, and District Levels. Centres may be referred to as National Emergency Operations Centre (NEOC), Divisional Emergency Operations Centre (DivEOC) and District Emergency Operations Centre (DisEOC). Emergency Phase/Period The period during which extraordinary emergency measures must be taken and special emergency procedures and authorities may be applied to save lives and property. It encompasses both the disaster alert and relief periods. Unless altered by the National Controller, the emergency period ends two weeks after the disaster impact. Emergency Operation The actions taken in response to a disaster warning or alert to minimise or contain the eventual negative effects, and those taken to save and preserve lives and provide basic
P a g e | 55
services in the immediate aftermath of a disaster impact for so long as an emergency situation prevails. Hazard A hazard is a natural or human-made phenomenon which may cause physical damage, economic losses, or threaten human life and well being if it occurs in an area of human settlement, agricultural, or industrial activity. Health Emergency Operations Centre Serve as a lead emergency response agency for all public health crises such as epidemics and pandemics Mass Casualty Management (MCM) This deals with victims of mass casualty, and is aimed at minimizing contingent loss of life. National DISMAC This acronym encompasses the National Disaster Management Council (NDMC), the National Disaster Management Operations (NDMO), and the National Emergency Operations Centre (NEOC) at the National Level and is used in communications to refer to these bodies collectively Non-Governmental Organisation (NGO) That body, whose function it is to provide, administer, and distribute under DISMAC advice and guidance, such material and physical assistance as may be made available from non-government sources both within Fiji and from overseas, in response to a declared disaster. Natural Hazard Natural phenomena which occur in proximity of, and pose a threat to, people, structures or economic assets, and which may cause disaster. They are caused by biological, geological, seismic, hydrological, or meteorological conditions or processes in the natural environment. Rehabilitation Actions taken in the aftermath of a disaster to enable basic services to resume functioning assist victims’ self-help efforts to repair dwellings and community facilities, and revive economic activities (including agriculture). State of Emergency That condition, in the whole country or parts of the country, where special emergency regulations are in force to enable the government to cope with a situation in which there are serious threats to human life and well being, or in which people are unable to meet their basic survival needs. In a state of emergency, the National Disaster Controller has control over all government resources in order to address the emergency situation, such as is in line with the National Disaster Management Plan. A State of Emergency is declared by the Prime Minister or the Minister for Regional Development in his capacity as chairman of the National Disaster Management Council.
54

55
P a g e | 54
Disaster Service Liaison Officer (DSLO) An officer, nominated by each of the Agencies that are members of the National Disaster Management Committee, who serves as the primary point of contact for that Agency in matters related to natural disasters. District Disaster Management Council (DDMC) The body at the district level comprising the heads of all Agencies and Non-Governmental Organizations, in the District, chaired by the District Officer and providing assistance to him in coping with disaster mitigation and emergency operations. District DISMAC This acronym encompasses the District Officer’s office, the Emergency Operations Centre (DEOC), and the District Disaster Management Council at the District level and is used in communications to refer to these bodies collectively. Divisional Disaster Management Council The body at the Divisional Level comprising the heads of all Agencies and Non-governmental organisations in the Division, chaired by the Divisional Commissioner, and responsible for providing assistance to the Commissioner in coping with disaster mitigation and emergency operations. Divisional DISMAC This acronym encompasses the Divisional Commissioner’s office, the Emergency Operations Centre (DivEOC), and the Divisional Disaster Management Council at the Division level and is used in communications to refer to these bodies collectively. Emergency An extraordinary situation in which people are unable to meet their basic survival needs, and there are serious and immediate threats to human life and well being. Emergency Operations Centre A suitably equipped and staffed area or room, within which an emergency operation is conducted. Emergency Operations Centres are set up as and when required by the disaster controllers at National, Divisional, and District Levels. Centres may be referred to as National Emergency Operations Centre (NEOC), Divisional Emergency Operations Centre (DivEOC) and District Emergency Operations Centre (DisEOC). Emergency Phase/Period The period during which extraordinary emergency measures must be taken and special emergency procedures and authorities may be applied to save lives and property. It encompasses both the disaster alert and relief periods. Unless altered by the National Controller, the emergency period ends two weeks after the disaster impact. Emergency Operation The actions taken in response to a disaster warning or alert to minimise or contain the eventual negative effects, and those taken to save and preserve lives and provide basic
P a g e | 55
services in the immediate aftermath of a disaster impact for so long as an emergency situation prevails. Hazard A hazard is a natural or human-made phenomenon which may cause physical damage, economic losses, or threaten human life and well being if it occurs in an area of human settlement, agricultural, or industrial activity. Health Emergency Operations Centre Serve as a lead emergency response agency for all public health crises such as epidemics and pandemics Mass Casualty Management (MCM) This deals with victims of mass casualty, and is aimed at minimizing contingent loss of life. National DISMAC This acronym encompasses the National Disaster Management Council (NDMC), the National Disaster Management Operations (NDMO), and the National Emergency Operations Centre (NEOC) at the National Level and is used in communications to refer to these bodies collectively Non-Governmental Organisation (NGO) That body, whose function it is to provide, administer, and distribute under DISMAC advice and guidance, such material and physical assistance as may be made available from non-government sources both within Fiji and from overseas, in response to a declared disaster. Natural Hazard Natural phenomena which occur in proximity of, and pose a threat to, people, structures or economic assets, and which may cause disaster. They are caused by biological, geological, seismic, hydrological, or meteorological conditions or processes in the natural environment. Rehabilitation Actions taken in the aftermath of a disaster to enable basic services to resume functioning assist victims’ self-help efforts to repair dwellings and community facilities, and revive economic activities (including agriculture). State of Emergency That condition, in the whole country or parts of the country, where special emergency regulations are in force to enable the government to cope with a situation in which there are serious threats to human life and well being, or in which people are unable to meet their basic survival needs. In a state of emergency, the National Disaster Controller has control over all government resources in order to address the emergency situation, such as is in line with the National Disaster Management Plan. A State of Emergency is declared by the Prime Minister or the Minister for Regional Development in his capacity as chairman of the National Disaster Management Council.
55

56
P a g e | 56
GUIDE TO DEVELOPING AN EMERGENCY & DISASTER MANAGEMENT PLAN FOR DIVISIONAL & SUB-DIVISIONAL TEAMS
Health Emergency and Disaster Management Action Plans must be developed to suit specific requirements; however there will be certain common elements among them to the National Plans. As a guide, there are five key elements to any operational plan:
a) Situation – a description of the existing or predicted circumstances and any assumptions that underpin the requirement for the plan.
b) Purpose Statement – what the plan sets out to do, expressed as a mission, objective or aim.
c) Execution – a complete description of how the objective will be achieved, including
the individuals or agencies involved and the principal tasks for each. Sometimes expressed as a Concept of Operations.
d) Support Arrangements – an outline of how the plan will be supported in terms of
logistics, finance, administration and other supporting elements.
e) Command/Management Arrangements – a clear assignment of responsibilities and
any key authorities and references. This section may include a description of communication systems or methods if they differ from those normally used.
Plans may be strategic in their approach, such as this one, or may be written at a more tactical, task-oriented level. The elements described above will be required in either option, although they may be framed or presented differently. According to literature, most emergency management plans follow the basic structure outlined above. There is no set format, although most plans group the elements, along with other relevant material, into sections or chapters determined by the objective and scope of the plan. For example, it is often convenient to group the situation, purpose statement and other lead-in material into an introductory section. Comprehensive plans will have an all-hazard orientation but will include hazard-specific information as necessary. Functional annexes, organized around the performance of each broad task or function, may be required.
P a g e | 57
LINKS TO RELATED PLANS AND DOCUMENTS
This appendix provides links to those plans most directly related to this Health Emergency & Disaster Management Plan.
Ministry of Health – Corporate Plan
Fiji National Disaster Management Plan 1995
Fiji Natural Disaster management Act 1998
Fiji National Disaster Risk Management Plan 2006
Fiji Communicable Diseases Surveillance and Diseases Outbreak Guidelines
Fiji National Influenza Pandemic Plan (FINIP)
Fiji National Dengue Strategic Plan 2010 – 2014
Fiji Guidelines for Diagnosis and Management of Typhoid Fever (2010 Revision)
MoH Food Safety Emergency Response Plan 2012
MoH Standard Operating Procedures (SOP) for MoH Emergency Operation Centre (2013)
56

57
P a g e | 56
GUIDE TO DEVELOPING AN EMERGENCY & DISASTER MANAGEMENT PLAN FOR DIVISIONAL & SUB-DIVISIONAL TEAMS
Health Emergency and Disaster Management Action Plans must be developed to suit specific requirements; however there will be certain common elements among them to the National Plans. As a guide, there are five key elements to any operational plan:
a) Situation – a description of the existing or predicted circumstances and any assumptions that underpin the requirement for the plan.
b) Purpose Statement – what the plan sets out to do, expressed as a mission, objective or aim.
c) Execution – a complete description of how the objective will be achieved, including
the individuals or agencies involved and the principal tasks for each. Sometimes expressed as a Concept of Operations.
d) Support Arrangements – an outline of how the plan will be supported in terms of
logistics, finance, administration and other supporting elements.
e) Command/Management Arrangements – a clear assignment of responsibilities and
any key authorities and references. This section may include a description of communication systems or methods if they differ from those normally used.
Plans may be strategic in their approach, such as this one, or may be written at a more tactical, task-oriented level. The elements described above will be required in either option, although they may be framed or presented differently. According to literature, most emergency management plans follow the basic structure outlined above. There is no set format, although most plans group the elements, along with other relevant material, into sections or chapters determined by the objective and scope of the plan. For example, it is often convenient to group the situation, purpose statement and other lead-in material into an introductory section. Comprehensive plans will have an all-hazard orientation but will include hazard-specific information as necessary. Functional annexes, organized around the performance of each broad task or function, may be required.
P a g e | 57
LINKS TO RELATED PLANS AND DOCUMENTS
This appendix provides links to those plans most directly related to this Health Emergency & Disaster Management Plan.
Ministry of Health – Corporate Plan
Fiji National Disaster Management Plan 1995
Fiji Natural Disaster management Act 1998
Fiji National Disaster Risk Management Plan 2006
Fiji Communicable Diseases Surveillance and Diseases Outbreak Guidelines
Fiji National Influenza Pandemic Plan (FINIP)
Fiji National Dengue Strategic Plan 2010 – 2014
Fiji Guidelines for Diagnosis and Management of Typhoid Fever (2010 Revision)
MoH Food Safety Emergency Response Plan 2012
MoH Standard Operating Procedures (SOP) for MoH Emergency Operation Centre (2013)
57

58P a g e | 58
SUPPORTING PLAN – CD & PANDEMIC PLAN
Linkages between the three (3) Ministry of Health Plans at National, Divisional & Subdivisions
To understand the links (above) between the 3 national plans, let’s consider the various scenarios: Scenario 1: CD Outbreak • If an outbreak occurs within any of the health service divisions, the CD Surveillance and Outbreak
Response Manual should be used to assist health workers on the field. • However, if this outbreak should continue and overwhelms the MoH’s capacity to response, then the CEO
could contact the National Disaster and Risk Management Committee for multisectorial participation. Scenario 2: Influenza Pandemic • During the Pre-pandemic phase (1-2), the CD Surveillance and Outbreak Response Manual should be used
simultaneously with the FiNIP. • However, if the country should enter into phase (3-6), the FiNIP plan in conjunction with the HEADMAP
Plan should be referenced. Scenario 3: During a National Disaster or Emergency • In the event of a national natural disaster/emergency; the HEADMAP will be the primary reference
document supplemented by the CD Manual
P a g e | 59
NATIONAL HEALTH EMERGENCY AND DISASTER MANAGEMENT TASK FORCE A stand-by Health Emergency and Disaster Management Task Force (HEAD MTF) is established to provide prompt, coordinate technical and administrative support to the Divisional Health Emergency and Disaster Management Unit (DHEADMU) and the focal point in supportive agencies such as National Disaster Management Office (NDMO), World Health Organization (WHO) and United Nations (UN), etc. The response of the HEAD MTF is activated by the Permanent Secretary for Health (PSH) or in his/ her absence the Deputy Secretary for Public Health (DSPH) following the occurrence of a major emergency situation requiring an integrated and inter-programmatic response (Health departmental representation and response). The Deputy Secretary for Public Health (DSPH) is the designated chairman and in his absence the Deputy Secretary for Hospital Services (DSHS) will chair the team. On their absence the Chief Health Inspector/ National Advisor Environmental Health (CHI/NAEH) take the chairmanship to ensure the proper technical response in the respective areas depending to the status and situation of the emergency. The HEAD MTF will be responsible for the following functions for emergency and disaster response: PRE EMERGENCY AND DISASTER
1. Coordination with the Divisional Emergency and Disaster Management Unit (DEDMU) to uplift the standard of Ministry of Health (MoH) facilities so that it’s not so vulnerable during disasters.
2. The HEAD MTF through the National Health Emergency Coordinator (NHEC) should ensure a sound preparedness of the MoH prior to the emergency and disastrous situations. The tasking includes the following:
Physical structures All the MOH facilities are to be in a safe and sound status or condition at all times.
Communication The communication facilities are to be in a good standard at all times.
Drugs The emergency drug supplies are to be at the centre’s always and the expiry is to be monitored.
Surgical supplies For the emergency surgeries as per diagnosis
Ambulances
To be in excellent condition at all times to tackle any road condition and preferably adverse weather in order to provide the best of the quality service during an emergency
Blood supplies To cater for anticipation of worst emergency scenarios and surplus blood supply in be in the bank to meet the demands
Med vacs (airlifts)
Contingency plans could be drafted to divert emergency cases to a preferably safer route during an emergency and evade the anticipated route e.g. Cyclone or flooding etc.
Awareness
Identifying the type of emergency or disaster and the emergency plan that best suits the situation.
PPE Enough in stock at Sub-Divisional and Divisional Level
58

59P a g e | 59
NATIONAL HEALTH EMERGENCY AND DISASTER MANAGEMENT TASK FORCE A stand-by Health Emergency and Disaster Management Task Force (HEAD MTF) is established to provide prompt, coordinate technical and administrative support to the Divisional Health Emergency and Disaster Management Unit (DHEADMU) and the focal point in supportive agencies such as National Disaster Management Office (NDMO), World Health Organization (WHO) and United Nations (UN), etc. The response of the HEAD MTF is activated by the Permanent Secretary for Health (PSH) or in his/ her absence the Deputy Secretary for Public Health (DSPH) following the occurrence of a major emergency situation requiring an integrated and inter-programmatic response (Health departmental representation and response). The Deputy Secretary for Public Health (DSPH) is the designated chairman and in his absence the Deputy Secretary for Hospital Services (DSHS) will chair the team. On their absence the Chief Health Inspector/ National Advisor Environmental Health (CHI/NAEH) take the chairmanship to ensure the proper technical response in the respective areas depending to the status and situation of the emergency. The HEAD MTF will be responsible for the following functions for emergency and disaster response: PRE EMERGENCY AND DISASTER
1. Coordination with the Divisional Emergency and Disaster Management Unit (DEDMU) to uplift the standard of Ministry of Health (MoH) facilities so that it’s not so vulnerable during disasters.
2. The HEAD MTF through the National Health Emergency Coordinator (NHEC) should ensure a sound preparedness of the MoH prior to the emergency and disastrous situations. The tasking includes the following:
Physical structures All the MOH facilities are to be in a safe and sound status or condition at all times.
Communication The communication facilities are to be in a good standard at all times.
Drugs The emergency drug supplies are to be at the centre’s always and the expiry is to be monitored.
Surgical supplies For the emergency surgeries as per diagnosis
Ambulances
To be in excellent condition at all times to tackle any road condition and preferably adverse weather in order to provide the best of the quality service during an emergency
Blood supplies To cater for anticipation of worst emergency scenarios and surplus blood supply in be in the bank to meet the demands
Med vacs (airlifts)
Contingency plans could be drafted to divert emergency cases to a preferably safer route during an emergency and evade the anticipated route e.g. Cyclone or flooding etc.
Awareness
Identifying the type of emergency or disaster and the emergency plan that best suits the situation.
PPE Enough in stock at Sub-Divisional and Divisional Level
59

60
P a g e | 60
DURING EMERGENCY AND DISASTER • Coordinate and supervise the response from divisions and NDMO on special emphasis in
the assessment of the health needs. • Collect, compile and interpret the information on the impact of health and health
services, health conditions and needs and health risks of the affected areas from the divisions.
• Facilitate the immediate dissemination of the above information with health recommendation to the divisions and the NDMO so that there is a collective approach to the problem but bearing in mind the overlap of duties to avoid duplication.
• Facilitate and coordinate the temporary mobilization of human resources to strengthen the office of affected divisions.
• Facilitate the mobilization of emergency equipment and supplies to the affected areas. • All communication to be channelled between the HEAD MTF first and then it will be
relayed to NDMO representing the divisions affected when the magnitude of the situation deserves it.
• Inform the media and the public on the needs of the affected members and the response of the MoH
• Identifying priorities for extra – budgetary allocations for funding of next phase, REHABILITAION
COMPLETION OF RESPONSE TO EMERGENCY • A SWOT analysis is conducted. Extract and compile the lessons learnt and share with
other division and concurrently a review of the Special Operational Procedures • Provide technical advisors for the rehabilitation projects in the affected divisions.
P a g e | 61
NATIONAL HEALTH EMERGENCY AND DISASTER MANAGEMENT TASK FORCE MEMBERS
1. Permanent Secretary for Health 2. Deputy Secretary for Public Health 3. Deputy Secretary for Hospital Services 4. Deputy Secretary for Administration and Finance 5. National Advisor Non Communicable Disease 6. National Advisor Communicable Disease 7. Chief Health Inspector 8. Director Pharmacy and Biomedical Supply 9. Senior Health Inspector – Environmental Management 10. Senior Health Inspector – Vector 11. Public Health Epidemiologist 12. National Advisor Nutrition 13. Medical Superintendent –CWMH 14. Medical Superintendent –Saint Giles 15. Medical Superintendent –Lautoka 16. Medical Superintendent –Labasa 17. Medical Superintendent – P.J.Twomey 18. Manager Ambulance Services 19. National Blood Bank Coordinator 20. Transport personnel 21. Communication specialist 22. Logistics coordinator 23. National Health Emergency Coordinator 24. WHO, UNICEF
60

61
P a g e | 60
DURING EMERGENCY AND DISASTER • Coordinate and supervise the response from divisions and NDMO on special emphasis in
the assessment of the health needs. • Collect, compile and interpret the information on the impact of health and health
services, health conditions and needs and health risks of the affected areas from the divisions.
• Facilitate the immediate dissemination of the above information with health recommendation to the divisions and the NDMO so that there is a collective approach to the problem but bearing in mind the overlap of duties to avoid duplication.
• Facilitate and coordinate the temporary mobilization of human resources to strengthen the office of affected divisions.
• Facilitate the mobilization of emergency equipment and supplies to the affected areas. • All communication to be channelled between the HEAD MTF first and then it will be
relayed to NDMO representing the divisions affected when the magnitude of the situation deserves it.
• Inform the media and the public on the needs of the affected members and the response of the MoH
• Identifying priorities for extra – budgetary allocations for funding of next phase, REHABILITAION
COMPLETION OF RESPONSE TO EMERGENCY • A SWOT analysis is conducted. Extract and compile the lessons learnt and share with
other division and concurrently a review of the Special Operational Procedures • Provide technical advisors for the rehabilitation projects in the affected divisions.
P a g e | 61
NATIONAL HEALTH EMERGENCY AND DISASTER MANAGEMENT TASK FORCE MEMBERS
1. Permanent Secretary for Health 2. Deputy Secretary for Public Health 3. Deputy Secretary for Hospital Services 4. Deputy Secretary for Administration and Finance 5. National Advisor Non Communicable Disease 6. National Advisor Communicable Disease 7. Chief Health Inspector 8. Director Pharmacy and Biomedical Supply 9. Senior Health Inspector – Environmental Management 10. Senior Health Inspector – Vector 11. Public Health Epidemiologist 12. National Advisor Nutrition 13. Medical Superintendent –CWMH 14. Medical Superintendent –Saint Giles 15. Medical Superintendent –Lautoka 16. Medical Superintendent –Labasa 17. Medical Superintendent – P.J.Twomey 18. Manager Ambulance Services 19. National Blood Bank Coordinator 20. Transport personnel 21. Communication specialist 22. Logistics coordinator 23. National Health Emergency Coordinator 24. WHO, UNICEF
61

62P a g e | 62
BASIC DUTIES OF HEALTH REPRESENTATIVES AT AN EMERGENCY OPERATION CENTRE (EOC)
During an emergency or disaster phases, health representatives will be asked to perform extra-ordinary duties in manning EOC’s. This appendix provides guidance on the responsibilities of health representatives. General Description of Position Represent the Health Authority in:
(a) Public health (Prevention & Early Intervention, Health Protection, Population Health, Primary Health Care);
(b) Health services (Mental Health, Home & Community Care, and Acute Care); and (c) Corporate services.
The primary focus of the health representative position will be: (a) Establish and maintain communication pathways between the NHEC Unit (Ministry of
Health EOC) and the Health Facility EOC; and (b) Provide advice and clarification about health and health service delivery operational
matters, including the relationship with other health partners and stakeholders such as District Office, Provincial Office, Divisional Officer, and Commissioners Office.
The EOC is expected to be provided a suitable work space, computer, applicable communications services and office supplies. The management may provide a cellular telephone, contact lists, documentation binder and health-related forms. Responsibilities of Position Activation Phase:
(a) Review health documentation and contact information to ensure currency and completeness;
(b) Ensure that that EOC knows of your position and how to contact you; and (c) Provide health related advice to the National Office as necessary.
Operational Phase:
(a) Attend EOC orientation if provided;
(b) Establish and operate the EOC work station;
(c) Determine and arrange for staffing in the EOC;
(d) Provide communication between the Sub-Divisional, Divisional & National Levels
P a g e | 63
(e) Provide status and availability updates on facility and other health services relevant to the emergency to assist with response effort, including:
i Facility capacity to receive casualties ii Public health measures such as epidemic control, potable water, food
quality, sewage systems iii Mental health capacity for psychosocial trauma iv Community based client needs v Logistics capacity for provision/transport of needed
supplies/pharmaceuticals vi Assist with coordination of casualty
vii Identify, communicate, and facilitate problem-solving concerning all issues related to health
viii Coordinate discussions regarding resources
(f) Liaise with District/Divisional (Commissioner) regarding the need for: i Sheltering of displaced community based clients
ii Professional mental health services including critical incident stress debriefing
iii Health care service availability in health centres or alternate sites iv Health protection inspection for mass feeding initiatives, potable water
availability and other sanitation matters related to relocation of emergency victims.
Demobilization Phase:
(a) Advise on health services demobilization in the area;
(b) Document and communicate follow-up actions required;
(c) Ensure expenditures and financial claims have been coordinated appropriately;
(d) Provide final documentation report
62

63P a g e | 62
BASIC DUTIES OF HEALTH REPRESENTATIVES AT AN EMERGENCY OPERATION CENTRE (EOC)
During an emergency or disaster phases, health representatives will be asked to perform extra-ordinary duties in manning EOC’s. This appendix provides guidance on the responsibilities of health representatives. General Description of Position Represent the Health Authority in:
(a) Public health (Prevention & Early Intervention, Health Protection, Population Health, Primary Health Care);
(b) Health services (Mental Health, Home & Community Care, and Acute Care); and (c) Corporate services.
The primary focus of the health representative position will be: (a) Establish and maintain communication pathways between the NHEC Unit (Ministry of
Health EOC) and the Health Facility EOC; and (b) Provide advice and clarification about health and health service delivery operational
matters, including the relationship with other health partners and stakeholders such as District Office, Provincial Office, Divisional Officer, and Commissioners Office.
The EOC is expected to be provided a suitable work space, computer, applicable communications services and office supplies. The management may provide a cellular telephone, contact lists, documentation binder and health-related forms. Responsibilities of Position Activation Phase:
(a) Review health documentation and contact information to ensure currency and completeness;
(b) Ensure that that EOC knows of your position and how to contact you; and (c) Provide health related advice to the National Office as necessary.
Operational Phase:
(a) Attend EOC orientation if provided;
(b) Establish and operate the EOC work station;
(c) Determine and arrange for staffing in the EOC;
(d) Provide communication between the Sub-Divisional, Divisional & National Levels
P a g e | 63
(e) Provide status and availability updates on facility and other health services relevant to the emergency to assist with response effort, including:
i Facility capacity to receive casualties ii Public health measures such as epidemic control, potable water, food
quality, sewage systems iii Mental health capacity for psychosocial trauma iv Community based client needs v Logistics capacity for provision/transport of needed
supplies/pharmaceuticals vi Assist with coordination of casualty
vii Identify, communicate, and facilitate problem-solving concerning all issues related to health
viii Coordinate discussions regarding resources
(f) Liaise with District/Divisional (Commissioner) regarding the need for: i Sheltering of displaced community based clients
ii Professional mental health services including critical incident stress debriefing
iii Health care service availability in health centres or alternate sites iv Health protection inspection for mass feeding initiatives, potable water
availability and other sanitation matters related to relocation of emergency victims.
Demobilization Phase:
(a) Advise on health services demobilization in the area;
(b) Document and communicate follow-up actions required;
(c) Ensure expenditures and financial claims have been coordinated appropriately;
(d) Provide final documentation report
63

64P a g e | 64
SITUATION REPORT FORMAT - MINISTRY OF HEALTH
This format is to be used to report to the National Health Emergency Coordinator any significant incident relating to emergency & disaster by respective sub-divisions and divisional health teams.
DIVISION SUB-DIVISION IDENTIFICATION OF EMERGENCY
CURRENT SITUATION / GENERAL INFORMATION
MEDIA ISSUES
COMMENTS
Period: Date: Prepared by:
The information above should be passed by the most appropriate method, usually email or fax. If being passed by email or fax it is important to ensure that the receiving agency is warned that the report is being sent so that it will be received immediately. The report may be transmitted orally by telephone or radio if a written report is not practicable in the circumstances.
P a g e | 65
RAPID HEALTH ASSESSMENT SURVEY Location (area affected):_____________________________________________________
Date: ______________ Prepared by: ___________________________________________
Cleared/authorised: _________________________________________________________
Executive Summary: main problems & needs, the likely evolution, the local response capacity and the additional requirements. 1. Main Issue
Nature of the Emergency The affected area The affected population
2. Health Impact
The direct impact: reasons for alert Other reasons for concern Indirect health impact Pre-emergency baseline morbidity and mortality data, when available Projected evolution of the health situation: main causes of concern in the coming
months
3. Vital Needs: The Current Situation 4. Critical Constraints 5. Response Capacity: Resources that are functioning and close to the affected area 6. Conclusions 7. Recommendations for immediate action.
64
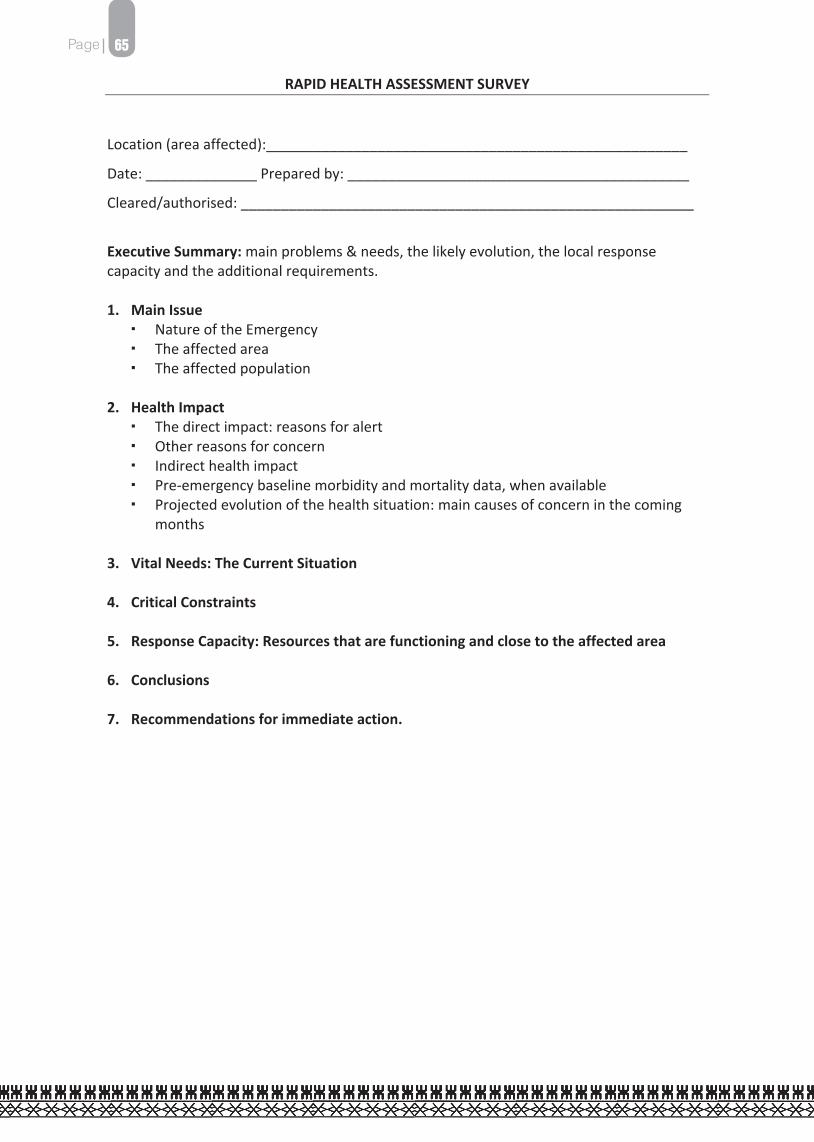
65P a g e | 64
SITUATION REPORT FORMAT - MINISTRY OF HEALTH
This format is to be used to report to the National Health Emergency Coordinator any significant incident relating to emergency & disaster by respective sub-divisions and divisional health teams.
DIVISION SUB-DIVISION IDENTIFICATION OF EMERGENCY
CURRENT SITUATION / GENERAL INFORMATION
MEDIA ISSUES
COMMENTS
Period: Date: Prepared by:
The information above should be passed by the most appropriate method, usually email or fax. If being passed by email or fax it is important to ensure that the receiving agency is warned that the report is being sent so that it will be received immediately. The report may be transmitted orally by telephone or radio if a written report is not practicable in the circumstances.
P a g e | 65
RAPID HEALTH ASSESSMENT SURVEY Location (area affected):_____________________________________________________
Date: ______________ Prepared by: ___________________________________________
Cleared/authorised: _________________________________________________________
Executive Summary: main problems & needs, the likely evolution, the local response capacity and the additional requirements. 1. Main Issue
Nature of the Emergency The affected area The affected population
2. Health Impact
The direct impact: reasons for alert Other reasons for concern Indirect health impact Pre-emergency baseline morbidity and mortality data, when available Projected evolution of the health situation: main causes of concern in the coming
months
3. Vital Needs: The Current Situation 4. Critical Constraints 5. Response Capacity: Resources that are functioning and close to the affected area 6. Conclusions 7. Recommendations for immediate action.
65

66 P a g e | 66
EMERGENCY RATION SCALE This ration Scale will provide approximately 2300 kilocalories and 68 grams protein daily.
Full Scale Sliding Scale Cessation Food Item Amount
for 1 Adult
(for 1 wk)
Amount for 1 Household (average 4
adults) for 1 week
Additional items for
Families with Vulnerable
groups
End of 3 months
(1/2 Ration)
End of 4 months
End of 6 months
Rice 2kg 8kg 4kg Nil Ration Distribution
Stops at6 Months
Flour 1kg 8kg 4kg 10kg Dhal 1/2kg 2kg 1kg 1kg Tinned Meat * 1 tins 4 tins 2 tins Nil Nil Tinned Fish* 1tin 4 tins 2tins 4 tins Nil Skimmed Milk 1/4kg 1kg Nil 1kg 1kg Full Cream Milk Nil Nil 1 packet Nil Nil Sugar 1/4kg 1kg 1kg Nil Oil 1 bottle 1 bottle 1 bottle Nil Salt 1 packet 1 packet 1 packet Nil Curry Powder 100 grams 400 grams Nil Nil Tea Leaves 25 grams 100 grams Nil Nil Water: Children (1L/day) Adults (1.5L/day)
Nil
66
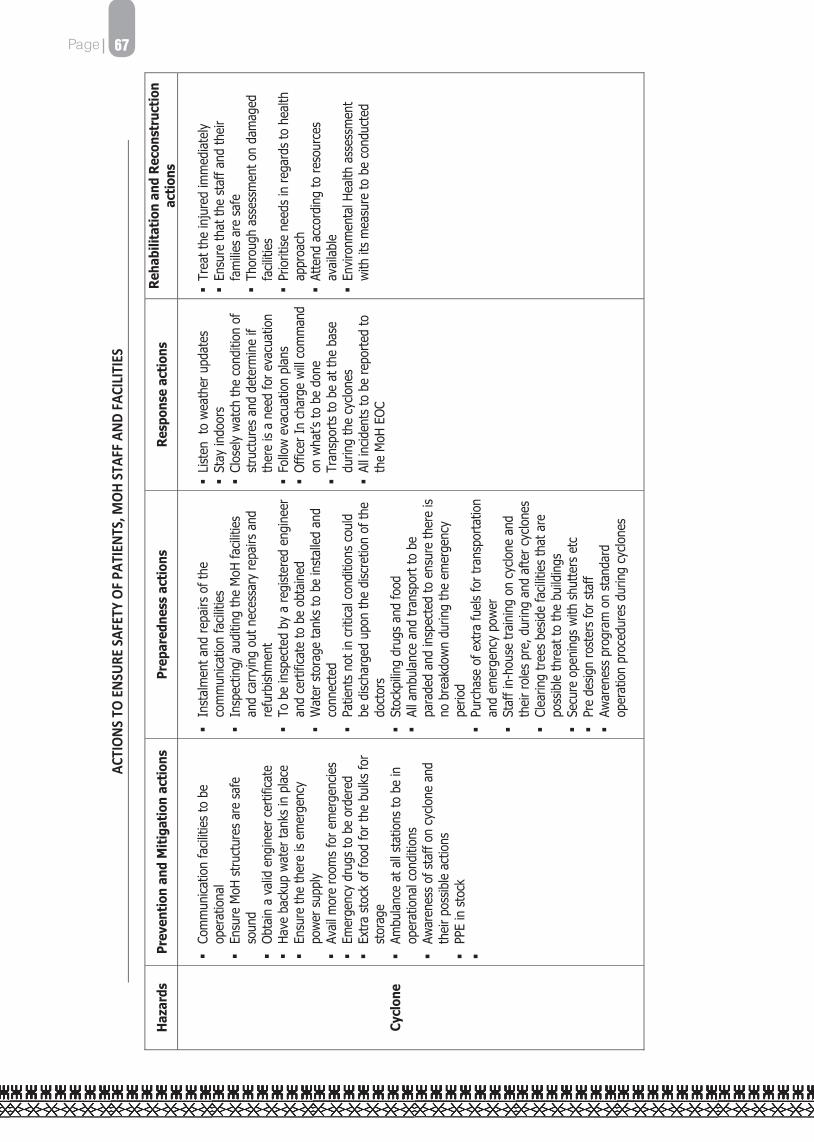
67P a g e | 66
EMERGENCY RATION SCALE This ration Scale will provide approximately 2300 kilocalories and 68 grams protein daily.
Full Scale Sliding Scale Cessation Food Item Amount
for 1 Adult
(for 1 wk)
Amount for 1 Household (average 4
adults) for 1 week
Additional items for
Families with Vulnerable
groups
End of 3 months
(1/2 Ration)
End of 4 months
End of 6 months
Rice 2kg 8kg 4kg Nil Ration Distribution
Stops at6 Months
Flour 1kg 8kg 4kg 10kg Dhal 1/2kg 2kg 1kg 1kg Tinned Meat * 1 tins 4 tins 2 tins Nil Nil Tinned Fish* 1tin 4 tins 2tins 4 tins Nil Skimmed Milk 1/4kg 1kg Nil 1kg 1kg Full Cream Milk Nil Nil 1 packet Nil Nil Sugar 1/4kg 1kg 1kg Nil Oil 1 bottle 1 bottle 1 bottle Nil Salt 1 packet 1 packet 1 packet Nil Curry Powder 100 grams 400 grams Nil Nil Tea Leaves 25 grams 100 grams Nil Nil Water: Children (1L/day) Adults (1.5L/day)
Nil
Page
| 67
ACTI
ONS T
O EN
SURE
SAFE
TY O
F PAT
IENT
S, M
OH ST
AFF A
ND FA
CILIT
IES
Haz
ards
Pr
even
tion
and
Mit
igat
ion
acti
ons
Prep
ared
ness
act
ions
R
espo
nse
acti
ons
Reh
abili
tati
on a
nd R
econ
stru
ctio
n ac
tion
s
Cycl
one
Co
mm
unic
atio
n fa
cilit
ies
to b
e op
erat
iona
l
Ensu
re M
oH s
truc
ture
s ar
e sa
fe
soun
d
Obt
ain
a va
lid e
ngin
eer c
ertif
icat
e
Have
bac
kup
wat
er ta
nks
in p
lace
Ensu
re th
e th
ere
is em
erge
ncy
pow
er s
uppl
y
Avai
l mor
e ro
oms
for e
mer
genc
ies
Em
erge
ncy
drug
s to
be
orde
red
Ex
tra
stoc
k of
food
for t
he b
ulks
for
stor
age
Am
bula
nce
at a
ll st
atio
ns to
be
in
oper
atio
nal c
ondi
tions
Awar
enes
s of
sta
ff on
cyc
lone
and
th
eir p
ossib
le a
ctio
ns
PP
E in
sto
ck
Inst
alm
ent a
nd re
pairs
of t
he
com
mun
icat
ion
faci
litie
s
Insp
ectin
g/ a
uditi
ng th
e M
oH fa
cilit
ies
and
carr
ying
out
nec
essa
ry re
pairs
and
re
furb
ishm
ent
To
be
insp
ecte
d by
a re
gist
ered
eng
inee
r an
d ce
rtifi
cate
to b
e ob
tain
ed
W
ater
sto
rage
tank
s to
be
inst
alle
d an
d co
nnec
ted
Pa
tient
s no
t in
criti
cal c
ondi
tions
cou
ld
be d
ischa
rged
upo
n th
e di
scre
tion
of th
e do
ctor
s
Stoc
kpili
ng d
rugs
and
food
All a
mbu
lanc
e an
d tr
ansp
ort t
o be
pa
rade
d an
d in
spec
ted
to e
nsur
e th
ere
is no
bre
akdo
wn
durin
g th
e em
erge
ncy
perio
d
Purc
hase
of e
xtra
fuel
s fo
r tra
nspo
rtat
ion
and
emer
genc
y po
wer
Staf
f in-
hous
e tr
aini
ng o
n cy
clon
e an
d th
eir r
oles
pre
, dur
ing
and
afte
r cyc
lone
s
Clea
ring
tree
s be
side
faci
litie
s th
at a
re
poss
ible
thre
at to
the
build
ings
Secu
re o
peni
ngs
with
shu
tters
etc
Pre
desig
n ro
ster
s fo
r sta
ff
Awar
enes
s pr
ogra
m o
n st
anda
rd
oper
atio
n pr
oced
ures
dur
ing
cycl
ones
List
en t
o w
eath
er u
pdat
es
Sta
y in
door
s C
lose
ly w
atch
the
cond
ition
of
stru
ctur
es a
nd d
eter
min
e if
ther
e is
a ne
ed fo
r eva
cuat
ion
Fol
low
eva
cuat
ion
plan
s O
ffice
r In
char
ge w
ill co
mm
and
on w
hat’s
to b
e do
ne
Tra
nspo
rts
to b
e at
the
base
du
ring
the
cycl
ones
A
ll in
cide
nts
to b
e re
port
ed to
th
e M
oH E
OC
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
mili
es a
re s
afe
Tho
roug
h as
sess
men
t on
dam
aged
fa
cilit
ies
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
67

68
Page
| 68
Haz
ards
Prev
enti
on a
nd M
itig
atio
n ac
tion
s Pr
epar
edne
ss a
ctio
ns
Res
pons
e ac
tion
s R
ehab
ilita
tion
and
R
econ
stru
ctio
n ac
tion
s
St
orm
su
rges
Bu
ild s
eaw
alls
to s
top
sea
wat
er
dam
ages
to th
e co
astli
nes
and
heal
th
faci
litie
s al
ong
it
Plan
t coa
stal
tree
s th
at c
an m
inim
ise
salt
spra
y
Cons
truc
tion
of h
ealth
faci
litie
s in
land
Ev
acua
te fr
om c
oast
lines
liste
n cl
osel
y to
war
ning
s of
pot
entia
l st
orm
sur
ges
espe
cial
ly d
urin
g cy
clon
es
Aw
aren
ess
prog
ram
on
stan
dard
op
erat
ion
proc
edur
es d
urin
g st
orm
sur
ge
list
en to
wea
ther
bul
letin
s a
sses
situ
atio
n on
the
grou
nd if
fa
cilit
ies
besid
e co
astli
ne a
nd
evac
uate
if th
ere
is a
need
A
ll in
cide
nts
to b
e re
port
ed to
th
e M
oH E
OC
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
mili
es a
re s
afe
Tho
roug
h as
sess
men
t on
dam
aged
fa
cilit
ies
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Fl
ood
Av
oid
cons
truc
ting
heal
th fa
cilit
ies
near
rive
r ban
ks a
nd lo
w ly
ing
area
s
Obt
ain
flood
insu
ranc
e fo
r med
ical
eq
uipm
ent
St
ore
reco
rds
in a
saf
e pl
ace
Ev
acua
te fr
om M
oH fa
cilit
ies
besid
e riv
erba
nks
and
low
-lyin
g ar
eas
pron
e to
flo
odin
g
Awar
enes
s pr
ogra
m o
n st
anda
rd
oper
atio
n pr
oced
ures
dur
ing
flood
Li
sten
clo
sely
to w
arni
ngs
of
pote
ntia
l flo
ods
espe
cial
ly
durin
g cy
clon
es a
nd h
igh
tides
S
tay
indo
ors
Clo
sely
wat
ch th
e le
vel o
f w
ater
and
det
erm
ine
if th
ere
is a
need
for e
vacu
atio
n F
ollo
w e
vacu
atio
n pl
ans
Offi
cer I
n-ch
arge
will
com
man
d on
wha
t’s to
be
done
T
rans
port
s to
be
mov
ed to
hi
gh g
roun
ds
All
inci
dent
s to
be
repo
rted
to
the
MoH
EO
C
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
mili
es a
re s
afe
Tho
roug
h as
sess
men
t on
dam
aged
fa
cilit
ies
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
68

69
Page
| 68
Haz
ards
Prev
enti
on a
nd M
itig
atio
n ac
tion
s Pr
epar
edne
ss a
ctio
ns
Res
pons
e ac
tion
s R
ehab
ilita
tion
and
R
econ
stru
ctio
n ac
tion
s
St
orm
su
rges
Bu
ild s
eaw
alls
to s
top
sea
wat
er
dam
ages
to th
e co
astli
nes
and
heal
th
faci
litie
s al
ong
it
Plan
t coa
stal
tree
s th
at c
an m
inim
ise
salt
spra
y
Cons
truc
tion
of h
ealth
faci
litie
s in
land
Ev
acua
te fr
om c
oast
lines
liste
n cl
osel
y to
war
ning
s of
pot
entia
l st
orm
sur
ges
espe
cial
ly d
urin
g cy
clon
es
Aw
aren
ess
prog
ram
on
stan
dard
op
erat
ion
proc
edur
es d
urin
g st
orm
sur
ge
list
en to
wea
ther
bul
letin
s a
sses
situ
atio
n on
the
grou
nd if
fa
cilit
ies
besid
e co
astli
ne a
nd
evac
uate
if th
ere
is a
need
A
ll in
cide
nts
to b
e re
port
ed to
th
e M
oH E
OC
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
mili
es a
re s
afe
Tho
roug
h as
sess
men
t on
dam
aged
fa
cilit
ies
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Fl
ood
Av
oid
cons
truc
ting
heal
th fa
cilit
ies
near
rive
r ban
ks a
nd lo
w ly
ing
area
s
Obt
ain
flood
insu
ranc
e fo
r med
ical
eq
uipm
ent
St
ore
reco
rds
in a
saf
e pl
ace
Ev
acua
te fr
om M
oH fa
cilit
ies
besid
e riv
erba
nks
and
low
-lyin
g ar
eas
pron
e to
flo
odin
g
Awar
enes
s pr
ogra
m o
n st
anda
rd
oper
atio
n pr
oced
ures
dur
ing
flood
Li
sten
clo
sely
to w
arni
ngs
of
pote
ntia
l flo
ods
espe
cial
ly
durin
g cy
clon
es a
nd h
igh
tides
S
tay
indo
ors
Clo
sely
wat
ch th
e le
vel o
f w
ater
and
det
erm
ine
if th
ere
is a
need
for e
vacu
atio
n F
ollo
w e
vacu
atio
n pl
ans
Offi
cer I
n-ch
arge
will
com
man
d on
wha
t’s to
be
done
T
rans
port
s to
be
mov
ed to
hi
gh g
roun
ds
All
inci
dent
s to
be
repo
rted
to
the
MoH
EO
C
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
mili
es a
re s
afe
Tho
roug
h as
sess
men
t on
dam
aged
fa
cilit
ies
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Page
| 69
Haz
ards
Pr
even
tion
and
Mit
igat
ion
acti
ons
Prep
ared
ness
act
ions
R
espo
nse
acti
ons
Reh
abili
tati
on a
nd
Rec
onst
ruct
ion
acti
ons
La
ndsl
ide
Avoi
d co
nstr
uctin
g M
oH fa
ciliti
es o
n st
eep
slope
Avoi
d co
nstr
uctin
g M
oH fa
ciliti
es a
t fo
ot o
f ste
ep s
lope
Iden
tify
loca
tion
that
is n
ot
vuln
erab
le to
any
of t
hese
men
tione
d di
sast
ers
Ide
ntify
pos
sible
land
slide
site
s th
at a
nd
crea
te a
war
enes
s on
it
Disc
uss
the
haza
rd w
ith y
our s
uper
iors
Eva
cuat
e th
e pa
tient
s, s
taff,
fa
mily
and
em
erge
ncy
supp
lies
as s
oon
as p
ossib
le f
rom
the
dang
er a
rea
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
milie
s ar
e sa
fe
Tho
roug
h as
sess
men
t on
dam
aged
fa
ciliti
es
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Ea
rthq
uake
Bu
ildin
g co
de is
follo
wed
stri
ctly
w
hen
cons
truc
ting
heal
th fa
ciliti
es
Reg
ular
repa
ir an
d m
aint
enan
ces
of
heal
th fa
ciliti
es
Aw
aren
ess
prog
ram
mes
to th
e st
aff a
nd
stick
on
post
er in
all
thre
e la
ngua
ges
on
the
war
d w
alls
for t
he p
atie
nts.
Get
und
er ta
ble
or b
eds
whi
le
at h
ome
to a
void
fallin
g ob
ject
s P
atie
nts
staf
f and
fam
ilies
be
mov
ed a
way
from
slo
pes
with
ro
cks/
tall
build
ings
whi
le
outs
ide
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
milie
s ar
e sa
fe
Tho
roug
h as
sess
men
t on
dam
aged
fa
ciliti
es
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
69

70
Page
| 70
Haz
ards
Pr
even
tion
and
Miti
gatio
n ac
tions
Pr
epar
edne
ss a
ctio
ns
Res
pons
e ac
tions
R
ehab
ilita
tion
and
Rec
onst
ruct
ion
actio
ns
Ts
unam
i
Av
oid
cons
truct
ing
heal
th fa
ciliti
es
alon
g co
astli
ne
Re
loca
te h
ealth
facil
ities
to h
ighe
r gr
ound
s aw
ay fr
om c
oast
s
Em
erge
ncy
evac
uatio
n pl
an
Em
erge
ncy
med
ical s
uppl
ies
Em
erge
ncy
esca
pe ro
ute
Aw
aren
ess
on e
arly
war
ning
sig
ns to
the
MoH
sta
ff an
d fa
mily
at t
he v
ulne
rabl
e ar
eas.
Ru
n to
hig
her g
roun
ds le
avin
g be
hind
all
poss
essio
n
Pr
actic
e of
em
erge
ncy
Sop’
s,
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
milie
s ar
e sa
fe
Tho
roug
h as
sess
men
t on
dam
aged
fa
ciliti
es
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Fi
re
In
stal
l sm
oke
dete
ctor
s an
d fir
e al
arm
in h
ealth
facil
ities
Ensu
re e
lect
rical
wiri
ng is
cer
tifie
d
Cons
truct
kitc
hen
of fi
re re
sista
nt
mat
eria
l
Ensu
re c
ooki
ng a
rea
in th
e ki
tche
n ha
ve a
n ex
haus
t fan
Inst
all f
ire e
xtin
guish
er n
ear k
itche
n
Cons
truct
esc
ape
rout
e w
ithin
hom
e
Iden
tify
an a
ssem
bly
poin
t out
side
of
heal
th fa
ciliti
es
Em
erge
ncy
esca
pe p
lan
Co
nduc
t fire
figh
ting
train
ing
for M
oH
facil
ities
Cond
uct f
ire fi
ghtin
g dr
ills fo
r MoH
sta
ffs
Co
nduc
t fire
esc
ape
dril
ls at
hea
lth
stat
ions
Awar
enes
s on
the
haza
rd a
t all
stat
ions
Fo
llow
ing
esca
pe p
lan
Pr
iorit
ising
wha
t’s to
be
evac
uate
d
Aler
t by
alar
m o
r cal
ling
out
Tsun
ami
No
tify
NFA
Mak
e a
head
cou
nt o
f fam
ily
mem
bers
upo
n ar
rival
at t
he
asse
mbl
y ar
ea
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
milie
s ar
e sa
fe
Tho
roug
h as
sess
men
t on
dam
aged
fa
ciliti
es
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
70

71
Page
| 70
Haz
ards
Pr
even
tion
and
Miti
gatio
n ac
tions
Pr
epar
edne
ss a
ctio
ns
Res
pons
e ac
tions
R
ehab
ilita
tion
and
Rec
onst
ruct
ion
actio
ns
Ts
unam
i
Av
oid
cons
truct
ing
heal
th fa
ciliti
es
alon
g co
astli
ne
Re
loca
te h
ealth
facil
ities
to h
ighe
r gr
ound
s aw
ay fr
om c
oast
s
Em
erge
ncy
evac
uatio
n pl
an
Em
erge
ncy
med
ical s
uppl
ies
Em
erge
ncy
esca
pe ro
ute
Aw
aren
ess
on e
arly
war
ning
sig
ns to
the
MoH
sta
ff an
d fa
mily
at t
he v
ulne
rabl
e ar
eas.
Ru
n to
hig
her g
roun
ds le
avin
g be
hind
all
poss
essio
n
Pr
actic
e of
em
erge
ncy
Sop’
s,
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
milie
s ar
e sa
fe
Tho
roug
h as
sess
men
t on
dam
aged
fa
ciliti
es
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Fi
re
In
stal
l sm
oke
dete
ctor
s an
d fir
e al
arm
in h
ealth
facil
ities
Ensu
re e
lect
rical
wiri
ng is
cer
tifie
d
Cons
truct
kitc
hen
of fi
re re
sista
nt
mat
eria
l
Ensu
re c
ooki
ng a
rea
in th
e ki
tche
n ha
ve a
n ex
haus
t fan
Inst
all f
ire e
xtin
guish
er n
ear k
itche
n
Cons
truct
esc
ape
rout
e w
ithin
hom
e
Iden
tify
an a
ssem
bly
poin
t out
side
of
heal
th fa
ciliti
es
Em
erge
ncy
esca
pe p
lan
Co
nduc
t fire
figh
ting
train
ing
for M
oH
facil
ities
Cond
uct f
ire fi
ghtin
g dr
ills fo
r MoH
sta
ffs
Co
nduc
t fire
esc
ape
dril
ls at
hea
lth
stat
ions
Awar
enes
s on
the
haza
rd a
t all
stat
ions
Fo
llow
ing
esca
pe p
lan
Pr
iorit
ising
wha
t’s to
be
evac
uate
d
Aler
t by
alar
m o
r cal
ling
out
Tsun
ami
No
tify
NFA
Mak
e a
head
cou
nt o
f fam
ily
mem
bers
upo
n ar
rival
at t
he
asse
mbl
y ar
ea
Tre
at th
e in
jure
d im
med
iate
ly
Ens
ure
that
the
staf
f and
thei
r fa
milie
s ar
e sa
fe
Tho
roug
h as
sess
men
t on
dam
aged
fa
ciliti
es
Prio
ritise
nee
ds in
rega
rds
to h
ealth
ap
proa
ch
Atte
nd a
ccor
ding
to re
sour
ces
avai
labl
e E
nviro
nmen
tal H
ealth
ass
essm
ent
with
its
mea
sure
to b
e co
nduc
ted
Page
| 71
Haz
ards
Pr
even
tion
and
Mit
igat
ion
acti
ons
Prep
ared
ness
act
ions
R
espo
nse
acti
ons
Reh
abili
tati
on a
nd R
econ
stru
ctio
n ac
tion
s
D
roug
ht
In
stal
l bac
k-up
wat
er ta
nks
at
hosp
itals
In
stal
latio
n of
wat
er e
fficie
nt
laun
drie
s, to
redu
ce w
ater
use
Stoc
k up
on
extra
line
n an
d eq
uipm
ent f
or u
se d
urin
g dr
ough
t sit
uatio
ns
Emer
genc
y w
ater
sup
ply
plan
for h
ealth
fa
ciliti
es
Co
nduc
t wat
er s
avin
g dr
ills
Aw
aren
ess
amon
g he
alth
sta
ff on
wat
er
savi
ngs
Re
gula
r mai
nten
ance
of w
ater
tank
s
Ensu
re w
ater
tank
s ar
e fu
ll
Follo
w c
limat
e fo
reca
sts
to a
ntici
pate
dr
ough
t per
iods
Emer
genc
y sa
nita
tion
and
hygi
ene
plan
s
Im
plem
enta
tion
of w
ater
sa
ving
pla
n
Emer
genc
y w
ater
sup
ply
e.g.
vi
a tru
cks
from
WAF
.
Impl
emen
t em
erge
ncy
sani
tatio
n an
d hy
gien
e pl
ans
Ev
alua
tion
of e
mer
genc
y w
ater
, sa
nita
tion
and
hygi
ene
plan
s
Iden
tifica
tion
of le
sson
s le
arnt
Inco
rpor
atin
g le
sson
s le
arnt
in
futu
re e
mer
genc
y w
ater
, san
itatio
n an
d hy
gien
e pl
ans.
71

72P a g e | 72
EMERGENCY CONTACT NUMBERS
Listed below are the contacts of the prominent staff from Divisional to Sub – divisional level, those that will be needed before, during and after disasters.
DMOs & SDMO’s List
No. TITLE ADDRESS PHONE 1. DMO Central Cent/East Office, Namosi Hs. Suva 3315331 2. DMO Eastern Cent/East Office, Namosi Hs. 3314988 3. DMO Northern Northern Health, Ro Qomate Hs, Labasa 8812522 4. DMO Western Western Health, Vidilo House, Lautoka 6660411 5 SDMO Macuata Northern Health, Ro Qomate Hs Labasa 8812522 Ext 7402 6 SDMO Savusavu Savusavu Hospital, Savusavu 8850444 7 SDMO Bua Nabouwalu Hosp, Nabouwalu 8836044 8 SDMO Taveuni Waiyevo Hospital, Taveuni 8880444 9 SDMO Nadroga/Navosa Sigatoka Hosp, Sigatoka 6500455 10 SDMO Serua/Namosi Navua Hosp, Navua 3460007 / 3460090 11 SDMO Nadi Nadi Hospital, Nadi 6701128 12 SDMO Lautoka/Yasawa Western Health, Vidilo Hs. Lautoka 6660411 13 SDMO Ba Ba Mission Hosp, Ba 6674022 14 SDMO Tavua Tavua Hosp, Tavua 6680444 15 SDMO Ra Rakiraki Health Centre, Ra 6694368 16 SDMO Kadavu Vunisea Hosp, Tavuki, Kadavu 3620788 17 SDMO Lakeba Lakeba Hospital, Lakeba, Lau 8823153 18 SDMO Lomaloma Lomaloma Hosp, Vanuabalavu 8282222 19 SDMO Lomaiviti Levuka Hosp 3440221 / 3440088 20 SMO Rotuma Rotuma Hosp 8891090 21 SDMO Rewa Nausori Health Centre 3477195 22 SDMO Tailevu Korovou Hosp, Korovou, Tailevu 3430044 23 SDMO Naitasiri Vunidawa Hosp, Naitasiri 3435096 24 SDMO Suva 2nd Floor Cent/East, Namosi Hs 3314988 25 MS CWMH CWM Hospital 3215247 26 MS Labasa Labasa Hospital 8811444 27 MS Lautoka Lautoka Hospital 6660399 28 MS St. Giles St Giles Hospital 3381399 29 MS Tamavua Tamavua/Twomey Hospital 3321499
72

73
P a g e | 73
External Contact Listing
Hazards Lead warning agency Lead response agency Supporting agencies Cyclone Meteorology Department
Namaka, Nadi Phone: 672 4888
National Disaster Management Office1 Knolly Street, Suva Phone: 331 9255/331 9250/331 8099
Police, RFMF, Navy, National Fire Authority, Divisional Commissioners, District Officers, Red Cross
Flood Meteorology Department Namaka, Nadi Phone: 672 4888
National Disaster Management Office1 Knolly Street, Suva Phone: 331 9255/331 9250/331 8099
Police, RFMF, Navy, National Fire Authority, Divisional Commissioners, District Officers, Red Cross
Drought Meteorology Department Namaka, Nadi Phone: 672 4888
National Disaster Management Office1 Knolly Street, Suva Phone: 331 9255/331 9250/331 8099
Landslide NDMO, RFMF, National Fire Authority, Divisional Commissioners, District Officers, Red Cross
Earthquake Mineral Resource Department, 241 Mead Road, Nabua Phone: 338 3910
National Disaster Management Office1 Knolly Street, Suva Phone: 331 9255/331 9250/331 8099
Police, RFMF, Navy, National Fire Authority, Divisional Commissioners, District Officers, Red Cross
Tsunami Meteorology Department Namaka, Nadi Phone: 672 4888
National Disaster Management Office1 Knolly Street, Suva Phone: 331 9255/331 9250/331 8099
Police, RFMF, Navy, National Fire Authority, Divisional Commissioners, District Officers, Red Cross
Volcano Mineral Resource Department, 241 Mead Road, Nabua Phone: 338 3910
National Disaster Management Office1 Knolly Street, Suva Phone: 331 9255/331 9250/331 8099
Police, RFMF, Navy, National Fire Authority, Divisional Commissioners, District Officers, Red Cross
73
74 74



















