The MHS Capital Investment Decision Model Transforming the Decision-Making Process Tri-Service...
24
The MHS Capital Investment Decision Model Transforming the Decision-Making Process Tri-Service Symposium, Boston, MA 13 July 2006
-
Upload
loreen-jennings -
Category
Documents
-
view
214 -
download
1
Transcript of The MHS Capital Investment Decision Model Transforming the Decision-Making Process Tri-Service...

The MHS Capital Investment Decision
Model
Transforming the Decision-Making Process
Tri-Service Symposium, Boston, MA
13 July 2006
2
WHY AM I HERE?
The MHS Capital Investment Decision Model (CIDM)
What is CIDM?
Why do it?
Is there a relationship to the MHS Strategic Plan & QDR 8?
What have we accomplished so far?
How does CIDM work?
Where are we in the process?
How will we implement CIDM?
What are the benefits?

3
WHAT IS CIDM?
Structured decision making that employs the Analytical Hierarchy Process (AHP)
Allows for structuring a decision into smaller parts, proceeding from the goal to objectives down to the alternative courses of action
Employs pairwise comparison judgments throughout the hierarchy to arrive at overall priorities for the alternatives
The decision problem can involve qualitative and quantitative factors
Allows for the consideration of a range of criteria across an organization’s goals and objectives
Provides for an optimization functions as well as provision for policy constraints
Supported by COTS software

4
WHY DO IT?
a. OMB wants us to
b. It works for VA
c. It’s the right thing to do for the MHS
d. All of the above
e. None of the above

5
OMB WAKEUP CALLPBD 726 and the FY05 Program
We lost money, projects, and scope in PBD 726
We could not make succinct and compelling arguments that the FY05 program represented good investments for the MHS.
What’s obvious and compelling to you may not be to others.

6
FINDINGS OF THE 1986 BLUE RIBBON PANEL
Create an office to centrally plan, program, and budget medical facilities
Issues Resolved
No consistent functional and design criteria across Services
Construction cost variation
Medical projects not comparable
Consistent cost models
Central Management
Centralized Advocacy
MILCON based only
Issues Resolved
No consistent functional and design criteria across Services
Construction cost variation
Medical projects not comparable
Consistent cost models
Central Management
Centralized Advocacy
MILCON based only
Issues Still Pending
No coherent method to define priorities and select projects for recommended funding
Inconsistent planning assumptions
Lack consistent programmatic ability to prioritize capital projects
Issues Still Pending
No coherent method to define priorities and select projects for recommended funding
Inconsistent planning assumptions
Lack consistent programmatic ability to prioritize capital projects

7
WHY DO IT (cont)?CIDM Helps in Many Ways
Expedites planning/acquisition timeline
Simplify and standardize project planning
Articulates real MILCON requirements beyond current TOA
Supports programming of most critical needs of MHS
Provides a logical and consistent rationale for selecting projects
Allows us to articulate what is important and why
Ensures inclusiveness and transparency of decision making
Engages clinical operators and resource managers
Incorporates executive review by the SMMAC
Supports QDR transformation initiatives
Links to strategic and business planning

8
WHAT HAVE WE ACCOMPLISHED SO
FAR? Conducted extensive research
Selected software and model
Received ASD(HA) guidance and resources
Developed, weighted, and scaled criteria
Conducted “Top Ten” exercise
Refined criteria
Developed draft implementation guide
Established QDR 8 IPT from HFSC Planning Subcommittee
Obtained funding for site license and additional consulting

9
IS THERE A RELATIONSHIP TO MHS STRATEGY?
Balanced Scorecard Mission & Customers
Mission Elements
Medically ready and protected force and homeland defense for communities
Deployable Medical Capability
Manage and deliver the health benefit
Mission Elements
Medically ready and protected force and homeland defense for communities
Deployable Medical Capability
Manage and deliver the health benefit
MHS Customers
Combatant Commanders & Service Members
Beneficiaries
People of the MHS
MHS Customers
Combatant Commanders & Service Members
Beneficiaries
People of the MHS

10
IS THERE A RELATIONSHIP TO QDR 8?
Medical Infrastructure Transformation
1. Systematic and strategic approach to provide comprehensive visibility of assets
1. Systematic and strategic approach to provide comprehensive visibility of assets
2. Link facility investments with MHS strategic and business goals and enhance joint operations
2. Link facility investments with MHS strategic and business goals and enhance joint operations
3. Transform the MILCON planning, acquisition and recapitalization processes
3. Transform the MILCON planning, acquisition and recapitalization processes

11
GOAL 2 OF QDR 8 Link Facility Investments with MHS
Strategic/Business Goals & Joint Operations
Project focus To Market based portfolio focus linked to strategic and business goals
No consistent programmatic ability to prioritize capital projects across the MHS
To Consistent basis for making capital investments and improved focus for articulating Service investment candidates
Current planning and selection process does not acknowledge dynamic nature of MHS operating environment (GWOT, BRAC, Jointness)
To Evaluation criteria that supports investments consistent with unique requirements of military medicine
Inconsistent planning assumptions across Services
To Consistent investment proposal methodology and evaluation
As IsAs Is To BeTo Be

12
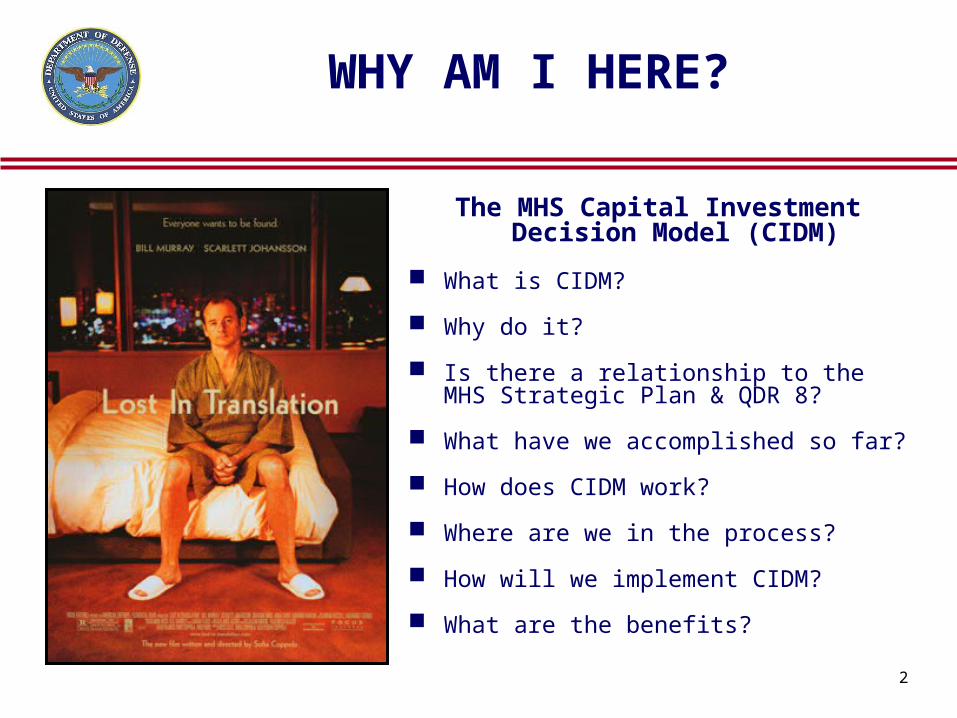
HOW DOES CIDM WORK?Annual Cycle
1. TMA & Services jointly develop/update evaluation criteria
2. TMA updates CIDM Selection & Proposal Guide
3. Services review business plans
4. Services review strategic guidance
5. Services develop and submit concept papers
6. TMA & Services jointly review concept papers
7. Services develop and submit capital investment proposals
8. Capital Investment Review Board scores proposals
9. SMMAC reviews/approves output
10.TMA submits POM/BES/BCP
And repeat…..And repeat…..
(HA, Army, Navy, Air Force, TMA, Functional Experts)
Coordination/Optimization potential
Capital Investment Review Board (CIRB)
Prioritize/Select
Investments
Concept Paper Submit/Forum
Senior Executive Review
SMMAC Ensure Alignment With Strategic Objectives
and Approve Portfolio
PPMD/Service Execution
Acquire/Field/Maintain Capabilities
TMA
Navy
Army
Air Force
JS
HA
MHSStrategic
Plan
PPMD
FINAL
DOD/
National
Strategy
Guidance
Service Recommendations
Business CaseAnalysis
Business Planning
Mission Imperatives
Strategic Guidance
MHS
Capital
Facility
Planning
Guidance
TMA
Navy
Army
Air Force
HA
NovNov
MayMay
Cap Investment Proposals
JunJun
JulJul
SepSep
Budget SubmitTo Comptroller
Coherent method to define priorities Consistent process Linkage to MHS Strategic Plan Senior executive review Reduced acquisition cycle
Coherent method to define priorities Consistent process Linkage to MHS Strategic Plan Senior executive review Reduced acquisition cycleO
bje
ctiv
es
MHS Facilities Capital Facility Development Process
FeedbackModel Revisions
Updated Guidance
& Criteria

14


17

18
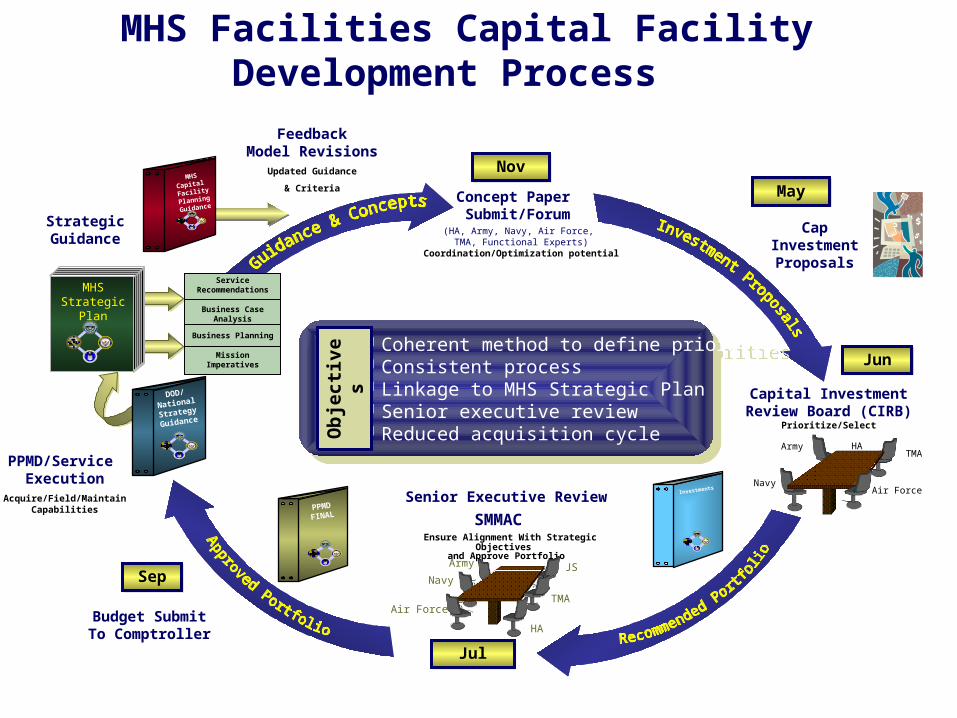
Priority # Project Overall Score
1 USAMRIID 0.8852 USAMRICD 0.8623 NH Gaum replacement 0.8624 Ramstein Clinic Replacement 0.8625 Federal Healthcare Facility 0.8606 MacDill Clinic Replacement 0.8357 Vicenza Women Ctr 0.8318 Tinker Clinic Replacement 0.8209 Spangdahlem Clinic/Dental Clinic Rpmt 0.818
10 Lackland Dental Clinic Replacement 0.81611 Ft Richardson 0.78212 Ft Drum Dental Cl 0.75213 NH Camp Pendleton replacement 0.74614 Ft Hood Women Ctr 0.72715 Ft Irwin Dental Cl 0.72016 Langley Hospital Alteration 0.69717 Fort Hood Replacement hospital 0.67918 Ft Benning Hosp Repl 0.67719 Ft Riley Hosp Repl 0.67220 Peterson Dental Clinic Rpmt 0.66721 CHPPM 0.66122 Scott AHCC Rpmt 0.64923 NEPMU - 6 replacement 0.64524 NH Beaufort replacement 0.64325 Naval Academy replacement 0.63426 Osan Hospital Addition/Alteration 0.57127 Shaw Clinic Replacement 0.56128 NS Pearl Harbor alt/replacement 0.53929 Boone Clinic replacement 0.53630 Patuxent River replacement 0.50231 NH Jacksonville alteration 0.464
“TOP 10” EXERCISE February
2006
Services’ submitted unconstrained Top 10 capital projects
Based on 2 minute verbal briefs of each initiative – no tangible material or data

19
FEB 06 POST EXERCISE PROCESS REVIEW
Lessons Learned
Range of reasons that drive new capital development
The results reflect a point in time based on imperfect criteria and imperfect data
Business planning disconnect
Difficult to provide judgment based on oral presentations – need greater specificity/data/tangible review materials
Some installations may have greater value than others

20
WHERE ARE WE IN THE PROCESS?
Finalizing implementation guide
Templates for concept paper and submission
Standardized business case analysis
Developing SMMAC approval plan

How Will We Implement CIDM?
SMMACCIDM
IPTPPMD Services
Revise c r iter ia and sc ales (05/01/2006 - 05/30/2006)
Team W orkshop - Cr iter ia adjustments, Guide Development, Timeline (06/22/2006)
Team W orkshop - Cr iter ia review/update ( if needed) (07/18/2006)
Prepare Draft Capital Decision Guide (06/23/2006 - 07/29/2006)
Staff Development Guide, Concept Paper, and Investment Templates (07/30/2006 - 09/27/2006)
Rec eive c omments and revise mater ials (09/28/2006 - 10/18/2006)
Present to SMMA C for approval (10/19/2006)
Y
NSMMAC approval (10/20/2006)
Implementation Guidance Complete (10/21/2006)
60 Day Service Review
60 Day Service Review

Capital Planning
Submission Process
Approximately 12 monthFor capital submission
Capital Investment Submission Components
1391 Through Block 12
HCRA or functional narrative for non-healthcare
Departmental PFD
Alternatives Analysis
Business Case/EA
Linkage to Evaluation Criteria
Parametric Cost Estimate
Capital Investment Submission Components
1391 Through Block 12
HCRA or functional narrative for non-healthcare
Departmental PFD
Alternatives Analysis
Business Case/EA
Linkage to Evaluation Criteria
Parametric Cost Estimate
C a p In ve s tm e n tR e v B o a r d ( C IR B )
P P M D S e r v i c e s S M M A C
B u s i n e s s P l a n s D e ve l o p e d ( 1 0 /2 2 /2 0 0 6 )
R e q u e s t fo r C o n c e p t P a p e r s ( 1 1 / 0 1 /2 0 0 6 )
D e ve l o p C o n c e p t P a p e r s ( 1 1 /0 2 / 2 0 0 6 - 1 2 /0 1 / 2 0 0 6 )
R e c i e v e C o n c e p t P a p e r s ( 1 2 /0 2 /2 0 0 6 )
T r i S e r v i c e F o r u m ( 1 2 /0 6 /2 0 0 6 )
D e ve l o p In v e s tm e n t P a c k a g e ( 1 2 /0 7 /2 0 0 6 - 0 5 /2 2 / 2 0 0 7 )
Y
NA p p l i c a ti o n Q A R e v i e w /V a l i d i ty /F e e d b a c k ( 0 5 /2 3 /2 0 0 7 - 0 6 /2 1 /2 0 0 7 )
R e v i s e d In v e s tm e n t P a c k a g e s u b m i tt e d ( 0 6 /2 2 /2 0 0 7 - 0 6 /2 4 /2 0 0 7 )
C I R B S c o r e s P r o p o s a l s ( 0 6 / 2 5 /2 0 0 7 - 0 6 / 2 9 /2 0 0 7 )
S M M A C E xe c u ti ve S u m m a r y D e ve l o p e d ( 0 6 /3 0 /2 0 0 7 - 0 7 /1 3 /2 0 0 7 )
Y
NS M M A C A p p r o ve s /M o d i f i e s p r o g r a m ( 0 7 /1 4 /2 0 0 7 - 0 8 /0 3 /2 0 0 7 )
D e ve l o p b u d g e t s u b m i s s i o n ( 0 8 / 0 4 /2 0 0 7 - 0 9 / 1 7 /2 0 0 7 )
B u d g e t S u b m i tt e d to C o m p tr o l l e r ( 0 9 / 1 8 /2 0 0 7 )

23
SUMMARY
A more structured systematic approach to capital investment decision-making across the MHS
A coherent method to define priorities and select projects for recommended funding
Consistent and programmatic ability to prioritize capital investments
A consistent basis for selection of investments
MHS Senior executive review of proposed investments
Greater probability of OSD and OMB concurrence
* DOD Blue Ribbon Panel on Sizing of Military Medical Facilities, 1986

Questions