The International Journal of Periodontics & Restorative ... › articles ›...
12
The International Journal of Periodontics & Restorative Dentistry
Transcript of The International Journal of Periodontics & Restorative ... › articles ›...

The International Journal of Periodontics & Restorative Dentistry

The application of osseointegratedimplants in the anterior maxilla has cre-ated pointed interest in obtaining anoptimal esthetic result. A prominentroot position is almost always accom-panied by a thin, frail buccal plate thatmay be damaged during toothremoval, resulting in a deformed eden-tulous ridge whose bone morphologywould require augmentation to placean implant in an optimal position forprosthetic restoration (Fig 1a). The shiftin paradigm from the fixed partial den-ture to the implant has placed newemphasis on management of theextraction wound.
Alveolar ridge resorption follow-ing tooth removal is a physiologicallyundesirable and possibly avoidablephenomenon1 (Figs 1b and 1c).Significant knowledge exists of thehealing process of extraction wounds,including contour changes caused2 bybone resorption and the cascade ofhistologic events in both animals andhumans.3–5 The resorption of the alve-olar process following tooth extractionin both jaws is significantly greater onthe buccal aspect than the lingual orpalatal, so that the reduction in widthof the maxillary alveolar ridge is greaterthan the loss of height.6–8 The signifi-cant loss of tissue contour takes place
A Study of the Fate of the Buccal Wallof Extraction Sockets of Teeth withProminent Roots
Myron Nevins, DDS1/Marcelo Camelo, DDS2/Sergio De Paoli, MD, DDS3
Bernard Friedland, BchD, MSc, JD4/Robert K. Schenk, MD, Prof Dr Med5
Stefano Parma-Benfenati, MD, DDS6/Massimo Simion, MD, DDS7
Carlo Tinti, MD, DDS8/Barry Wagenberg, DMD9
The objective of this investigation was to determine the fate of thin buccal bone encasingthe prominent roots of maxillary anterior teeth following extraction. Resorption of the buccalplate compromises the morphology of the localized edentulous ridge and makes it challeng-ing to place an implant in the optimal position for prosthetic restoration. In addition, the useof Bio-Oss as a bone filler to maintain the form of the edentulous ridge was evaluated. Ninepatients were selected for the extraction of 36 maxillary anterior teeth. Nineteen extractionsockets received Bio-Oss, and seventeen sockets received no osteogenic material. All siteswere completely covered with soft tissue at the conclusion of surgery. Computerized tomo-graphic scans were made immediately following extraction and then at 30 to 90 days afterhealing so as to assess the fate of the buccal plates and resultant form of the edentuloussites. The results were assessed by an independent radiologist, with a crest width of 6 mmregarded as sufficient to place an implant. Those sockets treated with Bio-Oss demonstrateda loss of less than 20% of the buccal plate in 15 of 19 test sites (79%). In contrast, 12 of 17control sockets (71%) demonstrated a loss of more than 20% of the buccal plate. In conclu-sion, the Bio-Oss test sites outperformed the control sites by a significant margin. No investi-gator was able to predict which site would be successful without the grafting material eventhough all were experienced clinicians. This leads to the conclusion that a patient has a sig-nificant benefit from receiving grafting materials at the time of extraction. (Int J PeriodonticsRestorative Dent 2006;26:19–29.)
1Clinical Associate Professor, Department of Periodontology, Harvard University School of DentalMedicine, Boston, Massachusetts.
2Director, Brazil Institute for Advanced Dental Studies, Belo Horizonte, Brazil. 3Private Practice, Ancona and Rome, Italy.4Assistant Professor, Department of Oral and Maxillofacial Radiology, Harvard University School ofDental Medicine, Boston, Massachusetts.
5Professor Emeritus, University of Bern, Bern, Switzerland.6Clinical Instructor, Department of Periodontology, University of Ferraro, Ferraro, Italy.7Professor, Department of Periodontology and Implant Rehabilitation, University of Milan School ofDentistry, Italy.
8Private Practice, Flero (Brescia) Italy.9Associate Clinical Professor of Periodontics, New York University Dental School, New York, New York.
Correspondence to: Dr Myron Nevins, 90 Humphrey Street, Swampscott, Massachusetts 01907;fax: 781-598-8050.
19
Volume 26, Number 1, 2006

during the first month after toothextraction, averaging 3 to 5 mm at 6months.9–13 Schropp et al10 reported areduction of 50% of the width of thealveolar ridge at 12 months. Hence,preservation of the alveolus at the timeof extraction of prominent roots in theanterior maxilla is crucial to allow opti-mal implant placement.
Several studies have proposedvarious ridge preservation techniquesfollowing tooth extractions,14–16 includ-ing the placement of graft materialsand/or the use of occlusive mem-branes with success rates of implantsplaced in regenerated bone compa-rable to the success rates of implantsplaced in native bone.17–19 Lekovic etal11,12 used nonresorbable and resorb-able barrier membranes to coverextraction sockets and found that bothoutperformed the controls, ie,untreated extraction sockets, in termsof alveolar process preservation.
While many of these studiesshowed positive clinical results, histo-logic evaluation of grafted sockets hasbeen mixed. The use of grafting mate-rials in fresh extraction sockets hasbeen questioned because of the pos-sibility of interference with the normalhealing process.20 Studies in humansusing demineralized freeze-dried boneallografts, deproteinized bovine bonemineral, or bioactive glass have shownthe presence of graft particles sur-rounded by connective tissue orwoven bone in the alveolar sockets at6 to 9 months following insertion.21–23
However, Serino et al24 reported his-tologic findings when using a polylac-tide and polyglycolide sponge of newmature mineralized bone, with no par-ticles of the filling material identifiedafter 6 months.
A deproteinized bovine bone min-eral (Bio-Oss, Osteohealth) has beenused to graft bone defects and extrac-
tion sockets in dog mandibles; theauthors concluded that it acted as ascaffold for new bone formation.25
Artzi et al21 placed this material in 15fresh human extraction sockets andharvested bone for histologic exami-nation after 9 months. They concludedthat Bio-Oss is an appropriate bio-compatible bone derivative for ridgepreservation. In contrast, Becker et al20
reported that Bio-Oss particles placedin extraction sockets were present after3 to 7 months. Carmagnola et al22
reported that only 40% of the circum-ference of the Bio-Oss particles werein contact with woven bone; however,clinically the quantity and quality ofthe grafted sites allowed for success-ful implant placement. In an animalstudy25 where Bio-Oss was used toresolve artificially created dehiscencedefects around implants, it wasreported that the contact between the Bio-Oss and the bone tissue
20
The International Journal of Periodontics & Restorative Dentistry
Fig 1a Anterior teeth frequently demon-strate prominent roots with thin buccalplates that may have fenestrations or dehis-cences. Even the most careful extractiontechnique may result in the loss of all orsome of the buccal plate.
Fig 1b The four maxillary incisors withprominent roots were extracted 28 daysbefore the CT scan.
Fig 1c The sagittal images demonstratevery weak, resorbing buccal plates (arrows)with minimal connection to the alveolarprocess after 28 days. This deformed alveo-lar process demonstrates what occurs whenprominent roots are extracted without anosteogenic procedure to retain the form ofthe localized edentulous ridge.

amounted to about 85% of the totalgraft surface.
Many variables, including the typeand size of defects, flap closure, typeof graft, and the absence of reliablereference points, make study com-parisons difficult. Few studies10–12,23
have attempted to establish a reliablemodel to investigate the effect of var-ious materials on extraction sockethealing.
A multicenter randomized con-trolled trial evaluated the prognosis ofthe buccal plate after extraction in theesthetic zone.26 Treatment with recom-binant human bone morphogenic pro-tein-2 (rhBMP-2) was compared to notreatment or treatment with only thecarrier. Preoperative and postopera-tive computerized tomographic (CT)scans served as a quantitative methodto compare alveolar ridge resorption orpreservation following grafting proce-dures. The results demonstrated that 9of 20 control patients with noosteogenic material (45%) were able toreceive implants without additionalgrafting. Eighteen of 21 patientstreated with 1.5 mg/mL of rhBMP-2(86%) received implants with additionalgrafting.
Method and materials
The study included three male and sixfemale patients who had a minimumof two periodontally compromised,prominent maxillary anterior teeththat were candidates for extraction.The buccal plate was compromisedbut had to be intact enough to sup-port bone formation in the extractionsocket. Exclusion criteria were:
• Age less than 18 years • Existence of metabolic bone dis-
eases• Current pregnancy• History of malignancy, radiother-
apy, or chemotherapy for malig-nancy in the past 5 years
• History of autoimmune disease• Presence of periapical pathology
Clinical procedures
Tooth extraction was performed byraising a partial-thickness flap to pre-serve the periosteum on the surface toprotect the remaining thin buccal boneplate. The sockets were carefully curet-ted to remove granulation tissue. Arandomization procedure was used toallocate the teeth to either the testgroup or the control group. Nineteenextraction sockets were allocated tothe test group and were grafted withBio-Oss, while the 17 control siteshealed spontaneously. The soft tissuewas completely closed, and all patientswere covered with appropriate antibi-otic therapy for 1 week. Patients worea removable partial denture to replacethe missing teeth.Each patient went directly from theextraction surgery for a CT scan. After30 to 90 days, a second CT scan wasperformed. The mean time period untilthe second CT scan was performedwas 67.68 ± 18.85 days for Bio-Oss–treated extraction sites and 85.53± 16.52 for the control sites. Based onthe postsurgical CT scan, implantswere placed at the discretion of thesurgeon. During implant placement,a total of 10 biopsies (five control andfive test) were harvested for the pur-
21
Volume 26, Number 1, 2006
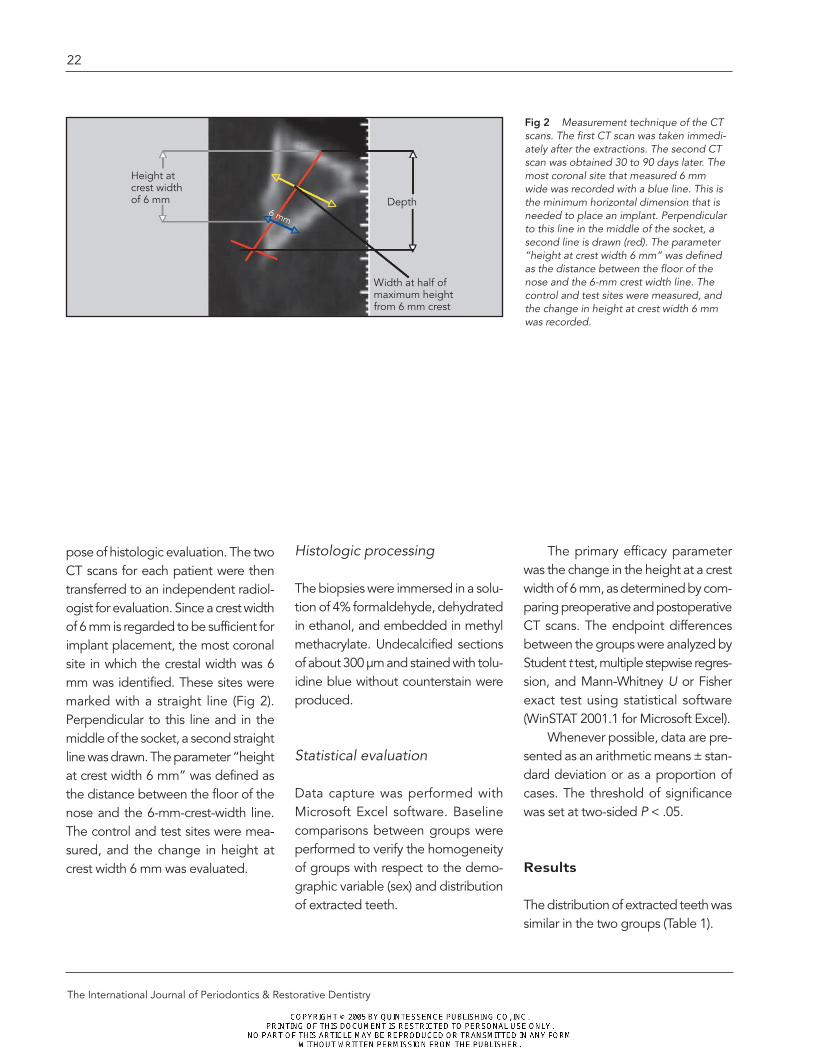
pose of histologic evaluation. The twoCT scans for each patient were thentransferred to an independent radiol-ogist for evaluation. Since a crest widthof 6 mm is regarded to be sufficient forimplant placement, the most coronalsite in which the crestal width was 6mm was identified. These sites weremarked with a straight line (Fig 2).Perpendicular to this line and in themiddle of the socket, a second straightline was drawn. The parameter “heightat crest width 6 mm” was defined asthe distance between the floor of thenose and the 6-mm-crest-width line.The control and test sites were mea-sured, and the change in height atcrest width 6 mm was evaluated.
Histologic processing
The biopsies were immersed in a solu-tion of 4% formaldehyde, dehydratedin ethanol, and embedded in methylmethacrylate. Undecalcified sectionsof about 300 µm and stained with tolu-idine blue without counterstain wereproduced.
Statistical evaluation
Data capture was performed withMicrosoft Excel software. Baselinecomparisons between groups wereperformed to verify the homogeneityof groups with respect to the demo-graphic variable (sex) and distributionof extracted teeth.
The primary efficacy parameterwas the change in the height at a crestwidth of 6 mm, as determined by com-paring preoperative and postoperativeCT scans. The endpoint differencesbetween the groups were analyzed byStudent t test, multiple stepwise regres-sion, and Mann-Whitney U or Fisherexact test using statistical software(WinSTAT 2001.1 for Microsoft Excel).
Whenever possible, data are pre-sented as an arithmetic means ± stan-dard deviation or as a proportion ofcases. The threshold of significancewas set at two-sided P < .05.
Results
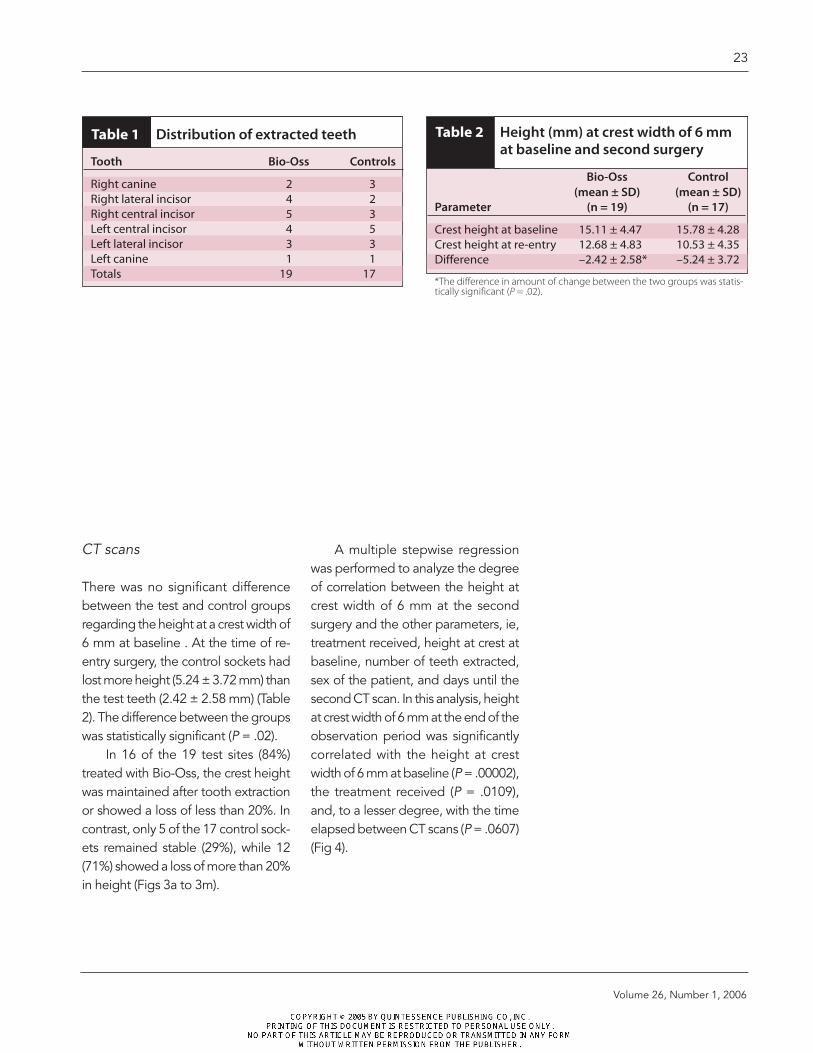
The distribution of extracted teeth wassimilar in the two groups (Table 1).
22
The International Journal of Periodontics & Restorative Dentistry
Height at crest width of 6 mm Depth
Width at half ofmaximum heightfrom 6 mm crest
6 mm
Fig 2 Measurement technique of the CTscans. The first CT scan was taken immedi-ately after the extractions. The second CTscan was obtained 30 to 90 days later. Themost coronal site that measured 6 mmwide was recorded with a blue line. This isthe minimum horizontal dimension that isneeded to place an implant. Perpendicularto this line in the middle of the socket, asecond line is drawn (red). The parameter“height at crest width 6 mm” was definedas the distance between the floor of thenose and the 6-mm crest width line. Thecontrol and test sites were measured, andthe change in height at crest width 6 mmwas recorded.
CT scans
There was no significant differencebetween the test and control groupsregarding the height at a crest width of6 mm at baseline . At the time of re-entry surgery, the control sockets hadlost more height (5.24 ± 3.72 mm) thanthe test teeth (2.42 ± 2.58 mm) (Table2). The difference between the groupswas statistically significant (P = .02).
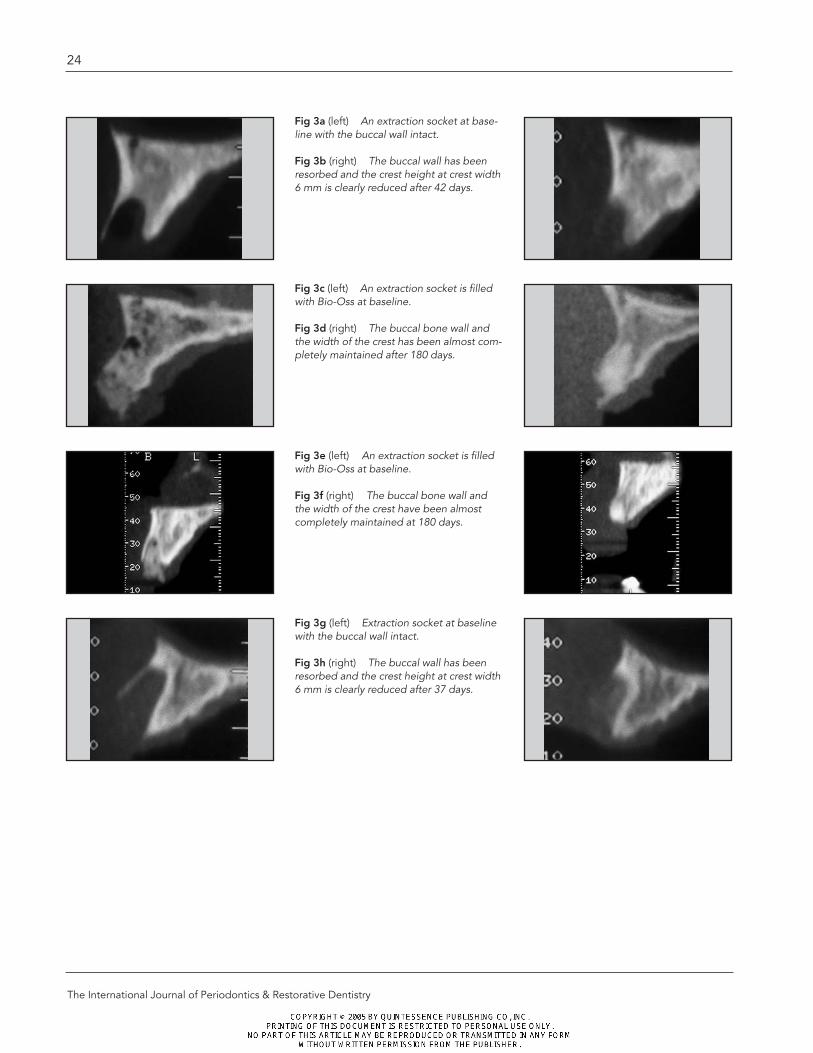
In 16 of the 19 test sites (84%)treated with Bio-Oss, the crest heightwas maintained after tooth extractionor showed a loss of less than 20%. Incontrast, only 5 of the 17 control sock-ets remained stable (29%), while 12(71%) showed a loss of more than 20%in height (Figs 3a to 3m).
A multiple stepwise regressionwas performed to analyze the degreeof correlation between the height atcrest width of 6 mm at the secondsurgery and the other parameters, ie,treatment received, height at crest atbaseline, number of teeth extracted,sex of the patient, and days until thesecond CT scan. In this analysis, heightat crest width of 6 mm at the end of theobservation period was significantlycorrelated with the height at crestwidth of 6 mm at baseline (P = .00002),the treatment received (P = .0109),and, to a lesser degree, with the timeelapsed between CT scans (P = .0607)(Fig 4).
23
Volume 26, Number 1, 2006
Table 1 Distribution of extracted teeth
Tooth Bio-Oss Controls
Right canine 2 3Right lateral incisor 4 2Right central incisor 5 3Left central incisor 4 5Left lateral incisor 3 3Left canine 1 1Totals 19 17
Table 2 Height (mm) at crest width of 6 mmat baseline and second surgery
Bio-Oss Control (mean ± SD) (mean ± SD)
Parameter (n = 19) (n = 17)
Crest height at baseline 15.11 ± 4.47 15.78 ± 4.28 Crest height at re-entry 12.68 ± 4.83 10.53 ± 4.35 Difference –2.42 ± 2.58* –5.24 ± 3.72
*The difference in amount of change between the two groups was statis-tically significant (P = .02).
24
The International Journal of Periodontics & Restorative Dentistry
Fig 3a (left) An extraction socket at base-line with the buccal wall intact.
Fig 3b (right) The buccal wall has beenresorbed and the crest height at crest width6 mm is clearly reduced after 42 days.
Fig 3c (left) An extraction socket is filledwith Bio-Oss at baseline.
Fig 3d (right) The buccal bone wall andthe width of the crest has been almost com-pletely maintained after 180 days.
Fig 3e (left) An extraction socket is filledwith Bio-Oss at baseline.
Fig 3f (right) The buccal bone wall andthe width of the crest have been almostcompletely maintained at 180 days.
Fig 3g (left) Extraction socket at baselinewith the buccal wall intact.
Fig 3h (right) The buccal wall has beenresorbed and the crest height at crest width6 mm is clearly reduced after 37 days.

25
Volume 26, Number 1, 2006
Fig 3i (left) Extraction socket at baselinewith the buccal wall intact.
Fig 3j (right) The buccal wall has beenresorbed, and the crest height at crestwidth 6 mm is clearly reduced after 61 days.
Fig 3k An extraction socket filled withBio-Oss at baseline.
Fig 3l The buccal bone wall and the widthof the crest have been almost completelymaintained at 150 days.
Fig 3m Clinical observation of sites shownin 3i to 3l at the time of implant placement.A= test site (treated with Bio-Oss); B= con-trol site (no treatment).
Fig 4 Distribution of extraction sockets by percent change in crestal height versusbaseline. Stable means less than 20% crestal height was lost. 16
14
12
10
8
6
4
2
0Stable 20% to 40%
loss40% to 60%
loss> 60% loss
No.
of s
ites
Bio-Oss
Control
A
B
Histologic results
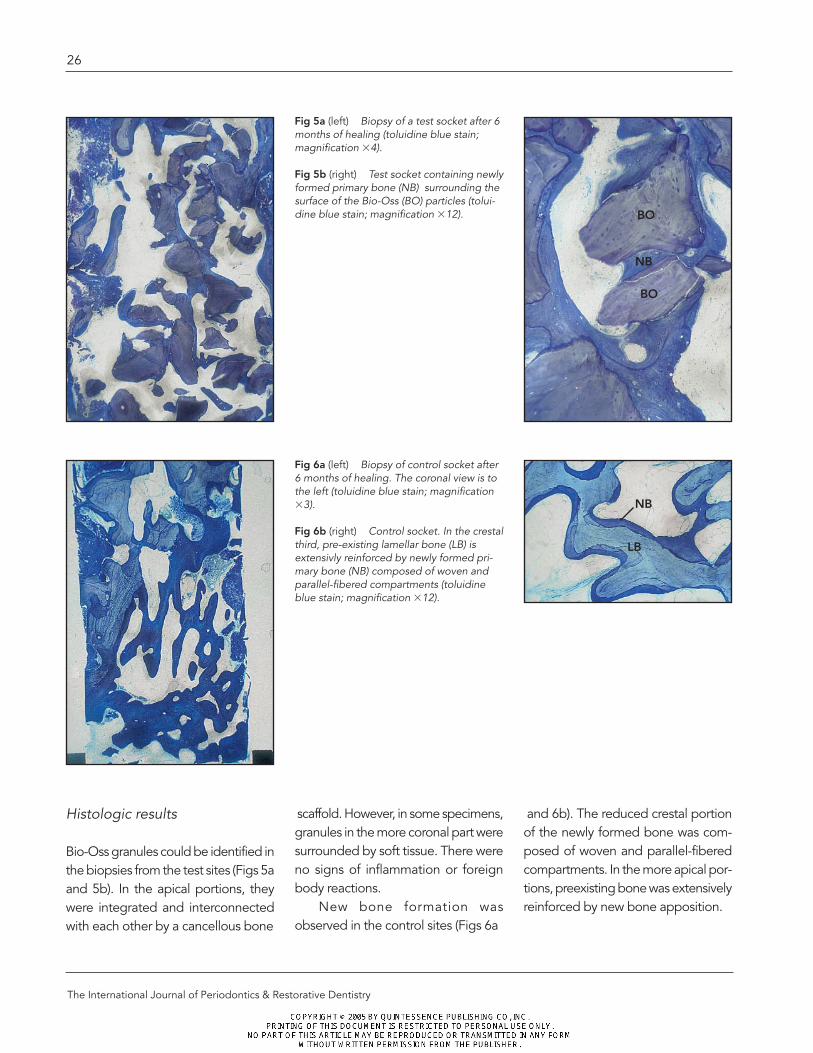
Bio-Oss granules could be identified inthe biopsies from the test sites (Figs 5aand 5b). In the apical portions, theywere integrated and interconnectedwith each other by a cancellous bone
scaffold. However, in some specimens,granules in the more coronal part weresurrounded by soft tissue. There wereno signs of inflammation or foreignbody reactions.
New bone formation wasobserved in the control sites (Figs 6a
and 6b). The reduced crestal portionof the newly formed bone was com-posed of woven and parallel-fiberedcompartments. In the more apical por-tions, preexisting bone was extensivelyreinforced by new bone apposition.
26
The International Journal of Periodontics & Restorative Dentistry
Fig 5a (left) Biopsy of a test socket after 6months of healing (toluidine blue stain;magnification �4).
Fig 5b (right) Test socket containing newlyformed primary bone (NB) surrounding thesurface of the Bio-Oss (BO) particles (tolui-dine blue stain; magnification �12).
Fig 6a (left) Biopsy of control socket after6 months of healing. The coronal view is tothe left (toluidine blue stain; magnification�3).
Fig 6b (right) Control socket. In the crestalthird, pre-existing lamellar bone (LB) isextensivly reinforced by newly formed pri-mary bone (NB) composed of woven andparallel-fibered compartments (toluidineblue stain; magnification �12).
BO
NB
BO
NB
LB
Discussion
The successful introduction of osseoin-tegrated implants into dental treat-ment planning requires an astute eval-uation of the site that will receive theimplant. Significant considerationsbegin with the preservation of the alve-olar process that houses the roots to beextracted and decisions as to whetherit is advantageous to augment theseareas to protect the morphology ofthe proposed implant site (see Fig3).This becomes a major concern whenteeth with prominent roots are to beextracted because of their thin, fragilebuccal plates.
Previous investigators proposedthat a significant proportion of the buc-cal plate would be lost to resorption insuch cases, and a recent study sup-ports this position.26 A randomized,controlled trial concluded that a cohortof patients whose extraction socketswere treated with rhBMP-2 were ableto receive implants 86% of the timewithout further grafting procedures,
The results of this comparativestudy demonstrate that the loss in cre-stal height after extraction of maxillaryanterior teeth is significantly reducedby the treatment of the extraction sock-ets with Bio-Oss. Over the observa-tion period, control sockets lost moreheight (5.24 ± 3.72 mm) than the testsites (2.42 ± 2.58 mm) (see Table 2).The difference between the twogroups was statistically significant (P = .02).
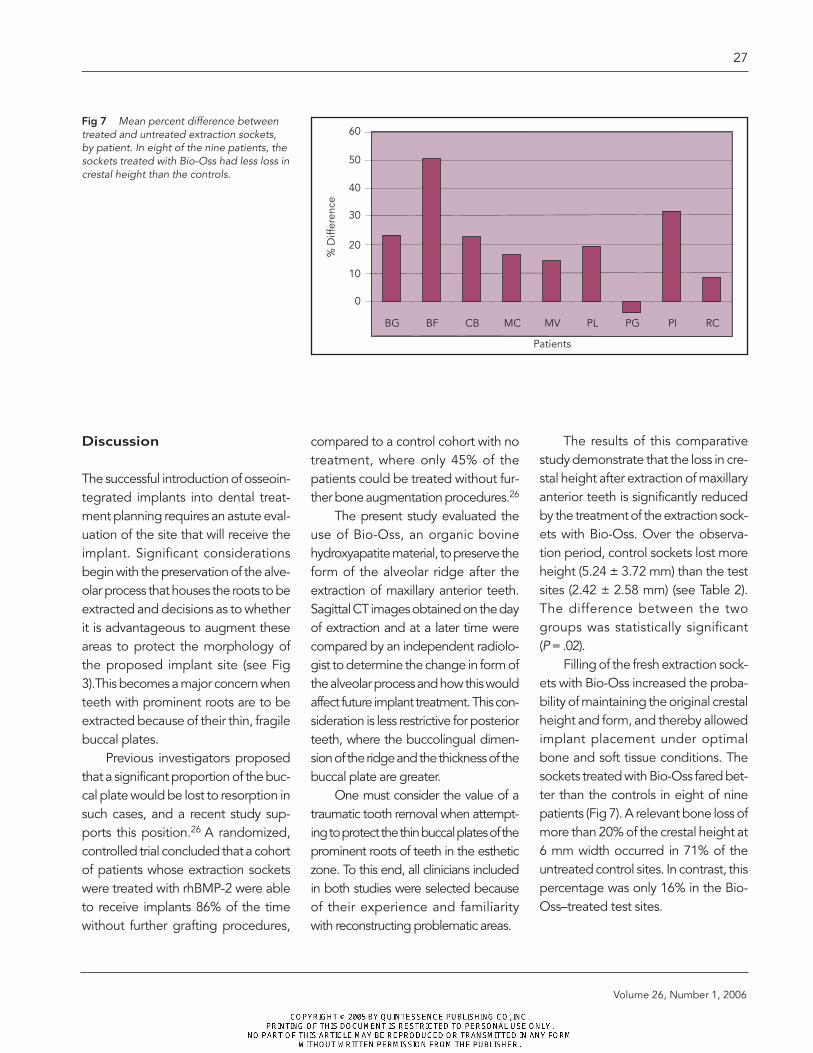
Filling of the fresh extraction sock-ets with Bio-Oss increased the proba-bility of maintaining the original crestalheight and form, and thereby allowedimplant placement under optimalbone and soft tissue conditions. Thesockets treated with Bio-Oss fared bet-ter than the controls in eight of ninepatients (Fig 7). A relevant bone loss ofmore than 20% of the crestal height at6 mm width occurred in 71% of theuntreated control sites. In contrast, thispercentage was only 16% in the Bio-Oss–treated test sites.
compared to a control cohort with notreatment, where only 45% of thepatients could be treated without fur-ther bone augmentation procedures.26
The present study evaluated theuse of Bio-Oss, an organic bovinehydroxyapatite material, to preserve theform of the alveolar ridge after theextraction of maxillary anterior teeth.Sagittal CT images obtained on the dayof extraction and at a later time werecompared by an independent radiolo-gist to determine the change in form ofthe alveolar process and how this wouldaffect future implant treatment. This con-sideration is less restrictive for posteriorteeth, where the buccolingual dimen-sion of the ridge and the thickness of thebuccal plate are greater.
One must consider the value of atraumatic tooth removal when attempt-ing to protect the thin buccal plates of theprominent roots of teeth in the estheticzone. To this end, all clinicians includedin both studies were selected because of their experience and familiarity with reconstructing problematic areas.
27
Volume 26, Number 1, 2006
Fig 7 Mean percent difference betweentreated and untreated extraction sockets,by patient. In eight of the nine patients, thesockets treated with Bio-Oss had less loss increstal height than the controls.
60
50
40
30
20
10
0
BG BF CB MC MV PL PG PI RC%
Diff
eren
cePatients

Conclusion
There were a significant number ofbuccal plate casualties even whencarefully selected clinicians extractedteeth with prominent roots. Thisresulted in a deformed localized eden-tulous ridge for the control group,compared to those extraction woundsthat received Bio-Oss. Some woundshealed correctly with no treatment, butwe were unable to identify thesebefore extraction in this randomizedstudy. Therefore, it would seem pru-dent to introduce an osteoconductivesubstance into the extraction socketsof teeth with prominent roots to avoidloss of the buccal plate and the result-ing compromises in implant treatment.
Acknowledgments
We thank Dr Reto Brignoli, Tradyser, Zurich,Switzerland, for performing the statistical analy-sis and Isabella Rocchietta for her contributionsto this manuscript. We also greatly appreciatethe guidance of Dr Birgit Wenz and BettinaLey.
References
1. Carlsson H, Thilander H, Hedegard B.Histologic changes in the upper alveolarprocess after extractions with or withoutinsertion of an immediate full denture. ActaOdontol Scand 1967;25:21–43.
2. Huebsch RF, Hansen LS. A histopatholog-ic study of extraction wounds in dogs. OralSurg Oral Med Oral Pathol 1969;28:187–196.
3. Amler MH, Johnson PL, Salsman I.Histologic and histochemical investigationof human alveolar socket healing in undis-turbed extraction wounds. J Am DentAssoc 1960;61:46–48.
4. Iasella JM, Greenwell H, Miller RL, et al.Ridge preservation with freeze dried boneallograft and a collagen membrane com-pared to extraction alone for implant sitedevelopment. J Periodontol 2003;74:990–999.
5. Pietrokovski J, Massler M. Alveolar ridgeresorption following tooth extraction. JProsthet Dent 1967 Jan;17(1):21–27.
6. Cardaropoli G, Aravjo M, Lindhe J.Dynamics of bone tissue formation in toothextraction sites. An experimental study indogs. J Clin Periodontol 2003;30:809–818.
7. Johnson K. A study of the dimensionalchanges occurring in the maxilla followingclosed face immediate denture treatment.Aust Dent J 1969 Dec;14(6):370–376.
8. Araujo MG, Lindhe J. Dimensional ridgealterations following tooth extraction. Anexperimental study in the dog. J ClinPeriodontol 2005;32:212–218.
9. Lam RV. Contour changes of the alveolarprocess following extractions. J ProsthetDent 1960;10:25–32.
10. Schropp L, Wenzel A, Kostopoulos L,Karning T. Bone healing and soft tissuecontour changes following single-toothextraction: A clinical and radiographic 12-month prospective study. Int J PeriodonticsRestorative Dent 2003;23:313–323.
11. Lekovic V, Kennev EB, Weinlaender M, etal. A bone regenerative approach to alve-olar ridge maintenance following toothextraction. Report of 10 cases. J Perio-dontol 1997 Jun;68:363–370.
28
The International Journal of Periodontics & Restorative Dentistry
12. Lekovic V, Camargo PM, Klokkevold PR, etal. Preservation of alveolar bone in extrac-tion sockets using bioabsorbable mem-branes. J Periodontol 1998;69:1044–1049.
13. Camargo PM, Lekovic V, Weinlaender M,et al. Influence of bioactive glass onchanges in alveolar process dimensionsafter exodontias. Oral Surg Oral Med OralPathol Oral Radiol Endod 2000 Nov;90(5):581–586.
14. Mellonig JT, Triplett RG. Guided tissueregeneration and endosseous dentalimplants. Int J Periodontics RestorativeDent 1993;13:108–119.
15. Simion M, Dahlin C, Trisi P, Piattelli A.Qualitative and quantitative comparativestudy on different filing materials used inbone tissue regeneration: A controlledclinical study. Int J Periodontics RestorativeDent 1994 Jun;14(3):198–215.
16. Simion M, Trisi P, Piattelli A. Vertical ridgeaugmentation using a membrane tech-nique associated with osseointegratedimplants. Int J Periodontics RestorativeDent 1994;14:496–511.
17. Nevins M, Mellonig JT, Clem DS III, ReiserGM, Buser DA. Implants in regeneratedbone: Long-term survival. Int J Periodon-tics Restorative Dent 1998 Feb;18(1):34–35.
18. Fugazzotto PA. Success and failure rates ofosseointegrated implants in function inregenerated bone for 6 to 51 months: Apreliminary report. Int J Oral MaxillofacImplants 1997;12:17–24.
19. Buser D, Dula K, Lang NP, Nyman S. Long-term stability of osseointegrated implantsin bone regenerated with the membranetechnique. 5-year results of a prospectivestudy with 12 implants. Clin Oral ImplantsRes 1996;7:175–183.
20. Becker W, Cameron C, Sennerby L, UristM, Becker B. Histologic findings afterimplantation and evaluation of differentgrafting materials and titanium microscrews into extraction sockets: Casereports. J Periodontol 1998;69:414–421.
21. Artzi Z, Tal H, Davan D. Porous bovinebone mineral in healing of human extrac-tion sockets. Part 1: Histomorphometricevaluations at 9 months. J Periodontol2000;21:1015–1023.
22. Carmagnola D, Adrisens P, Berglundh T.Healing of human extraction sockets filledwith Bio-Oss. Clin Oral Implants Res2003;14:137–143.
23. Froum S, Cho SC, Rosenberg F, Rohrer M,Tarnow D. Histological comparison of heal-ing extraction sockets implanted withbioactive glass or demineralized freeze-dried bone allograft: A pilot study. JPeriodontol 2002 Jan;73(1):94–102.
24. Serino G, Biancu S, Iezzi G, Piattelli A.Ridge preservation following tooth extrac-tion using a polylactide and polyglycolidesponge as space filler: A clinical and his-tological study in humans. Clin OralImplants Res 2003;14:651–658.
25. Berglundh T, Lindhe J. Healing aroundimplants placed in bone defects treatedwith Bio-Oss. An experimental study in thedog. Clin Oral Implants Res 1997;8:117–124.
26. Fiorellini J, Howell TH, Cochran D, et al.Randomized study evaluating recombi-nant human bone morphogenetic protein-2 for extraction socket augmentation. JPeriodontol 2005;76:605–613.
29
Volume 26, Number 1, 2006