The Hashemite Kingdom of Jordan Ministry of · PDF fileThe Hashemite Kingdom of Jordan...
The Hashemite Kingdom of Jordan Ministry of Health Non-Communicable Diseases Directorate National Registry of End Stage Renal Disease ( ESRD ) Annual Report 2013 www.moh.gov.jo Tel: 5678197 Fax: 5656489 Jordan
-
Upload
nguyenthien -
Category
Documents
-
view
226 -
download
3
Transcript of The Hashemite Kingdom of Jordan Ministry of · PDF fileThe Hashemite Kingdom of Jordan...
The Hashemite Kingdom of Jordan
Ministry of Health
Non-Communicable Diseases Directorate
National Registry of End Stage Renal Disease
( ESRD )
Annual Report 2013
www.moh.gov.jo
Tel: 5678197 Fax: 5656489
Jordan

The Hashemite Kingdom of Jordan
Ministry of Health
Non-Communicable Disease Directorate
National Registry of End Stage Renal Disease
(ESRD)
Annual Report 2013
Prepared by:
Dr. Ayyob As-Sayaideh Dr. Salem Al-Qaisi

His Majesty King Abdullah II


5
List of the team who participated in achieving this ESRD annual report:
Dr Mohammad Salameh El-Lozi
Senior Consultant in Internal Medicine,
Nephrology and Transplantation. MRCP (UK). FRCP (London). FRCP (Glasgow), Private
sector and P.H.H.
Dr Khaled Ali zayed
Nephrologist, MOH.
Dr Elias Turk
Nephrologist, MOH.
Dr Kamal Hassan Arkoub
Specialist in Community Medicine. MOH.

6
Foreword
sixth
2013

7
Acknowledgement
The National ESRD Registry operates under the umbrella of the Ministry of Health;
however, it works in cooperation with a large number of hospitals from all health sectors,
Nephrologists and Nurses working in dialysis units who provide the registry with valuable
and vital data required for success.
We would like to thank all those who cooperate with us, report and facilitate our work,
namely Nephrologists, Physicians, Nurses and staff of the Dialysis Units. The obvious sup-
port of focal points in all dialysis units is highly appreciated.
We would like to thank Mrs. Rasha Kokash for her effort in data entry of all ESRD Data to
special designed software for the Registry.
Special thanks to our focal points-head of Renal unit in all governmental , private , military
and university hospitals for the timely collection and submission of data to the registry.
The interaction between the Registry and the Jordan Society of Nephrology is very positive
and greatly appreciated.
The dedicated hard work during the process of data collection and data entry of the staff in
the registry is acknowledged.
We are very grateful to the World Health Organization for its support in preparing and pub-
lishing this report.
Dr. Ayyob As-SayaidehDr.Basheer AL-Qaseer

8
Name of HospitalsRoyal Medical Services Hospital Name Site Phone numberKing Hussein Medical center Amman 5804804Queen Alia Military Hospital Amman 5157100Prince Hashem Bin Al Hussein Zarqa’a 3962002Prince Hashem Bin Abudullah Aqaba 2014111Prince Ali Bin Al Hussein Karak 2386370Prince Rashid bin Al Hassan Irbid 7100890Prince Zeid bin Hussein Tafiela 2242982Queen Rania Hospital Amman 5804804
Ministry of Health Hospital Name Site Phone number Al-Basher Hospital Amman 4775111Abu Obaida Hospital Irbid 026570018Hussein Hospital Balqa 053551140Karak Hospital Karak 032386190Ruweished Hospital Mafraq 026292183Maan Hospital Maan 032132222Mafraq Hospital Mafraaq 026231234 Princess Iman Balqa 053584934AL-Zarqa’a Hospital Zarqa 05398332Jamel Altotnge Amman 4020096Yarmouk Hospital Irbid 027585980Princess Raya Irbid 026521666Ghor Safi Hospital Karak 032302436Prince Hamza Hospital Amman 5053826Queen Rania Al-Abdullah Maan 032150636Ramtha Hospital Irbid 027384384Iman Hospital / Ajloun Ajloun 026421914Princess Salma Hospital Madaba 053207104 AL-Dleal Hospital Zarqa 053825145Jerash Hospital Jerash 026351114Maaz bin Jabal Irbid 026587011Princess Basma Teaching Irbid 027275555Nadeem Hospital Madaba 053244008 AL-Shoneh AL-Janobyeh Balqa 053581364Prince Hussein Balqa 5351731Aqleh Hospital Amman 4642441AL-Ahli Hospital Amman 5664164AL-Dleel Hospital Zarqa 053825144 Rom-ALkatholik Hospital Irbid 027257900AL Haya Hospital Amman 4391111Prince Faisal Hospital Zarqa 053740251Al-Qawasmi Hospital Irbid 027243401

9
University Hospitals
Hospital Name Site Phone numberJordan University Hospital Amman 5353666King Abdullah University Irbid 027200600
Private Sector Hospitals
Hospital Name Site Phone Number
Islamic Hospital Amman 5101010
Jordan Hospital Amman 5608080
AL-Qouds Hospital Amman 4387181
Shmeisani Hospital Amman 5607431
Al Khalidi Hospital Amman 4644281
Ibn al-Haytham Hospital Amman 5205555
Arab Medical Center Amman 5921199
AL Mowasah Hospital Amman 4896842
Dr. Ahmed Hamayda Amman 4785555
AL Esteqlal Hospital Amman 5652600
Lozmelah Hospital Amman 4624345
AL Isra Hospital Amman 5300300
Marka Islamic Amman 4893855
Palestine Hospital Amman 5607071
Philadelphia Hospital Amman 5854801
Tla Al Ali Hospital Amman 5339008
AL Hanan Hospital Amman 4750800
Amman Surgical Hospital Amman 4641261
Italian Hospital / Amman Amman 4777101
Jordanian Red Crescent Amman 4779131
Italian Hospital / Karak Karak 032355345
AL Mahaba Hospital Madaba 053245541
AL Hekma Hospital Zarqa 053990990
AL Razi Hospital Zarqa 053744167
Jabal Al-Zayton Hospital Zarqa 053655555
Qaser Al-Shibib Hospital Zarqa 053987995Irbid Specialty Hospital Irbid 027103100Bin Al-Nafees Hospital Irbid 027102100Al-Najah Hospital Irbid 027100170Al-Rahbat Al-Wardyeh Irbid 027102011Islamic Irbid Hospital Irbid 027273111 AL-Rasheid Hospital Amman 4777444Islamic Irbid Hospital Irbid 027273111 Dar AL-Salam Hospital Amman 5850008
10
Table of Contents
pageList of Abbreviations 11
List of tables 12
List of Figures 13
Part One: 15
Introduction 16
Geography 17
Population 17
Jordan Renal Registry 25
Methodology 29
Part Two: 31
Dialysis Units in Jordan 31
Part Three: 33
ESRD Patients in Jordan 33
Trend of ESRD patients in Jordan during (2008-2013)
Part Four 50
Incidence of ESRD Patients
Part Five: 57
Pediatric ESRD 57
Part Six: 62
ESRD patients among Non-Jordanians,
Part seven: 64
ESRD Mortality
References 67

11
List of Abbreviations
ESRD End Stage Renal Disease
MOH Ministry of Health
CDC Centers of Disease Control and Prevention
WHO World Health Organization
BRFSS Behavioral Risk Factors Surveillance System
NCD Noncommunicable disease
PHH Prince Hamza Hospital
DOS Department of Statistics (Jordan)
OR Odds ratios
BMI Body mass index
CI Confidence Interval
PS Private Sector
CKD Chronic Kidney Disease
GFR Glomerular Filtration Rate
RRT Renal Replacement Therapy
RMS Royal Medical Services
PPM Prevalence per Million Populations
ASIR Age Specific Incidence Rate

12
List of tables
Table N. Description Page
Table (1) Estimated Population of Jordan 2013 19
Table (2) Population distribution by Governorate and gender, Jordan 2013 20
Table (3) Selected Demographic, Socio-economic and Health Indicators 2013 21
Table (4) Distribution of ESRD according to age groups & gender and Prevalence Rateper million (PPM), 2013
36
Table (5) Distribution of ESRD patients according to marital status and gender 2013 38
Table (6) Distribution of ESRD patients by employment status and gender,2013 39
Table (7) Distribution of ESRD patients by type of insurance and gender 2013 40
Table (8)Distribution of ESRD patients by Governorate and prevalence per million populations (PPM)
41
Table (9) Distribution of primary causes of ESRD for the year 2013 42
Table (10) Prevalence of co-morbidity and some risk factors with ESRD 43
Table (11) Distribution of ESRD patients by fitness for transplantation 46
Table (12) Causes of unfitness for transplantation 46
Table (13) Priority level for patient candidate for transplant 48
Table (14) Prevalence of Hepatitis B and C in ESRD patients 49
Table (15) Distribution and ASIR of ESRD cases by gender and age group Incidence 2013 50
Table (16) Primary causes of ESRD for the year 2013 - Incidence 53
Table (17) Causes of ESRD in Pediatric patients 2013 59
Table (18) Distribution of ESRD patients among Non-Jordanians according to age groupsand gender, 2013
66
13
List of Figures
Figure N. Description Page
Figure (1) Map of the Hashemite Kingdom of Jordan 18Figure (2) Population Pyramid – Jordan 2013 19Figure (3) Distribution of dialysis units by health sector, Jordan 2013 31Figure (4) Distribution of Dialysis Machines by Health Sector, 2013 32Figure (5) Number of prevalent ESRD patients in Jordan during (2008-2013) 33Figure (6) International comparison of prevalence rate of Hemodialysis (PPM) 2013 34Figure (7) Distribution of ESRD patients by gender 35Figure (8) ESRD cases according to age groups and gender 37Figure (9) Distribution of ESRD cases less than 19 years and over 60 years 37
Figure (10) Distribution of prevalent ESRD patients by Health sector,2013 39Figure (11) Distribution of ESRD patients according to Blood group 44Figure (12) Distribution of ESRD patients by type of Dialysis 44Figure (13) Distribution of Hemodialysis patients by number of sessions /week 45Figure (14) Causes of unfitness for transplantation 47Figure (15) Distribution of fitness of ESRD patients by Priority level for Transplantation 47Figure (16) Distribution of ESRD patients by availability of a donor 48
Figure (17) Distribution of ESRD cases according to age groups and gender 2013 51
Figure (18) Distribution of ESRD patients by health sector, 2013 52
Figure (19) Distribution of ESRD patients by gender, 2013 52
Figure (20) Distribution of ESRD patients by Nationality 2013 54
Figure (21) Distribution of ESRD patients by type of Dialysis, 2013 54
Figure (22) Distribution of ESRD patients by fitness for transplantation 55
Figure (23) Distribution of fitness of ESRD patients by Priority level for transplantation 2013 55
Figure (24) Distribution of mortality in ESRD patients 2013 56
Figure (25) Distribution of ESRD pediatric patients by gender 57
Figure (26) Distribution of Pediatric patients according to type of Dialysis 58
Figure (27) Distribution of pediatric patients according to age groups and gender 2013 60
Figure (28) Distribution of Pediatric ESRD by fitness for transplantation 60
Figure (29) Distribution of mortality in Pediatric patients 61
Figure (30) Distribution of mortality in ESRD patients 62
Figure (31) Distribution of mortality in ESRD patients according to gender 63
Figure (32) Distribution of mortality in ESRD patients by age group and gender 63
Figure (33) Distribution of ESRD patients by Nationality 64
Figure (34) Distribution of ESRD patients among Non-Jordanians by gender 65
Figure (35) Distribution of ESRD patients among Non-Jordanians according to age groupsand gender 2013
66


15
Part one
Introduction
Geography
Population
Health Status
Jordan Renal Registry
Methodology

16
Part One
Introduction
ESRD remains one of the leading causes of morbidity and mortality in Jordan. As life expectancy
increases in Jordan, the proportion of elderly population is expected to increase; this will lead
to higher prevalence of non-communicable diseases including renal diseases that may lead
eventually to ESRD, although chronic kidney disease sometimes results from primary diseases
of the kidneys themselves, diabetes and hypertension remained the major causes of ESRD.
Chronic kidney disease could not be prevented in most circumstances, but screening and
control of chronic diseases mainly diabetes mellitus and hypertension will decrease the
occurrence of renal complications of these diseases with resulting reduction of ESRD.
In the ESRD Registry we are collecting all data relevant for ESRD patients and create
a data base for the problem in Jordan, this enables us to determine the incidence,
prevalence, epidemiologic characteristics of patients including age, sex, governorate; it
also enables us to determine mortality and burden of the disease in our country. The
Registry provides researchers and scientists with data that help in conducting further
research on ESRD, and present important data, figures and statistics for decision
makers for the process of planning and implementing preventive programs for ESRD.
With great pleasure we present our 6th annual ESRD report, including prevalence and
the incidence of ESRD in Jordan for the year 2013, reviewing the ongoing changes in the
ESRD Registry, using the data to give direction to renal-control planning and programs
in the fields of prevention, screening, treatment, and to monitor and evaluate the impact
of these programs. This report will help understand the ESRD incidence in Jordan and
thus will enhance prevention and control efforts of the National Renal Registry Program.
The team involved in producing this report had made great efforts to present the graphics and
tables in a clear, very concise and user-friendly way hoping this will facilitate their utilization
and comprehension.

17
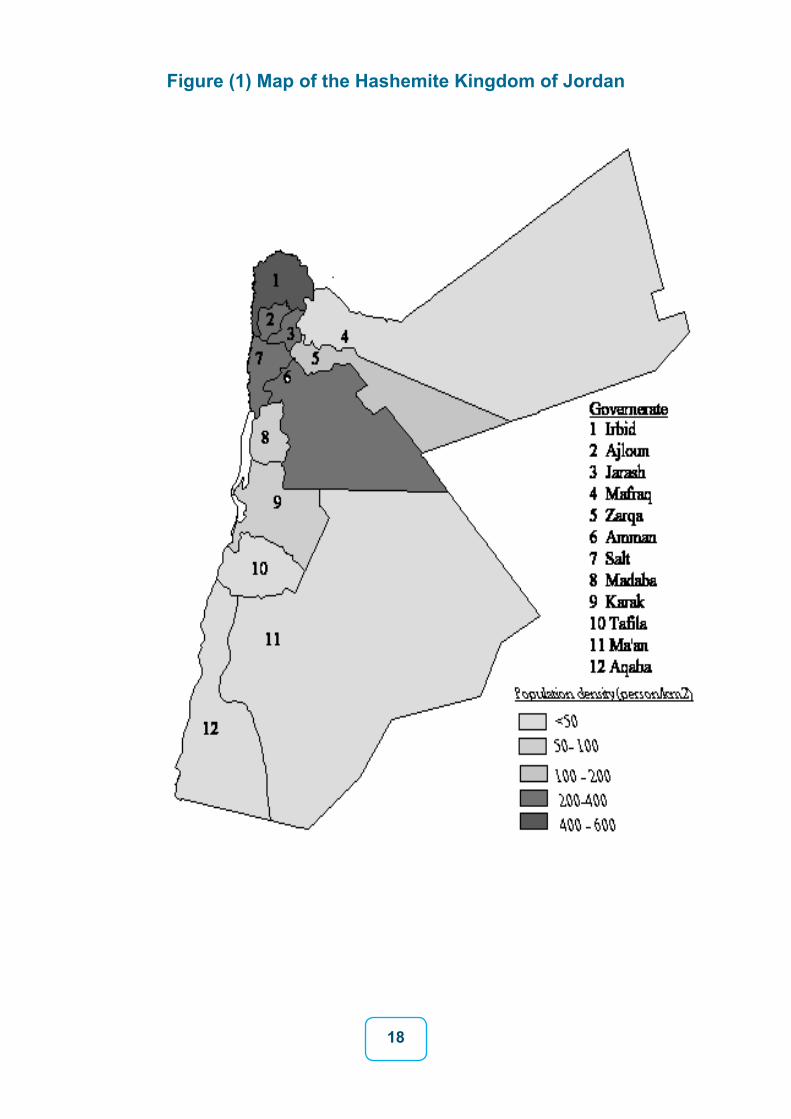
Geography
Jordan is located in the Middle East, between Latitudes 29-33 north and between Longi-
tudes 35-39 east, extending about 500 Kilometers from North to South, it is bounded in the
North by Syria, East by Iraq and Saudi Arabia, South also by Saudi Arabia and West by
Palestine Authority. The total surface area is 89318 Km2. Out of the total area, 75% is des-
ert along the Eastern part of the country. Mountains height ranged between 1100 – 1854
meters above sea level. The Dead Sea area is the lowest area in the world and it is around
416 meter below sea level.
The climate of the country as a whole is moderate, there are four seasons. The temperature
ranged from 0°C in winter to 38°C in summer. Jordan is divided into three regions (Middle,
Northern and Southern) and twelve governorates..
Population
The estimated population of Jordan in mid-2013 was 6530000 millions. Including 3366000
males and 3164000 females (male: female ratio 106: 4). (Department of Statistics Jordan,
2013). About 12.7% of the population under the age of 5 years, 37.3% under the age
of 15 years and 59.4% of the population at the age 15-64 years, only 3.3 % of the total
population above the age of 65(Sex Ratio in 2013: 106.4 males for 100 females).Table (1)
and figure (2) show the age distribution of Jordan population, 2012 (Jordanian Population
Pyramid ).Table (2) shows the population distribution of Jordanians by governorates and
gender, which is used to calculate incidence rates for different regions. Jordan divided into
three regions: each region consists of four governorates. The Central region (Amman,
Balqaa, Zarqa, and Madaba) constitutes about 62.8% of the total population with
population density of (249.7) person per Km2. North region includes (Irbid, Mafraq, Jarash,
Ajloun) which constitute 27.8% of the population with a population density of (55) person
per Km2. South region includes (Karak, Tafila, Ma’an, Aqaba) which constitutes 9.4% of the
population with a population density of 11.7 per Km2
18
Figure (1) Map of the Hashemite Kingdom of Jordan

19
Table (1) Estimated Population of Jordan 2013
Gender age group
Male Female TotalN % N % N %
0-4 427485 12.7 405300 12.8 832785 12.75-9 422095 12.5 400880 12.7 822975 12.6
10-14 401900 11.9 379680 12.0 781580 11.915-19 368915 10.9 347720 11.0 716635 11.020-24 358485 10.7 333170 10.5 691655 10.625-29 307650 9.1 276855 8.7 584505 8.930-34 265915 7.9 245520 7.7 511435 7.835-39 215425 6.4 199015 6.3 414440 6.340-44 155720 4.7 149975 4.7 308850 4.745-49 111750 3.3 106630 3.4 218380 3.350-54 82805 2.5 81320 2.6 164125 2.555-59 71360 2.1 74040 2.3 145400 2.260-64 66645 2.0 59800 1.9 126445 1.9+65 106695 3.2 104095 3.3 210790 3.2Total 3293000 100.0 3164000 100.0 6530000 100.0
Figure (2) Population Pyramid – Jordan 2013
Female Male
85+80-8475-7970-4065-6960-6455-5950-5445-4040-4435-3935-3630-3425-2920-2415-1910-14
5-90-4
420 315 210 105 105 210 315 4200

20
Table (2) Population distribution by Governorate and gender, Jordan, 2013
gender
Governorate
Male Female Total
N % N % N %
Amman 1300000 38.6 1228500 38.8 2528500 38.7
Balqa 227200 6.7 205800 6.6 437500 6.7
Zarqa 503400 15.0 469500 14.8 972900 14.9
Madaba 84100 2.5 79200 2.5 163300 2.5
Central region 2114700 62.8 1987500 62.8 4102200 62.8
Irbid 595300 17.7 567000 17.9 1162300 17.8
Mafraq 159100 4.7 147800 4.7 306900 4.7
Jarash 100800 3.0 95100 3.0 195900 3.0
Ajloun 76400 2.3 73800 2.3 150200 2.3
North Region 931600 27.7 883700 27.9 1815300 27.8
Karak 128900 3.8 125800 4.0 254700 3.9
Aqaba 79200 2.4 63100 2.0 142300 2.2
Maan 65000 1.9 59100 1.9 124100 1.9
Tafeilah 46600 1.4 44800 1.4 91400 1.4
South Region 319700 9.5 292800 9.3 612500 9.4
Total 3366000 100.0 3164000 100.0 6530000 100.0

21
Table (3) Slected Demographic, Socio-economic and Health Indicators 2013
Indicators 2013
Population 2013 6.530.000
Population Density (Person per km2) 73.5
Population Growth Rate 2.2 %
Rate of Natural Increase 2.1%
Population Doubling Time (Year) 31.5
Population Less Than 15 Year of Age 37.3%
Percentage of Population Age 15-64 Years 59.4%
Percentage of Population Age 65+ 3.3
Dependency Ratio 68.2
Percentage of Urban Population 82.6%
Percentage of Rural Population 17.4%
Total Fertility Rate (Women 15-49 Years) 3.5
Urban 3.8
Rural 4.0
Sex Ratio 106.4
Total Households (000) 1,157.2
Crude Marriage Rate (Per 1000 Population) 10.9
Crude Divorce Rate (Per 1000 Population) 2.9
Singulate Mean Age at First Marriage (Year) 28.4
Male 29.4
Female 25.8
Jordanian Married of Total Population 15+ 55.4
Male 54
Female 56.8
Average Household Size (person) 5.4
Population Median Age (year) 20.3
Crude Birth Rate (Per 1000 Population) 27.6
Crude Death Rate (Per 1000 Population) 5.8
Infant Mortality Rate (Per 1000 Live Births) 17.0
Under Five Mortality Rate (Per 1000 Live Births) 28.0
Life Expectancy at Birth (Year) 74.4
Male 72.7
Female 76.7
Unemployment Rate (%) 12.2
Male 10.4
Female 19.9
22
Health Status
Morbidity Data
Jordan is witnessing an epidemiologic transition, which is characterized by rapid decline
in mortality from infectious diseases coupled with an increase of non-communicable
diseases (NCDs). Unhealthy diet, Physical inactivity, obesity and smoking are major
determinants of NCDs and represent major risk factors for the development of
cardiovascular diseases, cancer and diabetes. According to epidemiologic surveys/
Behavioral Risk Factors Surveillance survey (BRFSS) which have been conducted by
Ministry of Health over the last few years; 2002, 2004 and 2007 among those aged 18
years and above revealed that determinants and levels of risk factors for NCDs are rising.
The Behavioral Risk Factor Surveillance Survey, 2007 showed the following:
- Diabetes represent major health problems; reported to affect more than 16% of adults,
impaired glucose tolerance (IGT) was found in an additional 24%, bringing the total preva-
lence of glucose tolerance abnormalities to over 40 % for 18 years and above.
- The prevalence rate of hypertension was 25.6 %.
- The prevalence rate of hypercholesterolemia was 36 %.
- The prevalence rate of HDL-C (low level) was 33.8 %.
- The prevalence rate of high LDL-C was 24.2 %.
-The prevalence rate of high Triglyceride was 48.8 %.
- The prevalence of overweight was 30.5%, (BMI 25-29.9 Kg/m2) and the prevalence of
obesity was 35.9 %,( BMI 30 Kg/m2 and more).
- Smoking is a major problem, with more than 49.6% of adult men and 5.7% of women
smoking regularly.
The last 16th annual report for the year 2011, JCR registered 6971 cancer cases, of these
4675 (67.1%) were among Jordanians and 2296 (32.9%) were among non-Jordanians.
The crude incidence rate of all cancers among Jordanians was 74.8 per 100,000 populations
(68.1 for males and 81.9 for females).
The male to female ratio was 0.88: 1.

23
Mortality data
It provides information on annual death rates of a population. It also provides information
on specific diseases in terms of clinical and public health perspectives. Major achievements
have been made during the last several decades. The Infant Mortality Rate (IMR) fell from
135 in 1960 to 17 deaths per 1,000 live births in 2013. This impressive decline occurred as a
result of focused maternal and child health activities, increased vaccination coverage rates,
improvements in education, birth spacing, sanitation and access to safe drinking water and
improvement of general conditions.
By law, all deaths must be registered in Jordan. However, registration is not universal and
death certification by cause is not completely accurate. According to Jordan Mortality Data in
2011, cardiovascular diseases accounted for about 37.6 % of deaths for both sexes. Cancer
was the second leading cause of death accounting for 14.3 % of total deaths, while external
causes of mortality were the third leading cause responsible for 8.6 % of total deaths.
While diseases of Genitourinary system constitute about 2.5% total deaths, 366 patients
(91%) of these deaths were due to renal failure (acute and chronic renal failure) according
to mortality report in 2011 (5).

24
When it is right, no one remembers.
But when it fails, all have to remember”
It is described as a small- sized, light-weighted, bean- shaped but a smart organ. Some
consider it as the secretary of the body as it deals with each inbox and outbox in the body.
Its dysfunction may affect the functions of other organs and systems. It may be affected
by dysfunctions of other organs and systems. When it fails, whether acutely or chronically,
this may manifest as multiple signs and symptoms relating to multiple systems in the body.
So the patient of kidney failure is considered as all patients in one. As a consequence, the
Nephrologists must also be all physicians in one.
In the past Stewart Cameron said,” for those who have chosen a career in Nephrology there
can be no better basic moto than to strive to be a person with some technical skill, a broad
spectrum of scientific knowledge, and with those personal characteristics of warmth and
humanity that serve to cement the science of medicine to the art of medicine.
Kidneys are the first and so far the only organs whose function can be replaced by
a machine. Kidney Failure can be acute, called Acute Kidney Injury (AKI) or chronic,
called Chronic Kidney Disease (CKD).
When patients of Chronic Kidney Disease (CKD) have reached stage 4 CKD i.e. Glomerular
Filtration Rate (GFR) < 30 ml /min / 1.73 m2, ideally they are under a Nephrologists’ care.
Stage 5 CKD i.e. GFR is < 15ml/min /1.73 m2, is called dialysis stage. Renal Replacement
Therapy “RRT” means of dialysis and transplantation.
Worldwide, the machine of dialysis had served millions of ESRD patients.

25
Jordan Renal Registry
Historical development of Nephrology and dialysis
1840-Pierre Priory defined uremia
1861-Thomas Graham coined the term dialysis for the first time
1913- John Abel invented first dialysis apparatus, first animal dialysis was done.
1928 –George Has –first human dialysis was done.
1943-Dr.Willem Kolff introduced Kolff rotating drum dialyzers.
1948-Waters and Beall –first successful human dialysis.
1950- Introduction of dialysis into clinical practice.
The subsequent successful development of a technique to create an adequate arterio-venous fistula in 1972 permitted the rapid growth of dialysis programs. Equipment has been developed to faster home-care hemodialysis and chronic ambulatory peritoneal dialysis.
Technical advances in hemodialysis followed the use of bicarbonate dialysate, more biocompatible membranes, membranes of higher porosity and ultra filtration.
The numbers of patients reaching to ESRD continue to increase annually, and this situation is leading to challenge to the existing system of RRT.
Causes of ESRD are multiple; the most common ones are diabetes mellitus and hypertension. Unless some form of RRT is available, ESRD is eventually fatal. Mortality in patient with ESRD is high.
However, the cost of RRT represents a great social burden, due to the evolving health care environment, growing elderly population, renewing and innovating healthcare technologies, increasing expectations of the population and the dilemma of economic constraints. There should always be a balance between the three key factors of a health care system: access to healthcare, quality of health care and the cost.
In conclusion, ESRD is a growing disease all over the world, it is caused by many etiologies, diagnosed by physicians, and must be cared by the Nephrologists.
New awareness programs of the disease must be established, and new strategies toward
the burden of it must be started. It needs global collaboration and teamwork schedule.

26
Status of “Renal Replacement Therapy” in Jordan
Proudly speaking, Jordan is one of the first countries in the Middle East that early started
programs of dialysis and kidney transplantation. There are many renal dialysis units all over
the country, belonging to Ministry of Health, Royal Medical Services, University hospitals
and Private Sector. In addition, there are many kidney transplant centers in all sectors deal-
ing with the best medical care.
Jordan has approved to be one of the pioneer countries in Nephrology and its modalities.
Jordan achieved many in the field of nephrology like:
1968- the first dialysis was done at the Military Hospital “the Main Hospital” in Marka area
– Amman.
- The first dialysis machine used in Jordan was”TRAVENOL” machine type.
- The first kidney transplantation done in Jordan was on 18/05/1972 at the same main
Military Hospital. It was the first to be done in the Middle East.
1981- The establishment of renal dialysis unit at Jordan university Hospital. The machine
type was REDY “Sorbs system”. It was portable, moving to Khaldi and Islamic Hospitals.
1982- The first renal dialysis Unit was established in private sector, it was at Al-Khaldi
Hospital.
1984- The first kidney transplantation was done in private sector at Islamic Hospital, then at
Al- Khaldi Hospital.
2009- The first kidney transplantation in Jordanian public hospital was done at Prince
Hamza Hospital in October 2009 according to The Jordanian National Program Of Renal
Transplantation of the JMOH.

27
So dialysis was introduced in Jordan in 1968. Ever since, there has been a continuous
expansion of the dialysis centers in terms of the geographic coverage and capacity. The
economic prosperity helped building the services all over the country.
Modern hemodialysis machines were installed in the vast majority of units, which allowed
for the performance of bicarbonate dialysis, controlled ultra filtration, and sodium profile
modeling. Also a wider choice of biocompatible dialyzers has become available during the
last few years.
Recently, there has been an emerging concern about the projection of the increasing
number of patients on dialysis and the future cost. Therefore, close observation of the
development of dialysis has been a demand of the Jordan center for organ transplantation.
Preparing annual reports about all the modalities of RRT has become a demand activity.
National ESRD Registry, which is based on center and patient forms, is a useful tool
to assess the quality of dialysis services and activities used to improve the adequacy of
hemodialysis.
Jordan has had a growing number of persons developing CKD leading to ESRD. It is
important to have a national registry in order to define the cause of ESRD, and to be able
to perform (Inter) National comparisons in renal epidemiology.
Such a registry will monitor the causes, incidence, and prevalence of ESRD and any
emerging trend.
A national ESRD registry will allow the determination of the burden of disease as well as
planning and policy formulation in the health care sector.
As the Registry develops, data will become available for patients with ESRD, as is reported
here.
Finally, it is a great achievement to establish the National ESRD Registry, a new achievement
in renal events in Jordan.

28
National Registry of End Stage Renal Disease:
The National Registry of End Stage Renal Disease was created in May 3 rd, 2007 under the
jurisdiction of the Ministry of Health by the order of his Excellency the Minister of Health.
Objectives of the National Registry of End Stage Renal Disease:
· Establish a national database system about patients of ESRD.
· Determine the burden of that disease, on country basis.
· Determine governmental payment on dialysis.
· Provide data about patients and their suitability to be transplanted, on a basis of priority.
· Stimulate beginning studies and researches about ESRD.
· Improve facilities of diagnosis and treatment for ESRD patients. Moreover, train
dialysis technicians and national registry employees.
Action plan of National Registry of End Stage Renal Disease:
* Prepare special form for the notification of ESRD from all hospitals and updated annually
(annex1).
* Training workshops for all focal point working in dialysis units about how to fill this form
and how and when to send it to the national registry through either passive or active
method of surveillance.
* Good Communication with all dialysis units in the hospitals from all sectors to complete
and improve documentation in this form.
* Collection of all data about ESRD patients and all renal dialysis units in Jordan, through
filling the prepared forms by dialysis technicians and attending Nephrologists.
* Enter data about those patients and dialysis units into a computerized software program.
* Analysis of the data, reporting the results and then delivering it to specialized people to
stratify and build special schedules about the of ESRD.

29
Methodology:
The National Registry of End Stage Renal Disease was created in 2007 and supported
by the Ministry of Health. It is a database-system that collects data and information
about almost all patients undergoing Renal Replacement Therapy (RRT), i.e. either
dialysis (hemodialysis and peritoneal dialysis) or Kidney transplantation.
This is the sixth national ESRD Registry report. Data were received from all (76) dialysis
units in Jordan. It is assumed that those undergoing treatment in these units are represent
the number of all ESRD cases , because all cases are treated on the expense of the
government and even the patients undergoing home peritoneal dialysis.
Data about ESRD patients who are receiving long term (RRT) during 2013 were collected
from all dialysis units in the hospitals and then analyzed using special software statistical
analysis( SPSS).
Two questionnaires (forms) used for data collection from hospitals. The first one is for the
dialysis units: including number of beds, type of insurance of patient, nationality (Annex1).
The second form is for the patients, this form consist of demographic data, clinical data,
source of treating facility, follow up and vital status of the patients and all these data will
entered on special software for ESRD patients (Annex2). Patients who are not on Renal
Replacement Therapy (RRT) and those who only received urgent dialysis or died shortly
afterwards (less than 90 days) were not included in this report.

30
Methods of Data Collection:
Data was collected from all renal dialysis units in Jordan, through the following methods:
two types of data collection methods were applied:
1. Passive Data Collection: in this system forms filled by dialysis units technicians and send
to national renal registry - MOH/NCDs Directorate.
2. Active Data Collection: In this system the head of Renal Registry Unit visited the dialysis
units and fills the forms on the unit and complete all the variables from medical record
of those patients. This to ensure more complete and accurate data
All forms were reviewed at the Renal Registry Unit and filtered and checked for any
duplication and also document follow up data if the patient still alive or dead
cause of death dates of last dialysis.
Data entered to special software designed for data of renal patients, Data analysis was done
by using statistical package for the social sciences SPSS version 17.0.
Incidence and prevalence calculations in this report are based on the estimation of the na-
tional population by Department of Statistics (DOS) 2013.

31
Part Two
Dialysis Units in Jordan
By the end of 2013, there were 76 working Dialysis Units distributed all over the country.
32 units (42%) administered by Ministry of Health (MOH), 8 units (10 %) administered by
Royal Medical Services (RMS), 2 units (3%) administered by university hospitals: one
administered by Jordan University Hospital, one by King Abdullah University Hospital
(KAUH) and 34 units (45%) administered by Private Sector (PS), (Figure 3).
Figure (3) Distribution of dialysis units by health sector, Jordan 2013.

32
Distribution of Dialysis Machines by Health Sector, Jordan 2013
The total number of dialysis machines (895) in all units was distributed as followed: 362
(40%) machines in MOH units, 77(9%) machines in RMS, 34(4%) machines in universities
hospitals and 422 (47%) machines in private sector hospitals, (Figure 4).
Figure (4) Distribution of Dialysis Machines by Health Sector,2012
The focal points in all 76 Dialysis Units filled the special form of data collection and send
it to National ESRD Registry located in the Ministry of Health. (Annex1), data about ESRD
patients was received from all hospitals.

33
Part three
ESRD patients in Jordan
Prevalence of ESRD patients in Jordan (2013)
The total numbers of patients treated and registered in the Jordan Renal Registry by the end of 2013 was ( 4272) patients; of them 4097 were Jordanians (95.9%) and 175 were non Jordanians (4.1%). This part of the report only include Jordanian patients –prevalence 2013The number of Jordanian patients that registered in ESRD and treated in hospitals for the year 2013 was 4097 patients, while the number of new cases of ESRD for the year 2013 was 728 patients , out of them 650 patients (89%) were Jordanians,78 (11%) were nonJordanians.The number of Jordanian ESRD patients for the year 2013 was decreased due to kidney transplant that done where (380) Jordanian patients did kidney transplant in our hospitals in Jordan for the years from (2011-2013), also after excluding the number of deaths for each year from 2008-2013 as shown in the figure below. For this year we improve surveillance system for ESRD patients from 2008-2013 from all ESRD units in all governorates we did both active and passive surveillance for vital status for those patients from civil registration data and if the patients were alive or dead.
Figure (5) Number of prevalent ESRD patients in Jordan during ((2008-2013)

34
International comparison of prevalence rate of Hemodialysis ESRD patients
Figure (6) shows the International comparison of prevalence rate of Hemodialysis
patients Per Million Population (PMP) in Jordan and other countries in 2013. The
overall Prevalence Per Million Populations in Jordan in 2013 is (627.4/1,000,000)
compared with other countries.
Figure (6): International comparison of prevalence rate of Hemodialysis (PMP)2013
PMP: per million population
Prevalence of ESRD Patients in Jordan, 2013
The total number of ESRD patients during the year 2013 was 4097 patients who are
receiving hemodialysis or peritoneal dialysis in the hospitals from all sectors.
1. Socio demographic characteristics of ESRD prevalent patients:
Figure (7) shows the distribution of ESRD prevalent patients who attended renal
dialysis units in all Jordanian hospitals during the year 2013 according to gender. The
number of patients treated in the Dialysis Units was 4097 patients , out of them 2344
were male patients which accounted (57%) and 1753 were female patients accounted
( 43% ),with male to female ratio 1.3:1.

35
Figure (7) Distribution of ESRD patients by Gender
Distribution of ESRD patients according to age groups and gender, 2013
Table (4) shows the distribution of ESRD patients according to the age groups and gender,
the mean age of patients was (51) years, (51 years for males and 51.5 years for females).
The median age of patients was (53) years, (53 years for males and 54 years for females).
Table (4) also shows the distribution of ESRD cases by prevalence rate per million
populations (PPM), the overall prevalence per Million Populations in Jordan was
(627.4/1,000,000).

36
Table (4) Distribution of ESRD according to age groups and gender and Prevalence Rate per million (PPM), 2013
gender
Age groupMale Female Total
N % N PPM N PPM %
0-4 9 21.1 7 17.3 16 19.2 0.4
5-9 19 45.0 12 29.9 31 37.7 0.8
10-14 23 57.2 34 89.5 57 72.9 1.4
15-19 59 159.9 36 103.5 95 132.6 2.3
20-24 85 237.1 75 225.1 160 231.3 3.9
25-29 130 422.6 88 317.9 218 373.0 5.3
30-34 127 477.6 104 423.6 231 451.7 5.6
35-39 173 803.1 95 477.4 268 646.7 6.5
40-44 192 1208.5 126 840.1 318 1029.6 7.8
45-49 216 1932.9 154 1444.2 370 1694.3 9.0
50-54 242 2922.5 161 1979.8 403 2455.4 9.8
55-59 258 3615.5 166 2242.0 424 2916.1 10.4
60-64 238 3571.7 189 3160.5 427 3377.0 10.4
65+ 571 5351.7 505 4851.3 1076 5104.6 26.3
Total 2342 695.8 1752 553.7 4094 627.4 100.0
*PMP: Per Million Populations

37
Figure (8) ESRD cases according to age groups and gender-2013
Figure (9) Distribution of ESRD cases by age group-2013

38
Distribution of ESRD patients according to marital status and gender
Table (5) shows that the majority of ESRD patients were married (71.2%), (married males
78.9% and married females 61%), while (19.4%) of the ESRD patients were singles (single
males 18.4% and single males 20.7% ),( 1.8%) of the patients were divorced .
Tables (5) Distribution of ESRD patients according to marital status and gender 2013
gender
MaritalStatus
Male Female Total
N % N % N %
Married 1849 78.9 1070 61.0 2919 71.2
Single 430 18.4 363 20.7 793 19.4
Divorced 38 1.6 272 15.5 310 7.6
Widow 25 1.1 50 2.8 75 1.8
Total 2342 57.2 1755 42.8 4097 100.0
Distribution of ESRD patients according to employment status and gender
Table (6) shows the distribution of the ESRD patients according to their employment status
for both genders. House wife’s accounted (67.7 %) of the females, (4.3%) of the patients
were employed either governmental or non-governmentally and military services, (14.0%)
were retired, and (3.8%) were students, (26.2%) of the patients were unemployed, missing
data about employment was (12.6%).
39
Table (6) Distribution of ESRD patients by employment status and gender, 2013
gender
Job
Male Female Total
N % N % N %
House Wife 0 0.0 1188 67.7 1188 29.0
Unemployed 842 36.0 232 13.2 1074 26.2
Retired 537 22.9 35 2.0 572 14.0
Private 347 14.8 18 1.0 365 8.9
Student 80 3.4 76 4.3 156 3.8
Employed 143 6.1 35 2.0 178 4.3
Military 42 1.8 7 0.4 49 1.2
Missing 351 15.0 164 9.3 515 12.6
Total 2342 57.2 1755 42.8 4097 100.0
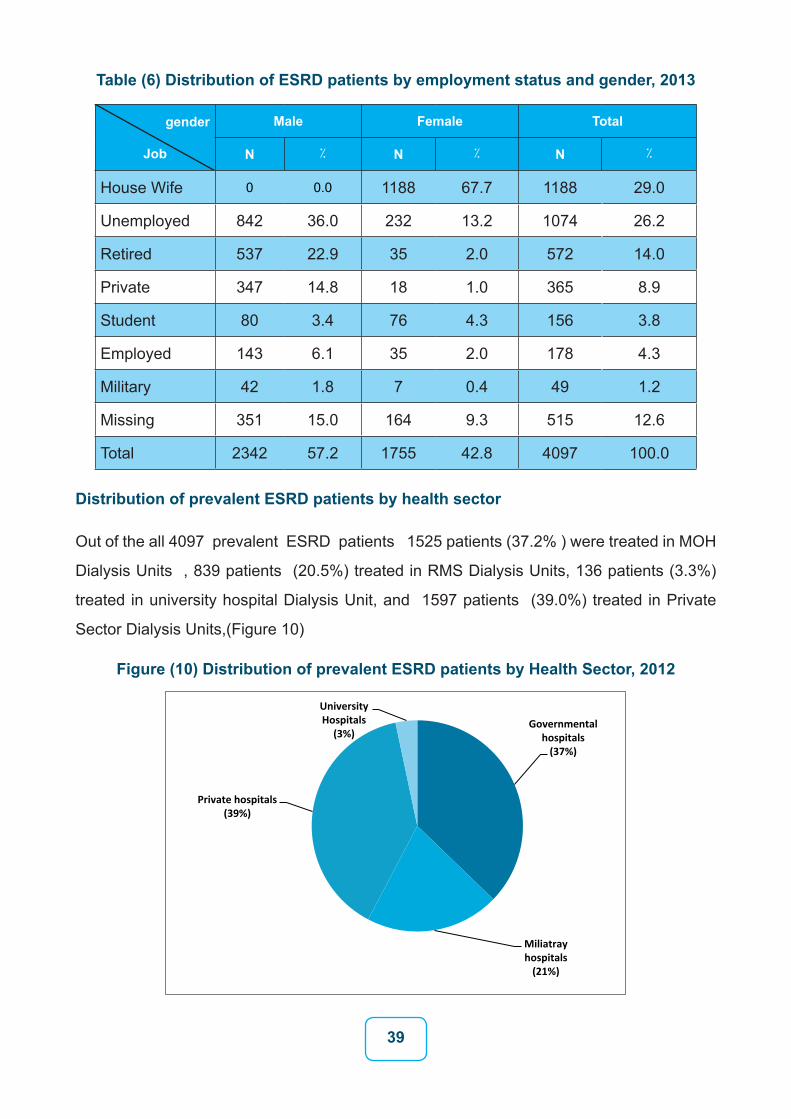
Distribution of prevalent ESRD patients by health sector
Out of the all 4097 prevalent ESRD patients 1525 patients (37.2% ) were treated in MOH
Dialysis Units , 839 patients (20.5%) treated in RMS Dialysis Units, 136 patients (3.3%)
treated in university hospital Dialysis Unit, and 1597 patients (39.0%) treated in Private
Sector Dialysis Units,(Figure 10)
Figure (10) Distribution of prevalent ESRD patients by Health Sector, 2012

40
Distribution of ESRD cases according to the type of insurance
Table (7) shows the distribution of ESRD patients according to insurance type. (97%) of
patients were insured by one of the various types of health insurance. (42.9%) of the patients
were insured by Kidney Patients Fund in health insurance directorate in Ministry of health.
Civilian (24.1%), Military (24.0%), Private (1.1%). only (1.4%) were not covered by any type
of insurance. Missing data regarding the insurance type accounts for (1.2) % of the cases.
Table (7) Distribution of ESRD patients by type of insurance and gender
gender
Insurance Type
Male Female Total
N % N % N %
Kidney patientsfund 1033 44.1 724 41.3 1757 42.9
Civilian 579 24.7 407 23.2 986 24.1
Military 514 21.9 468 26.7 982 24.0
Private 28 1.2 18 1.0 46 1.1
Universities 28 1.2 13 0.7 41 1.0
Others 101 4.3 77 4.4 178 4.3
No insurance 9 0.4 8 0.5 17 0.4
Missed 50 2.1 40 2.3 90 2.2
Total 2342 57.2 1755 42.8 4097 100.0

41
Distribution of ESRD patients by Governorate
The overall prevalence per Million Population in Jordan is (627.4/1,000,000), the highest
prevalence was found in Madaba governorate (728.7/1,000,000) followed by Amman gov-
ernorate (714.7/1,000,000) Zarka governorate (631.1/1,000,000) and Ajloun governorate (
625.8 / 1,000,000 ) Table (8).
Table (8) Distribution of ESRD patients by Governorate and prevalence per million populations (PPM)
gender
Insurance Type
Male Female Total
N % N % N % Rate
Amman 1051 44.9 756 43.1 1807 44.1 714.7
Zarqa 346 14.8 268 15.3 614 15.0 631.1
Madaba 61 2.6 58 33.3 119 2.9 728.7
Balqa 141 6.0 118 6.7 259 6.3 592.0
Centra Region 1599 68.3 1200 68.4 2799 68.3 682.3
Irbid 405 17.3 267 15.2 672 16.4 578.2
Mafraq 75 3.2 63 3.6 138 3.4 449.7
Jarash 46 2.0 52 3.0 98 2.4 500.3
Ajluon 46 2.0 48 2.7 94 2.3 625.8
North Region 572 24.4 430 24.5 1002 24.5 552.0
Karak 88 3.8 65 3.7 153 3.7 600.7
Aqaba 25 1.1 24 1.4 49 1.2 344.3
Maan 29 1.2 13 0.7 42 1.0 338.4
Tafeile 29 1.2 23 1.3 52 1.3 568.9
South Region 171 7.3 125 7.1 296 7.2 483.3
* PMP: Per Million Populations
Number of total cases in Jordan as received from renal dialysis units are 4097

42
Distribution of ESRD prevalent patients by primary cause
Table (9) shows the main primary causes of ESRD:
The most common primary cause is Diabetes Mellitus (29.3%), followed by Hypertension
(25.1%), Diabetes Mellitus and Hypertension (12.2%), Glomerulonephritis (10.4%) and
then Polycystic kidney disease (2.7%) congenital causes(2.6 %), Infection (2.2%).
Table (9) Distribution of primary causes of ESRD for the year 2013
Primary cause of ESRDMale Female Total
N % N % N %
Diabetes Mellitus 625 26.7 475 27.1 1127 29.3
Hypertension only 635 27.1 395 22.5 1057 25.1
DM and Hypertension 375 16.0 305 17.4 696 12.2
Glomerulonephritis 242 10.3 184 10.5 436 10.4
Polycystic kidney 59 2.5 50 2.8 112 2.7
Congenital 64 2.7 43 2.5 110 2.7
Infection 55 2.3 36 2.1 93 2.3
Vesico uretric reflux 41 1.8 27 1.5 70 1.7
Drug 21 0.9 25 1.4 46 1.1
SLE 11 0.5 26 1.5 37 0.9
Neurogenic bladder 13 0.6 23 1.3 37 0.9
Stone 16 0.7 12 0.7 29 0.7
Alport syndrom 8 0.3 4 0.2 12 0.3
Nephrotic syndrom 7 0.3 5 0.3 12 0.3
FMF 5 0.2 2 0.1 7 0.2
Others 47 2.0 46 2.6 95 2.3
Unknown 118 5.0 97 5.5 220 5.4
Total 2342 100.0 1755 100 4097 100.0

43
Co-morbidity and some risk factors with ESRD
The data showed `the presence of other medical conditions coexisting with the ESRD
condition itself. The prevalence of co-morbidity in ESRD patients showed that (60.8%) of
patients were hypertensive, while cardiovascular diseases were found in (14.4%) of ESRD
patients. The prevalence of diabetes constitutes (37.5 %). The prevalence of smoking in
ESRD was (9.6%) and (5 %) of the patients had family history of renal diseases, Table
(10).
Table (10) Prevalence of co-morbidity and some risk factors with ESRD
Comorbidity Frequency %
Hypertension 2492 60.8
Diabetes 1538 37.5
Cardiac disease 592 14.4
Smoking 393 9.6
Urinary tract disease 305 7.4
Familial kidney disease 203 5.0
Malignanacy 41 1.0
Distribution of ESRD patients according to Blood Group
Figure (11) shows that approximately one third of the patients 1260 (31.0%), were blood
group A and 1320 (32.0%) were blood group O, 298 (7.0%), were blood group AB and
634(16.0%) were blood group B . Data was not available for 585 ESRD patients which
constitutes (14.0%), of the ESRD patients.

44
Figure (11) Distribution of ESRD patients according to Blood group
Distribution of ESRD patients according to type of Dialysis
Figure (12) shows that only 69 patients (2%) were treated by peritoneal dialysis, while
4028 patients (98%) were treated by hemodialysis.
Figure (12) Distribution of ESRD patients by type of Dialysis

45
Distribution of Hemodialysis patients by number of sessions /week
Figure (13) shows that 2965 patients (73.7%) underwent Hemodialysis thrice a week, 976
(24.2%) twice a week, 45 (1.1%) once a week, and 42 (1%) four times a week, the aver-
age duration of the every session is almost four hours
Figure (13) Distribution of Hemodialysis patients by number of sessions /week
Distribution of ESRD cases according to fitness for transplantation
Table (11) shows that 1689 (41.2%) from both genders were considered candidates for
transplantation, and 1874 not candidates for transplantation (45.7%) , no available data on
(534) (13%) of ESRD patients.

46
Table (11) Distribution of ESRD patients by fitness for transplantation
Candidate fortransplant
Male Female Total
N % N % N %
Yes 1039 44.4 650 37.0 1689 41.2
No 1015 43.3 859 48.9 1874 45.7
Unknown 288 12.3 246 14.0 534 13.0
Total 2342 100.0 1755 100.0 4097 100.0
Distribution of ESRD cases according to unfitness for transplantation
Table (12) and Figure (14) show that the main causes of unfitness for transplantation
were as followed: medical diseases 861 patients (45.9%) of all cases, age in 748 patients
(39.9%), malignancies in 36 patients (1.9%), while unknown causes for the cases were
134 patients (7.2%) of all patients.
Table (12) Causes of unfitness for transplantation
Causes Freqyency Percent
Medical causes 861 45.9
Age 748 39.9
Malignancies 36 1.9
Other causes 95 5.1
Missed 134 7.2
Total 1874 100.0
47
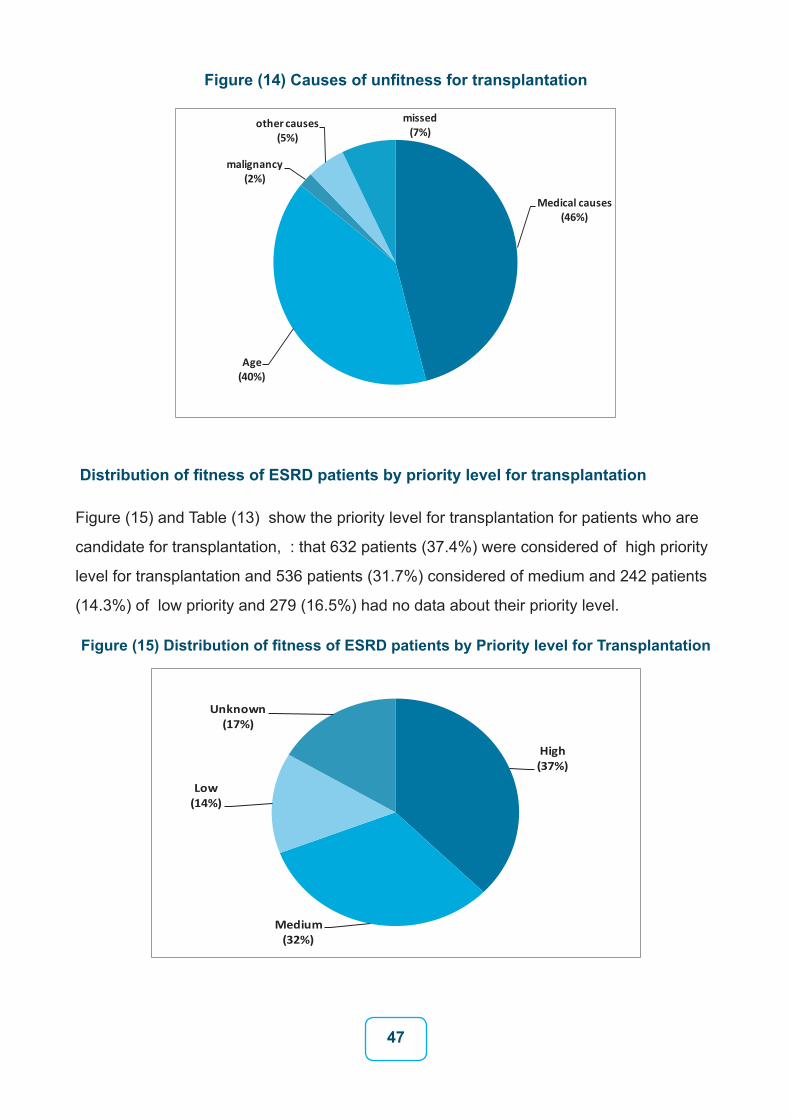
Figure (14) Causes of unfitness for transplantation
Distribution of fitness of ESRD patients by priority level for transplantation
Figure (15) and Table (13) show the priority level for transplantation for patients who are
candidate for transplantation, : that 632 patients (37.4%) were considered of high priority
level for transplantation and 536 patients (31.7%) considered of medium and 242 patients
(14.3%) of low priority and 279 (16.5%) had no data about their priority level.
Figure (15) Distribution of fitness of ESRD patients by Priority level for Transplantation

48
Table (13) Priority level for patient candidate for transplant
Priority levelMale Female Total
N % N % N %
High 412 39.7 220 33.8 632 37.4
Medium 325 31.3 211 32.5 536 31.7
Low 147 14.1 95 14.6 242 14.3
Unknown 155 14.9 124 19.1 279 16.5
Total 1039 100.0 650 100.0 1689 100.0
Distribution of ESRD cases according to availability of a donor
Figure (16) shows that 1309 patients (77.5%) had no available donor, and 313 patients
(18.5%) had available donor, 67 patients (4.0%) had no data about available donor, this
reflects the burden of ESRD in Jordan.
Figure (16) Distribution of ESRD patients by availability of a donor

49
Prevalence of Hepatitis B and C in prevalent ESRD patients
Table (14) shows the prevalence of hepatitis B and C in ESRD patients. (6.4 %) of the
cases had Hepatitis B and (2.5 %) had Hepatitis C.
Table (14) Prevalence of Hepatitis B and C in ESRD patients
Type of Hepatitis Hepatitis B Hepatitis C
Result Male Female Total % Male Female Total %
Positive 128 133 261 6.4 56 47 103 2.5
Negative 1934 1457 3391 82.8 2017 1543 3560 86.9
Missed 280 165 445 10.9 269 165 434 10.6
Total 2342 1755 4097 100.0 2342 1755 4097 100.0

50
Part Four:
Incidence of ESRD Patients
The total number of ESRD who treated in the dialysis units by the end of 2013 were (4272)
patients, but the number of new cases for the year 2013 was 728 (650 Jordanians and 78
non Jordanians).
Incidence of ESRD, 2013
Table (15) and Figure (17) show the distribution of ESRD incident patients in 2013 according
to the age group and gender, with a mean age of 52.7 years, and median age of 56 years.
Table (14) also shows the distribution of ESRD patients by Age-Specific Incidence Rate per
million (ASIR). The overall Incidence per Million Populations in Jordan was (99.5/1,000,000).
Table (15) Distribution and ASIR of ESRD cases by gender and age group
Incidence 2013
Gender
Age Groub
Male Female Total
N ASIR N ASIR N ASIR %
0-4 6 14.0 3 7.4 9 10.8 1.4
5-9 2 4.7 4 10.0 6 7.3 0.9
10-14 8 19.9 11 29.0 19 24.3 2.9
15-19 11 29.8 2 5.8 13 18.1 2.0
20-24 13 36.3 9 27.0 22 31.8 3.4
25-29 12 39.0 14 50.6 26 44.5 4.030-34 15 56.4 10 40.7 25 48.9 3.8
35-39 24 111.4 8 40.2 32 77.2 4.9
40-44 31 195.1 9 60.0 40 129.5 6.2
45-49 31 277.4 15 140.7 46 210.6 7.1
50-54 38 458.9 17 209.1 55 335.1 8.5
55-59 54 756.7 33 445.7 87 598.3 13.4
60-64 41 615.2 23 384.6 64 506.1 9.8
65+ 124 1162.2 82 787.7 206 977.3 31.7
Overall incidence 410 121.8 240 75.9 650 99.5 100.0

51
*ASIR per Million populations
Figure (17) Incidence of ESRD Jordanian by gender & age group-2013

52
Distribution of incident ESRD patients by health sector
Figure (18) shows that the new number of patients treated in the Dialysis Units in 2013
were 728 patients; 324 patients (44.5% ) treated in MOH Dialysis Units, 188 patients
(25.8% ) treated in RMS Dialysis Units, 12 patients ( 1.6% ) treated in university hospital
Dialysis Unit, and 204 patients (28.0 % ) treated in Private Sector Dialysis Units.
Figure (18) Distribution of ESRD patients by health sector, 2013
Distribution of ESRD incident patients by gender
In the years 2013, out of the total ( 728 ) new cases of ESRD , 464 patients (64%) were
males and 264 patients(36%) were females with male to female ratio 1.3:1 Figure (19).
Figure (19) Distribution of ESRD patients by gender, 2013

53
Distribution of ESRD Incident patients by primary cause
Table (16) shows the main primary causes of ESRD Incident patients: The most com-
mon primary cause was Diabetes Mellitus and Hypertension(combined)(37.1%), followed
by Hypertension (25.5%), Diabetes Mellitus (16.9%), Glomerulonephritis (4.4%) and then
congenital causes(2.8 %), Polycystic kidney disease (2.5%), chronic Pyelonephritis (1.4%),
the primary cause was undetermined in (5.2%) of the patients .
Table (16) Primary causes of ESRD for the year 2013 - Incidence
CausesMale Female Total
N % N % No %
Diabetes and hypertension 154 38.0 110 35.9 264 37.1
Hypertension 103 25.4 78 25.5 181 25.5
DM 67 16.5 53 17.3 137 16.9
Glomerulonephritis 15 3.7 16 5.2 31 4.4
Congenital Causes 8 2.0 12 3.9 20 2.8
Polycystic Kidney disease 15 3.7 3 1.0 18 2.5
(Pyelonephritis(chronic 6 1.5 4 1.3 10 1.4
SLE 4 1.0 2 0.7 6 0.8
Drugs induced nephropathy 2 0.5 1 0.3 3 0.4
Neurogenic bladder 2 0.5 4 1.3 6 0.8
VUR 8 2.0 2 0.7 10 1.4
Unknown 18 4.4 19 6.2 37 5.2
Others 3 0.7 2 0.7 5 0.7
Total 464 100.0 264 100.0 728 100.0
Distribution of ESRD patients by Nationality
Figure (20) shows the distribution of ESRD patients according to Nationality, in 2013 there
were (78) non-Jordanian patients accounted (11%) and 650 Jordanian patients accounted
(89%).

54
Figures (20) Distribution of ESRD patients by Nationality 2013
Distribution of ESRD patients according to type of Dialysis
Figure (21) shows that in 2013, only 9 patients (1%) were treated by peritoneal dialysis,
while 719 patients (99%) were treated by hemodialysis.
Figure (21) Distribution of ESRD patients by type of Dialysis, 2013
55
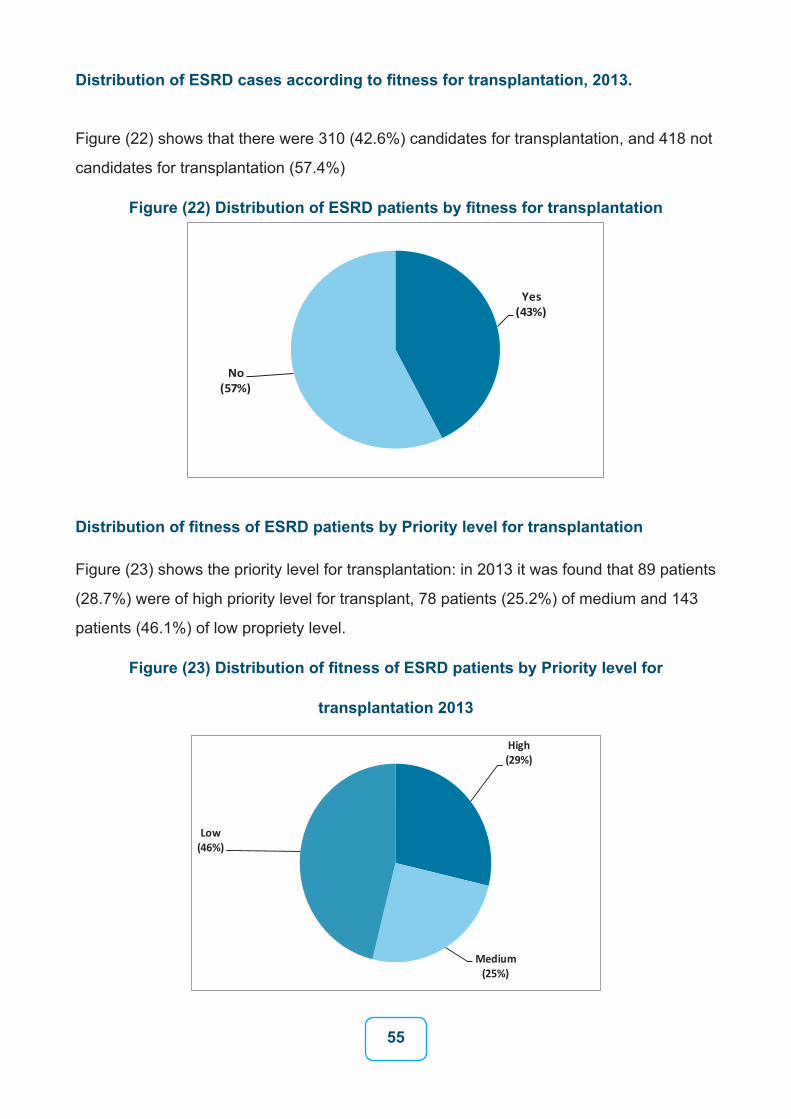
Distribution of ESRD cases according to fitness for transplantation, 2013.
Figure (22) shows that there were 310 (42.6%) candidates for transplantation, and 418 not
candidates for transplantation (57.4%)
Figure (22) Distribution of ESRD patients by fitness for transplantation
Distribution of fitness of ESRD patients by Priority level for transplantation
Figure (23) shows the priority level for transplantation: in 2013 it was found that 89 patients
(28.7%) were of high priority level for transplant, 78 patients (25.2%) of medium and 143
patients (46.1%) of low propriety level.
Figure (23) Distribution of fitness of ESRD patients by Priority level for
transplantation 2013

56
Distribution of mortality among ESRD patients
In the year 2013 a total of 40 ESRD patients (5.5%) died during this year, 19 of them were
females and 21 were males of different age group Figure (24).
Figure (24) Distribution of mortality in ESRD patients 2013

57
Part Five:
Pediatric ESRD
The total number of pediatric patients from 0-14 years was 104 patients in 2013.
Figure (25) shows the distribution of Pediatric ESRD who treated in renal dialysis units in
all hospitals during the year 2013 according to gender.
There were 104 patients, out of them 51 were males (49%) and 53 were female patients
accounted (51%).
Figure (25) Distribution of ESRD pediatric patients by gender
Distribution of Pediatric patients according to type of Dialysis
The total number of pediatric patients from 0-14 years was 104 patients. Out of them 82
patients were treated by hemodialysis and 22 on peritoneal dialysis. Figure (26) shows
distribution of pediatric patients according to type of dialysis.

58
Figure (26) Distribution of Pediatric patients according to type of Dialysis
Causes of ESRD in Pediatric patients
Table (17) shows that the primary cause of ESRD in pediatric patients (those below 14
years) : the commonest causes of ESRD Congenital renal anomalies (17.3%) followed
by Glomerulonephritis (16.3%) Vesicouretic reflux (13.5%) Neurogenic bladder (13.5%),
Hypertension (9.6%) Polycystic kidney (10.3), and Neurogenic bladder (8.0%), Hydrone-
phrosis (6.9), Nephrotic syndrome (6.7%) and Oxalosis (4.8%) while other causes were
not determined in (10.6%) of the pediatric patients.

59
Table (17) Causes of ESRD in Pediatric patients 2013
CausesMale Female Total
N % N % N %
Congenital 6 11.8 12 22.6 18 17.3
Glomerulonephritis 7 13.7 10 18.9 17 16.3
Vesicouretic reflux 10 19.6 4 7.5 14 13.5
Neurogenic bladder 4 7.8 10 18.9 14 13.5
Hypertension 6 11.8 4 7.5 10 9.6
Nephrotic syndrome 4 7.8 3 5.7 7 6.7
Oxalosis 4 7.8 1 1.9 5 4.8
Drug 1 2.0 1 1.9 2 1.9
Infection 2 3.9 0.0 2 1.9
Diabetes mellitus 0 0.0 2 3.8 2 1.9
SLE 0 0.0 2 3.8 2 1.9
Unknown 7 13.7 4 7.5 11 10.6
Total 51 100.0 53 100.0 104 100.0
Pediatric ESRD patients according to age groups and gender, 2013
Figure (27) shows the distribution of pediatric patients according to the age groups and
gender in 2013, which indicates that the highest occurrence of the cases was among the
age group (10-14) years 57 (54.8 %) for both genders, with a mean age of 9.5 years
and median 10.00.

60
Figure (27) Distribution of pediatric patients according to age groups and gender 2013
Distribution of Pediatric ESRD according to fitness for transplantation
Figure (28) shows that there were 65 (62.5%) candidates fit for transplantation, and 35 not
fit for transplantation (33.7%) missed data was 4 (3.8%).
Figure (28) Distribution of Pediatric ESRD by fitness for transplantation

61
Mortality data in Pediatric patients
A total of 10 (9.6%) pediatric patients in dialysis renal units died during the year 2013 out
of 94(90.4%) who were at risk. Figure (29)
Figure (29) Distribution of mortality in Pediatric patients

62
Part Six
ESRD Mortality
Distribution of mortality among ESRD patients
Figures (30-32) show the distribution of deaths for ESRD patients, 504 patients out of
4097 were died during the year 2013. 290 (55.8%) of them were males, and 230 (44.2%)
were females. Most of ESRD deaths occurred in the age group 65 and above. Median age
at death was 64 years, (63 years for males and 66 years for females).
Figure (30) Distribution of mortality in ESRD patients

63
Figure (31) Distribution of mortality in ESRD patients according to gender
Figure (32) Distribution of mortality in ESRD patients by age group and gender

64
Part Seven
ESRD patients among Non-Jordanians, 2013
Distribution of ESRD patients by Nationality
Figure (33) show the distribution of ESRD patients according to Nationality, The total
number of patients among Non-Jordanians was (175) accounting for (4%) of all patients
reported to Jordan Renal Registry 2013 , and (4097) patients among Jordanians ac-
counting for (96%) of all patients.
Figure (33) Distribution of ESRD patients by Nationality

65
Distribution of ESRD patients among Non-Jordanians by Gender
Figures (34) shows the distribution of Non-Jordanians ESRD patients who treated in
renal dialysis units in all Jordanian hospitals during the year 2013 according to gender
, the number of patients treated in the Dialysis Units were 175 patients , there were 110
male patients who accounted (63%) and 65 female patients accounted ( 37% ),with
male to female ratio 1.3:1.
Figure (34) Distribution of ESRD patients among Non-Jordanians by gender
ESRD patients among Non-Jordanians according to age groups, 2013
Table (18) Figure (35) shows the distribution of Non-Jordanians patients according to the
age groups and gender, which indicates that the highest occurrence of the cases was
among the age group (60-69) years for both genders, followed by age-group (40-49) years
for both genders .Mean age of the patients was 53 years, while median age of the patients
was 56 years, (55 years for males and 57 years for females).

66
Table (18) Distribution of ESRD patients among Non-Jordanians according to age groups and gender, 2013
gender
Insurance Type
Male Female Total %
0-9 1 0 1 0.7
10-19 5 1 6 1.7
20-29 10 5 15 8.8
30-39 14 9 23 13.4
40-49 21 11 32 18.5
50-59 22 9 31 18.1
60-69 32 13 45 26
70+ 14 8 22 12.8
Total 119 56 175 100
Figure (35) Distribution of ESRD patients among Non-Jordanians according to age groups and gender, 2013

67
References
1- Annual Report, Jordan, 2013. Department of Statistics (DOS)
2- BRFSS Survey, 2007 Ministry of Health (MOH) Jordan.
3- Cancer incidence in Jordan, MOH, 2011.
4- Global Youth Tobacco Survey, Anti-Smoking Society Association,
Jordan,
5- Mortality Data in Jordan, 2011, information and mortality section annual report
2011-Ministry of Health, Jordan.

7

6

5

4

3
وحدات غسيل الكلى:
يوجد في األردن 76 وحدة غسيل كلى موزعة كالتالي: 34 )45 % ( وحدة لدى مستشفيات القطاع الخاص
32 ) 42% ( وحدة لدى مستشفيات القطاع الحكومي 8 ) 10% ( وحدات لدى مستشفيات الخدمات الطبية الملكية
2 ) 3 % ( وحدة لدى المستشفيات الجامعية أجهزة غسيل الكلى:
يوجد في األردن 895 جهاز غسيل كلى موزعة كالتالي: 422 )47%( جهاز لدى مستشفيات القطاع الخاص
362 )40%( جهاز لدى مستشفيات القطاع الحكومي 77 )9%( جهاز لدى مستشفيات الخدمات الطبية الملكية
34 )4%( جهاز لدى المستشفيات الجامعية
1،000،000(، وهو الكلوي لكل مليون نسمة في األردن )627.4/ الفشل انتشار مرضى يبلغ نسبة حيث أعلى نسبة في محافظة مادبا )728.7/ 1،000،000( يليها محافظة عمان )714.7/ 1،000،0( ،محافظة
الزرقاء )631.1/ 1،000،000( و محافظة عجلون )625.8 / 1،000،000(

السجل الوطني لمرضى الفشل الكلوي
لقد جاء تأسيس السجل الوطني لمرضى الفشل الكلوي في المملكة األردنية الهاشمية بقرار من معالي وزير الصحة بتاريخ 2007/5/3 , وقد صدر أول تقرير سنوي للفشل الكلوي عام 2008.
ويهدف السجل الوطني لمرضى الفشل الكلوي إلى توفير قاعدة بيانات ديموغرافية وعلمية حول حجم مشكلة الفشل الكلوي في المملكة من حيث أعداد المرضى والتوزيع الجغرافي، والتوزيع حسب الفئات العمرية والجنس، الحكومي على عمليات غسيل اإلنفاق الغسيل، مما يساعد على تحديد حجم إلى متوسط عدد مرات باإلضافة الكلى وكلفة العالج باألدوية، وأهمية إيجاد البدائل وكلفتها. كما توفر قاعدة البيانات معلومات مرجعية ، تبين أهلية هؤالء المرضى لغايات زراعة الكلى بحيث تتسم هذه القاعدة المعلوماتية بسهولة الوصول والمصداقية للحاالت الوصول عملية يسهل مما الكلى لزراعة يحتاجون اللذين المرضى أولويات وترتيب والموثوقية، على شركاء جمعها سيتم التي المعلومات بتعميم السجل سيقوم كما دماغيا. المتوفين من بالكلى المتبرعة
وطنيين لالستفادة منها وخاصة للدفاع المدني.بلغ العدد اإلجمالي لمرضى الفشل الكلوي األردنيين 4097 مريض حتى نهاية عام 2013، منهم 2344 من الذكور بنسبة)57%( و1735 من اإلناث بنسبة )43% ( , ويعد مرض السكري والضغط من األسباب الرئيسية
للفشل الكلوي حيث يشكل مرض السكري نسبة )29.3%( والضغط نسبة )%25.1( .
وقد سجل 650 حاالت جديدة لالردنين في عام 2013 , منها 506 حالة أحياء.
أما عدد الحاالت األردنيين الذين يتلقون العالج في جميع وحدات الديلزة في األردن 3593 وذلك حتى نهاية عام 2013 باإلضافة إلى 175 غير أردني من مختلف الجنسيات.
عدد مرضى الفشل الكلوي حسب القطاعات الصحية 1597 ) 39% ( مريض لدى مستشفيات القطاع الخاص
1525 ) 37.2 % ( مريض لدى مستشفيات القطاع الحكومي 839 )20.5 % ( مريض لدى مستشفيات الخدمات الطبية الملكية
136 ) 3.3 % ( مريض لدى المستشفيات الجامعي
توزيع مرضى الفشل الكلوي حسب التامين الصحي فهو كالتالي: 986 ) 24.1 % ( مريض لديهم تامين صحي مدني
1757 ) 42.9% ( مريض لديهم إعفاء من صندوق مرضى الكلى 982 ) 24 % ( مريض لديهم تامين عسكري
41 ) 1% ( مريض لديهم تامين جامعات 46 ) 1.1%( مريض لديهم تأمين خاص )شركات(
178 )4.3 %( بدون تأمين وتأمينات أخرى وغير معروف
المملكة األردنية الهاشـمية
وزارة الصحة
مديرية األمراض غير السارية
السجل الوطني لمرضى الفشل الكلوي
وبائية الفشل الكلوي فى األردن لعام
2013
إعداد
الدكتور ايوب السيايدة الدكتور سالم القيسي