
the development of ultrasound Fetus as a...
12
1 Mark. D Kilby. Centre for Women’s & Children’s Health, University of Birmingham & Fetal Medicine Centre, Birmingham Women’s Foundation Trust. Sims Black Lecturer, 2015. The ‘fetus as a patient’ : the role of fetal therapy : is this as good as it gets? Visualization of the fetus. Leonardo's study of a fetus in the womb Lennart Nilsson. “A Child is born”. (c. 1510) Royal Library, Winsor Castle. Visualisation of the fetus : the development of ultrasound Ian Donald CBE MBE DSc FRCOG, FRCS, FRCR. 2D ultrasound to image the ‘fetus’ Regius Professor, University of Glasgow (1958). Fetus as a ‘patient’ Visualisation of the ‘second patient’ :Ultrasound Primarily as a consequence of ‘technological advance.’ The subspecialty of Fetal Medicine allowing a wide array of diagnostic & therapeutic interventions (ACOG,1988; AAP,1989)
Transcript of the development of ultrasound Fetus as a...

1
Mark. D Kilby.Centre for Women’s & Children’s Health, University of Birmingham &Fetal Medicine Centre, Birmingham Women’s Foundation Trust.
Sims Black Lecturer, 2015.
The ‘fetus as a patient’ : the role of fetal therapy : is this as good as it gets?
Visualization of the fetus.
Leonardo's study of a fetus in the womb Lennart Nilsson. “A Child is born”.(c. 1510) Royal Library, Winsor Castle.
Visualisation of the fetus : the development of ultrasound
Ian Donald CBE MBE DSc FRCOG, FRCS, FRCR. 2D ultrasound to image the ‘fetus’Regius Professor, University of Glasgow (1958).
Fetus as a ‘patient’
Visualisation of the ‘second patient’ :Ultrasound
Primarily as a consequence of ‘technological advance.’
The subspecialty of Fetal Medicine allowing a wide array of diagnostic & therapeutic interventions
(ACOG,1988; AAP,1989)

2
Fetal therapy
The impetus for fetal treatment came from obstetricians, pediatricians & surgeons frustrated by disease processes already untreatable at (still)birth.
Better visualization of the fetus led to the establishment of ‘perinatologists’.
Techniques for indirect and direct (endoscopic) visualization of the fetus made interventions possible.
Establishment of multi-disciplinary teams.
Understanding of disease & ‘developmental’ pathogenesis : but this has lagged behind visualization.
Red cell alloimunisation
Fetal IUTs : Outcome
% Live births: Overall Non-hydrops Hydrops
BWH, 1999-2003 92% 97% 89%
Literature (1998) 84% 94% 74%Over an 8-year period, 1997-2004, 221 in-utero transfusions were performed for fetal anemia(Somerset et al. Fetal Diagn Ther. 2006;21(3):272-6).
Intrahepatic vein puncture Placental cord root
Twin-to-twin transfusion syndrome
This complicates up to 1 in 5 DA / MC pregnancies and accounts for at least 40% of all twin perinatal mortality.
donor
recipient

3
Unidirectional arterio-venous anastomoses with different calibre
Fetoscopic laser ablation
(Kilby et al.Cochrane Database Syst Rev. 2014;(2):CD002073).
• 47 jaar ervaring
Survivors in each pregnancy
Fetoscopic laser ablation :
Per
cent
age
of p
regn
anci
es
12.9%
38.2%
48.9%
87.1%Systematic Review of the literature.
(Fox et al, Obstet Gynecol. 2005;105(6):1469-77)
0.1 0.5 1 2 5 10
Johnson 0.73 (0.15, 3.46)
1.26 (0.68, 2.31)
1.14 (0.54, 2.41)
1.76 (0.91, 3.39)
Quintero 1.32 (0.85, 2.03)Hecher 1.49 (0.87, 2.55)Senat 2.07 (1.30, 3.29)
Odds ratio (95% confidence interval)0.1 0.5 1 2 5 10
2.44 (1.22, 4.90)
2.57 (1.11, 5.94)
2.94 (1.48, 5.81)
Odds ratio (95% confidence interval)
Laser photocoagulation vs Serial amnioreduction
1.44 (0.78, 2.67)
2.02 (0.93, 4.41)
2.32 (1.21, 4.48)
1.00 (0.06, 17.90)
Serial amnioreduction vs Septostomy
QuinteroHecherSenat
Overall survival
Recipient survivalDonor survival
Overall survival
At least one survival
At least one survival
Study Odds ratio (95% CI)
Outcome Outcome Odds ratio (95% CI)
0.15 (0.07, 0.34)0.24 (0.07, 0.82)0.43 (0.27, 0.69)
QuinteroHecherSenat
Overall neurological Morbidity
4
Fetal structural malformations
Many congenital, structural anomalies (5% of pregnancies) are associated with increased risk of perinatal loss & morbidity.
Paediatric interest in altering the rate of progression of disease by surgical means.
Understanding of the pathogenesis is poor and incomplete.
Enthusiasm for fetal surgery between 1970-2002, especially in the USA.
Potential for fetal surgery.
Modification of progression of in-utero‘structural’ malformations is controversial.
Maternal morbidity (and theoretically mortality)
Potential fetal anomalies potentially managed by ‘fetal surgical’ intervention:
- Neural tube anomaly correction.- Congenital diaphragmatic hernia.- Lower urinary tract obstruction (LUTO).- Large fetal tumors.- Diseases with placental anomaly (i.e. TTTS).
The role of in-utero surgery?
Human ‘open surgery’ (Harrison et al,1993)- Hysterotomy at 23-27 wk.- Maternal HDU care- Aggressive tocolysis- Fetal surgery (i.e. reduction & repair / abdominoplasty).
San Francisco experience (1991-1993)- Still only variable survival (i.e. in CDH approximately 30%)
- Considerable maternal morbidity (i.e. haemorrhage / infection)
- Amniorrhexis (20%) & high risk of pre-term labor.
- Fetal distress and associated fetal cardiovascular
changes associated with liver return to abdomen.
In-utero surgery for myelomeningocele (1)
Prenatal diagnosis early in gestation.
Progressive neurologic impairment.
Poor prognosis (certainly high morbidity).
Animal models indicate that open operation (split skin graft held in place by fibrin glue) early in-utero (<24 weeks) leads to:
- prevent/reverse neurologic deficit.- preservation of spinal cord cytoarchitecture.(Copeland et al,1993; Meuliet et al,1995)
Case series in-utero surgical repair in humans : improved neurologic outcome (Meuliet et al. J Pediatr Surg. 1996. 31(3):397-402.).

5
In-utero surgery for myelomeningocele (2)
• Multicentre RCT (CHOP, San Francisco & Vanderbilt University Medical Center).
• Prior to 25th week & delivery at 38 weeks by C/S.
Open surgery for Spina Bifida.
At 30 months: Increased rates of children ‘walking independently’ (42% prenatal vs. 21% postnatal). Lower requirement for postnatal ventriculo-peritoneal shunt placement. Higher risks of PPROM, oligohydramnios & preterm birth in prenatal surgery. 33% of women had ‘scar thinning or dehiscence’.
(Adzick NS et al. N Engl J Med. 2011. MOA 1014379)
Congenital diaphragmatic hernia
“Despite antenatal diagnosis, more than 80% of babies with CDH on ultrasound will die” (Harrison,1990)
•Why does CDH carry a poor prognosis?
• What factors affect prognosis?
• Are there any ‘therapy’ to improve prognosis?

6
West Midlands Congenital Anomaly Register
All Congenital Diaphragmatic hernia (1995-2000).
(Somerset et al, Prenat Diagn. 2004. 24(8):596-604 )
Prediction of pulmonary hypoplasia
Left Right
(Deprest et al, Ultrasound Obstet Gynecol. 2006. 27(5):551-4).
Predictive of PH in CDH if:
a) Liver in the fetal chest.b) LHR<1 (More recentlythe O/E ratio has provento be more sensitive)
FETO for improving outcome in CDH
Fetoscopic laryngoscopy Fetal ‘transient tracheal occlusion’

7
Newsworthy
“Identical Twins Survive Cutting-Edge Laser Surgery”
(Houston, Texas, ABC News, 2012)
Critical appraisal of evidence for Fetal Therapy
• Evaluation of evidence usingsystematic reviews of cohortstudies.
• Robust evaluation of short &(importantly) long term outcomes.
• International collaboration
• RCTs / comparative cohort studies
• Robust evaluation of ‘techniques’.
• Institutional & personal governance

8
Fetal lower urinary tract obstruction (LUTO)
• 30% of renal tract anomalies detected at autopsy (Brand et al 1994)• Heterogeneous number of pathologies:
- Posterior urethral valves (PUV) 64%:(Commonest, usually males)
- Urethral atresia 39%- Cloacal plate anomalies, including megacystis microcolon syndrome- ‘Prune Belly syndrome’ 4%-
RCT PLUTO Study : Morris et al,2013. Lancet. In Press
Vesico-amniotic shunting vs. Conservative management in LUTO
Kaplan-Meier survival: PLUTO
• RCT data trend towards improved perinatal survival with shuntingbut with an increased risk of pregnancy loss. In RCT, the ‘as treated analysis’demonstrated that VAS improved perinatal survival to 60% as compared to no intervention (19%; p=0.03).
• At 2 years of age only 2 babies of 7 (28%) survivors post-VAS were alive with no renal impairment. Morris et al, 2013. Lancet. In Press
National initiatives for ‘standards’ in Medicine
“Standardised Mortality Rates”
Sir Bruce Keogh, the medical director of NHS England, said the figures were among a "constellation of reasons" to suspend operations.
Leeds Children’s Hospital Heart Surgery

9
What of Fetal Medicine and Therapy?
Fetal Medicine
“To set CQUINs (standards) in Fetal Medicine to which remuneration is linked”
Is this a problem & is it applicable to Fetal Medicine?
West Midlands Fetal Medicine CentreAnnual Report : since 1997
• Documentation of staff and resource.
• Documentation of workload in all areas (i.e. no: ultrasounds, amniocentesis,
CVS and therapeutic procedures).
• Documentation of overall outcomes (i.e. overall procedure related losses at amniocentesis/CVS and therapy outcomes).
• Outcomes are not individuals but institutional.
• Part of Regional CQUINS.
• Research and Development Strategy
Fetal intravascular transfusion
Intrahepatic vein puncture Placental cord root
Safe & low risk of vessel leak. Ease of access/risk of ‘tamponade’
Superior & safe results by transfusion via IHV. Fetal Diagn Ther. 2006;21(3):272-6
Fetal IUTs : Outcome
% Live births: Overall Non-hydrops Hydrops
BWH, 1999-2003 92% 97% 89%
Literature (1998) 84% 94% 74%
Over an 8-year period, 1997-2004, 221 in-utero transfusions were performed for fetal anemia(Somerset et al. Fetal Diagn Ther. 2006;21(3):272-6).
Recent national audit (BMFMS / BHS, 2013) :
• Not all centres publish outcomes in public domain. • Many Fetal Medicine units <20 IUTs per 5 yrs”• Some centres <5 IUTs per annum.
10
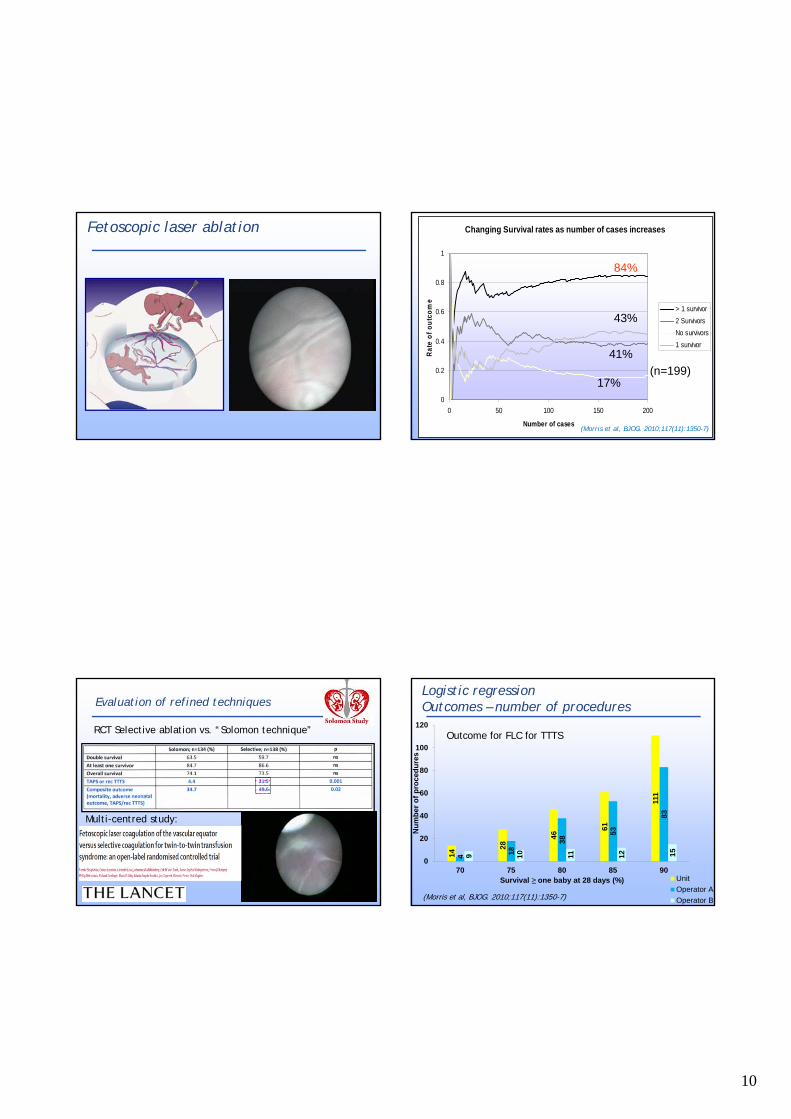
Fetoscopic laser ablation Changing Survival rates as number of cases increases
0
0.2
0.4
0.6
0.8
1
0 50 100 150 200
Number of casesR
ate
of
ou
tco
me
> 1 survivor
2 Survivors
No survivors
1 survivor
(n=199)17%
43%
41%
84%
(Morris et al, BJOG. 2010;117(11):1350-7)
Evaluation of refined techniques
RCT Selective ablation vs. “Solomon technique”
Multi-centred study:
Logistic regressionOutcomes – number of procedures
14
28
46
61
111
4 18
38
53
83
9 10 11 12 15
0
20
40
60
80
100
120
70 75 80 85 90
Nu
mb
er o
f p
roce
du
res
Survival ≥ one baby at 28 days (%) Unit
Operator A
Operator B
Outcome for FLC for TTTS
(Morris et al, BJOG. 2010;117(11):1350-7)

11
Cumulative summation test for learning curve
Fetoscopic laser ablation : 2004 – 2007. The first 199 cases.
• Centre-based learning : 76 cases to reach at least >1 in 85% FLC.• Continuing cumulative assessment.
Biau DJ, Morris RK , Kilby MD,2013.
Comparison of operator (& centre) competency
Fetoscopic laser ablation (2004-2007). First 199 cases
Tolerance 1 or 2 fetal survivor(s) in 85% of procedures.
MK
Biau DJ, Morris RK , Kilby MD,2013.
Conclusions
Better visualisation of the fetus by ultrasound and directly has allowed better forms of therapy to modify fetal pathologies.
Improved understanding of pathogenesis is important for success as noted by the treatment of Rhesus disease by in-utero transfusion & laser for severe TTTS.
New therapies are limited and critical appraisal of evidence for their introduction is important for both improvement of short and long term outcomes.
Methods for improved techniques need robust evaluation. Need for a debate on how many centres should be
performing these ‘relatively rare’ techniques and centre-based (individualised) outcome data.
Thank you for the invitation to give the Grand Rounds oration and for your
attention!
Sims Black Lecturer, 2015

12
Sims Black Lecturership, Buenos Aires, 2015


















