The Basics of Clinical Psychopharmacology: Therapeutic Alliance and Adherence Edition 2, Lecture 4...
80
The Basics of The Basics of Clinical Clinical Psychopharmacology Psychopharmacology : Therapeutic : Therapeutic Alliance and Alliance and Adherence Adherence Edition 2, Lecture 4 ASCP Model Curriculum for Medical Students
-
Upload
bartholomew-tate -
Category
Documents
-
view
223 -
download
1
Transcript of The Basics of Clinical Psychopharmacology: Therapeutic Alliance and Adherence Edition 2, Lecture 4...

The Basics of Clinical The Basics of Clinical Psychopharmacology: Psychopharmacology: Therapeutic Alliance and Therapeutic Alliance and AdherenceAdherence
Edition 2, Lecture 4
ASCP Model Curriculumfor
Medical Students

AuthorAuthor
Eric Peselow, MDEric Peselow, MD
Research ProfessorResearch Professor
NYU School of MedicineNYU School of Medicine

Objectivesfrom ADMSEP Psychiatry Learning
Objectives Taskforce, 2007
By completion of the By completion of the clerkship/medical school, the student clerkship/medical school, the student will be able to:will be able to:

ADMSEP Objectives—con’t
1. 1. Discuss the common, currently available psychotropic Discuss the common, currently available psychotropic medications with regard to clinical indications and medications with regard to clinical indications and contraindications, presumed mechanism of action and contraindications, presumed mechanism of action and relevant pharmacodynamics, common and serious relevant pharmacodynamics, common and serious adverse effects, pharmacokinetics, evidence for adverse effects, pharmacokinetics, evidence for efficacy, cost, risk of drug-drug interactions and drug-efficacy, cost, risk of drug-drug interactions and drug-disease interactions, and issues relevant to use in disease interactions, and issues relevant to use in special populations (e.g., pregnancy and lactation, special populations (e.g., pregnancy and lactation, childhood and adolescence, the elderly, persons using childhood and adolescence, the elderly, persons using herbal and over-the-counter treatments).herbal and over-the-counter treatments).
2. Propose selected psychotropic pharmacotherapy for 2. Propose selected psychotropic pharmacotherapy for designated patients and provide clinical reasoning that designated patients and provide clinical reasoning that includes discussion of factors influencing treatment includes discussion of factors influencing treatment selection (e.g.,patient-specific and drug-specific selection (e.g.,patient-specific and drug-specific variables, scientific evidence). variables, scientific evidence).

ADMSEP Objectives—con’t
3. Discuss the factors relevant to implementing, 3. Discuss the factors relevant to implementing, monitoring and discontinuing psychotropic monitoring and discontinuing psychotropic pharmacotherapy including drug dosing, treatment pharmacotherapy including drug dosing, treatment duration, and adherence, and make management duration, and adherence, and make management recommendations for dealing with an unsuccessful recommendations for dealing with an unsuccessful treatment trial (e.g., lack of efficacy, intolerability).treatment trial (e.g., lack of efficacy, intolerability).
4. Counsel patients about psychotropic 4. Counsel patients about psychotropic pharmacotherapy including risks and benefits of pharmacotherapy including risks and benefits of recommended treatment, treatment alternatives, recommended treatment, treatment alternatives, and no treatmentand no treatment
5. Identify and discuss resources to maintain an up-to-5. Identify and discuss resources to maintain an up-to-date knowledge of psychotropic pharmacotherapy date knowledge of psychotropic pharmacotherapy

ADMSEP Objectives—con’t
6. 6. Discuss special issues and concerns related to specific Discuss special issues and concerns related to specific psychotropic drug classes including metabolic, psychotropic drug classes including metabolic, hematologic, hepatic, etc.hematologic, hepatic, etc.
For For Anxiolytics and Sedative-Hypnotic AgentsAnxiolytics and Sedative-Hypnotic Agents: Be : Be able to discuss the risks, early detection, relevance and able to discuss the risks, early detection, relevance and interventions for drug toxicity, dependence and interventions for drug toxicity, dependence and consequences of abrupt discontinuation.consequences of abrupt discontinuation.

Objectives for MS II
At the end of this lecture, the student will:
Be able to articulate the basic mechanism of action of the anxiolytic drugs
Be able to name the basic drugs in this class and their clinical indications

Objectives for MS III
At the end of this lecture, the student will:
Be able to list appropriate dose ranges for at least 3 drugs in this class
Be able to elucidate the major side effects seen in the use of the various types of anxiolytic drugs

Outline
For each disorder:Definition of the disorders (with DSM criteria)Review of the phenomenology and
epidemiology of the disorderThe clinical psychopharmacology
Pitfalls and Pearls Questions

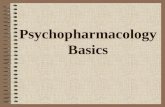
Total costs $42.3 billion in 1990
31% - Psychiatric treatment
54% - Medical treatment
10% - Workplace costs
3% - Mortality costs
2% - Pharmaceutical costs
Greenberg PE, et al. J Clin Psychiatry. 1999;60:427-435.
Economic Burden of Anxiety Disorders

Recognition and Treatment of Gernalized Anxiety Disorder

Generalized Anxiety Disorder (GAD)
In earlier versions of the DSM there was a residual anxiety category
Emphasis has changed from somatic to psychic manifestations
Increased duration of symptoms to 6 months Virtually a new disorder as currently defined Perceptions of psychiatrists and PCPs differ

DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.
Generalized Anxiety Disorder (GAD)
Excessive anxiety and worry about a number of events for the majority of days over 6 months
Difficulty in controlling the worry Associated physical and psychological
symptoms Causes significant distress or impairment Not due to a substance or a general
medical condition

American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: American Psychiatric Association; 1994.Schweizer E et al. J Clin Psychiatry. 1997;58(suppl 3):27-31.
GAD Symptoms
Psychic symptoms worry insomnia fatigue irritability feeling “on edge” poor concentration
Somatic symptoms muscle tension nausea or diarrhea sweating urinary frequency palpitations

Generalized Anxiety Disorder (GAD)
Under-recognized Under-treated
Health-care utilization
Disability/impairment
Psychiatric disorders

Epidemiology of GAD
Kessler RC et al. Arch Gen Psychiatry. 1994;51:8DSM-IV. Washington, DC: American Psychiatric Association, 1994
Lifetime prevalence 5.1 % Women outnumber men 2:1 Modal age of onset is early 20s High comorbidity in clinical cases; 1/3 “Pure” in
community samples Chronic (mean > 20 yrs) with low rate of
spontaneous remission (25% @ 2 yrs) 2nd most common psychiatric disorder after
depression in primary care 8% point prevalence in primary care

Kessler RC et al. Br J Psychiatry. 1996;168(suppl 30):17Wittchen H-U et al. Arch Gen Psychiatry. 1994;51:355
GAD Patients: Comorbidity
90% have another psychiatric disorder In patients with GAD
62% have lifetime major depression 40% have dysthymia
Anxiety disorders predict greatest riskof secondary MDD
58% of patients with lifetime MDDhave anxiety disorder

Depressed mood
Anhedonia
Appetite disturbance
Worthlessness
Suicidal ideation
Anxiety
Sleep disturbance
Psychomotor agitation
Concentration difficulty
Irritability
Fatigue
Worry
Muscle tension
Palpitations
Sweating
Dry mouth
Nausea
Overlapping Symptoms of Depression and GAD
DSM-IV-TR. Washington, DC: American Psychiatric Association. 2000.

Massion AO et al. Am J Psychiatry. 1993;150:600-607.
GAD: Complications
13%
37%
27%
0 10 20 30 40 50
Suicide Attempts
Receiving Public Assistance
Never Marrying
Rate (%)

90.4
62.4
23.5
34.4 37.6
0102030405060708090
100
Any Disorder MajorDepression
PanicDisorder
Social AnxietyDisorder
AlcoholAbuse and
Dependence
LifetimePrevalenceof Comorbid
Disorder(% of
Patients)
Lifetime Prevalence of Comorbid Disorders in Patients with GAD
Wittchen HU et al. Arch Gen Psychiatry. 1994;51:355-364.

Fernandez et al. J Clin Psychiatry. 1995;56(suppl 2):20–29.Fernandez et al. J Clin Psychiatry. 1995;56(suppl 2):20–29.Kirkwood et al. Anxiety disorders. In: DiPiro et al, eds. Pharmacotherapy: A Kirkwood et al. Anxiety disorders. In: DiPiro et al, eds. Pharmacotherapy: A Pathophysiologic Pathophysiologic Approach. 3rd ed. 1997:1443–1462.Approach. 3rd ed. 1997:1443–1462.
Differential Diagnosis Medications Which Can CauseAnxiety Symptoms
Thyroid supplementationAntidepressants CorticosteroidsOral
contraceptivesStimulants
(caffeine)
BronchodilatorsDecongestantsAbrupt withdrawal
of CNS depressants Alcohol Barbiturates Benzodiazepines

Differential Diagnosis Medical Conditions with Secondary Anxiety Symptoms
Endocrine disorders Thyroid disease Parathyroid diseases Hypoglycemia Cushings Disease
Cardio-respiratory disorders Angina Pulmonary embolism
Autoimmune disorders Neurological
Seizure disorder
Substance-related dependence/ withdrawal Nicotine Alcohol Benzodiazepines Opioids

“Pure” GAD: Treatment Options
AzapironesAzapirones
AntidepressantsAntidepressants BenzodiazepinesBenzodiazepines
Cognitive-BehaviorCognitive-BehaviorTreatmentTreatment
*GADTreatment
OptionsOptions

BENZODIAZEPINESRational use of benzodiazepines is based on:
•Presence of a benzodiazepine responsive syndrome-i.e anxiety spectrum disorder
•Use appropriate non-pharmacologic therapies when indicated•Assessment of the appropriate duration of treatment
•Short-term when possible, but recognize that many anxiety disorders require long-term treatment•Do not give as open ended treatment for insomnia
•Consideration of risk/benefit ratio associated with benzodiazepine treatment for individual patients
•Avoid in patients with an active substance abuse history unless there is a compelling indication or no good alternative; and if indicated, follow the patient closely.

BENZODIAZEPINESTreatment Issues
•Adjust dose to optimize therapeutic effect & minimize side effects, especially sedation•Monitor for abuse
•unsupervised dose increase•diversion of drug to others
•Slowly taper the drug after an appropriate trial to determine the need for any further treatment•Reconsideration of diagnosis and treatment strategy if
•patient is poorly responsive •higher than original doses are needed•medication is needed longer
•although for many patients long term treatment is appropriate

Benzodiazepines
Advantages Rapid onset Effective Well-tolerated General anti-anxiety
effects Safe in overdose Generics available
Disadvantages Withdrawal reactions Sedation Multiple daily dosing
often required Abuse potential in
patients with a history of substance abuse
Poor antidepressant effect

Benzodiazepines
Medication Daily Dosage Range (mg)
Alprazolam 2-6
Clonazepam* 1-3
Lorazepam 4-10
Diazepam* 15-20
*Slow elimination, longer to steady-state

Benzodiazepine Approximate Clinical Equivalents
Clonazepam 0.5 Alprazolam 1 mg Lorazepam 1.5 mg Diazepam 10 mg

BUSPIRONE (BUSPAR)Differences between benzodiazepines and buspirone
Benzodiazepines Buspirone
Mechanism of action-GABA Mechanism of action- 5HT
Effective as needed (prn) Ineffective as prn
Works quickly though full Takes 4-6 weeks to exert effect may take 3-4 weeks full effect
Tolerance, withdrawal and dependence No tolerance, withdrawal develops and dependence
Cross tolerant with alcohol and alleviates Not cross with alcohol and alcohol or other sedative hypnotic withdrawal does not alleviate alcohol
or benzodiazepine withdrawal

BUSPIRONE (BUSPAR)
Treatment Pearls:
•Buspirone does not work in any other anxiety disorder except GAD
•Due to perceived speed of onset it is felt that patients who have taken benzodiazepines in the past do not do as well on buspirone
•The clinical studies suggest it works but it is not the most commonly prescribed medication for GAD
•Buspirone can be give long-term without worry about “addiction”

BUSPAR (BUSPIRONE)
Initiation of Rx
Days 1-2 Buspirone 5 mg bidDays 3-7 Buspirone 10 mg bidWeek 2 Buspirone 10 mg bid Week 3 Buspirone 10 mg tid--------If no responseWeek 4-5 Buspirone 20 mg bid ------If no responseWeek 6-7 Buspirone 15 mg tid ------If no responseWeek 8 Buspirone 20 mg tid or 30 mg bid
Average dose range is 30-60 mg/day
If you are replacing a benzodiazepine with buspirone do not withdraw the benzodiazepine until 4-6 weeks, as it takes buspirone 4-6 weeks for full effectiveness. Then discontinue the benzodiazepine slowly, as buspirone does not protect against benzodiazepine withdrawal.

BUSPIRONE (BUSPAR)Side effects
Common side effects:•Headache•Nausea•Dizziness•Increased tension and agitation
•These are usually not major problems
•The relative merits of buspirone vs. selective serotonin reuptake inhibitors (SSRI’s) need to be examined
• Buspirone clearly has far fewer withdrawal symptoms than the 3 approved SSRI’s for GAD (venlafaxine, escitalopram and paroxetine)•One controlled trial shows venlafaxine XR at 75 and 150mg was more effective than 30mg/day of buspirone and placebo

Other GAD Medication Treatments Tricyclic antidepressants (TCAs)
Advantages Single daily dose Antidepressant effects No abuse potential Well studied Effective Generics available
Disadvantages Delayed onset Anticholinergic side-
effects Postural hypotension Weight gain Sexual side-effects Initial stimulation Dangerous in overdose

GAD Treatments Newer Antidepressants Venlafaxine and SSRIs (Venlafaxine, escitalopram and paroxetine have FDA approval for GAD)
Advantages Effective Benign side-effect profile Safety No dependence issues Once a day dosing
Disadvantages Delayed onset of action Early anxiogenic effect Sexual side-effects Usually requires dose
titration
*Nefazodone , bupropion, mirtazapine -insufficient information

Recognition and Treatment of Panic Disorder

Panic Disorder
One or more unexpected panic attacks as characterized by at least 4 symptoms that are described in the next slide, generally peaking in 10-20 minutes:
At least one month of worry, including change in cognition or behavior
With or without agoraphobia
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Panic attack symptoms
Palpitations, pounding heart Chest Pain or discomfortShortness of breathFeeling of chokingFeeling of dizzy, unsteady, lightheaded or faintParesthesias (numbness or tingling sensations)Chills or hot flushesTrembling or shakingSweatingNausea or abdominal stressDerealization (feelings of unreality) or depersonalization (being detached)Fear of losing control or going crazyFear of dying

Medical Utilization Top 10% of Users
Odds ratio 5 MD visits
Males Females
Major depression 1.5 3.4 Panic disorder 8.2 5.2 Phobic disorder 2.7 1.6
Simon and Von Korff, 1991

Percent Using Emergency Room for Emotional Problems Past Year
Weissman, 1991
28
11
20
5
10
15
20
25
30
Panic Disorder Major Depression Neither Disorder
Pe
rce
nta
ge

Medical conditions with increased frequency of co morbid diagnoses of panic disorder
Mitral valve prolapse Migraine Irritable bowel syndrome Chronic fatigue syndrome Vertigo Hyperventilation syndrome Premenstrual syndrome

Panic Disorder Treatment:General Principles
Pharmacotherapy Cognitive-Behavior Therapy (CBT)
Manual-driven CBT treatment to normalize “catastrophic thinking”
Exposure to panic symptoms and other feared situations

Panic Disorder Treatment:General PrinciplesPharmacotherapy Selective serotonin reuptake inhibitors first line
due to favorable side effect profile Other antidepressant classes work also Venlafaxine (Effexor) is effective Nefazodone(Serzone) no longer on US market due to
liver toxicity Benzodiazepines and Beta-blockers useful
adjunctive treatments for residual symptoms

SSRI’s -PRACTICAL USAGE IN PANIC DISORDERSertraline
•1st week------------------------25mg/day for 2-3 days & if no side effects 50mg days 4-7•2nd week-----------------------75mg/day-days 8-10 & if no side effects 100mg days 11-14 •3rd week-----------------------125 mg/day----if no response•4-6 week-----------------------150mg/day ----if no response•6 weeks & beyond-----------200mg/day & if partial response consider up to 250-300mg day•With sertraline might need a benzodiazepine (Xanax or Ativan-0.25-0.5mg bid-tid for breakthrough anxiety)
Paroxetine •1st week-------------------------10mg/day for 2-4 days & if no side effects 20mg days 4-7•2-3 weeks-----------------------30mg/day--if no response•4-6 weeks-----------------------40mg/day-- if no response•6 weeks & beyond-------------50-60mg/day as needed•With paroxetine less of a need for a benzodiazepine
Escitalopram•1st week------------------------ -5 mg/day for 2 days then 10mg days 3-7•2nd week------------------------ 10mg/day--if no response•3rd thru 5thweek--------------15mg/day ----if no response•6 weeks & beyond--------------20 mg/day as needed•Though 20mg is PDR recommended maximum, often 25-30 may be given to patients with partial responses at 20mg and no side effects

Recognition and Treatment of Obsessive Compulsive Disorder

Obsessive-Compulsive Disorder Obsessions:
1) recurrent or persistent thoughts, impulses, or images are experienced as intrusive or inappropriate and cause distress
2) not simply excessive worries about real-life problems3) person attempts to ignore or suppress thoughts or neutralize them
with another thought or action4) person recognizes that obsessions are product of his/her mind,
not imposed from without
Compulsions:1) repetitive behaviors or mental acts performed in response to an
obsession or according to certain rules2) designed to neutralize or prevent discomfort or some dreaded
event or situation The obsessions and compulsions cause marked distress,
are time-consuming, or significantly interfere with normal routine, occupational functioning, or usual social activities or relationships with others
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Rasmussen & Eisen (1992a) Zetin & Kramer (1992)
Common obsessions in OCD
Contamination Pathological doubt Aggressive impulse Somatic concerns Need for symmetry Sexual impulse

Rasmussen & Eisen (1992a) Zetin & Kramer (1992)
Common Compulsions in OCD
Washing Checking Counting Symmetry and precision Need to ask or confess Hoarding

Differentiating Obsessions vs. Delusions
Obsessions Doubt Minute possibility Insight
Delusions Certainty False/bizarre/impossible No insight

OCD Treatments
Behavior Therapy (Exposure and Response Prevention)
Pharmacotherapy (SSRI) Combination

Behavior Therapy for OCDExposure and Response Prevention
Systematic and intensive treatment Stimuli for rituals and avoidance identified
and assigned a place in a hierarchy of anxiety provocation
Intensive exposure to stimuli is done both with therapist and as homeworkExposure is graded from easiest to most difficultRituals omitted or, if not possible, delayed

Steiner et al. Presented at the American Psychiatric Association Annual Meeting, May, 1995.
Serotonergic antidepressants for OCD
Minimum duration of treatment: 10-12 weeks Therapeutic doses:
clomipramine 250 mg/day fluoxetine 60 mg/day fluvoxamine 300 mg/day sertraline 50-200 mg/day paroxetine 60 mg/day
Maintenance therapy prevents relapse Risk of relapse 2.7 times greater with placebo
than paroxetine

March et al Expert Consensus Guidelines
J. Clin Psychiatry vol 58 supplement 4 1997
Medication Choice
Fluoxetine 20mg 40-60mg 80mg long half-life 4-16 days
Fluvoxamine 50mg 200mg 300mg short half-life 13-15 hrs
Paroxetine 20mg 50mg 60mg half-life 21 hoursSertraline 50mg 150mg 225mg half-life 26 hours
Medication Start Target Max Comment

Recognition and Treatment of Posttraumatic Stress Disorder(PTSD)

Posttraumatic Stress Disorder
A characteristic set of symptoms following exposure to extreme traumatic stress Experience, witness, or confronted with actual or
threatened death or injury Response involves intense fear, helplessness, or
horror These symptoms include experiencing symptoms,
avoidance symptoms and arousal symptoms Duration more than one month Significant functional impairment
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Experiencing symptoms (1 necessary)
intrusive recollections
recurrent dreams
flashbacks
psychological distress with reminders
physiologic reactivity with reminders
Posttraumatic Stress Disorder
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Avoidance symptoms (3 necessary)avoid thoughts/feelings/conversationsavoid activities, places, people inability to rememberdiminished interest feelings of detachmentrestricted affect foreshortened future
Posttraumatic Stress Disorder
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Arousal symptoms (2 necessary)
sleep difficulty
irritability
concentration
hyper vigilance
exaggerated startle
Posttraumatic Stress Disorder
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Lifetime prevalence in community of 1% to 14% One of the least well-studied anxiety disorders Combat-related PTSD is best studied PTSD is associated with sexual abuse, physical
assault, torture, accidental trauma, natural or man-made disasters, diagnosis of threatening illness
American Psychiatric Association, 1994.
Posttraumatic Stress Disorder

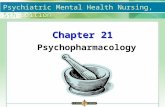
PTSD Risks of Specific Traumasin the US Population
Pe
rcen
tag
eP
erc
enta
ge
Natural Natural DisasterDisaster
RapeRapeCombatCombatCriminalCriminalAssaultAssault
MenMen
WomenWomen
Kessler RC et al. Kessler RC et al. Arch Gen PsychiatryArch Gen Psychiatry. 1995;52:1048–1060.. 1995;52:1048–1060.
About 30% of people exposed to trauma developed PTSD
N/AN/A

PsychosocialExposure therapyCognitive therapy
Anxiety managementDesensitization
EMDRHypnotherapy
PTSD Treatment Options
PharmacologicSSRIsTCAs
MAOIs Mood stabilizers
Antianxiety agents
EMDR = eye movement desensitization and reprocessing.

Recognition and Treatment of Social Anxiety Disorder

Social Anxiety Disorder
Fear that performance will prove humiliating or embarrassing
Not related to other axis I or III disorders Exposure to feared situation anxiety Avoidance or distress Social or occupational problems or worried
about fear Knows fear is excessive
DSM IV-TR. Washington, DC: American Psychiatric Association. 2000.

Social Anxiety Disorder Subtypes Generalized
Almost all domains affected Non-generalized
One or two social situation--usually public speaking only

Symptoms of social anxiety disorderFeared situations
Social Attending parties,
weddings etc Conversing in a group Speaking on telephone Interacting with authority
figure (eg teacher or boss)
Making eye contact Ordering food in a
restaurant
Performance Public speaking Eating in public Writing a check Using public toilet Taking a test Trying on clothes in a store Speaking up at a meeting

Symptoms of social anxiety disorder Precipitating situations
Being introduced Meeting people in authority Using the telephone Receiving visitors Being watched doing something Writing in front of others Speaking in public

Taylor and Arnow, 1991
Symptoms of social anxiety disorder Cognitive patterns Overestimation of scrutiny by others Overestimating possible rejection,
embarrassment or humiliation Misinterpretation of response of others Exaggerated response to rejection Discounting personal achievements /
overemphasizing failures

Social anxiety disorder
CombinationCBT + pharmacotherapy
MAOIs
Benzodiazepines CBT
SSRIs
Social anxiety disorderTreatment options

Social anxiety disorder Treatment goals
Control anxiety and phobic avoidance Reduce associated disability Treat depression / other comorbid disorders Tolerability over long term Eventual medication-free status

Pharmacological management of social anxiety disorder
Consider initial choice of an SSRI Initial dose for 2-4 weeks, then increase if necessary
example sertraline: 100mg/day with increase to 200mg/day
Some benefit evident by 2-4 weeks If no response by 6-8 weeks, switch to drug of
another class or augment Consider psychosocial treatments Continue pharmacotherapy for at least 1 year

Social Anxiety Disorder: Pharmacological Treatments Monoamine oxidase inhibitors
(standard/RIMAs) Benzodiazepines SSRIs--leading choice as sertraline and
paroxetine are FDA approved for this disorder

Pitfalls and Pearls
Pitfalls
Anxiety is a difficult condition to treat, as individuals often overestimate the level of their anxiety
Building a tolerance to anxiolytics and sedative hypnotics always happens. This easily can turn into addiction in high risk individuals.
Anxiolytics with longer half-lives are less likely to cause dependence.

Pitfalls and Pearls
Pearls
Because of the pitfalls, most of these medications are used only sparingly by psychiatrists.
buspirone is an exception to the pitfalls. However, it may not be as effective as the usual anxiolytics.
Withdrawal from anxiolytics/sedative hypnotics is similar to that from alcohol (with which they are cross=tolerant), but is more insidious and life-threatening
Never use combinations of these drugs

Question 1
In an average primary care practice, what percentage of patients will have GAD?
A. about 2 percent
B. about 4 percent
C. about 6 percent
D. about 8 percent
E. about 10 percent

Question 2
Which of these is not a good recommendation for someone with an anxiety disorder?
A. drink less coffee
B. monitor over-the-counter medications
C. have a glass of wine before bedtime
D. exercise moderately
E. pay attention to sleep hygiene

Question 3 What would be most useful for a person
who is dependent on alprazolam?
A. Tell the patient to stop the drug at once
B. Add a longer acting benzodiazepine
C. Tell the patient not to drink alcohol
D. Monitor the patient for liver failure
E. Change the patient to clonazepam

Question 4 Buspirone is most like what other drug
class with regard to mechanism of action?
A. “Typical” antipsychotics
B. Benzodiazepines
C. Antidepressants
D. Analeptic mood stabilizers
E. Beta blockers

Question 5 Which agent is most likely to abort an
acute panic attack?
A. alprazolam
B. clonazepam
C. buspirone
D. amitriptyline
E. diazepam

Question 6 What is a good treatment option for
PTSD?
A. SSRIs
B. MAOIs
C. Mood stabilizers
D. Antianxiety agents
E. All of the above

Answers to Questions
1. D
2. C
3. E
4. C
5. A
6. E

End of Lecture