Endcap shielding senarios : YE1-2 Gap senarios – (Ref. Boki C vs Surkov 6)

Thalassaemia Case Scenarios
Dr Emma Drasar Haematology Consultant The Whittington Hospital

With transfusion and chelation therapy, thalassemia patients can be expected to have a normal life, shifting the focus to managing the disease complications
IOL, iron overload; TDT, transfusion-dependent thalassemia.
Borgna-Pignatti C, et al. Haematologica. 2004;89:1187-93. Musallam KM, et al. Haematologica. 2013;98:833-44.
Non-transfusion-dependent thalassemias (NTDT)
β-thalassemia major (regularly transfused, TDT)
Silent cerebral ischemia
Pulmonary hypertension Right-sided heart failure
Splenomegaly
Gallstones
Hepatic fibrosis, cirrhosis, and cancer
Extramedullary hemopoietic pseudotumors
Leg ulcers
Venous thrombosis
Osteoporosis
Cardiac siderosis Left-sided heart failure
Hepatic failure Viral hepatitis
Diabetes mellitus
Hypogonadism
Hypothyroidism Hypoparathyroidism
Osteoporosis
Disease-related Disease- and IOL-related
Surv
ival
pro
bab
ility
p < 0.00005
0
1.00
0.75
0.50
0.25
0 5 10 15 20 25 30 Age (years)
Birth cohort
1960–1964 1965–1969 1970–1974 1975–1979 1980–1984 1985–1997

Guidance for the clinician
Yardumian et al. Standards for the Clinical Care of Children and Adults with Thalassaemia in the UK. 3rd Edition 2016. The United Kingdom Thalassaemia Society .
Cappellini MD, et al. Guidelines for the management of transfusion dependent thalassaemia (TDT). 3rd ed. Thalassaemia International Federation Publication No. 20; 2014.
Available from: http://www.thalassaemia.org.cy/educational-programmes/publications?issuu=18570602/30656661
Complication 1 • 26 year old man
• Attends for routine cross match
• Mentions to Thalassaemia nurse that he was found on the floor last night by flat mates
• Has no memory of what happened.
• What would you do?

Complication 1
• Now feels fine • Does say has had
sensation of “skipped beats” for last month.
• Poorly compliant with chelation
Next investigations?
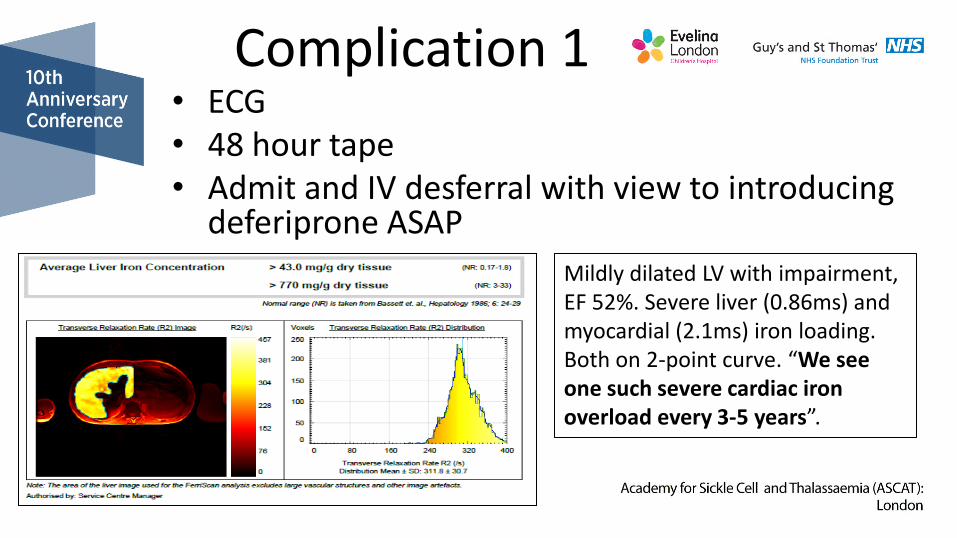
Complication 1 • ECG • 48 hour tape • Admit and IV desferral with view to introducing
deferiprone ASAP
Mildly dilated LV with impairment, EF 52%. Severe liver (0.86ms) and myocardial (2.1ms) iron loading. Both on 2-point curve. “We see one such severe cardiac iron overload every 3-5 years”.

Complication 1
Why does iron overload in the heart matter?
Guidelines for Iron Assessment Myocardial loading
Myocardial T2*(ms)
Hepatic loading
Hepatic T2* (ms)
Dry weight (Anderson)
None >20ms None >6.3ms <2mg/g
Mild >14-20ms Mild >2.7- 6.3ms 2->5mg/g
Moderate 10-14ms Moderate 1.4-2.7ms 5-10mg/g
Severe* <10ms Severe <1.4ms >10mg/g

Anderson LJ, et al. Eur Heart J. 2001;22:2171-9. Kirk P, et al. Circulation. 2009;120:1961-8.
LVEF, arrhythmia and cardiac failure associated with cardiac IOL Arrhythmia
0.15 0.10 0.05 0
0.20
0.25
0.30 < 10 ms
10–20 ms
> 20 ms
Pro
po
rtio
n o
f p
atie
nts
w
ith
arr
hyt
hm
ia
60 0 120 180 240 300 360
p < 0.001
Cardiac failure
Pro
po
rtio
n o
f p
atie
nts
d
evel
op
ing
card
iac
failu
re
0.1
0.3 0.2
0
0.4
0.5
0.6
< 6 ms
6–8 ms
8–10 ms
> 10 ms
Follow-up time (days)
60 0 120 180 240 300 360
p < 0.001
LVEF
(%
)
0
50
70
40
30
20
10
60
80
90
0 20 40 60 90 80 100 10 30 50 70 Cardiac T2*, ms
Cardiac T2* value of 37 ms in a normal heart
Cardiac T2* value of 4 ms in a significantly iron-overloaded heart
Normal T2* range
Normal LVEF range
Myocardial T2* values < 20 ms are associated with a progressive and
significant decline in LVEF

• The age at the time of death from cardiac
mortality increased in parallel with the
decrease of cardiac mortality
• The prognosis of β-TM patients
significantly improved with
– non-invasive methods to measure organ iron
– new chelators
– increased blood safety measures
Significant reduction in cardiac mortality in the past two decades with new chelators and diagnostics
Origa R, et al. Expert Rev Hematol. 2015;8:851-62. M
ean
age
at
de
ath
(y
ear
s)
0
8
24
32
40
16
Even
ts pe
r 1,0
00
pt/yr
1989– 1995
1996– 2000
2000– 2003
2004– 2006
2005– 2010
2010– 2014
0
3
9
12
15
6
Increase of the age at death (line) and decrease in cardiac deaths (bar chart) reported in Cagliari, Italy,
over 24 years

Complication 2
• 45 year old beta thal major patient presents to A&E with nausea, confusion and polyuria and polydypsia.
• How would you investigate them?
• What is the underlying cause?

Complication 2 • Treat as you would any other patient with HHS
but think about cardiac function • Screening for DM and control – annual OGTTs
and regular fructosamines • Role of joint clinics and MDT to improve
compliance • Diabetes nurse reviewing patient while they
have their transfusion • Phone clinics
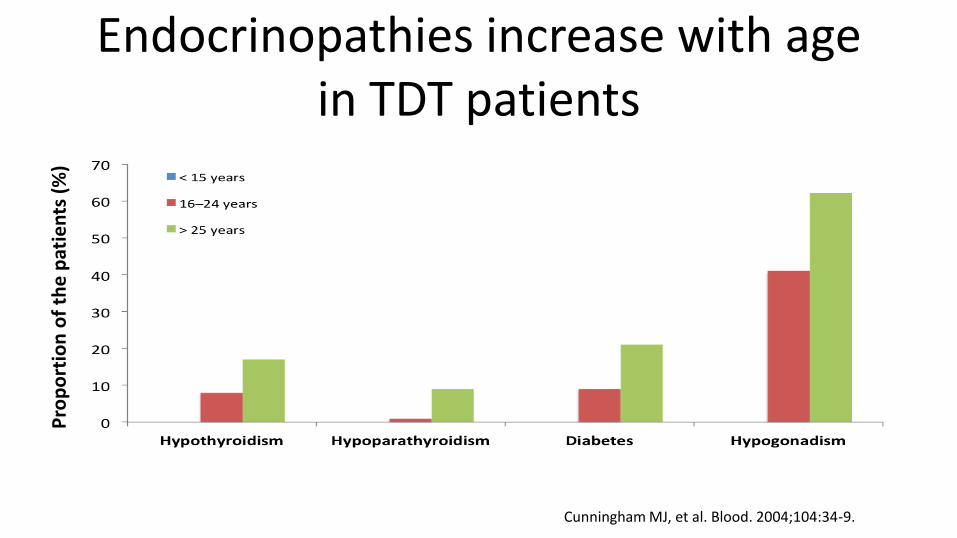
Endocrinopathies increase with age in TDT patients
Cunningham MJ, et al. Blood. 2004;104:34-9.
Pro
po
rtio
n o
f th
e p
atie
nts
(%
)

Older thalassaemia major patients
Ang et al 2013 EJH
60%

Complication 3
Complication 3 • What is this and what could have led to
its development in a patient with thalassaemia?
• What can we do to prevent it from happening to future patients?

Liver complications are becoming more prominent
• Voskaridou E, et al. Ann Hematol. 2012;91:1451-8.
0
5
10
15
20
25
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Heart disease
Liver disease
Year of death
Pat
ien
ts (n
) n = 4,506, of whom 2,485 (52.3%) with TM

HCC is a major cause of death in HH and NTDT • HCC generally occurs on a cirrhotic substrate
– yearly incidence rate approximately 3% in HH; no data for NTDT
• HCC is the main cause of morbidity and mortality in adult HH and is increasing in thalassaemia (particularly NTDT)
– of 36 thalassaemic patients with HCC, 22 (61%) had β-TI, including 6 who were HCV negative (probably almost all had liver cirrhosis)
• Reasons for increased risk
– IOL remains unnoticed and untreated
• patients are asymptomatic
• iron burden was underestimated in β-TI patients
– patients with an adult form of HH and β-TI patients survive longer
• higher risk of cirrhosis and more time for HCC development HCC, hepatocellular carcinoma; TI, thalassaemia intermedia.
• Borgna-Pignatti C, et al. Br J Haematol. 2004;124:114-7. • Fargion S, et al. Hepatology. 1994;20:1426-31. Fracanzani AL, et al. Hepatology. 2010;51:501-10.
Maakaron JE, et al. Ann Hepatol. 2013;12:142-6. Restivo Pantalone G, et al. Br J Haematol. 2010;150:245-7.

Recommendations? • All patients who have EVER had a liver biopsy with
evidence of cirrhosis or fibrosis should be on surveillance for HCC – Six monthly ultrasound scans – Endoscopy annually
• Any patients with severe iron overload at any time in the past should be tested to identify fibrosis/cirrhosis (fibroscan or other method) and then enter survailence

Complication 4 • 42 year old thalassaemia major patient
presents with high temperature, unwell with loin to groin pain.
• What could be causing this?
• Renal function has been deteriorating over past 5 years. What could be contributing to this situation?

Complication 4
• Renal complications increasingly common in thalassaemia:
– Renal tubulopathy
– Renal stones
– Renal cell carcinoma

Renal stones
Probability of forming a stone – Asia 1–5%
– Europe 5–9%
– North America 13%
– Saudi Arabia 20%
1–2% occurrence in children
Types – Ca2+ oxalate/phosphate 50–70%
– uric acid 10–23%
– struvite 5–10%
– cysteine 1–2%
Idiopathic hypercalciuria
Hyperparathyroidism
Sarcoidosis
Vitamin D intake
Distal renal tubular acidosis
Lithium
Hypercalcaemic syndromes – tumour, etc.
Hereditary
1. Ryall R, et al., editors. Urolithiasis 2. New York: Plenum Press; 1994.
Nephrolithiasis

Mussalam KM, Taher AT. J Am Soc Nephrol. 2012;23:1299-302.
Mechanisms of renal disease in thalassaemia
Vascular resistance
Renal plasma flow
GFR
Endothelial and epithelial
damage
Transudation of
macromolecules
Mesangial dysfunction GFR
Tubular cell damage
Epithelia–mesenchymal
transdifferentiation
Tubulointerstitial injury
Glomerular sclerosis GFR
GFR Iron overload Chronic anaemia or hypoxia
Chronic anaemia or hypoxia
Tubular cells
Iron overload
Oxidative stress
Lipid peroxidation
Cellular damage
Relative iron depletion
Abnormal mitochondrial
function and arachidonic acid
cascade
Tubuloglomerular feedback
and haemodynamic change GFR
Iron chelation
Nephrotoxicity
Iron chelation

Conclusion • New complications developing as well as the
preexisting ones
• Thalassaemia patients are reaping the benefits of longer survival but also a whole new lot of complications
• Long term impact of iron overload is resulting in new problems

Thanks