Testosterone Replacement - s3.amazonaws.com and lowered T - Age is not a specific risk factor for...
58
Testosterone Replacement Seacourses Dec 30, 2017 – January 6, 2018 Dr. Stacy Elliott
-
Upload
truongquynh -
Category
Documents
-
view
217 -
download
2
Transcript of Testosterone Replacement - s3.amazonaws.com and lowered T - Age is not a specific risk factor for...

Testosterone Replacement
Seacourses
Dec 30, 2017 – January 6, 2018
Dr. Stacy Elliott

Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
by any means – graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of
Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.

Arousal
(Erection)
Orgasmic
threshold
Ejaculation
Orgasm
Refractory
period
lIncreased durationplateau phase
May be elevated
May be altered↓Semen volume
Increased duration

Sexual Function Changes with Age
spontaneous & a.m. erections
rigidity of erection: faster detumescence
pre-ejaculatory sensation
force/volume of ejaculation
need to ejaculate
Less orgasmically driven: more intimacy driven

Aging and lowered T
- Age is not a specific risk factor for hypogonadism (HG)- Age alone is associated with little decline in mean total
T levels ( > 40 years) until 70s and 80s- SHBG does increase with age, so bioavailable T (BioT)
falls faster than total T (TT)- The lowering of T is more correlated with
comorbidites, (DM, hypertension, hyperlipidemia, asthma/COPD and/or kidney disease) regardless of age
- ≥ BMI of 30 kg/m² tripled the risk of symptomatic HG (normal weight men 1:6, BMI > 35 kg/m² 2:3)
- Low T likely a marker of poor health

Testosterone Biosynthesis
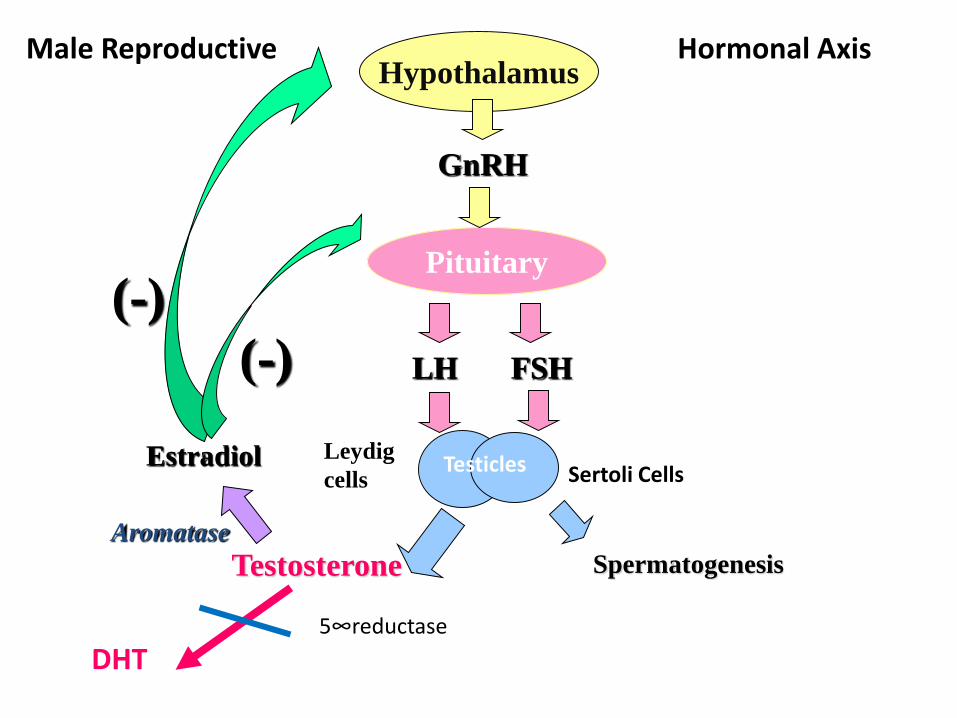
Hypothalamus
Pituitary
GnRH
LH FSH
SpermatogenesisTestosterone
Estradiol
Aromatase
(-)
(-)
Male Reproductive Hormonal Axis
Sertoli CellsLeydig
cells
DHT 5∞reductase
Testicles
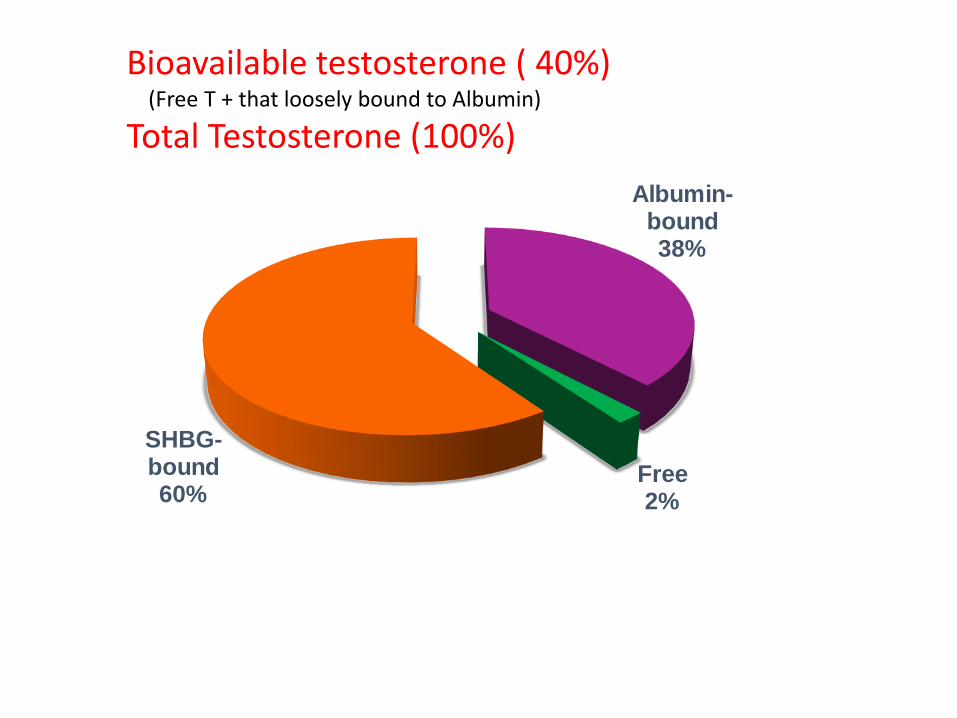
Albumin-bound38%
Free2%
SHBG-bound60%
Bioavailable testosterone ( 40%) (Free T + that loosely bound to Albumin)
Total Testosterone (100%)

Factors that Influence [SHBG]
Lower SHBG
• Obesity
• Diabetes
• Hypothyroidism
• Nephrotic syndrome
• Glucocorticoid use
• Progestins
• Androgenic steroids
Increase SHBG
• Aging
• Hepatic cirrhosis
• Hyperthyroidism
• HIV
• Estrogens

Diagnosis of Hypogonadism (HG)
• Classical primary HG: testicular failure ( Low T, elevated LH,FSH : hypergonadotrophic HG)
• Secondary HG: central (low T, low LH,FSH secondary to GNRH or LHRH failure : hypogonadotrophic HG)
• Adult onset hypogonadism (AOH) is a subgroup of men with signs and symptoms of HG without an adequate pituitary response to low T levels (normal or low levels of LH FSH) i.e. functional hyposecretion at the level of both the pituitary and the testes.

Testosterone: Target Organsbrainlibido, mood, cognition
heartcardiovascular health
liverprotein synthesis
kidneystimulation of erythropoietinproductionmale sexual organs
penile growthspermatogenesis, erection
prostate growth and function
bone marrowstimulation of stem cells
skinhair growth, balding,
sebum production
musclestrength, volume, energy
reduction in visceral fat
bonestrength and density
Post puberty: Homeostasis & Metabolic Agent

Signs and symptoms* associated with testosterone deficiency syndrome
• Sexual: Decreased libido; erectile dysfunction; decreased frequency of morning erections; delayed ejaculation , reduced seminal volume, anorgasmia
• Somatic: Increased visceral body fat/obesity; decreased lean muscle mass; decreased strength; fatigue/loss of energy; decreased physical activity/ vitality; low bone mineral density; anemia; flushes; loss of facial, axillary and pubic hair/slow beard growth; decline in general feeling of well-being
• Psychological: Depression/depressed mood; mood changes; irritability; inability to concentrate; insomnia/sleep disorders
* May be subtle

Signs and Symptoms of TDSOrder of Appearance
• Decreased libido• Decreased vitality• Fatigue• Mood changes• Insomnia• Anemia• Delayed ejaculation• Flushes• Erectile dysfunction• Decreased muscle mass• Increased visceral body fat• Testicular atrophy• Weakness• Osteopenia/osteoporosis• Loss of facial, axillary and pubic hair
Mild
Severe

Prevalence of Hypogonadism: HIM Study 1
1. Mulligan T, Frick MF et al. Int J Clin Pract. 2006; 60:762-9.

Watch for symptoms in high risk groups
• Metabolic syndrome and diabetes
• Obesity
• Untreated sleep apnea
• Head trauma or radiation
• Chronic neurological diseases ( SCI, MS,etc)
• Other chronic disease processes ( CRF, COPD)
• Refractory depression
• Anemia and sarcopenia of undetermined origin
• HIV and weight loss
• Glucocorticoid or opioid therapy
• ED with failed trial of PDE5i

What to order?
• Bioavailable T correlates best with symptoms• The level of SHBG will dictate how much
testosterone can actually get into the cells• Practically – total T if you are suspicious as Lifelabs
will not do the bioavailable T unless total T is under 8.4 nmol/L
• The key is low T + symptoms = treatment potential• Consistency is the key – get 2 values• Can have transient low T with comorbid illness,
medications or malnutrition or variable time of day

Daily and Weekly Variability in T
Examples of different response patterns1
1. Morley JE, et al. Metabolism. 2002;51:554-559.
Weekly Variability in T
100
150
200
250
300
350
400
450
500
0 2 4 6 8
42 6 8
Time (weeks)
Se
rum
te
sto
ste
ron
e (
ng
/mL
)
Up to 50% of young healthy men have temporary T levels below the normal range in a 24-hour period.( Spratt et al 1988)

What does the research say?
Remember the spectrum testosterone levels that will demonstrate symptoms – use common sense
Patients below 10.4 nmol/L have a greater likelihood of symptoms ( 1)
Low testosterone levels require confirmation and investigation of:1
– SHBG levels
– Serum luteinizing hormone (LH)
– Follicle-stimulating hormone (FSH)
– Prolactin
• Distinguish between primary and secondary causes
(1) Bhasin et al. J Clin Endocrinol Metab. 2010;95:2536-59.

Diagnosing
- Symptomatic by history
- Questionnaires can be too non-specific
- Take a serum total T sample between 7 – 11* or within 3 hours of waking for shift workers
- Investigate secondary or reversible causes

When to do Bioavailable T
• If your total testosterone comes back borderline or low normal on a symptomatic patient, you can ask for a BioT or SHBG to see how much bioavailable testosterone ( free T and that loosely attached to albumin) is available to the androgen receptor ( i.e. is he truly hypogonadal)
• But ask – why? Canadian recommendation is for 3 month trial of those symptomatic men in the grey area (9 – 12.5 nmol/L)

If you highly suspect hypogonadism…
Do appropriate bloodwork to save you and your patient time
- baseline total testosterone
- FSH, LH, prolactin , CBC ( Hct, Hb)
- optional: TSH, IGF-1, ferritin, Fe sat, Vit D
Assess prostate before instituting therapy
- mandatory DRE and PSA

Low testosterone levels have been associated with:
• Sexual dysfunction
• Diabetes
• Metabolic syndrome
• Decreased max. exercise capacity
• Osteoporosis and increased fracture risk
• Decreased muscle mass
• Lower quality of life
• Increased cardiovascular risk
• ALL CAUSE AND CV MORTALITY
Maggi et al. J Sex Med. 2007;4:1056-69; Shelton et al. Urol Clin North Am. 2012;39:63-75;
Ukkola et al. Ann Med. 2013;45:206-12

Lower T levels result in ….
Prostate Cancer IssuesGreater risk of prostate cancerHigh Gleason scoresWorse stage at presentationWorse survival
Mental Health Issues• Psychological effects, higher rate of depression in
men with HG• TRT alone may reverse dysthymia ( but not MDD)• TRT can improve refractory depression

Metabolic Syndrome and T
• Androgen deficiency contributes to metabolic components of MetS but this is a bidirectional process
• Obesity men are more likely to be HG
• Visceral obesity causes inflammatory cytokines
• If you lose 15% of BW - you will gain T
• If you gain 10% more BW – lose T by affecting cytokine level

T and insulin
• Testosterone maintains insulin sensitivity
• Men with normal / higher T levels have better insulin sensitivity and lower insulin levels than men with hypogonadism
• Insulin resistance is higher in men with lower T (hypogonadal)

T and Vascular system
• Men with higher T levels have lower carotid intimal thickness
• Since the health of endothelial cells depends on androgen ( due to improved eNO) – men with low levels of T have impaired flow mediated dilatation
• Men on ADT therapy are at higher risk for diabetes, CAD, MI and sudden death

Cardiovascular risk with low T
Keating et al.
20061
(Observational study)
•16% increase in the risk of coronary heart disease
events (death or myocardial infarction) in patients
on androgen deprivation therapy
Tsai et al.
20072
(Observational study)
2-fold increased risk of fatal cardiovascular events
over 10-year period in men on androgen
deprivation therapy
Ruige et al.
20113
(Meta-analysis)
In elderly men, low testosterone predicted
increased risk for cardiovascular disease and/or
mortality( it is uncertain if low T has a direct negative
effect of it it indicates poor general health)
1. Keating et al. J Clin Oncol. 2006;24:4448-56; 2. Tsai et al. J Natl Cancer Inst. 2007;99:1516-24;
3. Ruige et al. Heart. 2011;97:870-5

Low T and Mortality
Low endogenous testosterone
levels are associated with
an increased risk in mortality
T: testosterone.1. Shores et al. Arch Intern Med. 2006;166:1660-5.

Bottom Line
• Rule out potentially reversible causes first –sleep apnea , any way he can reduce his weight with lifestyle changes?
• If the man is low to low normal and symptomatic , it is worth a three month trial of androgen replacement
• If he is very low he is at risk for heart and bone issues – should treat

Does T replacement correct ED?T and PDE5i
• Appears to be a threshold level of TRT ( to low normal range) that will improve ED, beyond that , no further improvement seen in sexual motivation or performance
• HG states likely down regulate the PDE5 enzyme (which seems to be crucial in determining metabolic and structural imbalance of the CC) = venous leak
• Men with ED who did not respond to monotherapy may respond to combination therapy (TRT + PDE5i)
• Majority of studies suggest TRT for PDE5i failures but some state combination doesn’t help
• General consensus is to screen PDE5i failures for low T
Aversa 2009, Kalinchenko 2003, Rosenthal 2006, Shabisigh 2006, Bhasin 2001, Buvat 2013

Risk associated with TRTWhen levels are supraphysiological- Erythrocytosis• Gynecomastia• Lowering of HDL*Others• Testicular atrophy and infertility• Acne• Exacerbate pedal edema in heart failure patients ( esp early
on therapy) • Worsen untreated sleep apnea • Stimulate growth of known prostate cancer ( so far…not true)• Worsen symptoms of BPH ( so far…found to benefit!)
Bassil et al. Ther Clin Risk Manag. 2009;5:427-48;
Bhasin et al. Best Pract Res Clin Endocrinol Metab. 2011;25:251-70.

What about the prostate?
BPH• Testosterone is contraindicated in men with severe BPH-LUTS (IPSS >19)1
• Original consensus: testosterone therapy may worsen symptoms of BPH1,2
• Current view: testosterone therapy improves LUTS in men with low testosterone and mild BPH3
Prostate Cancer
• Old view: use of TRT accelerated PCa (throwing fertilizer on a plant)
• New View: Prostate cancer is largely unaffected by variations in serum testosterone levels within the naturally occurring ranges
• Androgen Receptors are saturated at 4 nmol/L – increasing beyond that will not cause further prostate growth ( providing water to a thirsty plant )
• No recurrence of prostate cancer upon testosterone therapy
.Bhasin et al. J Clin Endocrinol Metab. 2010;95:2536-59; 2. Bassil et al. Ther Clin Risk Manag. 2009;5:427-48;
Shigehara et al. Aging Male. 2011 Mar;14:53-8 Morgentaler. Urol Clin N Am. 2011;38:119-24; 2. Morgentaler
Eur Urol. 2006;50:935-9; Kaufman et al. J Urol. 2004;172:920-2; 4. Khera et al. J Sex Med. 2009;6:1165-70.

Saturation model in non-castrate men
• States that prostatic homeostasis is maintained by a relatively low level of androgenic stimulation
• Explains the observation that exogenous testosterone administration does not significantly increase intraprostatic androgen levels in hypogonadal men.
Giving men TRT with PCa
• Vancouver : treated 82 HG men with TRT
- no biochem recurrence on 22 RP
(PSA velocity 0.001 per year)
- 3/50 ( 6%) recurrence on radiation patients ( PSA velocity: 0.12 per year)
- N=8 Active Surveillance (PSA velocity 1.1 ug/L per
year increase) , but no higher grade Gleason on subsequent biopsy
Ory et al: J of Urology 196: 1082 – 1089 Oct 2016

TAKE HOME MESSAGESfor the prostate !
• Risks are associated with testosterone therapy and should be discussed and monitored in patients
• Prostate cancer is largely unaffected by variations in serum testosterone levels within the naturally occurring ranges
• Testosterone therapy may be considered on an individualized basis in patients who have had definitive local treatment for PCa with undetectable PSA levels
PSA: prostate specific antigen.

Who gets TRT/who doesn’tYes• Symptomatic men with low T who have been appropriately
worked up• Men with equivocal levels of T who are symptomatic can
undergo a three month trial • But TRT may worsen: erythrocytosis ( >50%), untreated
obstructive sleep apnea, severe congestive heart failure
No • Men who have breast cancer or metastatic ( or high grade)
prostate cancer• Men with suspicious prostate nodule or PSA > 3• Men wanting fertility within the next 1 -2 years• Men with class III or IV heart failure

Giving men TRT with Advanced PCaSMSNA November 2017
• Initial experience with TRT in 7 ( average age 69) selected HG men with advanced PCa wishing TRT despite recognizing potential risks of rapid PCa progression ( 2005 – 2016).
• Gleason 7 (n=4), 8 ( n=1), 9 ( n=2)
• 6/7 had had ADT and discontinued :1/7 refused ADT despite bone metastases
• Median PSA at initiation of TRT = 2.1 ng/ml
• 4/7 had asymptomatic bone mets at initiation of TRT
• All reported improved energy, cognition, libido, sexual function and sense of well being
• No cases of disease flare, acute pain, or vertebral collapse
• 3 patients continue TRT, 2 DC with PSA> 20 ng/ml, 2 deceased
Krawowsky Y, Morgentaler A : SMSNA Abstract 132 San Antonio 2017

Does TRT increase CV risk?
Testosterone therapy does not increase cardiovascular risk and has been reported to
have beneficial effects on patients with angina and heart failure (1-3)
THREE SCIENTIFALLY FLAWED BUT HIGH PROFILE STUDIES
Tom trial of 2010
• Vigen et al 2013
• Finkle et al 2014
1.Toma et al. Circ Heart Fail. 2012;5:315-21; 2. Malkin et al. Heart. 2004;90:871-6; 3. Carson et al. J Sex Med. 2012;9:54-67.

CARDIOVASCULAR EVENTS ARE NOT AFFECTED BY TESTOSTERONE TREATMENT
*Odds ratio significantly different from placebo. CABG: coronary artery bypass graft.1. Calof et al. J Gerontol A Biol Sci Med Sci. 2005;60:1451-7; 2. Carson et al. J Sex Med. 2012;9:54-67.
0
10
20
30
40
50
60
70
Even
t R
ate
per
1,0
00 P
ati
en
t Y
ears
Placebo
Testosterone
*

Testosterone Replacement Therapy (TRT)
• Goals:– Symptom improvement
– Achievement of physiological T levels
• Several safe and effective formulations available
• Use ASTEP acronym to choose formulation:
Availability
Safety
Tolerability
Efficacy
Preferences
Invasiv
en
ess
& solutions
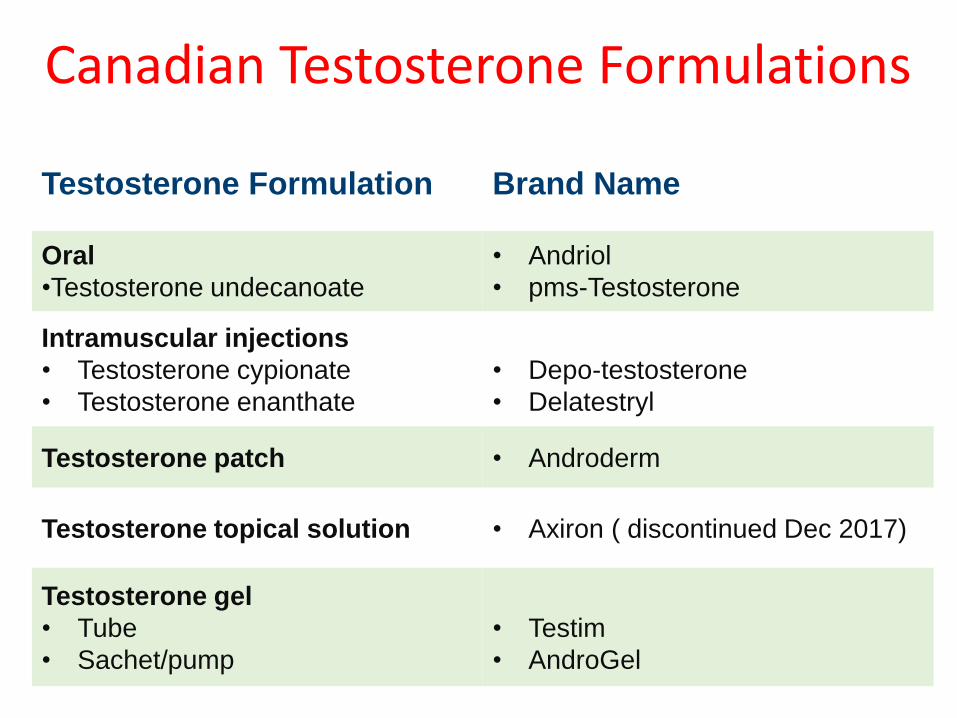
Canadian Testosterone Formulations
Testosterone Formulation Brand Name
Oral
•Testosterone undecanoate
• Andriol
• pms-Testosterone
Intramuscular injections
• Testosterone cypionate
• Testosterone enanthate
• Depo-testosterone
• Delatestryl
Testosterone patch • Androderm
Testosterone topical solution • Axiron ( discontinued Dec 2017)
Testosterone gel
• Tube
• Sachet/pump
• Testim
• AndroGel

Recommendations for TRT
• Men with TT levels <8.0 nmol/L usually benefit from testosterone therapy
• Symptomatic men with TT between 8.0 to 12 nmol/L can be considered for a 4 to 6 month trial– Continue testosterone therapy beyond 6 months, only in
cases where clinical benefit is demonstrated
• Caution is warranted in men with history of congestive heart failure
• Easily titratable formulations (gel, topical solution or patch) should be considered for men >70 years, and those with chronic illness
TT: total testosteone.
1. Nehra et al. Mayo Clin Proc. 2012 Aug;87(8):766-78.

Oral Medication
Generic Name Dosage
Testosterone undecanoate1,2
( Andriol)
120-160 mg daily divided
in 2 dosesa
a This dose should be taken for 2-3 weeks.
Subsequent dosages may be reduced to 40-120 mg
daily.
1. Product Monograph: Andriol (testosterone undecanoate capsules) 40 mg. Kirkland, Quebec: Schering-Plough
Canada Inc.; 2008.
2. Product Monograph: pms-Testosterone (testosterone undecanoate capsules) 40 mg. Montreal, Quebec:
Pharmascience Inc.; 2009.

The Effect of Food on Absorption of Testosterone Undecanoate1
1. Product Monograph: Andriol (testosterone undecanoate capsules) 40 mg. Kirkland, Quebec: Schering-Plough
Canada Inc.; 2008.
• T undecanoate should be taken with a normal meal or breakfast to
achieve proper T levels
Time (h)
Mean T
Concentr
ation
(ng/m
L)
80 mg Fed
80 mg Fasted
0
2
4
6
8
10
0 2 4 6 8 10 12 14 16 18 20 22 24
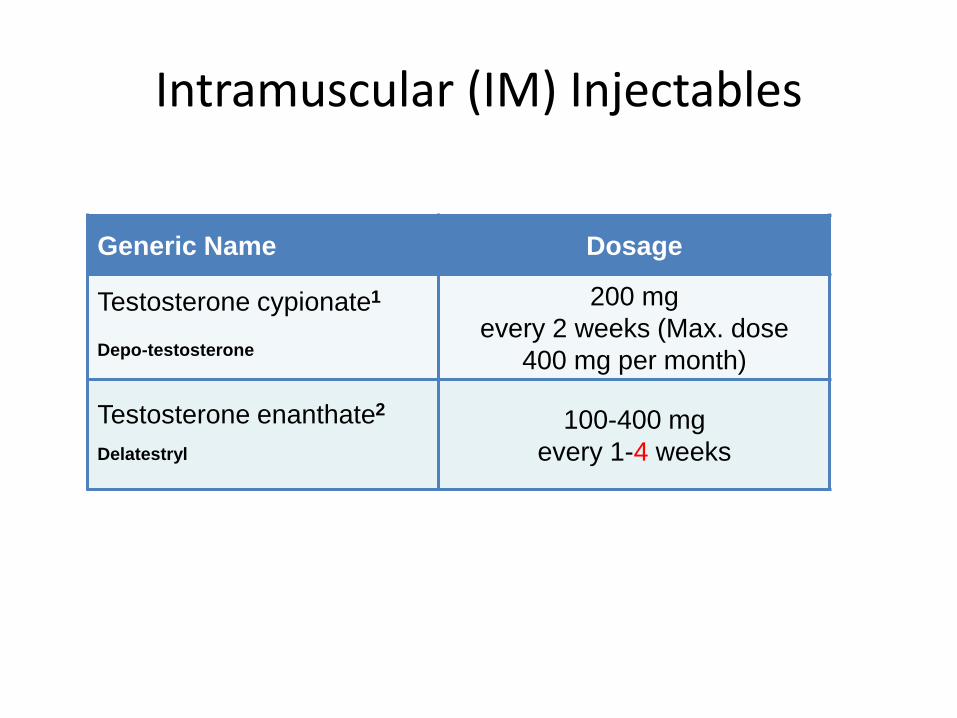
Intramuscular (IM) Injectables
Generic Name Dosage
Testosterone cypionate1
Depo-testosterone
200 mg
every 2 weeks (Max. dose
400 mg per month)
Testosterone enanthate2
Delatestryl
100-400 mg
every 1-4 weeks
1. Prescribing Information: Depo-Testosterone (testosterone cypionate injection USP, Sterile Solution) 100 mg/mL. Kirkland, Quebec: Pfizer Canada Inc.; 2007.
2. Prescribing Information: Delatestryl (testosterone enanthate, Solution for Injection) 200 mg/mL. Mississauga, Ontario: Theramed Corporation; 2007.

Transdermal Patch
• Dosage: 2.5 or 5 mg patch applied daily
• Mid-normal range 4 – 12 hours after application
• May require 2 x 5 mg patches in some men
Testosterone
Transdermal
Delivery System
(Testosterone1)
1. Product Monograph: Androderm (testosterone, Transdermal Delivery System) 12.2 mg and 24.3 mg.
Montreal, Quebec: Paladin Labs Inc.; 2007.
Main issue erythema 65.8%
Vs 5.3- 5.7% with Gels

Transdermal T Gels
• Dosage: 5-10 g daily, to deliver 50-100 mg of testosterone• Easy to apply ( daily)
Testosterone1% Gel
(Testosterone USP1)
Testosterone 1% Gel
(Testosterone, Ph.Eur2)
1. Product Monograph: AndroGel (testosterone gel) 1%. Markham, Ontario: Abbott Products Inc.; 2010.
2. Product Monograph: Testim (testosterone gel) 1%. Malvern, Pennsylvania: Auxilium Pharmaceuticals Inc.; 2009.

Transdermal Topical Solution
Product Concentration DoseApplication
Site
Axiron 2%
testosterone
2-4 actuations
daily
(60-120 mg daily)
Axilla
Ease of application (applied to axilla with applicator)
• Minimal side effects
• Flexible dosing ( 1 pump = 30 mg gel in 1.5 ml of solution)
• Low transference potential
1. Axiron Product Monograph. Eli Lilly Canada Inc.
Steady-state serum concentrations are attained
within approximately 1 week of daily dosingBEING DISCONTINUED !!

Natesto
• Ease of administration, low dose, and no risk of secondary transference
• two or three daily doses (5.5 mg per nostril, 11.0 mg single dose). Total daily doses were 22 mg or 33 mg.
• Lower incidence of LH and FSH suppression
• Natesto(™) 11 mg b.i.d. or 11 mg t.i.d. restores normal serum total testosterone levels in most hypogonadal men.
• Erectile function, mood, body composition, and bone mineral density improved from baseline.
• Adverse event discontinuation rates were 2.1% (b.i.d.) and 3.7% (t.i.d.)
• Furthermore, DHT, DHT/T, and PSA levels produced by the nasal gel are among the lowest levels observed with a commercial formulation of testosterone
• Intranasal gel testosterone is detectable using conventional anti-doping tests
Rogol et al Androlgoy Volume 5, Issue 4, 844, Article first published online: 17 July 2017

FORMULATION-SPECIFIC FOLLOW-UP
1. Bhasin et al. J Clin Endocrinol Metab. 2010;95:2536-59; 2. Bebb. BCMJ. 2011;53:474-79; 3. Axiron Product Monograph. Eli Lilly Canada.
Adjust dose (and/or frequency) to obtain testosterone levels in the mid-normal range
Testosterone TherapyWhen To Measure Serum
Testosterone:Evaluate Patient For:
Oral (Andriol,
Pms-Testosterone)1,2
3-5 hours after ingestion • Compliance
– Taken with fat, split doses
Testosterone patch
(Androderm) 1,2
2-12 hours after application • Skin reactions
Testosterone topical
solution (Axiron)3
Any time >1 week after initiation
of topical solution
• Adherence to protocols which minimize
transfer and maximize absorbance
Testosterone gel
(Testim, AndroGel) 1,2
Any time >1 week after initiation
of gel use — ideally 3-4 hours
after application
• Adherence to protocols which minimize
transfer and maximize absorbance
Intramuscular
injections (Delatestryl,
Depo-testosterone,)1,2
Midway between injections,
or at trough
• Fluctuations in mood/libido
• Cough after injections

Monitoring
• At each appointment monitor:
– Symptom response (clinic)
– Changes in blood parameters• T
• Hemoglobin
• Hematocrit
– PSA/DRE• Refer if abnormal
Year 1
Every
3–6 months
Annually
Frequency

Timeline of Symptom Improvement1
Duration of Treatment (months)
Sym
pto
mIm
pro
ve
me
nt
0 3 6 12
Enhanced libido
Improved emotional well-being
Increased energy
Reduced ED
Increased strength
Enhanced BMD
Improved cognition
Enhanced cardiovascular health
Decreased body fat
Improvement in some components of MetS
1. Morales A, et al. CUAJ. 2010;4:268-274.
MetS = Metabolic Syndrome

Non-response
• Non-response may be indicative of:– Compliance issues – Malabsorption– Insufficient dose– Unsatisfactory formulation– Symptoms unrelated to TDS
• Long-term lack of response – Consider referral to a specialist
(endocrinologist/urologist)
• ED patients who fail T or PDE5i alone:– Consider T plus PDE5i

Differences between men and women
• Objective arousal ( erections) is linked to subjective arousal/desire in men
• Physical changes of arousal ( vaginal lubrication, pelvic vasocongestion ) and the subjective experience can be two distinct entities in women – correlation between subjective and objective arousal is poor in women
• Sexual behavior in aging women ( and men) not solely dependant on androgen levels
• Depression, relationship changes, partner loss, religious issues, anxiety about future, estrogen levels in women ( vasomotor symptoms sleep disturbances, vaginal effects)
• Increased prevalence of HSDD and low desire is not direct result of endogenous levels

“Don’t order serum testosterone in women looking for low levels” ( Basson 2011)
• Clinical available assays are not accurate at the low levels found in women
• Intracellar testosterone is not measured by serum levels of testosterone until recently
• There is no evidence that low testosterone is linked to low desire when accurate testosterone assessment ( including intracrine peripheral cells levels) is used
• Hormone imbalance often not the reason ( mood changes, sexual self-image, partner feelings or sexual dysfunction more likely the cause)
Basson, Rosemary : This Changed My Practice , UBC CPD 2011

Long term risks of T in women
• Not known• Breast and uterine data so far good• CVD data controversial • Opinions and changes to post menopausal
women’s use of estrogen following the Women’s Health Initiative study serves as a warning in use of systemic sex hormone supplementation for a chronic disorder
• Long-term RCT’s are needed ( > 4 years , randomized, placebo controlled)

Lessons from Transgendered Men
• Quick escalation to male physiological ranges with T
• Goal is virilisation and masculinisation, but cannot reverse previous feminization if started post pubertal (subcut fat distribution, broader hips, etc)
• Within 3 months: amenorrhea, increased facial and body hair, skin changes and increased acne, changes in fat distribution, increases in muscle mass, increased libido & may have male pattern hair loss
• Later effects: deepening of the voice, atrophy of vaginal epithelium, increased clitoral size
Unger C. Hormone Therapy I transgender patients Trans Androl & Urol 2016;5:877 - 884

Cases