Testosterone Replacement Effectively Inhibits The Development
12
of April 14, 2018. This information is current as Cell Expansion Direct Role of Testosterone on Regulatory T Autoimmune Orchitis in Rats: Evidence for a Inhibits the Development of Experimental Testosterone Replacement Effectively Wygrecka, Jörg Gromoll and Andreas Meinhardt Bhushan, Holger Hackstein, Gerhard Schuler, Malgorzata Monika Fijak, Eva Schneider, Jörg Klug, Sudhanshu http://www.jimmunol.org/content/186/9/5162 doi: 10.4049/jimmunol.1001958 March 2011; 2011; 186:5162-5172; Prepublished online 25 J Immunol Material Supplementary 8.DC1 http://www.jimmunol.org/content/suppl/2011/03/25/jimmunol.100195 References http://www.jimmunol.org/content/186/9/5162.full#ref-list-1 , 12 of which you can access for free at: cites 51 articles This article average * 4 weeks from acceptance to publication Fast Publication! • Every submission reviewed by practicing scientists No Triage! • from submission to initial decision Rapid Reviews! 30 days* • Submit online. ? The JI Why Subscription http://jimmunol.org/subscription is online at: The Journal of Immunology Information about subscribing to Permissions http://www.aai.org/About/Publications/JI/copyright.html Submit copyright permission requests at: Email Alerts http://jimmunol.org/alerts Receive free email-alerts when new articles cite this article. Sign up at: Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved. Copyright © 2011 by The American Association of 1451 Rockville Pike, Suite 650, Rockville, MD 20852 The American Association of Immunologists, Inc., is published twice each month by The Journal of Immunology by guest on April 14, 2018 http://www.jimmunol.org/ Downloaded from by guest on April 14, 2018 http://www.jimmunol.org/ Downloaded from
Transcript of Testosterone Replacement Effectively Inhibits The Development

of April 14, 2018.This information is current as Cell Expansion
Direct Role of Testosterone on Regulatory T Autoimmune Orchitis in Rats: Evidence for aInhibits the Development of Experimental Testosterone Replacement Effectively
Wygrecka, Jörg Gromoll and Andreas MeinhardtBhushan, Holger Hackstein, Gerhard Schuler, Malgorzata Monika Fijak, Eva Schneider, Jörg Klug, Sudhanshu
http://www.jimmunol.org/content/186/9/5162doi: 10.4049/jimmunol.1001958March 2011;
2011; 186:5162-5172; Prepublished online 25J Immunol
MaterialSupplementary
8.DC1http://www.jimmunol.org/content/suppl/2011/03/25/jimmunol.100195
Referenceshttp://www.jimmunol.org/content/186/9/5162.full#ref-list-1
, 12 of which you can access for free at: cites 51 articlesThis article
average*
4 weeks from acceptance to publicationFast Publication! •
Every submission reviewed by practicing scientistsNo Triage! •
from submission to initial decisionRapid Reviews! 30 days* •
Submit online. ?The JIWhy
Subscriptionhttp://jimmunol.org/subscription
is online at: The Journal of ImmunologyInformation about subscribing to
Permissionshttp://www.aai.org/About/Publications/JI/copyright.htmlSubmit copyright permission requests at:
Email Alertshttp://jimmunol.org/alertsReceive free email-alerts when new articles cite this article. Sign up at:
Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved.Copyright © 2011 by The American Association of1451 Rockville Pike, Suite 650, Rockville, MD 20852The American Association of Immunologists, Inc.,
is published twice each month byThe Journal of Immunology
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

The Journal of Immunology
Testosterone Replacement Effectively Inhibits theDevelopment of Experimental Autoimmune Orchitis in Rats:Evidence for a Direct Role of Testosterone on RegulatoryT Cell Expansion
Monika Fijak,* Eva Schneider,* Jorg Klug,* Sudhanshu Bhushan,* Holger Hackstein,†
Gerhard Schuler,‡ Malgorzata Wygrecka,x Jorg Gromoll,{ and Andreas Meinhardt*
Despite the immune-privileged status of the male genital tract, infection and inflammation of the male genital tract are important
etiological factors in male infertility. A common observation in clinical and experimental orchitis as well as in systemic infection and
inflammation are decreased levels of testosterone. Emerging data point to an immunosuppressive role of testosterone. In our study,
we substituted testosterone levels in experimental autoimmune orchitis (EAO) in rat by s.c. testosterone implants. EAO development
was reduced to 17% when animals were treated with low-dose testosterone implants (3 cm long, EAO+T3) and to 33% when rats
were supplied with high-dose testosterone implants (24 cm, EAO+T24) compared with 80% of animals developing disease in the
EAO control group. In the testis, testosterone replacement in EAO animals prevented the accumulation of macrophages and
significantly reduced the number of CD4+ T cells with a strong concomitant increase in the number of regulatory T cells (CD4+
CD25+Foxp3+) compared with EAO control. In vitro testosterone treatment of naive T cells led to an expansion of the regulatory
T cell subset with suppressive activity and ameliorated MCP-1–stimulated chemotaxis of T lymphocytes in a Transwell assay.
Moreover, expression of proinflammatory mediators such as MCP-1, TNF-a, and IL-6 in the testis and secretion of Th1 cytokines
such as IFN-g and IL-2 by mononuclear cells isolated from testicular draining lymph nodes were decreased in the EAO+T3 and
EAO+T24 groups. Thus, our study shows an immunomodulatory and protective effect of testosterone substitution in the path-
ogenesis of EAO and suggests androgens as a new factor in the differentiation of regulatory T cells. The Journal of Immunology,
2011, 186: 5162–5172.
Infertility and subfertility affect between 10 and 15% of cou-ples with ∼50% of cases attributable to some form of malefactor (1). Of the known causes and/or cofactors of male in-
fertility, 13–15% of cases have been shown to result from infectionor inflammation of the male reproductive tract (2, 3). This highprevalence marks infection and/or inflammation as key etiologicalfactors of male reproductive dysfunction. Orchitis is characterizedby inflammatory infiltrates in the testicular interstitium with as-sociated damage to the seminiferous tubules, which can lead to
focal and in its most severe form also to total impairment ofspermatogenesis. In most cases, inflammation involves also the epi-didymis, resulting in a combined epididymo-orchitis (4). Where-as acute testicular inflammation is symptomatic and mainly relatedto infection, the subacute, or chronic, form of the diseaseis predominately asymptomatic (4–6). It should be noted that al-though the acute phase of the disease, which is the consequenceof infection, can be successfully treated with antibiotics and anti-phlogistics, the inflammatory reaction is more insidious in that itcan continue undetected in both testes slowly undermining testic-ular function (4, 7–10).Experimental autoimmune orchitis (EAO) in the rodent is an
established model of chronic testicular inflammation (11). Inducedby immunization with testicular homogenate in adjuvant, EAO ischaracterized by the production of auto-antibodies against testic-ular Ags, elevated levels of proinflammatory cytokines (e.g., TNF-a, IL-6) or chemokines (e.g., MCP-1), followed by the infiltrationof leukocytes (mainly macrophages, dendritic cells, T lympho-cytes) (12–14). An increase in the number of regulatory CD4+
CD25+Foxp3+ T cells is also observed (15). In the later stages ofthe disease, these infiltrates can form granulomas. The final phaseof EAO consists of the progressive apoptosis of germ cells, whichleads to aspermatogenesis and thus sterility (16–20). Decreasedlevels of testosterone and increased FSH concentrations in serumindicate that the detrimental influence of EAO is not limited totesticular germ cells alone but also extends to the dysfunction ofthe somatic, Sertoli, and Leydig cells (21).An increasing body of evidence suggests that sex hormones play
an important role in the modulation of the onset and/or perpetuationof autoimmune disease. In particular, steroid hormones have been
*Department of Anatomy and Cell Biology, Justus-Liebig-University Giessen, 35385Giessen, Germany; †Institute for Clinical Immunology and Transfusion Medicine,Justus-Liebig-University Giessen, 35392 Giessen, Germany; ‡Clinic for Obstetrics,Gynecology and Andrology of Large and Small Animals, Justus-Liebig-UniversityGiessen, 35385 Giessen, Germany; xDepartment of Biochemistry, Faculty of Medi-cine, Justus-Liebig-University Giessen, 35392 Giessen, Germany; and {Centre ofReproductive Medicine and Andrology, University of Munster, 48129 Munster, Ger-many
Received for publication June 11, 2010. Accepted for publication March 3, 2011.
This work was supported by a project grant of the Deutsche Forschungsgemeinschaft(ME 1323/4-4) and the LOEWE program grant “Male factor infertility due to in-fection and inflammation”.
Address correspondence and reprint requests to Dr. Andreas Meinhardt, Departmentof Anatomy and Cell Biology, Justus-Liebig-University Giessen, Aulweg 123, D-35385 Giessen, Germany. E-mail address: [email protected]
The online version of this article contains supplemental material.
Abbreviations used in this article: EAE, experimental autoimmune encephalomyeli-tis; EAO, experimental autoimmune orchitis; GOI, gene of interest; HKG, house-keeping gene; HPRT-1, hypoxanthine phosphoribosyltransferase 1; LH, luteinizinghormone; MNC, mononuclear cell; Treg, regulatory T cell; Tresp, responder T cell.
Copyright� 2011 by TheAmericanAssociation of Immunologists, Inc. 0022-1767/11/$16.00
www.jimmunol.org/cgi/doi/10.4049/jimmunol.1001958
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

implicated as crucial contributors to the immune response eitheras enhancers, as is the situation with estrogens, or as endogenousinhibitors, as is the case with testosterone and glucocorticoids (22,23). This is best exemplified by the much higher incidence ofautoimmune diseases such as multiple sclerosis in women, wherethe female to male ratio is significantly higher (2:1 to 3:1) (24,25). Beyond sex-linked genetic factors and gender differences inimmune responsiveness, a major contributing factor to this sexbias is thought to be the lesser degree of protection afforded tofemales due to their lower testosterone levels and hence the di-minution of its inhibitory/protective influence (26, 27). A cor-ollary is the later onset of multiple sclerosis in males comparedwith females, which coincides with a decline in bioavailable tes-tosterone in men (28) and which suggests that testosterone mayprovide a degree of protection to young men who are geneticallysusceptible to the disease. Further supporting evidence of testos-terone’s influence is provided by studies of animal models such asthe NOD mouse, where prepubertal castration results in an in-creased prevalence of immunologically mediated diabetes (29),and SJL mice, where castration increased the severity of experi-mental autoimmune encephalomyelitis (EAE) (30). Conversely,female NOD and SJL mice implanted with testosterone pelletsreveal lower incidences of diabetes and lesser forms of EAE, re-spectively, than in those without hormonal intervention (31, 32).Similar findings have also been reported on the increased in-cidence and severity of thyroiditis and adjuvant arthritis aftercastration, whereas testosterone treatment was found to be pro-tective in both cases (33, 34).Although some progress has been made in deciphering the
manner by which testosterone exerts its immunoprotective in-fluence, the precise mechanism of its actions is still unknown.Some hints as to the nature of the anti-inflammatory process havebeen provided by studies showing that testosterone supplemen-tation reduces the expression of IFN-g and increases the expres-sion of the anti-inflammatory cytokine IL-10 by autoantigen-specific T lymphocytes (32, 35). Complementary in vitro studieshave found CD4+ T lymphocytes treated with 5a-dihydrotesto-sterone also respond with increased IL-10 production (36).In the testis, high local testosterone concentrations (10-fold
higher than in serum in rats) seem to play an important role in themaintenance of testicular immune privilege, an effect strikinglydemonstrated by transplantation studies that showed that ratspretreated with estrogen to suppress Leydig cell testosteroneproduction promptly rejected intratesticular allografts that wereotherwise tolerated (37). As serum testosterone levels in EAOanimals are significantly decreased (21) and androgens are im-portant immunosuppressive factors, the rationale behind our studywas to investigate the putative protective influence that testoster-one may provide during the development and pathogenesis ofEAO.
Materials and MethodsAnimals
Adult male inbred Wistar Kyoto rats aged 50–70 d were purchased fromCharles River Laboratories (Sulzfeld, Germany). Animals were kept at22˚C with a 14-h light, 10-h dark schedule and fed with standard foodpellets and water ad libitum. All procedures conformed to National In-stitutes of Health guidelines for care and use of experimental animals andwere approved by local animal ethics committees (RegierungspraesidiumGiessen GI 20/23 - Nr. 33/2008) prior to their commencement.
Induction of EAO and testosterone replacement treatment(experimental design)
EAO was induced in 22 rats (the experimental group, E) by active im-munization three times every 2 wk with syngeneic testicular homogenate as
previously described (16, 19). Briefly, immunization on anesthetized ratswas performed on day 0 by injecting 0.4 ml syngeneic testicular homog-enate mixed with 0.4 ml CFA (Sigma-Aldrich) into the hind footpads (s.c.)and in different sites near the popliteal lymph nodes and the neck area(intradermally). These injections were repeated twice at 14-d intervals (day14 and day 28, see Fig. 1). The first two immunizations (day 0, day 14)were followed by an i.v. injection of 1010 inactivated Bordetella pertussisbacteria (strain DSM 4952; Deutsche Sammlung von Mikroorganismenund Zellkulturen, Braunschweig, Germany) dispersed in 0.5 ml isotonicsaline, and the third (day 28) was followed by an i.p. injection of B.pertussis at a concentration of 5 3 109 in 0.5 ml isotonic saline. Controlanimals received CFA only and B. pertussis following the same scheme.
Twenty days after the first immunization, testosterone capsules wereimplanted s.c. along the dorsal surface of the rats under anesthesia (day 20).The implants were prepared using medical-grade polydimethylsiloxanetubing (inner diameter 1.59 mm, outer diameter 3.18 mm; Dow Corning,Midland, MO) filled with testosterone powder (Sigma; T-1500) and sealedat each end with medical adhesive silicone type A as previously described(38, 39). The testosterone implants were either 3 cm (T3) or 24 cm (T24;3 3 8 cm = 24 cm) in length and had a release rate of 30 mg/cm/d. Aschematic demonstration of the immunization procedure including tes-tosterone treatment is shown in Fig. 1.
In numerous studies, it has been established that low-dose T3 implantscause a reduction in serum luteinizing hormone (LH) levels, a subsequentdecline in intratesticular testosterone, and loss of the developing sper-matogenic cells in the testis. In contrast, high-dose T24 similarly causesa drop in LH, but supplies sufficient testosterone to maintain intratesticularT levels adequate to support qualitatively normal seminiferous tubule func-tion (38, 40).
The animals were divided into the following seven groups each com-prising 6–10 rats: 1) E rats treated with T3 implant (EAO+T3); 2) E plusT24 implant (EAO+T24); 3) adjuvant controls treated with T3 implant(Adjuvant+T3); 4) adjuvant plus T24 implant (Adjuvant+T24); 5) EAOrats without hormone replacement (EAO control); 6) adjuvant control; 7)normal untreated rats (Normal). Fifty days after the first immunization,the animals were sacrificed by an overdose of isoflurane (Forene; Abbott,Wiesbaden, Germany), and the testes and seminal vesicles were removedunder sterile conditions and weighed. One testis was snap frozen in liquidnitrogen or fixed in Bouin’s solution to evaluate the degree of germ cellloss as an indirect parameter of seminiferous tubule damage. EAO animalsdisplay characteristic pathological changes such as significantly smallertestis size and weight, inhomogeneous testicular parenchyma, and testisredness. Histopathologically, EAO testis reveal premature release of de-veloping germ cells in the lumen resulting in impaired spermatogenesisand atrophy of germinal epithelia and leukocytic infiltration of the inter-stitium with occasional granuloma formation. The contralateral testis andthe testicular draining lymph nodes (LNs) were processed to generatesingle-cell suspensions. To determine intratesticular testosterone levels, apiece of left or right testis (∼300 mg) was decapsulated and homogenizedwith 3 volumes of ice-cold PBS. The resulted protein extract was frozen at220˚C and subsequently used for hormone measurement. Testicular cry-osections or paraffin-embedded sections were cut, processed, then stainedwith hematoxylin using standard procedures. Peripheral blood was col-lected by cardiac puncture and stored overnight at 4˚C prior to the serumbeing collected by centrifugation (1000 3 g for 15 min). Sera were thenstored at 280˚C for subsequent hormone assays.
Hormone assays
Intratesticular and serum testosterone levels were measured by RIA afterextraction of the samples with toluene as previously described (41). Fortestosterone, the intra-assay and interassay coefficients of variation werebetween 7.8 and 9% with the lower limit of detection being 0.1 ng/ml.Serum LH and FSH were determined by RIAs using reagents provided byDRG Instruments (Marburg, Germany) according to the manufacturer’sprotocols. Serum samples were assayed in duplicate across a single assay.The sensitivity of the assay was 0.18 ng/ml for LH and 2 ng/ml for FSH.
Preparation of testicular interstitial cell suspensions
Testicular interstitial cells were obtained by enzymatic digestion as de-scribed previously (42). Briefly, decapsulated testes were incubated with 1mg/ml collagenase D (Roche Diagnostics, Mannheim, Germany) plus0.1% BSA (fraction V; Sigma Chemical) in PBS in a shaking water bath at34˚C for 15 min. The enzyme was inactivated by adding ice-cold PBS, andthe tubule fragments were allowed to settle for 4 min, then the supernatantwas centrifuged at 300 3 g for 10 min at 4˚C. The pellet, containing in-terstitial cells, was washed with PBS and erythrocytes depleted by osmoticlysis using RBC lysis buffer (Gentra Systems, Minneapolis, MN) for 5 min
The Journal of Immunology 5163
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

at room temperature. The final cell suspension was washed with PBS at300 3 g for 10 min at 4˚C and processed directly for flow cytometricanalysis.
Flow cytometric analysis
The following mAbs were used: mouse anti-rat CD4-PE (clone OX-35),anti-rat CD25-FITC (clone OX-39), PE-conjugated mouse IgG1,k, mouseIgG1,k-FITC. Background staining was evaluated using appropriate iso-type controls. All Abs were purchased from BD Biosciences (Heidelberg,Germany), except for anti mouse/rat Foxp3-Alexa Fluor 647 (clone FJK-16s) and mouse IgG2a-Alexa Fluor 647 obtained from eBioscience (SanDiego, CA) and AbD Serotec (Oxford, U.K.), respectively. All incubationsteps were conducted at 4˚C for 30 min. Briefly, a maximum of 106 in-terstitial cells were incubated in PBS with 5% normal FCS, 1% BSA, and0.1% sodium azide for 10 min at 4˚C. After blocking with anti-CD16/32(Fc block; BD Biosciences), CD25 and CD4 Abs were added. Cells werewashed with PBS/BSA buffer. For intracellular staining of Foxp3, cellswere fixed and permeabilized for 30 min using Foxp3 staining buffer set(eBioscience) at 4˚C. Data were collected for 30,000 events using aFACSCalibur flow cytometer and analyzed with Cell Quest software (BDImmunocytometry Systems, San Jose, CA).
Preparation of mononuclear cell suspensions from testiculardraining LNs
Suspensions of mononuclear cells (MNCs) from renal LNs were preparedby grinding the organs through a 70-mm nylon mesh. After a subsequentwashing step, the cells were suspended at a concentration of 2 3 106/ml incomplete RPMI 1640 medium (PAA, Colbe, Germany) supplemented with10% FCS (PAA), 1% MEM (Sigma), 1 mM sodium pyruvate (Life Tech-nologies), 10 mM HEPES (Life Technologies), 100 U/ml penicillin, 100mg/ml streptomycin (PAA), and 50 mm 2-mercaptoethanol (Life Tech-nologies).
Rat IL-2, IFN-g, and IL-10 ELISA
For cytokine assays, 2 3 106 MNCs from renal LNs were cultured in 1 mlcomplete RPMI 1640 medium at 37˚C, 5% CO2. After 96 h, the super-natants were collected and measured for IL-2, IFN-g, and IL-10 concen-tration using commercially available rat IL-10, IFN-g OptiEIA ELISA(BD Biosciences) or rat IL-2 DuoSet ELISA kit (R&D Systems, Wies-baden, Germany) according to the instructions of the manufacturer.
RNA isolation and real-time RT-PCR
Total RNAwas obtained using RNeasy Mini kit (Qiagen, Hilden, Germany)according to the manufacturer’s protocol. To remove genomic DNA con-tamination, isolated RNA samples were treated with RNase-free DNase I(Qiagen) for 25 min at room temperature while on the column. The totaltestis mRNA (2.5 mg) and 2 ml oligo(dT)15 primer were preincubated at70˚C for 10 min. The RT-PCR reaction mixture (buffer, 10 mM of eachdeoxyribonucleotide triphosphate, 40U recombinant RNasin RNase in-hibitor) was preheated at 42˚C for 2 min before mRNA, oligo(dT)15primer, and 200 U Moloney murine leukemia virus reverse transcriptasewere added and incubation continued for 75 min at 42˚C. The reaction wasinactivated by incubation at 70˚C for 15 min. All RT-PCR reagents wereprovided by Promega (Mannheim, Germany). The cDNA quality waschecked by amplifying the b-actin message.
Real-time quantitative PCRwas performed using an I-cycler IQ detectionsystem (Bio-Rad, Munich, Germany) in combination with QuantiTectSYBR Green PCR Master Mix (Qiagen). The thermal cycling programconsisted of an initial denaturation of 15 min at 95˚C, followed by 45 cyclesof 15 s at 94˚C, annealing 30 s at 55˚C and 30 s at 72˚C. The primers forrat MCP-1, TGF-b1, and IL-10 were purchased as QuantiTect PrimerAssays from Qiagen. Primer sequences and amplicon sizes are shown inTable I. All analyses were conducted in duplicate and the mean of theresults used for comparisons. The mRNA expression of all investigatedgenes was normalized based on the expression of the two housekeepinggenes (HKGs) b-actin and hypoxanthine phosphoribosyltransferase 1(HPRT-1). The relative expression levels were calculated by the equation22(SΔCt 2 CΔCt), where ΔCt is the difference in the Ct (threshold cycle)value between the gene of interest (GOI) and the HKG as calculated by(GOI Ct) 2 (HKG Ct). SΔCt 2 CΔCt is the difference between the SΔCt(SΔCt = experimental) and the control ΔCt (CΔCt = untreated control).Comparison of both HKGs showed no significant differences betweenexperimental groups. Data for each animal from the experimental andcontrol groups were expressed in relation to the expression found in thecorresponding untreated (N) controls. All data are presented as the mean6SEM of six to seven different testicular samples for each treatment group.
Immunofluorescence microscopy
Cryosections (12 mm) were cut, air dried, and fixed in isopropanol for 15min at –20˚C. To prevent nonspecific binding, the sections were incubatedin blocking solution (5% BSA plus 5% normal horse serum in PBS) atroom temperature for 2 h. After blocking, the sections were washed threetimes with PBS for 10 min and incubated with the primary Ab [mouse anti-rat CD68 (ED1) and CD163 (ED2) 1:50; Serotec, Oxford, U.K.] at 4˚Covernight. After rinsing in PBS/0.05% Tween 20, the slides were incubatedwith the corresponding donkey anti-mouse Cy3-conjugated secondary Ab(Dianova, Hamburg, Germany) diluted in PBS for 1 h at room temperature.In controls, the primary Abs were omitted. Finally, washed sections weremounted with Vectashield Mounting Medium containing DAPI (Vector,Burlingame, CA).
Isolation of T cells and migration (chemotaxis) assay
To test the influence of testosterone on the chemotactic activity oflymphocytes, T cells from healthy Wistar rats were isolated after centri-fugation of a splenocyte suspension on a Ficoll-Paque PLUS gradient (GEHealthcare, Uppsala, Sweden). Splenocytes were prepared by injecting thespleen with RPMI 1640 medium and grinding through a 100-mm nylonmesh. Any erythrocytes present were osmotically lysed. The leukocyteenriched fraction was washed and further purified using magnetic beadscoated with monoclonal mouse anti-rat pan T cell Ab and a MACS column(Miltenyi Biotec). The positively selected cells were collected as T cells.Cells were washed and suspended in complete serum-free RPMI 1640medium. Purity (.95%) was examined by flow cytometry using FITC-conjugated anti-CD3 and R-PE–conjugated anti-CD4 Abs (BD Bio-sciences Pharmingen, Erembodegem, Belgium). For the chemotaxis assay,Transwell cell culture inserts (pore size 3 mm; BD Falcon, Erembodegem,Belgium) were placed in serum-free RPMI 1648 medium containing 25 ng/ml rat recombinant MCP-1 (Biosource, Camarillo, CA) as chemoattractantin the lower compartment. For each experiment, 3 3 105 cells were seededon the inserts and allowed to migrate overnight while being incubatedwith increasing doses of testosterone (10–1000 nM) at 37˚C. The cellsthat migrated into the lower well were counted using CasyCounter TT(Schaerfe Systems, Reutlingen, Germany).
Influence of testosterone on T cells
To determine the direct influence of testosterone on the differentiation ofregulatory T cells (CD4+CD25+Foxp3+), T cells from healthy Wistar ratspleens were purified using the magnetic bead selection described earlier.Isolated T cells were stimulated every 24 h with different doses of tes-tosterone (10–100 nM) or with 1 mM of the androgen antagonist flutamide(Sigma) in complete RPMI 1640 medium supplemented with 10%hormone-free serum (PAA) for 92 h at 37˚C. Cells treated with vehicle(0.1% DMSO) were used as control. The counting of regulatory T cells(Tregs) was performed by flow cytometry as described earlier. A total ofeight independent experiments was assessed.
Isolation of CD4+CD252 (Tresp) cells and CD4+CD25+
(Tregs)
LN cells from renal and iliacal LNs draining the testis were isolated fromEAO+T24, Adjuvant+T24, and from EAO and adjuvant control groups.Moreover, splenic T cells from healthy Wistar rats cultivated in vitro in thepresence of 100 nM testosterone or vehicle for 92 h at 37˚C as describedearlier were also sorted. Cell preparations were stained with anti-CD4–PE,anti-CD25–FITC (BD Biosciences), and subsequently sorted by flow cy-tometry (FACSAria II Cell Sorter; BD Biosciences). The cell purity wasroutinely greater then 98%.
Splenocytes, harvested from syngeneic rats, depleted of T cells bymagnetic beads (Miltenyi Biotech, Bergisch Gladbach, Germany), wereirradiated (20 Gy) and used as costimulatory cells at 105 cells/well.
Suppression assay
CD4+CD25+ Tregs were analyzed for their suppressive capacity by usinga coculture assay in 96-well round-bottom plates (Nunc, Roskilde, Den-mark). CD4+CD252 T cells (Tresp) were cultured at constant number (105
cells/well) with 105 irradiated T cell-depleted splenocytes in the presenceof varying amounts of CD4+CD25+ T cells (Tregs) in 200 ml completeRPMI 1640 medium. Cell cultures were stimulated with 2 mg/ml anti-CD3Ab (clone G4.18; BD Biosciences) for 5 d. At the end of day 4, cells werepulsed for 18–20 h with 1 mCi/ml [3H]thymidine (GE Healthcare). Sub-sequently, the medium was removed; cells were washed twice with coldPBS and then solubilized in 0.5 M NaOH. The amount of radioactivityincorporated into DNAwas determined by liquid scintillation spectrometry
5164 TESTOSTERONE REPLACEMENT INHIBITS DEVELOPMENT OF EAO
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

(Tri-Carb 1500; Packard) and expressed as counts per minute. The sup-pressive capacity of CD4+CD25+ Tregs toward responder cells in coculturewas calculated relative to the maximum proliferation of the responder cellsalone (100 3 1 2 mean cpm coculture/mean cpm responder cells).
Statistical analysis
Results are expressed as mean6 SEM. Comparisons between groups wereassessed using the non-parametric Kruskal–Wallis one-way ANOVA or theone-way ANOVA accompanied by the Bonferroni test when applicable. Ap value ,0.05 was considered statistically significant.
ResultsTestosterone supplementation inhibits development of EAO andthe inflammatory response in the testis
The histological architecture of rat testis was analyzed in animalssupplemented 20 d after the first immunization with differentdoses (T3 and T24) of testosterone versus EAO animals having notestosterone treatment (Fig. 1). The time point of intervention waschosen to coincide with the first signs of disease (i.e., auto-antibody formation becomes evident, data not shown). The his-tological appearance of the testes (Fig. 2) showed 80% of animalsdeveloped EAO in the control group (Fig. 2F) compared with only17% in the EAO+T3 group and 33% in the EAO+T24 group (Fig.2G). The histopathological changes seen were characteristic oforchitis and included reduced height of the seminiferous epithe-lium due to germ cell loss (Fig. 2) and lymphocytic infiltrationand/or granuloma formation in the interstitium. It is noteworthythat of the 17% of EAO+T3 animals that showed signs of orchitis,the histopathological alterations were milder (e.g., the seminifer-ous epithelium remained largely intact and no granuloma forma-tion was observed). Testosterone substitution caused a clear-cutreduction of the incidence of EAO with 83% of EAO animalssupplemented with T3 (Fig. 2D) or 67% of EAO rats substitutedwith T24 (Fig. 2E) protected from the disease. Control adjuvant andtestosterone-supplemented adjuvant animals showed no patholog-ical changes in the testis (Fig. 2A, 2B, 2C, respectively). Thus,interventive testosterone treatment either completely inhibited thedevelopment of orchitis (most cases) or strongly reduced the se-verity of disease (Table I).
Effect of exogenous testosterone administration on weight oftestis and seminal vesicles
As a measure of the androgenic effect of the testosterone implants,the weight of the testes and seminal vesicles was measured.Compared with normal and control adjuvant groups, EAO andadjuvant rats with the T3 implants had significantly decreasedtesticular weights commensurate with the observed loss of sper-matogenic activity (Fig. 3A, Fig. 2D). In contrast, adjuvant andEAO rats implanted with the T24 capsule showed no difference intesticular weight (Fig. 3A) nor was spermatogenesis seeminglyaffected (Fig. 2B, 2E). The weight of seminal vesicles was sig-nificantly increased after supplementation with either T3 or T24 inall treated groups compared with that in nontreated rats. No sig-nificant changes were seen between the groups of untreated ani-mals (Fig. 3B).
Hormone levels
The elevation of testicular testosterone levels seen in EAO andadjuvant groups was significantly suppressed after 30 d of treatmentwith exogenous testosterone (Fig. 4D).EAO+T3 (7.78 6 2.41 ng/g testis), EAO+T24 (10.69 6 0.79
ng/g testis), as well as adjuvant+T3 (3.26 6 0.16 ng/g testis) andadjuvant+T24 (8.15 6 0.2 ng/g testis) groups all showed signifi-cantly lower testosterone levels compared with those in normal(38.04 6 8.83 ng/g testis), adjuvant (62.48 6 16.87 ng/g testis),and EAO (109.61 6 25.99 ng/g testis) control groups (Fig. 4D).As a consequence of the exogenous application of testosterone,LH concentrations in all groups treated with implants were alsosignificantly decreased (0.32 6 0.02, 0.28 6 0.03, 0.35 6 0.02,0.28 6 0.02 ng/ml in EAO+T3, EAO+T24, adjuvant+T3, andadjuvant+T24, respectively) compared with those in EAO (0.77 60.07 ng/ml), adjuvant (0.61 6 0.03 ng/ml), and untreated controls(0.52 6 0.03 ng/ml). Conversely, LH levels in the EAO groupwere significantly increased compared with those in all othergroups (Fig. 4B). Notably, in contrast to testicular homogenates,
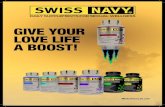
FIGURE 2. Representative testicular histology of animals substituted
with testosterone during the course of EAO. Adjuvant control animals were
supplemented with T3 (A) and T24 (B) testosterone implants 20 d after the
first immunization or no testosterone treatment was used (C). EAO group
was treated either with T3 (D) or T24 (E) testosterone implants or left
untreated (F). The table (G) shows the prevalence of animals developing
EAO in total numbers and percentages. Importantly, 83% of EAO animals
supplemented with T3 (D) or 67% of EAO rats substituted with T24 (E)
compared with 20% of EAO control rats (F) showed no pathological
changes characteristic for EAO. Adjuvant+T3 (A), adjuvant+T24 (B), as
well as adjuvant control (C) groups showed no pathological alterations.
Scale bars, 100 mm.
FIGURE 1. Schematic diagram illus-
trating the time course of treatments for
the in vivo experiments.
The Journal of Immunology 5165
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

the levels of testosterone measured directly in the interstitial fluidsurrounding the tubules and interstitial cells did not differ sig-nificantly in the EAO group compared with those in adjuvant andnormal control animals (Supplemental Fig. 1).Serum testosterone was found to be significantly elevated to
supraphysiological levels in animals supplemented with T24(16.2 6 1.24 ng/ml and 15.9 6 1.38 ng/ml in EAO and adjuvantgroups, respectively). Whereas the animals treated with T3 (3.4 60.27 and 2.74 6 0.32 ng/ml in EAO+T3 and adjuvant+T3 groups,respectively) did not show any significant changes compared withEAO control animals (2.04 6 0.19 ng/ml), the levels were sig-nificantly lower than those of the normal (5.3 6 1.12 ng/ml) andadjuvant (4.35 6 0.89 ng/ml) control groups (Fig. 4C).Serum FSH was significantly suppressed after treatment with
testosterone implants, independent of the capsule size (7.36 0.75,
7.336 0.49, 6.276 0.4, and 6.736 0.53 ng/ml in EAO+T3, EAO+T24, adjuvant+T3, and adjuvant+T24 groups, respectively), com-pared with that in normal (9.44 6 1.01 ng/ml) and adjuvant(12.38 6 0.54 ng/ml) control animals. In EAO animals with chro-nic inflammatory conditions, serum FSH level was ∼2-foldhigher (22.63 6 1.78 ng/ml) compared with that in normal un-treated rats (Fig. 4A).
Testicular macrophages, CD4+, and CD4+CD25+Foxp3 T cells
The infiltration of the testicular interstitial space by macrophagesand T cells represents a characteristic hallmark of EAO histopa-thology. In the large cohort of EAO animals, where disease de-velopment was prevented by supplementation with T3 or T24, theaccumulation of macrophages (ED1/ED2) was unchanged incomparison with that of adjuvant or untreated control groups. Asa consequence, substantially less infiltration of testicular macro-phages was seen compared with that in the orchitis animals (EAOcontrols, Fig. 5). The histological assessment was corroborated bythe flow cytometric measurement of the number of CD4+ T cells,which showed significantly fewer cells in EAO rats supplementedwith T24. A moderate decrease was also found in the EAO+T3group compared with that in the EAO-only animals (Fig. 6A).Notably, the number of immunosuppressive Tregs (CD4+CD25+
Foxp3) in the testis of EAO+T24 animals was significantly in-creased compared with the numbers seen in the EAO controls(Fig. 6B).
Quantification of testicular mRNA expression for MCP-1, IL-6,IL-10, TNF-a, and TGF-b1
The expression of the chemokine MCP-1 mRNA was highly up-regulated (80-fold) in the EAO group compared with the levels inadjuvant and normal controls. After testosterone supplementation,MCP-1 was significantly reduced in both the EAO+T3 and EAO+T24 groups compared with that in the EAO control group (Fig. 7A).In EAO rats, expression levels of the proinflammatory cytokinesTNF-a (Fig. 7B) and IL-6 (Fig. 7C) were elevated ∼20-fold incomparison with untreated and adjuvant controls. Supplementa-tion with T3 and T24 (EAO+T3 and EAO+T24 groups) resulted insubstantial but statistically non-significant reduction (∼50%) ofTNF-a and IL-6 expression compared with that in EAO ratswithout hormone intervention (Fig. 7B, 7C). The mRNA expres-sion of the regulatory cytokine IL-10 was significantly suppressedin the EAO+T3 group and decreased substantially in the EAO+T24 group compared with that in EAO controls (Fig. 7D). Theexpression of constitutively expressed TGF-b1 in the testis re-mained unaffected in all investigated groups (Fig. 7E). Controladjuvant animals treated with testosterone did not show any sig-nificant changes compared with normal untreated rats in any factorinvestigated (Fig. 7).
FIGURE 3. Weight (g) of testosterone-dependent organs: (A) testis, (B)
seminal vesicles in EAO and adjuvant animals supplemented with testos-
terone (EAO+T3, EAO+T24, adjuvant+T3, adjuvant+T24, respectively), as
well as in EAO, adjuvant, and normal control rats without testosterone
substitution. Data are expressed as mean 6 SEM (n = 5 to 7 animals/
group). Values with different superscript letters differ significantly com-
pared with EAO control group: ap . 0.05 (NS), bp , 0.01, cp , 0.001.
Table I. Primers used in quantitative real-time RT-PCR experiments in this study
Gene PrimerCatalog Number
(Qiagen)EntrezGene ID
Product Length(bp)
b-Actin Sense 59-ATGGTGGGTATGGGTCAGAA-39 — 81822 232Anti-sense 59-GGGTCATCTTTTCACGGTTG-39 —
HPRT-1 Sense 59-TCT GTC ATG TCG ACC CTC AG-39 — 24465 109Anti-sense 59-CCT TTT CCA AAT CTT CAG CA-39 —
TNF-a Sense 59-GCC TCT TCT CAT TCC TGC TC-39 — 24835 101Anti-sense 59-CCC ATT TGG GAA CTT CTC CT-39 —
CCL2 (MCP-1) QuantiTect Primer Assay QT00183253 24770 117TGF-b1 QuantiTect Primer Assay QT00187796 59086 145IL-6 QuantiTect Primer Assay QT00182896 24498 128IL-10 QuantiTect Primer Assay QT00177618 25325 69
5166 TESTOSTERONE REPLACEMENT INHIBITS DEVELOPMENT OF EAO
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

Secretion of Th1/Th2 cytokines (IL-2, IFN-g, and IL-10) byMNCs from testicular draining LNs
In EAO+T3 animals, the level of the proinflammatory Th1 cyto-kines IL-2 and IFN-g was significantly downregulated as was theexpression of IL-2 in EAO+T24 rats (Fig. 8A, 8B). EAO ratsshowed a strong upregulation of IL-10 compared with that innormal or adjuvant controls (Fig. 8C), which was reduced (not tothe level of statistical significance) in EAO rats treated with tes-tosterone (EAO+T3, EAO+T24) (Fig. 8C). LN cells from adjuvant
and normal control groups showed no significant differences in thesecretion level of investigated cytokines (Fig. 8).
Influence of testosterone on migration of T cells
In the presence of increasing concentrations of testosterone, adose-dependent migration of T cells toward the MCP-1 gradientwas observed. Incubation of cells with 100 nM testosteronesignificantly increased the MCP-1–stimulated chemotactic activ-ity of T cells, whereas 1000 nM testosterone had no influence(Fig. 9). Testosterone alone showed no effect on the chemotaxisof T cells (data not shown). Thus, testosterone required the pre-sence of MCP-1 to show its additive effect on chemotaxis.
Testosterone stimulates in vitro generation of Tregs
As the in vivo supplementation of EAO animals with testosteroneinhibited the development of testicular inflammation and in-duced an increase in the number of CD4+CD25+Foxp3+ Tregs inthe testis, we further investigated whether testosterone has adirect effect on the generation of Tregs from naive T cells. Invitro treatment of purified splenic T cells from healthy animalsgiven different doses of testosterone showed a prominent ex-pansion of the CD4+CD25+Foxp3 population within CD4+ T cells.Doses of 10 and 100 nM testosterone induced a 3- and 2.7-foldincrease in the percentage of Tregs in the total population ofT cells, respectively. This effect was abolished by the additionof the androgen antagonist flutamide (Fig. 10).
Suppressive capacity of Tregs expanded by testosterone in vitro
To determine the suppressive capacity of in vitro-cultivated Tregson the proliferative activity of Teffector cells, highly purified CD4+
CD252 and CD4+CD25+ T cells were cocultivated and polyclonal
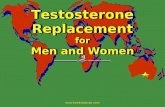
FIGURE 4. Serum FSH (A), serum LH (B), serum testosterone (C), and testicular testosterone levels (D) in EAO and adjuvant animals supplemented with
testosterone (EAO+T3, EAO+T24, adjuvant+T3, adjuvant+T24, respectively) during the development of orchitis and in control EAO, adjuvant, and normal
untreated groups. Hormone levels were measured by RIA in serum and testes of rats immunized with testicular homogenate and adjuvant and substituted
with T3 or T24 implants (EAO+T3, EAO+T24), as well as in respective control animals. Data are expressed as mean 6 SEM (n = 6 to 13 rats/group).
Values with different superscript letters differ significantly compared with EAO control group: ap . 0.05 (NS), bp , 0.05, cp , 0.01, dp , 0.001. T,
testosterone.
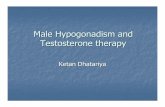
FIGURE 5. Immunofluorescence staining of testicular macrophages
using combined Abs directed against ED1 and ED2 in frozen sections of
animals supplemented with testosterone [(A) adjuvant+T3, (B) adjuvant+
T24, (D) EAO+T3, (E) EAO+T24] and in control animals without tes-
tosterone substitution [(F) EAO and (C) adjuvant]. In contrast to EAO
testis (F), no visible accumulation of macrophages is evident in EAO+T3
(D) and EAO+T24 (E) compared with that in adjuvant controls (A–C).
Scale bars, 100 mm.
The Journal of Immunology 5167
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

stimulated in the presence of irradiated splenocytes and anti-CD3Ab. In our setup, the CD4+CD25+ cells sorted from vehicle as welltestosterone-treated T cell in vitro culture showed typical Tregcharacteristics (i.e., hyporesponsiveness toward TCR stimulationand the ability to suppress the proliferation of Tresp cells) (Fig.11). Coculture of Tregs with Tresp cells from vehicle- as well astestosterone-treated cells resulted in reduced proliferation of Trespcells with the strongest suppression of proliferation (∼90%) atthe cell ratio 1:1. Tregs sorted from in vitro testosterone-treatedT cells showed a similar level of suppression; however, suppres-sive activity was stronger in view of the 3-fold higher proliferativecapacity of CD4+CD252 T cells from testosterone-treated culture(Fig. 11C) compared with vehicle-treated cells (Fig. 11A).Moreover, CD4+CD25+ T cells purified from testicular draining
LNs from EAO and adjuvant animals supplemented with T24as well as CD4+CD25+ T cells purified from EAO and adjuvantcontrol animals demonstrated inhibitory potential on the prolif-eration of CD4+CD252 Tresp cells. Of note, at a Tresp/Treg ratioof 10:1, the inhibitory activity of Tregs isolated from EAO+T24animals (86%) was much higher than that in those obtained fromEAO rats (34%). With increasing ratio of Tregs in the assay, thesuppressive activity is similar in all groups (Supplemental Fig. 2).
DiscussionIn the past few years, various experimental and clinical studieshave provided evidence for a possible immunosuppressive role fortestosterone. These recent studies have built upon the findings ofprevious animal investigations that showed that castration and the
associated deprivation of androgens aided in the development andexacerbated the consequences of experimental autoimmune dis-eases such as EAE, diabetes, thyroiditis, and adjuvant arthritis (29–31, 34, 43). In contrast, the provision of testosterone to females,
FIGURE 7. Relative mRNA expression of MCP-1 (A), TNF-a (B), IL-6
(C), IL-10 (D), and TGF-b1 (E) in testes from EAO and adjuvant rats
treated with T3 and T24 testosterone implants (EAO+T3, EAO+T24, ad-
juvant+T3, adjuvant+T24) and in normal, adjuvant, and EAO controls
without testosterone substitution. b-Actin was used for normalization of
expression data. Values are mean 6 SEM of relative expression units (RE)
of results for five to seven animals in each group. Values with different
superscript letters differ significantly compared with respective controls.ap . 0.05 (NS), bp . 0.05.
FIGURE 6. Presence of CD4+ (A) and regulatory CD4+CD25+Foxp3+
T cells (B) in the interstitial compartment of animals supplemented with
testosterone (EAO+T3, EAO+T24, adjuvant+T3, adjuvant+T24) and in
control animals without testosterone substitution (EAO, adjuvant, normal)
analyzed by FACS. Data are expressed as mean 6 SEM. Values with
different superscript letters differ significantly compared with EAO control
group (n = 5 to 7). ap . 0.05 (NS), bp , 0.05, cp , 0.05.
5168 TESTOSTERONE REPLACEMENT INHIBITS DEVELOPMENT OF EAO
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

generally more prone to autoimmunity than males, was shown toameliorate symptoms in a variety of autoimmune disease models(31, 32, 44). As the reduction of serum testosterone levels is acommon feature in systemic and acute testicular inflammation inhumans and experimental animal models alike, we investigatedwhether androgen supplementation at the onset of EAO could in-fluence the course and severity of the disease.Testosterone secreted by Leydig cells under the influence of
pituitary LH acts on the seminiferous epithelium to promotespermatogenesis. In our study, the administration of T3 implant asexpected resulted in the reduction of serum gonadotropin levelsbelow those necessary to sustain spermatogenesis. In contrast, thehigher-dose T24 implants cause supraphysiological serum con-centrations and resulted in sufficient levels (10–40% of normaltesticular levels) to support qualitatively normal seminiferous tu-bule function (40, 45, 46). The histological assessment of thetreated animals clearly showed that testosterone replacementprovided a significant degree of protection against the devel-opment of orchitis with only 17% of EAO+T3 and 33% of EAO+
T24 animals developing the disease, compared with 80% when nohormone intervention was performed. Furthermore, in the treatedanimals that did develop EAO, testosterone was found to reducestrongly the severity of disease, a finding that mirrors that seen inEAE where oral testosterone administration in castrated animalsreversed the clinical symptoms of the disease (47).Our data suggest that the presence of heightened testosterone
levels exerts a multifactorial influence resulting in a number ofsignificant modifications, all of which collectively constitute theobserved immunoprotective response. First, we found that testos-terone effectively inhibited the accumulation of macrophages andCD4+ lymphocytes while simultaneously selectively increasingthe number of immunosuppressive Tregs (CD4+CD25+Foxp3+) inthe testicular interstitial space. Second, testosterone supplementa-tion inhibited mRNA expression and as a corollary the presence ofproinflammatory cytokines (TNF-a, IL-6) and chemokines (MCP-1) in the testis. Finally, we found that its influence goes beyond thelocal (testicular) level, as systemically testosterone decreased thesecretion of the Th1 cytokines IFN-g and IL-2 seen in MNCs fromtesticular draining LNs. In shifting the balance of Th1/Th2 cyto-kines, a T cell-driven autoimmune response is inhibited thus pre-venting an excessive proinflammatory response and the ensuingtissue damage.The subtly of testosterone actions is illustrated by the finding that
although it prevented accumulation, the number of macrophagespresent in the testis was unaffected, yet the composition of immunecells present was altered; namely, heightened numbers of Tregs.The ability of testosterone to induce this transformation was clearlydemonstrated by our novel finding that in vitro after testosteronetreatment, CD4+CD25+Foxp3+ Tregs were derived from splenicCD4+ T lymphocytes. Furthermore, we showed that testosterone-derived Tregs were very effective in the inhibition of proliferativeresponses of effector T cells showing a higher capacity than Tregsisolated from vehicle control. This is of particular importance,considering Tregs are known both for their potent regulatory ca-pacity in controlling autoimmunity and their protective role againstimmunity-induced pathology (48). In conjunction with our func-tional studies, our finding that the CD4+CD25+ cells from the treatedanimals express Foxp3, the master regulator for the Treg lineage,indicates that these cells fulfill their role in the maintenance ofself-tolerance and tissue homeostasis in vivo. Conversely, othershave shown that although increased numbers of CD4+ and CD8+
effector Tregs are found in EAO (49) and various autoimmunediseases (50–52), their presence alone was insufficient to inhibitdisease development. As in our study, Jacobo et al. (49) reportedincreased CD4+ T cells with a concomitant proportional increaseof CD4+CD25+Foxp3+ Tregs in EAO testes. Thus, the relativeproportion of two subsets of cells remained unchanged. Thiscould explain why in EAO, the recorded absolute increase in Treg
FIGURE 9. Influence of testosterone on the chemotactic activity of
T cells. Cells were cultivated in medium containing 10, 100, or 1000 nM of
testosterone for 24 h at 37˚C. Values were normalized by setting T cells
without testosterone treatment to 100%. Values are mean6 SEM of results
from five independent experiments: *p , 0.05. T, testosterone.
FIGURE 8. Secretion of the Th1 cytokines IL-2 (A), IFN-g (B), and of
the regulatory Th2 cytokine IL-10 (C) by MNCs from testicular draining
LNs from EAO and adjuvant rats treated with T3 and T24 testosterone
implants (EAO+T3, EAO+T24, adjuvant+T3, adjuvant+T24) and in nor-
mal, adjuvant, and EAO controls without testosterone substitution. Cyto-
kine values are presented in picograms per milliliter as the mean 6 SEM
(n = 5 to 7) concentration from duplicate wells in each experiment, re-
spectively. Values with different superscript letters differ significantly
compared with EAO control group. ap . 0.05 (NS), bp , 0.05.
The Journal of Immunology 5169
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

numbers was ineffective in preventing disease outbreak. The addi-tion of testosterone, regardless of quantity, not only resulted in theincreased absolute number of Tregs, but also, compared with thatof the EAO-only animals, the Tregs constituted a higher propor-tion of the CD4+ lymphocyte population. Considering their pur-ported inhibitory abilities, this increase could provide an expla-nation as to how testosterone prevented the onset of EAO in themajority of treated rats. A further insight into the importance ofthe relative proportions of the differing types of T lymphocyte is
shown by the finding that the CD8+ effector population increasedmore than CD4+Foxp3+ Tregs during EAO. This imbalance couldbe sufficient to overwhelm the immunosuppressive actions ofCD4+Foxp3+ Treg function and thus lead to chronic testicularinflammation (49).Further evidence of testosterone’s involvement in a multifaceted
immunoprotective mechanism during EAO is the dual nature ofits subversion of the role of the chemokine MCP-1 during in-flammation. We found that the presence of testosterone, on the
FIGURE 11. Functional Treg suppressor
assay. CD4+CD252 (Tresp) and CD4+CD25+
(Treg) T cells from splenic T cells cultivated
in the presence of vehicle (A, B) or 100 nM
testosterone (C, D) were sorted by FACS and
cultivated for 5 d at different Tresp/Treg ratios
as indicated. Cells were stimulated with sol-
uble anti-CD3 (2 mg/ml) in the presence of
irradiated T cell-depleted splenocytes (1 3105). Proliferation of T cells was assessed by
standard [3H]thymidine incorporation and is
displayed as counts per minute. Level of
suppression of Tresp proliferation was calcu-
lated for several ratios of Tresp/Tregs com-
pared with culture of Tresp cells alone (sup-
pression = 0%). Data are the mean 6 SEM of
three independent experiments.
FIGURE 10. Testosterone-dependent differentiation of Tregs (CD4+CD25+Foxp3+) from naive T cells in vitro. A, Contour plots showing the percentage
of CD4+CD25+Foxp3+ cells within the total population of T cells. Isolated splenic T cells were incubated either alone or with 10 and 100 nM testosterone
(T) as well as with 100 nM testosterone and its antagonist flutamide (1 mM; Flut) for 92 h at 37˚C. B, Expression of Foxp3+ cells was normalized on vehicle
stimulated T cells, which were set to 100%. In all graphs, data are representative of eight independent experiments. Data are shown for cells gated on CD4+.
*p , 0.05 compared with vehicle.
5170 TESTOSTERONE REPLACEMENT INHIBITS DEVELOPMENT OF EAO
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

mRNA level, significantly decreased the level of expression andon the functional level ameliorated MCP-1–induced chemotaxisin vitro. In orchitis, high MCP-1 levels ameliorated by testosterone,which is found strongly elevated in testicular homogenates andclose to normal in testicular interstitial fluid, may concert the im-migration of leukocytes. In contrast, in testosterone-supplementedanimals, MCP-1 mRNA levels are reduced and testicular testos-terone concentrations are significantly lower than in EAO or evenuntreated controls. This observation may explain the lack of in-terstitial macrophage accumulation in the treated animals, which isotherwise characteristic of orchitis. Although our results may beindicative, our in vitro findings need to be cautiously interpreted fortheir role in vivo, also in view of the fact that in the chemotaxisexperiments, we studied T cells and not macrophages.Furthering the hypothesis that testosterone directly influences
LPS-induced production of TNF-a, IL-6, and MCP-1 by testicularmacrophages, we found that mRNA expression levels for thesegenes were significantly inhibited by 1000 nM testosterone in vitro(data not shown). Systemically, a T cell autoimmune responseis initiated in the draining LNs where dendritic cells presentcaptured autoantigens to naive T lymphocytes in the presenceof Th1 cytokines such as IL-2 and IFN-g. We were able to dem-onstrate clearly that the strongly elevated secretion of IL-2 andIFN-g, which is characteristic of orchitis, was suppressed almostto adjuvant control levels in testosterone-treated EAO animalswith the exception of IFN-g in EAO+T24. Thus, an essentialstimulus to trigger a T cell-based cellular autoimmune responseis lacking and may add on the systemic level to the local immu-nosuppressive mechanism elicited by testosterone treatment. Insupport, the increased incidence of EAO in animals treated withT24 (33% responders) compared with T3 (17% responders) maybe attributed to the larger implant’s inability to suppress the ex-pression of IFN-g with a concomitant inhibited IL-2 synthesisseen for both implants.In summary, our results demonstrate that testosterone supple-
mentation exerts a multifaceted protective effect during EAO de-velopment. Mechanistically, this is mediated systemically by theinhibition of Th1-specific cytokine production in testicular drainingLNs. In the testis itself, testosterone appears to induce an expansionof suppressive Tregs from naive T cells leading to an overpropor-tional representation of Tregs within the CD4+ T cell populationwhile simultaneously inhibiting the synthesis of proinflammatorymediators MCP-1, TNF-a, and IL-10. Clearly, the exact proportionof systemic and local actions of testosterone requires further elu-cidation. Taken together, these findings suggest that testosteroneplays an important role in the maintenance of immunologicalbalance in the testis and point to a previously unrecognized role oftestosterone in the differentiation of Tregs.
AcknowledgmentsWe thank Dr. Con Mallidis for critical reading of the manuscript. We thank
Dr. Nelli Baal and Gaby Haley from the Cell Sorting Co-Facility at the In-
stitute for Clinical Immunology and Transfusion Medicine, Justus-Liebig-
University Giessen for excellent help.
DisclosuresThe authors have no financial conflicts of interest.
References1. Whiteford, L. M., and L. Gonzalez. 1995. Stigma: the hidden burden of in-
fertility. Soc. Sci. Med. 40: 27–36.2. WHO. 1987. Towards more objectivity in diagnosis and managment of male
infertility. Int. J. Androl. 7(Suppl.): 1–53.3. Nieschlag, E., and H. Behre. 2000. Andrology. Male Reproductive Health and
Dysfunction. Springer, Berlin.
4. Schuppe, H. C., A. Meinhardt, J. P. Allam, M. Bergmann, W. Weidner, andG. Haidl. 2008. Chronic orchitis: a neglected cause of male infertility? Andro-logia 40: 84–91.
5. Schuppe, H. C., and A. Meinhardt. 2005. Immune privilege and inflammation ofthe testis. Chem. Immunol. Allergy 88: 1–14.
6. Haidl, G., J. P. Allam, and H. C. Schuppe. 2008. Chronic epididymitis: impact onsemen parameters and therapeutic options. Andrologia 40: 92–96.
7. Weidner, W., G. M. Colpi, T. B. Hargreave, G. K. Papp, J. M. Pomerol,C. Ghosh; EAU Working Group on Male Infertility. 2002. EAU guidelines onmale infertility. Eur. Urol. 42: 313–322.
8. Osegbe, D. N. 1991. Testicular function after unilateral bacterial epididymo-orchitis. Eur. Urol. 19: 204–208.
9. Fijak, M., and A. Meinhardt. 2006. The testis in immune privilege. Immunol.Rev. 213: 66–81.
10. Weidner, W., C. Garbe, L. Weissbach, J. Harbrecht, K. Kleinschmidt, H. G. Schiefer,and H. J. Friedrich. 1990. [Initial therapy of acute unilateral epididymitis usingofloxacin. II. Andrological findings]. Urologe A 29: 277–280.
11. Tung, K. S., and C. Teuscher. 1995. Mechanisms of autoimmune disease in thetestis and ovary. Hum. Reprod. Update 1: 35–50.
12. Rival, C., M. S. Theas, M. O. Suescun, P. Jacobo, V. Guazzone, N. van Rooijen,and L. Lustig. 2008. Functional and phenotypic characteristics of testicularmacrophages in experimental autoimmune orchitis. J. Pathol. 215: 108–117.
13. Iosub, R., J. Klug, M. Fijak, E. Schneider, S. Frohlich, K. Blumbach,G. Wennemuth, C. P. Sommerhoff, M. Steinhoff, and A. Meinhardt. 2006. De-velopment of testicular inflammation in the rat involves activation of proteinase-activated receptor-2. J. Pathol. 208: 686–698.
14. Rival, C., L. Lustig, R. Iosub, V. A. Guazzone, E. Schneider, A. Meinhardt, andM. Fijak. 2006. Identification of a dendritic cell population in normal testis andin chronically inflamed testis of rats with autoimmune orchitis. Cell Tissue Res.324: 311–318.
15. Guazzone, V. A., P. Jacobo, M. S. Theas, and L. Lustig. 2009. Cytokines andchemokines in testicular inflammation: A brief review. Microsc. Res. Tech. 72:620–628.
16. Fijak, M., R. Iosub, E. Schneider, M. Linder, K. Respondek, J. Klug, andA. Meinhardt. 2005. Identification of immunodominant autoantigens in rat au-toimmune orchitis. J. Pathol. 207: 127–138.
17. Guazzone, V. A., C. Rival, B. Denduchis, and L. Lustig. 2003. Monocyte che-moattractant protein-1 (MCP-1/CCL2) in experimental autoimmune orchitis. J.Reprod. Immunol. 60: 143–157.
18. Theas, M. S., C. Rival, S. Jarazo-Dietrich, P. Jacobo, V. A. Guazzone, andL. Lustig. 2008. Tumour necrosis factor-alpha released by testicular macro-phages induces apoptosis of germ cells in autoimmune orchitis. Hum. Reprod.23: 1865–1872.
19. Doncel, G. F., J. A. Di Paola, and L. Lustig. 1989. Sequential study of the his-topathology and cellular and humoral immune response during the developmentof an autoimmune orchitis in Wistar rats. Am. J. Reprod. Immunol. 20: 44–51.
20. Lustig, L., L. Lourtau, R. Perez, and G. F. Doncel. 1993. Phenotypic charac-terization of lymphocytic cell infiltrates into the testes of rats undergoing au-toimmune orchitis. Int. J. Androl. 16: 279–284.
21. Suescun, M. O., R. S. Calandra, and L. Lustig. 1994. Alterations of testicularfunction after induced autoimmune orchitis in rats. J. Androl. 15: 442–448.
22. Bouman, A., M. J. Heineman, and M. M. Faas. 2005. Sex hormones and theimmune response in humans. Hum. Reprod. Update 11: 411–423.
23. Snider, H., C. Lezama-Davila, J. Alexander, and A. R. Satoskar. 2009. Sexhormones and modulation of immunity against leishmaniasis. Neuro-immunomodulation 16: 106–113.
24. Orton, S. M., B. M. Herrera, I. M. Yee, W. Valdar, S. V. Ramagopalan,A. D. Sadovnick, G. C. Ebers; Canadian Collaborative Study Group. 2006. Sex ratioof multiple sclerosis in Canada: a longitudinal study. Lancet Neurol. 5: 932–936.
25. Duquette, P., J. Pleines, M. Girard, L. Charest, M. Senecal-Quevillon, andC. Masse. 1992. The increased susceptibility of women to multiple sclerosis.Can. J. Neurol. Sci. 19: 466–471.
26. Whitacre, C. C., S. C. Reingold, and P. A. O’Looney. 1999. A gender gap inautoimmunity. Science 283: 1277–1278.
27. Gold, S. M., and R. R. Voskuhl. 2009. Estrogen and testosterone therapies inmultiple sclerosis. Prog. Brain Res. 175: 239–251.
28. Swerdloff, R. S., and C. Wang. 2004. Androgens and the ageing male. BestPract. Res. Clin. Endocrinol. Metab. 18: 349–362.
29. Fitzpatrick, F., F. Lepault, F. Homo-Delarche, J. F. Bach, and M. Dardenne.1991. Influence of castration, alone or combined with thymectomy, on the de-velopment of diabetes in the nonobese diabetic mouse. Endocrinology 129:1382–1390.
30. Bebo, B. F., Jr., E. Zelinka-Vincent, G. Adamus, D. Amundson, A. A. Vandenbark,and H. Offner. 1998. Gonadal hormones influence the immune response to PLP139-151 and the clinical course of relapsing experimental autoimmune encepha-lomyelitis. J. Neuroimmunol. 84: 122–130.
31. Fox, H. S. 1992. Androgen treatment prevents diabetes in nonobese diabeticmice. J. Exp. Med. 175: 1409–1412.
32. Dalal, M., S. Kim, and R. R. Voskuhl. 1997. Testosterone therapy amelioratesexperimental autoimmune encephalomyelitis and induces a T helper 2 bias in theautoantigen-specific T lymphocyte response. J. Immunol. 159: 3–6.
33. Ansar Ahmed, S., P. R. Young, and W. J. Penhale. 1986. Beneficial effect oftestosterone in the treatment of chronic autoimmune thyroiditis in rats. J.Immunol. 136: 143–147.
34. Harbuz, M. S., Z. Perveen-Gill, S. L. Lightman, and D. S. Jessop. 1995. Aprotective role for testosterone in adjuvant-induced arthritis. Br. J. Rheumatol.34: 1117–1122.
The Journal of Immunology 5171
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

35. Bebo, B. F., Jr., J. C. Schuster, A. A. Vandenbark, and H. Offner. 1999.Androgens alter the cytokine profile and reduce encephalitogenicity of myelin-reactive T cells. J. Immunol. 162: 35–40.
36. Liva, S. M., and R. R. Voskuhl. 2001. Testosterone acts directly on CD4+T lymphocytes to increase IL-10 production. J. Immunol. 167: 2060–2067.
37. Head, J. R., and R. E. Billingham. 1985. Immune privilege in the testis. II.Evaluation of potential local factors. Transplantation 40: 269–275.
38. Sun, Y. T., D. M. Robertson, G. Gonzales, G. P. Risbridger, and D. M. de Kretser.1989. Effect of testosterone on serum immunoactive inhibin concentrations inintact and hypophysectomized male rats. J. Reprod. Fertil. 87: 795–801.
39. Sun, Y. T., N. G. Wreford, D. M. Robertson, and D. M. de Kretser. 1990.Quantitative cytological studies of spermatogenesis in intact and hypophysec-tomized rats: identification of androgen-dependent stages. Endocrinology 127:1215–1223.
40. Wang, J., N. G. Wreford, H. Y. Lan, R. Atkins, and M. P. Hedger. 1994. Leu-kocyte populations of the adult rat testis following removal of the Leydig cells bytreatment with ethane dimethane sulfonate and subcutaneous testosteroneimplants. Biol. Reprod. 51: 551–561.
41. Hoffmann, B., and A. Landeck. 1999. Testicular endocrine function, seasonalityand semen quality of the stallion. Anim. Reprod. Sci. 57: 89–98.
42. Rival, C., V. A. Guazzone, W. von Wulffen, H. Hackstein, E. Schneider,L. Lustig, A. Meinhardt, and M. Fijak. 2007. Expression of co-stimulatorymolecules, chemokine receptors and proinflammatory cytokines in dendriticcells from normal and chronically inflamed rat testis. Mol. Hum. Reprod. 13:853–861.
43. Ahmed, S. A., and W. J. Penhale. 1982. The influence of testosterone on thedevelopment of autoimmune thyroiditis in thymectomized and irradiated rats.Clin. Exp. Immunol. 48: 367–374.
44. Sato, E. H., H. Ariga, and D. A. Sullivan. 1992. Impact of androgen therapy inSjogren’s syndrome: hormonal influence on lymphocyte populations and Ia
expression in lacrimal glands of MRL/Mp-lpr/lpr mice. Invest. Ophthalmol. Vis.Sci. 33: 2537–2545.
45. McLachlan, R. I., N. G. Wreford, S. J. Meachem, D. M. De Kretser, andD. M. Robertson. 1994. Effects of testosterone on spermatogenic cell pop-ulations in the adult rat. Biol. Reprod. 51: 945–955.
46. Meinhardt, A., M. Bacher, C. Metz, R. Bucala, N. Wreford, H. Lan, R. Atkins,and M. Hedger. 1998. Local regulation of macrophage subsets in the adult rattestis: examination of the roles of the seminiferous tubules, testosterone, andmacrophage-migration inhibitory factor. Biol. Reprod. 59: 371–378.
47. Maccio, D. R., G. Calfa, and G. A. Roth. 2005. Oral testosterone in male ratsand the development of experimental autoimmune encephalomyelitis. Neuro-immunomodulation 12: 246–254.
48. Sakaguchi, S., N. Sakaguchi, M. Asano, M. Itoh, and M. Toda. 1995. Immu-nologic self-tolerance maintained by activated T cells expressing IL-2 receptoralpha-chains (CD25). Breakdown of a single mechanism of self-tolerance causesvarious autoimmune diseases. J. Immunol. 155: 1151–1164.
49. Jacobo, P., V. A. Guazzone, S. Jarazo-Dietrich, M. S. Theas, and L. Lustig. 2009.Differential changes in CD4+ and CD8+ effector and regulatory T lymphocytesubsets in the testis of rats undergoing autoimmune orchitis. J. Reprod. Immunol.81: 44–54.
50. Cao, D., V. Malmstrom, C. Baecher-Allan, D. Hafler, L. Klareskog, andC. Trollmo. 2003. Isolation and functional characterization of regulatoryCD25brightCD4+ T cells from the target organ of patients with rheumatoidarthritis. Eur. J. Immunol. 33: 215–223.
51. Mottonen, M., J. Heikkinen, L. Mustonen, P. Isomaki, R. Luukkainen, andO. Lassila. 2005. CD4+ CD25+ T cells with the phenotypic and functionalcharacteristics of regulatory T cells are enriched in the synovial fluid of patientswith rheumatoid arthritis. Clin. Exp. Immunol. 140: 360–367.
52. Dejaco, C., C. Duftner, B. Grubeck-Loebenstein, and M. Schirmer. 2006. Im-balance of regulatory T cells in human autoimmune diseases. Immunology 117:289–300.
5172 TESTOSTERONE REPLACEMENT INHIBITS DEVELOPMENT OF EAO
by guest on April 14, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from