Testicular tumors
98
TESTICULAR TUMORS Dr Pankaj Bharadva
-
Upload
pankaj-bharadva -
Category
Education
-
view
1.351 -
download
1
Transcript of Testicular tumors

TESTICULAR TUMORS
Dr Pankaj Bharadva

INTRODUCTION INTRODUCTION
Most common malignancy in the age group of 15-35 males.
Improved survival due to variety of reasons.
- accurate tumor markers - improved diagnostic techniques - effective chemotherapy - well defined tumor biology
99% of tumors are malignant.

More common in higher socioeconomic classes.
More common on Right side than left (cryptorchidism --- Rt > Lt).
In primary testicular tumors, 1-2% bilateral.
Seminoma most common GCT in B/L primary testicular tumors.
Malignant lymphoma most common B/L tumor of testis.

They are divided into two major categories:
1)Germ cell tumors → Approximately 95% of testicular tumors
2)Sex cord– stromal tumors
Most germ cell tumors are aggressive cancers → capable of rapid & wide dissemination, although → current therapy most can be cured
In contrast → Sex cord–stromal tumors are generally benign

RISK FACTORSRISK FACTORSCongenital:
Cryptorchidism
7-10% of all testicular tumors, 3-14 times
Relative risk : intraabdominal highest 1 in20, inguinal lowest 1 in 80
Seminoma is the commonest tumor in this group.

Acquired :
Trauma
Exogenous estrogens (mother while pregnancy)
Infection related testicular atrophy

Family predispositionFamily predispositionDevelopment of testicular germ cell tumors →
strong family predisposition
The relative risk of development of these tumors in fathers & sons → 4 times higher than normal, and 8-10 times higher between brothers
Genetic polymorphisms at Xq27 locus → may be responsible for this susceptibility
7

CLASSIFICATIONCLASSIFICATION1. WHO CLASSIFICATION.
Germ cell tumors:90-95%
* Pure forms. - Seminoma - Embryonal Carcinoma - Yolk sac tumors - Trophoblastic tumors - Teratoma
* Mixed forms

Gonadal stromal tumors
- leydig cell tumor - sertoli cell tumor
Both germ cell and stromal elements
- Gonadoblastoma

2. ACCORDING TO CELL TYPE
Seminoma Teratoma
differetiated.(TD) intermediate(MTI) anaplastic (MTA): embryonal
carcinoma trophoblastic(MTT):choriocarcinoma

Secondary tumors
Lymphoid and hemopoietic tumors - lymhoma - leukemia
Tumors of collecting ducts and rete
Tumors of tunica,epididymis,cord and appendices
Soft tissue tumors
Tumors like lesions -orchitis -epidermal cyst -sperm granuloma

Germ Cell TumorsGerm Cell Tumors Incidence of testicular tumors in the USA → 6
per 100,000 → 300 deaths per year
For unexplained reasons → worldwide increase in the incidence
In the 15- to 34-year age group, they constitute the most common tumor of men → 10% of all cancer deaths
In the USA → much more common in whites than in blacks
12

TUMORIGENIC MODEL FOR GCTTUMORIGENIC MODEL FOR GCT
C h oriocarc in om a( Trop h b las tic p a th w ays )
Y o lk sac tu m or(Y o lk sac p a th w ay)
E xtraem b ryon ic d iffe ren tia tion
Tera tom a
In traem b royon ic d iffe ren t ia tion
E m b ryon a l ca rc in om a( To tip o ten t tu m or ce ll)
To tip o ten t g e rm ce ll sem in om a
N orm al s p e rm atocyte

PathogenesisPathogenesisMost testicular germ cell tumors
originate from lesions called intratubular germ cell neoplasia (ITGCN or IGCN) or ITGCN unclassified (ITGCNU or IGCNU)
However, ITGCN has not been implicated as a precursor lesion of pediatric yolk sac tumors and teratomas, or of adult spermatocytic seminoma.
ITGCN is believed to occur → in utero and stay dormant until puberty
14

ITGCNITGCN The lesion consists of: Atypical Primodal Germ Cells with large nuclei
and clear cytoplasm → twice the size of normal germ cells.
Retain the expression of OCT3/4 and NANOG, which are associated with pluripontentiality
50% → develop invasive germ cell tumors within five years after diagnosis → practically all patients with ITGCN eventually develop invasive tumors.
ITGCN is essentially a type of carcinoma in situ (CIS), although the term CIS is not frequently used to refer to this lesion.
15

ITGCNITGCN ITGCN share some of the genetic alterations found
in germ cell tumors such as the gain of additional copies of the short arm of chromosome 12 (12p) in the form of an isochromosome of its short arm, i(12p).
This change is invariably found in invasive tumors regardless of histological type.
Activating mutations of c-KIT, which may be present in seminomas, are also present in ITGCN.
16

SeminomaSeminoma Most common type of germ cell tumor (50%)
Peak incidence → 3rd decade & almost never occur in infants
Identical tumor in ovary → dysgerminoma
Seminomas contain → an isochromosome 12p and express OCT3/4 & NANOG
25% of these tumors → c-KIT activating mutations
c-KIT amplification has also been repeated, but increased c-KIT expression may occur without genetic defects.
17

MorphologyMorphology Seminoma → uniform population of cells Spermatocytic seminoma → nosologic
similarity → a distinct tumor
Seminomas → produce bulky masses, sometimes 10 times the size of the normal testis.
Typical seminoma: Homogeneous, gray-white, lobulated cut
surface Devoid of hemorrhage or necrosis
Generally Tunica albuginea → not penetrated → but occasionally extension to the epididymis, spermatic cord, or scrotal sac
18

Fairly well-circumscribed, pale, fleshy, Fairly well-circumscribed, pale, fleshy, homogeneous masshomogeneous mass
19

MicroscopyMicroscopy Sheets of uniform cells divided into poorly
demarcated lobules by delicate septa of fibrous tissue containing a moderate amount of lymphocytes.
Seminoma cell → large and round to polyhedral, distinct cell membrane, clear or watery-appearing cytoplasm, a large central nucleus with 1-2 prominent nucleoli
Mitoses vary in frequency.
The cytoplasm contains varying amounts of glycogen. Seminoma cells → diffusely positive for c-KIT ,
(regardless of c-KIT mutational status) OCT4, and placental alkaline phosphatase (PLAP), with sometimes scattered keratin-positive cells.
20

(a) Clear seminoma cells divided into poorly demarcated (a) Clear seminoma cells divided into poorly demarcated lobules by delicate septa.lobules by delicate septa.
(b) Large cells with distinct cell borders, pale nuclei, (b) Large cells with distinct cell borders, pale nuclei, prominent nucleoli, and a sparse lymphocytic infiltrate.prominent nucleoli, and a sparse lymphocytic infiltrate.
21

MicroscopyMicroscopy15% → contain syncytiotrophoblasts →
elevated serum HCG → though not to the extent seen in patients with choriocarcinoma
May also be accompanied by an ill-defined granulomatous reaction, in contrast to the well-formed discrete granulomas seen with tuberculosis.
22

PATHOLOGYPATHOLOGY
CHARACTERISTICTYPICAL/CLASSIC
SEMINOMA ANAPLASTC SEMINOMA
SPERMATOCYTIC
INCIDENCE 82-85% 5-10% 2-12%
AGE 35-39 yrs 35-39 yrs >65 yrs
HISTOLOGY Large cells with distinct borders, pale nuclei and
prominent nucleoli; syncitiotrophoblast
Lymphocitic infiltrate
Increased mitotic activity,
nuclear pleomorphism and anaplasia
Same as typical seminoma, cells may resemble spermatogonia
METASTATICPOTENTIAL
Slow growing, not aggresive
Aggressive locally as well as
systemically
Low and thus favourable prognosis
SEMINOMATOUS GCT ( 35%)

Anaplastic seminoma Anaplastic seminoma
Indicates greater cellular and nuclear irregularity with more frequent giant cells & many mitoses.
Is not associated with a worse prognosis & is not treated differently
Most authorities do not recognize anaplastic seminoma as a distinct entity.
24

Spermatocytic Spermatocytic SeminomaSeminoma
Uncommon tumor → 1-2% of all testicular germ cell neoplasms
Age of involvement → much later than for most testicular tumors → generally over age of 65 years
In contrast to classic seminoma → slow-growing, does not produce metastases → prognosis is excellent
In contrast to typical seminomas → lack lymphocytes, granulomas, syncytiotrophoblasts, extra-testicular sites of origin, admixture with other germ cell tumors, and association with ITGCN 25

Embryonal CarcinomaEmbryonal Carcinoma Occur mostly in the 20- to 30-year age group. More aggressive than seminomas. Share some markers with seminomas → OCT 3/4 &
PLAP, but positive for cytokeratin & CD30, and negative for c-KIT
90% elaborate hCG or AFP
Morphology Smaller than seminoma → usually does not replace the
entire testis. On cut surfaces: Often variegated, poorly demarcated at the
margins, and punctuated by foci of hemorrhage or necrosis
Extension through the tunica albuginea → into the epididymis or cord frequently occurs.
26

In contrast to the seminoma, the embryonal carcinoma In contrast to the seminoma, the embryonal carcinoma is a is a Hemorrhagic mass.Hemorrhagic mass.
27

MicroscopyMicroscopyCells grow in alveolar or tubular
patterns, sometimes with papillary convolutions.
Lack well-formed glands with basally situated nuclei and apical cytoplasm seen in teratomas.
More undifferentiated lesions → may display sheets of cells 28

Neoplastic cells → epithelial appearance, are large & anaplastic, have hyperchromatic nuclei with prominent nucleoli.
In contrast to seminoma → cell borders are usually indistinct, there is considerable variation in cell and nuclear size and shape.
Mitotic figures and tumor giant cells are frequently seen.

Sheets of undifferentiated cells as well as primitive Sheets of undifferentiated cells as well as primitive glandular differentiation. The nuclei are large and glandular differentiation. The nuclei are large and
hyperchromatic.hyperchromatic.
30

The entire tumor is composed of undifferentiated cells The entire tumor is composed of undifferentiated cells that have overlapping nuclei and scant cytoplasm. that have overlapping nuclei and scant cytoplasm. Tumor cells form solid nests with some slit spaces, Tumor cells form solid nests with some slit spaces, allowing for the focal formation of short papillae.allowing for the focal formation of short papillae.
31

Yolk Sac TumorYolk Sac TumorAlso known as endodermal sinus
tumor , yolk sac tumor is of interest because it is the most common testicular tumor in infants and children up to 3 years of age.
In this age group it has a very good prognosis.
In adults → pure form is rare → frequently occurs in combination with embryonal carcinoma.
32

MorphologyMorphology Non-encapsulated, homogeneous, yellow-
white, mucinous appearance.
MICROSCOPIC:
Lacelike (reticular) network of medium-sized cuboidal or flattened cells.
Papillary structures, solid cords of cells, and a multitude of other less common patterns
33

50% → endodermal sinuses (Schiller-Duval bodies) → consist of a mesodermal core with central capillary and visceral and parietal layer of cells resembling primitive glomeruli.
Within and outside cytoplasm → eosinophilic, hyaline-like globules with α-fetoprotein (AFP) & α1-antitrypsin activity.
AFP → highly characteristic → underscores differentiation to yolk sac cells.

An endodermal sinus pattern is composed of complex cords An endodermal sinus pattern is composed of complex cords and solid groups of cuboidal cells focally forming glomeruloid and solid groups of cuboidal cells focally forming glomeruloid
Schiller–Duval bodies (arrows). Also present are a fibrous Schiller–Duval bodies (arrows). Also present are a fibrous stroma and eosinophilic globules (asterisk).stroma and eosinophilic globules (asterisk).
35

ChoriocarcinomaChoriocarcinoma Highly malignant form of testicular tumor In its “pure” → rare → less than 1% of all germ
cell tumors
Morphology Often → no testicular enlargement → are
detected only as a small palpable nodule .
Typically → small → rarely larger than 5 cm in diameter.
Hemorrhage & necrosis → extremely common. 36

MicroscopyMicroscopy Contain two cell types:
1.Syncytiotrophoblastic → large and have many irregular or lobular hyperchromatic nuclei and an abundant eosinophilic vacuolated cytoplasm → HCG can be readily demonstrated in the cytoplasm
2.Cytotrophoblastic → more regular and tend to be polygonal, with distinct borders and clear cytoplasm → grow in cords or masses and have a single, fairly uniform nucleus
37

Clear cytotrophoblastic cells (arrowhead) with central Clear cytotrophoblastic cells (arrowhead) with central nuclei and syncytiotrophoblastic cells (arrow) with nuclei and syncytiotrophoblastic cells (arrow) with
multiple dark nuclei embedded in eosinophilic multiple dark nuclei embedded in eosinophilic cytoplasm. Hemorrhage and necrosis are seen in the cytoplasm. Hemorrhage and necrosis are seen in the
upper right field .upper right field .
38

TeratomaTeratoma Group of complex testicular tumors having various
cellular or organoid components reminiscent of normal derivatives from more than one germ layer.
Occur at any age from infancy to adult life.
Pure forms → fairly common in infants & children, second in frequency only to yolk sac tumors.
In adults → pure teratomas are rare → 2-3% of germ cell tumors
Frequency of teratomas mixed with other germ
cell tumors → 45%.39

MorphologyMorphologyUsually large, ranging from 5-10 cm in
diameter
Because they are composed of various tissues → gross appearance is heterogeneous: solid, sometimes cartilaginous, and cystic areas.
Hemorrhage & necrosis → usually indicate admixture with embryonal carcinoma, choriocarcinoma, or both.
40

Composed of: Heterogeneous, helter-skelter collection of
differentiated cells or organoid structures ((e.g. neural tissue, muscle bundles, islands of cartilage, clusters of squamous epithelium, structures reminiscent of thyroid gland, bronchial or bronchiolar epithelium, and bits of intestinal wall or brain substance, all embedded in a fibrous or myxoid stroma))
Elements may be mature (resembling various adult tissues) or immature (sharing histologic features with fetal or embryonal tissue)
Common form in ovary → dermoid cysts and epidermoid cysts (with benign behavior) → but rare in testis.
41

The variegated cut surface with cysts reflects the The variegated cut surface with cysts reflects the multiplicity of tissue found histologically.multiplicity of tissue found histologically.
42

Teratoma of the testis consisting of a disorganized Teratoma of the testis consisting of a disorganized collection of lands,collection of lands,
cartilage, smooth muscle, and immature stroma.cartilage, smooth muscle, and immature stroma.
43

This tumor is composed of mature somatic tissue, This tumor is composed of mature somatic tissue, including squamous epithelium, fat, and bone.including squamous epithelium, fat, and bone.
44

Immature teratoma. This tumor contains numerous Immature teratoma. This tumor contains numerous immature nerve cell precursors arranged in neuroblastic immature nerve cell precursors arranged in neuroblastic
tubelike rosettes and nests.tubelike rosettes and nests.
45

Teratoma with malignant Teratoma with malignant transformationtransformation
Rare → when malignancy exists in derivatives of one or more germ cell layers → thus → there may be a focus of squamous cell carcinoma, mucin-secreting adenocarcinoma, or sarcoma
Importance of recognizing non–germ cell malignancy arising in a teratoma → non–germ cell component does not respond to chemotherapy when it spreads outside of the testis
The only hope → resectability of tumor
Have an isochromosome 12p → similar to the germ cell tumors from which they arose
46

Mixed TumorsMixed Tumors60% of testicular tumors → composed of more
than one of the “pure” patterns.
Common mixtures include: Teratoma + embryonal carcinoma + yolk
sac tumor; seminoma + embryonal carcinoma; and embryonal carcinoma + teratoma (teratocarcinoma)
In most instances → prognosis is worsened by inclusion of the more aggressive element.
47

Seminomas Vs. NSGCTsSeminomas Vs. NSGCTs Seminomas → tend to remain localized to testis
for a long time → 70% present in clinical stage I. In contrast → 60% of NSGCTs → advanced clinical
disease (stages II and III). Metastases from seminomas → typically lymph
nodes → hematogenous spread occurs later in the course of dissemination.
NSGCTs not only metastasize earlier → also use hematogenous route more frequently.
From a therapeutic viewpoint:Seminomas → extremely radiosensitive,
whereas NSGCTs → relatively radioresistant → poorer prognosis
48

NON GERM CELL NON GERM CELL TUMORS OF TESTISTUMORS OF TESTIS
LEYDIG CELL TUMORS:
Commonest non germ cell tumor of testis.
1-3% of all testicular tumors.
Bimodal age distribution: 5-9 yrs. And 25-35.
Reinke’s crystals– fusiform shaped cytoplasmic inclusions

Clinical features:
prepubertal- precocious puberty;tumors are usually benign in this age group
adults may present with gynecomastia and impotence;10% of tumors may be malignant.
Lab. Findings: increased 17-ketosteroids(10 to 30 times elevation may be found in malignancy.) and increased estrogens.
Treatment: radical inguinal orchidectomy f/b RPLND if malignant

Constitute < 1% of all testicular tumors.
Bimodal age distribution: <1 yr and 20-25 yrs.
Clinical features:Testicualr mass usually associated with
feminisation(gynecomastia)
Treatment: Radical inguinal orchidectomy f/b RPLND if malignant(10% of tumors are malignant)
SERTOLI CELL TUMOR:SERTOLI CELL TUMOR:

SECONDARY TUMORS OF SECONDARY TUMORS OF TESTISTESTIS
LYMPHOMA:
Commonest secondary tumor and also commonest tumor in pt. Over the age of 50 yrs.(5% of all testicular tumors)
Commonest b/l tumor-50% of cases but ususally asynchronously
Pathology: diffuse histiocytic lymphoma is commonest.
Clinical features: painless enlargement of testis, constitutional symptoms.(25% of pt)
Treatment: radical orchidectomy f/b treatment according to stage of dz.

LEUKEMIC INFILTRATION: Usually presents as a relapse in children with diagnosed acute lymphocytic leukemia.B/l involvement in 50% of cases. Testicular biopsy rather than orchiectomy should be performed. Treatment: b/l testicular irradiation with 20 Gy and adjuvant chemotherapy.
METASTASIS: Very rare;usually are incidental findings at autopsy. Commonest site is prostate f/b lung,git,melanoma and kidney.

PATHOGENESIS AND PATHOGENESIS AND NATURAL HISTORYNATURAL HISTORY
NATURAL HISTORY: short in fast growing tumors like NSGCT.
SPREAD: predictable and stepwise
1.LOCAL: tunica albugenia is a natural barrier to local invasion
2.HEMATOGENOUS: especially in choriocarcinoma lung,liver,brain,bone adrenal,git.
Lymph nodes of the testes extend from T1 to L4 but are concentrated at the level of the renal hilum because of their
common embryologic origin with the kidney.

PATHOGENESIS AND NATURAL PATHOGENESIS AND NATURAL HISTORYHISTORY
3.LYMPHATIC:
Rt.testes: interaortocavalprecavalpreaorticparacaval f/b retrograde spread
Lt.testes:paraaorticpreaortic f/b retrograde spread(common– ext.iliac)
cross over from Rt to left may occur
Inv.of scrotum or tunica albugeniainguinal mets
Inv.of epididymis or cord Distal ext.ernal iliac & obturator mets
Utimately spread to blood stream occur through cisterna chyli and thoracic duct

SYMPTOMSSYMPTOMSPainless lump more common on the Rt., may be
bilateral(2-3%)
Pain: dull ache or heavy sensation in scrotum (30-40%)
acute (10%) because of infarction or hemorrhage.
Due to metastasis (10%)
Rarely gynecomastia (1-5%, mainly in Teratomas) or infertility
Asymptomatic: may be detected incidentally following trauma or by the sexual partner.

Atypical cases-
- may simulate epididymo-orchitis / a urinary infection.
- all testicular swellings should be treated
with suspicion & failure to respond to antibiotics should raise the possibility of a testicular tumor.

SIGNSSIGNS LOCAL EXAMINATION:
Firm, nontender, heavy testes with loss of sensation Look for scrotal and epididymal involvement ( initially epididymis is normal but later difficult to feel as incorporated by the growth). Thickened spermatic cord due to cremastric hypertrophy & enlargement of testicular vessels. Vas is never thickened Prostate & Seminal vesicles are normal on P/R. Lax secondary hydrocele may be present (10%). Illac and inguinal lymphadenopathy.

PER ABDOMEN:
Enlarged retroperitoneal lymph nodes.
Hepatomegaly
Supraclavicular lymphadenopathy(Virchow’s node.)
SIGNSSIGNS

Clinical stagesClinical stagesBODEN AND GIBB(1971)
Stage I: tumor confined to testis, epididymis, or spermatic cord.
Stage II: distant spread confined to retroperitoneal nodes below diaphragm.
Stage III: metastases outside retroperitoneal nodes or above diaphragm.
60

61

STAGINGSTAGINGTNM CLASSIFICATION: (AJCC 1996)
Tx :cannot be assessed. To:no evidence of primary tumor. Tis:intratubular cancer(carcinoma in situ) T1:tumor limited to the testis and epididymis and
no vascular invasion. T2:tumor limited to the testis and epididimis with
vascular /lympatic invasion or tumor extending through the tunica albuginea with involvement of tunica vaginalis
T3:tumor invades the spermatic cord T4:tumor invades the scrotum

STAGING (CONT.)STAGING (CONT.) REGIONAL LYMPH NODES
Nx:regional lymph nodes cannot be assessed. N0:no regional lymph node metastasis. N1:lymph node mass 2 cm or less,or multiple
lymph node masses (</=6) none >2cm N2:lymph node mass > 2 cm but <5 cm in >6
nodes N3:lymph node mass >5 cm DISTANT METASTASIS(M): Mo:no evidence of distant metastasis M1:non regional nodal or pulmonary mets M2:non pulmonary visceral masses

SERUM TUMOR SERUM TUMOR MARKERS(S)MARKERS(S)
LDH hCG(mIU/ml)
AFP(ng/ml)
So </= N and
</= N and
</= N
S1 < 1.5 x N and
< 5000 and
< 1000
S2 1.5-10 x N or
5000-50000 or
1000-10000
S3 > 10 x N or
>50000 or
>10000

STAGE GROUPINGSTAGE GROUPING
STAGE 1: T1-T4 No Mo So
STAGE 2 : Any T N1,N2,N3, Mo So/S1 a b c
STAGE 3 : Any T, any N, Mo M1 S2/S3 any S

TUMOR MARKERSTUMOR MARKERSCHARACTERISTC AFP hCG LDHCHEMICALLY Single chain
glycoproteinGlycoprotein
composed of alpha and B chains
Cellular enzyme
T half 5-7 days 24-36 hrs variable
TUMORS PRODUCING
Pure embryonic carcinoma, terato
ca.,yolk sac tumor, not by pure choriocarcinoma
or pure seminoma
Choriocarcinoma, embryonal
carcinoma(40-60%),seminoma(5-
10%)
Advanced GCT especially seminoma
FALSE +VE Malignancies,(liver, pancreas,stomach,lung),benign liver dz.,ataxia
telengectesia
Malignancies(liver,pancreas,stomach,
lung,breast), hypogonadism
Found in smooth,cardiac
and skeletal muscle ,liver
COMMENTS Normal levels: < 10 ng/ml
Alpha subunit cross reacts with
LH,FSH,TSH
non specific. But is a marker
of tumor burden and recurr.

TUMOR TUMOR MARKERS(CONT.)MARKERS(CONT.)
NORMAL LEVELS: A preop baseline level must be done
AFP: < 10 ng/ml hCG: < 4mIU/ml LDH: < 1.5 times reference range

CLINICAL SIGNIFICANCE:
1. Reflect the amount of tumor burden: persistant elevation following an orchiectomy suggests a metastatic disease rather than a tumor confined to retroperitoneum.
2. Monitoring therapeutic response: failure to decline proportional to half life indicates an incomplete response.
3. Prediction of histologic subtype: 4. Prognostic value:

INVESTIGATIONSINVESTIGATIONSFOR DIAGNOSIS: 1)USG scrotum: hypocehoic
testicular mass is s/o malignancy. calcification and cysts may be found in non seminomas.
2)FNAC: previously contraindicated ,recently shown that there is no scrotal violation
3)Biopsy: rarely requre and should be performed through inguinal route.

INVESTIGATIONS(CONT.)INVESTIGATIONS(CONT.) FOR STAGING :
1. Chest X-ray : P/A and lateral view 2. CT scan: abdomen to detect
retroperitoneal lymphadenopathy.Chest CT may be done if abnormal abdominal CT .Per se chest CT is non specific for detecting pulmonary mets in absence of negetive abd. CT
3. MRI: no added advantage over CT. tumors are hypointense on T2 weighted and show brisk enhancement with gadolinium.
4. Tumor markers:

INVESTIGATIONS

TREATMENT OF GCTTREATMENT OF GCT
PRINCIPLES:1.Radical inguinal
orchiectomy with clamping of cord at deep ring is the first and the essential step in treatment.
2. Histological diagnosis of the tumor is mandatory to plan adjuvant therapy.

TREATMENT(CONT.)TREATMENT(CONT.)

TREATMENT OF SEMINOMA TREATMENT OF SEMINOMA LOW STAGELOW STAGE
S PE RM A T O C YT ICno a djuva nt the rapy
S URV E IL L A NC Ere l ia ble a nd m otiva ted pt.
NO RIS K F A C T O RS
RA D IA T ION L O W D O S Eabdom ina l a nd pe lvic
C HE M O T HERA PYsingle a ge nt ca rbopla tin
RIS K F A C T O RS PRE S E NT
T YPIC A L A ND A NA PL A S T ICl/f r isk fac tors-tum or > 6cm
-vas cular or lym phatic invas ion
S T A G E 1 S E M INOM AT 1 -3 No M o S o
S T A G E 1 S E M INO M A
RA D IA T ION- A BD OM INA L &PE L V IC
C HE M OT HE RA PYIf lym phnodes c los to k idne y
S T A G E 2 A A ND 2 B S E M INO M AT 1 -3 N1M o S o/S 1 and T 1 -3 N2 M o S 0 /S 1
S E M INO M A

RADIOTHERAPY INRADIOTHERAPY IN SEMINOMASEMINOMASTAGE FIELD OF EBRT DOSE RELAPSES
1-2A Para aortic and ipsilateral renal hilar(previously pelvic nodes were included)
25 Gy over 3 wks.@ 150 cGy/day
2-4%
2B Ipsilateral pelvic( but B/L common illac),para aortic,para caval-hockey stick field
Shield the kidney.H/o herniorraphy or orchidopexy
contralat.inguinal region to be included with sheilding of testis.
35 GyConventional fractionation used
4%

RADIOTHERAPY(CONT.)RADIOTHERAPY(CONT.) FIELDS OF RADIOTHERAPY:
1. PARA AORTIC: boundaries : superiorly T10/11 at the origin of thoracic duct and laterally upto internal inguinal ring.The contralateral nodes are treated on individual basis.
2. PELVIC : L4 vertebra to inguinal ligament including the orchiectomy scar.
LIMITED FIELD(limited to retroperitoneum) To decrease the chronic complications Used only in stage 1 disease.
Mediastinal irradiation is no longer recommended.

RADIOTHERAPY(CONT.)RADIOTHERAPY(CONT.)COMPLICATIONS:
ACUTE: nausea dry squamation and erythema of skin transient decrease in spermatogenesis
CHRONIC: temporary decrease in spermatogenesis secondary malignancies(e.g.leukemia.) gastrointestinal complications
SURVIVAL RATES: STAGE 1: >95% STAGE 2: 80%(70-92%)

TREATMENT OF ADVANCED TREATMENT OF ADVANCED SEMINOMA(STAGE 2C AND 3)SEMINOMA(STAGE 2C AND 3)
diffuse desm oplastic reaction:OBSERVAT ION
Observation3m thly/1yr6 m thly/5yr
Histology :fibrosis/necrosis
Salvage chem otherapyV I C
Histology:GCT
Discrete w ell delineated m ass >3 cm :SURG ICAL RESECT ION
Residual retroperitoneal m ass(on CT )
Cisplatin based chem otherapy
ST AGE 2C (T1-4 N3 M 0 S0/S1)AND ST AG E 3 SEM INOM A(T 1-4 NO-3 M 1-2 S0-3)

TREATMENT OF STAGE 1 TREATMENT OF STAGE 1 NSGCTNSGCT
S U R V E IL L E N C Ein m otiva ted re liab le p t.
ris k fac to rs ab s en t
s tag e N 0 :/N 1 (< 2 cm )O B S E R V A TIO N
s tag e N 2 (> 2 cm )A D JU V A N T C H E M O TH E R A P Y
B E P 2 cyc les
M O D IF IE DR P L N D
P R IM A R Y C H E M O TH E R A P YB E P - 3 C Y C L E S
risk fac tors p resen t
R IS K F A C TO R ST2 o r h ig h er
em b ryon a l > 4 0 %vascu la r / lym p h atic in vas ion
S TA G E 1 Sp ers is ten t tu m or m arker e leva tion
an d n o rad io log ic d z .
S TA G E 1T1 -4 N 0 M 0 S 0

SURVEILLANCE IN STAGE SURVEILLANCE IN STAGE 1 NSGCT1 NSGCT
INDICATIONS: Risk factors for relapse Pt is motivated and reliable for regular follow up.
PROTOCOL:
1. History examination 2m/1st 2yr CBC,LFT,tumor markers 4m/3-4yr Chest x-ray 6m/5yr2. CT scan 4m,6m,12m
respectively TOTAL PERIOD: 5yrs

TREATMENT OF STAGE TREATMENT OF STAGE 2A AND 2B NSGCT2A AND 2B NSGCT
no adjuvant chem otherapy
m inim al nodal involvem ent<2 cm
adjuvant chem otherapyBEP 2 Cycles
nodal involvem ent>2 cm
RPLND-bilateral PRIMARY CHEMOTHERAPYBEP 3 cycles if
suprahilar,pelvic or inguinal LNbackache or contralateral dz.
STAGE 2A(T1-4 N1 M O SO/S1)STAGE 2B(T1-4 N2 M 0 S0/S1)

RETROPERITONEAL LYMPH RETROPERITONEAL LYMPH NODE DISSECTIONNODE DISSECTION
RATIONALE: Retroperiteoneal nodes are usually and often
the only site of metastatic disease. 15-40% of the pts.are understaged even with
the most sophisticated imaging modalities Untreated retroperitoneal nodal metastasis
are usually fatal.
APPROACHES:Thoracoabdominal and midline abdominal.Recently lap.methods introduced.

RPLND(CONT.)RPLND(CONT.) BOUNDARIES:
STANDARD RPLND: Indications: non bulky stage 2
disease.(2A and 2B) Boundaries are renal
hilum superiorly, upto the bifurcation of common illac vessels inferiorly removing all nodal tissue betweeen the ureters

MODIFIED RPLNDMODIFIED RPLND INDICATIONS:stage 1
disease only.
Boundaries :resect all interaortocaval and ipsilateral nodes between the renal hilum and the bifurcation of common illac and minimise contralateral dissection below the level of IMA.
Avoid suprahilar dissections. Advantages: less chances
of retrograde ejaculation bcoz important symp. fibres from opp. side are preserved.

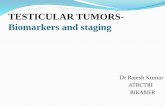
LAPAROSCOPIC RPLNDLAPAROSCOPIC RPLNDPort placement
for laparoscopic retroperitoneal lymph node dissection.
Four 10/12-mm equally spaced trocars are placed in the midline.





RPLNDRPLND- - COMPLICATIONSCOMPLICATIONS
LYMPHATIC: chylous ascites (2-3%); symptomatic cases require therapeautic paracentesis.
PULMONARY: Atelectesis pneumonia ARDS
Judicious monitoring of peri operative fluid administration is essential esp.in pts. Treated with Bleomycin.
WOUND INFECTIONS:

VASCULAR INJURIES(INTRA-OP.) renovascular injury can cause postop. Hypertension and bleeding intraoperatively.
GASTROINTESTINAL: prolonged ileus pancreatitis gastrointestinal bleeding duodenal hematomas and lacerations.
ERECTILE & EJACULATORY DISTURBANCES

ROLE OF ROLE OF RADIOTHERAPY RADIOTHERAPY IN NSGCTIN NSGCT◦DISADVANTAGES OF RADIOTHERAPY:
Many stage 2 bulky tumors have spread beyond the retroperitoneum
Does not provide pathological staging. Lack of comparable survival data.(24% relapse.) Post irradiation relapse: surgery and
chemotherapy are ineffective/not possible or cumulative toxicity precludes their use.
Complications of radiotherapy.

CHEMOTHERAPYCHEMOTHERAPYINDICATIONS: Stage 2 bulky(2c) and 3-all GCTs. Stage 2 nonbulky(2a and 2b) NSGCT as an
alternative to RPLND(esp. in suprahilar disease)
PROTOCOLS: CURATIVE INTENT:in good risk patients-3 cycles of
BEP every 21 days or 4 cycles of PE SALVAGE/POOR RISK:• 4 cycles of BEP• VIP –more toxic • ABMT with high dose:4 cycles of BEP f/b 2 EP
RESPONSE RATES: 70-80%

CHEMOTHERAPY (CONT.)CHEMOTHERAPY (CONT.)
DRUG DOSE ADR COMMENTS
BLEOMYCIN 30 U IV on day 2,9,16
Fever, chills, Pulmonary
fibrosis
Be careful with FiO2 and Iv fluids postop
ETOPOSIDE 100 mg/sq.m IV days
1-5
myelosupression
CISPLATIN 20 mg/sq.m Days 1-5
Renal insufficiency
peripheral neuropathy,mye
losupression
Monitor renal function

TREATMENT OF HIGH TREATMENT OF HIGH STAGE NSGCT STAGE NSGCT
RECURRANCEgo for SALVAGE CHEM O.
OBSERVAT ION
RESOLUTIONN s.m arkers,N CT scan
OBSERVATION
Histology - necrosis,fibrosisteratom a
SALVAG E CHEM OT HERAPYVIP
GERM CELL TUM OR
RESIDUAL RP M ASSgo for b/l RPLND
EXCLUDE FALSE POSIT IVE
PERSISTENT TUM OR M ARKERELEVATION
CHEM OTHERAPYBEP 3 CYCLES
GOOD RISK DZ.
POOR RESPONSEgo for SALVAG E CHEM OTHERAPY
CHEM OTHERAPY1. Ifosfam ide replaces etoposide2.high dose chem o w ith ABM T
POOR RISK DZ.
STAG E 2C AND STAGE 3

PROGNOSTIC CLASSIFICATIONPROGNOSTIC CLASSIFICATION GOOD RISK DISEASE:(NSGCT)
Testis or retroperitoneal primary No nonpulmonary ,visceral metastasis S1 or S2 disease.
POOR PROGNOSIS:
Mediastinal primary Non pulmonary visceral metastasis S3 disease

PROGNOSISPROGNOSISSGCT: STAGE 1: 98% STAGE 2 nonbulky: 92-94% STAGE 2 bulky and 3: 35-75%
NSGCT: STAGE 1: 96-100% STAGE 2 non bulky: 90% STAGE 2 bulky and 3: 55-80%

THANK THANK YOUYOU