Pediatric Testicular Tumors - The University of Tennessee ... .pdf · Pediatric Testicular Tumors...
63
Pediatric Testicular Tumors Mark A. Williams, MD Joe Welser, MD February 12, 2014
Transcript of Pediatric Testicular Tumors - The University of Tennessee ... .pdf · Pediatric Testicular Tumors...
Pediatric Testicular Tumors
Mark A. Williams, MD
Joe Welser, MD
February 12, 2014
Testicular Tumors
• 1% to 2% of all Pediatric Solid Tumors
• Annual Incidence of 1 in 100,000
• Majority occur in children < 2 years of age
• Teratoma now thought to be most common type
• Benign Tumors Account for 38% of cases
• Metastasis (Occurs in < 15% of tumors) – 28% to Lymph Nodes
– 40% Hematogenous
– 20% Both
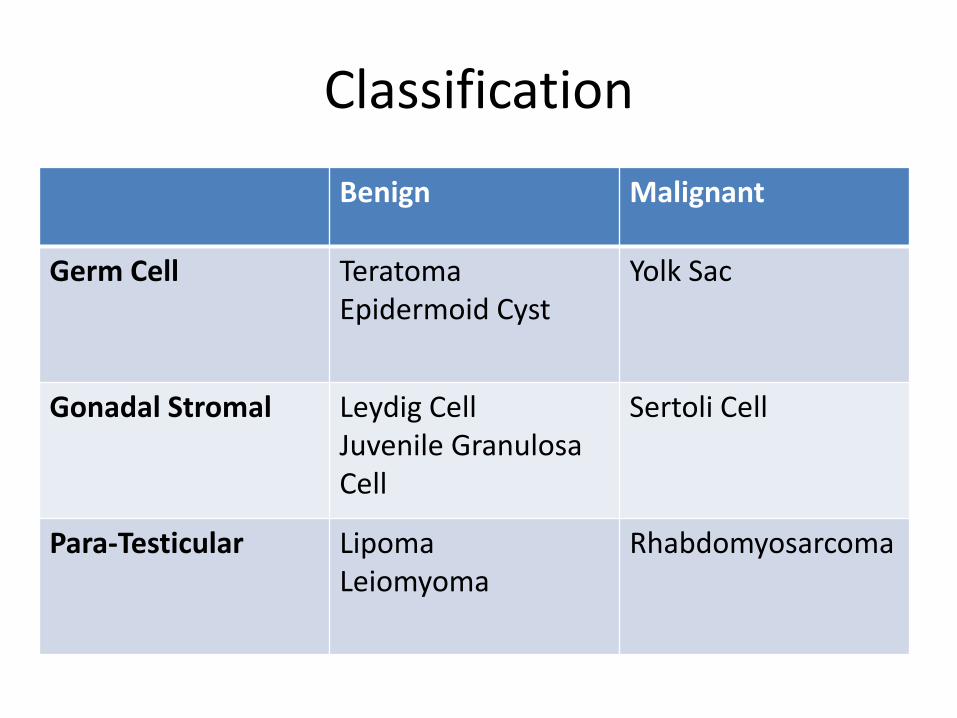
Classification
Benign Malignant
Germ Cell Teratoma Epidermoid Cyst
Yolk Sac
Gonadal Stromal Leydig Cell Juvenile Granulosa Cell
Sertoli Cell
Para-Testicular Lipoma Leiomyoma
Rhabdomyosarcoma
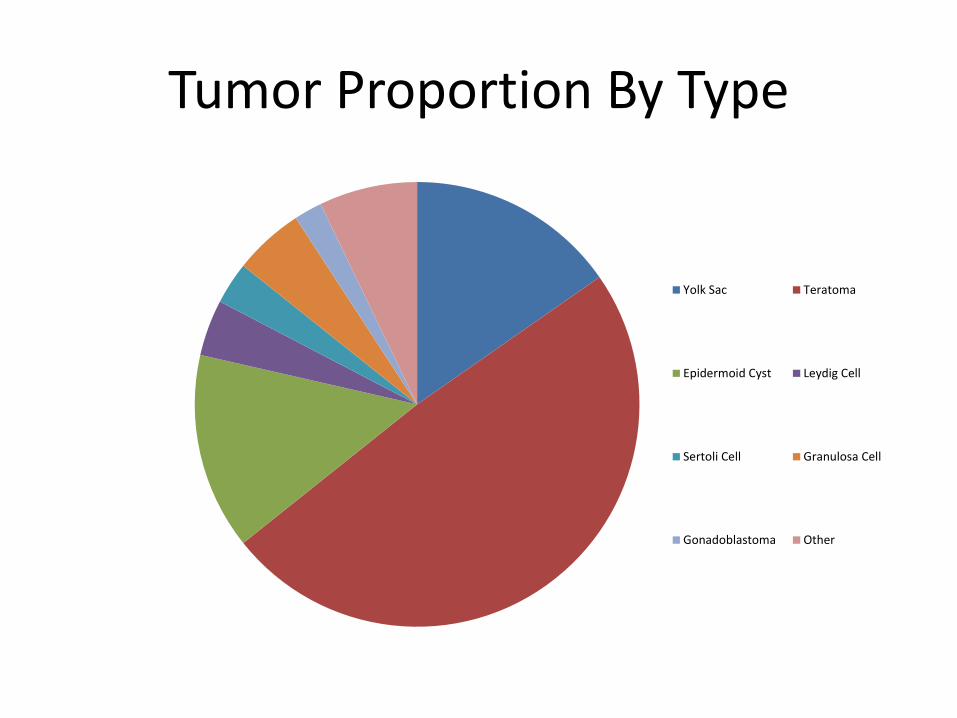
Tumor Proportion By Type
Yolk Sac Teratoma
Epidermoid Cyst Leydig Cell
Sertoli Cell Granulosa Cell
Gonadoblastoma Other
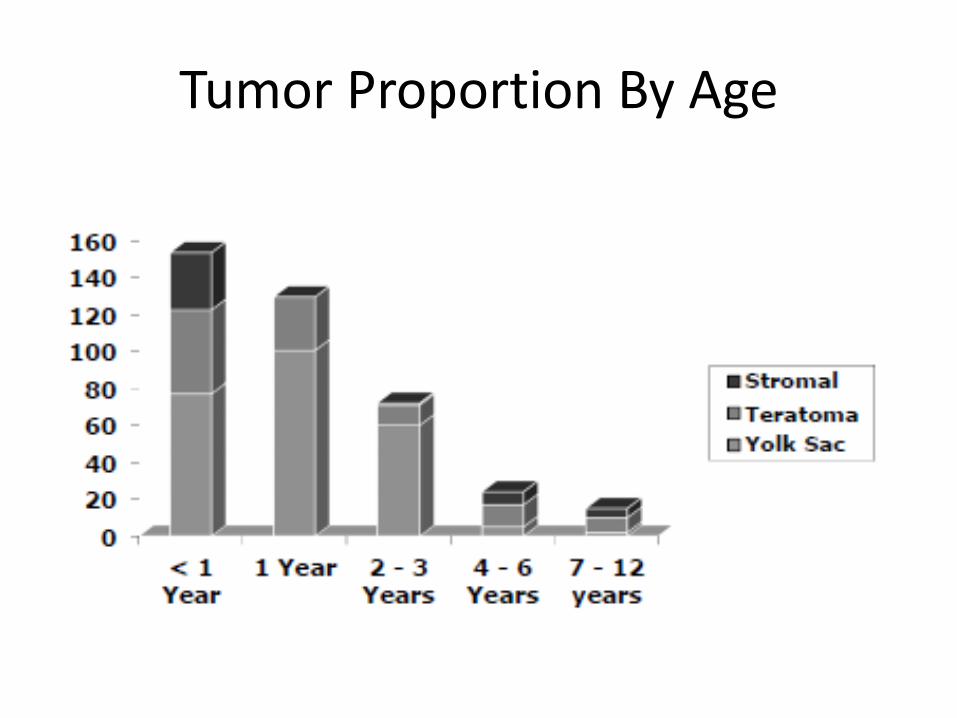
Tumor Proportion By Age
Link to Cryptorchidism
• Incidence of testicular cancer in general population is approximately 5.4 per 100,000
• Wood and Elder (2009): Relative Risk of Malignant Transformation – 2.75 to 8 overall (< 0.5%) – 2 to 3 in boys undergoing prepubertal orchiopexy – Boys undergoing postpubertal orchiopexy are 2 to 6 times more
likely to develop testicular cancer – 74% of malignancies in persistent cryptorchid testes, are
seminoma – 63% of malignancies in post-orchiopexy patients, are non-
seminoma – No increased risk for tumors in the contralateral normally
descended testis
Link to Cryptorchidism (ctd)
• Cortes, et al (2004): Incidence of Pediatric Testicular Tumors in Patients with Cryptorchidism – 3.8% of children with abdominal undescended testes, abnormal
external genitalia, or abnormal karyotype – In patients without these characteristics, no cases of testicular
neoplasia – Found most often in bilateral cryptorchidism
• Petterson, et al (2007): Relative risk increases with age at orchiopexy
• Relative risk increases the more cephalad the undescended testis
• Other studies show presence of cancer in contralateral testis in 20% of cases
Chromosomal Abnormalities
• Benign Teratoma: No abnormality • Yolk-Sac Tumors: del(1p36) in 80% - 100% of cases • Intratubular Germ Cell Neoplasia: i(12p) • Post-Pubertal Germ-Cell Tumors
– Loss of chromosomes 11, 13, or 18 – Gain of chromosomes 7, 8, or X
• Patients with Disorders of Sex Development (DSD) have increased incidence – Hypovirilization and gonadal dysgenesis are at higher risk – Presence of Y chromosome in gonadal dysgenesis increases risk
to 10% by age of 20 – Intratubular germ cell neoplasia has been noted in 6% of
children with DSD
Diagnosis
• Most common Presentation: Painless testicular mass – 10% with history of hernia or hydrocele – 15% - 50% have hydrocele on physical exam
• May also present with acute abdominal pain • Must rule out epididymitis, hydrocele, hernia, and
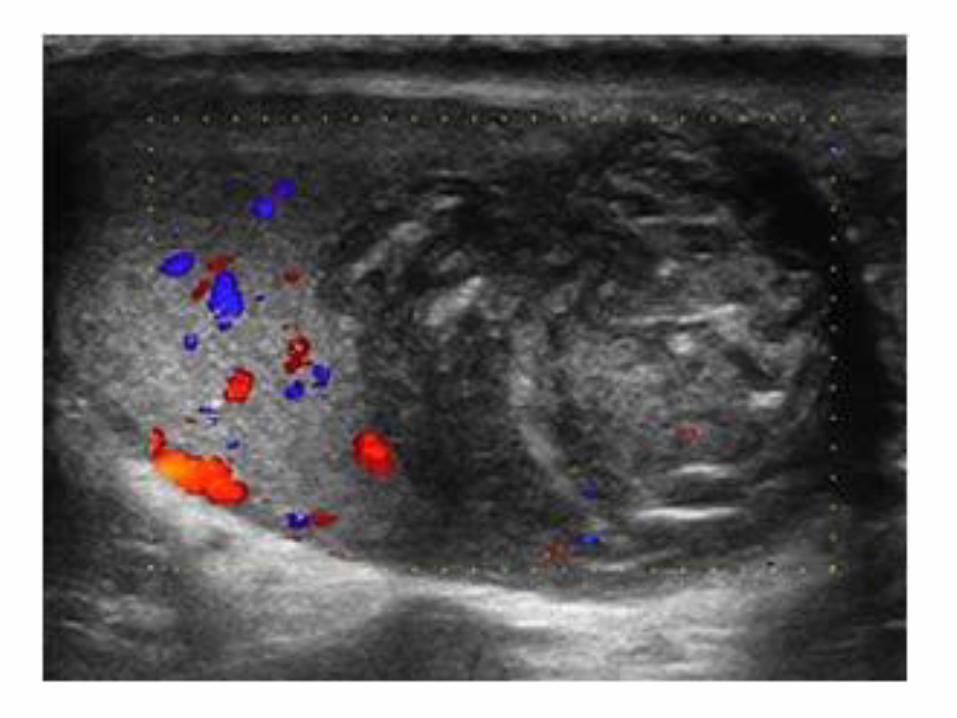
torsion (neonate) • Testicular Ultrasound (with doppler): Cannot reliably
distinguish benign and malignant tumors – Anechoic cystic lesions suggest benign lesion – Sharp borders and low flow suggest benign – Useful to evaluate whether there is enough useful testicle
to salvage
Tumor Markers
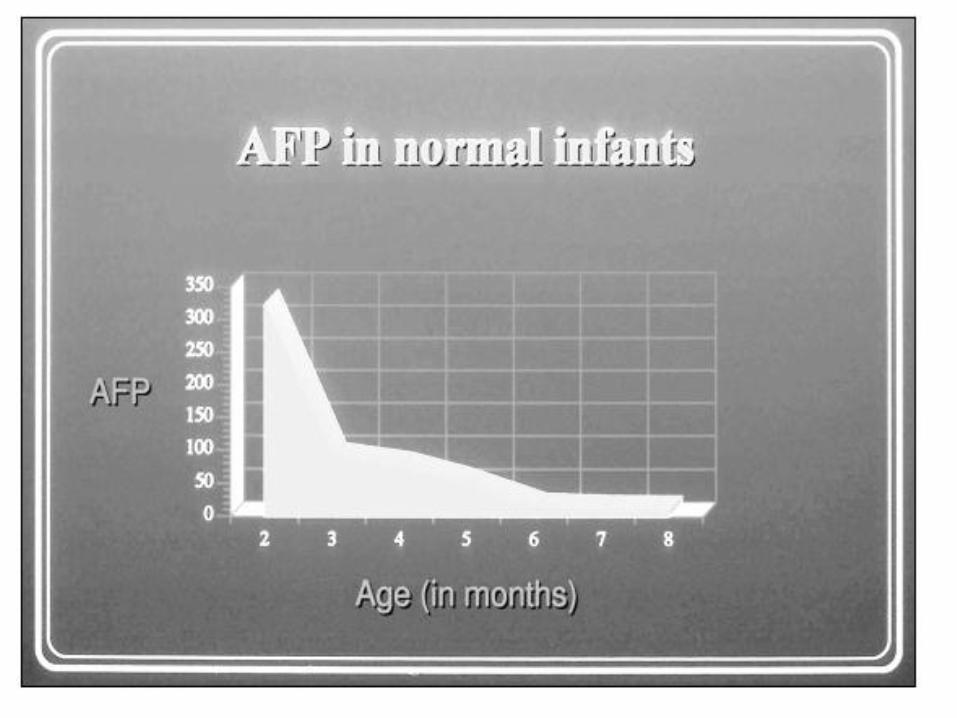
• a-fetoprotein elevated in > 90% of yolk-sac tumors – All a-fetoprotein producing tumors have yolk-sac
elements
– T1/2 of 5 days
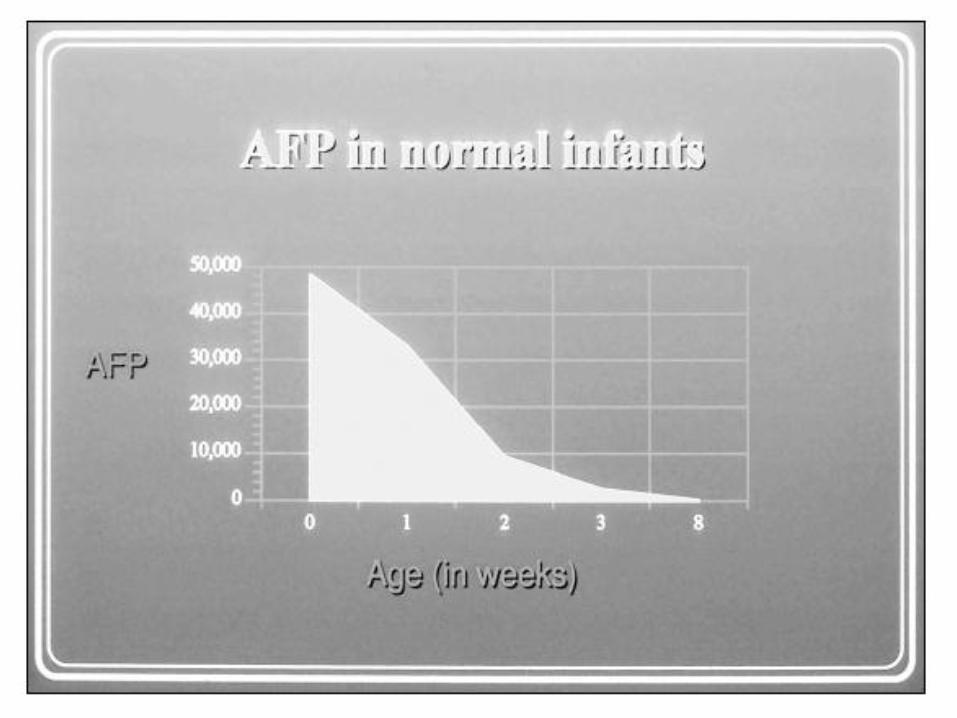
– Elevated for 6-9 months postpartum
– Also elevated in hepatoblastoma
• b-hCG not useful in prepubertal patients – Embryonal carcinoma and choriocarcinoma are rare
– Produced by some mixed teratomas
Yolk Sac Tumor
• AKA endodermal sinus tumor, embryonal adenocarcinoma, infantile adenocarcinoma of the testis, orchidoblastoma, or Telium tumor
• Most common malignant tumor in infants and young boys
• 3% of cases have a positive history of trauma
• Staging – a-fetoprotein
– CT of chest and abdomen
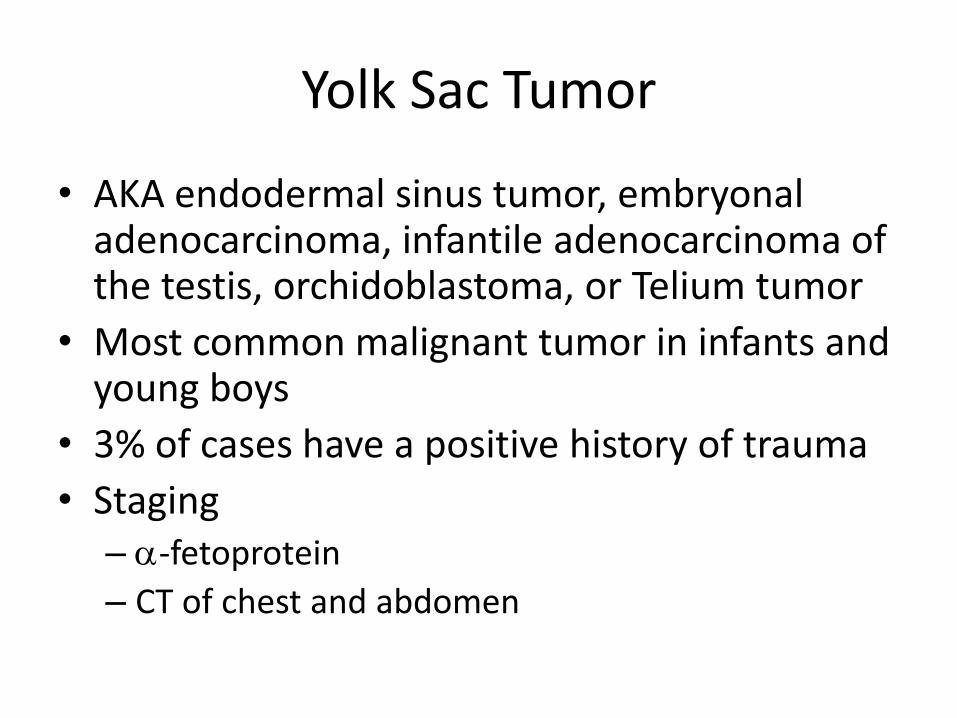
Yolk Sac Tumor - Pathology
Gross Pathology Microscopic Appearance
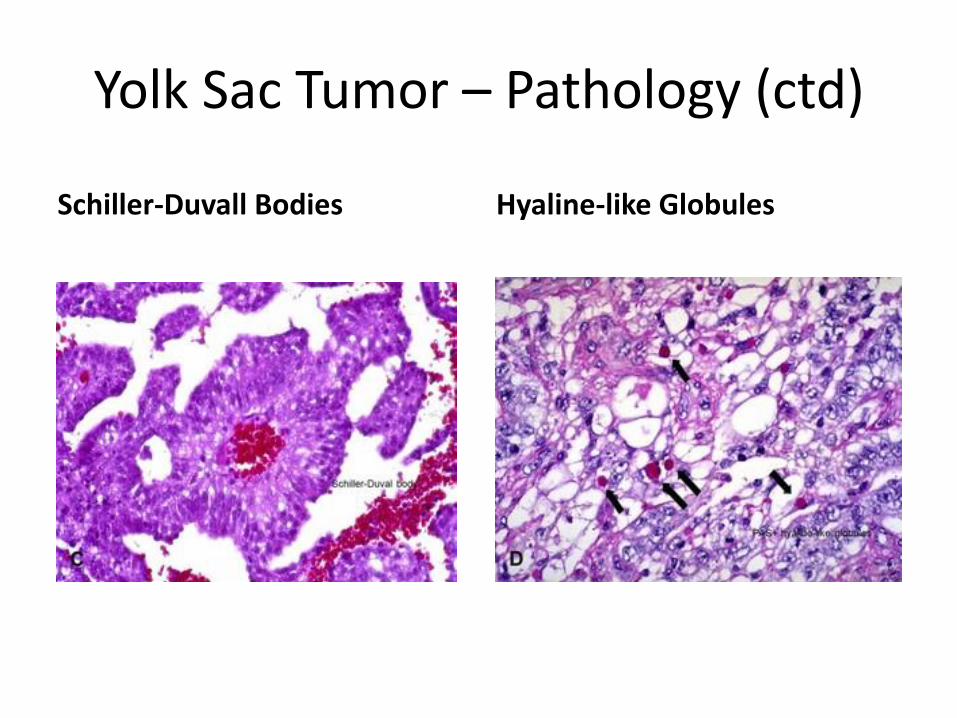
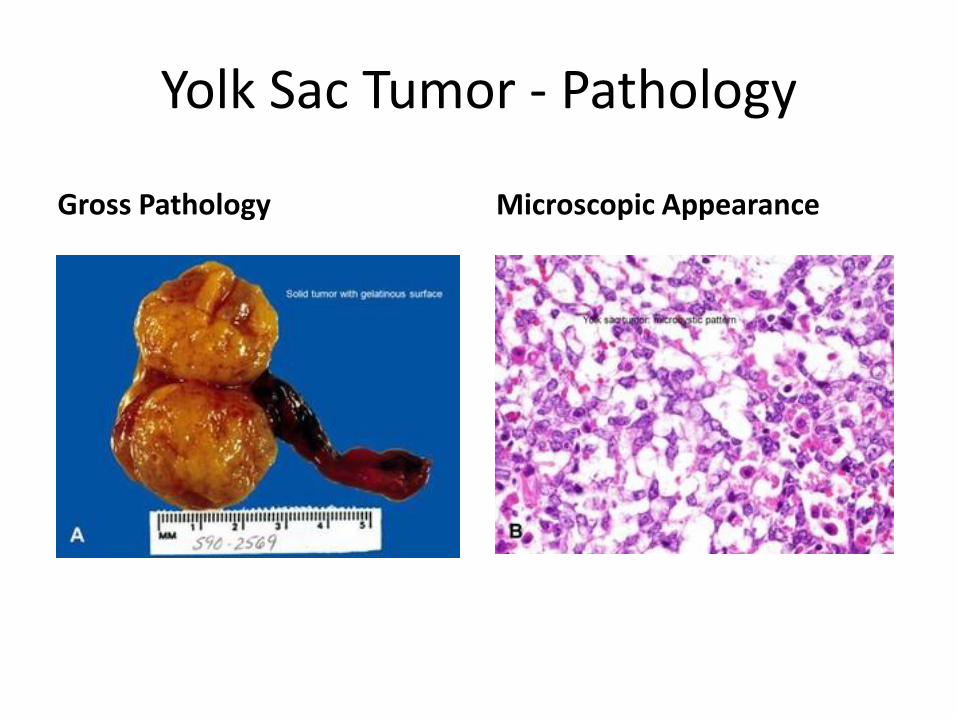
Yolk Sac Tumor – Pathology (ctd)
Schiller-Duvall Bodies Hyaline-like Globules
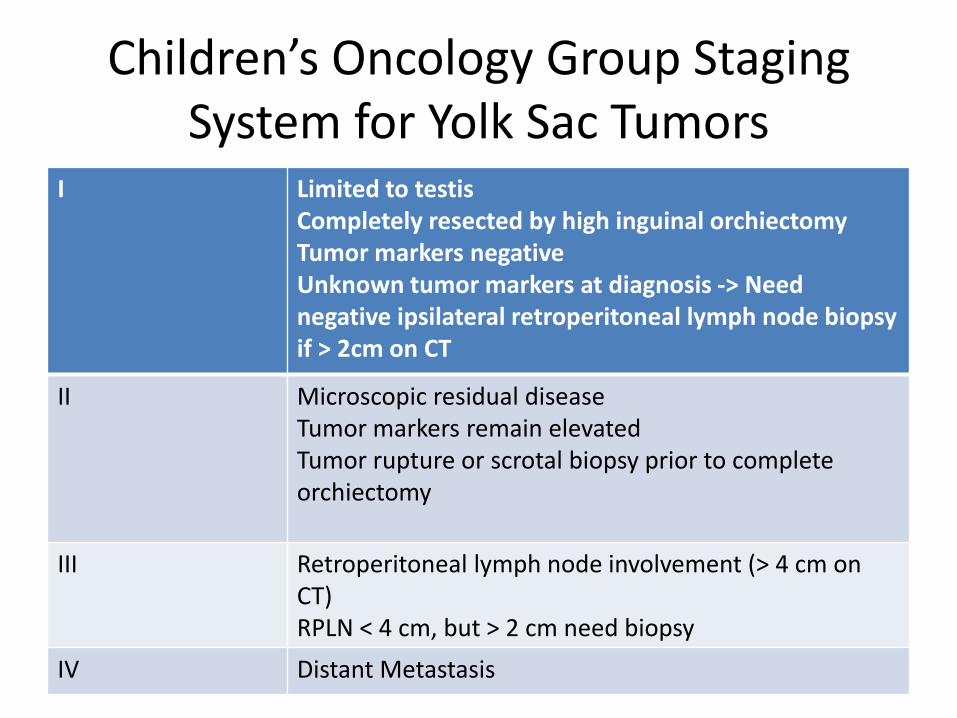
Children’s Oncology Group Staging System for Yolk Sac Tumors
I Limited to testis Completely resected by high inguinal orchiectomy Tumor markers negative Unknown tumor markers at diagnosis -> Need negative ipsilateral retroperitoneal lymph node biopsy if > 2cm on CT
II Microscopic residual disease Tumor markers remain elevated Tumor rupture or scrotal biopsy prior to complete orchiectomy
III Retroperitoneal lymph node involvement (> 4 cm on CT) RPLN < 4 cm, but > 2 cm need biopsy
IV Distant Metastasis
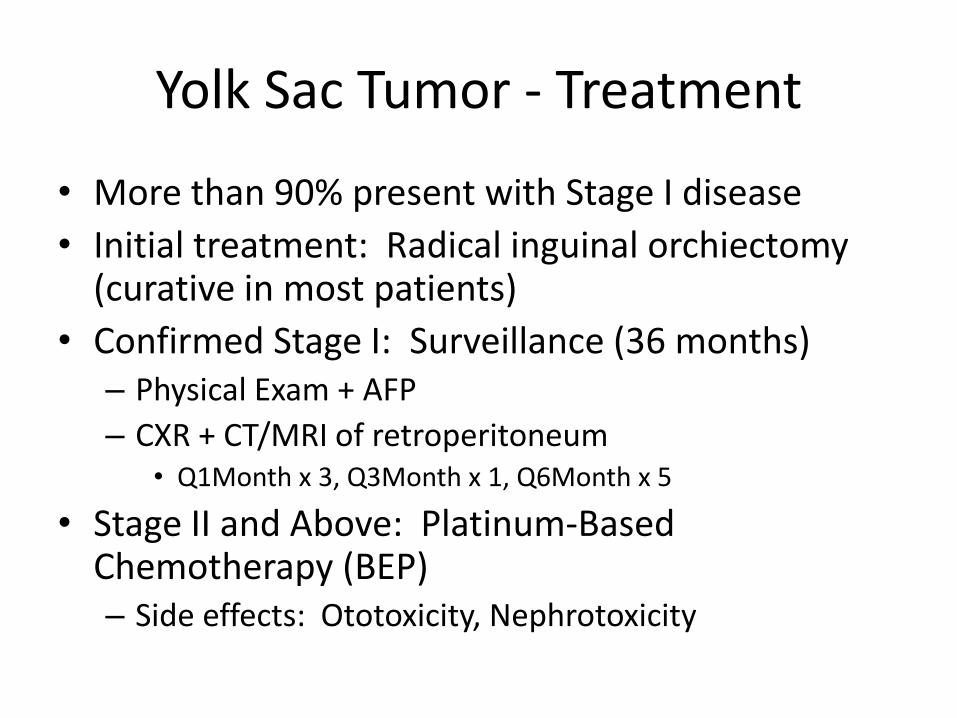
Yolk Sac Tumor - Treatment
• More than 90% present with Stage I disease
• Initial treatment: Radical inguinal orchiectomy (curative in most patients)
• Confirmed Stage I: Surveillance (36 months) – Physical Exam + AFP
– CXR + CT/MRI of retroperitoneum • Q1Month x 3, Q3Month x 1, Q6Month x 5
• Stage II and Above: Platinum-Based Chemotherapy (BEP) – Side effects: Ototoxicity, Nephrotoxicity
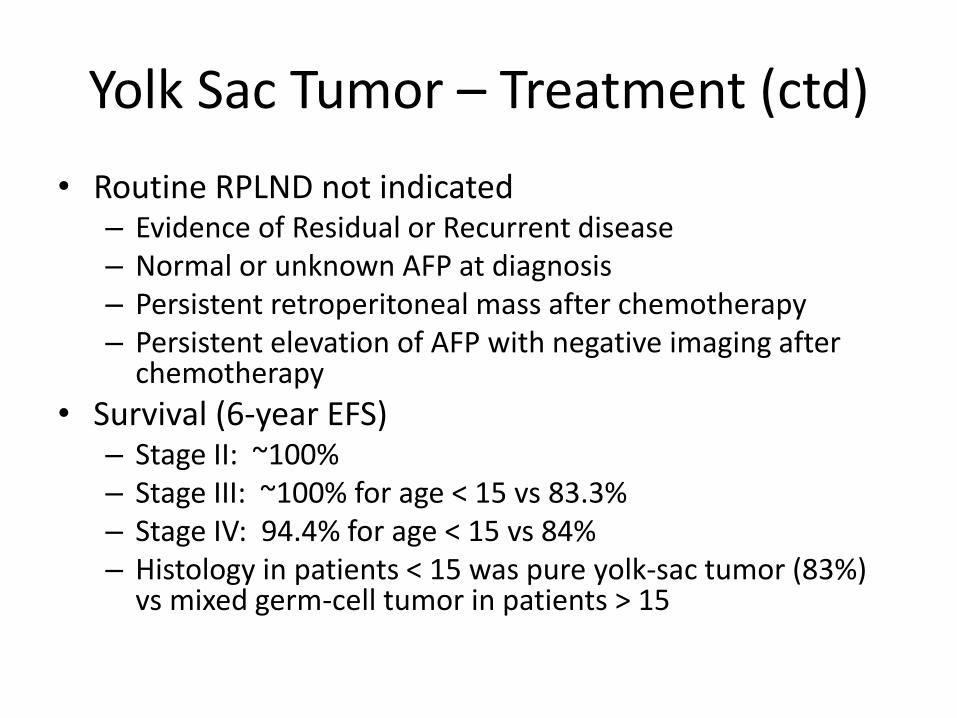
Yolk Sac Tumor – Treatment (ctd)
• Routine RPLND not indicated – Evidence of Residual or Recurrent disease – Normal or unknown AFP at diagnosis – Persistent retroperitoneal mass after chemotherapy – Persistent elevation of AFP with negative imaging after
chemotherapy
• Survival (6-year EFS) – Stage II: ~100% – Stage III: ~100% for age < 15 vs 83.3% – Stage IV: 94.4% for age < 15 vs 84% – Histology in patients < 15 was pure yolk-sac tumor (83%)
vs mixed germ-cell tumor in patients > 15
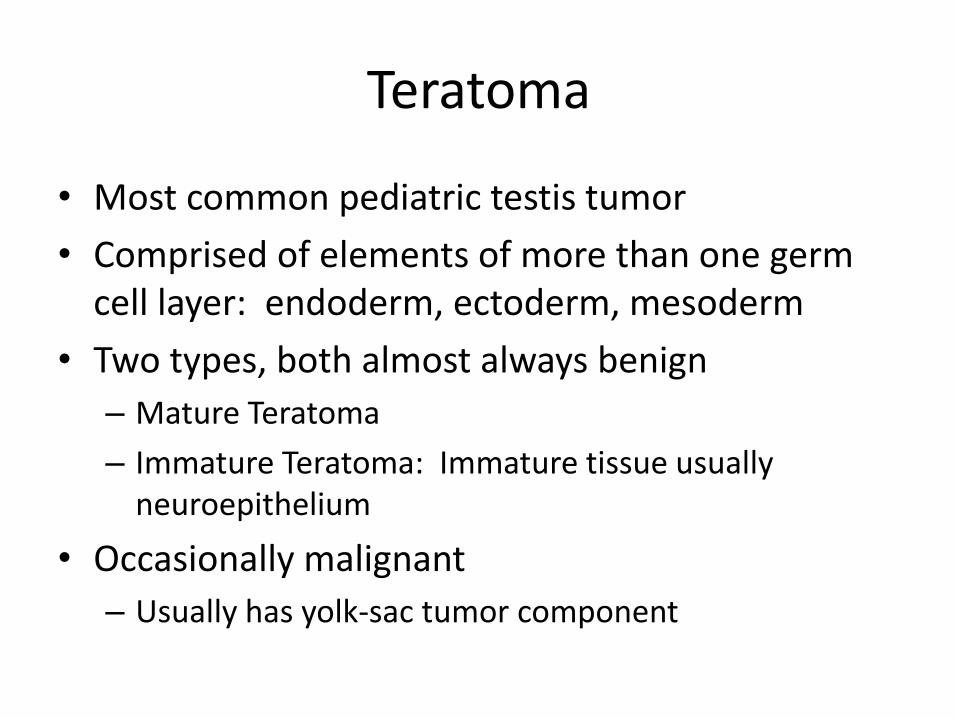
Teratoma
• Most common pediatric testis tumor
• Comprised of elements of more than one germ cell layer: endoderm, ectoderm, mesoderm
• Two types, both almost always benign
– Mature Teratoma
– Immature Teratoma: Immature tissue usually neuroepithelium
• Occasionally malignant
– Usually has yolk-sac tumor component
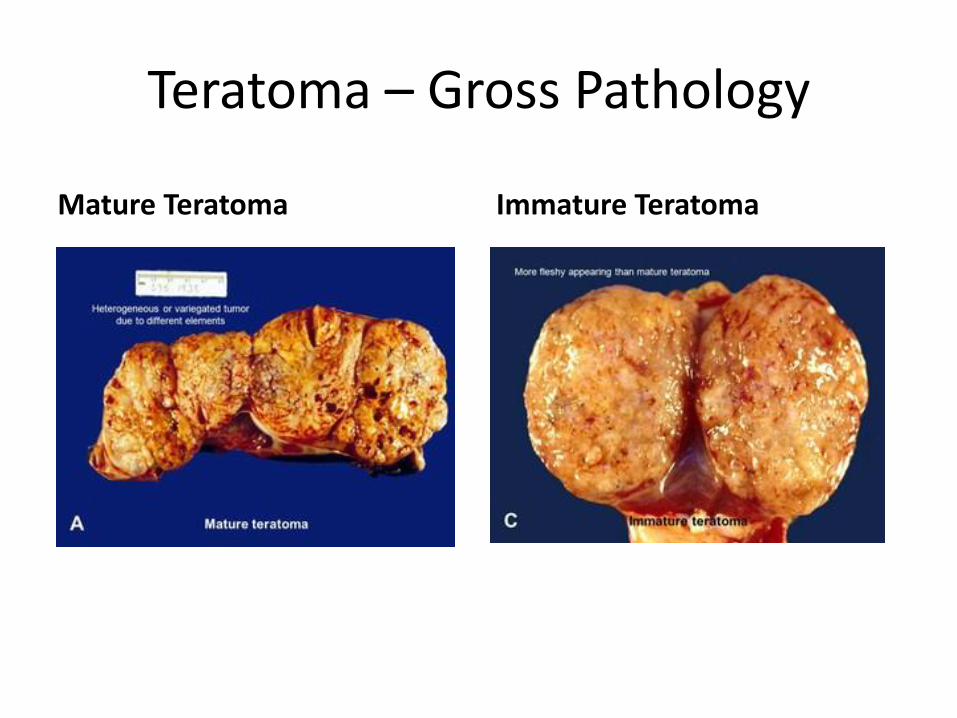
Teratoma – Gross Pathology
Mature Teratoma Immature Teratoma
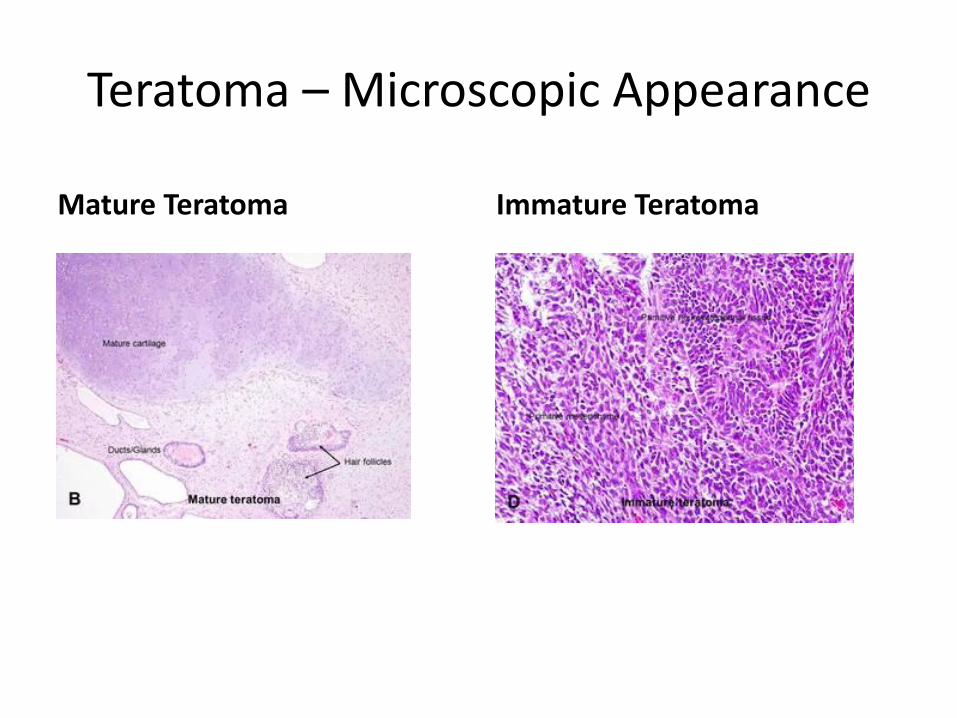
Teratoma – Microscopic Appearance
Mature Teratoma Immature Teratoma
Teratoma (ctd)
• Diagnosis – Ultrasound of testis reveals a heterogeneous
lesion with internal echoes (calcification)
– AFP not elevated for the patient’s age
• Treatment – Testis-sparing procedures (enucleation)
– Should be done through inguinal incision
– Teratomas generally “shell out” easily due to pseudocapsule around the lesion
Epidermoid Cyst
• Monodermal Teratoma – Differentiated squamous-lined cysts
– Filled with keratinous debris
• AFP levels normal
• Suggested by characteristic appearance on ultrasound: Concentric rings of alternating hypo and hyperechoic layers (“onion-skin” appearance)
• Benign: May be managed by eneucleation
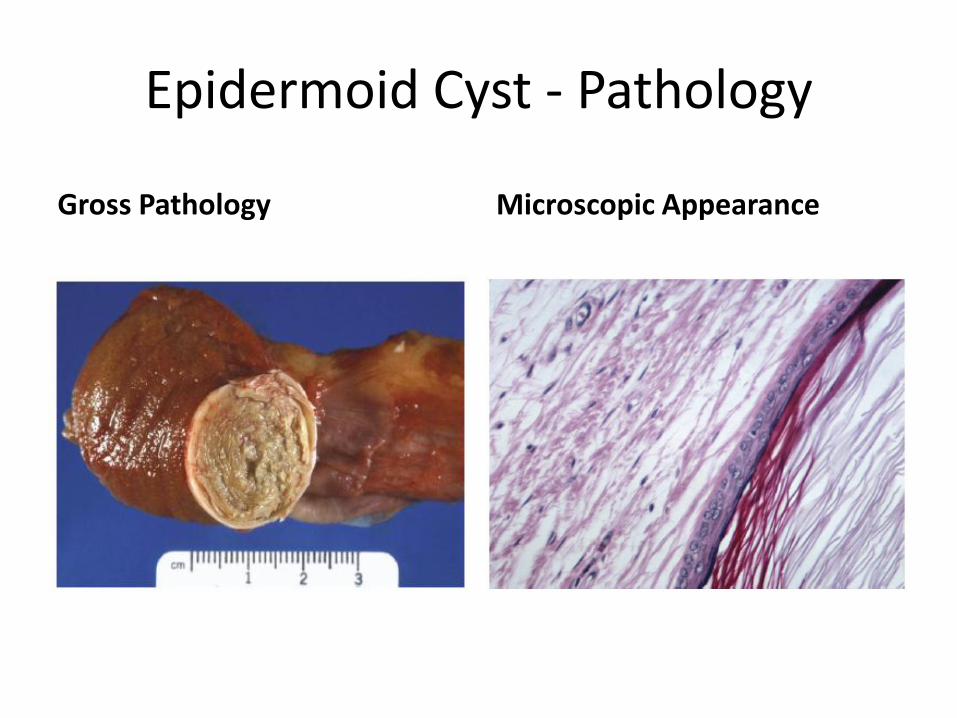
Epidermoid Cyst - Pathology
Gross Pathology Microscopic Appearance
Leydig Cell Tumor
• Most common stromal tumors of testis in children • Peak incidence at 4 to 5 years old • Arise from a common mesenchymal stem cell that can
differentiate into Leydig cells, Sertoli Cells, or granulosa cells
• Secrete testosterone: Cause 10% of precocious puberty in boys < 9 years old
• Classic triad – Testis mass – Precocious puberty – Elevated serum testosterone and urinary 17-ketosteroids
Leydig Cell Tumor (ctd)
• Differential Diagnosis
– Pituitary Lesions
– Leydig Cell Hyperplasia
– Large Cell Sertoli Cell Tumors
– Hyperplastic Testicular Nodules in Boys with CAH
• Treatment
– Resection (testis-sparing) is curative
– Hormonal effects not reversible
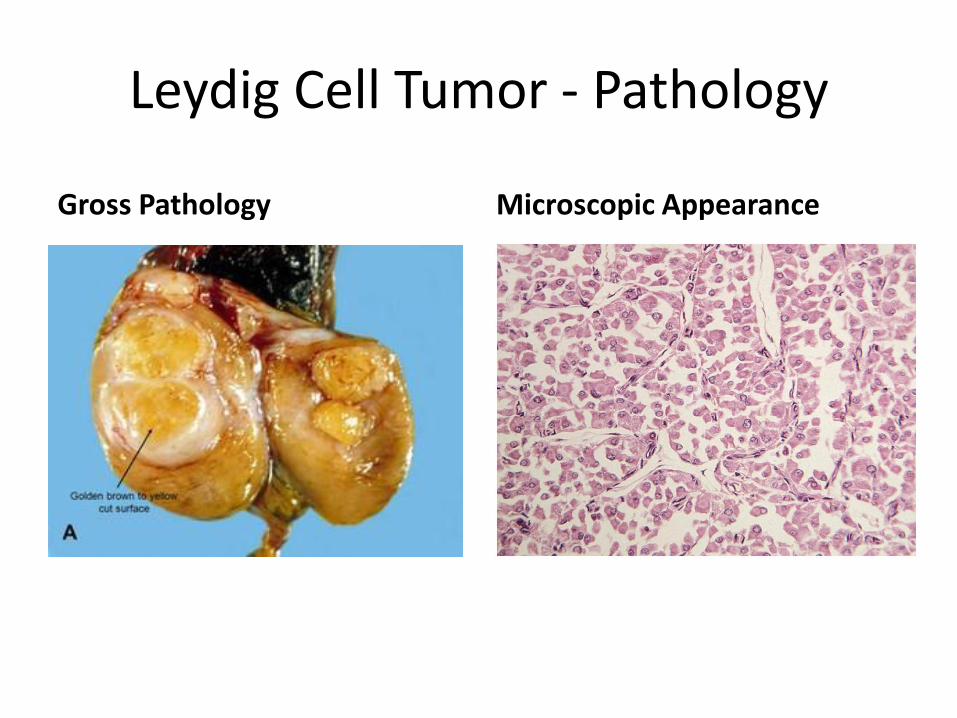
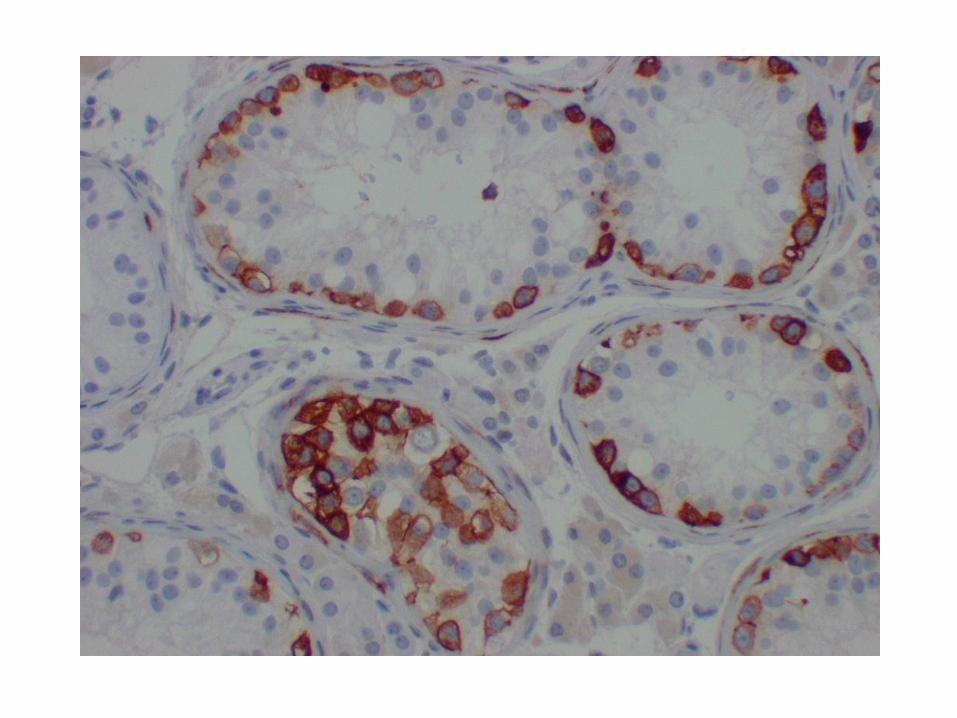
Leydig Cell Tumor - Pathology
Gross Pathology Microscopic Appearance
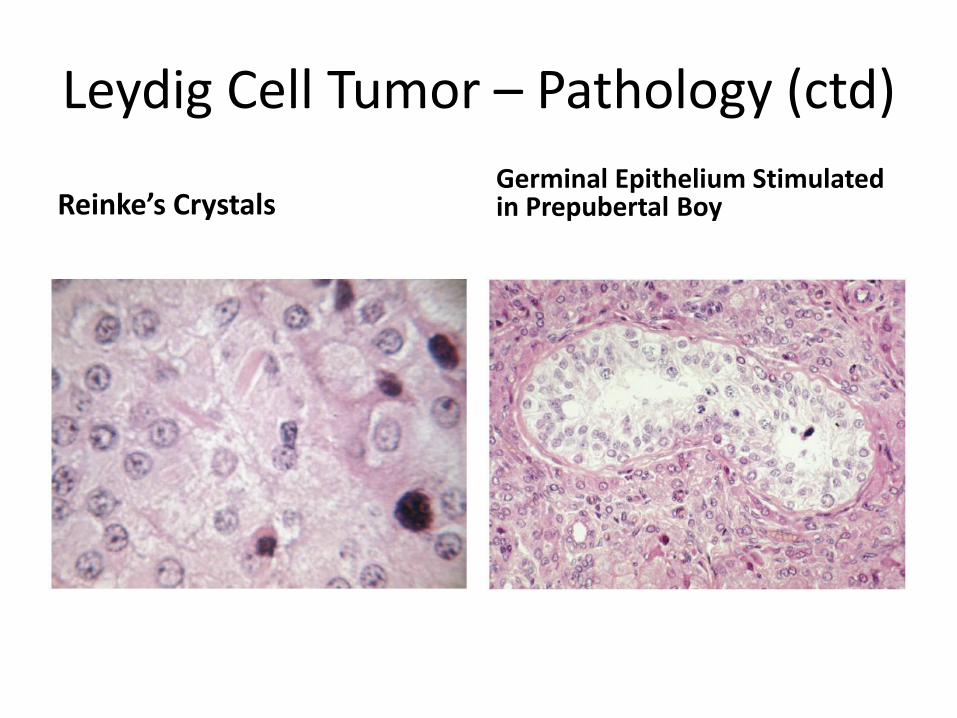
Leydig Cell Tumor – Pathology (ctd)
Reinke’s Crystals Germinal Epithelium Stimulated in Prepubertal Boy
Sertoli Cell Tumors
• Presents at earlier age than Leydig Cell Tumors • 10% Hormonally Active: Gynecomastia most
common effect • 1/3 Associated with Genetic Syndromes
– Peutz-Jehgers syndrome – Carney Complex
• Treatment – Observation in Infants (Metastasis Rare) – Metastasis Can Occur in Older Boys (10% overall rate)
• Orchiectomy (Eneucleation in pre-pubertal boys) • Must Exclude Retroperitoneal Spread
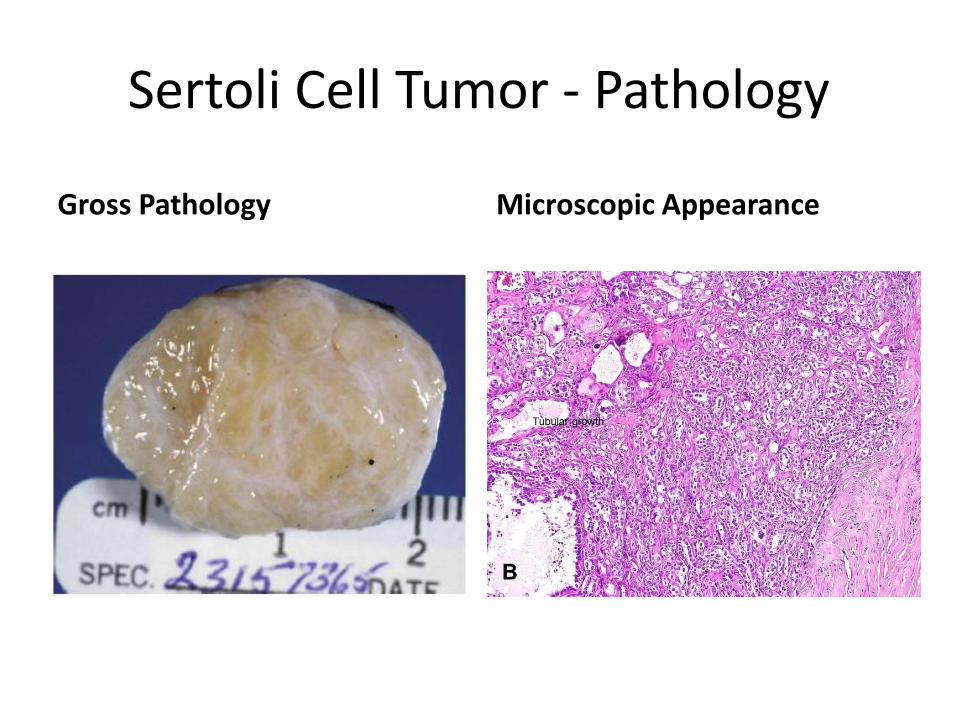
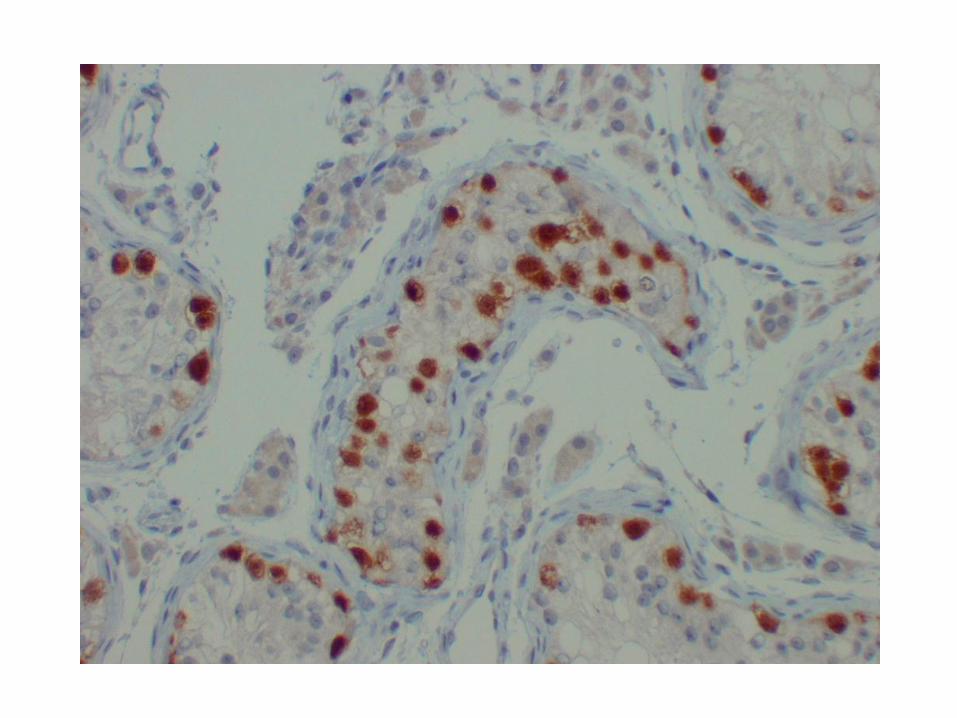
Sertoli Cell Tumor - Pathology
Gross Pathology Microscopic Appearance
Juvenile Granulosa Cell Tumor
• Most common testicular tumor of neonates
• Presents most often in the first 6 months of life (often detected at birth)
• May occur in children with ambiguous genitalia, intersex disorders, and sex-chromosome mosaicism
• Not associated with precocity
• Benign without recurrence
• Eneucleation (testis-sparing) is curative
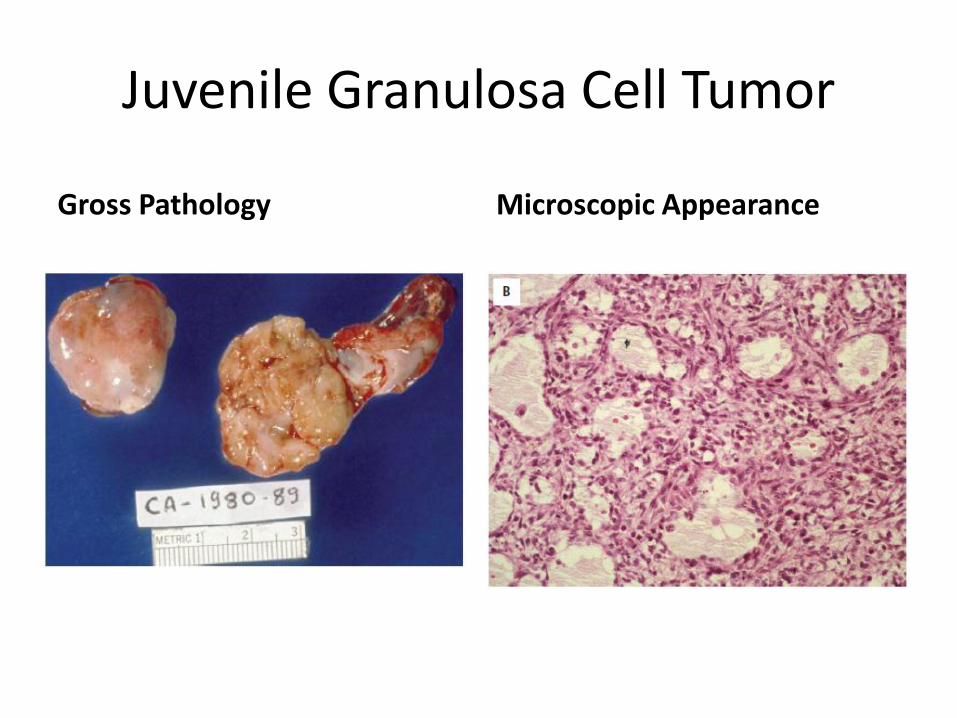
Juvenile Granulosa Cell Tumor
Gross Pathology Microscopic Appearance
Gonadoblastoma
• Found in association with disorders of sex differentiation – Occur in abnormal gonads
• 22% streak, 18% dysgenetic, 60% indeterminate
• Originate in Surviving OCT-3/4 Positive Germ Cells in Areas of Undifferentiated Gonadal Tissue
• Combination of Germ-Cell Tumor and Gonadal Stromal Tumor
– Associated with the presence of Y chromosome • 80% occur in phenotypic females with 46 XY
– Mixed gonadal dysgenesis • 25% risk of tumor formation
• Incidence increases with age
Gonadoblastoma (ctd)
• Occur bilaterally in 10% – 33% of cases
• Benign in childhood
• As germ-cell elements outgrow stroma 10% - 60% will progress to dysgerminoma (seminoma) after puberty
• Treatment: Prepubertal gonadectomies in at-risk patients – All streak gonads should be removed
– All undescended testes should be removed
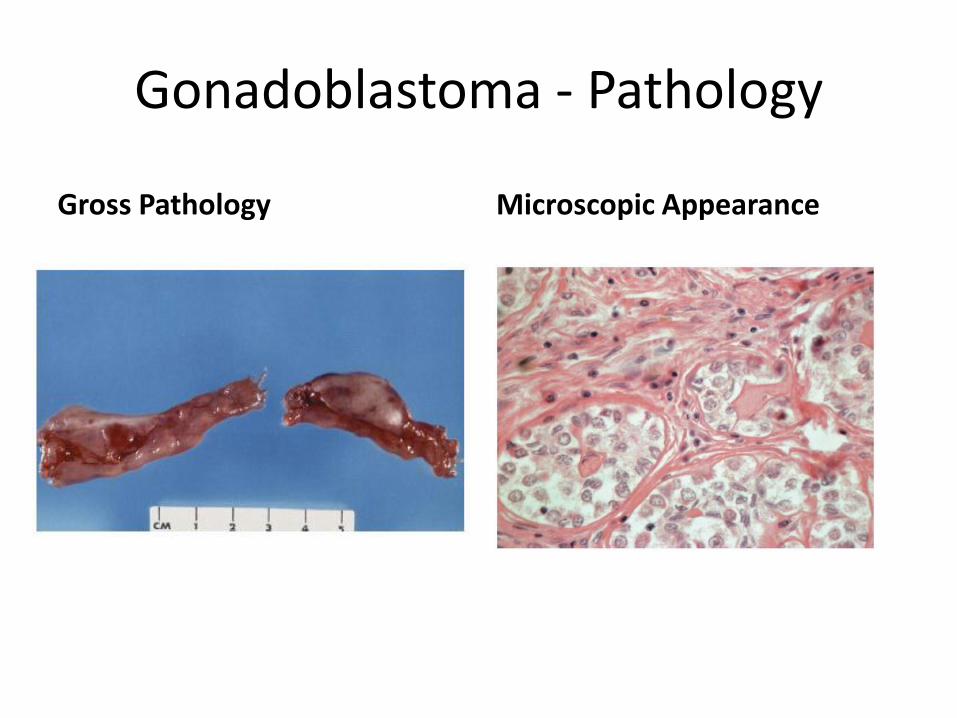
Gonadoblastoma - Pathology
Gross Pathology Microscopic Appearance
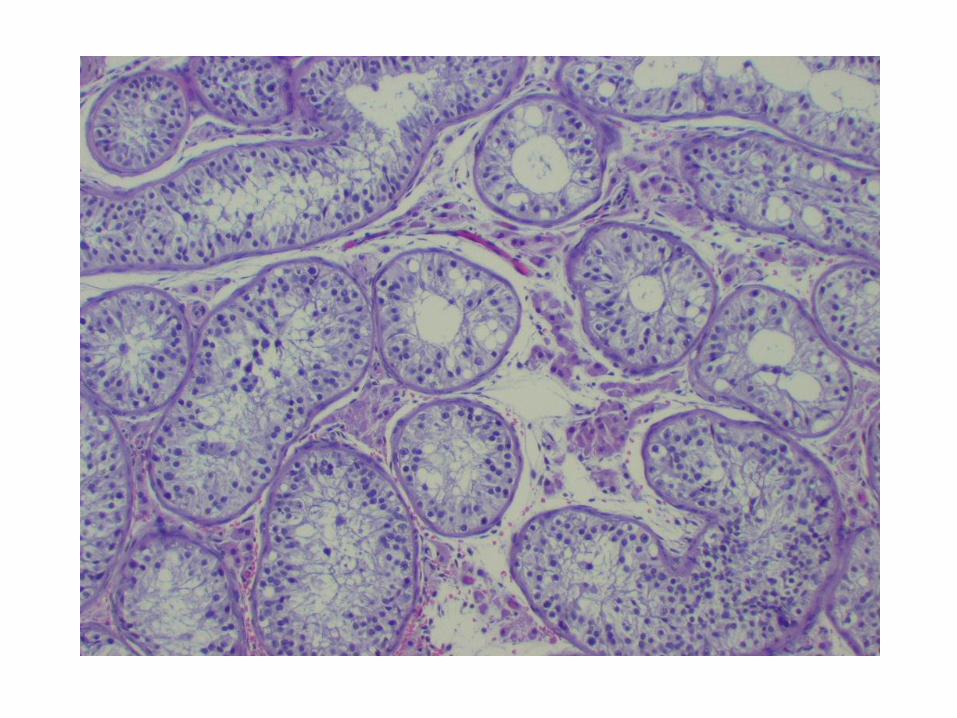
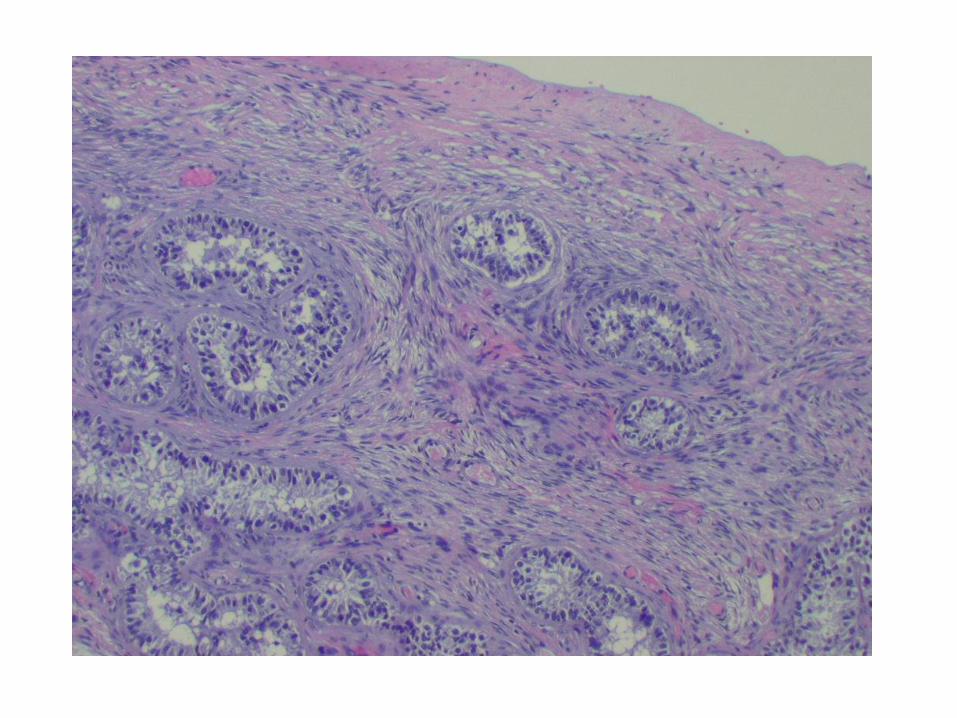
Intratubular Germ Cell Neoplasia
• Carcinoma In Situ
• Found in 80% of testes with malignant germ-cell tumors (8% contralateral) – Rarely in prepubertal germ-cell tumors
• Found in 2% - 8% of testes with cryptorchidism
• 90% of adults will develop a clinical germ-cell tumor within 7 years
• Treatment: Orchiectomy or Radiation
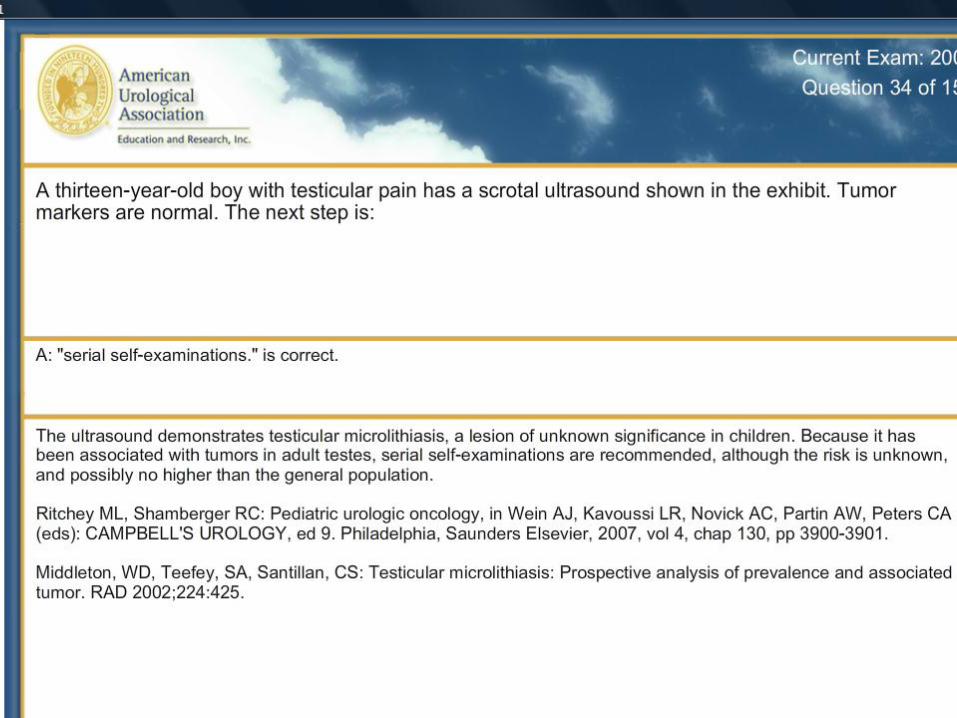
Testicular Microlithiasis
• Calcium testicular stones
• Found (usually incidentally) in 0.5% - 1% of all men, being discovered more frequently in children
• 80% Bilateral
• No confirmed relationship with testicular cancer – But, found in 50% of testes removed for tumors
• Treatment: Testicular Self-Examinations
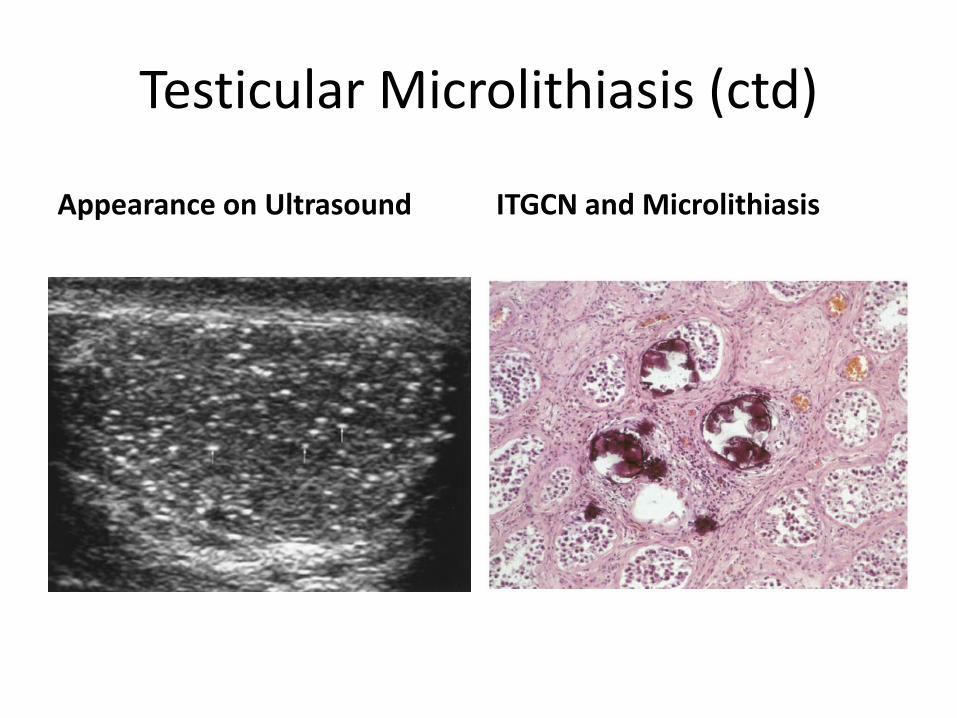
Testicular Microlithiasis (ctd)
Appearance on Ultrasound ITGCN and Microlithiasis
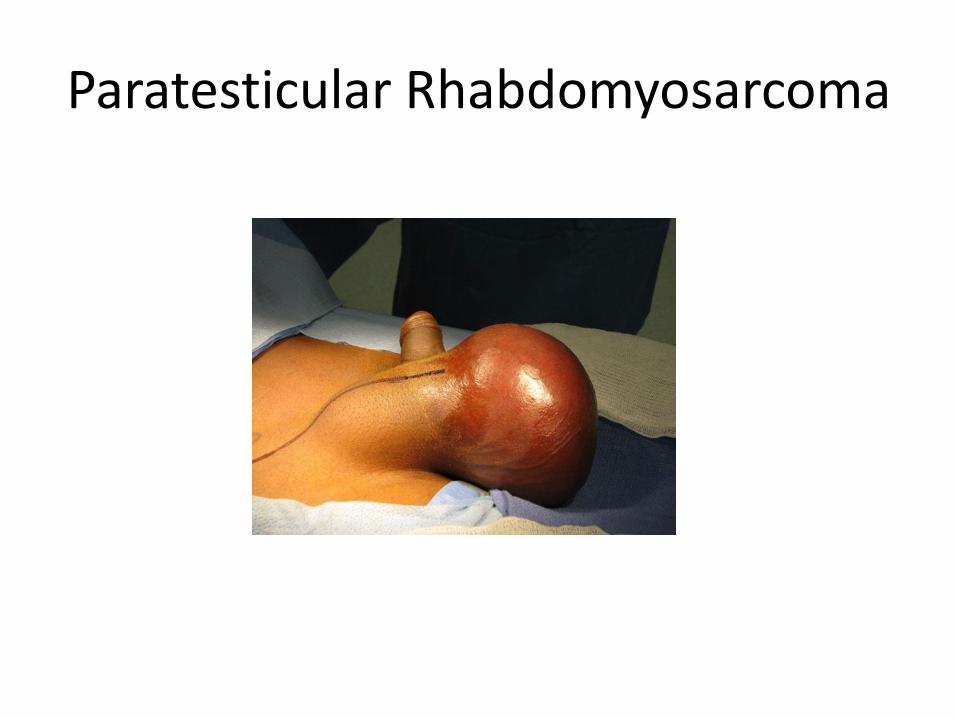
Paratesticular Rhabdomyosarcoma
• 5% of “testicular” tumors • Most often arises in distal portion of spermatic cord
and may invade testis of surrounding tissues • 60% occur in the first 2 decades of life • Bimodal age distribution
– 3-4 months – 16 years
• Arises from mesenchymal tissue – 90% embryonal variant (better prognosis) – 30% - 50% have metastasis (usually lymph node) at
diagnosis
Paratesticular Rhabdomyosarcoma
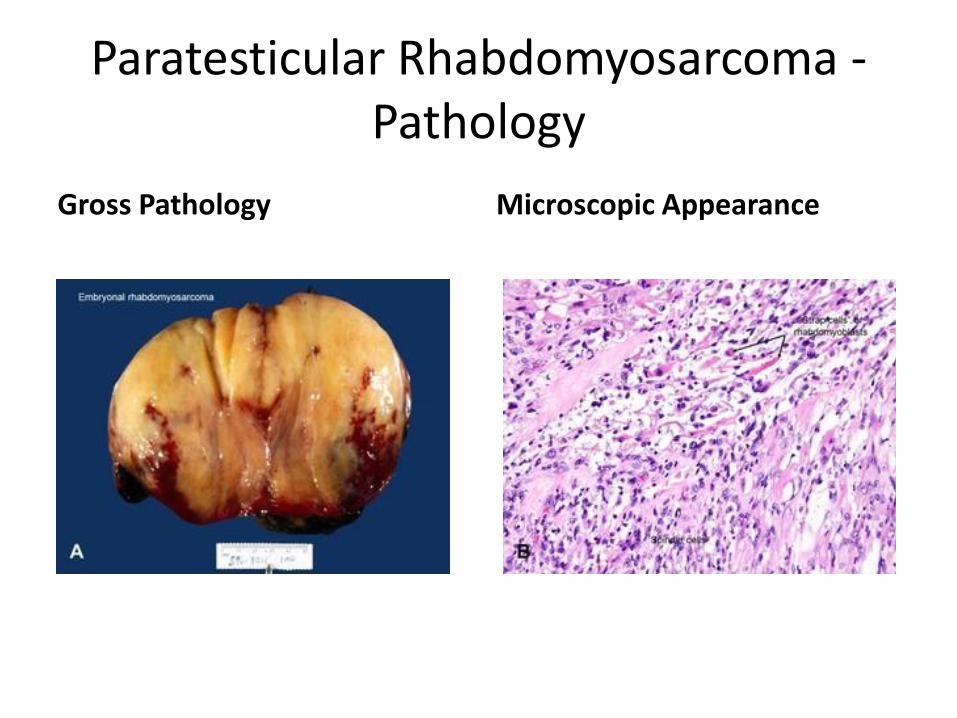
Paratesticular Rhabdomyosarcoma - Pathology
Gross Pathology Microscopic Appearance
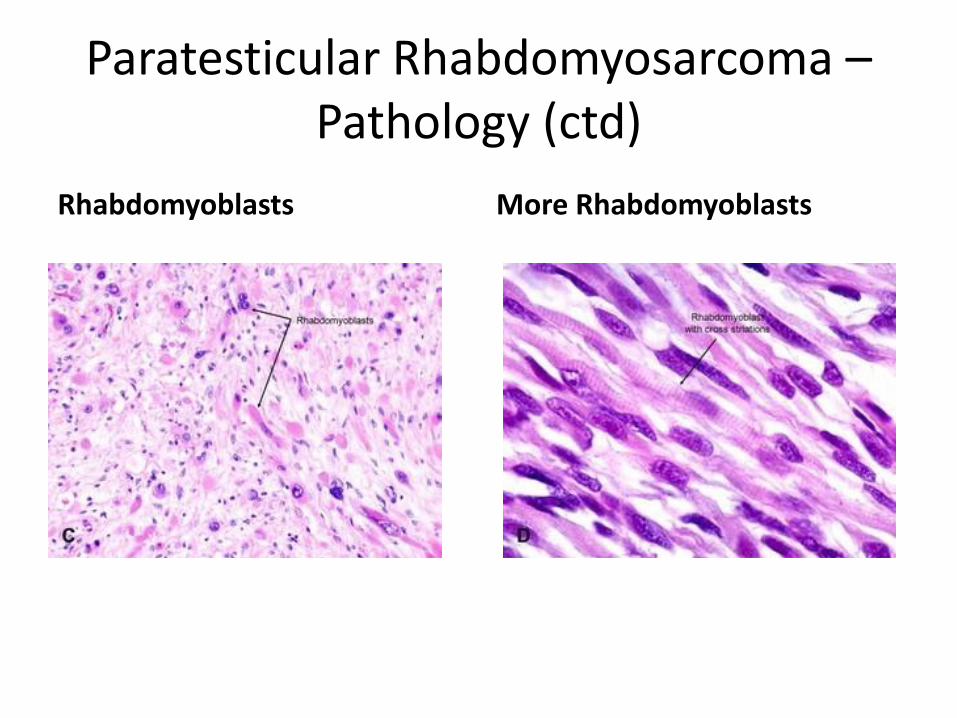
Paratesticular Rhabdomyosarcoma – Pathology (ctd)
Rhabdomyoblasts More Rhabdomyoblasts
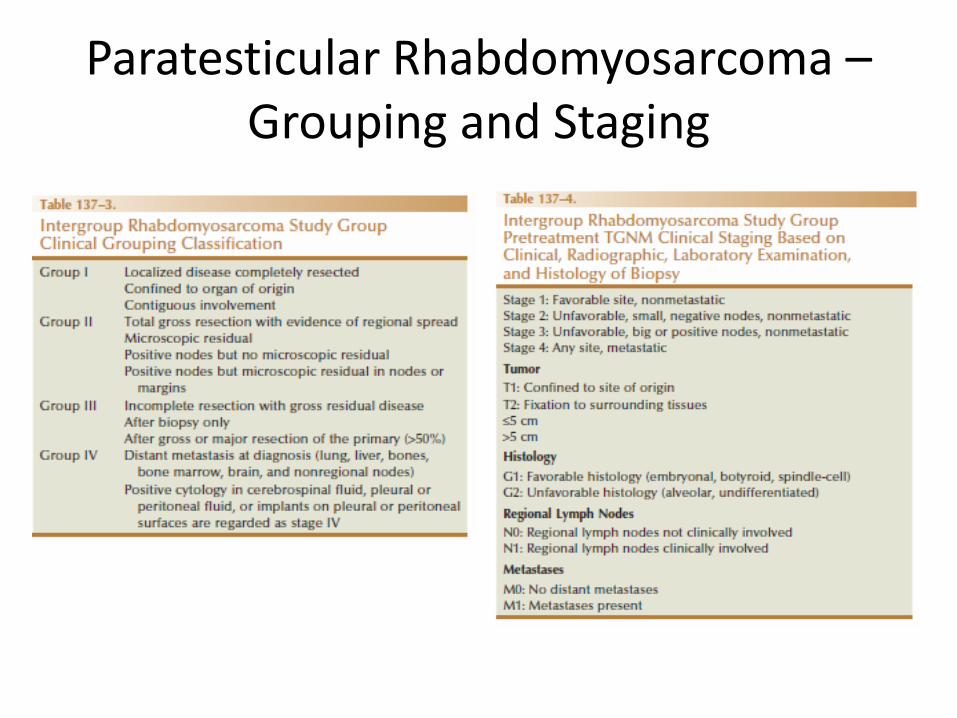
Paratesticular Rhabdomyosarcoma – Grouping and Staging
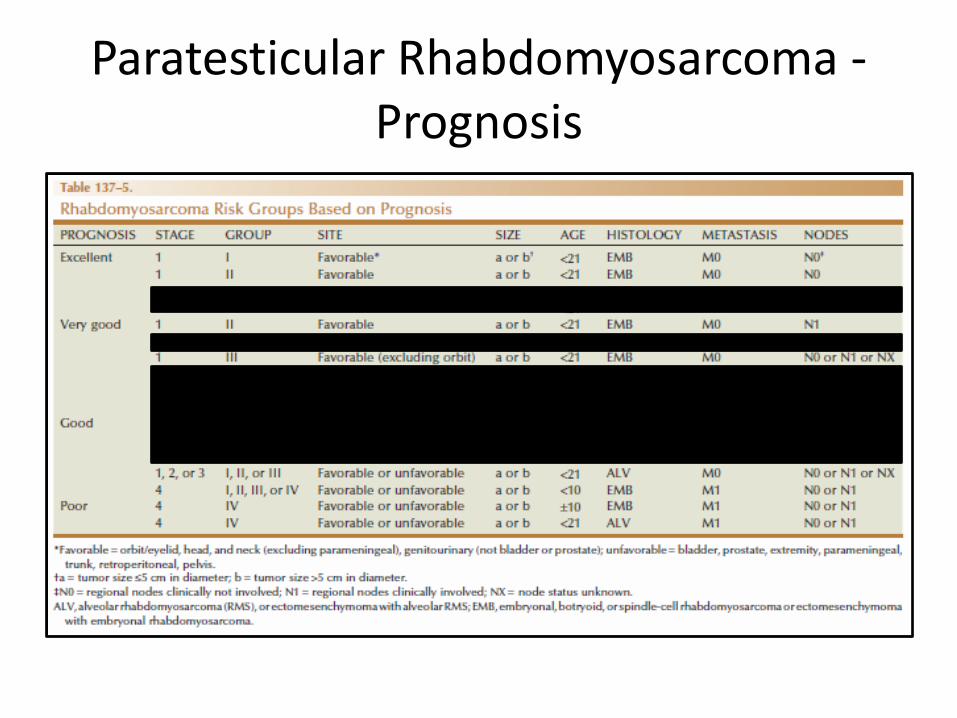
Paratesticular Rhabdomyosarcoma - Prognosis
Paratesticular Rhabdomyosarcoma – Diagnosis and Management
• Usually presents as unilateral painless scrotal swelling or mass that is distinct from testis
• Ultrasound can be used to confirm solid nature of lesion • 60% to 80% are stage 1 at presentation • Initial Treatment: Radical Inguinal Orchiectomy • CT scan for staging
– Enlarged nodes have 65% - 94% chance of positive pathology – 14% false negative rate
• Chemotherapy alone (Vincristine and Actinomycin D) produced 5-year survival of 99.1% in low-risk patients (favorable histology, T1N0M0, Clinical Group I)

Paratesticular Rhabdomyosarcoma - RPLND
• Full RPLND morbid with up to 25% rate of serious complication
• Children > 10 years of age should have ipsilateral RPLND for staging before chemotherapy – Relapse-free survival lower than in younger boys
• Patients with positive lymph nodes require intensified chemotherapy as well as nodal irradiation – VAC = Vincristine, Actinomycin D, Cyclophosphamide
• Overall Survival > 90%