Sympathetic nervous regulation in patients with cirrhosis...
10
REVIEW Sympathetic nervous regulation in patients with cirrhosis: Pathogenesis of fluid retention and formation of ascites JENS H 1-ll:NRIKSEN, MD, HE LMER RING- L A RSE N, MD, NIEL:. JUEL Cl IRIST ENSEN, MD JH HENRIKSEN, H RING-LARSEN, NJ CHRISTENSEN. Sympathetic nervous regulation in patients with cirrhosis: Pathogenesis of fluid retention and formation of ascites. Can J Gast r oentcrol 1991 ;5(3 ): 103- 111. Increased cir- culati l'~ noraJrena line in pat ients with ci rrhosis is Jue to enha nced sympathet ic nervous activity and is not merely the result of decreased clearance of cate - cholami nes. There is a direct relation between the level of arte rial nornJrenaline and severity of cirrhosis, increased portal pressure a nd !luid accumulation; pati ents with th e hepatorena l sy ndrome exhib it the highest values of plasma noradrenaline. In patients with cirrhosi s, the kidneys have been i dcnt ificJ as an unportant source of noradrena line 'spillover' into plasma, which indicates en- hanced sy mpathetic nervous activity in these orgam. Moreover, the level of plasma noradrena li ne is inversely related to renal bloodflow and urinary excre - tion of sodium, an d directly related to plasma renin, vasopress in a nd aldosterone. An increased spi llove r of noradrena line has recently been demonstrateJ in the spl anchn ic sys tem and superior po rtosystemic co llateral s. ReduceJ cent ra l and arterial blood vol ume a nd l ow arterial blood pressure seconda,y to peripheral vasodilation are probably importa nt afferent st im uli for enhanced sympathet ic nervous activity, although a nonvolume-dependent hep atic baroreceptor may also be present. The a utho rs co nclude that the sy mpathetic nervous system, in concert with ot her regulatory sys tems, plays an important role in sodium-water homeostasis a nd fluid retent i on, as well as in the systemic and hepatosplanchnic circ ulatory derange ment seen in pat ients with cirrhosis. (Pour resume, voir page 104) Key Words: Adrenaline , Ascit es, Cirrhosis , Noradrenaline, Sympatheti c over- activity, Underf illing, V asodilation De parrrne nL, of Clinic al rliysiol ogy and Hc /1acol ogy, f ll • idov re Hos pira/ . and Dc/>arcmenc of lnie mal Me dicin e ,md Endo crinol ogy. He rlet•I los/ > i ral. Urn t•ersiry of Copenhagen , Co penhagen, Denmark Corr esponden ce and re/>rint 1: Dr Jens H Hemiklen , Assocza w Professor of Cl mica/ Physiol ogy, Departme nt ofClirncal rh ysrology n9, H111dovre Urnvernr"I I l os f>iwl , DK-2650 Hl'l(lovre, Denmark R eceived for />ublicauon Ja nuary I I , 1 99 /. Acce/> ted Ma y 3, I 99 J CAN J GASTROENTcROL VOL 5 No 3 MAY/JUNE 1991 A IWANCED LI VER DI SEASE (,IVES ri se to serious ahnormalities in fluid dynamics anJ neurohumo ra l rcgul at ion (1 ). The renin-angiotcnsin - aldosteronc syste m, neurohypophyseal release of vasoprcssin anJ the sym- path etic nervous system exhibit major changes in patient s with cirrhosis. Recent re views in these areas have dealt with renin, angiotensin, al do- s tcmnc and vasopress in (2 -4 ). The past decade has seen a major advance in knowledge of the physiology anJ pathoph ys iology of the sympathe tic nervous system. The sympa th etic nerv- ous system and circulating catechola- mines arc cons id ered in this review. Shaldon and co-workers (5) , report- ed in 1961 that there we re high levels nf noradrenaline and aJ renaline in the ponal venous plasma of patients with cirrhns is , and suggested that c at echnl- amines play a role in pona l wnous hy- pertension. However, subseque nt studies with fluorometric assays were una ble to confirm th eir h1oassay find- ing (6-9). Fluorome cr ic methods have now been replaced hy a spt.'Cific isotope- derivative techn i que (1 0, l I) and high performance liquid ch romatography ( l 2). In a 1981 study wh i ch employed an 1socopc-derivacive technique, the 1 03
Transcript of Sympathetic nervous regulation in patients with cirrhosis...

REVIEW
Sympathetic nervous regulation in patients with cirrhosis:
Pathogenesis of fluid retention and formation of ascites
JENS H 1-ll:NRIKSEN, MD, H ELMER RING-L ARSEN, MD, NIEL:. JUEL Cl IRISTENSEN, MD
JH HENRIKSEN, H RING-LARSEN, NJ CHRISTENSEN. Sympathetic nervous regulation in patients with cirrhosis: Pathogenesis of fluid retention and formation of ascites. Can J Gastroentcrol 1991 ;5(3 ): 103- 111. Increased circulati l'~ noraJrenaline in pat ients with cirrhosis is Jue to enhanced sympathetic nervous activity and is not merely the result of decreased clearance of catecholamines. There is a direct relation between the level of arteria l nornJrenaline and severity of c irrhosis, increased portal pressure and !luid accumulation; patients with the hepatorenal syndrome exhibit the highest values of plasma noradrenaline. In patients with cirrhosis, the kidneys have been idcnt ificJ as an unportant source of noradrenaline 'spillover' into plasma, which indicates enhanced sympathetic nervous activity in these orgam. Moreover, the level of plasma noradrenaline is inversely related to renal bloodflow and urinary excretion of sodium, and directly related to plasma renin, vasopressin and aldosterone. An increased spi llover of noradrenaline has recently been demonstrateJ in the splanchnic system and superior portosystemic colla tera ls. ReduceJ centra l and arterial blood volume and low arterial blood pressure seconda,y to peripheral vasodilation are probably important afferent stimuli for enhanced sympathetic nervous activity, a lthough a nonvolume-dependent hepatic baroreceptor may also be present. The authors conclude that the sympathetic nervous system, in concert with other regulatory systems, plays an important ro le in sodium-water homeostasis and fluid retention, as well as in the systemic and hepatosplanchnic circulatory derangement seen in patients with c irrhosis. (Pour resume, voir page 104)
Key Words: Adrenaline, Ascites, Cirrhosis , Noradrenaline, Sympathetic overactivity, Underfilling, V asodilation
DeparrrnenL, of Clinical rliysiology and Hc/1acology, f ll•idovre Hospira/ . and Dc/>arcmenc of lniemal Medicine ,md Endocrinology. Herlet• I los/>iral. Urnt•ersiry of Copenhagen , Copenhagen, Denmark
Correspondence and re/>rint1: Dr Jens H Hemiklen , Assoczaw Professor of Cl mica/ Physiology, Department ofClirncal rhysrology n9, H111dovre Urnvernr"I I losf>iwl , DK-2650 Hl'l(lovre, Denmark
Received for />ublicauon January I I , 199 / . Acce/>ted May 3, I 99 J
CAN J GASTROENTcROL VOL 5 No 3 MAY/JUNE 1991
A IWANCED LIVER DISEASE (,IVES
rise to serious ahnormalities in fluid dynamics anJ neurohumora l rcgulat ion (1 ). The renin-angiotcnsinaldosteronc system, neurohypophyseal release of vasoprcssin anJ the sympathetic nervous system exhibit major changes in patients with c irrhosis. Recent reviews in these areas have dealt with renin, angiotensin, aldostcmnc and vasopressin (2-4 ). The past decade has seen a major advance in knowledge of the physiology anJ pathophysiology of the sympathetic nervous system. The sympathet ic nervous system and c irculating catecholamines arc considered in th is review.
Shaldon and co-workers (5) , reported in 1961 that there were high levels nf noradrenaline and aJrenaline in the ponal venous plasma of patients with c irrhnsis, and suggested that cat echnl amines play a role in ponal wnous hypertension. However, subsequent studies with fluorometric assays were unable to confirm their h1oassay finding (6-9). Fluoromecric methods have now been replaced hy a spt.'Cific isotopederivative technique (1 0, l I) and high performance liquid chromatography ( l 2). In a 1981 study wh ich employed an 1socopc-derivacive technique, the
103

HENRIKSEN et a/
Regulation du systeme nerveux sympathiquc chez les cirrhotiques: Pathogenese de la retention hydrique et formation d'ascite
RESUME: L'augmentation de la noradrenaline circulante chez les cirrhociques est due i'l !'intensification de l'activitc nervcusc sympathiquc et ne rcsu lte pas sculement d'une dim1m1t1on de la clairance des catecholamines. II existc un lien direct entre les taux arteriels Jc noradrenaline et la gravitc de la cirrhosc, l'clevation de la pression porrnle et l'accumulation li4u1dicnne; les patients atteims J'un syndrome heparo-rcnal presencent les valcurs lcs plus clcvecs de noradrenaline plasmatique. Chez les patients ponems Jc cirrhnsc, on a Jctcrm inc que lcs reins sont une source importance de devcrsemcnt de noradrenaline dans le plasma, ce qui mdique unc majorar1on de l'acnv1te nerveuse sympathique au niveau <le cet organc. De plus, lcs tnux plasmatiqucs de noradrenaline som inversement relies au debit sanguin renal et a l'excrcoon de sodium Jans les urines, et directemem relies a la renine, a la vasoprcssme ct a l'aldosrerone plasmatiques. Une augmentation du devcrsemenr de noradrenaline a rcccmment ere demontree au niveau du sysccme splanchnique et Jes branches cnllaterales porto-sysrem1ques superieures. Une reduction Ju volume sanguin aneriel ct central, ct unc baisse Jc la pression artcrielle consecutive a unc vasodilatatton penphenque constituent probablemenc des srunuli afferents importants, qui intens1fient l'activite ncrveuse sympathique bicn que !'action J'un barorcccptcur hepatiquc ne rcpondant pas au volume puisse aussi etrc incriminee. Les auteurs concluent quc, chez les patients souffrant de cirrhosc, le systemc ncrveux ~ympathiquc, agissant de concert avec d'autres mecanismes de regulatton, iouc un role important dans l'homeostase sodium-eau ct la retention hydrique, ains1 quc les perturbations de la circulation sysremique ct hepato-splanchniquc.
present authors found increased levels of circulating noradrenal inc and adre naline in patients with cirrhosis and portal hypertension, which suggested that sympatheu c nervous activity was e nhanced in these patients ( 13 ).
The present review deals with the role of the sympathetic n ervous system in homeostatic derangement, fluid retention and hemodynamic changes in the splanchnic, renal and systemic c irculations m patients with c irrhosis.
PLASMA NORADRENALINE AND ADRENALINE
Sympathetic activity may be assessed by measuring noradrenaline in plasma or by recording impulses m sympathetic nerves by microneurography. Noradrenaline is the ma in neurotransmitter of the sympathe tic nervo us system. It leaks from the synaptic cleft mto plasma, where its concentration reflects its neurotransmitter function (l 1, 14-16). T ungsren microelectrodes can be used to record sympathetic action potentials in human peripheral nerves at rest and during various
maneuvres. A c lose correlation has been observed between plasma noradrenaline in forearm venous blood and sympathetic nerve acttvity m muscles not on ly at rest but also durmg dynamic exercise, mental stress and hypoglycemta. Both plasma noradrenaline and sympathetic nervous activity increase with age (16, I 7).
The arterial plasma concentratio ns of noradre na line and adrenaline are determined from the dynamic equilibrium between overall neuronal and adrenal 'spillover', respectively, as well as from removal of the catecholamines from organs and tissues (18-21). The metabo lic clearance rate can be determined using intravenous infusion of tritium-labelled noradrena line and adrenaline and measuring the steadystare concentration of the tracer in arterial blood. However, the clearance values thus obtained reflect the clearance of catecholamines from all tissues and organs into the systemic c irculat ion. The clearance concept proposed by Esle r et a l ( 19) i:; not valid for n euronally released noradrenaline
(22). C learance of adren a line can l,e interpreted with confiJencc, ~mce it can be pred icted that Lhc specific ac, Livity of adrenaline in plasma ts the same as that at hreakJnwn sites, a pre requisi te for va lid clcarnnce measure, men ts.
Sympathe tic nervous activity minte rnal organs may be stuJicd by measurmg the release of noradrenaline from these organs. The difference between arterial and venous noradrcnalmc 1, corrected for cxrrac.uon of noradrenaline across the organ mcasureJ using intravenous infusion of tritium-labelled noradrenaline mulcipl icd by hloodflow to the organ ( 16,20). S tudies m animal1 have mdicaceJ that overspill 1~ corre, lated to impube activity in sympa1het1c nerves. Presynapnc receptors anJ lex 11
factors, such as bloodflow and capillary permeability, may influence noradrenaline release and overflow (16,20). The effect of activation of the sympathoaJrenal system is dependent not only on impulse activity in nerves or amounts of noradrenaline and adrenal me relea ed, but also on the responsivenci>S of tissue to ca techolamines. This may be altered during vanou, physiological and pathophys1olog1cal states by changes in the number anJ affinity of receptors, as well as by fll.N synaptic mechanisms. Sympathetic nervous system acttvity is highly d1f. fcrenrimed; sympathoadrenal activ1r,, sens1 t1v1ty to catecholamines anJ respom1veness should therefore h.: measured in specific organs or tissues.
The circulating level of nora<lren aline is normal or a lmost normal in cirrhotic patients without flu id retention, whereas patients with asrne, generally have highly elevated value (13,23-28). The increased circulating noradrenaline seen m c irrhosis 1, caused by inc reased release of noradrenaline from po t gang lionic ympathetic nerve fibres because of enhanced sympathetic ne rvous activ1, ty, and is not merely the result of decreased clearance of catecholamines in liver and other tissue (23,29-31). Floras and co-workers (3 2) receml1· found a close relationship between burst frequency in sympathetic nerve fibres to skeleta l muscles and circulat·
104 CAN J GASTROENTEROL VOL 5 No 3 MAY/JUNE 1991

Noradrenaline and ascites formation
PRC • mlU /1 ,.-... 60 0)
2000 I E
• E 50 1000 ...._, Q)
• .... ~
40 • 50 0 U) -U)
• Q) .... Q. • • C 30- • 200 • ·m ••• > • •
100 •• 0 20 -+= •
0 .. r= 0.86 • Q. • 50 Q) • P<0.001 • .c. 10 -• r = 081 D
• P<OOOI Q)
20- • 0) 0 • D I I I
•• • Plasma NA Q) 1.50 10 • • I I I s 0.0 0.50 1.00
0 00 050 100 150ng/ml Plasma NA ng/ml
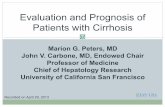
Figure 1) Relatmn between plasmll renrn concenrrntwn ( PRC) and I plasma noradrenalin<! (NA) in />arienrs wir/1 m,·lwsis. ( ReJm1duced from
reference 34)
Figure 2) Relacion ht!tween />cmal />ressure ( assessed as 1uedged he/)CHic 1•em />ressurc) and ancnal plasma noradrenaline (NA) rn J)atiencs with cirrhmi5. ( Rcprnclucecl from reference 13)
ing n0raJ rcnaline in patients with cirrhosis, thus confirming the u5efulne5s o( plasma noradrenaline as an index of sympathetic nervous activity in these patients. Diurnal variat ion in plasma noradrena line anJ urinary excretion of noradrenaline and catecholamine metabolites ind icate that even in the compensated state some pmien ts have a moderate increase in sympatheuc nervous activity (33).
In patients with c irrhosis, c irculat ing norad renaline is d irectly corrclateJ wi th plasma renin activity anJ plasma concentrations of a lJostcrone and vasopressin (24,27,34 ), ind icating that the sympathetic nervous system acts in concert with o the r important regulatory systems (Figure I ).
HEPATOSPLANCHNIC HEMODYNAMICS
Using tritium-labelled noradrenaline, significant proJuction and spilloverof noradrenaline has recen tly been demonstrated in the heparosplanchnic system of patients with c irrhosis, but not in normal subjects (35 ). Cathe terization of the azygos vein substantiated
noradrenaline spillover in the prehcpatic splanch nic area :md superior portosystemic collaterals, including esophageal var ices (36). These resu lts indicate that sympathetic nervous activity is enhanced in different parts of the hepatosplanchnic system, inc luJing porrosystemic collatera ls in patients with ci rrhosis. Moreover, the arteria l level of noradrena line is d irectly related tu portal venous pressure and azygos bloodnow (Figure 2) (13.23.37).
T he exact role of the sympathetic nervous system in the progression of porta l hypertension and increased splanch nic bloodflow is not known; however, Mena et a l (38) reported chat rhentolamine, an alpha-adrcnergic antagonist , lowered hepatic venous wedge pressure. C lo nidine, a cen trally acting a lpha-a<lrcnergic blocker, dec reases both circu lating noraJ renaline and porta l pressure (37 ), and propran o lol, a nonselect ive beca-adrenc rgic blocke r, decreases porta l p ressu re in some patients (39-43). These find ings suggest that the sympathetic nervous system docs play a role in portal hypertension . O n the o ther hand, a sym-
CAN J GASTROENTEROL VOL 5 NO 3 MAY/JUNE 1991
pathetic hepatic baroreccptor has been described m animal experiments, in which a primary inc rease in porral anJ sinusoidal pressure enhances sympathetic nervous activity in heart and kidney ( 44 ). Dogs with experimenta l cirrhosis, but without sinusoiJal hype rtension , do not retain soJ ium and water (45). That such a nonvolume-depcn<lcnt hepauc baroreceptor r lays a role in the increased renal sympathetic tone seen in cirrhotic patients has a lso been suggcstctl ( 46). Thus, the sympathetic nervous system may have imporrnn t afferent as well as effe rent functions in the pathophysio logy of hepacosplanchnic vascular derangement in ci rrhosis.
SODIUM-WATER HOMEOSTASIS
Stimulation of renal sympathetic nerve fibres brings abou t a decrease in rena l bloodflow and glo merular filtration anJ an increase in sodium resorption in the proximal t ubules, the latter occurs because of a combination of decreased bloodflow a.nJ glomerular filtration and a direct effect on alphaadrcnoccptors in the proximal tubules;
105

HENRIKSEN et al
Renal Blood Flow Renal Blood Flow ml/g -min ml/g ·min
5.0 00 r:-0.71 5.0 0 r= - 0.69 4.0
0 0 P<0.001 4.0 0 P<OOOl
3.0 • q,o 3.0 • Bo 0 • 0 • . ~. • • •
2.0 • 2.0 ~ • •
I • J' • •• •• ..- .. • • ,.,. ..
• ,/A • • • • • • •
1.0 • • • 1.0 I • • •
05 0.5
0.3 0 .6 1.2 1.8 3.0 6.0 12 nmol/1
0.3 0.6 1.2 1.8 3.0 6.0 12 nmol/l
Arterial Plasma NA Renal Venous Plasma NA
Figure 3) Relarion between renal bloodflow and arterial and renal venous noradrenaline (NA) . • Cirrhosis wicliow rucire.1; 0 Comrols; • Pau~m with ascites. (Retmxlucedfrom reference 84)
(46-50). In addition , the sympathetic nervous system activates the reninangiotensin-aldosterone system secm, c.lary to a ltered autoregulation, decreased d 1ivery of so<l ium to the distal tubules and a direct effect on the macula densa suhsequent to heta-a<lrenocepcor stimulation (46-48,5 1,52).
Experiments in dogs have shown that gra<led stimulation of the renal nerves, increasing renal sympathetic nervous activity, causes a graded increase of noradrenaline spillover into the renal veins (53). In patients with cirrhosis, the kidneys have been identified as a major source of increased circulating noradrena line ( 13,23.25).
Renal bloodflow is inversely correlated with the plasma concentration of noradrenaline in the renal artery as well as the renal vein (54), which indicates that enhance<l renal sympathetic nervous activity is important for renal vasoconstriction (Figure 3). It is still unclear at which point in the natural history of ascites the sympathetic nervous system begins to play a role. Thus, in the early stages of asc ires some patients may have elevated noradrenaline, but normal renal bloodflow and glomerular filtration rate (31). Using kinetic techniques, considerable spillover of noradrenaline into renal
106
veins has been demonstrated in most patients with fluid retention (23,30, 31 ), as well as a significantly negative corre lat ion between the plasma concentration of noradrenaline and the urinary excretion of sodium (24 ). Moreover, there is an inverse relationship between plasma noradrenaline and the tubular rejection fraction of sodium, and it has been proposed that the sympathetic nervous tone seen in proximal tuhular sodium reabsorption, independent of flow and glomerular filtration, plays a role in patients with ci rrhosis (55). These results suggest that enhanced sympathetic nervous activity plays an important role in the reduced rena l bloodflow and the avid sodium-water retention seen in decompensated cirrhosis and functional renal failure - the hepatorenal syndrome (56).
T he hemodynamic changes point cowards renal hypoperfusion being, at least initially, a normal response to changes in the systemic or splanchnic circulation , leading to decreased urinary excretion of sodium and water ( 46,56). It seems like ly that enhanced sympathoadrenal activity is a primary pathogenic factor, but several connected systems regulating hemodynamics and sodium water homeostasis are secondarily activated (2-4). Nearly a ll
studies of these syMems in chronic liwr disease in<licate that they counteract <lecreascd systemic vascular resistance. In addition, increased urinary excre· tion of proscaglandin Ez has been o~served in patients with decompensateJ cirrhosis; there is decreased excretion in patients with the hepatorenal syndrome. A deficit of local vasodilato~ such as prostaglan<lim has therefore been suggeste<l as a concurrent cause of renal failure in patients with hepato· renal syndrome (27).
Stimulation of renal sympathetic nerves or infusion of noradrenaline into the renal artery in dog~ has revealed that the autoregulation curve may be shifted to the right, so that renal blood flow is diminished at a higher perfusion pressure than normal (52,57). Since the renal perfuskm pressure (te, arterial mean rressure minus renal venous pressure) in advanced cirrhosis is often reduced to a c rit ical level (about 70 mmHg), such a mechanism may play a role in the renal hypoper· fusion seen in patients with decornpensated c irrhosis. The importance of low renal sympathetic tone and a sufficiently high renal perfusion pressure for filtration and sodium-water excretion has been demonstrated by Lenz and CO·
workers (58). In patients with decom-
CAN J GA!:>'TROENTEROL VOL 5 No 3 MAY/JUNE 1991

Arterial Plasma Noradrenaline Concentrat ion ng I ml
- p < 0.01 - •
1.0 - • • -
- • •
• • I 0.5 - • -a-
- 1- • • •
I •
0.0 I I T
CHILD A CHILD B CHILD C
Figure 4) Circulating l>la.sma noradrenaline and severity of cirrhosis as assessed by different C/1i/d classes (A, Band C). Normal range of arterial />lasma noradrenaline: 0.0R to 0.35 ng/mL. (Reproduced from reference 43)
pensate<l c irrhosis they demonstrated that an increase in a rte rial blood pressure maintained by o rnithine-vasopressin infusion, increased the glomerular fil tration rate from 26 to 43 ml/min an<l decreased plasma noradrenaline from 1.74 to 0.87 ng/mL (indicat ing a fall in sympathetic nervous activity). This presumahly was the result nf stimulus to rhe arterial baroreceptors.
There is a better diu retic respome in supine patients than in upright and ambulant ones; th is is probably due to a decrease in enhanced sympathetic nervous activity in the supine position (59), but in the study of Ring-Larsen ct al (59) it was probably due to stimulauon of receptors in the venous pan of the circulation. Recent animal experiments have shown that symp:nhetic renal denervation normalizes sodium and water excretion in experimental cirrhosb (60), and that lumbar sympathetic block improves renal function in cirrhotic patients with severely impaired renal function (61 ), confirming the central role of the sympathetic
nervous system in the pathogenesis of ascites. Moreover, enhanced renal sympathetic nervous activity seems to play a role in the decreased responsiveness to atrial natriuretic factor observed in decompcnsated c irrhosis (62). This is consistent with the concept of an important sympathetic neuronal contrihution to the development of refractory ascites.
Fina lly, increased renal sodium and water excretion follows normalization of c irculating noradrenaline after implantation of a peritoneal-venous shunt (63). T hese resu lts stress the virnl role played by the sympathetic nervous system in lluiJ homeostasb in patients with c irrhosis.
SYSTEMIC HEMODYNAMICS The leve l of plasma noradrenaline is
directly related to the severi ty of cirrhosis determined by C hild-Turcotte classes (41) (Figure 4), and changes in the systemic circulation are related co deranged splanchnic hemodynamics and portal hypertension (27,56,64.65).
CAN J GA~TROENTEROl VOL 5 No 3 MAY/JUNE 1991
Noradrenaline and ascites formation
The etiology of the hyperkinet ic circu lat ion seen in cirrhosis is unknown. The find ing of increased lol:11 p lasma volume in human and experimental c irrhosis suggests overfill ing of the circulation (66,67). On the other hand, the effect of head-tiut water immersion or implantation of a peritoneal-venous shun t hringing ahout natriuresis in some patients suggests central underfilling (63,68). Thu~. the me of t he 'effective blood volume' in cirrhosis i~ not settled (69). However, using cardiac output and mean circulatory transit time, centra l anc.l arter ial blood volume has recently been shown to he reduced in patients with c irrhosis ( 70) and inversely related to the level of arteria l noradrenaline, as well as to renal venous noradrenaline (unpublished data). This finding indicates that 'unloaded' volume-receptors and hamreceptors may serve as a stimulus for the increased sympathetic nervous activity seen in patients with cirrhosis. In line with this theory, it has been hypothesized that peripheral arteriola r vasodilation is an initiator of enhanced sympathetic nervous acuvrty and sodium-water reten tion in the presence of c irrho~is (65).
Enhanced sympathet ic nervous activity is important in maintaining the level of arterial blood pressure in cirrhosis. Thus, administration of alphaadrenergic blocking agents such as phentolam ine results in a decrease in the arterial blood pressure of dccompensated p,itients, a result which underl ines the importance of the sympathetic nervous system in counteracting the effect of peripheral vasodilation in c irrhosis (3, 7 I). Beta-adrenergic hlock~ ers, such as propranolol, increase circulating noradrenaline (43), possib ly due to the comhined effect of a decrease in the whole-body clearance of ca techolamines and a further increase 111 sympathet ic nervous tone (36). Further enhancement of sympathetic nervous activity after beta-adrenergic blockade may be caused by: unopposed alpha-adrenergic receptors; induction tif hernodynamic changes with reduced arteria l hlood pressure and cardiac and splanchnic flow rates; and metabol ic <.: hanges (42). A relationship between
107

H ENRIKSEN et al
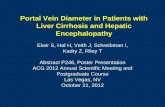
CUMULATIVE SURVIVAL PROBABILITY IN 81 PATIENTS WITH CIRRHOSIS
I. 0
0 .8
!L------, f," : 11 ... ,
11 ... , ... ... , ...... I
f1, a NA ~1.5 nmol/1 -1~ -· - ·-1 - · - · ·:... _; .............. ( ........ ..... . ,
0. 6
1 ·-·- · - · - · , , .... . .. ... . ... b l.5<NA~25nmol/l -: ·- ·- · - · - · - · - · c 2.5<NA=i;;5.0nmol/l
0 4
-------, 0 . 2 1 --- ---- -d 5.0nmol/l<NA
0.0-!.--~-~-- ~-~~-~-~--,---, 0 2 3 4 5 6 7 8
Observation period (years )
Figure 5) Cumulative survival probability in 8 / Cirrhotic />auenr.s with different leveL~ of circulating noradrenaline (NA). ( Heproduced from reference 88)
sympathetic ne rvous ac tivity anJ vasndilaror systems (cg, glucagon, prosrnglandins, substance P, cnkephalin , calc ironin gcn e- rclateJ peptide, amt endothclia l-J erived relaxing facrnr) has been described (27 ,71 -7 5) , but the role of sympa thetic ne rvous activity in hemodyna mic adjustment anJ parhophysio logy of the ci rculato ry derangement seen in c irrhosis is stilt unclear.
VASCULAR REACTIVITY AND SYMPATHETIC NEUROPATHY
Head-up til t increases sympathetic nervous acn vity anJ c irc ulating no radrena line in patients wirh c irrhosis (25 ) as well as in norma l subjects. Ho wever, autonomic J ysfunct i\ln in ci rrhosis, owing to fab e o r we,1k neurotransmiucrs, has been implied. Bernardi ct a l (28 ) repo rted that octopamme a nd bcta-phe nylechano la mine inc reased in pa rallel with noradrena line in patients with cirrhosis during head-up tilt. The patients did no t achieve an adequate rn rdiovascul,1r response, and the <1uthors concluded that hyperproduct iun of weak neurotransmitters was, at least in pa rt, responsible for the attenuatio n. However, post synaptic alpha-adrenoccptors might already be occupied by endogenous catecho lamines Jue to enhanceJ sympathetic nervou~ rest ing tone, consistent with the blunted prcssor response co exogeno us no radrenaline in the pre ence of cirrhosis (76). Reduced vascular reactivity to angiotensin II and noradrena line has been
described in experimental ponal hypertension an<l c irrhosis (77,78), but the results produced by exogenous vasoconscric tivc agents on vascular react iv ity in humans are conflicting. In patients with advanced liver <liscase, Lenz ct a l (79) recorded a normal inc rease in systolic blood pressure in respo nse to infusion of vasoconscrictive agem s, noradrenaline and angiorcnsin II. In fact. t he response was greate r than m a group of young healthy controls.
By tilting cirrho tic patients to a 60° head-up position , Ring-La rsen e t a l (25 ) observed a no nnal noradrenaline response, ic, rapi<lly increasing concentrations of noradrenaline in .-1rterial plasma. The a bsolute level of arterial noradrenaline was well above no rmal in t hcse patients, but the incre ment was normal, which indicates cha t their volume and ba rorecep tor-mediated responses were intact.
A lte red hcta-adrcnc rgic respo nsiveness may a lso play a role in sqme of the hemodyn amic disturbances in liver disease. Gerhes ct a l (80) found evidence of decreased betaadrcnocepwrs in leukocytes, and Ramond e t al (81) found a decreased sensitivity to isoprc na line in patients with c irrhosis. Lee ct al (82) recently fo un<l evidence for a selective down-regula tion of bc ta- 1-adrenergic receptors in experimenta l ci rrhosis whc ih may be responsible for the ohscrveJ myocardia l hyporcsponsivcncss ro catecho lamines.
An alcoho lic sympathetic neuropathy has been suggcsteJ and accor<l-
ingly there arc indications that sympathet ic fi bres may he damage<l in alcoho lics ( 83 ,84). Most paticncs with ad vanced alcoho lic liver disease have raised levels of c irculating noradren· a line indicating a high degree of sym· pa the tic react iv it y, al t hough the maximal sympathetic response may be somewhat blunted. T hus, alcoholic sympathe tic ncurop,llhy remains to he proven (85 ).
CONCLUSIONS Most of the current knowledge of
the sympathetic ne rvous ~ystcrn has been gaincJ from stud ies of groups of patients wi th c irrhosis of varying seve rity. Longitudinal srud ies of the s ingle pa t ient from the we ll compen. sate stage to inc ipie nt fl uid retention to tense asc ites, and full -blown hepato· renal syndrome may reveal unknown facets of the sympathet ic nervous system and other regulatory systems in cirrhosis. T his ho lds especia lly tnic forche time course of activat ion of the sym· pathetic nervous system, the renin-angio tcnsin-aldostcronc sysrem, anJ vasoprcssin release. The re lat ivc contribu tions of these sys tems to maintenance o f a rteria l hlood pressure is not suffic ientl y elucidated. Peripheral bloodflow (shunt flow and capillary bloodflow in ske letal muscles, suhcutancous tissue, fau y tissue and skin) and the coronary circula tion are poorly investigated in re la tion to sympathetic nervous activity.
C ha nges in body position, phy,ical exerc ise and food intake arc m hcr issues which involve rhe sympathcuc nervous system, hue knowledge ts limi ted in patients with c irrhosis. The role of a numbe r of o ther important regulatory systems, incluJing atrial natriuretic fac to r, po tent vasoJ ilator systems and important humoral metabo lic mediators such ,ls insu lin anJ g
0
lucagon , a rc also top ics for future re· search . A ltered renal au toreguh1tion, fa lse neurotransmitters, c hangcJ affinity of a lpha- and bern-adrenocept<m, and auto nomic neuropathy a lso Jc. mand furt her research ( 86,87), as docs rena l sympa thetic de nervation , either surgical o r pharmacological.
A lthough major prob lems arc un·
108 CAN J ClASTROE:.NTl:ROL VOi 5 No> M A Y/jUNF 1991

solved, it is the authors' v iew that the sympathetic nervous system plays a vital role in the pathophysiology of the circulato ry and homeostatic derangement seen in c irrhosis (88). This view 1s partly borne out by thc- fact that the
ACKNOWLEDGEMENTS: The author, txpress their gratitude to Ms Bente Henriksen and MsGri th lngemann for their skillfu l secretarial help.
REFERENCES l. Sknreck, KL. Brenner BM. BoJ y nuiJ
homc,i,tasis in patients w1rh cirrh,1s1, of the liver. Am J MeJ 1982;72:323-38.
l. Better OS, Schrier RW. Dbturhed volume homeostasis in patients with cirrhosis of the liver. Kidney Int 1983;21:303-1 l.
3. Epsrcin M. The Kidney in Liver Disease, 3rd cdn. R,1ltimure: William, and Wilkins, 1988.
4. Bichet D, Swrnlmv,cz V, Chaimovitz C, Schncr RW. Role of vasopress tn 111 abnormal warer excret ion in cirrhmic patients. Ann Intern Med 1982;96:4 13-7.
5. Shaldon C, Peacock JI I, Walker RM, Palmer DB, B,1drick FE. The p,,rrnl venou, content of adrenaline ,md nurnJrenaline in porrnl hyr,cn cmiun. Lancet 1961;i:957-6l.
6. Siegal JI-I, I hirri,on RC. Portal vcnou, catecholamine:, in portal hyperten,ion. Lancet 1963; 11:1157-8.
7. Evans CS, K,1y W. Catecholamine;, in portal venous hluod in portal hypertensinn. Lancet 1964;ii :387-8.
8. Joly J-G, Leduc J, Bernier J, Lavoire P, Viallet A. Catecholamine levels in portal , hepatic anJ systemic venous blood in portal hype rtension. Lancet 1967;it: 121-3.
9. Cipilc,1 A, Buhuianu E. Cerchrospinal fluid -, blnoJ-, and a,citcscatccholamincs in hepatic cirrhosis. Physiologic 1979; 16: 19-24.
JO. Christensen NJ. Plasm:ci noradrenaline and adrenaline in patient, with thyroroxico~is and myxcdcma. Clin Sci 1973;45: 163-71.
II. Cryer PE. lsotope-Jerivari vc mcnsurcmcnt, of plasma norcpinephrmc and epinephrine in man. Diabetes 1976;25: l071 -85.
12. HjcmJahl P. Catecholamine measurement, hy high-peformance liquid chromatography. Am J Physiol 1984;24 7:E 13-20.
I}. Henriksen JH, Christensen NJ, Ring-Larsen 1-1 . Noradrenaline and adrenaline concentrations in vannus
ci rculm ing level of nnrndrenal inc hears a close relationship to the ~urvival of patients with c irrhosis (Figure 5) (89, 90). There may be discrete signs of autonomic sympathetic neuropathy, but most investigatinns of cirrhotic
vascular hcd, in pattcnts with cirrhosis. Rclatilm to haemt1dynamics. Clm Physil1l 1981; 1:293-304.
14. Cryer PE. Workshop on catecholamines anJ meraholbm. Am J Physiol 1984;247:El-74,EI 37-220.
15. Hjcmd,11 P. Plasma c.itechnlamincs a, markers for ,ympatheuc-,1drrnal activity in man: A workshllp. Acta Phys1ol Scand 1984;(Suppl 527):1-54.
16. Christensen NJ, Henriksen 0, Lassen NA. The sympatho-adrenal system. Physiology and Pachophys1nlogy. New York: Raven Press, 1986: 1-512.
17. Wallin BG, Sund liifG. Eri ks,on BM. Dominiak P, Grobecker 11, Lindhlad LE. Plasma noradrenaline correlate~ m sympathet ic mu,cl.: n.:rve ,Kti,·ity in normurrnsivc man. Ac ta Physiol Scand 1981; 111 :69-7'l.
18. Brown MJ, Jenner DA, Alltson DT, Dolcry C..'T. Variations in inJividunl mgan release of nnradrcnal inc me,hured by an improved raJ1ocn:ymai1c technique; l1mm11inns of peripheral venous measurements in rhe assessment of sympathetic nervous activity. C lin Sci 1981;61:585-90.
19. Es ler M, Willet I. Leonard P, ct al. Plasma nmadrcnalin.: kinetic, in humans. J Autun Ncrv Syst 1984;11: 125-44.
20. Ch.ri,ten,cn NJ, H.:nnkscn J 11 . Degrndatton of en,k1genous catecholamines. In: I knrikscn JI I, eJ. Degradation of B1oact1ve Substance,: Physiology and Pathophysiology. B,1ca Raton: Uniscicncc CRC, 1991:289-305.
21. Pcronnet F, Bel iveau L, Boudreau G, Trudeau F, Bn,son G. Nadeau R. Regional plasm,1 catecholamine removftl and release Ht rc,,i and cxerctst' in dogs. Am J Physiul 1988;2 54:R663-72.
22. C hrbtenscn NJ, Hcnrtkscn J 11. Tora I norepincphrinc spi llover. Hypcrtenswn l 988; 12:468-9.
2 3. I lcnriben JI!, Ring-Larsen H, Kanstrup 1-L. Christemen NJ. Splanch111c and rena l elimination nnd release li( catecholamines in cirrho,b. Evidence nf enhanced ,ymparhettc nervnus activity in patients with decompensated cirrho~is. Gut 1984;25: 1034-4 3.
24. Bichet DG. Van Putten VJ, Schrier RW. Potential role of increased sympathetic activity in 1mpaireJ
CAN J GASTROENTEROL VOL 5 No 3 MAY/JUNE 1991
Noradrenaline and ascites formation
patients point to an intact sympathetic nerVllUs system, highly activated secondary to ch ronic stimulation of volume receptors and harorcccptors, ;is a result uf unJcri.illmg of the central and arterial parts of the circulation .
sodium and wmer cxcrct ton in cirrhosis. N Engl J Med 1982;307: 1552-7.
25. Ring-bmcn l l, I lcsse B. I lcnribcn JH, Chri.tcnsen NJ. Sympmhctic nervous activity and renal and systemte hemuJynamics in cirrhusi> - Plasma norcpmephrinc conccntr:ition, hepatic extraction, anJ renal relea,c. l lcpatology I 982;2:304- 10.
26. Burghardt W, Wemzc H, Schaffrath I. Changes of circuhu ing noradrcnalme and adrenaline in hepatic cirrhosi> -Relation to stage of J iseasc, liver and renal function. Acta Endocrinol I 982;99(Suppl 246): 100-l.
27. Arroyo V, Pl:inas R, Gaya J, ct al. Sympni hct1c nervous ac tivi ty, rcnin-,mgiotcnsin system and renal cxcrcttcm of prostaglandin E-2 in c1rrhos1s. Relation to functional renal f:11lurl' and sodium and water cxuet tlln. Eur J Clin I nvcst 1983;13:271-8.
28. Bernardi M, Trev1siani F, Santini C, el al. Plasma nmcpincphrine weak nrumtr:insmttters, and renin activity durmg acrive tilting in liver cirrhosis: Rclatiunship with cardiovm,cular lmmeo,t11,1s and renal function. I lcpatolngy l 983; 3:56-64.
29. Nicholls KM, Shapirn MD, Van Puttcn VJ, ct al. Elevated plasma nl1rcpmephnnc conccnrrn tions in J ec,impcns;ncd cirrhosis. Association with increased secretion rates, normal de,mmcc rates, :rnd supprcssihility by comm) hlood volume expansion. Circ Res 1985;56:457-61.
30. Wi llet I, S ier M, Burke F, Leonard P, Uudl.:y F. Tmal and renal sympathetic nervous system activity in alcoholic Ltrrhosis. J I lcpatol 1985;1 :639-48.
'3 I. Henriksen JI !, Chrbtcnscn NJ, Ring-Larsen H. Continuou:, infusion of tracer norcpincphrine may miscalculate unidirectional nerve uptake of nt1rcpinephrine in man. Circ Res 1989;65: 388-95.
'lZ. Floras JS, Legault L, Morali GA, I Iara K, Blend is LM. Increased sympathetic outflow in cirrhosb and ascitcs: Direct evidence from intrancural recordings. Ann Intern Med 1991;114:373-80.
3 'l. Bcmardi M, Trcvisoni F. DcPalm,1 R, ct al. Chronolob1ological evaluation of sympathoadrcncrgic function 111
cirrhosis. Relationship with arte rial pressure and hcnrt rate.
109

HENRIKSEN er al
Gastrocnterology 1987;93: 1178-86. H. Hennl..:,en JI l, Rmg-Lmcn 1 !,
Christensen NJ. Plasma n11raJrcnalmc m patient, with liverc irrh1,,is 111 relation to ascirc, and treatment. C lm Phys1ol 1981 ;(Suppl 1 ):66-70.
35. I lcnrikscn JH, Ring-Lar-.cn 11 , Chmtern.cn NJ. I lcp,11 ic imc.,tinal uprnkc anJ rcle.1,c of catet:holamme, m alcoholic cirrhns,,. EviJcncc of cnh,mceJ hepatic mtc,tmal ,ympathctic nervou, act1v IL y. Gue 1987;28: 16}7-42.
36. BenJt<;en F, Christensen NJ, Swcn,cn TIA, I lennbcn JI l. Effeu of oral propranolol on ;1zygos, renal and hepatic uptake .111J output 1if rntcchol.11nme, in urrhosi,. I lcpmology. (Jn press)
37. Moreau R, Lee SS, I laJcnquc A, Brnillon LA, Lchrcc D. Hcmo<lynamic dfcct nf a do111J111c-111<luu:J Jccrca,c in sympathetic rnnc 111 patients with c1rrhos1s. I lcpatnlogy 1987;7:149-54.
38. Men., I, Orrego 11, Bamona E. Maqucs S. Effect of reg1t1ne and rcscrp111c on portal hypertension. Am J Dig Dis 1963;8:895-903.
39. Lebrcc D, Noucl (), Corh1c M, Bcnhamou J-P. Pmprnnolnl. A meJicnl treatment for portal hypcncns1on ! Lant:er I 980; ii : 180-2.
40. Bosch J, Masri R, Kravec: D, ct al. Effects of pmpranolol on azygm venou, hloo<l flm1 nd hepatic and systemil hemodynamics in cirrho:,i,. I lepatology 1984;4: 1200-5.
41. Garcia TG, Grnce ND, Grnszmann RJ, ct al. Short term cffcLL of propranolol on portal venous prl",surc. I lcparnlogy 1986;6: IO 1-6.
42. Bendtsen F, Henriksen JH, Becker U, S0rcnscn TIA. Effect of orn l propranolol on splanchnic oxygen uptake and hacmodynam1c:, in p:irient, with cirrhosis. J I lcparol 1987;5:137-43.
43. Bendn,en F, I lennbcn JI I, &,,rensen TIA, Christensen NJ. Effect of oral propranolol on c1 rcu laung catecholamines in cirrhosis. Rehuionsh1p to severity of Ii vcr di~ea:,e and splanchnic haemoJynamics. J Hcpaml 1990; 10: l98-204.
44. Kostreva DR, Casrnner A, Kamp inc JP. Reflex effect of hepatic b:irorcccptors on renal anJ carJiac sympathetic nerve activity. Am J Physiol I 980;238:R390-4.
45. Unikowsky B, Wexler MJ, Levy M. Dogs with experimental c1 rrho:,1:, of the liver hut without intrnhepatic hypcrtens1cm do not retain sodium or form ascites. J C lin Invest 1983;72: 1594-604.
46. Oi&ma FG. Renal neural activity 111
hcparorenal syndrome. Kidney Int 1984;25:841-53.
11 0
47. D1Bon.1 CiF. NeumgeniL regulations of renal tubular sodium re-absorption. AmJ Phys1011977;233:F73-81.
48. D1Bona GF. The functions of the renal nerves. Rev Physiol Ph.1 rmacol I 982;94:75- 18 1.
49. Pn'l>nirz EH, D1B0na GF. Effect of decrc..iscd renal sympathetic nerve ,Kuvity of renal tubular soJ1um reahsorpt1on. Am J Phys1ol 1978;2 35:F55 l-63.
50 &,llo-Ruc:;.., E. EffcLl of carecholammcs in fluid reabsnrption hy the 1,olateJ proximal convolutl·J tuhule. Am J Physiol I 980;238:F347-52.
51. Yandongrn R, Pearl WS, &iyd QW. Adrcnergic stm1ulat1on of rc111n ~ecrction 111 the isolntcd perfused rat kidney. C,rc Res 1973;32: 190-6.
52. L.mgaard 0. I lolJ,ms H, Eide I, Kill F. Conditions for humoral alph,1-adrcnocepror stimularnm of rcnin release 111 anacsthct izcd dogs. Scam! J Cl111 Lah lnvc,t 1981;41:527-34.
5 3. K1>pp U, Bradley T, Hjcmdahl P. Renal venous outflow and urinary excretion of norepincphrmc, epincphnne and dopamme during graded renal nerve stimulation. Am J Physiol I 983;244:E52-60.
54. Ring-Larsen H, llenribcn JII , Chmtcnscn NJ. Prerenal failure. N Engl J MeJ 1989; 320: 397 -8.
5 3. Bernard, M, Santini C, Trev1sa111 F. Renal function impairment mducl'd by change 111 po:,ture in patients with cirrhosis and a~ircs. Gut 1985;26:629- 35.
56. Rmg-Larscn H. Hepatic nephropathy, rehucd ro hacmcxlynam,c:,. Liver I 983;3:265-89.
57. Finke R, Grrn,s R, I lackenthall E, Huher J, Kirchhe1m HR. Threshold pres.~ure for the prcssurc-<lepl'ndent renin release m the autoregulating kidney nf conscious dogs. Pflugers Arch 1983;39: 102-10.
58. Len: K, 1 lortnagl 11, Druml W, et al. Beneficial effect of 8-orn1 thmc vasoprcssin on renal function in dccnmpensate<l cirrho:,is. Gut 1989; 30:90-6.
59. Ring-Larsen 11, I lenribcn JI I, Wilken C, C lausen J, Pals 11, Christensen NJ. Diuretic treatment in <lccompensated cirrhosis and congestive heart failure: Effect of posture. Br Med J 1986;292: l 35 t -3.
60. Zambm~ki E, O'!-lagan K, Thomas G, Hora D. Chronic renal denervation prevents sodium rctent1on in cirrhotic mmialllre sw111e. Proceedings of lnternallnnal Mectmg on Liver and Kidney Dbeases, Florence, l 990: 15.
61 Solis-Herruso JA, Duran A, Favela V, er al. Effects of lumbar sympathetic block on kidney function in cirrhot ic
patients w1tl1 hl'p,1mrenal syndrome. JI lcpmol l987;5:167-73.
62. Mor.iii GA, Flor.,, JS, Lcgmilt L, Log,1r AG, Sl..oreck, KL, Blcndi, !.M. Atn.11 namurct1c focrnr (ANF) responsiveness 111 compen,ated and dccompcnsared l 1rrhos1,: fhe role of the symparhcr1e nervous sy,rem (SNS). Hcpmology I 990; I 2:856.
63. Blcndis LM, Sole DP, Campncll P, ct al. The cffccr of pern<mcovcnous ,hunting on c,Hl·cholamim· metabolism in patients with hq1at1l asutcs. Hepawlogy 1987;7: 14 Hl.
64. Epstein M, Berg DF, I lollcnherg NK. Renal fa1lurl' m rhc pat1c111 with cirrhosis The role of active vasoconstr1ct1on. Am J Med 1970;49: I 7 5-98.
65. Schrier RW, Arroyo V, BcrnarJ1 M, Epstein M, I lennl..,cn JI I, Rodc,J. Peripheral nrtcrml vasndd,11 ,nn hypothesis: A proposal for the 111iriat1on of renal sodium and water recent10n 111 cirrh,1s1,. l lepatol1ig) 1988; 5: I I 51-7.
66. Lieberman FL, Denl',1111 EK, Reynold, TB. The rcl.nicmship of plasma volume, portal hypertension, ,1St1u;,, and renal sodium rl'tcnrion 111 c1rrhos1s. T he overflow theory of a,c1tcs formation. Ann NY Acad Su 1970; 170:202-12.
67. Levy M, Allotcy JBK. Temporal relationship between urinary sah rctentmn and altered syscen11c hcmcxlynamics in Jogs with expenmencal c1rrhoS1s. J Lah Cl111 lvkd I 978;92:560-9.
68. Epsrem M. The '<xl1um rctentmn of cirrhosis. A rcapprn1sal. Hcpatology 1986;6: 312-5.
69. Epstem Fl I. UnJcrfilling versu, nverf,lling 111 hcpatK asc1tes. N Engl J Med 1982; 307: 1577 8.
70. Henriksen JI I, Bendtsen F, Svin:1hCn TIA, Stade,1ger C, Rmg-Lirsen 11. Reduced cenrrnl blood volume 111
cirrhosis. G,1srrocntcrol,1gy 1989;97: 1506-1 3.
71. I Wrtnagl 11 , S111gcr EA, Lenz K SuhMancl' r i, markedly increased m plasma of patients w1th hepatic coma. Lmccl I 984;i:480- 3.
72. Thornton JR, De,m 11, Losowsky MS. b asc1tes caLl',ed hy impaired hepatic 111acu vat1on of hlood home cndogenow, op1md peptide:,? G ur 1988;29:1167.
73. Ames RP, Borkowsky AJ, S1ciusk1 AM, Laragh J H. Prolonged infusion- of ,mg10tensin II and norcp111cphrmc anJ hkxxl pressure, electrolyte hah1m;c, and al<lostcrone and cortisol :,cuet1on m normal man and in cirrhosis with ,,srnes. J C l111 Invest 1965;44: 117-24.
74. Bendt,cn F, Shifter S, I lenrikscn JH lncrca,ed c1rculatmg calciwnin
CANJ GASTROENTEROL VOL 5 No~ MAY/jUNE 1991

gene- re lated peptide (CGRP) in cirrhosis. J Hepatol 1991 ; 12: 11 8-2 3.
75. Vall ance P, Moncada S. Hyperdynamic circulat ion in c irrhosis: A role for nitric oxide? Lancet 199 1 ;337:776-8.
76. Murray BM, Paller MS. Decreased pressor reactivity ro :m giotensin II in cirrhosis in c irrhotic rats. Evidence for a post-receptor defect in angiotensin action . C irc Res I 985;57:424-31.
)7. Bomzom A, Blendis LM . Vascular react ivity in experienced portal hypertension. Am J Physio l 1987;252:G 158-62.
78. Mashford ML, Makow WA, C halmers TC. Studies of the ca rdiovascular system in the hypmension of liver fa ilure. N Engl J Med 1962;267: 107 1-6.
79. Lenz K, Hiirtnagl 1-1, Magometschnigg D, Kleinberger G, Druml W, Lagger A. Function of the ,1uronomic nervous system in patients with hepatic encephalopathy. Hcpatology 1985;5:83 1-6.
80. Gerbes AL, Remien l, Jungst D, Sauerhruch T, Paumgartner G. Evidence for a down regulation o(
heta-2 -adrenoceprors m cirrhot ic patients with severe ascices. Lancet I 986;i: 109- 10.
81. Ramond MJ , Comoy E, Lebrec D. Alternations in isoprenaline sensitiv ity in patients with cirrhosis: Evidence of abnormality of the sympathetic nervous activity. Br J Pharmacol 1986;2 I : 19 1-6.
82. Lee S, Marty J, Mantz J, Samain E, Brai llon A, Lebrec 0. Desensitization of myocardial bern-adrenergic receptors in c irrhotic rats. I Iepatology 1990;12:48 1-5.
83. Novak DJ, Victor M. The vagus and aympathetic nerves in alcoholic po lyneuro pathy. Arch Neuml l 974;30:273-8.
84. Eiscnhofer G , Whiteside EA, Johnson RH. Plasma catecholamine respon~es to change of posture in alcoholics during withdrawal and after continued absti nence from alcohol. C lin Sci 1985;64:7 l -8.
85. MacGilchrist AJ , Reid JL. Impai rment of autonomic reflexes in cirrhosis. J Gastrocnterol I 990;85:288-92.
86. Henriksen JI-I , Ring-Larsen H,
CAN J GASTROENTEROL VOL 5 NO 3 MA Y/JUNI:. 199 1
Noradrenaline and ascites formation
C hrbtcn en NJ. Sympathetic nervous ;icriv ity in cirrhosb. A survey of plasma catecholammc stud ies. J I leparol 1985; I :55-65.
87. Henriksen JI I, Ring-Larsen 11, C hristern,cn NJ. Autonomic nervou;, function in liver d isease. In: Blendis LM , Romzom A, eds. Cardiovascular Complication of Liver Oise;ise. Boca Raton: C RC Press Inc, 1990:63-79.
88. Henriben JH, Ring-Larsen 11, C hristensen NJ. Aspects of symp;1thetic ncrvou, system regul,ttion in patients wnh c1rrhos1s. A I 0-years experience. C lin Physiol. ( In press)
89. Llach J, G ines P, Arroyo V, Tito L, Badalamenti A, Jimenez W. Prognostic value of arreri;il pressure endogenous vasoactive systems, and rem1l function in c irrhosis with ascires. Gastroenrerology I 988;94:482-7.
90. Tagc-Jensen U, Henriksen JI I, Christensen E, Widding A, Ring-Larsen H, C hristensen NJ. Plasma catecholamine level and portal venous pressure as guides ro prognosis in p,1tienrs with cirrhosis. J Hepaml ! 988;6:350-8.
11 1

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com