Sx Polipos Hamartomatosos

If you can't read please download the document
-
Upload
boris-ariel-hernandez-briones -
Category
Documents
-
view
20 -
download
1
Transcript of Sx Polipos Hamartomatosos
reviewwww.nature.com/clinicalpractice/gasthep
Hamartomatous polyposis syndromesKevin M Zbuk and Charis Eng*
S U M M A RYThe hamartomatous polyposis syndromes are a heterogeneous group of disorders that share an autosomal-dominant pattern of inheritance and are characterized by hamartomatous polyps of the gastrointestinal tract. These syndromes include juvenile polyposis syndrome, PeutzJeghers syndrome and the PTEN hamartoma tumor syndrome. The frequency and location of the polyps vary considerably among syndromes, as does the affected patients predisposition to the development of gastrointestinal and other malignancies. Although the syndromes are uncommon, it is important for the clinician to recognize these disorders because they are associated with considerable morbidity and mortality, not only from malignancy but also from nonmalignant manifestations such as bleeding, intussusception, and bowel obstruction. Each hamartomatous polyposis syndrome has its own distinctive organ-specific manifestations and each requires a different surveillance strategy, which makes accurate diagnosis crucial for appropriate patient management. The availability of clinical genetic testing for these disorders means that appropriate recognition allows for timely referral for cancer genetic counseling, and often allows for predicative testing in at-risk family members. Promisingly, an understanding of the molecular pathogenesis of these disorders offers insights into the mechanisms underlying the development of sporadic malignancy, and enables rational selection of targeted therapies that warrant further investigation.Keywords cancer, hamartomatous polyposis syndromes, inherited
Continuing Medical Education online Medscape, LLC is pleased to provide online continuing medical education (CME) for this journal article, allowing clinicians the opportunity to earn CME credit. Medscape, LLC is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide CME for physicians. Medscape, LLC designates this educational activity for a maximum of 1.0 AMA PRA Category 1 CreditsTM. Physicians should only claim credit commensurate with the extent of their participation in the activity. All other clinicians completing this activity will be issued a certificate of participation. To receive credit, please go to http://www.medscape.com/cme/ncp and complete the post-test. Learning objectives Upon completion of this activity, participants should be able to: 1 Identify the different autosomal dominant types of hamartomatous polyposis syndromes. 2 Describe the risk for cancer associated with juvenile polyposis syndrome. 3 List clinical features of and cancer risks associated with PeutzJeghers syndrome. 4 List the types of cancers that Cowdens syndrome predisposes to. 5 Describe surveillance strategies recommended for the hamartomatous polyposis syndrome PTEN hamartoma tumor syndrome.
Review criteria This Review is based on a PubMed search performed in January 2007 with the following terms alone or in combination: hamartomatous polyps, hamartomas, juvenile polyposis syndrome, juvenile polyps, PeutzJeghers syndrome, Cowden syndrome, BannayanRileyRuvalcaba syndrome, BRRS, PTEN hamartoma tumor syndrome, small bowel polyps, PTEN, BMPR1A, LKB1, SMAD4, germline, mTOR inhibitors, rapamcyin. Full-length, original research and review articles published in English were used.
INTRODUCTION
cmeKM Zbuk is a Cancer Genomic Medicine Fellow and Crile Fellow at the Genomic Medicine Institute, Cleveland Clinic and C Eng is Chair and Director of the Genomic Medicine Institute and Director of the Center for Personalized Genetic Healthcare, Cleveland Clinic and Professor and Vice Chairman, Department of Genetics, Case Western Reserve University School of Medicine, Cleveland, OH, USA.Correspondence*Cleveland Clinic Genomic Medicine Institute, 9500 Euclid Avenue, NE-50, Cleveland, OH 44195, USA [email protected] 22 February 2007 Accepted 14 June 2007www.nature.com/clinicalpractice doi:10.1038/ncpgasthep0902
The hereditary gastrointestinal polyposis syn dromes can be broadly divided into those in which the polyps are predominantly adenomatous and those in which the polyps are predominantly hamartomatous. Hamartomatous polyps are composed of the normal cellular elements of the gastrointestinal tract, but have a markedly distorted architecture. The hamartomatous poly posis syndromes are a heterogeneous group of disorders that are inherited in an autosomaldominant manner. The syndromes include juvenile polyposis syndrome (JPS), PeutzJeghers syndrome (PJS), and PTEN hamartoma tumor syndrome (PHTS). PHTS includes Cowden syn drome, BannayanRileyRuvalcaba syndrome (BRRS), and all syndromes in which there are germline PTEN mutations. The hamartomatous polyposis syndromes are uncommontogether, they account for fewerseptember 2007 vol 4 no 9
492 nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
than 1% of colon cancer cases in North America.1 Nonetheless, it is important that these syndromes are recognized and managed appropriately for several reasons. First, most of these syndromes are associated with a markedly increased risk for the development of colon cancer. Second, they are associated with the development of extra-colonic manifestations, both malignant and nonmalig nant, which often result in considerable morbidity and mortality. Insights into the molecular patho genesis of malignancy in these rare disorders have advanced our knowledge of the pathogenesis of their sporadic counterparts. This advancement is illustrated by the evolution of the concept of the hamartoma to carcinoma sequence,2 which is an alternative sequence to the adenoma to carcinoma paradigm of colorectal cancer pathogenesis. Although the field of hamartomatous polyposis is broad, in this Review we discuss the diagnosis and clinical features of the different hamartoma tous polyposis syndromes, the risk of malignancy associated with each syndrome, appropriate surveillance recommendations, and what is known about the genetics of these syndromes. Other disorders that are associated with the presence of hamartomatous polyps are briefly discussed, and the Review additionally summa rizes the potential for targeted therapy of hamarto matous polyposis syndromes and the malignant potential of hamartomatous polyps.PEUTZJEGHERS SYNDROME Diagnosis and clinical features
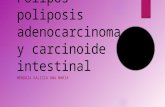
seen on the vermillion border of the lips, the buccal mucosa, and the hands and feet.4 Perinasal, perianal, genital, and periorbital pigmentation can also be observed, but this pigmentation often fades after puberty. In contrast to the lentigines seen in individuals with PJS, common freckles spare the buccal mucosa, and are usually rare around the lips and nose. The diagnostic criteria for PJS include the pres ence of characteristic mucocutaneous pigmenta tion, the presence of small-bowel hamartomatous polyps and a family history of PJS. Patients need to fulfill two of these three criteria for a clinical diagnosis of PJS to be made.7 On endoscopy, the polyps seen in patients with PJS have no defining features, although they can develop long stalks that predispose the intestine to intussusception.5 Microscopically, extensive smooth-muscle proliferation, with an elongated, arborized pattern of polyp forma tion, can be seen (Figure 1).8 This characteristic microscopic appearance of PJS polyps enables experienced gastrointestinal pathologists to confirm the clinical diagnosis.Cancer risk
PJS, which has an incidence of 1 in 150,000 in North America and Western Europe,3 is charac terized by the presence of hamartomatous polyps in the gastrointestinal tract, and is associated with a distinctive mucocutaneous pigmentation. Polyps occur most commonly in the small intes tine (64%), although involvement of the colon (53%), stomach (49%), and rectum (32%) is also seen.4 Polyps have also been found in the upper and lower respiratory tract and bladder.5 There are usually fewer than 20 polyps present in each case, and the polyps vary in size from several millimeters to more than 5cm in diameter.6 Patients usually present with PJS in the second or third decade of life, and the presenting symp toms include abdominal pain, rectal bleeding, anemia, small intestinal intussusception, bowel obstruction, and rectal prolapse of polyps.5 The characteristic pigmentation, which is usually dark blue to dark brown in color, is present in 95% of patients with PJS and is most commonlyseptember 2007 vol 4 no 9 ZBUK AND ENG
PJS is associated with a markedly increased risk of malignancy that is not confined to the gastro intestinal tract. A meta-analysis found that, compared with the general population, patients with PJS have a relative risk (RR) of greater than 15 for developing any type of cancer.9 According to this meta-analysis, the cumulative risk of developing any type of cancer was 93% by the time a PJS patient was 65years old. Very high RRs for the development of cancer were observed for the small intestine (520), stomach (213), pancreas (132), colon (84), and esophagus (57), with RRs of greater than 10 for the development of breast, lung and ovarian cancer. A follow-up study restricted to patients with PJS who had a germline mutation in the tumor suppressor gene STK11 (also known as LKB1) confirmed that these patients have a very high risk of developing cancer.10 The cumulative risk of developing any type of cancer was 81% by the time these patients were 70years of age, the cumulative risk of developing any gastro intestinal cancer (including small intestine, colorectal, esophageal and pancreatic cancer) was 66% by the time they were 70years of age, and for female patients the cumulative risk of developing breast cancer was 32% by the time they were 60years of age.10nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 493
2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
by advances in capsule and double-balloon endo scopy. Although the precise role of these tech niques in the management of patients with PJS has not yet been established, they will undoubt edly prove useful in the nonsurgical treatment of patients with polyps of the small intestine,13 and might replace surveillance performed by small-bowel barium follow-through.Genetics
mm
Figure 1 A typical PeutzJeghers syndrome polyp demonstrating the arborizing pattern of smoothmuscle proliferation. Abbreviation: mm, muscularis mucosa. Permission obtained from Macmillan Publishers Ltd Bronner (2003)79 Modern Pathology 16: 359365.
PJS also predisposes females to development of cervical adenoma malignum, a rare and very aggressive adenocarcinoma of the cervix.11 In addition, females with PJS commonly develop benign ovarian sex-cord tumors with annular tubules, whereas males with PJS are predisposed to development of Sertoli-cell testicular tumors;12 although neither of these two tumor types is malignant, they can cause symptoms related to increased estrogen production.Surveillance recommendations
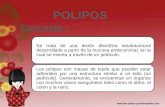
Germline mutations of STK11 are documented in up to 7080% of patients with PJS; up to 15% of cases have germline deletions of all or part of STK11.14 Although the classic clinical and histopathologic features of PJS might sometimes obviate the need for genetic testing, analysis of germline STK11 mutations can be helpful when the clinical features are subtle or when the histo logical diagnosis is in question.15 STK11 encodes a serinethreonine kinase that modulates cellular proliferation, controls cell polarity, and seems to have an important role in responding to low cellular energy levels.16 In the performance of this last role, the STK11 protein is involved in the inhi bition of AMP-activated protein kinase (AMPK), and signals downstream to inhibit the mTOR (mammalian target of rapamycin; also known as FRAP; FKBP12-rapamycin complex-associated protein) pathway;17 the mTOR pathway is dysreg ulated in patients with PJS and in patients with PHTS (Figure 3). Genotypephenotype correlation suggests that patients with PJS who have mutations in STK11 that result in truncation of the encoded STK11 protein have a significantly earlier age of onset than those who have a missense mutation or no detectable mutation of STK11.18 Interestingly, heterozygous Stk11 knockout mice develop hamartomatous polyps in the stomach and small intestine, but the predominant malignancy they develop is hepatocellular carcinoma, which is not a malignancy characteristic of human PJS.19PTEN HAMARTOMA TUMOR SYNDROME Diagnosis and clinical features
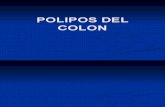
Surveillance recommendations for the hamarto matous polyposis syndromes are based on expert opinion, but no randomized trials have evaluated the efficacy of surveillance for the management of these disorders. The surveillance recommenda tions for patients with PJS are complex, and focus on the increased risk of gastrointestinal, gyneco logic, breast, and testicular neoplasms. A strategy proposed in 2006 by Giardiello and Trimbath is illustrated in Figure 2.8 Surveillance and management of polyposis of the small intestine has been markedly improved
The term PHTS was developed to unify the hetero geneous group of disorders that are all caused by germline mutations of the tumor suppressor gene PTEN.20 PHTS encompasses the disorders Cowden syndrome, BRRS, and Proteus syndrome. Several other disorders have also been associated with germline PTEN mutations, but a detailed discus sion of this group of disorders is beyond the scope of this Review, and the prevalence of polyposis in many of these disorders is unknown.ZBUK AND ENG september 2007 vol 4 no 9
ncpgasthep_2007_042f1.eps494 nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
Both sexes
Gastrointestinal polyps/malignancies UGI endoscopy and small-bowel series every 23 years Colonoscopy every 23 years EUS pancreas +/ CT scan/ CA199 every 12 years
Females
Breast cancer Monthly breast self-examination Annual mammogram and breast MRI and semi-annual clinical examination Benign and malignant ovarian neoplasia Annual TVUS and CA125 Benign ovarian neoplasia Annual Hx and Px AdenoCA cervix and ovarian neoplasia Pelvic examination and Pap smear
Males
Sertoli tumor testes Annual Hx and Px Consider US testes every 2 years
Birth
8 years
12 years
18 years
21 years
25 years
Figure 2 The suggested age-range-specific surveillance recommendations for patients with PeutzJeghers syndrome. Abbreviations: EUS, endoscopic ultrasound; Hx, history; Pap smear, Papanicolaou smear; Px, physical examination; TVUS, transvaginal ultrasound; UGI, upper gastrointestinal; US, ultrasound. Adapted from data presented in Reference 8.
Cowden syndrome is an uncommon, underrecognized disorder with an estimated incidence of 1 per 200,000 of the population, at least in Europe and North America;21 the syndrome confers an increased risk of breast, thyroid, and endometrial cancer. Other features of the disorder include the following: macrocephaly; gastrointestinal polyps; benign breast, thyroid, and endometrial manifestations; and character istic mucocutaneous lesions (Table 1). Many of the benign manifestations are hamartomatous in nature, and Cowden syndrome has previously been referred to as the multiple hamartoma syndrome. Operational diagnostic criteria for Cowden syndrome are updated annually by the National Comprehensive Cancer Network.22 BRRS is characterized by the presence of multiple lipomas, gastrointestinal hamartoma tous polyps, macrocephaly, hemangiomas, developmental delay and, in males, pigmented macules on the glans penis.23 Formal diagnostic criteria have not been established. Proteus syndrome is a complex multisystem disorder that is characterized by congenital
malformations, hemihypertrophy, hamartomatous overgrowths, epidermal nevi and hyperostosis.24 Historically, it was felt that gastrointestinal polyps were more commonly seen in patients with BRRS than in patients with Cowden syndrome, as these polyps are present in approximately 50% of patients with BRRS.23 It is possible, however, that asymptomatic polyps are at least as common in patients with Cowden syndrome. Series have suggested that diminu tive colonic polyps, mostly present distal to the hepatic flexure, occur in 6090% of patients with Cowden syndrome.2527 One small study of patients with this syndrome, which has been presented in abstract form only, reported that such polyps have a markedly varied histology, with adenomatous, juvenile, hyperplastic, lipomatous, and ganglioneuromatous polyps all being described.26 Whether such varied polyp pathology is common in patients with Cowden syndrome is, however, questioned by some in he field. Another manifestation of Cowden syndrome is glycogenic acanthosis. This manifestation isnature clinical practice GASTROENTEROLOGY & HEPATOLOGY 495
ncpgasthep_2007_042f2.epsseptember 2007 vol 4 no 9 ZBUK AND ENG 2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
P13K TSC1 TSC2 Rapamycin CCI-779
PIP2
PIP3
AKT
PTEN STK11 AMPK mTOR
Protein synthesis
Angiogenesis
Figure 3 Signaling pathways dysregulated in patients with PeutzJeghers syndrome or PTEN hamartoma tumor syndrome. PTEN and STK11 both downregulate the mTOR pathway, a growth promoting pathway, which when dysregulated contributes to the pathogenesis of PJS and PHTS. Both PTEN and STK11 act indirectly on mTOR through modulation of the TSC1TSC2 complex upstream of mTOR. By contrast, the mTOR inhibitors, which include rapamycin and CCI-779, inhibit mTOR directly, downstream of both PTEN and STK11, making them potentially useful agents for the treatment of both PJS and PHTS. Abbreviations: AKT, protein kinase B; AMPK, AMP-activated protein kinase; mTOR, mammalian target of rapamycin (also known as FRAP; FKBP12rapamycin complex-associated protein); PI3K, phosphoinositide-3 kinase; PIP2, phosphoinositol 4,5-bisphosphate; PIP3, phosphoinositol 3,4,5-trisphosphate; PHTS, PTEN hamartoma tumor syndrome; PJS, PeutzJegher syndrome; PTEN, phosphatase and tensin homolog, deleted on chromosome TEN; STK11, serine threonine protein kinase 11 (also known as LKB1); TSC1, tuberous sclerosis 1 protein; TSC2, tuberous sclerosis 2 protein.
One study sought to classify patients with gastrointestinal polyposis syndromes on the basis of the germline mutation status of several genes known to confer predisposition to gastro intestinal polyps.15 All the patients studied had more than five colorectal polyps in their life time, one of which was either hamartomatous or hyperplastic. Germline PTEN mutations were identified in 2 of the 23 patients (9%) who had a combination of hyperplastic and adenomatous polyps. These two patients had features remini scent of Cowden syndrome, but did not meet diagnostic criteria.Cancer risk
Table 1 Common manifestations of Cowden syndrome.29Feature Mucocutaneous manifestations Trichilemmomas Papillomatous papules Acral keratosis Breast lesions Fibrocystic breast disease Adenocarcinoma Macrocephaly Thyroid abnormalities Multinodular goiter Adenomas Thyroid carcinoma (usually follicular) Gastrointestinal lesions Hamartomatous polyps Esophageal glycogenic acanthosis Genitourinary abnormalities Multiple uterine leiomyomas (fibroids) and/or bicornuate uterus Percentage of patients affected 99%
76% of affected females 3050% of affected females 3040% 5067% 310%
Among the different PHTS disorders, cancer risk has been clearly documented only in patients with Cowden syndrome. In female patients the syndrome is associated with up to a 50% life time risk of developing breast cancer25 and a 510% risk of developing endometrial cancer.29 The risk of developing breast cancer might also be increased for male patients with the syndrome,30 and all patients with the syndrome have a 10% lifetime risk of developing follicular thyroid cancer.25 The risk of colon cancer associated with Cowden syndrome is not well characterized. One case report described a patient with Cowden syndrome who had a PTEN mutation and meta chronous colon carcinomas, both of which appeared to arise from within hamartomatous polyps.31 In addition, the authors reported the presence of a somatic mutation (i.e. the second hit according to the two-hit hypothesis of cancer development) in PTEN within the carcinoma. In a large cohort of patients with PTEN mutations, a modestly increased RR for the development of colon cancer has been noted (Pilarski R and Eng C, unpublished data); however, further research is necessary to confirm this association.Surveillance recommendations
30% 44% of affected females
recognized as elevated gray-white plaques in the distal mucosa of the esophagus that, on histological examination, demonstrate epithe lial thickening associated with the prolifera tion of large glycogen-filled squamous cells.28
Current clinical opinion is that, irrespective of their phenotype, all patients who have germline PTEN mutations should be monitored by use of the surveillance recommendations established for Cowden syndrome.29 At present, the National Comprehensive Cancer Network guidelines for Cowden syndrome make no specific recommen dations for gastrointestinal system screening (Table 2), but rather focus largely on the increased risk of breast, thyroid and endometrial cancer.22 Nevertheless, these guidelines are updated annu ally, and will incorporate screening for colorectalZBUK AND ENG september 2007 vol 4 no 9
ncpgasthep_2007_042f3.eps496 nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
Table 2 We do not have permission to reproduce this table on the website. Please refer to the print issue of the journal. To view the most recent and complete version of these surveillance recommendations, go online to www.nccn.org.
cancer if ongoing research confirms that patients with Cowden syndrome are at an increased risk of colon cancer.Genetics
Germline PTEN mutations are found in 85% of patients with Cowden syndrome and in more than 60% of patients with BRRS.20,32,33 Mutations have been detected in the promoter region of PTEN in patients with Cowden syndrome, whereas deletions of all or part of PTEN (not normally detectable by conven tional polymerase chain reaction) have been documented in patients with BRRS.34 The PTEN protein is a ubiquitously expressed, dualspecificity phosphatase that has both lipid and protein phosphatase activity. The lipid phos phatase activity of PTEN is best characterized; its major substrate is phosphoinositol triphosphate. By regulating the levels of phosphoinositol triphosphate, PTEN acts as a negative regulator of the AKT pathway.35 As a tumor suppressor, PTEN has a crucial role in the control of cell growth, proliferation and angiogenesis (reviewed by Waite and Eng36), and somatic PTEN mutations are prevalent in various malignancies.37september 2007 vol 4 no 9 ZBUK AND ENG
Mouse models often provide helpful comple mentary insights into the human disease; however, although mouse models of Pten deficiency are available their usefulness in helping to dissect the pathogenesis of human PHTS and/or Cowden syndrome is limited. Heterozygous Pten+/ mice develop hamartomatous polyps of the gastro intestinal tract, but the spectrum of neoplasia and malignancies observed bears little resemblance to that seen with Cowden syndrome; mice often develop thymic and peripheral lymphomas and prostate cancer at a young age.35,38JUVENILE POLYPOSIS SYNDROME Diagnosis and clinical features
JPS is characterized by the presence of multiple juvenile polyps. These polyps are named for their histological appearance and can occur at any age. The presence of isolated juvenile polyps in the colorectum is relatively common; up to 2% of chil dren who are under 10years of age have an isolated juvenile polyp.39,40 The diagnosis of JPS, therefore, requires the presence of more than three to five juvenile polyps in the colorectum, or the presence of juvenile polyps throughout the gastrointestinal tract, or the presence of any number of juvenilenature clinical practice GASTROENTEROLOGY & HEPATOLOGY 497
2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
cancer might be as high as 4050%;43 a study by Brosens et al. demonstrated that, compared with the general population, patients with JPS have a RR for colon cancer of 34, with a mean age at diagnosis of 43years.48 There are probably also increased risks of gastric cancer, carcinoma of the small intestine and possibly pancreatic cancer associated with JPS, although there were no upper gastrointestinal malignancies detected in the cohort described by Brosens et al.43,48Figure 4 A typical juvenile polyp demonstrating gland dilatation, inflammatory cell infiltrate and absence of smooth-muscle proliferation. Permission obtained from Macmillan Publishers Ltd Bronner (2003)79 Modern Pathology 16: 359365.
Surveillance recommendations
polyps in an individual who has a family history of juvenile polyposis syndrome.41,42 The appearance of the polyps associated with JPS can be indistin guishable from that of those seen in other hamarto matous polyposis syndromes (especially those in Cowden syndrome), and the features of these syndromes should, therefore, be carefully sought when evaluating a patient with suspected JPS. On endoscopy, the characteristic juvenile polyp is spherical in shape, often pedunculated, and has a smooth and often shiny appearance.1 Juvenile polyps can reach several centimeters in diameter. At the microscopic level, these polyps appear as mucous-filled, dilated glands that are often associ ated with inflammatory cell infiltration (Figure 4).41 Unlike the PJS polyp there is no smooth-muscle proliferation. Most juvenile polyps occur in the colon and rectum; the frequency of polyps in the stomach and small intestine is less than 20%,43 although individuals who have SMAD4 muta tions (see below) have a much higher frequency of upper gastrointestinal polyps than this.44,45 Tens to hundreds of polyps are often present in affected individuals, and a diagnosis of JPS is usually made before a patient reaches 20years of age.46 Common presenting symptoms include rectal bleeding, anemia, abdominal pain, obstruction, and less commonly rectal prolapse of polyps.47Cancer risk
There are several surveillance recommenda tions for individuals affected with JPS.43,49 First, affected individuals should be monitored for rectal bleeding, anemia, abdominal pain, constipation, diarrhea, or change in stool size, shape, and/or color; these symptoms might warrant additional investigation including endoscopy. Second, CBC, colonoscopy, and upper endoscopy should begin by the time the affected individual is 15years of age. Third, if screening results are negative, screening should be repeated in 3years time. Fourth, if only a few polyps are identified, they should be removed; screening should then be performed annually until no additional polyps are found, at which time screening every 3years can resume. Fifth, if the polyp burden or dysplastic changes necessitate colectomy, or gastrectomy/small-bowel resection, subsequent screening should be performed annu ally until no additional polyps are found, at which time screening every 3years can resume. Importantly, there have been families with SMAD4 mutations described (see below) that have family members with both JPS and heredi tary hemorrhagic telangectasia.50 This situation indicates the need to screen patients with SMAD4 mutations for occult vascular malformations; however, a discussion of the details of this is beyond the scope of this Review.Genetics
The predisposition to the development of malig nancy conferred by JPS seems to be confined to malignancies of the gastrointestinal system. Colorectal cancer is by far the most common malignancy that develops, and the lifetime risk of an individual with JPS developing this form of498 nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 2007 Nature Publishing Group
Germline mutations of SMAD4, BMPR1A, and ENG have all been described in patients with JPS, and all three genes encode proteins that are involved in the transforming growth factor (TGF-) signaling pathway.15 The TGF- sign aling pathway is an important modulator of many cellular processes, including proliferation, differ entiation and adhesion (reviewed by Waite and Eng51), and TGF- itself has a major role in the control of colonic epithelial growth.52 The importance of the TGF- pathway in colon cancer development is illustrated by theZBUK AND ENG september 2007 vol 4 no 9
reviewwww.nature.com/clinicalpractice/gasthep
finding that somatic mutations of the TGF- receptor II are present in most colorectal cancers from patients with Lynch syndrome, and are also common in sporadic colorectal cancers that exhibit microsatellite instability. In addition, somatic mutations in the part of the gene that encodes the kinase domain of TGF- receptor II are seen in approximately 15% of sporadic microsatellite stable colorectal cancers.53 Somatic mutations of other members of the TGF- signaling pathway, including SMAD2 and SMAD4, are found in sporadic colon cancers; SMAD4 mutations are more commonly found in advanced malignancy or metastasis. Although such mutations occur only in approximately 15% of sporadic colorectal cancers, loss of heterozygosity at 18q, the region containing both of the SMAD2 and SMAD4 loci, is found in up to 70% of adenocarcinomas and in at least 10% of early adenomas.54 It is possible, but yet to be confirmed, that such mutations occur at increased frequency in patients with JPS, representing a somatic second hit within the TGF- pathway. The prevalences of germline mutations of BMPR1A and SMAD4 are 20% each in patients with JPS.55 The prevalence of germline ENG mutations is currently unknown, but germ line ENG mutations seem to predispose to the development of JPS in early childhood.15 One additional study has documented missense varia tion in ENG in patients with JPS who are younger than 10years of age, but it is not clear whether these variants are pathogenic.56 In addition, several cases of JPS of infancy, characterized by generalized polyposis and often diagnosed in the first 2years of life, have been associated with germline deletions that encom pass both PTEN and BMPR1A.15,5759 These patients clinical features often overlap with those seen in patients with Cowden syndrome and BRRS. These patients usually present with a fulminant disease course characterized by intus susception, rectal bleeding, and protein-losing enteropathy, which is often fatal early in life. The similarity of the polyps associated with JPS and Cowden syndrome initially led to speculation that PTEN mutations might cause some cases of JPS. It is now realized however, that these cases were in fact Cowden syndrome cases that were not recognized as such.60,61 Genotypephenotype correlation analyses have demonstrated that patients who have SMAD4 mutations are more likely to develop massive upper gastrointestinal polyps and haveseptember 2007 vol 4 no 9 ZBUK AND ENG
a family history of upper gastrointestinal poly posis than are those patients who have BMPR1A mutations.44,45 The Smad4+/ mouse exhibits a phenotype that is similar to that of human JPS; this mouse develops multiple gastric and small intestinal polyps that are very similar histo logically to juvenile polyps, although no polyps are seen in the colon.62 Moreover, areas of adeno carcinoma are also seen in the stomach and small intestine. Heterozygous Bmpr1a knockout mice appear grossly normal,63 while the Eng+/ hetero zygous knockout mouse exhibits features of hereditary hemorrhagic telangiectasia, but does not develop overt gastrointestinal polyps.64 It is not clear from the literature, however, how carefully either of these mice models was exam ined for evidence of polyposis, as their generation preceded by several years the recognition of ENG and BMPR1A mutations as causes of JPS.OTHER DISORDERS
Several other disorders are associated with hamartomatous polyps of the gastrointestinal tract. A detailed discussion of these disorders is not possible in this Review, but they are mentioned briefly. Multiple endocrine neoplasia type 2B is characterized by medullary thyroid cancer, pheo chromocytoma, marfinoid habitus, and multiple ganglioneuromas. The ganglioneuromas affect the gastrointestinal tract in approximately 40% of affected patients65 and can lead to constipation, diarrhea, abdominal pain and bowel obstruction. Similarly, in patients with neurofibro matosis type 1, neurofibromas can involve the gastrointestinal tract, and sometimes lead to gastrointestinal bleeding and/or abdominal pain.66 The basal cell nevus syndrome (Gorlin syndrome), which is characterized by multiple cutaneous basal cell carcinomas, has been associ ated with multiple gastric hamartomatous polyps,67 but many affected families have no gastrointestinal manifestations. Finally, hereditary mixed polyposis is charac terized by polyps of mixed histological types, which include atypical juvenile polyps, hyper plastic polyps, sessile serrated adenomas, adeno matous polyps. Hereditary mixed polyposis also confers a predisposition to colorectal carci noma.68 Evidence has suggested that in some families the CRAC1 locus is involved,69 but we suspect that this syndrome is heterogeneous, as supported by a report of BMPR1A mutations occurring in a family with this disorder.49nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 499
2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
TARGETED THERAPEUTICS
The potential of targeted therapies for the treat ment of hamartomatous polyposis syndromes deserves discussion given the relatively robust molecular characterization of these disorders. The most promising agents at this point in time are those that modulate the mTOR pathway, a target directly relevant to PHTS as well as to PJS (Figure 3). The mTOR inhibitor rapamycin has demon strated efficacy for the treatment of neoplastic manifestations of the hamartomatous condi tion tuberous sclerosis.70 This condition results from germline mutations of TSC1 or TSC2, and the proteins encoded by these genes also down regulate the mTOR pathway.70 Rapamycin and the related drug CCI-779 have been successfully used as prophylactic treatment for transplant rejection, and have been studied extensively in early trials to investigate the treatment of various malignancies.71 The drugs have proven reason ably safe and well tolerated, especially when used as monotherapy.71 There have, however, been no published trials on the use of mTOR inhibitors in hamartomatous polyposis syndromes. Some preliminary data suggest that cyclo-oxygenase 2 inhibitors might also show promise in the treatment of both JPS and PJS.72,73MALIGNANT POTENTIAL OF HAMARTOMATOUS POLYPS
coincidental. Abnormalities in cell polarity are believed to underlie the predisposition to malig nancy, possibly through the association between altered cell polarity and expansion of the stem cell compartment of the colon.78 Similar debate exists regarding the malignant potential of juvenile polyps in patients with JPS. Further research is necessary to resolve these conflicting hypotheses.CONCLUSIONS
Advances in the understanding of the genetic etiologies of the hamartomatous polyposis syndromes has led to the availability of clinical genetic testing, which has revolutionized the practice of cancer genetics for these disorders, and has important implications for affected individuals and at-risk family members. An important challenge will be to determine the underlying pathomechanisms involved for those affected patients who have no currently identifi able genetic mutation. Such efforts will not only benefit the small number of patients affected by these disorders, but will also serve to increase knowledge of the mechanisms underlying the development of sporadic malignancies.Key points Hamartomatous polyposis syndromes are inherited autosomal-dominant syndromes that confer predisposition to cancers and have divergent clinical features, but often involve interconnected molecular pathways Juvenile polyposis syndrome is caused by germline mutations of SMAD4, BMPR1A and ENG, and it predisposes individuals to colon cancer, and, to a lesser extent, upper gastrointestinal malignancies Cowden syndrome, the most common PTEN hamartoma tumor syndrome, is caused by germline PTEN mutations and is characterized by benign and malignant breast, thyroid and endometrial manifestations, in addition to macrocephaly and characteristic mucocutaneous findings PeutzJeghers syndrome is caused by germline STK11 mutations and is associated with a markedly increased risk of gastrointestinal, breast and gynecologic malignancies Timely diagnosis of hamartomatous polyposis syndromes allows for appropriate surveillance and management, which varies considerably between syndromes Clinical testing for germline mutations should occur in the setting of appropriate genetic counseling and offer predictive testing for family members
The malignant potential of hamartomatous polyps is not known and is an important and unresolved issue. For JPS and Cowden syndrome there has been documentation of patients who have both adenomatous and hamartomatous polyps, and malignant transformation might be occurring within adenomatous polyps in this situation.15 An alternative hypothesis is that hamartomatous polyps might undergo adenoma tous followed by carcinomatous transformation, or possibly transform directly from hamartomas to carcinomas.2,74,75 In patients with PJS, PHTS, or JPS hamarto matous polyps have been detected that contain areas of adenoma and/or carcinoma.2,31,75,76 Hamartomatous polyps have traditionally been viewed as nonmalignant, and in the case of PJS it has been argued that germline STK11 muta tions lead to altered cell polarity, which results in mucosal prolapse.77 In this model, the hamarto matous polyp develops as an epiphenomenon and is nonneoplastic; the occurrence of cancer or adenomas within a hamartomatous polyp is500 nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 2007 Nature Publishing Group
ZBUK AND ENG september 2007 vol 4 no 9
reviewwww.nature.com/clinicalpractice/gasthep
References 1 Nagy R et al. (2004) Highly penetrant hereditary cancer syndromes. Oncogene 23: 64456470 2 Wang ZJ et al. (1999) Allelic imbalance at the LKB1 (STK11) locus in tumours from patients with Peutz Jeghers syndrome provides evidence for a hamartoma(adenoma)-carcinoma sequence. J Pathol 188: 913 3 Kutscher AH et al. (1960) Incidence of PeutzJeghers syndrome. Am J Dig Dis 5: 576577 4 Utsunomiya J et al. (1975) PeutzJeghers syndrome: its natural course and management. Johns Hopkins Med J 136: 7182 5 McGarrity TJ and Amos C (2006) PeutzJeghers syndrome: clinicopathology and molecular alterations. Cell Mol Life Sci 63: 21352144 6 Giardiello FM and Trimbath JD (2006) PeutzJeghers syndrome and management recommendations. Clin Gastroenterol Hepatol 4: 408415 7 Giardiello FM et al. (1987) Increased risk of cancer in the PeutzJeghers syndrome. N Engl J Med 316: 15111514 8 Estrada R and Spjut HJ (1983) Hamartomatous polyps in PeutzJeghers syndrome. A light-, histochemical, and electron-microscopic study. Am J Surg Pathol 7: 747754 9 Giardiello FM et al. (2000) Very high risk of cancer in familial PeutzJeghers syndrome. Gastroenterology 119: 14471453 10 Lim W et al. (2004) Relative frequency and morphology of cancers in STK11 mutation carriers. Gastroenterology 126: 17881794 11 Srivatsa PJ et al. (1994) Disseminated cervical adenoma malignum and bilateral ovarian sex cord tumors with annular tubules associated with Peutz Jeghers syndrome. Gynecol Oncol 53: 256264 12 Scully RE et al. (1970) Sex cord tumor with annular tubules a distinctive ovarian tumor of the Peutz Jeghers syndrome. Cancer 25: 11071121 13 Terauchi S et al. (2006) Double-balloon endoscopy and PeutzJeghers syndrome: a new look at an old disease. Proc (Bayl Univ Med Cent) 19: 335337 14 Volikos E et al. (2006) LKB1 exonic and whole gene deletions are a common cause of PeutzJeghers syndrome. J Med Genet 43: e18 15 Sweet K et al. (2005) Molecular classification of patients with unexplained hamartomatous and hyperplastic polyposis. JAMA 294: 24652473 16 Alessi DR et al. (2006) LKB1-dependent signaling pathways. Annu Rev Biochem 75: 137163 17 Corradetti MN et al. (2004) Regulation of the TSC pathway by LKB1: evidence of a molecular link between tuberous sclerosis complex and Peutz Jeghers syndrome. Genes Dev 18: 15331538 18 Amos CI et al. (2004) Genotype-phenotype correlations in PeutzJeghers syndrome. J Med Genet 41: 327333 19 Miyoshi H et al. (2002) Gastrointestinal hamartomatous polyposis in Lkb1 heterozygous knockout mice. Cancer Res 62: 22612266 20 Zbuk KM and Eng C (2007) Cancer phenomics: RET and PTEN as illustrative models. Nat Rev Cancer 7: 3545 21 Nelen MR et al. (1997) Germline mutations in the PTEN/ MMAC1 gene in patients with Cowden disease. Hum Mol Genet 6: 13831387 22 The NCCN Genetic/Familial High-Risk Assessment: Breast and Ovarian Guideline (V.1.2007) 2006 National Comprehensive Cancer Network, Inc. To view the most recent and complete version of the guideline, go online to www.nccn.org (accessed July 1 2007) 23 Gorlin RJ et al. (1992) BannayanRileyRuvalcaba syndrome. Am J Med Genet 44: 307314 24 Wiedemann HR et al. (1983) The proteus syndrome. Partial gigantism of the hands and/or feet, nevi,
25 26
27 28
29 30
31 32 33 34
35
36 37 38 39 40 41 42 43 44 45
46
hemihypertrophy, subcutaneous tumors, macrocephaly or other skull anomalies and possible accelerated growth and visceral affections. Eur J Pediatr 140: 512 Starink TM et al. (1986) The Cowden syndrome: a clinical and genetic study in 21 patients. Clin Genet 29: 222233 Weber HC et al. (1998) Germline PTEN/MMAC1/TEP1 mutations and association with gastrointestinal manifestations in Cowden disease. Gastroenterology 114: 2902 Marra G et al. (1994) Cowdens disease with extensive gastrointestinal polyposis. J Clin Gastroenterol 18: 4247 McGarrity TJ et al. (2003) GI polyposis and glycogenic acanthosis of the esophagus associated with PTEN mutation positive Cowden syndrome in the absence of cutaneous manifestations. Am J Gastroenterol 98: 14291434 Eng C (2000) Will the real Cowden syndrome please stand up: revised diagnostic criteria. J Med Genet 37: 828830 Marsh DJ et al. (1998) Mutation spectrum and genotype-phenotype analyses in Cowden disease and Bannayan-Zonana syndrome, two hamartoma syndromes with germline PTEN mutation. Hum Mol Genet 7: 507515 Bosserhoff AK et al. (2006) Multiple colon carcinomas in a patient with Cowden syndrome. Int J Mol Med 18: 643647 Carethers JM et al. (1998) Absence of PTEN/MMAC1 germ-line mutations in sporadic BannayanRiley Ruvalcaba syndrome. Cancer Res 58: 27242726 Zigman AF et al. (1997) Localization of the Bannayan RileyRuvalcaba syndrome gene to chromosome 10q23. Gastroenterology 113: 14331437 Zhou XP et al. (2003) Germline PTEN promoter mutations and deletions in Cowden/BannayanRiley Ruvalcaba syndrome result in aberrant PTEN protein and dysregulation of the phosphoinositol-3-kinase/Akt pathway. Am J Hum Genet 73: 404411 Suzuki A et al. (1998) High cancer susceptibility and embryonic lethality associated with mutation of the PTEN tumor suppressor gene in mice. Curr Biol 8: 11691178 Waite KA and Eng C (2002) Protean PTEN: form and function. Am J Hum Genet 70: 829844 Chow LM and Baker SJ (2006) PTEN function in normal and neoplastic growth. Cancer Lett 241: 184196 Di Cristofano A et al. (1998) Pten is essential for embryonic development and tumour suppression. Nat Genet 19: 348355 Toccalino H et al. (1973) Juvenile polyps of the rectum and colon. Acta Paediatr Scand 62: 337340 Doxey BW et al. (2005) Inherited polyposis syndromes: molecular mechanisms, clinicopathology, and genetic testing. Clin Gastroenterol Hepatol 3: 633641 Jass JR et al. (1988) Juvenile polyposisa precancerous condition. Histopathology 13: 619630 Giardiello FM et al. (1991) Colorectal neoplasia in juvenile polyposis or juvenile polyps. Arch Dis Child 66: 971975 Howe JR et al. (1998) The risk of gastrointestinal carcinoma in familial juvenile polyposis. Ann Surg Oncol 5: 751756 Sayed MG et al. (2002) Germline SMAD4 or BMPR1A mutations and phenotype of juvenile polyposis. Ann Surg Oncol 9: 901906 Friedl W et al. (2002) Juvenile polyposis: massive gastric polyposis is more common in MADH4 mutation carriers than in BMPR1A mutation carriers. Hum Genet 111: 108111 Coburn MC et al. (1995) Malignant potential in intestinal juvenile polyposis syndromes. Ann Surg Oncol 2: 386391
september 2007 vol 4 no 9 ZBUK AND ENG
nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 501 2007 Nature Publishing Group
reviewwww.nature.com/clinicalpractice/gasthep
AcknowledgmentsKM Zbuk is a Crile Fellow of the Cleveland Clinic, USA. C Eng is a recipient of the Doris Duke Distinguished Clinical Scientist Award and is supported by grants from the US National Institutes of Health, US National Cancer Institute and the American Cancer Society. Dsire Lie, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscapeaccredited continuing medical education activity associated with this article.
Competing interestsThe authors declared no competing interests.
47 Schreibman IR et al. (2005) The hamartomatous polyposis syndromes: a clinical and molecular review. Am J Gastroenterol 100: 476490 48 Brosens LA et al. (2007) Risk of colorectal cancer in juvenile polyposis. Gut 56: 965967 49 Cao X et al. (2006) Mapping of hereditary mixed polyposis syndrome (HMPS) to chromosome 10q23 by genomewide high-density single nucleotide polymorphism (SNP) scan and identification of BMPR1A loss of function. J Med Genet 43: e13 50 Gallione CJ et al. (2004) A combined syndrome of juvenile polyposis and hereditary haemorrhagic telangiectasia associated with mutations in MADH4 (SMAD4). Lancet 363: 852859 51 Waite KA and Eng C (2003) From developmental disorder to heritable cancer: its all in the BMP/TGFbeta family. Nat Rev Genet 4: 763773 52 Wang J et al. (1995) Demonstration that mutation of the type II transforming growth factor beta receptor inactivates its tumor suppressor activity in replication error-positive colon carcinoma cells. J Biol Chem 270: 2204422049 53 Grady WM et al. (1999) Mutational inactivation of transforming growth factor beta receptor type II in microsatellite stable colon cancers. Cancer Res 59: 320324 54 Grady WM and Markowitz SD (2002) Genetic and epigenetic alterations in colon cancer. Annu Rev Genomics Hum Genet 3: 101128 55 Howe JR et al. (2004) The prevalence of MADH4 and BMPR1A mutations in juvenile polyposis and absence of BMPR2, BMPR1B, and ACVR1 mutations. J Med Genet 41: 484491 56 Howe J et al. (2007) ENG mutations in MADH4/ BMPR1A mutation negative patients with juvenile polyposis. Clin Genet 71: 9192 57 Delnatte C et al. (2006) Contiguous gene deletion within chromosome arm 10q is associated with juvenile polyposis of infancy, reflecting cooperation between the BMPR1A and PTEN tumor-suppressor genes. Am J Hum Genet 78: 10661074 58 Tsuchiya KD et al. (1998) Deletion 10q23.2-q23.33 in a patient with gastrointestinal juvenile polyposis and other features of a Cowden-like syndrome. Genes Chromosomes Cancer 21: 113118 59 Jacoby RF et al. (1997) Del(10)(q22.3q24.1) associated with juvenile polyposis. Am J Med Genet 70: 361364 60 Eng C and Ji H (1998) Molecular classification of the inherited hamartoma polyposis syndromes: clearing the muddied waters. Am J Hum Genet 62: 10201022 61 Eng C (2001) To be or not to BMP. Nat Genet 28: 105107
62 Takaku K et al. (1999) Gastric and duodenal polyps in Smad4 (Dpc4) knockout mice. Cancer Res 59: 61136117 63 Mishina Y et al. (1995) Bmpr encodes a type I bone morphogenetic protein receptor that is essential for gastrulation during mouse embryogenesis. Genes Dev 9: 30273037 64 Bourdeau A et al. (1999) A murine model of hereditary hemorrhagic telangiectasia. J Clin Invest 104: 13431351 65 Chan OT and Haghighi P (2006) Hamartomatous polyps of the colon: ganglioneuromatous, stromal, and lipomatous. Arch Pathol Lab Med 130: 15611566 66 Jacob S et al. (1998) Neurofibromatosis of the colon: an unusual manifestation of von Recklinghausens diseasesa case report. Indian J Pathol Microbiol 41: 113116 67 Schwartz RA (1978) Basal-cell-nevus syndrome and gastrointestinal polyposis. N Engl J Med 299: 49 68 Whitelaw SC et al. (1997) Clinical and molecular features of the hereditary mixed polyposis syndrome. Gastroenterology 112: 327334 69 Jaeger EE et al. (2003) An ancestral Ashkenazi haplotype at the HMPS/CRAC1 locus on 15q13-q14 is associated with hereditary mixed polyposis syndrome. Am J Hum Genet 72: 12611267 70 Fran DN et al. (2006) Rapamycin causes regression of astrocytomas in tuberous sclerosis complex. Ann Neurol 59: 490498 71 Rubio-Viqueira B and Hidalgo M (2006) Targeting mTOR for cancer treatment. Adv Exp Med Biol 587: 309327 72 Udd L et al. (2004) Suppression of PeutzJeghers polyposis by inhibition of cyclooxygenase-2. Gastroenterology 127: 10301037 73 Brazowski E et al. (2005) Characteristics of familial juvenile polyps expressing cyclooxygenase-2. Am J Gastroenterol 100: 130138 74 Bosman FT (1999) The hamartoma-adenoma-carcinoma sequence. J Pathol 188: 12 75 Perzin KH and Bridge MF (1982) Adenomatous and carcinomatous changes in hamartomatous polyps of the small intestine (PeutzJeghers syndrome): report of a case and review of the literature. Cancer 49: 971983 76 Mills SE and Fechner RE (1982) Unusual adenomatous polyps in juvenile polyposis coli. Am J Surg Pathol 6: 177183 77 Jansen M et al. (2006) Mucosal prolapse in the pathogenesis of PeutzJeghers polyposis. Gut 55: 15 78 Clevers H (2005) Stem cells, asymmetric division and cancer. Nat Genet 37: 10271028 79 Bronner M (2003) Gastrointestinal inherited polyposis syndromes. Mod Path 16: 359365
502 nature clinical practice GASTROENTEROLOGY & HEPATOLOGY 2007 Nature Publishing Group
ZBUK AND ENG september 2007 vol 4 no 9