Stroke rehabilitationEBS
16
DR.HEENA SOLANKI (PT)
-
Upload
heenasolankimpt -
Category
Health & Medicine
-
view
34 -
download
0
Transcript of Stroke rehabilitationEBS

DR.HEENA SOLANKI (PT)
Purpose of maintaining timely and accurate information on effective stroke rehabilitation, identifying ideas for further research, supporting continuous peer-review and encouraging improved evidence-based practice.
Be an up-to-date review of the current evidence in stroke rehabilitation.
Provide a comprehensive and accessible review to facilitate best practice.
Provide specific conclusion based on evidence that could be used to help direct stroke care at the bedside and at home.

Data Extraction and Quality Assessment Tool collected data relating to the study methodology,
identification of outcome measures, results, and final conclusions and also quantitatively evaluated the study’s methodological quality using the Physiotherapy developed by the Centre for Evidence Evidence Database (PEDro) scale, Based Physiotherapy (CEBP) in Australia.

Formulating Conclusions Based on Levels of Evidence The levels of evidence used to summarize the findings
are based, in part on the Eastern Ontario/Queen’s Evidence Based Report, which in turn were based on the levels of evidence used by the United States Agency for Health Care Policy and Research (AHCPR) Guidelines for Stroke Rehabilitation.

There are so many intervention is available in stroke rehabilitation in:
Upper limb
Lower limb
Aphasia
Perceptual Disorder
Dysphasia and aspiration
etc

It is so vast so upper limb in that bilateral arm training selected 6 RCT

Author/ Country PEDro score
Methods Results
Stinear et al. 2008 New Zealand 6 (RCT)
32 patients with upper limb weakness at least 6 months after stroke were randomized to a 1-month intervention of self-directed motor practice with their affected upper limb (control group)(n=16) or to Active-Passive Bilateral Therapy (APBT)(n=16), using a device that mechanically couples the two hands, for 10-15 min prior to the same motor practice (manipulating wooden blocks). Upper extremity portion of the Fugl-Meyer (FM) score was assessed at baseline, post intervention and 1 month after the intervention.
Immediately after the intervention, motor function of the affected upper limb improved in both groups (p < 0.005). One month after the intervention, the APBT group had better upper limb motor function than control patients.

Author/ Country PEDroscore
Methods Results
Lin et al. 2009 a) Taiwan 7 (RCT)
60 patients > 6 months post stroke with a Brunnstrom stage II or greater in the proximal and distal part of thearm were randomized to one of 3 groups.subject recive CIMT, bilateral arm training (BAT), or a control intervention of less- specific but active therapy.Each group received intensive training for 2 hours/day, 5 days/week, for 3 weeksOutcomesassessed included. Fugl-Meyer Assessment (FMA), FIM, Motor Activity Log (MAL), and Stroke Impact Scale (SIS).The proximal and distal scores of FMA were used to examine separate upper limb (UL) elements of movement.
The CIT and BAT groups showed better performance in the overall and the distal part score of the FMA than the control group. The BAT group exhibited greater gains in the proximal part score of the FMA than the distributed CIT and control groups. Enhanced performance was found for the distributed CIT group in the MAL, the subtest of locomotion in the FIM, and certain domains of the SIS (e.g., ADL/IADL).
Author/ Country PEDroscore
Methods Results
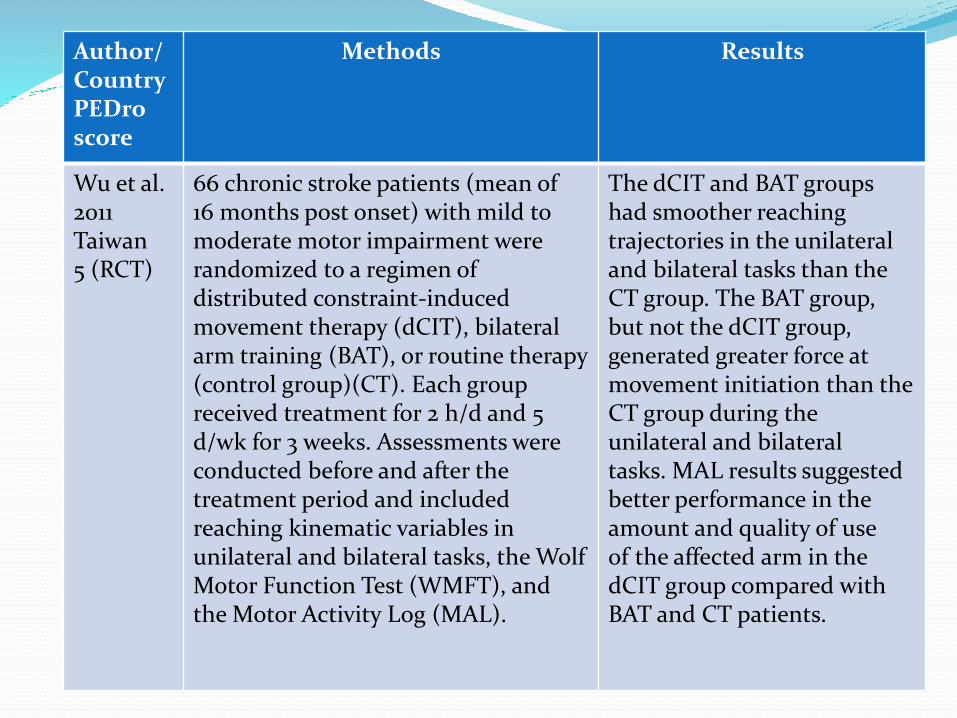
Wu et al. 2011 Taiwan 5 (RCT)
66 chronic stroke patients (mean of 16 months post onset) with mild to moderate motor impairment were randomized to a regimen of distributed constraint-induced movement therapy (dCIT), bilateral arm training (BAT), or routine therapy (control group)(CT). Each group received treatment for 2 h/d and 5 d/wk for 3 weeks. Assessments were conducted before and after the treatment period and included reaching kinematic variables in unilateral and bilateral tasks, the Wolf Motor Function Test (WMFT), and the Motor Activity Log (MAL).
The dCIT and BAT groups had smoother reaching trajectories in the unilateral and bilateral tasks than the CT group. The BAT group, but not the dCIT group, generated greater force at movement initiation than the CT group during the unilateral and bilateral tasks. MAL results suggested better performance in the amount and quality of use of the affected arm in the dCIT group compared with BAT and CT patients.

Author/ Country PEDro score
Methods Results
Brunner et al. 2012 Norway 7 (RCT)
30 patients 2-16 weeks post stroke were randomized to receive modified constraint-induced movement therapy with an emphasis on unimanual tasks, and to wear a restraining mitt on the unaffected hand for 4 hours a day for four weeks or bimanual task-related training. All patients trained with a therapist 4 hours a week for four weeks, followed by a 2-3 hours daily self-training program. Assessments were conducted before and after treatment and after three months. They included the Action Research Arm Test (ARAT), Nine-Hole Peg Test and Motor Activity Log.
Patients in both groups improved significantly over the treatment period and at follow-up, but there were no significant differences between groups on any of the outcomes. At 3 months, mean ARAT scores for patients in the mCIMT and bilateral training groups were 17.8 and 15.5, respectively.

Author/ Country PEDro score
Methods Results
Morris & Van Wijck 2012 UK 7 (RCT)
Additional reporting from Morris et al. 2008. Outcome assessments included Action Research Arm Test and Nine Hole Peg Test (9HPT) of the ipsilateral arm
The median change in ARAT scores for patients in both groups was 0 at 6 and 18 weeks. Patients in the bilateral training group moved a significantly greater number of pegs compared with the control group at 6 (0.06 vs. 0.02, p=0.03) but not 18 weeks (0.04 vs. 0.05, p=.93)

Conclusions Regarding Bilateral Arm Training
By this evidence that bilateral arm training is superior to unilateral training.
9 HPT
Fugl Meyer
ARAT
WMFT
All this shows improvement in ADL by using bilateral arm training….


bilateral arm training is more effective than unilateral training.
So during rehabilitation use bilateral arm training for good recovery.
Thank you