Streptococcus pneumoniae serotypes isolated from the middle ear fluid of Costa Rican children...
5
Vaccine 30 (2012) 3857–3861 Contents lists available at SciVerse ScienceDirect Vaccine jou rn al h om epa ge: www.elsevier.com/locate/vaccine Streptococcus pneumoniae serotypes isolated from the middle ear fluid of Costa Rican children following introduction of the heptavalent pneumococcal conjugate vaccine into a limited population Silvia Guevara a , Arturo Abdelnour a , Carolina Soley a,b , Nurith Porat c , Ron Dagan c , Adriano Arguedas a,b,∗ a Instituto de Atención Pediátrica, San José, Costa Rica b Universidad de Ciencias Médicas, San José, Costa Rica c Pediatric Infectious Disease Unit, Soroka University Medical Center and the Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel a r t i c l e i n f o Article history: Received 2 February 2012 Received in revised form 26 March 2012 Accepted 4 April 2012 Available online 19 April 2012 Keywords: Streptococcus pneumoniae Serotypes Otitis media Vaccines a b s t r a c t Background: The heptavalent pneumococcal conjugate vaccine (PCV-7) was introduced in high risk chil- dren and into the private market in Costa Rica in 2004 (<5% annual birth cohort). The aim of this study was to compare the Streptococcus pneumoniae serotype (ST) distribution, antibiotic resistance patterns and potential coverage before and after partial introduction of PCV-7. Methods: A comparison between the S. pneumoniae isolates obtained and serotyped from the middle ear fluid (MEF) of Costa Rican children with otitis media between years 1999 and 2003 (before PCV-7 usage) and those isolates obtained from 2004 to 2008. Results: A total of 145 and 218 MEF S. pneumoniae were serotyped between years 1999 and 2003 and 2004 and 2008, respectively. Considering a 19F outbreak observed between years 1999 and 2003, the following statistically significant changes in serotype distribution were detected between1999 and 2003 and 2004 and 2008: ST 3: 4.8–12.8% (P = 0.01); ST 11A: 0–4.1% (P = 0.01); ST 14: 3.5–21.1% (P < 0.001) and ST 19F: 52.4–18.3% (P < 0.05). Comparison of the two study periods demonstrated that during 2004 and 2008 a statistically significant decrease in penicillin non-susceptible serotypes (36.2–20.4% [P = 0.003]) and a statistically significant increase in trimethoprim-sulfametoxazole resistant serotypes (54.9–68.5%, respectively [P = 0.03]) was observed. Potential pneumococcal vaccines coverage between 1999 and 2003 and between 2004 and 2008 were: for PCV-7: 77.2–60.5%, respectively (P = 0.001); for the 10-valent con- jugated vaccine (PCV-10): 78.6–61.4%, respectively (P = 0.0008) and for the 13-valent conjugated vaccine (PCV-13): 84.8–79.3%, respectively (P = 0.2). Conclusions: Changes in the serotype distribution and antimicrobial susceptibility of MEF S. pneumoniae have been observed in Costa Rican children with OM. Because of the limited use of PCV-7 during the study period, these changes probably cannot be attributed to PCV-7 use. Between 2004 and 2008, PCV-13 offered the highest potential vaccine coverage. © 2012 Elsevier Ltd. All rights reserved. 1. Introduction Streptococcus pneumoniae is the most frequent pathogen iso- lated from the middle ear fluid (MEF) of Costa Rican children with otitis media (OM) and worldwide [1–4]. Based on the results of two efficacy clinical trials, the heptavalent pneumococcal conju- gated vaccine (PCV-7) was approved in the United States of America in 2000 for the prevention of OM episodes caused by the seven serotypes included in the vaccine [5,6]. ∗ Corresponding author at: Instituto de Atención Pediátrica, P.O. Box 607-1150, La Uruca, San José, Costa Rica. Tel.: +1 506 22332301; fax: +1 506 22213894. E-mail address: [email protected] (A. Arguedas). Following the introduction of PCV-7 in the National Immuniza- tion Program (NIP) of different countries, the effectiveness of PCV-7 in OM has been compared with historical data before introduction of PCV-7 and an important reduction in the number of ambulatory visits for OM (42.7%), in the number of antimicrobial prescriptions for the treatment of OM (41.9%) and in the number of antimicrobial resistant S. pneumoniae isolates have been documented following PCV-7 introduction [7–9]. Of interest, various studies have also demonstrated that PCV-7 vaccinated children had a reduction in the number of recurrent OM episodes and tube insertions rates when compared against non-PCV-7 vaccinated children [7,10]. The reduction in S. pneumoniae OM episodes following PCV-7 introduction has been associated with a proportional increase in non-typable H. influenzae and pneumococcal non-PCV-7 serotype disease, particularly serotypes 3 and 19A [11,12]. 0264-410X/$ – see front matter © 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.vaccine.2012.04.010
-
Upload
silvia-guevara -
Category
Documents
-
view
216 -
download
4
Transcript of Streptococcus pneumoniae serotypes isolated from the middle ear fluid of Costa Rican children...

SRc
Sa
b
c
a
ARRAA
KSSOV
1
lotgis
L
0h
Vaccine 30 (2012) 3857– 3861
Contents lists available at SciVerse ScienceDirect
Vaccine
jou rn al h om epa ge: www.elsev ier .com/ locate /vacc ine
treptococcus pneumoniae serotypes isolated from the middle ear fluid of Costaican children following introduction of the heptavalent pneumococcalonjugate vaccine into a limited population
ilvia Guevaraa, Arturo Abdelnoura, Carolina Soleya,b, Nurith Poratc, Ron Daganc, Adriano Arguedasa,b,∗
Instituto de Atención Pediátrica, San José, Costa RicaUniversidad de Ciencias Médicas, San José, Costa RicaPediatric Infectious Disease Unit, Soroka University Medical Center and the Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel
r t i c l e i n f o
rticle history:eceived 2 February 2012eceived in revised form 26 March 2012ccepted 4 April 2012vailable online 19 April 2012
eywords:treptococcus pneumoniaeerotypestitis mediaaccines
a b s t r a c t
Background: The heptavalent pneumococcal conjugate vaccine (PCV-7) was introduced in high risk chil-dren and into the private market in Costa Rica in 2004 (<5% annual birth cohort). The aim of this studywas to compare the Streptococcus pneumoniae serotype (ST) distribution, antibiotic resistance patternsand potential coverage before and after partial introduction of PCV-7.Methods: A comparison between the S. pneumoniae isolates obtained and serotyped from the middle earfluid (MEF) of Costa Rican children with otitis media between years 1999 and 2003 (before PCV-7 usage)and those isolates obtained from 2004 to 2008.Results: A total of 145 and 218 MEF S. pneumoniae were serotyped between years 1999 and 2003 and2004 and 2008, respectively. Considering a 19F outbreak observed between years 1999 and 2003, thefollowing statistically significant changes in serotype distribution were detected between1999 and 2003and 2004 and 2008: ST 3: 4.8–12.8% (P = 0.01); ST 11A: 0–4.1% (P = 0.01); ST 14: 3.5–21.1% (P < 0.001) andST 19F: 52.4–18.3% (P < 0.05). Comparison of the two study periods demonstrated that during 2004 and2008 a statistically significant decrease in penicillin non-susceptible serotypes (36.2–20.4% [P = 0.003])and a statistically significant increase in trimethoprim-sulfametoxazole resistant serotypes (54.9–68.5%,respectively [P = 0.03]) was observed. Potential pneumococcal vaccines coverage between 1999 and 2003and between 2004 and 2008 were: for PCV-7: 77.2–60.5%, respectively (P = 0.001); for the 10-valent con-
jugated vaccine (PCV-10): 78.6–61.4%, respectively (P = 0.0008) and for the 13-valent conjugated vaccine(PCV-13): 84.8–79.3%, respectively (P = 0.2).Conclusions: Changes in the serotype distribution and antimicrobial susceptibility of MEF S. pneumoniaehave been observed in Costa Rican children with OM. Because of the limited use of PCV-7 during the studyperiod, these changes probably cannot be attributed to PCV-7 use. Between 2004 and 2008, PCV-13 offeredthe highest potential vaccine coverage.. Introduction
Streptococcus pneumoniae is the most frequent pathogen iso-ated from the middle ear fluid (MEF) of Costa Rican children withtitis media (OM) and worldwide [1–4]. Based on the results ofwo efficacy clinical trials, the heptavalent pneumococcal conju-ated vaccine (PCV-7) was approved in the United States of America
n 2000 for the prevention of OM episodes caused by the sevenerotypes included in the vaccine [5,6].∗ Corresponding author at: Instituto de Atención Pediátrica, P.O. Box 607-1150,a Uruca, San José, Costa Rica. Tel.: +1 506 22332301; fax: +1 506 22213894.
E-mail address: [email protected] (A. Arguedas).
264-410X/$ – see front matter © 2012 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.vaccine.2012.04.010
© 2012 Elsevier Ltd. All rights reserved.
Following the introduction of PCV-7 in the National Immuniza-tion Program (NIP) of different countries, the effectiveness of PCV-7in OM has been compared with historical data before introductionof PCV-7 and an important reduction in the number of ambulatoryvisits for OM (42.7%), in the number of antimicrobial prescriptionsfor the treatment of OM (41.9%) and in the number of antimicrobialresistant S. pneumoniae isolates have been documented followingPCV-7 introduction [7–9]. Of interest, various studies have alsodemonstrated that PCV-7 vaccinated children had a reduction in thenumber of recurrent OM episodes and tube insertions rates whencompared against non-PCV-7 vaccinated children [7,10].
The reduction in S. pneumoniae OM episodes following PCV-7introduction has been associated with a proportional increase innon-typable H. influenzae and pneumococcal non-PCV-7 serotypedisease, particularly serotypes 3 and 19A [11,12].

3 cine 3
iiuocJa(bo
sMlMs([opacaP
mp22ta
2
2
tlmtp(
mrocmowp
tt
2
wptcw
858 S. Guevara et al. / Vac
PCV-7 was licensed in Costa Rica in 2004 and has been usedn high risk patients and private practice until 2009, when it wasntroduced into the NIP. Since 2004, PCV-7 has been recommendedsing a regimen that includes 3 primary doses during the first yearf life followed by a booster after 12 months of life. Taking intoonsideration the total number of PCV-7 vials distributed betweenanuary 2004 and December 2008 (52,366 vials) and the averagennual birth cohort in Costa Rica during the same period of time72,683 births per year), we estimate that less than 5% of the annualirth cohort were fully vaccinated with PCV-7 following local rec-mmendations.
The microbiology of Costa Rican children with OM have beentudied since 1991, and from 1999 to 2008, most (89%) of theEF S. pneumoniae isolated have been serotyped [1,2]. Data pub-
ished previously describing the serotype distribution among 145EF S. pneumoniae isolates indicated that the most common MEF
erotypes were: 19F (52.4%), 6B (10.3%), 3 (4.8%), 9V (4.1%), 143.5%), 16F (4.1%), 23F (3.5%), 6A (1.4%), 10A (2%) and 18C (2%)1,4]. It was interesting to observe the difference in the prevalencef serotype 19F among all the S. pneumoniae isolated between theeriods of 1999–2001 (54/55; 98%) and 2002–2003 (22/90; 24.4%),
phenomenon associated with the presence of three different cir-ulating clones reported among 1999–2001 [1,4]. Between 1999nd 2003, 112/145 (77.2%) of the MEF S. pneumoniae serotypes wereCV-7 serotypes [1,4].
The main objective of this study was to analyze the S. pneu-oniae serotype distribution, antimicrobial susceptibility andotential vaccine coverage among MEF isolates obtained between004 and 2008, following the introduction of PCV-7 in January of004 and the subsequent limited use and to compare this informa-ion to that of a previous period, 1999–2003 when PCV-7 was notvailable.
. Material and methods
.1. Study population
As part of various OM antimicrobial drug efficacy clinicalrials conducted between 2004 and 2008, 226 S. pneumoniae iso-ates were obtained from the MEF of Costa Rican children, 4–83
onths old (median age 26.1 months) who underwent a baselineympanocentesis. Data collected during years 2004–2008 (studyeriod) was compared against previously published historical data1999–2003) obtained from children with similar conditions [1,4].
The following definitions were used for this analysis: acute otitisedia (AOM), signs and symptoms of otitis media for ≤72 h; recur-
ent otitis media (ROM), history ≥3 episodes of OM in 6 monthsr ≥4 episodes in 12 months; and AOM failing therapy (OMTF),hildren with persistent signs and symptoms of otitis media, withiddle ear findings compatible with an active infection after 72 h
f appropriate antimicrobial therapy, or a OM episode occurringithin 14 days of the last dose of an antimicrobial prescribed for arevious OM episode.
All the study protocols (1999–2008) were approved by an Insti-utional Review Board, and informed consent was obtained fromhe parents of each study participant before enrollment.
.2. Middle ear fluid sampling
Basal diagnostic tympanocentesis was performed on all subjectsho had an intact tympanic membrane according to our standard
rocedures [1]. In case the participant presented with perforatedympanic membrane for ≤24 h, removal and cleaning of the earanal material was done and a deep aspiration of the MEF materialas obtained. Samples were immediately transferred to the local0 (2012) 3857– 3861
research laboratory in Amies medium without charcoal (COPANDiagnostics INC., CORONA, CA®).
2.3. Microbiology
MEF samples were inoculated onto blood agar and chocolateagar at 37 ◦C in a 5% CO2 environment for 18–72 h. If growth waspresent, identification was performed by standard procedures. S.pneumoniae identification was performed following the ClinicalCommittee for Clinical Laboratory Standards [13].
2.4. Antimicrobial susceptibility
Susceptibility testing for trimethoprim-sulfametoxazole(TMP/SMX) was done by Kirby-Bauer disk diffusion. Susceptibilitytesting for penicillin, azithromycin, ceftriaxone and levofloxacinminimal inhibitory concentration [MIC] was tested by the E-test(PDM Epsilometer, AB Biodisk, Solma, Sweden). Because of thecharacteristics of the strips and as recommended by the manufac-turer, when the E-test method was used, MIC values intermediatebetween two marks were rounded up to the next higher 2-folddilution. Interpretation of the results was performed accordingto the National Committee for Clinical Laboratory Standardsrecommendations [13].
MIC50 was defined as the MIC of a given antimicrobial drugthat inhibited growth of 50% of isolates and MIC90 was defined asthe MIC that inhibited growth of 90% of the isolates. S. pneumo-niae isolates with an MIC ≤0.06 mg/L were considered susceptibleto penicillin; isolates with a MIC value between 0.125 mg/L and1.0 mg/L were considered intermediate to penicillin and those witha MIC value >1.0 mg/L were defined as penicillin resistant. Peni-cillin intermediate and resistant isolates were grouped as penicillinnon-susceptible strains.
2.5. Serotyping
Isolates were stored at −70 ◦C at the Centro de InvestigacionesMédicas in Costa Rica using Micro Bank vials (Pro-Lab Diagnostics,Austin, TX) and then shipped on dry ice or on transport media atroom temperature to the Research Laboratory of the Pediatric Infec-tious Disease Unit at Soroka University Medical Center, Beer-Sheva,Israel. S. pneumoniae serotyping was performed, in Beer-Sheva,Israel by the Quellung reaction using antisera from Statens SerumInstitute of Copenhagen, Denmark [14].
2.6. Statistical analysis
The statistical package EPI INFO (version 6.0) was used to testdifferences on vaccine type (VT) and non-vaccine type (non-VT) S.pneumoniae isolates distribution between periods 1999 and 2003and between periods 2004 and 2008, between the different agegroups and between AOM versus ROM or/and OMTF OM diagnosisby the Fisher’s exact test, Yates chi square test, as appropriate. A Pvalue ≤0.05 was considered statistically significant.
3. Results
Between 2004 and 2008, a total of 226 S. pneumoniae isolateswere obtained from the MEF of Costa Rican children with OM of
which 218 (96%) were serotyped. Demographics characteristics ofthe subjects were compared against the group of children with S.pneumoniae OM enrolled at the same study center between 1999and 2003 (Table 1).
S. Guevara et al. / Vaccine 30 (2012) 3857– 3861 3859
Table 1Demographics characteristics of Costa Rican children with Streptococcus pneumoniaeotitis media between years 1999 and 2003 and between years 2004 and 2008.
1999–2003 2004–2008
Total number of Streptococcuspneumoniae isolates serotyped
145 218
Patients median age in months(standard deviation)
24.1 (SD ± 17.34) 25.8 (SD ± 18.55)
Patients age range (months) 5–90 4–83Patient distribution by age in months
≤24 m 92 (63.5)a 130 (59.6)a
>24 m 53 (36.5) 88 (40.4)Distribution by gender
Male 92 (63.5) 129 (59.2)Female 53 (36.5) 89 (40.8)
Distribution by diagnosisAOM 81 (55.8) 183 (83.9)ROM 37 (25.5) 28 (18.8)OMTF 19 (13.1) 6 (2.8)
3
M(a((co
2citb(ib
3
d
m1tmsd
Table 3Streptococcus pneumoniae serotype distribution among isolates obtained from CostaRican children with otitis media between years 1999 and 2003 and between years2004 and 2008.
1999–2003 2004–2008 P value
Total number of S.pneumoniae strains
145 (100)a 218 (100)a
14 5 (3.5) 46 (21.1) <0.00119F 76 (52.4) 40 (18.3) <0.056B 15 (10.3) 16 (7.3) NSb
23F 5 (3.5) 19 (8.7) NS18C 3 (2.0) 5 (2.3) NS9V 6 (4.1) 3 (1.4) NS4 2 (1.4) 4 (1.8) NS
PCV-7 coverage 112 (77.2) 133 (60.5) 0.0011 1 (0.7) 0 (0) NS7F 1 (0.7) 2 (0.9) NS5 0 (0) 0 (0) NS
PCV-10 coverage 114 (78.6) 135 (61.4) <0.0013 7 (4.8) 28 (12.8) 0.0016A 2 (1.4) 8 (3.7) NS19A 0 (0) 2 (0.9) NS
PCV-13 coverage 123 (84.8) 173 (79.3) NSOther serotypes 22 (15.2) 45 (20.6) NS
11A 0 (0) 9 (4.1) 0.0110A 3 (2.0) 4 (1.8) NS15A 0 (0) 4 (1.8) NS35B 1 (0.7) 4 (1.8) NS16F 6 (4.1) 4 (1.8) NS2 0 (0) 2 (0.9) NS18A 4 (2.8) 2 (0.9) NS9A 0 (0) 1 (1.4) NS15B/C 6 (4.1) 7 (3.2) NS18B 0 (0) 1 (1.4) NS11F 0 (0) 1 (1.4) NS23A 0 (0) 1 (1.4) NS17F 0 (0) 1 (1.4) NS9L 0 (0) 1 (1.4) NS28A 0 (0) 1 (1.4) NS6C 2 (1.4) 1 (1.4) NS34 0 (0) 1 (1.4) NS13 1 (0.7) 0 (0) NS10F 1 (0.7) 0 (0) NS
TPt
a
OMTF/ROM 8 (5.5) 1 (0.5)
a Numbers in parentheses, percent.
.1. Streptococcus pneumoniae serotyping
The most common S. pneumoniae serotypes isolated from theEF between 2004 and 2008 were: 14 (21.1%), 19F (18.3%), 3
12.8%), 23F (8.7%), 6B (7.3%), 11A (4.1%), 6A (3.7%), 15B/C (3.2%),nd 18C (2.3%). Other less common serotypes were: 10A (1.8%), 15A1.8%), 35B (1.8%), 16F (1.8%), 9V (1.4%), 2 (0.9%), 18A (0.9%), 19A0.9%), 7F (0.9%) and 9A (0.4%). MEF serotype distribution amonghildren of 24 months of age or less and those older than 24 monthsf age was similar.
Distribution of the S. pneumoniae serotypes isolated between004 and 2008, by diagnosis (AOM versus ROM and/or OMTF) wereompared against those isolated between 1999 and 2003 show-ng significant changes in the serotype distribution, mostly dueo a decline in the prevalence of serotype 19F, following the out-reak previously described and observed between 1999 and 2001Table 2) [1]. Table 3 compares the serotype distribution amongsolates obtained between 2004 and 2008 against those isolatedetween 1999 and 2003.
.2. Antimicrobial susceptibility
The MIC values observed for all S. pneumoniae serotypes areisplayed in Table 4.
Between 2004 and 2008, the overall percentage of penicillin,acrolide, TMP/SMX and ceftriaxone resistant isolates was: 20.4%,
1.1% and 68.5% and 3.8, respectively. No isolates were resistant
o levofloxacin. No statistically significant differences in penicillin,acrolide and TMP/SMX resistant isolates were seen betweentrains collected from children ≤24 months of age versus chil-ren >24 months of age. A statistically significant decrease in the
able 2revalence of Streptococcus pneumoniae serotypes according to otitis media diagnosis: areatment failure (OMTF) in Costa Rican children with otitis media between years 1999 a
AOM
1999–2003 2004–2008
Total number of S. pneumoniae strains 81 (100)a 183 (100)
Serotypes19F 40 (49.4) 35 (19.1)
6B 7 (8.6) 13 (7.1)
14 3 (3.7) 38 (20.8)
23F 2 (2.5) 15 (8.2)
9V 4 (4.9) 3 (1.6)
3 4 (4.9) 23 (12.6)
Numbers in parentheses, percent.
a Numbers in parentheses, percent.b NS: non-statistical significant.
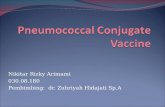
penicillin non-susceptible of S. pneumoniae was observed amongisolates obtained in 1999–2003 compared to those isolates from2004 to 2008 (36.2% and 20.4%, respectively, P = 0.003). Fig. 1shows the changes, in the percentage of penicillin non-susceptibleS. pneumoniae serotypes among the two study periods. Clearlythe 19F outbreak observed between 1999 and 2001 had an influ-ence in the penicillin susceptibility results of some of the PCV-7serotypes.
Fig. 2 compared the antimicrobial susceptibility rates to differ-ent antimicrobial observed among S. pneumoniae isolates duringthe two periods. A statistically significant increase in TMP/SMX
cute otitis media (AOM) versus recurrent otitis media (ROM) and/or otitis mediand 2003 and between years 2004 and 2008.
P-value ROM and/or OMTF P-value
1999–2003 2004–2008
64 (100) 35 (100)
<0.001 36 (56.2) 5 (14.3) <0.0010.8 8 (12.5) 3 (8.6) 0.7
<0.001 2 (3.1) 8 (22.8) 0.030.2 3 (4.7) 4 (11.4) 0.20.2 2 (3.1) 0 (0) 0.50.09 2 (3.2) 6 (17.6) 0.002

3860 S. Guevara et al. / Vaccine 3
Table 4Minimal inhibitory concentration values among Streptococcus pneumoniae strainsisolated from middle ear fluid of Costa Rican children with otitis media between2004 and 2008, according to serotypes included in the heptavalent (PCV-7), decav-alent (PCV-10) and 13 valent (PCV-13) S. pneumoniae conjugated vaccines.
Antibiotic class na Range (mg/L) MIC50 (mg/L) MIC90 (mg/L)
PCV-7 serotypePenicillin 132 ≤0.06 to 4.0 0.023 1.5Ceftriaxone 128 0.006 to 2.0 0.032 0.75Azithromycin 127 0.002 to >256 0.38 4.0Levofloxacin 128 0.008 to 3.0 0.75 1.0
PCV-10 serotypePenicillin 134 ≤0.06 to 4.0 0.023 1.5Ceftriaxone 130 0.006 to 2.0 0.032 0.75Azithromycin 129 0.02 to >256 0.38 4.0Levofloxacin 130 0.008 to 3.0 0.75 1.0
PCV-13 serotypePenicillin 173 ≤0.06 to 4.0 0.023 1.5Ceftriaxone 167 0.006 to 2.0 0.023 0.75Azithromycin 166 0.002 to >256 0.25 2.0Levofloxacin 167 0.008 to 3.0 0.75 1.0
Others serotypesPenicillin 44 <0.06 to 0.75 0.016 0.094Ceftriaxone 41 0.006 to 0.38 0.019 0.064Azithromycin 41 0.032 to 256 0.38 0.5Levofloxacin 80 0.038 to 1.0 0.75 1.0
a n = number of isolates.
0
5
10
15
20
25
30
35
14 19 F 23 F 6B 9V 6A 19 A 9A 11F 15 A 15B
% o
f Is
ola
tes
tha
t w
ere
Pen
icil
lin
No
nsu
scep
tib
le
S. pneumoniae Serot ypes
1999-2003 2004 -2008
Fig. 1. Percentage of penicillin non-susceptible Streptococcus pneumoniae serotypesisolated from the middle ear fluid of Costa Rican children with otitis media betweenyears 1999 and 2003 and between years 2004 and 2008.
0
10
20
30
40
50
60
70
80
% o
f is
ola
tes t
hat
were
Pen
icillin
No
n-
Su
sc
ep
tib
le
1999-2003 2004-2008
a b
P = 0.00 3
P = 0.2
P = 0.1
P = 0.03
Fig. 2. Proportion of non-susceptible Streptococcus pneumoniae isolated from themiddle ear fluid of Costa Rican children with otitis media between years 1999 and2003 and between years 2004 and 2008. a, MDR: nonsusceptible >3 antibiotic. b,trimethoprim-sulfametoxazole by Kirby-Bauer.
0 (2012) 3857– 3861
resistance was observed among the two periods (54.9% and 68.5%,respectively; P = 0.03).
3.3. Potential vaccine coverage
The overall potential vaccine coverage for isolates obtainedbetween years 2004 and 2008, with PCV-7, PCV-10 and PCV-13was: 60.5%, 61.4% and 79.3% respectively. PCV-13 showed a highervaccine coverage than that observed with PCV-7 or PCV-10 but thisdid not achieve statistical significant (P = 0.2).
Among children ≤24 months of age, potential vaccine cover-age with PCV-7, PCV-10 and PCV-13 was: 60.8%, 62.3% and 77.7%respectively and among children >24 months it was: 60.2%, 60.2%and 81.9% respectively.
Vaccine coverage per OM diagnosis for PCV-7, PCV-10 and PCV-13 was: AOM 59%, 62.3% and 78.7% respectively; ROM 60.7%, 60.7%and 82.1% respectively; and for OMTF 85.7% for the three formula-tions.
4. Discussion
S. pneumoniae is the most common bacterial pathogen knownto cause respiratory diseases such as AOM and historically, beforeuniversal introduction of PCV-7, was the most common pathogenisolated from MEF in Costa Rican children [1–4]. Prevalence of S.pneumoniae serotypes varies by geography, age group and season[15].
The 7-valent pneumococcal conjugate vaccine is recommendedfor the prevention of OM, pneumonia and invasive diseases causedby the 7 serotypes included in the vaccine [6,16,17]. Since the intro-duction of PCV-7, the incidence of invasive pneumococcal diseaseand pneumonia in young children has decreased significantly glob-ally. In addition, effectiveness for OM has been documented withsignificant decreases of 42.7% in ambulatory visits attributable toOM and, 41.9% for antibiotic prescriptions for the treatment of thiscondition in the United States [7,8,18].
PCV-7 was introduced in Costa Rica in January 2004 and useduntil 2009 only in high risk children and in private practice con-sultations (approximately 20% of all pediatric care). The analysisof the birth cohort and number of PCV-7 vials distributed indicatethat between 2004 and 2008 less than 5% of the total birth cohortreceived the 3 + 1 PCV-7 recommended regimen.
Since 2004, a decrease in the prevalence of PCV-7 serotypesisolated from the MEF of Costa Rican children with OM has beenobserved at our research center which is the only center thatsystematically have been performing tympanocentesis in chil-dren with OM since 1991: 77.2% of the isolates collected between1999 and 2003 were PCV-7 serotypes versus 60.5% of the isolatesdetected between 2004 and 2008 (P = 0.001). Middle ear fluid PCV-7 serotypes distribution between years 2004 and 2008, was similaramong children ≤24 and children >24 months.
Following an outbreak of three different serotype 19F clones,observed in the MEF of Costa Rican children with OM between1999 and 2001, this specific serotype declined from 75% to 18.3%(P <0.05) during years 2004 and 2008. This decline of serotype19F was compensated by a significant increase in various PCV-7serotypes such as serotype 14 (43.5–21.1%, respectively [P < 0.001])and 23F (3.5–8.7%, respectively [P = 0.07]), of 11A (0–4.1%, respec-tively [P = 0.01]) and 3 (4.8–12.8%, respectively, [P = 0.01]). Theincrease in non-PCV-7 serotypes has been observed in variouscountries following the introduction of PCV-7 and the proportionalincrease of PCV-7 serotypes 14, and 23F observed in the current
study may be associated with the resolution of the 19F outbreakobserved between 1999 and 2001 [1,4,19,20].Upon an analysis of the S. pneumoniae serotype distributionby OM diagnosis, it was interesting to observe that there were

cine 3
swtt(r
stscu([
rTdtisc
actyts[7P
PbfsP
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
S. Guevara et al. / Vac
ignificant differences by OM category. The following serotypesere more commonly isolated from the MEF of children with AOM
han among children with ROM/FOM: 3 (10.2% versus 3% respec-ively; P = 0.003); 14 (16.3% versus 4% respectively; P = 0.001); 19F16.8% versus 1% respectively; P = 0.001) and 6A (3.5% versus 0.5%espectively; P = 0.05).
Although serotype 19A has been reported as a common MEFerotype in children with OM following introduction of PCV-7 intohe NIP of different countries, so far this was not the case in ourtudy between 2004 and 2008 where 19A was found in <1% of thehildren evaluated. This may have been attributed to the limitedse of PCV-7 in the Costa Rican population during the study period<5%), thus lacking the selective pressure to have an increase in 19A21].
As shown, PCV-7 serotypes demonstrated greater antibioticesistance than non-PCV-7 serotypes, for penicillin, macrolides andMP-SMX and this was more commonly observed among chil-ren ≤24 months of age. We and others have previously reportedhis phenomenon among the 7 most common serotypes coloniz-ng the nasopharynx and OM and most likely is related to thiserotypes been more widely expose to different antimicrobiallasses [22–24].
To our knowledge this is the largest Latin America set of datanalyzing the serotype dynamics of S. pneumoniae in the MEF ofhildren with OM before PCV-7 and following a limited introduc-ion of PCV-7. Clearly the limited use of the vaccine during thoseears in less than 5% of the cohort did not have a major impact onhe MEF serotype distribution with lack of an increase of non-PCV-7erotypes as observed in countries with a largest vaccine coverage19]. However, the serotypes dynamics changes may be due to PCV-
use. Further studies are needed to investigate the real impact ofCV-7 and PCV-13 inclusion in NIP.
Currently, three PCVs are been used in Latin America (PCV-7,CV-10 and PCV-13) and our data suggest that PCV-13 offers theroadest protection against the S. pneumoniae serotypes isolatedrom the MEF of Costa Rican children with OM. Further ongoingtudies, following the introduction of PCV-7 and more recentlyCV-13 into the NIP of Costa Rica will provide more sensitive data.
eferences
[1] Arguedas A, Dagan R, Soley C, Loaiza C, Knudsen K, Porat N, et al. Microbiologyof otitis media in Costa Rican children, 1999 through 2001. Pediatr Infect Dis J2003;22:1063–8.
[2] Arguedas A, Loaiza C, Perez A, Vargas F, Herrera M, Rodriguez G, et al. Microbiol-ogy of otitis media in Costa Rican children. Pediatr Infect Dis J 1998;17:680–9.
[3] Guevara S, Soley C, Arguedas A, Porat N, Dagan R. Seasonal distributionof otitis media pathogens among Costa Rican children. Pediatr Infect Dis J2008;27:12–6.
[4] Arguedas A, Dagan R, Gttevara S, Porat N, Soley C, Perez A, et al. Middle ear fluidStreptococcus pneumoniae serotype. Distribution in Costa Rican children withotitis media. Pediatr Infect Dis J 2005;24:631–4.
[5] Eskola J, Kilpi T, Palmu A, et al. Efficacy of pneumococcal conjugate vaccineagainst acute otitis media. N Engl J Med 2001;344:403–9.
[
0 (2012) 3857– 3861 3861
[6] Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, et al. Efficacy,safety and immunogenicity of heptavalent pneumococcal conjugate vaccine inchildren: Northern California Kaiser Permanente Vaccine Study Center Group.Pediatr Infect Dis J 2000;19:187–95.
[7] Zhou F, Shefer, Nourti JP. Trends in acute otitis media-related health care uti-lization by privately insured young children in the United States, 1997–2004.Pediatr J 2008;121:253–60.
[8] Fireman B, Black SB, Shinefield HR, Henry R, Lee J, Lewis E, Ray P. Impactof the pneumococcal conjugate vaccine on otitis media. Pediatr Infect Dis J2003;22:10–6.
[9] Grijalva CG, Nuorti JP, Griffin MR. Antibiotic prescription rates for acute respi-ratory tract infections in US ambulatory settings. JAMA 2009;302(7):758–66.
10] Palmu AA, Verho J, Jokinen J, Karma B, Kilpi TM. The seven-valent pneumococcalconjugate vaccine reduces tympanostomy tube placement in children. PediatrInfect Dis J 2004;23:732–8.
11] Porat N, Soley C, Marengolciene MM, Greenberg D, Givon-Lavi N, Trefler R, et al.An international serotype 3 clone causing pediatric noninvasive infections inIsrael, Costa Rica, and Lithuania. Pediatr Infect Dis J 2008;27:709–12.
12] Dagan R, Givon-Lavi N, Leibovitz E, Creenberg D, Porat N. Introduction andproliferation of multidrug-resistant Streptococcus pneumoniae serotype 19Aclones that cause acute otitis media in an unvaccinated population. J InfectDis 2009;199:776–85.
13] National Committee for Clinical and Laboratory Standards: fifteenth informa-tional supplement. NCCLS document. M100-S12 (ISBN 1-56238-454-6). NCCLS,940 West Valley Road, Suite 140, Wayne, Pennsylvania 19087, USA, January2005.
14] Austrian R. The quellung reaction, a neglected microbiologic technique. MtSinai J Med 1976;43:699–709.
15] Hausdorff WP, Yothers G, Dagan R, Kilpi T, Pelton SI, Cohen R, et al. Multinationalstudy of pneumococcal serotypes causing acute otitis media in children. PediatrInfect Dis J 2002;21:1008–16.
16] Policy statement recommendations for the prevention of pneumococcalinfections, including the use of pneumococcal conjugate vaccine (Prevnar),pneumococcal polysaccharide vaccine, and antibiotic prophylaxis. Committeeon Infectious Diseases. Pediatrics 2000;106(2):362–6.
17] Advisory Committee on Immunization Practices. Preventing pneumococcaldisease among infants and young children: recommendations of the Advi-sory Committee on Immunization Practices (ACIP). MMWR Recomm Rep2000;45(RR-9):1–35.
18] Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lynfield R, et al.Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugated vaccine. N Engl J Med 2003;348:1737–46.
19] McEllistrem MC, Adams J, Mason EO, Wald ER. Epidemiology of acuteotitis media caused by Streptococcus pneumoniae before and after licen-sure of the 7-valent pneumococcal protein conjugate vaccine. J Infect Dis2003;188:1679–84.
20] Pelton S, Loughlin A, Marchant C. Seven valent pneumococcal conjugate vaccineimmunization in two Boston communities: changes in serotypes and antimi-crobial susceptibility among Streptococcus pneumoniae Isolates. Pediatr InfectDis J 2004;23(11):1015–22.
21] Moore MR, Gertz Jr RE, Woodbury RL, Barkocy-Gallagher GA, Schaffner W,Lexau C, et al. Population snapshot of emergent Streptococcus pneumoniaeserotype 19A in the United States, 2005. J Infect Dis 2008;197(7):1016–27,http://dx.doi.org/10.1086/528996.
22] Farrel D, Klugman K, Pichichero M. Increased antimicrobial resistance amongnonvaccine serotypes of Streptococcus pneumoniae in the pediatric populationafter introduction of 7-valent pneumococcal vaccine in the United States. Pedi-atr Infect Dis J 2007;26(2):123–8.
23] Tyrrell GJ, Kellner JD, Scheifele D, Vanderkooi OG, MacDonald J, ChurchDL. Effects of routine infant vaccination with the 7-valent pneumococ-cal conjugate vaccine on nasopharyngeal colonization with Streptococcus
pneumoniae in children in Calgary, Canada. Pediatr Infect Dis J 2008;27:526–32.24] Dagan R. Impact of pneumococcal conjugate vaccine on infections causedby antibiotic-resistant Streptococcus pneumoniae. Clin Microbiol Infect2009;15(Suppl. 3):16–20.