Stomach and Duodenum AnatomyAnatomy PhysiologyPhysiology Operative proceduresOperative procedures...
78
Stomach and Duodenum Stomach and Duodenum • Anatomy Anatomy • Physiology Physiology • Operative procedures Operative procedures • Gastric disorders Gastric disorders peptic ulcer diseases tumors structural disorders inflammatory and infectious diseases traumas
-
Upload
dwayne-phelps -
Category
Documents
-
view
226 -
download
0
Transcript of Stomach and Duodenum AnatomyAnatomy PhysiologyPhysiology Operative proceduresOperative procedures...

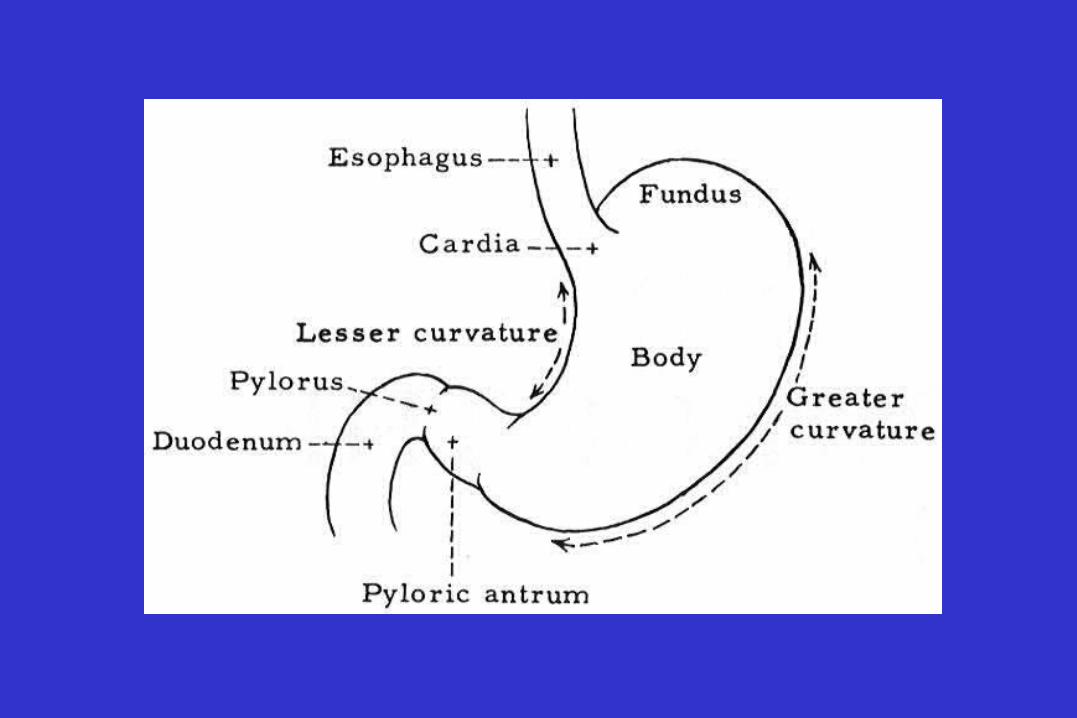
Stomach and DuodenumStomach and Duodenum• AnatomyAnatomy
• PhysiologyPhysiology
• Operative proceduresOperative procedures
• Gastric disordersGastric disorders
peptic ulcer diseases
tumors
structural disorders
inflammatory and infectious diseases
traumas



Peptic ulcer diseases• Major types ;
duodenal ulcer
gastric ulcer
stomal ulcer
• Other types ;
stress ulcer
ulcers caused by gastric irritants
steroid induced ulcer

Pathogenesis of peptic ulcer
• Lack of protection of the mucosa
• Acid production

Duodenal ulcer ;pathogenetic factors
• Increased acid secretion
• Environment ; 흡연 , NSAIDS, Helicobacter
• Mucosal defense ; decreased bicarbonate production,
decreased gastric prostaglandin production

Duodenal Ulcer : goals of operative therapy
• promotion of ulcer healing
• treatment of specific complications
• reduction of the possibility of recurrence
• minimization of postoperative side effects

surgically correctable components to reduce the acid secretion
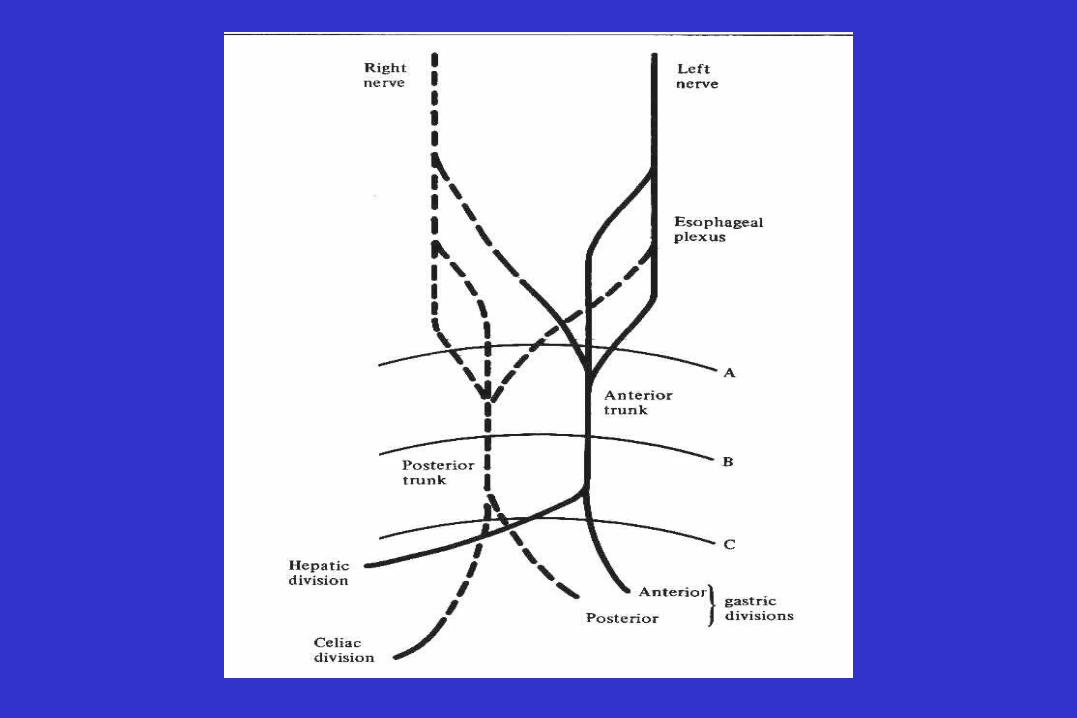
• Cholinergic vagal stimuli
• Parietal cell mass
• Gastrin secretion

Duodenal Ulcer : operative procedures
• Truncal vagotomy and drainage
• Truncal vagotomy and antrectomy
• Parietal cell vagotomy
• Alternative methods
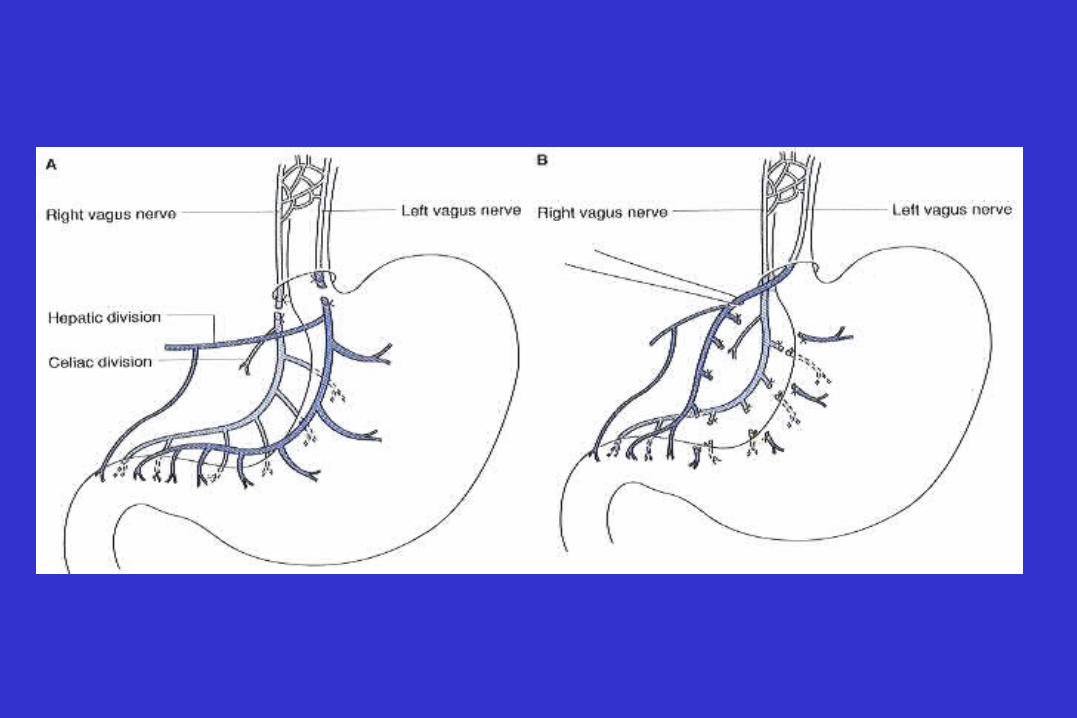


Gastric effects of truncal vagotomy
• Decreased acid secretion
• Increased serum gastrin
• Gastrin cell hyperplasia
• Accelerated liquid emptying
• Altered emptying of solid
Nongastric effects of truncal vagotomy
• Decreased pancreatic exocrine secretion
• Decreased postprandial bile flow
• Increased gallbladder volume
• Diminished release of vagally mediated peptide hormones

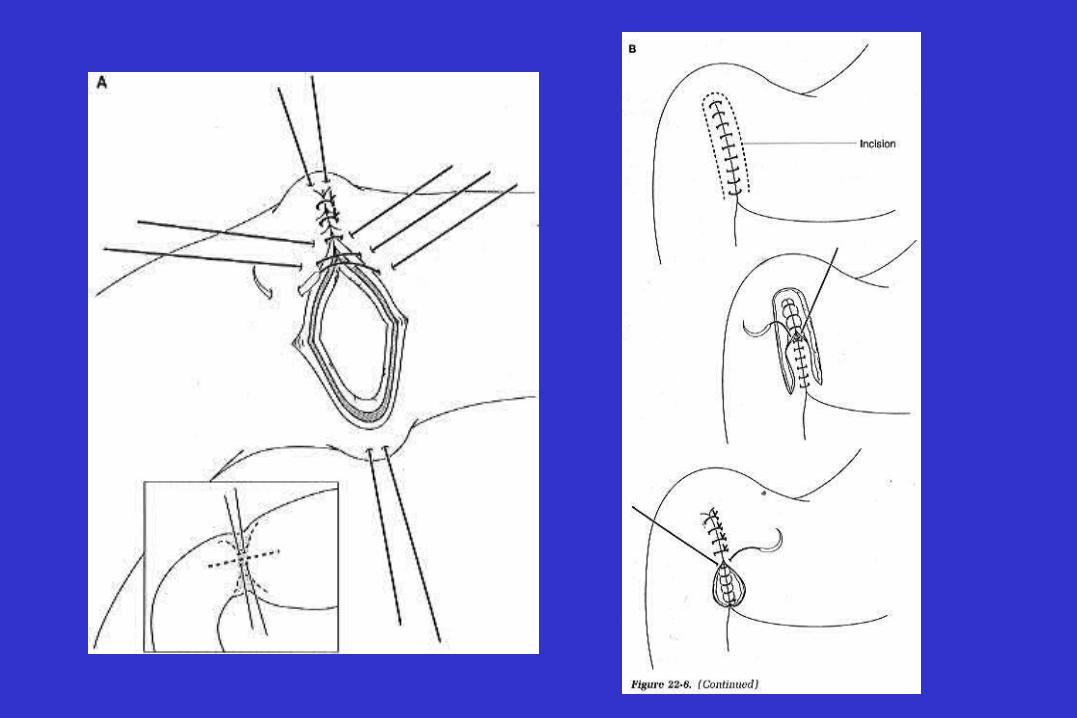
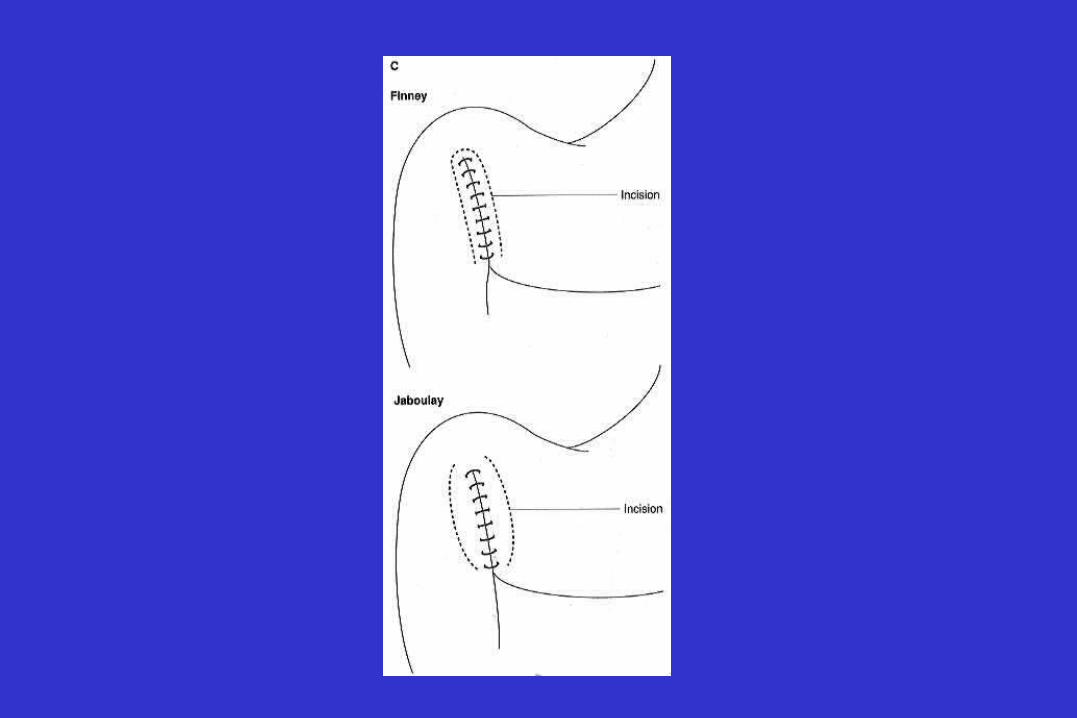
Drainage procedures : pyloroplasty
• Heineke-Mikulicz
• Finney
• Jaboulay

Duodenal Ulcer : operative procedures
• Truncal vagotomy and drainage
• Truncal vagotomy and antrectomy
• Parietal cell vagotomy
• Alternative methods



Duodenal Ulcer : operative procedures
• Truncal vagotomy and drainage
• Truncal vagotomy and antrectomy
• Parietal cell vagotomy
• Alternative methods






Duodenal Ulcer : operative procedures
• Truncal vagotomy and drainage
• Truncal vagotomy and antrectomy
• Parietal cell vagotomy
• Alternative methods
Duodenal Ulcer : choice of operation
• Location of ulcer• Indication for operation• Chronicity of the ulcer diathesis• Age and sex, nutritional status of the patient• Presence of concomitant illness• Stability of the patient during the perioperative
period• Experience and personal preference of the surgeon
Duodenal Ulcer : indications for operation
• Intractability
• Perforation
• Obstruction
• Hemorrhage

Duodenal Ulcer : indications for operation
• Intractability
• Perforation
• Obstruction
• Hemorrhage

Intractability ; criteria
• Initial healing is delayed, so that ulceration persists at 3
months despite active drug therapy
• Ulcers recur within 1 year of initial healing despite
maintenance therapy
• The ulcer disease is characterized by cycles of prolonged
activity with brief or absent remissions
Operative procedures : intractability
• First choice; parietal cell vagotomy
• Alternatives ; truncal vagotomy and antrectomy
laparoscopic vagotmy
Duodenal Ulcer : indications for operation
• Intractability
• Perforation
• Obstruction
• Hemorrhage

Clinical features ; perforated duodenal ulcer
• Symptoms ; sudden onset of severe epigastric pain spreading throughout the abdomen, variable degree of shock
• Signs ; abdominal tenderness, rigidity
• Plain X-ray ; peritoneal free air


Differential diagnosis ; perforated duodenal ulcer
• Acute cholecystitis
• Acute pancreatitis
• Strangulation obstruction
• Acute appendicitis
• Perforation of other G-I tract
• Mesenteric thrombosis

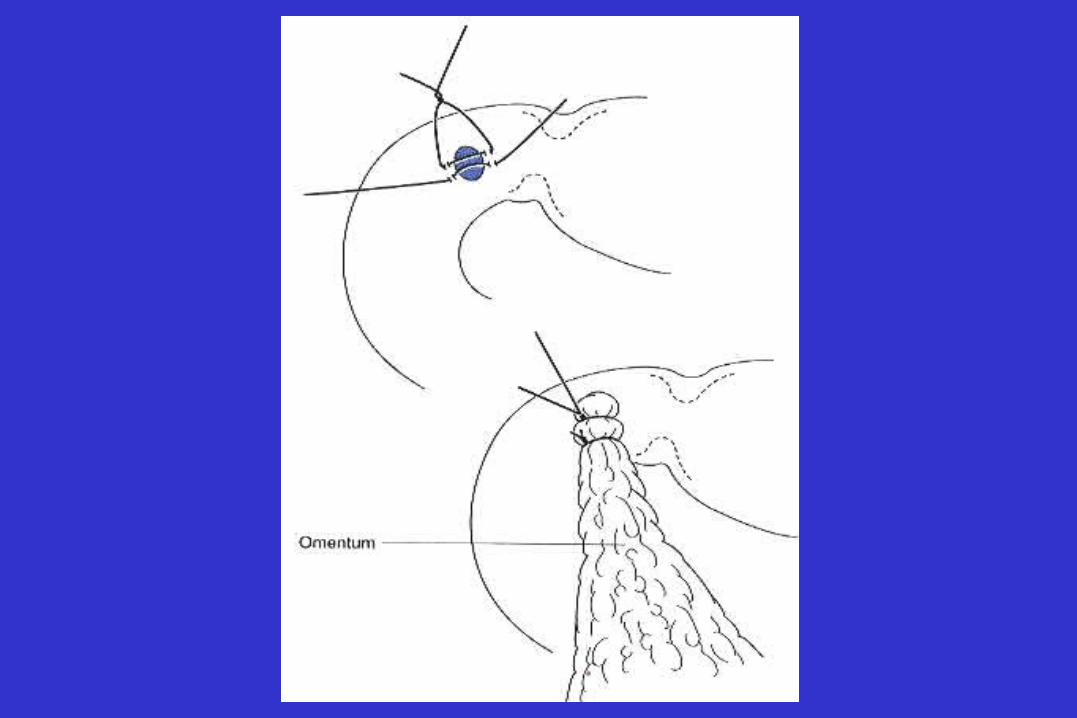
Operative procedures : perforation
• Simple closure
• Definitive surgery
parietal cell vagotomy and omental patch
truncal vagotomy and pyloroplasty
truncal vagotomy and antrectomy

Indications for definitive operation
• No preoperative shock
• No life-threatening medical illness
• Perforation has been present for less than 48 hours

Duodenal Ulcer : indications for operation
• Intractability
• Perforation
• Obstruction
• Hemorrhage

Causes of obstruction in duodenal ulcer
• Inflammation and edema
• Fibrosis

Operative procedures : obstruction
• Truncal vagotomy and antrectomy
• Truncal vagotomy and gastrojejunostomy
• Parietal cell vagotomy with dilatation


Duodenal Ulcer : indications for operation
• Intractability
• Perforation
• Obstruction
• Hemorrhage

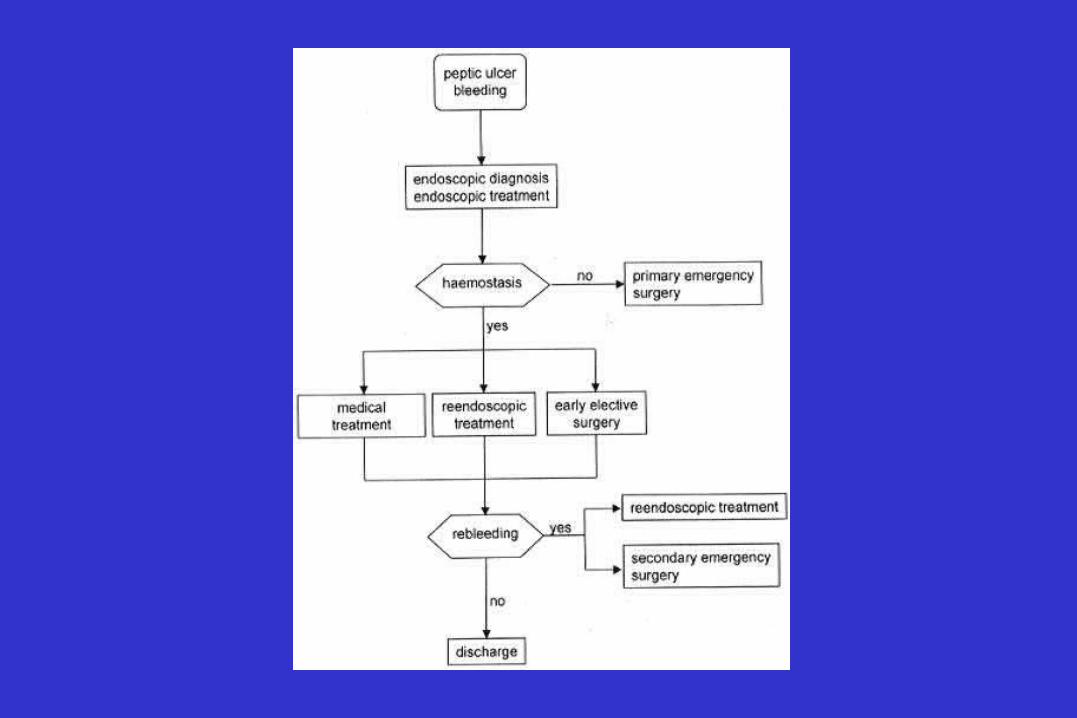
Indications for operative intervention ; duodenal ulcer bleeding
• Massive hemorrhage leading to shock
• Prolonged blood loss requiring continuing transfusion
• Recurrent bleeding during medical therapy or after endoscopic therapy
• Recurrent bleeding requiring hospitalization

Operative procedures : hemorrhage
• Truncal vagotomy and pyloroplasty with
suture ligation of bleeding vessel
• Truncal vagotomy and antrectomy
including ulcer or
suture ligation of bleeding vessel

Timing of operation : hemorrhage
• Primary emergency
• Secondary emergency
• Early elective surgery



Location of gastric ulcers

Type I gastric ulcer
• 60% of GU• Large volume of
secretion with low or normal acid secretion
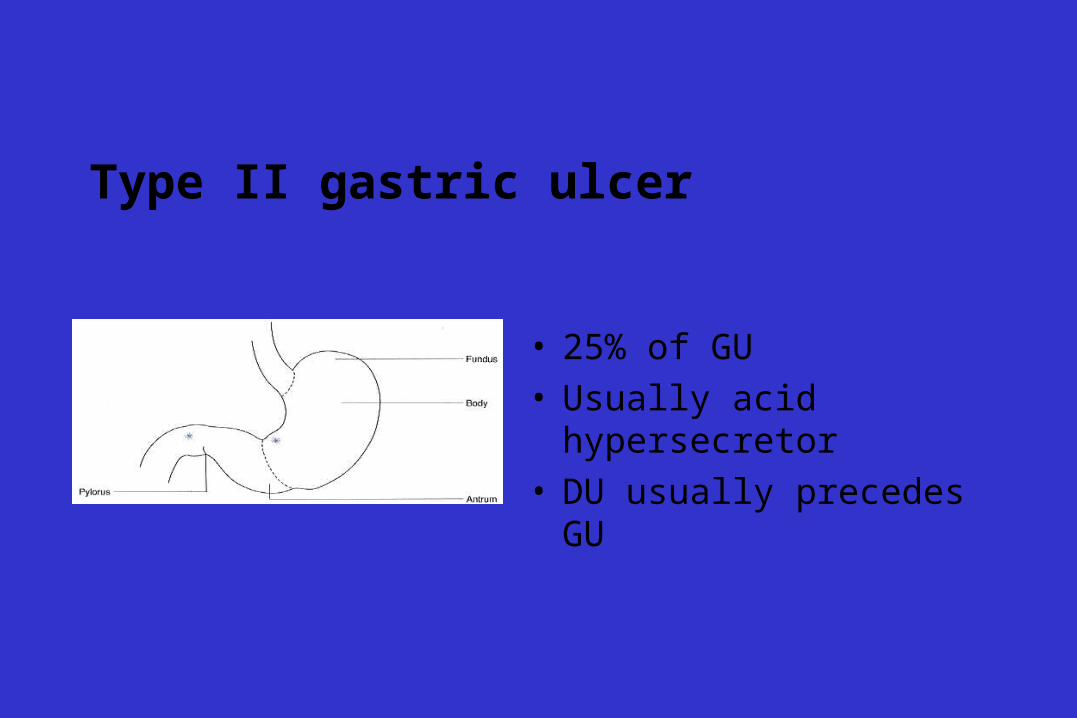
Type II gastric ulcer
• 25% of GU• Usually acid hypersecretor• DU usually precedes GU

Type III gastric ulcer
• 23% of GU• Prepyloric ulcer• Typically acid hypersecretor

Type IV gastric ulcer
• Less than 10% of GU• High-lying ulcer

Predisposing factors ; gastric conditions
• Acid and pepsin
• Gastric stasis
• Coexisting duodenal ulcer
• Duodenogastric reflux
• Gastritis
• Helicobacter pylori

Predisposing factors ; clinical conditions
• Chronic alcohol use
• NSAIDS
• Smoking
• Long-term steroid therapy
• Infection
• Intraarterial chemotherapy

Gastric Ulcer : goals of elective operation
• Primary goals ;
to excise the ulcer
to reduce acid/pepsin output
• Secondary goals ;
to minimize bile reflux and gastric stasis
Gastric ulcer : standard operations
• type I ; Distal gastrectomy and B-I anastomosis
• type II, III ; Distal gastrectomy with vagotomy
• type IV ;
TV and draiage and biopsy/excision of ulcer
Distal gastrectomy with ulcer excision
Distal gastrectomy with biopsy of ulcer
Proximal gastrectomy



Gastric Ulcer : indications for elective operation
• Failure to heal on optimal medical therapy
• Suspicion of malignancy
• Distal gastric obstruction
• Giant gastric ulcer


Gastric Ulcer : emergency operation
• Bleeding gastric ulcer
• Perforated gastric ulcer

Bleeding gastric ulcer : operative procedures
• Gastric resection including ulcer
• simple oversewing
• excision of ulcer
with TV and drainage
without TV and drainage

Gastric Ulcer : emergency operation
• Bleeding gastric ulcer
• Perforated gastric ulcer

Perforated gastric ulcer : operative procedures
• Gastric resection
• Biopsy and simple closure

New Surgical Strategy for Gastroduodenal Ulcer : New Surgical Strategy for Gastroduodenal Ulcer : Laparoscopic approachLaparoscopic approach
• Truncal vagotomy
• Thoracoscopic truncal vagotomy
• Parietal cell vagotomy

Stress Ulcer
• Multiple superficial mucosal erosions
after major physical trauma, shock,
sepsis, hemorrhage, respiratory failure,
or severe burns.



Surgical therapy
• Truncal vagotomy and drainage
• Truncal vagotomy and antrectomy
• Truncal vagotomy and subtotal gastrectomy
• Total gastrectomy
• Gastric devascularization