Steven J. Morris MD JD FACP Atlanta Gastroenterology Associates, LLC October, 2013.
23
STRUCTURING THE PRACTICE- HOSPITAL ALIGNMENT – INNOVATIVE APPROACHES Steven J. Morris MD JD FACP Atlanta Gastroenterology Associates, LLC October, 2013
-
Upload
jemimah-reed -
Category
Documents
-
view
217 -
download
0
Transcript of Steven J. Morris MD JD FACP Atlanta Gastroenterology Associates, LLC October, 2013.

STRUCTURING THE PRACTICE-HOSPITAL
ALIGNMENT – INNOVATIVE APPROACHES
Steven J. Morris MD JD FACPAtlanta Gastroenterology Associates,
LLCOctober, 2013
TransparencyFebruary 8, 2011
Colonoscopy - Diagnostic$
88
7$
91
6$
92
5$
93
2$
96
5$
98
1$
1,0
15
$1
,11
0$
1,1
69
$1
,24
9$
1,4
28
$1
,46
3$
1,5
30
$1
,53
5$
1,6
42
$1
,64
3$
1,7
13
$1
,72
1$
1,7
28
$1
,96
3$
1,9
94
$2
,09
9$
2,3
09
$2
,32
0$
2,4
51
$2
,77
1$
2,8
16
$2
,87
6$
2,8
81
$2
,98
7$
3,0
13
$3
,03
9$
3,0
49
$3
,27
1$
3,3
01
$3
,31
8$
3,3
33
$3
,36
7$
3,6
47
$3
,76
9$
3,7
93 $4
,51
8$
4,5
76 $
5,5
96
$5
,68
2$
5,7
34
$7
,24
5
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
AA
BB
CC
DD EE
FF
GG
HH II JJ KK LL
MM NN
OO
PP
RR
SS TT
UU
Room & Supplies Professional Medications Diagnostics
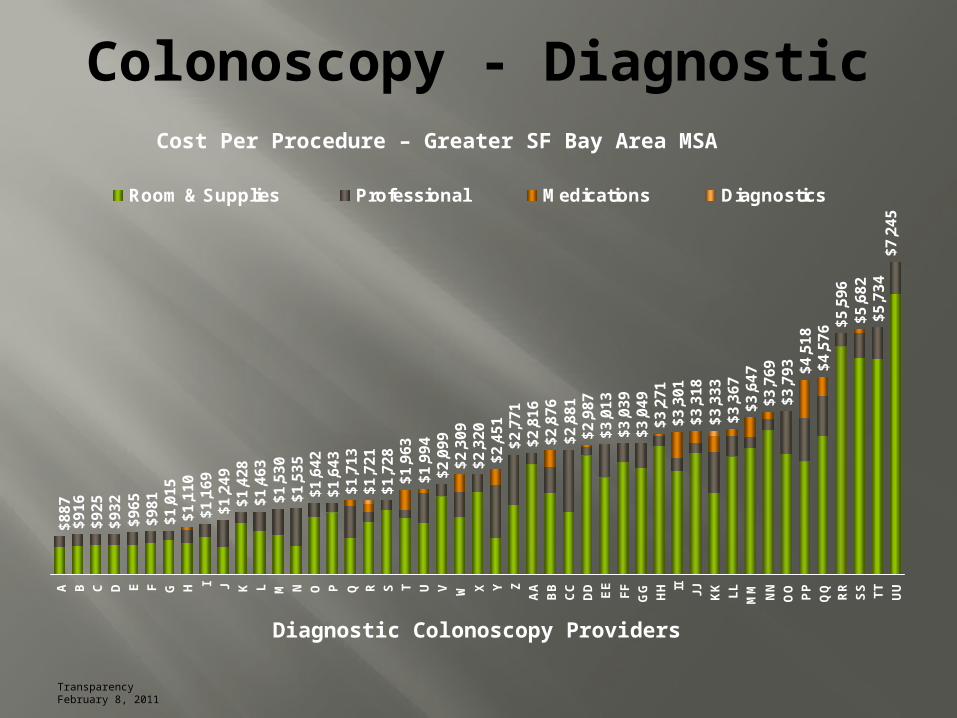
Cost Per Procedure – Greater SF Bay Area MSA
Diagnostic Colonoscopy Providers

Colonoscopy in the SF Bay Area*
$887$1,249
$1,963
$2,876$3,333
$3,769
$5,596
$7,245
A J T BB KK NN RR UU
Room & Supplies Professional Medications Diagnostics
* Safeway Health 2011
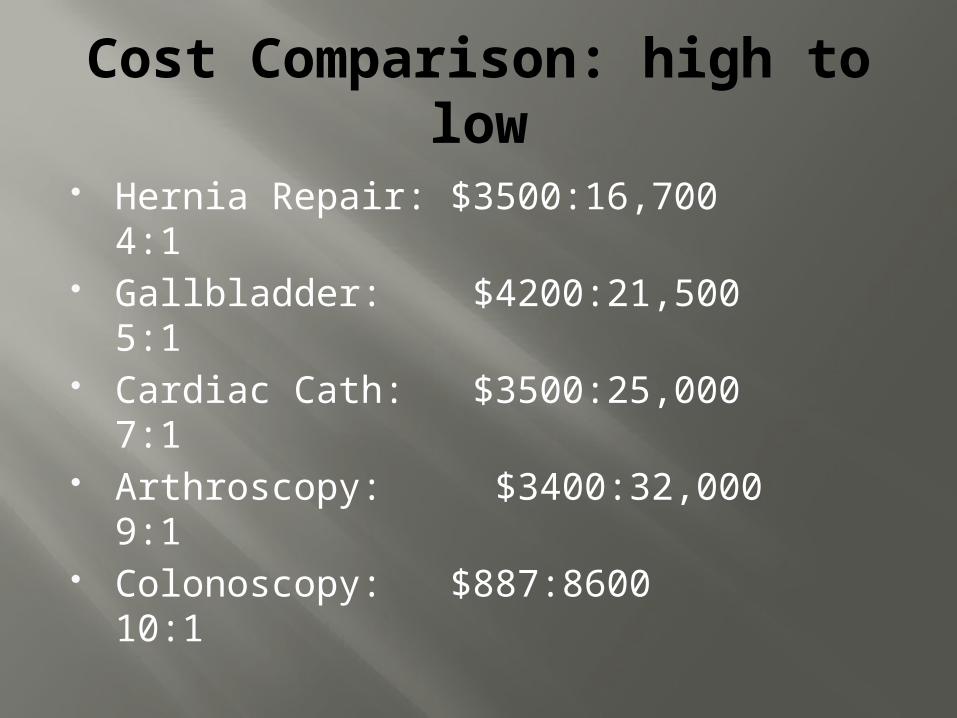
Cost Comparison: high to low
Hernia Repair: $3500:16,700 4:1 Gallbladder: $4200:21,500 5:1 Cardiac Cath: $3500:25,000 7:1 Arthroscopy: $3400:32,000 9:1 Colonoscopy: $887:8600 10:1

Non Profit HospitalsHospital Name Operating Profit CEO Compensation
U of Pittsburgh M.C. $769,000,000 $6,000,000
Cleveland Clinic $572,000,000 $2,600,000
Barnes Jewish Hospital $489,000,000 $2,335,000
N.Y. Presbyterian/Weill Cornell M.C.
$383,000,000 $4,360,000
Indiana U. Health- Methodist Hospital
$360,000,000 $2,100,000
Florida Hospital -Orlando
$352,000,000 $3,000,000
Montefiore M.C.- Bronx $196,000,000 $4,000,000
Methodist U. Hospital - Memphis
$151,000,000 $2,200,000
Norton Hospital- Louisville, Ky.
$118,000,000 $2,200,000
** Brill, StevenTime Magazine 3/4/2013
Hospital Physician Alignment
• Traditional Relationship• Hospital Based Service
Agreements• Professional Service
Agreements• Employment

Hospital Based Service Agreements
Co-management service agreements between health systems and physician groups
Variety of services: Medical director services Strategic planning Human resource duties Scheduling and staffing
Legal Considerations: service agreements
Stark Law Structure to meet FMV or Personal Service
exceptions Anti-Kickback Statutes (AKS)
Never tie compensation to volume/value False Claims Act CMS requirements Tax Exempt status

Hospital Employment
National trend towards hospital employment
Reasons: Scarcity of Primary Care Physicians Mantra of “work-life” balance Quality Initiatives
Pay-for Performance, PQRIHealthcare Reform
Accountable Care Act

Hospital Employment
Direct Hospital Employment Simplest model if no state statutory
prohibitions Foundation Model
States with corporate practice of medicine laws
Hospital controls board and obtains tax exempt status
Physician leasing model Subsidiary/Affiliated Entity Models
Transitional models

Professional Service Agreeement
Employment Lite Independent Contractor Agreement -
usually with a group Physicians remain within their corporate
structure Physicians reassign their right to
payment to the hospitals Hospital bills all payers for their services
Employment v PSA
EMPLOYMENT PSA
W2 Employee More favorable
reimbursement Less Overhead No Complex
Regulation Lifestyle Safer Legal Model Fear
Remain Independent Maintain group
dynamics Easier to unwind Avoid employment
stigma Collaboration with
hospital on quality and other initiatives

PSA Basic Scenarios
Global Payment PSA Hospital K with practice for global payment rate
Practice Management Arrangements Hospital employs physicians Practice entity is retained and enters into another
K with hospital for management services Traditional PSA
Hospital K with physicians via practice Hospital employs the practice staff
Hybrid Arrangements

Compensation
Parties calculate wRVU based compensation and conversion factor
Combination of historical productivity and payer mix
Length of conversion factor Length of agreement/renewal Usually all parties do separate valuations
and negotiate the final number

2012 MGMA Annual Report
Specialty Median Physician work RVU
Median Compensation to work RVU Ratio
Median Physician Compensation
Cardiology- Invasive
9,406 $57.03 $521,454
Dermatology 7,840 $55.46 $428,382
Gastroenterology
8,492 $56.44 $481,347
Internal Medicine
4,795 $46.35 $215,689
Orthopedic Surgery
7,981 $63.54 $520,1119
Source: MGMA Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. Used with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado, 80112. www.mgma.com.
Betsy Holt
Needs permissions

Applicable Healthcare Laws
Stark Law Anti-kickback Statute IRS Rules on Employment/Independent
contractor 501(c) (3) principles Antitrust
Monopolization Concerted Action

Process – Your Group
Evaluate your group Size Geography Community
Goals of Transaction Stabilization Future Growth
Bundling ASC’s; Pathology; Imaging

Process- Your Group
What strengths does your group have Size, geography, quality initiatives, service
lines, centers of excellence What can you add to your partner? What needs do you have: ? EMR ? Capital Transaction timing
Earnings and growth New ASC’s Market place consolidation: early movers do
better!!
Do’s and Don’t’s
Yes: Combine PSA with other transactions Use PSA as an employment segue Use PSA to adapt to a changing marketplace
No Unrealistic compensation expectations Unwillingness to truly “partner”
Strategic planning Increase market share Quality initiatives Align hospital and practice goals

Process - Hospital Partner
Vision Open to PSA v Employment Model
Alignment Geography Inpatient v Outpatient
Size and Financial Strength Bigger not always better
Local v National

Hybrid Agreement
‘Crossing the Rubicon’ Maintain employees, office space, EMR, Equipment
Five Year Term with Renewal Reevaluate wRVU Bilateral renewal options
Bundled Sales Pathology Research division Existing ASC’s
Coverage Agreements Hospitals Geographic regions

Hybrid Agreements
Service Lines Governance
Committees : Practice, Ancillarieso Compositiono Dispute resolution
Growth Practice – organic, acquisition Research ASC
Summary
Advantages Accounts Receivable Growth Financial & Strategic Partner Maintain Independence
Disadvantages Complex regulatory environment Financial risk mitigated but still present “Backlash” Obligations of partnership