
Prof. Leung-Wing Chu MD, FRCP ( Lond ., Edin . & Glas .) , FHKCP, FHKAM (Medicine)
Upload
hayden-murrellCategory
view
215download
1
Endoscopic Stenting for Pancreatic Diseases
Joseph Leung, MD., FRCP., FACP., MACG., FASGE., Joseph Leung, MD., FRCP., FACP., MACG., FASGE., FHKCP., FHKAMFHKCP., FHKAM
Chief, Section of Gastroenterology,Chief, Section of Gastroenterology,VA Northern California Health Care System,VA Northern California Health Care System,Mr. & Mrs. C.W. Law Professor of Medicine,Mr. & Mrs. C.W. Law Professor of Medicine,
University of California, Davis Medical CenterUniversity of California, Davis Medical Center

Pancreatic Stents ShapeShape
– Geenen - curve, multiple Geenen - curve, multiple side holes/distal flapsside holes/distal flaps
– Sherman - straight, Sherman - straight, multiple side holes, multiple side holes, proximal flap/distal pigtailproximal flap/distal pigtail
– Modified Cotton-Leung Modified Cotton-Leung stent – S-shaped with stent – S-shaped with distal flapdistal flap
Size 3,5,7 or 10 Fr Size 3,5,7 or 10 Fr Length 3,5,7,9,12 cmLength 3,5,7,9,12 cm

Pancreatic Stents – Design and Application Pancreatic Stents – Design and Application
Common IndicationsCommon Indications Acute pancreatitisAcute pancreatitis
– Drainage to prevent post Drainage to prevent post ERCP pancreatitisERCP pancreatitis
– Assist endoscopic therapyAssist endoscopic therapy PapillotomyPapillotomy LeaksLeaks
MalignancyMalignancy– Drainage to relief painDrainage to relief pain
Chronic pancreatitisChronic pancreatitis– Adjuvant therapy for stone Adjuvant therapy for stone
and stricture and stricture
Optimal design of stentsOptimal design of stents Size (small)Size (small) Material (soft)Material (soft)
– Less irritation to ductal Less irritation to ductal epitheliumepithelium
Migrate out spontaneouslyMigrate out spontaneously

Technique of Pancreatic Stent PlacementTechnique of Pancreatic Stent Placement
Deep cannulation Deep cannulation with guide wire with guide wire across papilla or across papilla or stricturestricture
++ Pancreatic Pancreatic papillotomypapillotomy
Stent inserted over Stent inserted over wire and positioned wire and positioned with pusherwith pusher

Pancreatic Stenting using Pancreatic Stenting using Mechanical SimulatorMechanical Simulator
Stenting with Fusion Stenting with Fusion systemsystem
External wire lock External wire lock anchors guide anchors guide wire allowing wire allowing minimal exchange minimal exchange over guide wireover guide wire
Stent deployment Stent deployment is easily is easily coordinated coordinated

Post-ERCP PancreatitisPost-ERCP Pancreatitis
IncidenceIncidence Most common Most common
complication of ERCPcomplication of ERCP Incidence 5-10%, 1% Incidence 5-10%, 1%
severe, 0.1% fatalsevere, 0.1% fatal Significant medical/ Significant medical/
social/economic and social/economic and liability problemliability problem
Possible causesPossible causes Acinarization – overfillingAcinarization – overfilling Hyperosmolarity / Hyperosmolarity /
contrast allergy contrast allergy Trauma – guide wireTrauma – guide wire Coagulation injuryCoagulation injury Impaired drainage from Impaired drainage from
pancreas pancreas Bacterial contaminationBacterial contamination Bile contaminationBile contamination

Mechanism of Post ERCP PancreatitisMechanism of Post ERCP Pancreatitis
Papillary manipulation results in edema and Papillary manipulation results in edema and sphincter spasm obstructing PD flow, leading to sphincter spasm obstructing PD flow, leading to intracellular activation of enzymesintracellular activation of enzymes
Improving drainage with PD stent may prevent Improving drainage with PD stent may prevent post ERCP pancreatitispost ERCP pancreatitis

PD Stenting Prevents PEP in SOD PtsPD Stenting Prevents PEP in SOD Pts
80 Pts with pancreatic SOD after biliary EST 80 Pts with pancreatic SOD after biliary EST were randomized to PD stent or no stent were randomized to PD stent or no stent
Post ERCP pancreatitis occurred in Post ERCP pancreatitis occurred in – 10/39 (26%) with “No stent” 10/39 (26%) with “No stent” – 1/41 (2.4%) with “Stent” 1/41 (2.4%) with “Stent”
2 Pts (7%) developed PEP after stent removal2 Pts (7%) developed PEP after stent removal
Tarnasky Gastroenterol 1998
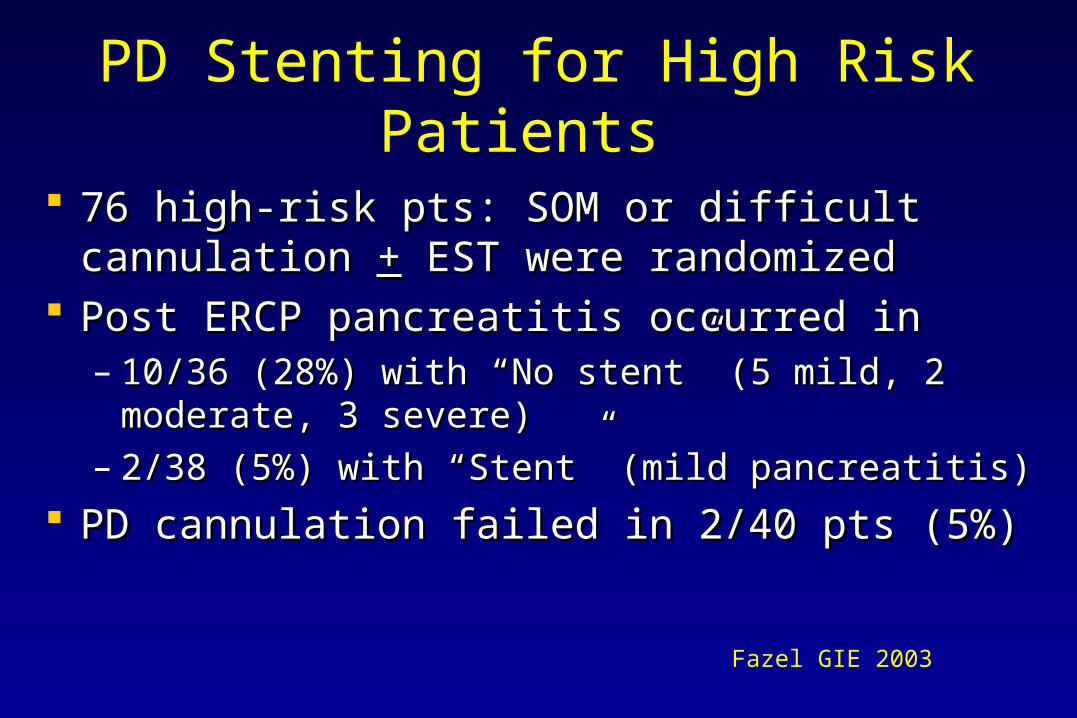
PD Stenting for High Risk Patients
76 high-risk pts: SOM or difficult cannulation 76 high-risk pts: SOM or difficult cannulation ++ EST were randomized EST were randomized
Post ERCP pancreatitis occurred in Post ERCP pancreatitis occurred in – 10/36 (28%) with 10/36 (28%) with “No stent” “No stent” (5 mild, 2 moderate, 3 (5 mild, 2 moderate, 3
severe)severe)– 2/38 (5%) with 2/38 (5%) with “Stent”“Stent” (mild pancreatitis) (mild pancreatitis)
PD cannulation failed in 2/40 pts (5%)PD cannulation failed in 2/40 pts (5%)
Fazel GIE 2003

Is PD Stent Necessary for Every ERCP?Is PD Stent Necessary for Every ERCP?
Probably NOTProbably NOT Increased time and difficultyIncreased time and difficulty Increased riskIncreased risk Increased costIncreased cost Risk of ductal changes from stent irritationRisk of ductal changes from stent irritation Need follow–up to insure stent migrationNeed follow–up to insure stent migration May need 2May need 2ndnd procedure for stent removal procedure for stent removal

Who Will Benefit from PD Stenting?
Patient FactorsPatient Factors Suspected SODSuspected SOD Young femaleYoung female Prior post-ERCP Prior post-ERCP
pancreatitispancreatitis Normal serum bilirubinNormal serum bilirubin
Technical FactorsTechnical Factors Difficult cannulationDifficult cannulation Pre-cut sphincterotomyPre-cut sphincterotomy
Pancreatic sphincterotomyPancreatic sphincterotomy AmpullectomyAmpullectomy Balloon sphincteroplastyBalloon sphincteroplasty

Potential Risks of Pancreatic Stenting
RisksRisks Failed stent placementFailed stent placement Proximal tip of stent Proximal tip of stent
damages PDdamages PD Stent occlusion causing Stent occlusion causing
pancreatitispancreatitis Chronic ductal changesChronic ductal changes Inward stent migrationInward stent migration
DilemmaDilemma To consider PD stent To consider PD stent
placement in a “high-risk” placement in a “high-risk” patient is a serious patient is a serious decisiondecision
If successful, risk of PEP If successful, risk of PEP is reduced. is reduced.
However, failed attempt However, failed attempt INCREASES the risksINCREASES the risks

Outcome of Failed PD Stenting
225 high-risk therapeutic ERCP’s225 high-risk therapeutic ERCP’s PEP 32/222 (14%) with successful PD stentsPEP 32/222 (14%) with successful PD stents PEP in 2/3 (67%) with failed PD stent insertionPEP in 2/3 (67%) with failed PD stent insertion Severe pancreatitis occurred only in failed stentsSevere pancreatitis occurred only in failed stents Multivariate analysis: failed stent RR 16, SOD RR Multivariate analysis: failed stent RR 16, SOD RR
3.2, prior PEP RR 3.23.2, prior PEP RR 3.2 Not significant: EST, NK precut, # PD injections Not significant: EST, NK precut, # PD injections
or difficult cannulationor difficult cannulation
Freeman GIE 2004

Balloon Sphincteroplasty & Double StentsBalloon Sphincteroplasty & Double Stents
Double wiresDouble wires Balloon Balloon
sphincteroplastysphincteroplasty Double stents for Double stents for
drainagedrainage PD stent for PD stent for
prophylactic prophylactic drainagedrainage

Assisted Precut Biliary SphincterotomyAssisted Precut Biliary Sphincterotomy
PD stent protects PD stent protects pancreas pancreas
Needle knife Needle knife precut along precut along biliary axisbiliary axis

Pancreas DivisumPancreas DivisumMinor Papillotomy with PD StentingMinor Papillotomy with PD Stenting

Chronic Pancreatitis - Stone & Stricture

EndoTherapy for Chronic Pancreatitis
Less invasive than surgery Results comparable to
surgery Surgery is still possible
after failed endotherapy ? Predicts outcome after
surgery

Dilation/Stenting of Pancreatic Stricture
Guide wire (hydrophilic) Guide wire (hydrophilic) across stricture across stricture
DilatorsDilators– Graded dilators Graded dilators – Pneumatic balloons (4-6 mm) Pneumatic balloons (4-6 mm)
Short-term pancreatic stenting Short-term pancreatic stenting to insure drainage to insure drainage

Dilation of Tight PD Stricture with Soehendra Stent Retriever

Dilation of Pancreatic Stricture via Minor Papilla

Basket Stone Extraction

Pancreatic Stone Extraction
Pancreatic sphincterotomy Pancreatic sphincterotomy .035” guide wire.035” guide wire Dilation of orifice/stricture Dilation of orifice/stricture Stone extraction with wire Stone extraction with wire
basket (e.g. 22Q)basket (e.g. 22Q) ? Mechanical lithotripsy? Mechanical lithotripsy
– limitations limitations
PD stent for drainage PD stent for drainage ESWL to fragment large ESWL to fragment large
(calcified) stone (calcified) stone

Endoscopic Stenting for Chronic PancreatitisEndoscopic Stenting for Chronic PancreatitisInitial Technical SuccessInitial Technical Success
NN StentStent Succ CompSucc Comp ImprovImprov SurgSurg Mean Mean F/UF/U
(Fr) (%) (%) (%) (n)(months)
Cremer (91) 76 10 99 16 94 11 37
Ponchon (95) 23 10 100 43 91 3 12
Smits (95) 51 5,7 96 22 82 4 34
Binmoeller (95) 93 5,7,10 100 6 74 24 3-12
Stent ex-change mean 2-6 monthsStent ex-change mean 2-6 months
Complications included pancreatitis (15), cholangitis (3), bleeding (3), Complications included pancreatitis (15), cholangitis (3), bleeding (3), pain (4), fever (3), infection (8) and abscess (2)pain (4), fever (3), infection (8) and abscess (2)

Endoscopic Stenting for Chronic PancreatitisEndoscopic Stenting for Chronic PancreatitisOutcome after Stent RemovalOutcome after Stent Removal
AuthorAuthor ContinuousContinuous Mean F/UMean F/U StrictureStrictureimprovementimprovement (month) (month) resolvedresolved
Cremer Cremer (91)(91) 7/64 (11%)7/64 (11%) 2525 11%11%
Ponchon Ponchon (95)(95) 12/21 (57%)12/21 (57%) 1414 38%38%
Smits Smits (95)(95) 23/33 (70%)23/33 (70%) 2929 20%20%
BinmoellerBinmoeller (95)(95) 41/69 (59%)41/69 (59%) 3333 NDND
TotalTotal 83/187(44%)83/187(44%) 25.325.3 23%23%

ESWL for Pancreatic Stone
Courtesy of Dr. N Reddy
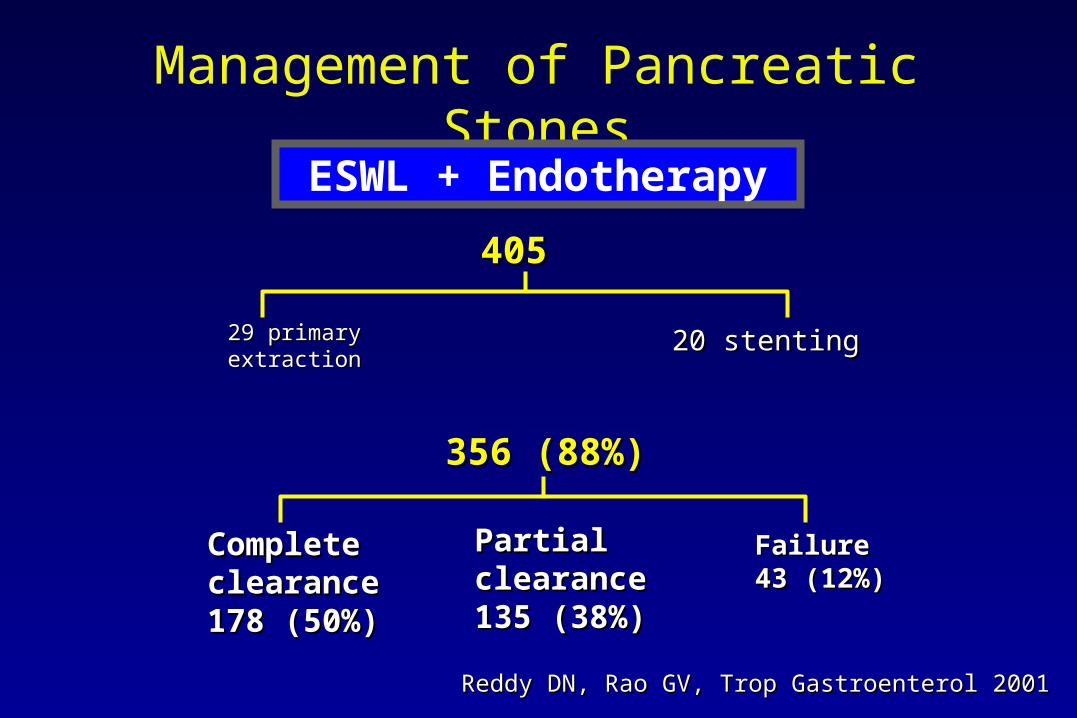
Management of Pancreatic Stones
405405
29 primary extraction29 primary extraction 20 stenting20 stenting
356 (88%)356 (88%)
Complete Complete clearanceclearance178 (50%)178 (50%)
Partial Partial clearanceclearance135 (38%)135 (38%)
Failure 43 Failure 43 (12%)(12%)
ESWL + Endotherapy
Reddy DN, Rao GV, Trop Gastroenterol 2001Reddy DN, Rao GV, Trop Gastroenterol 2001

Management of Pancreatic Stones
CompleteComplete 178178 170170
PartialPartial 135135 102102
NoneNone 4343 00
272/356 (76%)272/356 (76%)
ESWL + Endotherapy
MPD Painclearance relief
Reddy DN, Rao GV, Trop Gastroenterol 2001Reddy DN, Rao GV, Trop Gastroenterol 2001

Summary
Successful pancreatic stenting and drainage Successful pancreatic stenting and drainage prevents post ERCP pancreatitisprevents post ERCP pancreatitis
Pancreatic stenting is a useful adjunct for assisted Pancreatic stenting is a useful adjunct for assisted papillotomypapillotomy
Pancreatic stenting provides drainage in patients Pancreatic stenting provides drainage in patients undergoing ESWL for stone obstructionundergoing ESWL for stone obstruction
Stenting helps to improve stricture post dilation Stenting helps to improve stricture post dilation and provides short term pancreatic drainageand provides short term pancreatic drainage


















