
Stereotactic lesional surgery for the treatment of tremor in - Brain
14
Brain (2001), 124, 1576–1589 Stereotactic lesional surgery for the treatment of tremor in multiple sclerosis A prospective case-controlled study S. H. Alusi, 1 T. Z. Aziz, 1 S. Glickman, 2 M. Jahanshahi, 3 J. F. Stein 4 and P. G. Bain 1 1 Division of Neurosciences and Psychological Medicine, Correspondence to: Dr Peter Bain, Department of Imperial College School of Medicine, Charing Cross Neurology, Division of Neuroscience and Psychological Hospital Campus, 2 The Multiple Sclerosis Unit, North West Medicine, Imperial College School of Medicine, Charing London NHS Trust, Central Middlesex Hospital, Cross Hospital Campus, Fulham Palace Road, London 3 Department of Clinical Neurology Institute of Neurology, W6 8RF, UK London and 4 University Department of Physiology, E-mail: p.bain@ic.ac.uk Oxford University, Oxford, UK Summary The effect of stereotactic lesional surgery for the treatment one case. Two patients developed hemiparesis and in two cases epilepsy recurred. Two surgical patients and one of tremor in multiple sclerosis was examined in a prospective case-controlled study. Surgery was not control patient died between the 3 and 6 months assessments. Both groups had a significant deterioration undertaken in 33 patients (72% of 46 cases referred for stereotactic surgery), two of whom died within 4 months in EDSS but not Barthel ADL Index scores at 1 year, but the difference between the groups was not significant. of referral. Twenty-four multiple sclerosis patients were included in the study; 13 underwent surgery and were Similarly, no differences between the groups’ rates of deterioration of speech or swallowing or MMS were matched against 11 controls on the basis of age, sex, expanded disability system scores (EDSS) and disease found. Significant improvements in contralateral upper limb postural (P2) and kinetic tremors, spiral scores and duration. Assessments were carried out at baseline/ preoperatively, and then 3 and 12 months later; these head tremor were detected at 3 and 12 months after surgery (but not handwriting or nine-hole peg test included accelerometric and clinical ratings of tremor, spirography, handwriting, a finger-tapping test, nine-hole performance). Tremor-related disability and finger- tapping speed were also significantly better 12 months peg test, tremor-related disability, general neurological examination, Barthel Activities of Daily Living (ADL) after surgery, the latter having significantly worsened for the control group. A 3 Hz ‘filter’ for postural (P2) Index of general disability, EDSS, a 0–4 ataxia scale, Mini- Mental State (MMS) examination, speech and swallowing upper limb tremor was detected by accelerometry/spectral analysis above which tremor was always abolished and at assessments and grip strength. Postoperative MRI scans demonstrated that tremor could be attenuated by lesions or below which some residual tremor invariably remained. Criteria for selecting multiple sclerosis patients for this centred on the thalamus in seven cases, on the zona incerta in five cases and in the subthalamic nucleus in form of surgery are discussed. Keywords: tremor; frequency; multiple sclerosis; thalamotomy Abbreviations: AC anterior commissure; ADL Activities of Daily Living; ANOVA analysis of variance; EDSS expanded disability system scores; FTT finger-tapping test; MMS Mini-Mental State; PC posterior commissure; Vim nucleus ventralis intermedius; Vop nucleus ventralis oralis posterior Introduction Although, over the last 40 years, a considerable number of available for addressing the crucial questions: (i) What degree of benefit can be expected from thalamotomy in terms of stereotactic thalamotomies have been performed for the treatment of tremor in multiple sclerosis, it is remarkable tremor suppression, functional gain and overall disability? (ii) What is the optimal intracerebral target site for treating how little accurate information is available about the effects of these procedures. In particular, there are very few data multiple sclerosis tremor? (iii) Does this form of surgery © Oxford University Press 2001
Transcript of Stereotactic lesional surgery for the treatment of tremor in - Brain

Brain (2001), 124, 1576–1589
Stereotactic lesional surgery for the treatment oftremor in multiple sclerosisA prospective case-controlled study
S. H. Alusi,1 T. Z. Aziz,1 S. Glickman,2 M. Jahanshahi,3 J. F. Stein4 and P. G. Bain1
1Division of Neurosciences and Psychological Medicine, Correspondence to: Dr Peter Bain, Department ofImperial College School of Medicine, Charing Cross Neurology, Division of Neuroscience and PsychologicalHospital Campus, 2The Multiple Sclerosis Unit, North West Medicine, Imperial College School of Medicine, CharingLondon NHS Trust, Central Middlesex Hospital, Cross Hospital Campus, Fulham Palace Road, London3Department of Clinical Neurology Institute of Neurology, W6 8RF, UKLondon and 4University Department of Physiology, E-mail: [email protected] University, Oxford, UK
SummaryThe effect of stereotactic lesional surgery for the treatment one case. Two patients developed hemiparesis and in two
cases epilepsy recurred. Two surgical patients and oneof tremor in multiple sclerosis was examined in aprospective case-controlled study. Surgery was not control patient died between the 3 and 6 months
assessments. Both groups had a significant deteriorationundertaken in 33 patients (72% of 46 cases referred forstereotactic surgery), two of whom died within 4 months in EDSS but not Barthel ADL Index scores at 1 year, but
the difference between the groups was not significant.of referral. Twenty-four multiple sclerosis patients wereincluded in the study; 13 underwent surgery and were Similarly, no differences between the groups’ rates of
deterioration of speech or swallowing or MMS werematched against 11 controls on the basis of age, sex,expanded disability system scores (EDSS) and disease found. Significant improvements in contralateral upper
limb postural (P2) and kinetic tremors, spiral scores andduration. Assessments were carried out at baseline/preoperatively, and then 3 and 12 months later; these head tremor were detected at 3 and 12 months after
surgery (but not handwriting or nine-hole peg testincluded accelerometric and clinical ratings of tremor,spirography, handwriting, a finger-tapping test, nine-hole performance). Tremor-related disability and finger-
tapping speed were also significantly better 12 monthspeg test, tremor-related disability, general neurologicalexamination, Barthel Activities of Daily Living (ADL) after surgery, the latter having significantly worsened for
the control group. A 3 Hz ‘filter’ for postural (P2)Index of general disability, EDSS, a 0–4 ataxia scale, Mini-Mental State (MMS) examination, speech and swallowing upper limb tremor was detected by accelerometry/spectral
analysis above which tremor was always abolished and atassessments and grip strength. Postoperative MRI scansdemonstrated that tremor could be attenuated by lesions or below which some residual tremor invariably remained.
Criteria for selecting multiple sclerosis patients for thiscentred on the thalamus in seven cases, on the zonaincerta in five cases and in the subthalamic nucleus in form of surgery are discussed.
Keywords: tremor; frequency; multiple sclerosis; thalamotomy
Abbreviations: AC � anterior commissure; ADL � Activities of Daily Living; ANOVA � analysis of variance; EDSS �expanded disability system scores; FTT � finger-tapping test; MMS � Mini-Mental State; PC � posterior commissure;Vim � nucleus ventralis intermedius; Vop � nucleus ventralis oralis posterior
IntroductionAlthough, over the last 40 years, a considerable number of available for addressing the crucial questions: (i) What degree
of benefit can be expected from thalamotomy in terms ofstereotactic thalamotomies have been performed for thetreatment of tremor in multiple sclerosis, it is remarkable tremor suppression, functional gain and overall disability?
(ii) What is the optimal intracerebral target site for treatinghow little accurate information is available about the effectsof these procedures. In particular, there are very few data multiple sclerosis tremor? (iii) Does this form of surgery
© Oxford University Press 2001

Multiple sclerosis surgery 1577
adversely affect the natural history of the condition? (iv) that are present in patients referred for stereotactic surgery.Thus Nguyen and Degos proposed that a more effectiveWhat is the incidence of adverse effects when modern
stereotactic techniques are deployed? (v) Are there predictive target for alleviating multiple sclerosis tremor might benucleus ventralis oralis posterior (Vop) (Nguyen and Degos,markers or criteria that can aid patient selection? This study
attempts to address these issues. 1993).Consequently, in order to examine the efficacy ofIn most cases, the action tremors present in patients with
multiple sclerosis respond poorly to medication (Alusi et al., stereotactic lesional surgery for alleviating arm tremor inmultiple sclerosis and to assess its influence on disease1999). Consequently, stereotactic surgery has been performed
for multiple sclerosis patients with incapacitating tremors. progression, a prospective case-controlled study was carriedout.However, current knowledge of this form of surgery is based
predominantly on retrospective studies and reports, whichhave shown highly variable results: thalamotomy is reported
Patientsinitially to alleviate contralateral limb tremor in 65–96% oftremulous multiple sclerosis patients, although tremor is Ethicsnoted to return in ~20% of patients within 12 months. Approval was obtained for this study from the RiversideFunctional improvement of the relevant arm is estimated to Ethics Committee and informed consent obtained from alloccur in only 25–70% of multiple sclerosis patients after the subjects included in it. Forty-six tremulous multiplethalamotomy (Cooper, 1960; Broager and Fog, 1962; sclerosis patients were referred to the tremor clinic at CharingKrayenbuhl and Yasargil, 1962; Speelman and Van Manen Cross Hospital from February 1996 to May 1999 for1984; Kandel and Hondcarian, 1985; Barnett et al., 1992; consideration of sterotactic surgery and, in every case, afterWhittle and Haddow, 1995; Haddow et al., 1997; Critchley consideration of medical treatments, their suitability forand Richardson, 1998; Hooper and Whittle, 1998). thalamotomy was assessed.Nevertheless, some patients were reported to regain theircapacity to eat and drink independently (Shahzadi et al.,1995). Head tremor was noted by Cooper to be improved by Patients excluded from the studythalamotomy in five out of six patients (Cooper, 1960). Surgery was not undertaken in 33 patients (72% of 46
The adverse effects caused by thalamotomy have not been referred cases). The excluded patients consisted of 10 males,measured and quantified accurately, although their reported 23 females; mean age: 43 years (range 26–72); mean diseaseincidence varies from 0 to 45% of cases in different series. duration: 12 years (range 2–29); mean duration of tremor:The most common complications are gait deterioration, 4 years (range 0.25–18). Two patients (4% of referred cases)hemiparesis and dysarthria, but epilepsy, sensory died within 4 months of referral, before they were assesseddisturbances, dysphagia and transient bladder disturbance, for surgery, and four others did not attend their assessments.confusion, depression, lethargy and somnolence have also The rest were not offered surgery for the following reasons:been described (Cooper, 1960; Samra et al., 1970; Van (i) seven patients declined surgery after the risks wereManen, 1974; Speelman and Van Mannen 1984; Barnett explained to them; (ii) disability was related mainly to headet al., 1992; Siegfried, 1993; Whittle and Haddow, 1995; tremor rather than upper limb tremor (five patients); (iii) theShazadi et al., 1996; Haddow et al., 1997; Hariz et al., 1998; upper limb movement disorder was caused predominantly byHooper and Whittle, 1998). other components of ataxia rather than tremor (two patients)
There have been no prospective studies evaluating the or was associated with profound sensory impairment (twoinfluence of thalamotomy on the progression of overall patients); (iv) good upper limb functional capacity could bedisability and handicap of tremulous multiple sclerosis obtained by using the less tremulous arm (two patients) orpatients, although this issue has been raised (Speelman and functional improvement had been achieved with medicationVan Manen 1984; Kandel and Hondcarian, 1985; Haddow (propranolol) (two patients); (v) the tremulous arm was tooet al., 1997; Critchley and Richardson, 1998). weak (MRC scale �4/5) in two patients or there was
The optimal intracerebral target location for the alleviation significant truncal weakness resulting in the patient beingof multiple sclerosis tremor is not defined adequately. In one bedridden and profoundly disabled (one patient); (vi) tremorstudy, peroperative stimulation of the coordinate location for was mild and did not justify the risks associated with surgicalnucleus ventralis lateralis of the thalamus, the classic target intervention at that stage (three patients); and (vii) thefor tremor suppression, failed to relieve tremor adequately multiple sclerosis action tremor had been exacerbated by(Whittle and Haddow, 1995). Furthermore, Hirai and prochlorperazine, which also caused a rest tremor componentcolleagues noted that lesions centred on the lower part of that disappeared when the drug was withdrawn (one patient).nucleus ventralis intermedius (Vim) needed to be large toalleviate kinetic tremor, particularly if the tremor was lowfrequency and high amplitude or involved proximal or widely Patients included in the study
All the patients included in the study fulfilled Poser’s criteriadistributed muscle groups (Hirai et al., 1983)—all of whichare characteristic of some types of multiple sclerosis tremor for the diagnosis of definite multiple sclerosis (Poser et al.,

1578 S. H. Alusi et al.
1983). Thirteen patients underwent unilateral stereotactic Holmes’ tremor. The following criteria apply to thistremor: (i) rest and intention tremor with irregularsurgery between March 1997 and May 1999 in order to relieve
arm tremor. Thirteen control multiple sclerosis patients, who presentation. In many patients, postural tremor is also present.The tremor is often not as rhythmic as other tremors; (ii)were matched to the surgical patients by age (�5 years),
sex, expanded disability system scores (EDSS) and disease slow frequency, usually �4.5 Hz; (iii) if the time when alesion occurred can be identified (e.g. a stroke), a variableduration (�5 years), were entered into the study. Two control
subjects withdrew from the study shortly after recruitment, delay (typically 4 weeks to 2 years) between that lesion andthe first appearance of tremor is typical of this tremor type.leaving a total of 24 participating patients.It has been labelled in the past under different names includingrubral tremor, midbrain tremor, thalamic tremor, myorythmiaand Benedikt’s syndrome (Deuschl et al., 1998).Medical treatment
Ten of the 13 patients who underwent surgery had beentreated previously with propranolol (dose range 80–240 mgper day), one of the remaining three patients had asthma (a Assessments
A clinical and in particular a tremor history was obtainedcontraindication to the drug’s use) and the others declinedmedical treatment. Propranolol produced considerable from each of the 24 patients included in the study. They
were all assessed at baseline/preoperatively and at 3 and 12temporary benefit (for 4–6 months) in two patients. In afurther five cases, there was partial tremor suppression but months later. The tremor was assessed in three states of
muscle activity: rest, posture and movement. In the arms,tremor still compromised arm function, and in the remainingthree cases no benefit was obtained. Four patients had been tremor was assessed at rest and in two postures: (P1) with
the arms held outstretched and (P2) with arms in the ‘bat-treated with clonazepam (0.5–1.5 mg per day), which wasof little or no help to three of them and caused intolerable wing position’ (flexed at the elbows and the forearms pronated
with the fingers held near the nose). Upper limb kineticside-effects in the fourth. Isoniazid was administered to onepatient but without benefit. tremor (K) was assessed during a finger–nose–finger test.
Arm tremor severity was rated in each of these situations ona 0–10 scale (Bain and Findley, 1993; Bain et al., 1993a;Alusi et al., 2000). The upper limb postural tremors’Methods
A prospective case-controlled design was used in order to frequencies were recorded using EGAX-5-/L2M/MiMminiature accelerometers, using a technique previously(i) monitor the response of tremor and arm function to
thalamotomy over a 1-year period and (ii) compare the rates described (Bain et al., 1993a, b).The following tests, which previously have been shown toof multiple sclerosis disease progression in the surgical
patients with that of their matched controls who did not have be reliable and valid ways of measuring tremor in patientswith multiple sclerosis, were also performed: (i) a finger-any intervention.tapping test (FTT), in which the patient is asked to press akey on a calculator as many times as possible in 10 s(Worthington et al., 1989; Alusi et al., 2000); (ii) a nine-Definitions
The following definitions, published in a Consensus Statement hole peg test—results expressed as number of pegs insertedper second (Mathiowetz et al., 1985; Alusi et al., 2000); (iii)of the Movement Disorder Society (Deuschl et al., 1998),
were used to describe the various tremor components detected rating tremor from samples of the patients’ handwriting anddrawings of an Archimedes’ spiral were obtained and scoredin the patients.on a 0–10 clinical rating scale (Bain and Findley, 1993; Bainet al., 1993a, b; Alusi et al., 2000); and (iv) tremor-relatedRest tremor. This is a tremor present in a body part that
is not activated voluntarily and is completely supported disability, using a Tremor-Activities of Daily Living (ADL)Disability questionnaire (Bain and Findley, 1993; Bain et al.,against gravity (ideally resting on a couch).1993a; Alusi et al., 2000).
In addition, the following were also performed: (i) aAction tremor. This tremor is any tremor that is producedby voluntary contraction of a muscle. It includes postural, standard general neurological examination carried out on
every patient by one of the authors (S.H.A.) in order toisometric, kinetic and intention tremor: (i) postural tremor ispresent whilst voluntarily maintaining a position against establish their EDSS (Kurtzke, 1983); (ii) the Barthel ADL
Index of general disability (Collin et al., 1988); (iii) a (0–gravity; (ii) kinetic tremor is tremor occurring during anyvoluntary movement; and (iii) intention tremor or tremor 4) clinical scale from the dysmetria, dysdiadochokinesia,
dysarthria and gait ataxia (Alusi et al., 2000); (iv) the Mini-during target-directed movement is present when tremoramplitude increases during visually guided movements Mental State (MMS) examination (Folstein et al., 1975), the
results of which were expressed as a fraction of the maximumtowards a target at the termination of movement and thepossibility of position-specific tremor or postural tremor score physically achievable for that patient at the assessment;
(v) speech and swallowing: the former assessed by a (0–4)produced at the beginning and end of a movement is excluded.

Multiple sclerosis surgery 1579
Table 1 Lesion number, intended target coordinates (fromscale and the latter using a 150 ml swallowing test (amid-commissural point) and distance the electrode wasswallowing speed of �10 ml/s was taken to indicate abnormaladvanced from targetswallowing) (Nathadwarawala et al., 1992); and (vi) grip
strength—quantified using the Jaymar (Jackson, Mich., USA) Parameters Mean and rangehand-held dynamometer
Number of lesions 3 (2–7)AP coordinate 0.4 mm (–0.9 to 3)Lateral coordinate 13 mm (12–16)Outcome measures Vertical coordinate 1.94 mm (–0.50 to 3.6)
The study’s main outcome measures were (i) tremor severity Distance from target 7 mm (–0.5 to 13)in the operated arm (clinical rating of postural tremor P2,kinetic tremor, spiral drawing and handwriting scores), (ii)arm function in the targeted arm (FTT and nine-hole peg testscores, (iii) general disability (EDSS and Barthel ADL Indexresults) and (iv) tremor-related disability (measured by the and alcoholic chlorhexidine and just a few hairs shaved at
the point of entry. A 2.7 mm twist drill hole was made alongTremor-ADL Disability questionnaire). Other outcomemeasures were the severity of dysarthria, swallowing time the planned trajectory and the dura punctured with a biopsy
cannula, to minimize CSF leak and thus brain sag. Theand the MMS score.average collar and arc angles were 62.3° (range 48–75°) and11.9° (range 2–20°), respectively, with the frame appliedapproximately parallel to the orbital–meatal line. A 1.8 mmSurgical technique
Surgery was covered with a 3-day course of intravenous diameter electrode (5 mm exposed tip) was then passed totarget, and macrostimulation studies were performed whilstmethyl-prednisolone (1 g/day), commencing the day before
surgery. Preoperatively, under general anaesthesia, a T1- the patient’s neurological signs were examined. Observationsof the effects of macrostimulation on the (voltage) thresholdweighted MRI scan using a 3D-Turbo-FLASH sequence [TE
(echo time) 7 ms, (TR) repetition time 15 ms] and a Siemans for adequate tremor suppression led us (in some cases) tomove the electrode millimetre by millimetre along its1.5 T Magnetom Vision Scanner was performed and a
Cosman–Roberts–Wells (CRW©) head ring fixed to the trajectory from the intended target site to a mean of 7 mm(range –0.5 to 13 mm) beyond the calculated target alongpatient’s head. A stereotactic CT scan of the entire skull was
acquired using 3 mm contiguous slices and then the MRI and the trajectory of the electrode’s tract. Typically, tremorsuppression could be achieved at 100 Hz and 2–5 V (pulsestereotactic CT images were transferred to the StereoPlan©
(Radionics Inc.) workstation. The StereoPlan© software was width: 1 ms), and capsular responses could not be elicitedwith stimulation of �2 V at 2 Hz (pulse width: 1 ms).used for anatomic localization of the thalamic target
(Papanastassiou et al., 1998; Orth et al., 1999). Further Temporary lesions were placed by heating the electrode tipto 45°C for 60 s. Then, providing that the patient’s clinicalanatomic verification was performed with the AtlasPlan©
module of StereoPlan©. This co-registers the Schaltenbrand status was satisfactory, permanent lesions were induced byheating the electrode tip to 75°C for 90 s.and Wahren atlas to the patient’s scans using the anterior and
posterior commissures (AC and PC). The AtlasPlan© module The coordinates of the intracerebral targets and the distancethat the electrode was moved away from the target are showndisplays the target on the Schaltenbrand and Wahren atlas
images. in Table 1. All the patients had postoperative MRI scans toidentify the locations of the lesions.Targets within the thalamus are chosen relative to the AC–
PC line so that for multiple sclerosis tremor our chosen targetis located 10–14 mm lateral to the mid-commissural point(Vop) compared with placement 3–5 mm posteriorly in Vim. Statistics
A series of one-way analyses of variance (ANOVA) wereThe initial choice of Vop was based on our intraoperativeobservation that macrostimulation in the Vop region, rather used to assess change in the main outcome measures (postural
tremor P2, kinetic tremor, head tremor, spiral drawing,than more posteriorly in Vim, was more effective atsuppressing multiple sclerosis tremor—a finding supported handwriting and tremor-related disability) for the surgical
group from the baseline assessment to the short- (3 months)by the literature that has suggested that Vop might be a moreeffective target than Vim for suppressing multiple sclerosis and long (12 months) -term follow-up assessments. Group
differences in change in a number of pertinent outcometremor (Hirai et al., 1983; Nguyen and Degos, 1993; Whittleand Haddow, 1995). measures (FTT, nine-hole peg test, speech scale, swallowing
time, MMS, EDDS and Barthel ADL Index) were examinedPatients had an arterial line inserted so that systolicblood pressure was maintained 20 mmHg below preoperative with a series of two-way ANOVAs, with group (surgical
versus control patients) as the between-groups variable andvalues. Anaesthesia was then reversed. An entry point 1.0 cmanterior to the coronal suture and 2.0 cm lateral to the mid- time of assessment (baseline, and 3 and 12 months follow-
up) as the within-subject repeated measures factor. A prioriline was used. The patients’ hair was cleaned with aqueous
1580 S. H. Alusi et al.
Table 2 Summary of clinical details of surgical patients and their matched controls
Clinical features Surgical patients Control patients
Age (mean, years) 44.4 (range 34.2–53.3) 45.12 (range 33.1–50.9)Disease duration (mean, years) 13.3 (range 4–24) 18.6 (range14–28)EDSS (median) 8 (range 5.5–9) 7 (range 5–8.5)Barthel ADL Index (median) 8 (range 0–18) 7.25 (range 1–18)
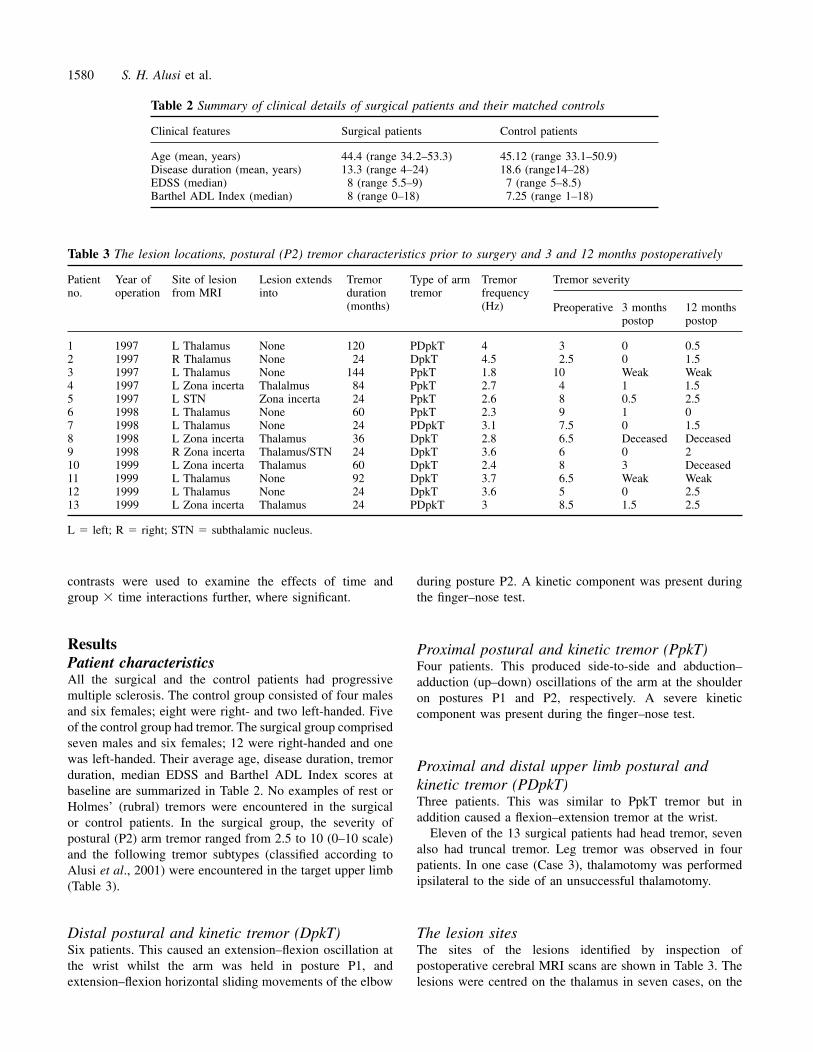
Table 3 The lesion locations, postural (P2) tremor characteristics prior to surgery and 3 and 12 months postoperatively
Patient Year of Site of lesion Lesion extends Tremor Type of arm Tremor Tremor severityno. operation from MRI into duration tremor frequency
(months) (Hz) Preoperative 3 months 12 monthspostop postop
1 1997 L Thalamus None 120 PDpkT 4 3 0 0.52 1997 R Thalamus None 24 DpkT 4.5 2.5 0 1.53 1997 L Thalamus None 144 PpkT 1.8 10 Weak Weak4 1997 L Zona incerta Thalalmus 84 PpkT 2.7 4 1 1.55 1997 L STN Zona incerta 24 PpkT 2.6 8 0.5 2.56 1998 L Thalamus None 60 PpkT 2.3 9 1 07 1998 L Thalamus None 24 PDpkT 3.1 7.5 0 1.58 1998 L Zona incerta Thalamus 36 DpkT 2.8 6.5 Deceased Deceased9 1998 R Zona incerta Thalamus/STN 24 DpkT 3.6 6 0 210 1999 L Zona incerta Thalamus 60 DpkT 2.4 8 3 Deceased11 1999 L Thalamus None 92 DpkT 3.7 6.5 Weak Weak12 1999 L Thalamus None 24 DpkT 3.6 5 0 2.513 1999 L Zona incerta Thalamus 24 PDpkT 3 8.5 1.5 2.5
L � left; R � right; STN � subthalamic nucleus.
contrasts were used to examine the effects of time and during posture P2. A kinetic component was present duringthe finger–nose test.group � time interactions further, where significant.
Results Proximal postural and kinetic tremor (PpkT)Patient characteristics Four patients. This produced side-to-side and abduction–All the surgical and the control patients had progressive adduction (up–down) oscillations of the arm at the shouldermultiple sclerosis. The control group consisted of four males on postures P1 and P2, respectively. A severe kineticand six females; eight were right- and two left-handed. Five component was present during the finger–nose test.of the control group had tremor. The surgical group comprisedseven males and six females; 12 were right-handed and onewas left-handed. Their average age, disease duration, tremor Proximal and distal upper limb postural andduration, median EDSS and Barthel ADL Index scores at
kinetic tremor (PDpkT)baseline are summarized in Table 2. No examples of rest orThree patients. This was similar to PpkT tremor but inHolmes’ (rubral) tremors were encountered in the surgicaladdition caused a flexion–extension tremor at the wrist.or control patients. In the surgical group, the severity of
Eleven of the 13 surgical patients had head tremor, sevenpostural (P2) arm tremor ranged from 2.5 to 10 (0–10 scale)also had truncal tremor. Leg tremor was observed in fourand the following tremor subtypes (classified according topatients. In one case (Case 3), thalamotomy was performedAlusi et al., 2001) were encountered in the target upper limbipsilateral to the side of an unsuccessful thalamotomy.(Table 3).
Distal postural and kinetic tremor (DpkT) The lesion sitesThe sites of the lesions identified by inspection ofSix patients. This caused an extension–flexion oscillation at
the wrist whilst the arm was held in posture P1, and postoperative cerebral MRI scans are shown in Table 3. Thelesions were centred on the thalamus in seven cases, on theextension–flexion horizontal sliding movements of the elbow

Multiple sclerosis surgery 1581
Fig. 1 Postoperative cerebral MRI scans showing examples of (A) a thalamotomy; (B) a lesion in the zona incerta and (C) a subthalamiclesion.

1582 S. H. Alusi et al.
Table 4 Means and standard deviations (given in parentheses) of the outcome measures at baseline, 3 and 12 months forthe surgical and control groups
Outcome measure Baseline 3 months 12 months
Surgery Control Surgery Control Surgery Control
No. of finger taps in 10 s 8.6 (12.3) 23.8 (13.2) 12.1 (12.8) 21.4 (14.1) 14.6 (13.4) 17.4 (16.6)Nine-hole peg test (pegs/s) 0.06 (0.12) 0.13 (0.13) 0.08 (0.11) 0.11 (0.12) 0.06 (0.10) 0.10 (0.12)Speech 0–4 scale 1.6 (0.94) 1.2 (0.69) 1.9 (0.74) 1.0 (0.87) 1.9 (0.98) 1.3 (0.69)Swallowing time (s) 43.6 (34.7) 19.9 (16.4) 41.2 (41.5) 24.6 (15.6) 56.3 (42.21) 24.9 (17.9)MMS 0.95 (0.60) 0.86 (0.11) 0.86 (0.16) 0.86 (0.14) 0.86 (0.15) 0.87 (0.11)EDSS 7.5 (1.3) 7.2 (1.3) 7.8 (1.2) 7.4 (1.2) 8.2 (1.2) 7.8 (1.5)Barthel ADL Index 8.2 (6.7) 10.9 (7.5) 8.1 (7.3) 11.4 (7.4) 7.5 (6.6) 10.7 (7.9)Grip strength (kgF) 19.4 21.1 16.1 19.0 15.7 16.7
zona incerta in five cases and in the subthalamic nucleus in Effect on speech and swallowingone case (see Fig. 1A–C for examples). Twelve of the surgical patients (92%) and eight of the
control patients (73%) had evidence of dysarthria on the 0–4 dysarthria scale at their baseline assessment. Ten of the
Adverse effects and complications surgical (77%) and five control patients (45.5%) had abnormalSeveral patients were noted to develop profound transient swallowing time at baseline (Table 4). No significantglobal weakness, lasting for a couple of minutes, as the difference between the two groups’ rates of deterioration oflesioning electrode was heated to 75°C—a vivid form of either speech [group, F(1,16) � 2.67, P � 0.122; time,Uhtoff’s phenomenon. Two patients suffered adverse effects F(2,32) � 0.94, P � 0.401; group � time, F(2,32) � 2.18,at the time of surgery. These were not caused by intracerebral P � 0.130] or swallowing [group, F(1,12) � 2.76, P �haemorrhage. The first (Case 3), who had an ipsilateral 0.121; time, F(2,26) � 1.16, P � 0.330; group � time,thalamotomy 10 years previously, developed worsening of F(2,26) � 0.68, P � 0.514] was detected over the 12-monthdysarthria and a contralateral hemiparesis that persisted. period of the study.The second (Case 11) developed severe drowsiness and acontralateral hemiparesis that initially resolved, until she hadseizures, after which a permanent hemiparesis and a mixed Speechreceptive and expressive dysphasia became apparent. This Three patients (23%) reported a transient deterioration ofwas one of two patients (Cases 7 and 11) with a past speech after surgery and two (15%) complained of permanenthistory of epilepsy, and seizure recurrence developed in both worsening of speech at 1 year. The trend towards deteriorationafter surgery. in the mean dysarthria scores from baseline to the 3 and 12
Six of the 13 patients (46%) reported worsening fatigue months assessments are shown in Table 4 for both the surgicalthat lasted for between 3 and 12 weeks postoperatively. Three and control patient groups, but this was only statisticallypatients (23%) had transient worsening of bladder function significant for the surgical cases at the 3-month assessmentlasting up to 1 month and one required permanent (t � 2.18, P � 0.044).catheterization after surgery. (Five patients had an indwellingcatheter prior to surgery and therefore change could not beidentified without further investigation.) Bowel function was
Swallowingsaid to worsen in one patient who had severe dysfunction priorDeterioration in swallowing after surgery was noted by twoto thalamotomy. Three patients (23%) reported depressionpatients, being transient in one and permanent in the other.postoperatively, which responded to antidepressant treatmentObjectively, both groups showed a trend towards deteriorationin two of them. The remaining patient had a severe recurrencein their swallowing time at 12 months. The mean swallowingof depression, leading to suicide.time of the surgical group deteriorated by 30% whilst thatof the control group deteriorated by 17% from their baselinevalues at 12 months (not statistically significant) (Table 4).Grip strength
Two surgical patients with hemipareses had markeddeterioration in grip strength postoperatively. However,although there were trends towards reduced grip strength for Effect on cognitive function
The mean baseline, 3 and 12 months postoperative MMSboth the surgical and control patient groups over the studyperiod, these were not statistically significant (Table 4). scores are shown in Table 4. Although there was a gradual

Multiple sclerosis surgery 1583
Fig. 3 The reduction in postural (P2) tremor severity afterthalamotomy. The error bars represent the 10–90% and boxes the25–75% percentiles.
scores across the two groups at 3 (t � 2.17, P � 0.041) and12 months (t � 2.49, P � 0.021) relative to the baselineassessment. This deterioration in EDSS scores was presentacross the two groups, and the rate of deterioration was notdifferent in the two groups as shown by the fact that thegroup � time interaction was not significant. Figure 2illustrates the changes in the Barthel ADL Index over the12-month study for each surgical and control patient.
MortalityFig. 2 The change in Barthel ADL Index scores for the control
Two surgical and one control patient died between 3 and 6patients (top) and the surgical patients (bottom) at 12 monthsmonths after their baseline assessments (χ2; not significant).from baseline. Please note that in A, control patient no. 8 diedThe causes of death were aspiration pneumonia andand, in B, surgical patients nos 8 and 10 died and thus were not
scored. A positive value indicates worsening scores; a negative depression/suicide in the surgical patients, and septicaemiavalue indicates improvement. from pyelonephritis in the control patient.
Beneficial effectsdecline in the mean MMS scores of the surgical but notcontrol group over the 12 months, the differences between Tremor relief
The surgical patients’ median postural (P2) tremor scores atthe two groups were not significant at the 5% level [group,F(1,13) � 0.21, P � 0.652; time, F(2,26) � 1.67, P � baseline, 3 and 12 months are shown in Fig. 3. Eleven of
the 12 living surgical patients had a �60% reduction in their0.208; group � time, F(2,26) � 2.89, P � 0.073]. Formalneuropsychological assessments were also undertaken postural (P2) arm tremor severity scores at 3 months, although
two of them had marked hemiparesis resulting in a weak(M. Jahanshahi and colleagues, unpublished results).non-tremulous arm (Table 3). One patient died a week beforethe 3-month assessment.
The relationship between preoperative postural (P2) tremorEffect on disease progression at 1 yearThe mean scores for the Barthel ADL Index and the EDSS frequency and complete suppression of arm tremor at 3
months is interesting: discounting the three patients whoat baseline, 3 and 12 months are shown in Table 4. Therewas no significant change in the Barthel ADL Index scores had either died or developed hemiparesis by the 3-month
assessment, all five patients who had complete tremorfor either group at either time interval [group, F(1,16) � 0.88,P � 0.362; time, F(2,32) � 0.27, P � 0.768; group � time, suppression postoperatively [postural (P2) tremor scores of
0] had preoperative tremor frequencies �3 Hz, whilst allF(2,32) � 0.07, P � 0.928]. For the EDSS scores, while themain effect of group [F(1,20) � 0.60, P � 0.446] and the five who had residual tremor [postural (P2) tremor scores
0.5–3] after surgery had frequencies of �3 Hz (χ2; P � 0.01).group � time interaction [F(2,40) � 0.04, P � 0.965] werenot significant, the main effect of time [F(2,40) � 5.59, P � In the 11 postoperative patients still alive at their 12-month
assessments, postural (P2) tremor was still suppressed by at0.007] was significant. A priori contrasts showed that thelatter effect was due to significant deterioration of the EDSS least 60% in nine patients (although two had persistent

1584 S. H. Alusi et al.
Table 5 Mean and standard deviation scores (in hence scored 0 taps in 10 s, whilst all the controls completedparentheses) showing the significant improvement in the the FTT. The mean baseline scores for the dominant armtremor-related scores at 3 and 12 months in the surgical were 8.6 taps in 10 s (including those who scored 0) in thegroup surgical group compared with 23.8 in the control group.
The group � time interaction was significant [F(2,30) �Tremor assessment Baseline At 3 At 123.36, P � 0.48], whereas the main effects of group [F(1,15) �months† months†
2.20, P � 0.159] and time [F(2,30) � 0.07, P � 0.933]Postural tremor P2 score 6.4 (2.6) 0.4 (0.57)* 1.5 (0.98)* were not significant. The significant interaction was due to(0–10)
the fact that at 3 months there was no significant differenceKinetic tremor score (0–10) 7.3 (2.6) 1.7 (1.8) * 2.1 (2.2)*in the FTT scores within either group compared with baseline,Spiral score (0–10) 8.4 (2.2) 7.2 (3.0)* 6.9 (2.9)*
Handwriting score (0–10) 7.8 (3.2) 7.3 (3.1) 6.6 (3.1) whilst at 12 months the scores of the surgical patients hadTremor related ADL (%) 85.2 (10.7) Not 79.0 improved significantly relative to baseline whilst those of the
measured (14.1)* controls had deteriorated significantly (Table 4).Head tremor (0–10) 2.4 (2.4) 1.2 (1.9)* 0.70 (1.2)*
*Statistically significant change relative to baseline scores. The nine-hole peg test†Compared with baseline.At baseline, eight of the surgical patients and one controlwere unable to place a single peg in a hole (0 pegs/s). Theaverage scores were 0.06 pegs/s (for either arm) for thehemipareses) but had returned to at least 50% of baselinesurgical patients (including those who scored 0 pegs/s) andvalues in two patients. The reduction by surgery of the0.14 and 0.13 pegs/s in the dominant and non-dominantpostural (P2) tremor [time, F(2,18) � 39.9, P � 0.0001] andhands, respectively, of the controls (Table 4). By the 3-the kinetic tremor [time F(2,16) � 20.76, P � 0.0001]and 12-month assessments, six and five surgical cases,severity scores were significant at 3 (postural tremor, t �respectively, were still unable to place at least one peg (but5.48, P � 0.00003; kinetic tremor, t � 6.5, P � 0.00018)one patient had died by 3 months and two by 12 months).and 12 months (postural tremor, t � 5.41, P � 0.00042;The changes in the nine-hole peg test scores were notkinetic tremor, t � 4.9, P � 0.001) postoperatively relativesignificantly different for the surgical and control groupsto the baseline assessment (Table 5).[group, F(1,16) � 0.74, P � 0.403; time, F(2,32) � 0.24,There was also a significant postoperative improvement inP � 0.787; group � time, F(2,32) � 0.58, P � 0.568]tremor severity scored from spiral drawings [time F(2,18) �compared either with baseline or with each other (Table 4).6.8, P � 0.006; baseline versus 3 months, t � 2.57, P �
0.030; baseline versus 12 months: t � 3.14, P � 0.011] butnot handwriting [time F(2,18) � 2.22, P � 0.137] (Table 5). Tremor-related disabilityFive of the 11 patients with head tremor had tremor The surgical patients’ tremor-related disability scores obtainedsuppression postoperatively, which was maintained at 1 year. from the Tremor-ADL Disability questionnaire wereTwo patients reported worsening of their head tremor significantly improved at 12 months after surgery comparedpostoperatively, but this was not reflected in the objective with preoperative values [t (8) � 2.78, P � 0.024] (Table 5).tremor scores. For the surgical group as a whole, head tremor Nine of the 11 surgical patients alive after 1 year stated thatwas significantly improved [time F(2,18) � 5.99, P � 0.01], there was reduction in the relevant/target arm’s tremorboth 3 months (t � 2.2, P � 0.05) and 12 months (t � 2.98, magnitude, but function was worse in two cases because ofP � 0.015) after surgery. Surgery had no effect on tremor weakness (hemipareses). Two others reported that they hadseverity in the ipsilateral arm of any of the patients. derived no benefit from surgery. Thus seven out of 11 (64%)
patients noted a decrease in their tremor-related disability1 year after surgery.
Effect of lesion site on tremor severity In those who did benefit from surgery, the extent varied:Comparing preoperative scores with those at 3 months after two regained the use of the relevant arm for eating andsurgery, the mean postural (P2) tremor severity scores were drinking as well as other fine tasks such as writing shortreduced from 5.5 to 0.25 by lesions centred on Vop (n � 5), sentences; three were able to eat with a fork and hold afrom 6.3 to 1.1 by those centred on zona incerta (n � 4) and modified cup; and two were only able to regain gross functionfrom 8.0 to 0.5 by the subthalamic nucleus-centred lesion (which helped their carers to feed and dress them). Four of(n � 1) (ignoring the two hemiparetic and the deceased the patients asked for contralateral surgery to be performed.patients).
DiscussionThe study designArm function—FTT
At baseline, seven of the 13 surgical patients were unable to The natural history of multiple sclerosis is difficult to predictin individual patients, although male sex, presentation withperform the FTT with either arm despite good power, and

Multiple sclerosis surgery 1585
cerebellar and/or brainstem deficits and older age at disease disease progression because (i) all the patients in the surgicalgroup received prophylactic high dose methyl-prednisoloneonset are all associated with a worse prognosis (Weinshenker
et al., 1989). Thus it is difficult to provide adequate matching at the time of surgery; (ii) the EDSS, although a goodindicator of the natural history of multiple sclerosis (Kurtzke,in a case-controlled trial involving patients with this disease.
Nevertheless, Weinshenker and colleagues established 1983; Weinshenker et al., 1989; The European Study Groupon Interferon β-1b in secondary Progressive Multipleguidelines for selecting controls in this context and showed
that disease duration and degree of disability are the two most Sclerosis, 1998), probably lacks adequate sensitivity to changeover a 12-month period, especially in the later stages of theimportant factors to equilibrate (Weinshenker et al., 1991).
We attempted to match our surgical patients with control disease (Weinshenker et al., 1996); (iii) the Barthel ADLIndex is designed for assessing the degree of dependence,multiple sclerosis patients, using age, sex, disease duration
and EDSS as controlling factors (see Methods). The presence and thus improvements in hand function caused bythalamotomy will influence scores; (iv) the results do notof tremor was not a prerequisite for entry into the control
group. However, the EDSS of the controls was lower than rule out the possibility of a longer term negative effect; and(v) the study’s sample size may prevent detection of small,that of the surgical cases by an average of 0.5 points. The
probable reason for this is that patients with severe cerebellar but significant, effects. Even so, it would appear that anyputative negative influence of thalamotomy on diseasedeficits (e.g. tremor) reach a higher level of disability at an
earlier age than patients without these signs (Weinshenker progression is not as profound as previously suggested(Broager and Fog, 1962; Speelman and Van Manen, 1984).et al., 1996; Alusi et al., 2001). However, it is possible that
closer matching might have been achieved by controllingfor cerebellar deficits as well, but this would have posedconsiderable practical difficulties for patient recruitment. Adverse events
MortalityIn this study, stereotactic surgery was not associated with
The choice of outcome measures any intra- or postoperative death. However, over the 12-Selecting appropriate outcome measures for use in therapeutic month study period, one control and two surgical patients,trials involving multiple sclerosis patients is difficult (Rudick who had lesions centred on the zona incerta, died. In addition,et al., 1996; Wingerchuk et al., 1997). Nevertheless, we two out of 33 patients referred for surgery died withinassessed the efficacy of thalamotomy by studying the 4 months of referral, giving a total mortality rate of five out ofreduction of tremor severity, the gain in arm function and 57 patients (8.8%). Consequently, the prognosis for severelythe change in the patient-reported tremor-related disability tremulous multiple sclerosis patients is poor, irrespective ofusing measures that have established validity and reliability whether or not stereotactic surgery is performed.in tremulous multiple sclerosis patients (Alusi et al., 2000).Other more extensive functional scoring systems may haveprovided more detailed information but would need validation
Morbidityin tremulous multiple sclerosis patients prior to deploymentThis study demonstrates that there is significant morbidity(Hariz et al., 1998; Lyons et al., 1998; Schuurman et al.,associated with stereotactic lesional surgery for patients2000).with multiple sclerosis. Immediate adverse effects includedhemiparesis in two cases (15%), which occurred even thoughthe thalamic lesions were placed accurately, demonstrating
Does stereotactic surgery have serious adverse the functional vulnerability of demyelinated brain tissue.effects on the overall condition of multiple However, in one of these cases, a previous ipsilateral partially
misplaced thalamotomy had been performed. In addition,sclerosis patients?There is considerable concern that trauma may have a two cases (15%) had postoperative seizures; a higher
incidence than previously reported (Samra et al., 1970).negative influence on the progression of multiple sclerosis(Poser, 1987; Sibley et al., 1991; Sibley, 1993; Jellinek, Transient postoperative fatigue and worsening of bladder
function, typically lasting 3–12 weeks, were detected in six1994; Kurland, 1994), particularly as short-term exacerbationof the disease after neurosurgical intervention has been (46%) and three (23%) of the patients, respectively. However,
it is pertinent to note that five patients had an in-dwellingreported (Samra et al., 1970).In this study, no significant difference in the rate of disease urinary catheter prior to surgery, so that a more profound effect
could not have been determined without further investigation.progression, as reflected in the EDSS and Barthel ADLIndex, of the surgical patients compared with their controls Depression developed in three patients (23%) after surgery,
in two cases responding to treatment, but in another leadingwas found at either 3 months or 1 year. This result providessome reassurance to those involved in this form of surgery. to suicide. No significant differences between the surgical
and control groups were detected in the rate of deteriorationHowever, it is possible that the study failed to demonstratea real negative effect of stereotactic lesional surgery on of either speech or swallowing over the 12-month study

1586 S. H. Alusi et al.
period although speech did deteriorate 3 months after surgery; tremor from a median tremor severity value of 4 to 2it then stabilized to some extent so that at 12 months there (severe to mild tremor, respectively) on a 0–4 tremor scalewere no significant differences compared with baseline or (Schuurman et al., 2000). However, at the beginning of thisthe control group’s values (Table 4). study, our preferred target for alleviating multiple sclerosis
tremors had been the Vop of the thalamus, particularly as ourprevious experience with distal, single frequency, upper limbBeneficial effectsmultiple sclerosis tremor showed that lesions placed in theStereotactic lesional surgery was associated with tremorVop attenuated multiple sclerosis tremor (Liu et al., 2001).attenuation in every case, irrespective of whether the lesion
However, intraoperatively, we noted that tremorwas sited predominantly in the thalamus (n � 7), zona incertasuppression was achieved in some patients at lower(n � 5) or subthalamic nucleus (n � 1), indicating thatstimulation voltages more ventromedially and up to 13 mmlesions at any one of these sites may alleviate multiplebeyond the thalamic target along the trajectory of thesclerosis tremor (Table 3). However, irrespective of the lesionelectrode. Thus lesions were placed here and the sitessite, complete postural tremor suppression in the targetconfirmed on postoperative MRI scans (Table 3 and Fig. 1).arm was invariably evident 3 months after surgery if the
These findings led us to conclude that multiple sclerosispreoperative postural (P2) tremor frequencies were �3 Hz,tremors, particularly those with a proximal component, maybut total tremor suppression was never obtained withbe attenuated more easily by lesions in the subthalamic orpreoperative frequencies of �3 Hz (Table 3). This significantzona incerta regions than the thalamus. The anatomical reasonfinding has at least two possible explanations, namely that afor this is that both the medial globus pallidus and thelow (�3 Hz) frequency spectral peak may (i) originate fromcerebellar nuclei project not only to the thalamus, but alsotremor in more proximal muscles or (ii) indicate a differentcaudally to the upper brainstem, particularly to the fields ofunderlying tremorgenic mechanism; that in either case doesForel and the zona incerta above the red nucleus, and to thenot respond as well to stereotactic lesional surgery.pedunculo-pontine nuclei and reticular pontine nuclei belowIn this study, significant improvements in upper limbit. These areas contain many neurones whose dischargepostural (P2) and kinetic tremors and spiral drawings as wellcorrelates with activity of the proximal spinal and limb girdleas head tremor were detected at 3 and 12 months aftermuscles during reaching and locomotion, and their axonssurgery (Table 5), although tremor reappeared to some
degree by 12 months (Fig. 3). No significant postoperative cross over to the other side to project directly or indirectlyimprovement in handwriting was evident for the group as a to the ventromedial grey matter of the spinal cord thatwhole, although two patients regained the ability to write contains the motor neurones that control these muscles.short sentences. The results of upper limb function testing, Proximal tremor is mediated not by distal muscles that areusing the nine-hole peg test and FTT, showed that for finger controlled predominantly by thalamocortical circuits, buttapping there was a significant group by time interaction, so mainly by these paraspinal and limb girdle muscles which,that at 3 months there was no significant change in the finger- as Lawrence and Kuypers first showed, are controlled mainlytapping scores within either group but at 12 months the from areas in the medial part of the upper brainstemscores of the surgical patients had improved significantly (Lawrence and Kuypers, 1968). This probably explains whyrelative to baseline whilst those of the controls had lesions in the region of the zona incerta can alleviate proximaldeteriorated. The nine-hole peg test results showed no multiple sclerosis tremor, as they interrupt aberrant oscillatorysignificant change over the duration of the study for either activity in the cerebellar and basal ganglia outputs, whichthe surgical patients or the controls, although there was a cause this form of tremor.slight trend for the latter to deteriorate over the study period.Stereotactic surgery was also associated with significantimprovement in tremor-related disability (assessed using a Selection criteriavalidated Tremor-ADL Disability questionnaire) 1 year after Haddow and colleagues, having reviewed the literature, foundsurgery (Table 5), although good tremor suppression was not very little useful information about the criteria for selectingalways mirrored by improvement in specific arm functions tremulous multiple sclerosis patients for thalamotomy(e.g. writing) or disability, a finding that has been reported
(Haddow et al., 1997). However, in spite of variations in thepreviously (Speelman and Van Manen, 1984; Barnett et al.,
quality of previous studies and paucity of data about1992; Whittle and Haddow, 1995; Shahzadi et al., 1995). In
individual patients, they concluded that surgery benefitssummary, stereotactic surgery produced variable results, withthose patients who have stable tremors and relatively non-overall benefit occurring in seven of the 11 multiple sclerosisprogressive disease, a view taken by other authors in thispatients alive 1 year later.field (Broager and Fog, 1962; Barnett et al., 1992).
In addition, it has been stated that thalamotomy has aIs there an optimal surgical target for predominantly palliative role for those with severe axial and
proximal arm tremor (Kandel and Hondcarian, 1985; Whittlealleviating multiple sclerosis tremor?and Haddow, 1995) or those who suffer from associatedSchuurman and colleagues reported that lesions (n � 5) or
stimulation (n � 5) of the Vim decreased multiple sclerosis truncal ataxia, which may cause persistent instability of the

Multiple sclerosis surgery 1587
upper limb despite good tremor relief (Shahzadi et al, 1995; stimulation would be preferable to bilateral thalamotomies,as the latter are associated with high risks of producingAlusi et al., 1999). Furthermore, the presence of severe
arm incoordination/ataxia in a tremulous arm is likely to speech and swallowing deficits (Krayanbuhl and Yasargil1962; Samra et al., 1970; Andrew et al., 1982).undermine the benefit of tremor suppression, and patients
with marked weakness and/or significant sensory deficits arealso unlikely to regain functional capacity after thalamotomy.This moderation of benefit can be explained by the effect of Prolonging the benefit of surgerythe underlying ataxic disorder on arm function (Speelman The long-term immunological consequences of having anand Van Manen, 1984; Whittle and Haddow, 1995; Alusi electrode implanted in multiple sclerosis brain tissue are notet al., 1999). However, preoperative assessment of the severity yet known, although Nguyen and colleagues demonstratedof incoordination/ataxia in tremulous multiple sclerosis that the results of thalamic stimulation were similar to thosepatients is difficult, particularly in patients with proximal obtained historically by thalamotomy (Nguyen et al., 1998).tremors that may interfere with ataxia testing (Alusi et al., However, developments in disease-modifying agents may1999, 2000). In this regard, Liu and colleagues have shown, allow the benefits obtained by stereotactic surgery to beusing a computerized tracking task, that multiple sclerosis prolonged by minimizing the effects of disease progressionpatients with distal tremor and minimal ataxia (i.e. pure (Haddow et al., 1997).tremor, manifest as a single frequency peak on spectralanalysis in the frequency domain) obtained �50% tremorsuppression after Vop thalamotomy, but that those patients Conclusionwith multiple spectral peaks (indicating a complex ataxic This study demonstrates that stereotactic lesional surgery canmovement disorder) obtained �50% suppression of their provide benefit to a highly selected group of tremulousmovement disorder (Liu et al., 2001). This led Liu and multiple sclerosis patients by suppressing limb and, to acolleagues to speculate that pallidal surgery may be a more lesser extent, head tremor and thus improve tremor-relatedappropriate procedure for this latter group of patients. disability. Lesions centred on the Vop of the thalamus, zona
Our finding of a 3 Hz frequency ‘filter’ at or below which incerta or subthalamic nucleus can decrease upper limbstereotactic surgery did not abolish upper limb tremor may tremor magnitude. The detection of a 3 Hz postural tremorprovide a useful addition to the criteria for selecting tremulous frequency ‘filter’ at or below which upper limb tremor couldmultiple sclerosis patients for this form of surgery. However, not be abolished is intriguing and merits further study. Thisfurther studies are required to confirm this observation. type of surgery is associated with a high rate of morbidity,
In this study, we rejected the majority (77%) of the cases but this could be improved by more stringent selectionreferred for surgery. Nevertheless, in view of our data, we criteria, specifically excluding those patients with a previouswould now also exclude those patients with a previous thalamotomy or a history of epilepsy. Finally, we could notthalamotomy or a history of epilepsy. detect evidence demonstrating a negative influence of lesional
surgery on the rate of progression of this unpleasant disease,although the mortality rate for severely tremulous multiplesclerosis patients was 8.8% over the 12-month study,
Lesional surgery or deep brain stimulation for irrespective of whether or not surgery was performed.multiple sclerosis tremor?Deep brain thalamic stimulation has been advocated as analternative treatment to lesional surgery for tremors of various Acknowledgementsaetiologies including multiple sclerosis (Brice and McLellan, We would like to thank SEARCH and the Smith’s charities1980; Pollak et al., 1993; Nguyen et al., 1996; Geny et al., for funding this study, and the MRC for funding T.Z.A.1996; Tasker, 1998; Whittle et al., 1998; Schuurman et al.,2000). However, the results of a randomized controlled trialof Vim thalamotomy versus stimulation that included 10 Referencesmultiple sclerosis patients demonstrated that thalamic Alusi SH, Glickman S, Aziz TZ, Bain PG. Tremor in multiplestimulation was no better than thalamotomy at suppressing sclerosis [editorial]. J Neurol Neurosurg Psychiatry 1999; 66: 131–4.multiple sclerosis tremor and induced less improvement in
Alusi SH, Worthington J, Glickman S, Findley LJ, Bain PG.disability, although these differences were not statisticallyEvaluation of three different ways of assessing tremor in multiple
significant (Schuurman et al., 2000). Furthermore, adversesclerosis. J Neurol Neurosurg Psychiatry 2000; 68: 756–60.
effects were detected in two (of five) lesioned and three (ofAlusi SH, Glickman S, Worthington J, Bain PG. A study of tremorfive) stimulated patients, respectively, and included severein multiple sclerosis. Brain 2001: 124: 720–30.gait disturbance, arm ataxia and dysarthria. Nevertheless, we
take the view that if a bilateral procedure is being considered Andrew J, Fowler CJ, Harrison MJ. Tremor after head injury andfor treating multiple sclerosis tremor, bilateral deep brain its treatment by stereotactic surgery. J Neurol Neurosurg Psychiatry
1982; 45: 815–9.stimulation or possibly a unilateral lesion and contralateral

1588 S. H. Alusi et al.
Aziz TZ, Bain PG. A multidisciplinary approach to tremor [editorial]. Kandel EI, Hondcarian OA. Surgical treatment of the hyperkineticform of multiple sclerosis. Acta Neurol (Napoli) 1985; 7: 345–7.Br J Neurosurg 1996; 10: 435–7.
Bain PG, Findley LJ. Assessing tremor severity. London: Smith- Krayanbuhl H, Yasargil MG. Relief of intention tremor due toGordon; 1993. multiple sclerosis by stereotaxic thalamotomy. Confin Neurol 1962;
22: 368–74.Bain PG, Findley LJ, Atchison P, Behari M, Vidailhet M, Gresty M,et al. Assessing tremor severity. J Neurol Neurosurg Psychiatry Kurland LT. Trauma and multiple sclerosis. Ann Neurol 1994; 361993a; 56: 868–73. Suppl: S33–7.
Bain PG, Mally J, Gresty M, Findley LJ. Assessing the impact of Kurtzke JF. Rating neurologic impairment in multiple sclerosis: anessential tremor on upper limb function. J Neurol 1993b; 241: 54–61. expanded disability status scale (EDSS). Neurology 1983; 33:
1444–52.Barnett GH, Kinkel RP, Bashin C, Palmer J, Namey M, Rudick R.Stereotactic thalamotomy for intractable tremor in multiple sclerosis Lawrence DG, Kuypers HG. The functional organization of the[abstract]. Neurology 1992; 42 Suppl 3: 327. motor system in the monkey. Brain 1968; 91: 15–36.
Brice J, McLellan L. Suppression of intention tremor by contingent Liu X, Aziz TZ, Miall RC, Rowe J, Alusi SH, Bain PG, et al.deep-brain stimulation. Lancet 1980; 1: 1221–2. Frequency analysis of involuntary movements during wrist tracking:
a way to identify MS patients with tremor who benefit fromBroager B, Fog T. Thalamotomy for the relief of intention tremorthalamotomy. Stereotactic Funct Neurosurg. In press 2001.in multiple sclerosis. Acta Neurol Scand 1962; 38 Suppl 3: 153–6.
Lyons KE, Pahwa R, Busenbark KL, Troster AI, Wilkinson S,Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index:Koller WC. Improvements in daily functioning after deep braina reliability study. Int Disabil Stud 1988; 10: 61–3.stimulation of the thalamus for intractable tremor. Mov Disord
Cooper IS. Neurosurgical alleviation of intention tremor of multiple 1998; 13: 690–2.sclerosis and cerebellar disease. New Engl J Med 1960; 263: 441–4.
Mathiowetz V, Weber K, Kashman N, Volland G. Adult norms forCritchley GR, Richardson PL. VIM thalamotomy for the relief of the nine-hole peg test of finger dexterity. Occup Ther J Res 1985;the intention tremor in multiple sclerosis. Br J Neurosurg 1998; 12: 5: 24–37.559–62.
Nathadwarawala KM, Nicklin J, Wiles CM. A timed test ofDeuschl G, Bain P, Brin M. Consensus statement of the Movement swallowing capacity for neurological patients. J Neurol NeurosurgDisorder Society on Tremor. Ad Hoc Scientific Committee. Psychiatry 1992; 55: 822–5.[Review]. Mov Disord 1998; 13 Suppl 3: 2–23.
Nyguyen JP, Degos JD. Thalamic stimulation and proximal tremor.European Study Group on Interferon beta-1b in secondary
Arch Neurol 1993; 50: 498–500.progressive MS. Placebo-controlled multicentre randomised trial ofinterferon beta 1-b in treatment of secondary progressive multiple Nguyen JP, Feve A, Keravel Y. Is electrostimulation preferable tosclerosis. Lancet 1998; 352: 1491–7. surgery for upper limb ataxia? [Review]. Curr Opin Neurol 1996;
9: 445–50.Folstein MF, Folstein SE, McHugh PR. ‘Mini-Mental State’: apractical method for grading the cognitive state of patients for the Nguyen JP, Feve A, Cesaro P, Keravel Y. Long term follow-up ofclinician. J Psychiatr Res 1975; 12: 189–98. patients with multiple sclerosis and action tremor treated by thalamic
stimulation [abstract]. Mov Disord 1998; 13 Suppl 2: 132.Geny C, Nguyen JP, Pollin B, Feve A, Ricolfi F, Cesaro P, et al.Improvement of severe postural cerebellar tremor in multiple Orth RC, Sinha P, Madsen EL, Frank G, Korosec FR, Mackie RT,sclerosis by chronic thalamic stimulation. Mov Disord 1996; 11: et al. Development of a unique phantom to assess the geometric489–94. accuracy of magnetic resonance imaging for stereotactic localization.
Neurosurgery 1999; 45: 1423–31.Haddow LJ, Mumford C, Whittle IR. Stereotactic treatment oftremor due to multiple sclerosis. Neurosurg Q 1997; 7: 23–34. Papanastassiou V, Rowe J, Scott R, Silburn P, Davies L, Aziz T.
Use of the Radionics Image Fusion© and Stereoplan© programs forHariz GM, Bergenheim AT, Hariz MI, Lindberg M. Assessment oftarget localization in functional neurosurgery. J Clin Neurosci 1998;ability/disability in patients treated with chronic thalamic stimulation5: 28–32.for tremor. Mov Disord 1998; 13: 78–83.
Poser CM. Trauma and multiple sclerosis. An hypothesis. J NeurolHirai T, Miyazaki M, Nakajima H, Shibazaki T, Ohye C. The1987; 234: 155–9.correlation between tremor characteristics and the predicted volume
of effective lesions in stereotaxic nucleus ventralis intermediusPoser CM, Patty DW, Scheinberg L, McDonald WI, Davis FA,
thalamotomy. Brain 1983; 106: 1001–18.Ebers GC, et al. New diagnostic criteria for multiple sclerosis:guidelines for research protocols. Ann Neurol 1983; 13: 227–31.Hooper J, Whittle IR. Long-term outcome after thalamotomy for
movement disorders in multiple sclerosis [letter]. Lancet 1998;Pollak P, Benabid A-L, Gervason CL, Hoffmann D, Seigneuret E,352: 1984.Perret J. Long-term effects of chronic stimulation of the ventralintermediate thalamic nucleus in different types of tremor. AdvJellinek EH. Trauma and multiple sclerosis. Lancet 1994; 343:
1053–4. Neurol 1993; 60: 408–13.

Multiple sclerosis surgery 1589
Rudick R, Antel J, Confavreux C, Cutter G, Ellison G, Fischer J, Van Manen J. Stereotaxic operations in cases of hereditary andintention tremor. Acta Neurochir Suppl (Wien) 1974; 21: 49–55.et al. Clinical outcomes assessment in multiple sclerosis. [Review].
Ann Neurol 1996; 40: 469–79. Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W,Baskerville J, et al. The natural history of multiple sclerosis: aSamra K, Waltz JM, Riklan M, Koslow M, Cooper IS. Relief ofgeographically based study. 1. Clinical course and disability. Brainintention tremor by thalamic surgery. J Neurol Neurosurg Psychiatry1989; 112: 133–46.1970; 33: 7–15.Weinshenker BG, Rice GP, Noseworthy JH, Carriere W,
Schuurman PR, Bosch DA, Bossuyt PM, Bonsel GJ, van Someren Baskerville J, Ebers GC. The natural history of multiple sclerosis:EJ, de Bie RM, et al. A comparison of continuous thalamic a geographically based study. 4. Applications to planning andstimulation and thalamotomy for suppression of severe tremor. interpretation of clinical therapeutic trials. Brain 1991; 114: 1057–67.N Engl J Med 2000; 342: 461–8.
Weinshenker BG, Issa M, Baskerville J. Long-term and short-termoutcome of multiple sclerosis. A 3-year follow-up study. ArchShahzadi S, Tasker RR, Lozano A. Thalamotomy for essential andNeurol 1996; 53: 353–8.cerebellar tremor. Stereotact Funct Neurosurg 1995; 65: 11–7.
Whittle IR, Haddow LJ. CT guided thalamotomy for movementSibley WA . Physical trauma and multiple sclerosis [editorial]. disorders in multiple sclerosis: problems and paradoxes. Acta[Review]. Neurology 1993; 43: 1871–4. Neurochir Suppl (Wein) 1995; 64: 13–6.
Sibley WA, Bamford CR, Clark K, Smith MS, Laguna JF. A Whittle IR, Hooper J, Pentland B. Thalamic deep-brain stimulationprospective study of physical trauma and multiple sclerosis. J Neurol for movement disorders due to multiple sclerosis [letter]. LancetNeurosurg Psychiatry 1991; 54: 584–9. 1998; 351: 109–10.
Wingerchuk DM, Noseworthy JH, Weinshenker BG. ClinicalSiegfried J. Therapeutic stereotactic procedures on the thalamus foroutcome measures and rating scales in multiple sclerosis trials.motor movement disorders. Acta Neurochir (Wien) 1993; 124: 14–8.[Review]. Mayo Clin Proc 1997; 72: 1070–9.
Speelman JD, Van Manen J. Stereotactic thalamotomy for the relief Worthington J, De Souza LH. A simple measurement of speed ofof intention tremor in multiple sclerosis. J Neurol Neurosurg index finger movement. Clin Rehabil 1989; 3: 117–23.Psychiatry 1984; 47: 596–9.
Tasker RR. Deep brain stimulation is preferable to thalamotomy for Received March 29, 2001. Revised March 29, 2001.Accepted April 5, 2001tremor suppression. Surg Neurol 1998; 49: 145–53.


















