Stem cells in ashermans syndrome Stem cells in...STEM CELLS IN REFRACTORY ASHERMAN SYNDROME Dr Neeta...
36
STEM CELLS IN REFRACTORY ASHERMAN SYNDROME Dr Neeta Singh, MD, FICOG, FCPS, FIMSA Professor Division of Reproductive Medicine Department of Obstetrics & Gynecology All India Institute Of Medical Sciences New Delhi , India
Transcript of Stem cells in ashermans syndrome Stem cells in...STEM CELLS IN REFRACTORY ASHERMAN SYNDROME Dr Neeta...

STEM CELLS IN REFRACTORY ASHERMAN
SYNDROME
Dr Neeta Singh, MD, FICOG, FCPS, FIMSA
Professor
Division of Reproductive MedicineDepartment of Obstetrics & Gynecology
All India Institute Of Medical Sciences New Delhi , India

INTRODUCTION
�Asherman syndrome (AS) an infrequent and complex gynecological abnormality due to damage to endometrium causing partial or complete obliteration of uterine cavity and/or cervical canal
�Symptoms- menstrual abnormalities (hypomenorrhoea or amenorrhoea), infertility and RPL
�Prevalence- 2% to 22% in infertile women
�Causes:� Invasive curettage most commonly of gravid uterus - 21.5 - 40%
� Trauma to non gravid uterus (diagnostic curettage - 1.6%, abdominal myomectomy - 1.3%, IUCD insertion - 0.2%)
� Infection - Genital TB, schistosomiasis
� Genetic predisposition
Yu D et al. Fertil Steril 2008

Treatment of AS
�Laparoscopic guided Hysteroscopic lysis of adhesions
�Placement of physical barriers in uterine cavity
�Estrogen supplementation to enhance endometrial proliferation
�Agents to increase vascular flow to endometrium (Vitamin E, L-arginine, sildenafil citrate)
�Recurrence rate for IUAs - 3.1% to 23.5% among all cases, 20-62.5% in those with severe adhesions
Tsui KH et al. Taiwanese J Obstet Gynecol 2014
BUT RECURRENT ADHESIVE DISEASE DESPITE ABOVE TREATMENT

�Thin endometrium despite treatment in AS – lower implantation and pregnancy rate
�Ongoing treatment for thin endometrium-� Intra-uterine granulocyte colony-stimulating factor
Persistent thin endometrium-
challenge to clinician
Promising treatment in poor endometrium- stem cell based therapies
� Intra-uterine granulocyte colony-stimulating factor
� Extended estrogen support
� Human chorionic gonadotropin priming in the follicular phase
� Drugs that increase endometrial blood flow (Pentoxyfilline tocopherol, sildenafil and l-arginine)

Pathophysiology
�Endometrium high capacity for self renewal- 400-500 cycles in reproductive life regulated by hormones
�Comparable to other high cellular turnover tissues – gut, epidermis, bone marrow
�Histologically endometrium has 2 layers�Histologically endometrium has 2 layers� Functional layer- responds to hormone, shed at menses
� Basal layer- regenerates mucosa
�Endometrium derived stem cells (EDRSCs) present in niche in basal layer – highly regenerative self renewal
AS – Absence of functional endometrium leads
to infertility

STEM CELLS
�Emerging role in regenerative medicine – treatment of tissue injury and fibrosis
�Stem cells - undifferentiated cells - potential to be multiplied in undifferentiated form (self renewal) and to mature and differentiated cells
�Self renewal and multi lineage differentiation – treatment of degenerative �Self renewal and multi lineage differentiation – treatment of degenerative disease
Potential of substituting damaged cells in the endometrium
�Multipotent and pluripotent stem cells beneficial paracrine effects -decrease cell death and provide growth/trophic support to host cells

STEM CELLS - TYPES
�Two types� Embryonic stem cells (ESCs) – origin from blastocyst
� Adult stem cells (ASCs)
�Both types can further differentiate into : Totipotent stem cells- totally undifferentiated, potency to produce whole embryonic germ � Totipotent stem cells- totally undifferentiated, potency to produce whole embryonic germ layers (ectoderm, endoderm, and mesoderm) such as zygote
� Pluripotent stem cells - end of a spectrum of differentiation, potential to generate all three germ layers cells, but not extraembryonic cells such as ICM of the blastocyst
� Multipotent stem cells can create variable but confined number of cell types limited to same lineage such as mesenchymal stem cells
� Unipotent stem cells stay restricted to the specific tissue and give rise to just one cell type

SourcesStem cells Source Properties
Bone marrow derieved stem cell (BMDSC)
Bone marrow Low quantity, ↓ differentiation with age
CD45 + Hematopoeitic progenitor stem cell (HPS)
Bone marrow Mesoderm in red bone marrow, umbilical cord blood, peripheral blood, cross bone marrow barrier
Human endometrial side population (hESP)
Endometrium Produce endometrial, endothelial, epithelial and stromal cellspopulation (hESP) stromal cells
Autologous adult stem cell Bone marrow Compensatory cells for generative tract
Mesenchymal stem cell (MSC) Adipose tissue Easy separation, plentiful proliferation, weakly immunogenic, large volume
Endometrial mesenchymal stem cell (eMSC)
Endometrium Multipotent, vastly proliferative, easily collected
Human endometrial stem cell (hESC)
Embryonic All three germ layers, limitless capacity
Human umbilical cord mesenchymal stem cell
Umbilical cord Best clinical tool, easy accessing, faster self renewal, HLA class 1 weakly expressed
Azizi R et al. Biomedicine and Pharmacotherapy. 2018

Mesenchymal stromal cells
Best option for cell/gene therapy and regenerative medicine in various tissues such as uterus -
� easy separation from various tissues
� plentiful proliferation capacity in vitro without any change in their � plentiful proliferation capacity in vitro without any change in their biological features
� injured tissues tropism
� weakly immunogenic
� secretion of anti-inflammatory molecules
� lowest hurt to normal cells/tissues

Endometrial Stem Cells (EnSCs)
�Prianishnikov (1978) for the first time introduced endometrial stem cells (EnSCs)
�Chan et al. isolated EnSCs from endometrial tissue in 2004
�Gargett et al. (2009) identified the extensive use of EnSCs in therapeutic �Gargett et al. (2009) identified the extensive use of EnSCs in therapeutic applications
�EnSCs – source of � Mesenchymal stem cells (MSCs)
� Epithelial stem cells (ESCs)
� Endometrial side population (ESP)
� Endometrial regenerative cell (ERC)

Endometrial Stem Cells (EnSCs)
� Properties� Self-renewal , high proliferative capacity
� Colony-forming unit activity
� capacity to differentiate into several cell types of mesodermal, ectodermal and endodermal originsendodermal origins
�Stem cells existing in endometrium might originate from bone marrow
�Bone marrow stem cells (BMSCs) might have important role in endometrial rebuilding
�Obstacle in BMSCs use – low quantity, ↓ differentiation potency with age, aggressive seclusion method

MECHANISM

PROCEDURE

PROCEDURE
�Stem cell isolation and identification by flow cytometry
�Intravenous or intrauterine (preferred) administration of stem cells
�Stem cells encapsulated in biomaterials such as hydrogels and scaffold to increase retention and survival
�New cells stick to ECM that provides suitable milieu for growth and �New cells stick to ECM that provides suitable milieu for growth and development
�ECM binds growth factors and restricts dissemination of stem cells


Endometrial regeneration using autologous adult stem cells followed by IVF in severe AS-
Case report
�Severe AS- curettage fb IUCD and cyclical hormonal therapy for 6 months failed
�Autologous stem cells isolated from bone marrow – endometrial angiogenic stem cells separated angiogenic stem cells separated
�Intrauterine instillation under USG guidance fb cyclical hormonal therapy
�Endometrial thickness reassessed- 8 mm good vascularity
�IVF-ET done- positive pregnancy
Nagori et al. J Hum Reprod Sciences 2011

STUDIES- ANIMAL AND HUMAN
Non uterine stem cells can regenerate endometrium
CD 45 cells migrate to endometrium in pregnancy
Mesenchymal origin can form Mesenchymal origin can form endometrium
Endometrial regeneration after xenografting in kidneyl
Cells deposited in cavity following curettage can reproduce endometrium
MSCs added to estrogenstimulate regenerationBMDSC functional role in regeneration

STUDIES- ANIMAL AND HUMANCollagen scaffolds support uterine
repair
Role in menstrual reconstruction
Immunomodulatory role by locating in endometrium
Clonogenic SUSD2+eMSCs recognised in regenerated
endometriumendometrium
Reduce fibrosis and enhance glandular count
Expression of ER and PR enhanced
Increased congestion of mature vessel and duration of menses
Increased endometrial thickness
Immunomodulatory role

CD133+ stem cells
�Bone marrow derived stem cells express biomarkers CD133/VEGFR2 –
subpopulation of cells with endothelial progenitor capacity (EPCs)
� Mobilised to peripheral circulation neoangiogenesis, healing, repair
� Can differentiate into non hematopoietic cell lineages� Can differentiate into non hematopoietic cell lineages
� Used in clinical trials in chronic total occlusion and ischemia, MI, hepatic fibrosis, liver
regeneration, bone regeneration - excellent safety profile
�CD133+ cells recently categorized as Advanced Therapy Medicinal Product
(ATMP) with regenerative properties
Santamaria X. Encyclopedia of Reproduction 2nd Edition, Vol 5. 2018

MOA

�Prospective, experimental, noncontrolled, open label study- 18 patients (30–45 yrs) with refractory AS or EA – 16 completed studywith refractory AS or EA – 16 completed study
�Recombinant human granulocyte colony stimulating factor (G-CSF) -10 mg/kg/day X 5 day
�Peripheral Blood Mononuclear Cells isolated by apheresis - CD133+ cells isolated
�Cells delivered into spiral arterioles by catheterisation
�Significant improvement in duration and intensity of menstrual period in first 3 months
�Statistically significant improvement in endometrial thickness
�Reproductive outcome- 3 patients spontaneous pregnancy, 7 pregnancy after ET

OUR EXPERIENCEOUR EXPERIENCE

�Prospective case series
�6 cases of refractory AS with failed standard treatment
�Resident endometrial stem or progenitor cells can be activated and bone marrow derived stem cells can be transplanted into uterine cavity for regeneration
�Mononuclear stem cells (MNCs) implanted in sub-endometrial zone followed by oral estrogen for 12 weeks
� ET was assessed at 3, 6, and 9 months

Contd…
�Procedure� Bone Marrow (30 ml) aspirated from iliac crest with BM aspiration
needle (Jamshidi, 11 G) in heparinized syringe
� Mononuclear cells (MNCs) isolation done by Ficoll density separation methodmethod
� MNCs suspended in 3 ml heparinized NS evaluated for viability (trypan blue dye), morphology and CD 34+ cells
� 3 ml of MNC injected in subendometrial zone at 2-3 sites (fundus, anterior and posterior part) under TVS guidance with ovum aspiration needle (17 gauge)
Singh N et al, J Hum Reprod Sci.2014 Apr-Jun; 7(2): 93–98

Singh N et al, J Hum Reprod Sci.2014 Apr-Jun; 7(2): 93–98
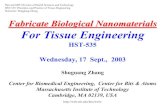
Contd..
�CD34+- endothelial progenitor cells that promote angiogenesis and tissue repair
� The correlation between no of MNC cells or CD 34+ cells and increase in ET was not significant.
Singh N et al, J Hum Reprod Sci.2014 Apr-Jun; 7(2): 93–98
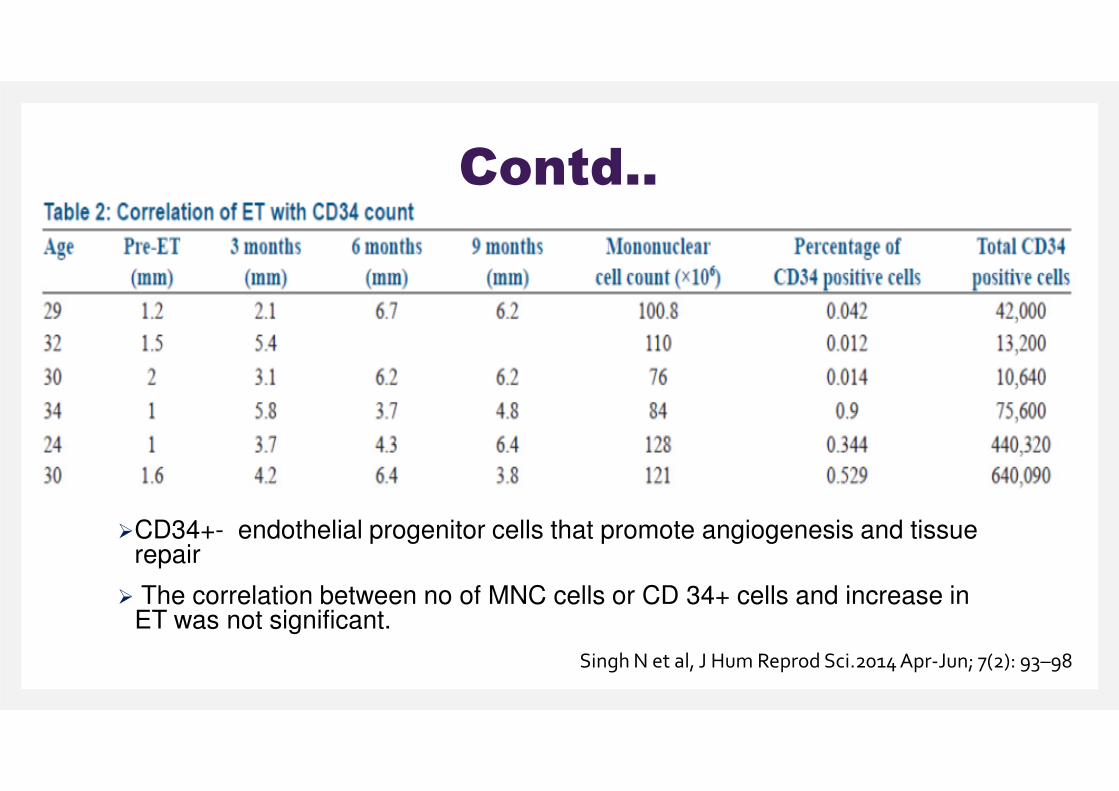
Contd..
�The maximum ET achieved by any patient was 6.7 mm
�1st study where adult stem transplant tried in patients of Asherman’s due to genital TBgenital TB
CONCLUSION
Autologous stem cell implantation- innovative therapy for endometrial
regeneration in AS. Since women resumed menstruation after implantation
this therapy holds promise for future fertility in these patients
Singh N et al, J Hum Reprod Sci.2014 Apr-Jun; 7(2): 93–98

Autologous bone marrow derived stem cell therapy for Asherman’s syndrome and endometrial atrophy:
5 year follow up study
�Prospective study - 25 women (24 -37 years) with Asherman’ssyndrome or endometrial atrophy after failed standard treatment
�Study duration: November 2011 and January 2013�Study duration: November 2011 and January 2013
�MNCs in 5 ml heparinized NS injected in uterine cavity through 6F pediatric foleys catheter and kept in situ for 36 hrs.
�Post procedure oral estradiol valerate tablets 2 mg thrice daily for 12 weeks
� ET and menstrual pattern assessed at 3, 6, and 9 months and at 5 years
UNPUBLISHED DATA. Singh N

Contd..Baseline characteristics Mean + SD/Percentage
Age (years) 29.6 + 4.1
BMI (kg/m2) 23.7 + 2.6
FSH (IU/ml) 6.5 + 2.3
LH (IU/ml) 5.1 + 2.8
Genital TB (%) 60
Baseline characteristics
Pre-ET ET at 3 months P value ET at 6
months P value ET at 9 months P value
3.33+ 1.03 5.15+ 1.93 0.001 5.61+ 1.56 0.164 6.14 + 1.75 0.135
Change in ET at 9 months follow up
UNPUBLISHED DATA. Singh N

Contd..Post stem cell treatment
AT 3 months (ET-6.6 mm)
Pre stem cell treatment endometrial
thickness of a patient (ET 3.3 mm)
(ET-6.6 mm)
AT 6 months (ET-6.8 mm)

Asherman syndrome
No Age Cause Preopmenstrual
history
Max preop
ET
Hysteroscopy Postop menstrual
history
Max postop
ET
Postop
4D USG
Pregnancy
outcome
Preop Postop
(5yrs)
1 29 C sec Amenorrhea 1.2 AS IV AS II Scanty 6.7 (6
months)
Tubular
cavityNo
2 34 D&C Amenorrhea 2.2 AS III - Normal 6.8 (9 Spontaneous 2 34 D&C Amenorrhea 2.2 AS III - Normal 6.8 (9
months)
Spontaneous conception, 38 wks, VD,
2750 gm
3 30 TB Amenorrhea 1.7 AS III AS II Scanty 6.4
(6 months)
Tubular
cavityNo
4 23 TB Scanty 3.3 AS I Normal Normal 7.4 (5 years) Normal No
5 30 TB Scanty 3.8 AS I Normal Normal 6.9 (6
months)Normal No
6 25 TB Amenorrhea 2.8 AS III AS III Scanty 4.4(5 years) Tubular
cavityNo

Asherman syndrome
7 24 D&C Amenorrhea 2.1 AS II Scanty 5 (9 mo)
Spont, 35 wks-CS, 2250 gm
8 32 TB Scanty 4.6 AS I - 6 mo- N, scanty at 9 mo
8.3 (9 mo)
No
No Age Cause Preopmenstrual
history
Max preop
ET
Hysteroscopy Postop menstrual
history
Max postop
ET
Pregnancy
outcomePreop Post op
at 9 mo (9 mo)
9 29 TB Scanty 3.7 AS I 3 months- N scanty at 6 and 9 mo
7.1 (6 mo)
No
10 30 TB Scanty 3.2 AS II Scanty 5.9 (9 mo)
No
11 24 TB Amenorrhea 2 AS II Amenorrhea 6.4 (6 mo)
No
12 30 TB Amenorrhea 3 AS IV Normal at 3 mo, scanty at 6, 9 mo
6.2 (9 mo)
No

Endometrial atrophyNo Age Cause Preop
menstrual
history
Max preop
ET
Hysteroscopy Postop menstrual
history
Max postop
ET
Pregnancy
outcomePreop Postop
(5yrs)
1 27 TB Scanty 3.6 Pale Scanty 6.1
(9 months)
2 yrs, ectopic,
salpingectomy
2 30 D&C Scanty 3.4 Pale scanty till 6 months then
7.8
(9 months)
4 yrs ,IVF conception, 34 months then
normal(9 months) conception, 34
wks, CS, 1500 gm
3 28 unknown Scanty 3.3 Pale Normal Normal 6.6 (9
months) No
4 35 D&C Scanty 3.5 Pale Normal Normal 7
(5 years) No
5 25 TB Scanty 4.1 Pale Normal Normal 9.3 (5 years) No
6 24 unknown Scanty 4.9 Pale Pale normal till 3 months then
scanty
8.8 (9 months) No

7 33 TB Scanty 3.5 Normal Normal scanty till 3 months then normal
12 (3 months)
no
8 38 TB Normal 2.5 Normal normal Normal 8.2 (5 years)
No
Endometrial atrophyNo Age Cause Preop
menstrual
history
Max preop
ET
Hysteroscopy Postop menstrual
history
Max postop
ET
Pregnancy
outcomePreop Postop
(5yrs)
8 38 TB Normal 2.5 Normal normal Normal(5 years)
9 30 CS Normal 4.2 Normal Normal Normal 6.4 (5 years)
No
10 37 unknown Normal 4 Pale Normal 6.3 (6 months)
No
11 34 CS Normal 4 Pale Normal 9.1 (6 months)
No
12 33 TB Normal 4.5 Normal Normal 7.5 (9 months)
No
13 28 TB Scanty 4.7 Pale normal till 3 months then scanty
5.6 (3 months)
No
RESULTS
�RESULTS� Majority of patients with amenorrhea resumed menses post stem cell
instillation (6 out of 7)
� Duration and intensity of menses - 20 patients with scanty or no menses progressively increased 3 and 6 months post therapy but declined at 9 progressively increased 3 and 6 months post therapy but declined at 9 months
� ET significantly increased after 3 months of therapy following which it plateaued
� 4 pregnancies achieved in 5 year follow up period. 2 conceived spontaneously and two through ART.
� 3 had a successful reproductive outcome and 1 was an ectopic pregnancy
UNPUBLISHED DATA. Singh N

CONCLUSION
�Regenerative medicine may play an important future role in the treatment of incurable infertility in AS
�Further studies are mandatory to better other important issues such as dosage, MoA and refining the protocol dosage, MoA and refining the protocol
�CD133+ cells as the first orphan drug designed (ODD) for the treatment of AS









![STEM CELLS EMBRYONIC STEM CELLS/INDUCED PLURIPOTENT STEM CELLS Stem Cells.pdf · germ cell production [2]. Human embryonic stem cells (hESCs) offer the means to further understand](https://static.fdocuments.net/doc/165x107/6014b11f8ab8967916363675/stem-cells-embryonic-stem-cellsinduced-pluripotent-stem-cells-stem-cellspdf.jpg)