STAT: Recognition and Management of Cardiac Emergencies
26
1 STAT: Recognition and Management of Cardiac Emergencies Anne Dabrow Woods, DNP, RN, CRNP, ANP-BC, AGACNP-BC Chief Nurse Wolters Kluwer Philadelphia, PA Acute Care Nurse Practitioner Critical Care Service, Penn Medicine, Chester County Hospital West Chester, PA Adjunct Faculty Drexel University, College of Nursing & Health Sciences Philadelphia, PA Copyright Anne Dabrow Woods; all rights reserved Disclosure: • I have nothing to disclose. Objectives: • At the conclusion of this session you will be able to: • Identify the etiology and pathophysiology of cardiac emergencies including: lethal dysrhythmias, hypotension, hypertension, cardiac tamponade, acute pulmonary edema, chest pain and acute coronary syndrome. • Identify the clinical signs and symptoms of a patient experiencing the selected cardiac emergencies. • Identify a treatment plan for the selected cardiac emergencies.
Transcript of STAT: Recognition and Management of Cardiac Emergencies

1
STAT: Recognition and Management of Cardiac Emergencies
Anne Dabrow Woods, DNP, RN, CRNP, ANP-BC, AGACNP-BC Chief Nurse
Wolters Kluwer Philadelphia, PA
Acute Care Nurse Practitioner
Critical Care Service, Penn Medicine, Chester County Hospital West Chester, PA
Adjunct Faculty
Drexel University, College of Nursing & Health Sciences Philadelphia, PA
Copyright Anne Dabrow Woods; all rights reserved
Disclosure:
• I have nothing to disclose.
Objectives:
• At the conclusion of this session you will be able to:
• Identify the etiology and pathophysiology of cardiac emergencies including: lethal dysrhythmias, hypotension, hypertension, cardiac tamponade, acute pulmonary edema, chest pain and acute coronary syndrome.
• Identify the clinical signs and symptoms of a patient experiencing the selected cardiac emergencies.
• Identify a treatment plan for the selected cardiac emergencies.

2
Chest Pain and Acute Coronary Syndrome
Etiology
• “Clot on Plaque”
Chest pain and ACS
• Chest pain
• Components of Acute Coronary Syndrome (ACS)
• Unstable angina (UA)
• Non-ST segment elevation myocardial infarction (NSTEMI)
• ST segment elevation myocardial infarction (STEMI)
• 3 reasons why treatment is delayed
• Onset of symptoms to patient recognition
• Older age, racial/ethnic issues, female gender, lower socioeconomic class, solitary living
• Delays in prehospital transport
• Delays with emergency evaluation
• Misinterpretation of patient data
• Inefficient system

3
Signs & Symptoms
• Chest discomfort • Angina
• “Squeezing” • Pain 20 minutes or less
• Myocardial infarction • “Heaviness or elephant on the chest” • Pain greater than 20 minutes
• Shortness of breath • Arm discomfort – often L arm • Pain in the jaw or teeth • Diaphoresis • Nausea • Vomiting • Dizziness
• Atypical symptoms: women, diabetes, elderly
Diagnostics
• 12 lead ECG
• Biomarkers
• Troponins – preferred over CK-MB
• Coagulation studies
• Chemistry
• CBC
• Risk stratification
• Braunwald
• Timi
• Cholesterol panel
Treatment
• Based on: • Clinical symptoms • Biomarkers • Risk factors • ECG
• Aspirin 160-325mg chewable • Oxygen for SpO2 < 94% • Nitroglycerin
• NTG SL – 1 every 5 minutes x 3; then drip • Contraindicated with PDE-5 inhibitors within 24 hours; 48 hours with
tadalafil (Cialis)
• Morphine – for chest pain unresponsive to nitrates • Beta-blocker – metaprolol 5 mg IV x 3 • No NSAIDS with STEMI
• Cause – increase risk mortality, reinfarction, HTN, heart failure, myocardial rupture

4
ECG changes
• Zone of Damage
• Ischemia – t wave inversion, ST segment depression
• Injury – ST segment elevation
• Infarction – Q waves (don’t occur in 30 to 50% MI’s)
• Location
• Inferior – II, III, aVF (RCA - R coronary artery)
• Lateral – I, aVL (Cx - circumflex)
• Anterior lateral – I, aVL, V5, V6 (LAD and Cx)
• Septal – V1 and V2 (LAD – L anterior descending)
• Anterior – V 3 and V4 (LAD)
ECG changes
Anticlotting agents…
• Heparin therapy
• UFH
• LMWH
• Glycoprotein IIb/IIIA inhibitors
• Abciximab (ReoPro) – during and after PCI with stent
• Eptifibatide (Integrilin) – used with UA, NSTEMI, PCI
• Tirofiban (Aggrastat) - NSTEMI
• Antiplatelet therapy – ADP receptor inhibitors
• Clopidogrel (Plavix) – prevent MI and CVA
• Prasugrel (Effient) – prevent ACS (UA, STEMI, NSTEMI)
• Ticagrelor (Brilinta) – prevent MI and CVA
• Evaluate for fibrinolysis therapy
• Evaluate for PCI

5
Acute Coronary Syndromes Algorithm.
Robert E. O'Connor et al. Circulation. 2010;122:S787-S817
Copyright © American Heart Association, Inc. All rights reserved.
Pulmonary edema
What is heart failure?
• HF is a complex clinical syndrome that results from any structural or functional impairment of ventricular filling or ejection of blood (HFSA, 2013)
• HF = pump issue
• HF types
• preserved ejection fraction (> 50%)
• reduced ejection fraction (< 40%)
• Borderline ejection fraction (41-49%)
• Characteristics
• Elevated cardiac filling pressures
• Inadequate peripheral oxygen delivery

6
Etiology: CO = HR x SV
Stroke volume
Preload
Contractility
Afterload
Heart rate
Pathophysiology
Renin-Angiotensin
System
Aldosterone System
Sympathetic Nervous System
Sympathetic Nervous System
Low blood volume or pressure recognized by baroreceptors (aorta, carotids)
Baroreceptors alert the brain
Brain signals the adrenals to produce epinephrine and norepinephrine
7
Sympathetic Nervous System
• Epinephrine and norepinephrine actions
• Beta-1 receptors - increased heart rate
• Beta-2 receptors - bronchodilation, vasodilation
• Alpha receptors – vasoconstriction and increase venous return
Renin-Angiotensin-Aldosterone System
Low blood volume through the kidneys
Kidneys produce renin
Renin converts angiotensinogen to angiotensin I
Angiotensin I converted to Angiotensin II in the presence of angiotensin converting enzyme (ACE)
RAAS
Angiotensin II activates receptors on blood vessels (angiotensin II receptors)
Vasoconstriction, increased BP, increased venous return to the heart

8
RAAS
• Aldosterone released from the adrenals in response to high angiotensin II and norepinephrine levels
aldosterone targets the kidneys
tubules retain water and sodium
increased blood volume and BP
Endothelial remodeling = Poor heart function/failure
Endothelial Remodeling
of the Heart
RAAS Action
Sympathetic Action
Aldosterone Action
Atherosclerosis, low Nitric Oxide
levels
Risk factors for HF
• CAD
• DM
• HTN
• Valve disease
• Alcohol
• Congenital heart defect
• Thyroid disease
• Age
• Obesity
• Reduced vital capacity
• Smoking
• LVH
• Sleep apnea

9
Pulmonary edema clinical presentation
• Tachypnea
• Dyspnea on exertion
• Acute shortness of breath/dyspnea
• Crackles
• Wheezes
• Frothy sputum
• Increase work of breathing
• Tachycardia
• Diaphoresis
• Chest pressure/pain
• Edema
Diagnostic studies
• 12 lead ECG
• Stat Chest X-Ray
• ABG
• BNP
• Cardiac enzymes – troponin and CPK, stat and serial enzymes
Pulmonary edema

10
Treatment
• High fowlers position
• Supplemental oxygen – keep SpO2 > 93%; PaO2 > 60 mm Hg
• Bipap (Inspiration/expiration pressure)
• Decrease afterload – vasodilator (Nitroglycerin), ACE inhibitor
• Decrease preload – loop diuretic (furosemide or bumetanide)
• Morphine
• Increase strength of contraction – positive inotropes
• Relieve cardiac ischemia
• Monitor intake/output
Cardiac Tamponade
Etiology
• Definition:
• Filling of the pericardial sac with blood causing an impairment in the heart’s ability to pump and a reduction in ventricular filling
• Causes
• Malignancy (30-60%)
• Uremia
• Idiopathic pericarditis
• Infection
• Anticoagulation
• Connective tissue diseases
• Postpericardiotomy syndrome or post MI (Dressler’s Syndrome)
• Any type of pericarditis – HIV (up to 24% of cases), infection, trauma, post PCI)

11
Presentation
• Beck’s triad
• Low blood pressure (or narrowed pulse pressure or difference between systolic and diastolic pressure)
• Jugular venous distention
• Muffled heart tones
• Dyspnea
• Tachycardia
• Tachypnea
• Cold and clammy extremities
Diagnostics
• CXR
• Water bottle shaped heart
• Echo – Gold standard
• CT Chest
• Lab tests
• Biomarkers (Troponin, CK)
• Chemistry
• CBC with diff
• Coagulation profile (PT/INR, PTT)
• Antinuclear Antibody
• ESR
• Rheumatoid Factor
• HIV titer
• PPD
Treatment
• Oxygen
• Volume – NSS or LR
• Inotropic support – milrinone or dobutamine (do not use dobutamine if hypotensive)
• Avoid high peep if on ventilator
• Emergent pericardiocentesis
• Intrapericardial catheter to closed drainage system
• 3 way stop cock
• Leave in place 24 to 48 hours
• Pericardial window – if re-accumulation is a concern

12
Lethal Dysrhythmias
ST is not a lethal dysrhythmia
• Sinus tachycardia
• Response to something going on physiologically
• Fever
• Hemorrhage
• Pain
Bradyarrhythmias
• Causes • Drug therapy: beta-blockers, Ca channel blockers, digoxin;
overdose
• Respiratory failure – hypoxia and hypercarbia
• Over sedation with narcotics and benzodiazepines
• Treatment – only for symptomatic bradycardia • Atropine
• 0.5 mg IV every 3-5 minutes up to 3mg maximum
• Dopamine • 2 – 10 mcg/kg/min
• Epinephrine • 2 – 10 mcg/min
• Consider pacing

13
Overdose
• Calcium channel blocker overdose • Atropine • Calcium gluconate
• 30 to 60 ml of a 10% solution; may repeat 4 times every 20 minutes
• Calcium chloride • 10 to 20 ml of a 10% solution over 10 minutes ; repeat up to 4 times every 20
minutes
• Glucagon
• 5 mg IV bolus; may repeat twice at 10 minute intervals • Causes nausea and vomiting
• Norepinephrine (Levophed) • Lipid emulsion therapy
• Beta blocker overdose • Glucagon • Lipid emulsion therapy • Insulin and dextrose
Tachyarrhythmias
• SVT
• Adenosine 6 mg IV followed by 12 mg IV in 1 to 2 minutes (give over 1-2 seconds)
• 20 ml NSS flush
• Give quickly
• Atrial fibrillation and atrial flutter – most commonly used drugs
• Diltiazem (cardizem)
• Metaprolol (lopressor)
• Amiodarone – if unknown ventricular function
Ventricular dysrhythmias
• Ventricular tachycardia
• With pulse
• Amiodarone 150 mg IV over 10 minutes followed by infusion
• Without pulse
• Amiodarone 300 mg IV followed by infusion
• Ventricular fibrillation • Amiodarone 300 mg IV followed by infusion
• Amiodarone infusion – 1.0 mg/minute for 6 hours and then 0.5 mg/min for 18 hours or until transitioned to oral dose

14
Hypotension
Recognizing Hypotension
• Definition – Systolic Blood Pressure (SBP) < 90 mm Hg or a mean arterial pressure (MAP) < than 70 mm Hg; or a SBP decrease > than 40 mm Hg or < than 2 SD below normal for age
• Clinical Presentation
• Asymptomatic
• Dizziness, lightheadedness
• Inability to think clearly
• Dry mucous membranes
• Anxiety
• Tachycardia
• Lethargy
• Confusion
• Low urine output
What Causes Hypotension?
• Drug therapy
• Narcotics
• Negative chronotropic or inotropic agents
• Antihypertensives
• Diuretics
• Heart related disorder
• Electrical issues – bradycardia, tachycardia
• Anatomical issues - cardiomyopathy
• Mechanical issues – heart failure (systolic or diastolic)

15
What Causes Hypotension?
• Acute blood loss
• Trauma
• GI Bleed
• Internal bleeding
• Third-space shift
• Shock
• Hypovolemic
• Septic
• Cardiogenic
• Anaphylactic
Keeping Fluid in the Right Compartment
• Body fluid composition (Total Body Water)
• Varies due to weight, height, and lean body mass
• Muscle has more water than fat
• Intracellular – 60% of TBW
• Potassium salts pull more water than total sodium salts in intracellular space
• Extracellular - 40% of total body water
• Intravascular (12% of extracellular TBW)
• Interstitial (80% of extracellular TBW)
• Transcellular – cerebrospinal fluid, pleural, peritoneal, synovial
Relative vs. Absolute Hypovolemia
• Absolute hypovolemia – measurable loss
• Hemorrhage
• Diarrhea
• High output fistulas
• Relative hypovolemia
• 3rd spacing, anasarca
• Ileus, intestinal obstruction
• Compartment syndrome
• Ascites
• Septic shock
• Fever

16
Crystalloid or Colloid, That is the Question
Crystalloid vs. Colloid Resuscitation
• Crystalloid and colloid solutions are considered equally effective for resuscitating patients
• Neither type of fluid provides survival benefit over another
• No difference in number of days spent in ICU, hospital stay, duration of mechanical ventilation or duration of renal replacement therapy
Normal Saline vs. Lactated Ringers
• Normal Saline (0.9%)
• Na: 154
• Cl: 154
• K: 0
• Ca: 0
• Mg: 0
• Buffers: 0
• pH: 5.6
• Osmolality: 295
• Lactated Ringers
• Na: 130
• Cl: 109
• K: 4
• Ca: 3
• Mg: 0
• Buffers: lactate 28 meq/L
• pH: 6.4
• Osmolality: 273

17
Choosing the Right Colloid
• 5% albumin • Oncotic pressure: 20 mm Hg • Change in plasma volume: 0.1 to 1.3 • Duration of effect: 16 hours
• 25% albumin • Oncotic pressure: 70 mm Hg • Change in plasma volume: 4.0 to 5.0 • Duration of effect: 16 hours
• (Halliwell 1988, Gen 1999, Moore 1995, Shires 1964, Weil 2004)
Patient Position
• Trendelenberg position – no longer recommended
Trendelenberg No More
• Passive leg raise position

18
Bring on the Fluids
• Volume resuscitation
• Crystalloids
• Boluses: 1,000 mL over 30 minutes
• NSS
• Lactated Ringers
• Colloids
• Boluses: 500 mL over 30 minutes
• Albumin • 500mL, 5%
• Packed RBCs • transfuse if Hb less than 7.0 g/dL
• target a hemoglobin of 7-9 g/dL
Vasopressor Therapy
• Should only be started when fluid resuscitation has been optimized
• Direct BP measurement with an arterial line
• Titrate to maintain MAP at a specified point
• Better to transfuse vasopressors through a central line to prevent extravasation
Dopamine
• Precursor to norepinephrine and epinephrine
• Mechanism of action • Dopaminergic effects (less than 5 mcg/kg/min) on the renal, mesenteric,
and coronary beds (Does not work this way in people, only in the lab) • Beta 1 adrenergic effects (5 - 10 mcg/kg/min) on the heart increasing
contractility and heart rate • Alpha 1 effects (10 - 20 mcg/kg/min) result in arterial vasoconstriction
• Undesirable effects
• Tachycardia, arrhythmias
• Dosage • 5 mcg/kg/min and titrate to MAP of 65 mm Hg or >, to max of 20
mcg/kg/min

19
Norepinephrine
• Alpha 1 adrenergic agonist, with a less Beta 1 adrenergic agonist effect
• Mechanism of action • More effect on efferent than afferent renal arterioles • Increases filtration fraction • Increases urine output, creatinine clearance • Optimizes renal blood flow and renal vascular resistance
• Dosage
• 1 mcg/min and titrate to MAP 65 mm Hg or greater
Phenylephrine
• Selective alpha 1 agonist
• Mechanism of action
• Increases MAP, systemic vascular resistance, cardiac index and stroke index
• Causes a reflex vagal stimulation due to the rapid rise in BP
• Dosage
• 20 to 200 mcg/min; titrate to MAP of 65 mm Hg or greater
Epinephrine
• Alpha 1 agonist; beta 1 and beta 2 agonist
• Mechanism of action
• Increases MAP, cardiac index, stroke volume, and heart rate
• Increases oxygen delivery and consumption
• Decreases splanchnic/gastric blood flow
• Increases lactate concentrations
• Dosage
• .02 to .5 mcg/kg/min and titrate to MAP of 65 mm Hg or greater

20
Vasopressin
• Peptide hormone synthesized in the hypothalamus and stored in the pituitary
• Mechanism of action
• Released in response to decrease in blood volume, decrease intravascular volume, and increased plasma osmolality
• Constricts vascular smooth muscle directly via V1 receptors
• increases responses of the vasculature to catecholamines
• Increase blood pressure by inhibiting vascular smooth muscle nitric oxide production
• Dose: 0.03 units/min
• Indication: used as an adjunct to norepinephrine
Dobutamine
• Positive catecholamine with inotropic and marginal vasodilator action
• Mechanism of action
• Increases the strength of myocardial contraction (Beta -1 action)
• Vasodilatory action (Beta – 2 action)
• Dosage
• 5 to 20 mcg/kg/min; titrate for hemodynamic effects
Hypovolemic Shock
21
Managing Hypovolemic Shock
• Volume resuscitation
• Crystalloids
• Boluses: 1,000 mL over 30 minutes
• NSS
• Lactated Ringers
• Colloids
• Boluses: 500 mL over 30 minutes
• Albumin
• 500mL, 5%
• Packed RBCs
• Transfuse if hemorrhagic shock
• transfuse if Hb less than 7 g/dL
• target a hemoglobin of 7-9 g/dL
Septic Shock
Pathophysiology of Sepsis

22
Managing Septic Shock
• Fluids, fluids, fluids
• Resuscitation goals
• CVP 8 – 12 mm Hg
• MAP greater than or equal to 65 mm Hg
• Urine output greater than or equal to 0.5 mL/kg/hr
• Central venous oxygen saturation greater than or equal to 70% or mixed venous greater than or equal to 65%
Managing 3rd Spacing
• Result of fluid shifting into the interstitial space
• Occurs within first hours to days following fluid resuscitation – capillary leak phenomenon
• Associated with hypoalbuminemia
• Best treatment is prevention – adequate nutrition
• Treatment
• Colloid with equal or greater oncotic pressure (25 or greater)
• Albumin 25% followed by loop diuretic
Anaphylactic Shock

23
The Picture of Anaphylaxis
Pathophysiology of Anaphylactic Shock
Managing Anaphylactic Shock
• Etiology: exposure to antigen leads to airway constriction and hypotension (vasodilatation, and capillary fluid leakage)
• Treatment: • ABC’s • Epinephrine: IM (anterolateral thigh); .03mL (1:1,000); IV infusion if
needed • Crystalloids • Norepinephrine if crystalloids ineffective • Glucagon – 1mg IM or IV (endogenous catecholamine release) • Antihistamines (H1 blockers) and H2 blockers (famotidine) • Bronchodilators • Steroids – methylprednisolone 1-2mg/kg IV Q6 hours
• Prevention • Epipen - 2 • Liquid antihistamines – H1 and H2 blockers • Med alert bracelet
24
Cardiogenic Shock
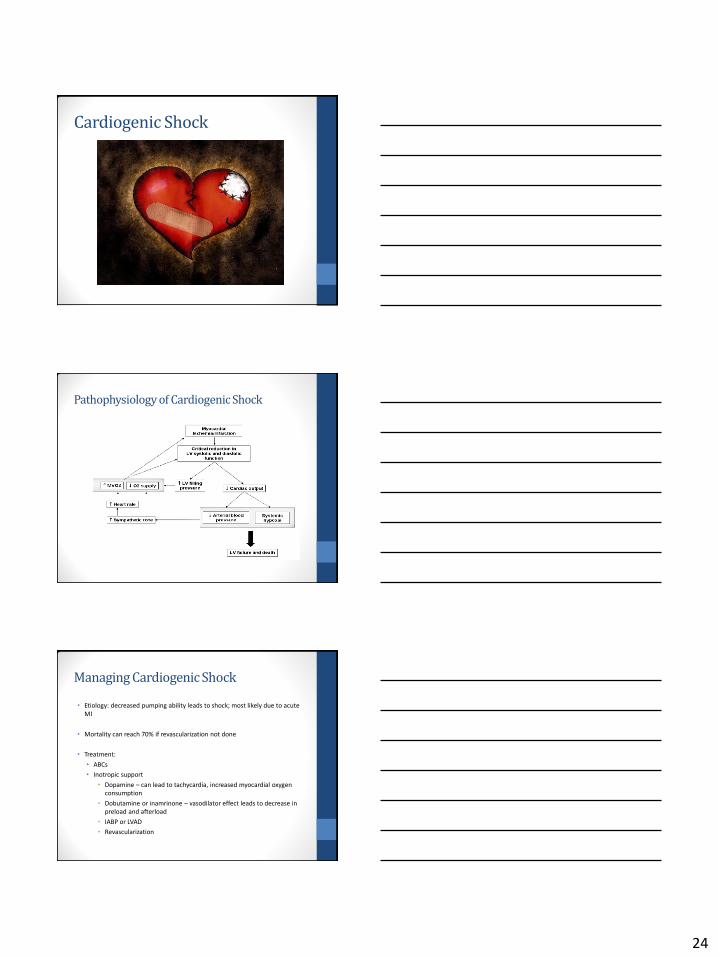
Pathophysiology of Cardiogenic Shock
Managing Cardiogenic Shock
• Etiology: decreased pumping ability leads to shock; most likely due to acute MI
• Mortality can reach 70% if revascularization not done
• Treatment:
• ABCs
• Inotropic support
• Dopamine – can lead to tachycardia, increased myocardial oxygen consumption
• Dobutamine or inamrinone – vasodilator effect leads to decrease in preload and afterload
• IABP or LVAD
• Revascularization
25
Hypertensive Urgencies and Emergencies
Definitions
• Hypertensive Urgency – BP > 180/120 mm Hg but no signs of end organ damage
• Hypertensive Emergency – BP > 180/120 mm Hg with signs of end organ damage
Hypertensive Urgency
• Goal • Reduce BP to 160/100 mm Hg but, the MAP should not be
lowered by more than 25 to 30% over the first several hours
• Treatment • Dark, quiet room
• First choice drug therapy • Furosemide 20 mg oral
• Clonidine 0.2 mg
• Captopril 6.25 mg to 12.5 mg
• Follow up drug therapy • Diruetics (hydrochlorothiazide)
• ACE inhibitors (captopril)
• Calcium channel blockers (norvasc)

26
Hypertensive Emergency
• MAP should be reduced gradually by 10-20% in the first hour
• Reduce MAP another 5 to 15% over next 23 hours
• Drug therapy
• Nitroglycerin infusion – reduces preload
• Nipride infusion – reduces afterload (needs arterial line)
• Nicardipine (Cardene) (Ca blocker)
• Infusion – start at 5 mg/hr and titrate to maximum of 15 mg/hr
• Labetalol (alpha and beta blocker)
• 20 mg iv followed by 20-80 mg every 10 minutes to a total dose of 300 mg. Infusion rate is 0.5 to 2 mg/min
• Hydralazine IV - 10 mg IV q 6 to 8 hours
• Enalapril IV – 1.25 mg IV q 6 hours
References • Barkley, T., & Myers, C. (2015). Practice Considerations for Adult-Gerontology Acute Care Nurse Practitioners, Vol. 1. Barkley & Associates:
West Hollywood, CA.
• Burnham, E., Janssen, W., Riches, D., Moss, M., Downey, G. (2014). The fibroproliferative response in acute respiratory syndrome:
Mechanisms and clinical significance. European Respiratory Journal, 43(1): 276-285.
• Camargo, C., Rachelefsky, G., & Schatz, M. (2009). Managing asthma exacerbations in the emergency department. Proceedings American Thoracic Society; (6), 357-366.
• Caironi, P. et al. Albumin replacement in patients with severe sepsis or septic shock.NEJM, 2014. 370:1412-1421.
• DeCramer, M., & Vestibo, J. (2014). Global initiative for Chronic Obstructive Pulmonary Disease.
• File, T. (2016). Treatment of communicty-acquired pneumonia in adults who require hospitalization. UptoDate.
• Kaynar, A., & Pinsky, M. (2015). Respiratory failure; Medscape; updated April 1, 2015.
• Jaff, M., & McMurtry, S. (2011). Management of massive and submassive pulmonary embolism, ileofemoral deep vein thrombosis, and chronic thromboemobolic pulmonary hypertension. Circulation, (123), 1788-1830.
• Coons, James, Seidl, Edward, Cardiovascular pharmacotherapy update for the intensive care unit; Critical Care Nursing Quarterly, Vol. 30, No. 1.
• Dellinger, R. Phillip, Levy, M. Rhodes, A. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2013. Critical Care Medicine, 2013. 41(2): 580-627.
• Hollengerg, S., Ahrens, T., Annane,D. et al: Practice parameters for hemodynamic support of sepsis in adult patients; Critical Care Medicine, 2004, Vol. 32, No. 9.
• Mandell, L., & Wunderlink R. (2007). Infectious Disease Society of America/American Thoracic Society Consensus guidelines on the
management of community-acquired pneumonia in adults. Clinical Infectious Disease. Suppl. 2:s27.
• NAEPP (2016). National Asthma Education and Prevention Guideline. • Napolitano, Lena, Kurek, Stanley, Luchette, Fred, et al; Clinical practice guideline: Red blood cell transfusion in adult trauma and critical
care. Critical Care Medicine 2009, Vol. 37, No. 12. • Porter, JM, Ivatury RR, In search of the optimal end points of resuscitation in trauma patients. Journal of Trauma. 1998, Vol. 44.
• Singh, A., Carlin, B. Shade, D., Kaplan, P.; The use of hypertonic saline for fluid resuscitation in sepsis; Critical Care Nursing Quarterly, Vol. 32, No.1.
• Stevens, W.; Fluid balance and resuscitation; Nursing2008 Critical Care; Vol. 3, No. 2. • Uhlig, C. Sliva, P., Dechert, S., et al. Alumin versus crystalloid solutions in patients with acute respiratory distress syndrome: A systematic
review and meta-analysis. Critical Care Open Access. 2014. 18:R:10.
• Papadarkis, M. & McPhee, S. (2015). Current Medical Diagnosis & Treatment. McGraw Hill: New York, NY.
• Stoller, J. (2016). Managing COPD Exacerbations. UptoDate. Accessed March 24,2016.
• Yancy, C. et al. (2013). ACCF/AHA Guideline for the management of heart failure. Circulation, 128; e240-327.
• Wunderlink, R. (2014). Clinical Practice. Community-acquired pneumonia. New England Journal of Medicine; 370:543.
Questions?