Managing Acute Cardiac Emergencies in special populationijncollege.edu.my/PDF/Managing Acute Cardiac...
87
Managing Acute Cardiac Emergencies in Special Population Dr Ika Faizura Bt Mohd Nor
Transcript of Managing Acute Cardiac Emergencies in special populationijncollege.edu.my/PDF/Managing Acute Cardiac...
Managing Acute Cardiac
Emergencies in Special Population
Dr Ika Faizura Bt Mohd Nor
CASE 1

34 years-old woman.
Transferred from Hospital Klang with SOB (NYHA 11)
Previously well, Sedentary lifestyle.
2/12 SOB with housework and shopping
Denies any palpitation, chest pain and dizzy spell
No PMH of DM, HPT
G5P1+ 3, 32 weeks pregnant.

Physical Examination
Comfortable at rest
Afebrile
P=100 regular, BP 99/50, RR 20
JVP 6cm
Soft 1HS EDM loud P2
Lungs bi-basal crepitations
Mild pedal oedema
Transferred to HDU for monitoring.
IV frusemide
Mitral stenosis
90 % in CRHD ( 50% of patient has childhood history of RF)
Others:
Congenital
Calcification
Endocarditis with vegetation
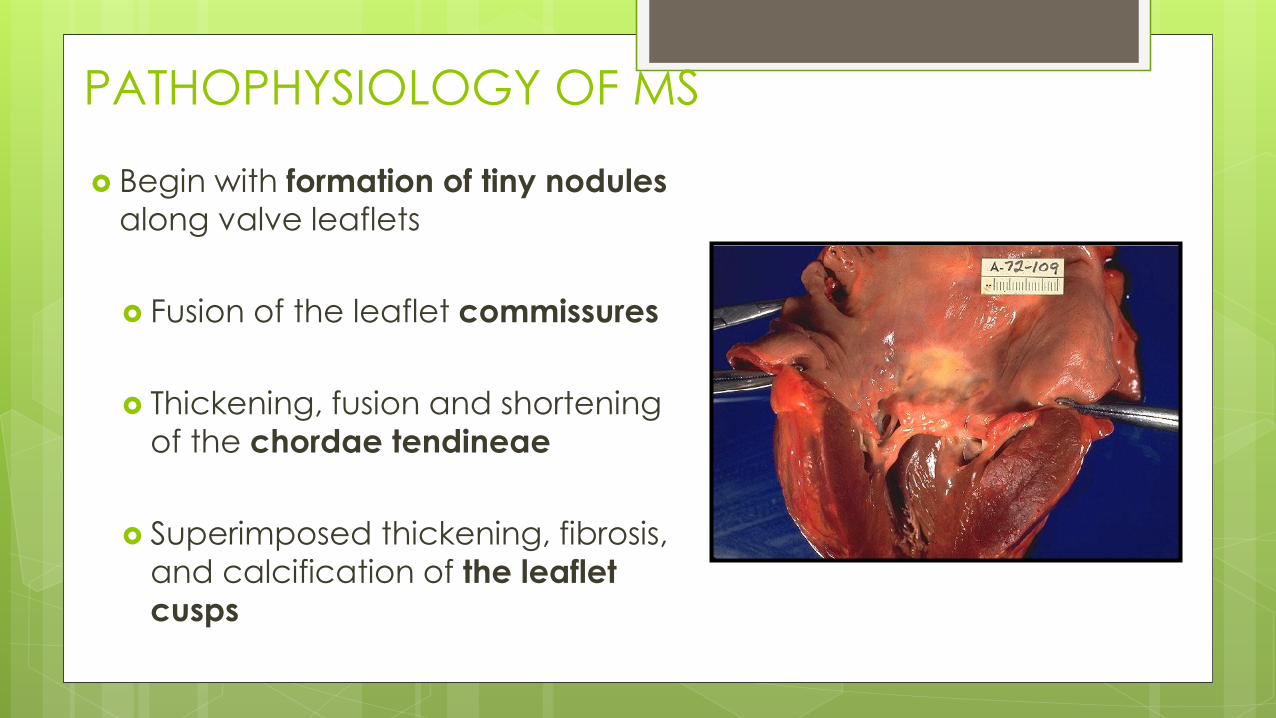
PATHOPHYSIOLOGY OF MS
Begin with formation of tiny nodules
along valve leaflets
Fusion of the leaflet commissures
Thickening, fusion and shortening
of the chordae tendineae
Superimposed thickening, fibrosis,
and calcification of the leaflet
cusps
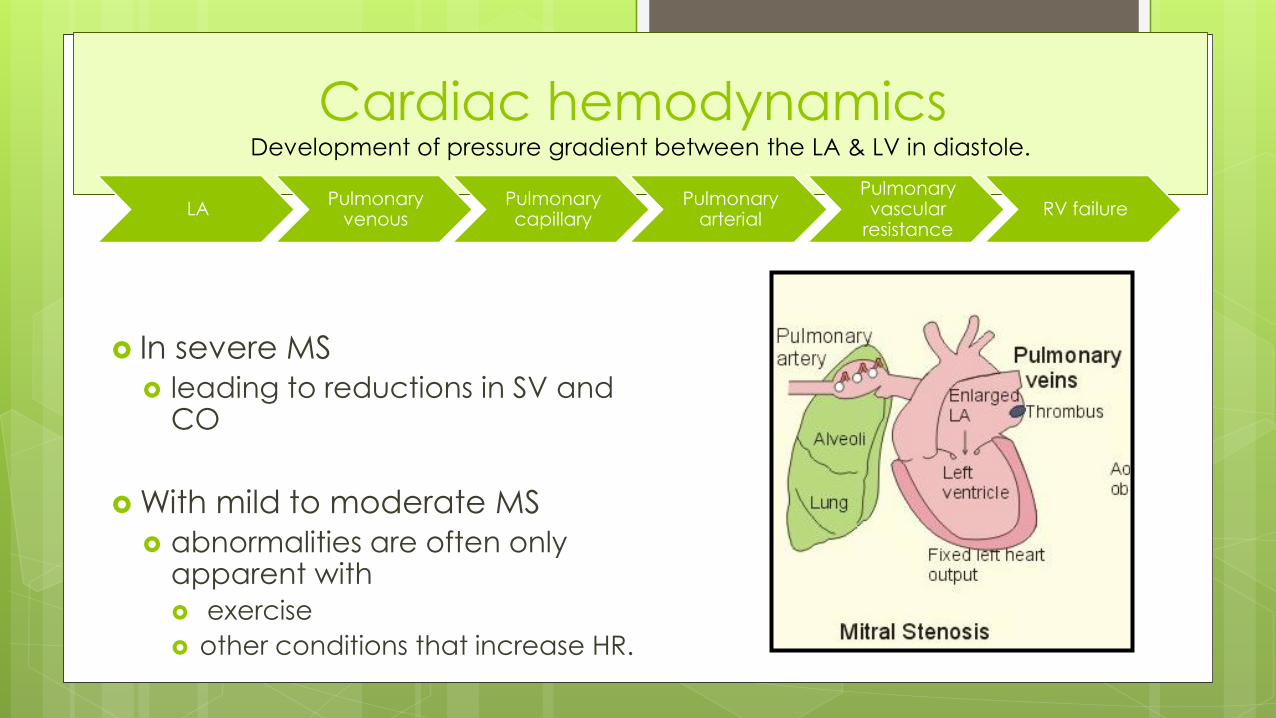
Cardiac hemodynamicsDevelopment of pressure gradient between the LA & LV in diastole.
In severe MS
leading to reductions in SV and CO
With mild to moderate MS
abnormalities are often only apparent with
exercise
other conditions that increase HR.
LAPulmonary
venousPulmonary capillary
Pulmonary arterial
Pulmonary vascular
resistanceRV failure

Severity of mitral stenosis
Degree of
MS
Mean gradient
(mmhg)
MVA (cm2 )PA press Symptoms
Normal 0 4 - 6 10-20
Mild MS <5 >1.5 <30 Exertional dyspnoea
Moderate
MS5 - 10 1.0 - 1.5 30-50
Symptom with minimal
exertion
Severe MS > 10 <1 >50 Symptom at rest

Natural progression Slow progressive disease.
Progression becomes more rapid after the onset of symptoms. Progression varies across geographical areas
The mean interval (rheumatic fever the onset of symptoms ) was 16.3 years.
At 25 years –
8 percent were asymptomatic,
9 percent were NYHA class II,
33 percent were NYHA class III,
50 percent were NYHA class IV or had undergone mitral valve surgery.
Progression from mild severe disability took an = 9.2±4.3 years.
34 years-old woman.
Transferred from Hospital Klang with SOB (NYHA 11)
Previously well, Sedentary lifestyle.
2/12 SOB with housework
Denies any palpitation, chest pain and dizzy spell
No PMH of DM, HPT
G5P2+ 2, 32 weeks pregnant.

Antepartum hemodynamic changes
The CO rises 30 to 50 % above
baseline during normal pregnancy
rise in blood volume
decline in SVR
maternal HR rises by 15 to 20
beats/min
Causes a 2 – 3 fold increase in the resting trans-mitral gradient.
Patient’s symptomatic status increase by about one NYHA class
Patient who is asymptomatic may develop mild symptoms.
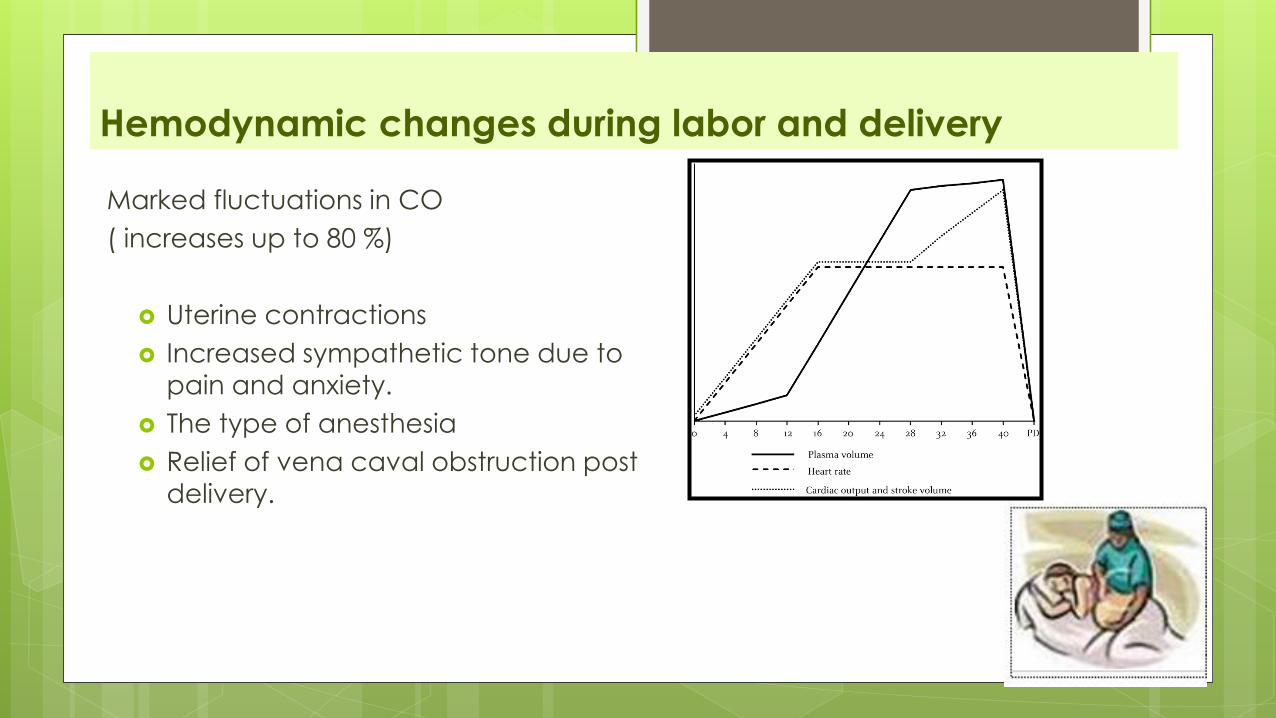
Hemodynamic changes during labor and delivery
Marked fluctuations in CO
( increases up to 80 %)
Uterine contractions
Increased sympathetic tone due to
pain and anxiety.
The type of anesthesia
Relief of vena caval obstruction post
delivery.


Pregnancy in women with MS
Cardiac Disease in Pregnancy (CARPREG) index –Four predictors of cardiac events were identified:
Poor functional class (>NYHA class 11) or cyanosis
Previous cardiac events (eg, DHF,TIA, stroke) or arrhythmia
Left heart obstruction
MVA of <2 cm2,
AVA of <1.5 cm2,
peak LVOT >30 mmHg
Left ventricular systolic dysfunction (EF <40 )
1point = 3%, 30%,66%

CXR

ECG
The QRS amplitude and morphology are normal unless there is mitral regurgitation or coexistent aortic valve disease.
Left atrial hypertrophy and enlargement P wave that becomes broader (duration in lead II>0.12 sec), is of increased amplitude,
and is notched (due to the delay in left atrial activation). "P-mitrale.“
The left atrial changes also produce a prominent negative terminal portion of the P wave in lead V1.
The P waves changes are not seen in patients with atrial fibrillation. The fibrillatorywaves are coarse, generally >0.1 mV in amplitude, reflecting left atrial hypertrophy.
Pulmonary hypertension and right ventricular hypertrophy. The frontal axis shifts to the right (S>R in lead I and aVL) and a tall R wave develops in V1
and V2 (R>S or R/S ratio >1).

ECHOCARDIOGRAPHY
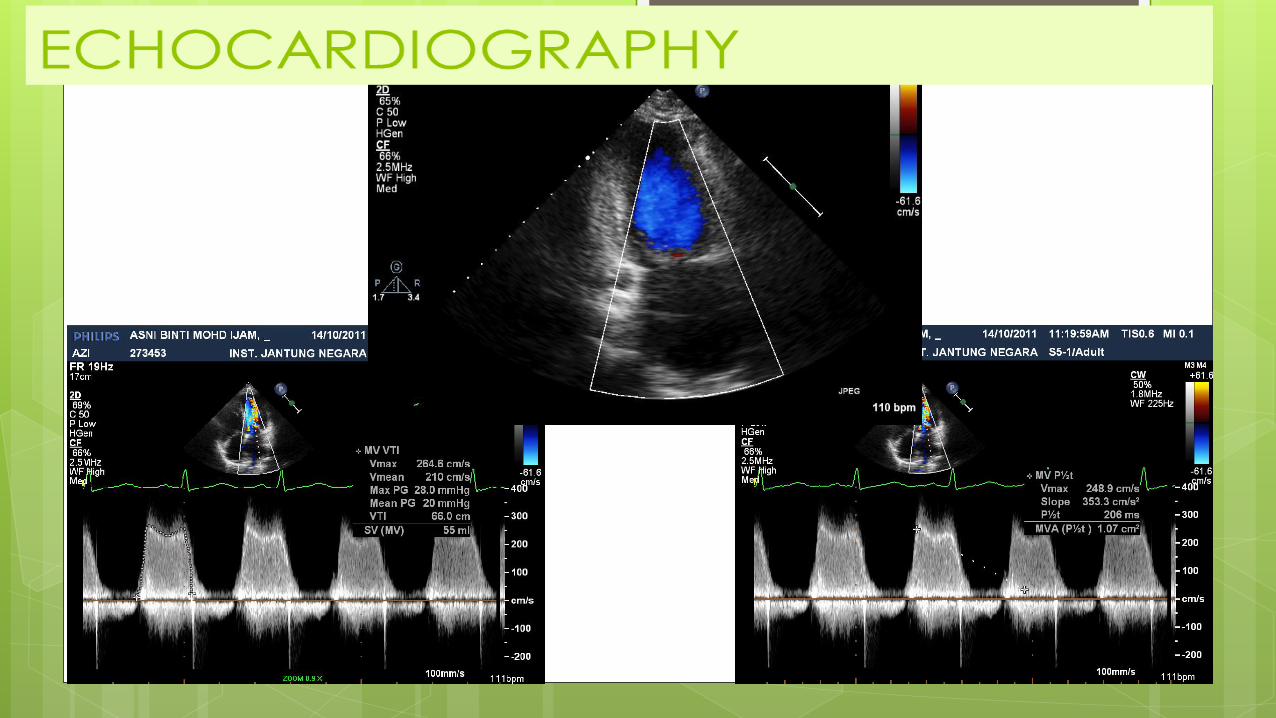


ECHOCARDIOGRAPHY
LA thrombus- TOE.

ManagementMedical
Surgical
Obstetric

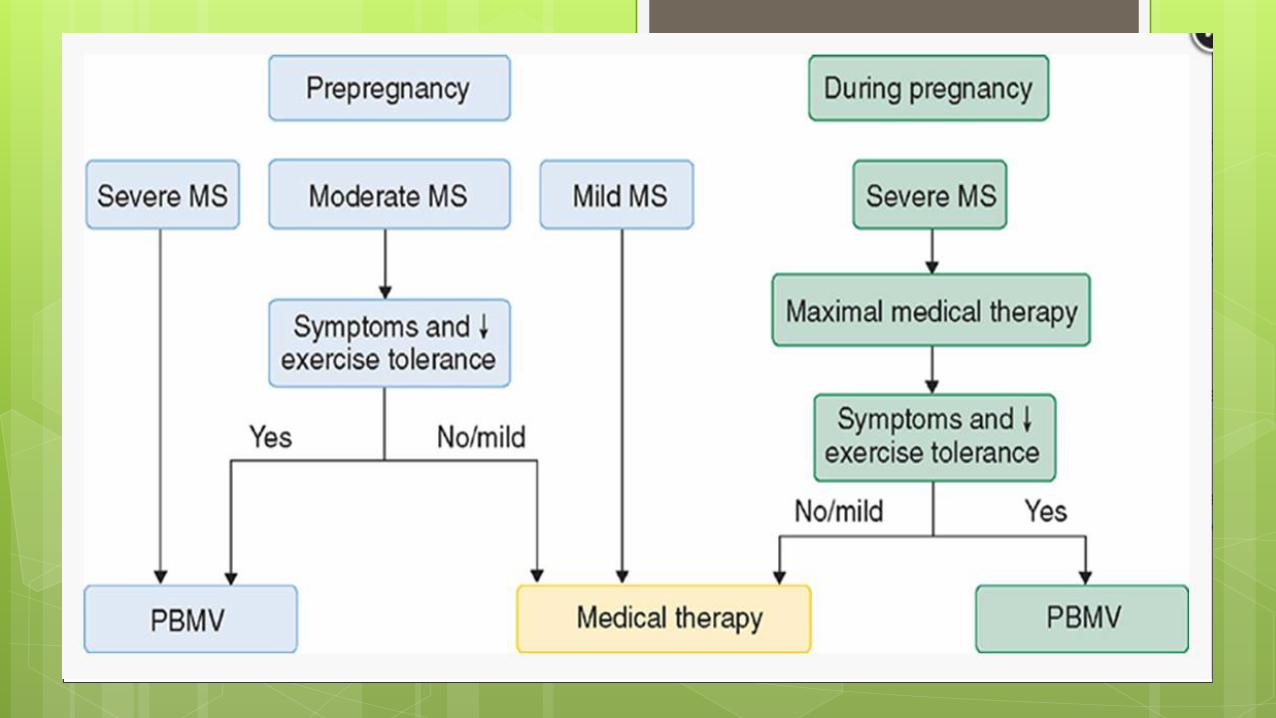
The 2006 ACC/AHA guidelines on the management of valvular heart disease
identified the following risk groups for adverse maternal and/or fetal outcomes in
patients with MS
High Risk : Prophylactic PTMC or open commissurotomy prior to becoming pregnant
34 years-old woman. G5P2+ 2, 32 weeks pregnant, SOB (NYHA 11),
Severe MS (MVA 0.9), Est PAP 82/23 mmhg
High risk —
Symptomatic MS(NYHA
class II to IV)
Severe PHT
PA press>75 % of
systemic press.
o Low risk
Mild MS
MVA >1.5 cm2 and a mean
gradient <5 mmHg
No severe pulmo HPT
Medical management Bed rest and oxygen therapy
IV diuretic
B blocker: propranolol
Avoidance of significant anemia
Treating infection early.
Medical management AF:
Digoxin/B Blocker
Cardioversion
Anticoagulant:
SC/IV heparin – up to 12 weeks
Oral warfarin -12 to 36 weeks
SC/IV heparin – after 36 weeks

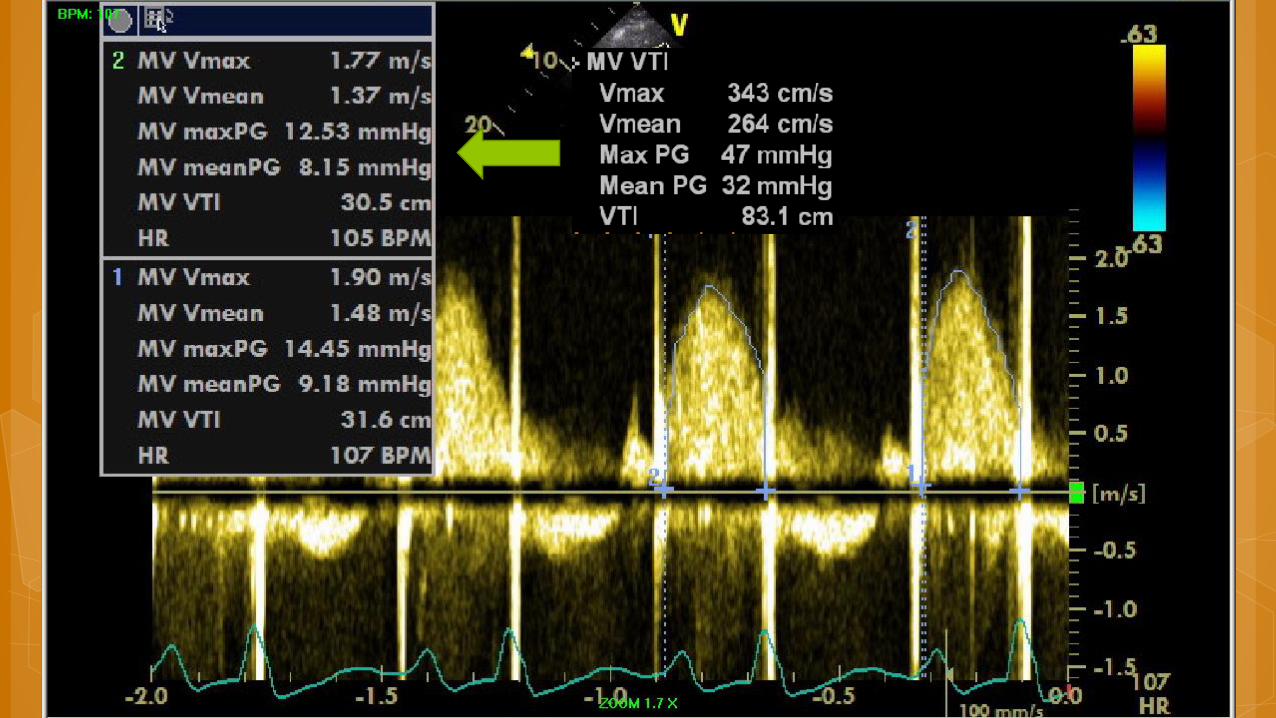
Percutaneous Transluminal Mitral Commisurotomy
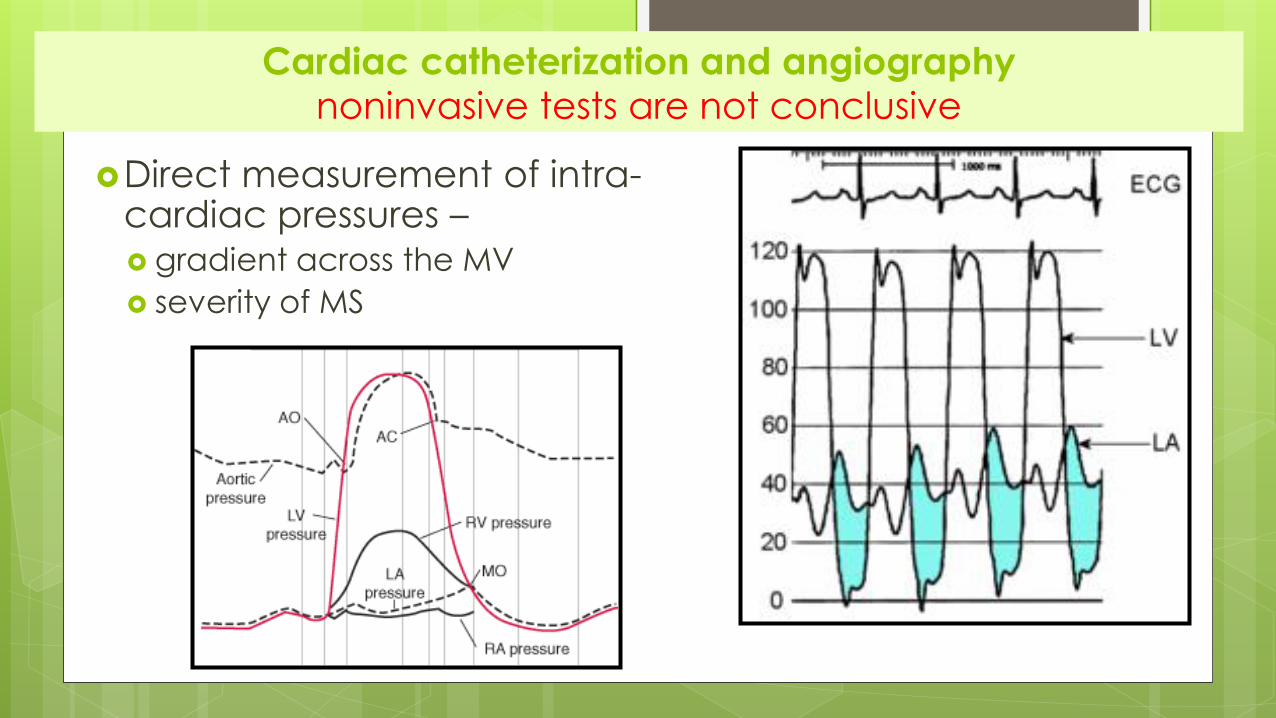
Cardiac catheterization and angiographynoninvasive tests are not conclusive
Direct measurement of intra-cardiac pressures – gradient across the MV
severity of MS
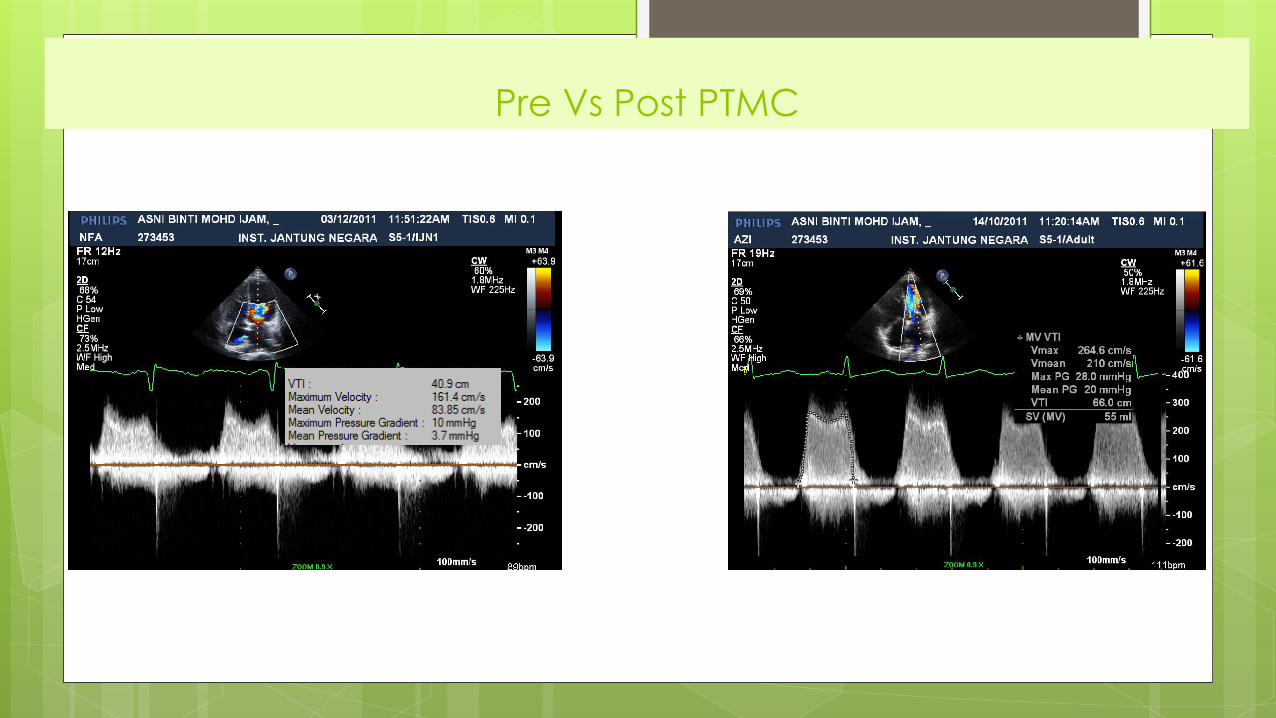
Pre Vs Post PTMC

Obstetric and labor management
Pulmonary oedema
Arrhythmia

Obstetric and labor management
Good labor analgesia (avoid tachycardia)
Mode of delivery:
Trans-vaginal with epidural analgesia -preferred
Shortened second stage
Invasive cardiac monitoring
Arterial BP
Pulmonary catheter

ANTIBIOTIC PROPHYLAXIS —
Routine endocarditis prophylaxis is not necessary for
either cesarean or vaginal delivery
However, continuation of antibiotics for secondary
prophylaxis of rheumatic fever is recommended
Obstetric and labor management

Surgical option
Closed commissurotomy,
Open commissurotomy,
Mitral valve repair,
Mitral valve replacement
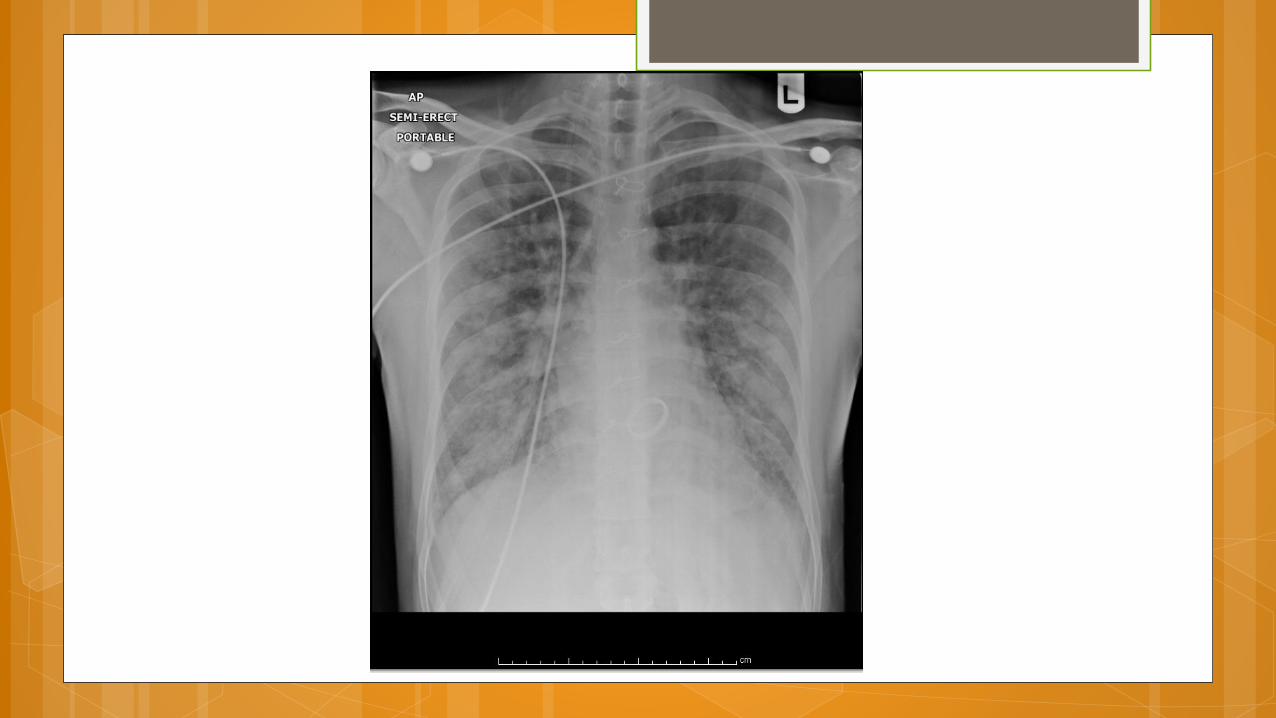
Case 2
20/10/2013 – 10 pm
23 year old college student in MIRI
MVR(mechanical-carbomedic)in Pakistan in 2011
Well post MVR on warfarin
2/52: SOB . 3/7:cough and orthopnea
Noted cannot hear prosthetic click:-2 weeks
Admitted in Miri hospital; treated as CAP with IV
augmentin
Physical Examination
SOB at rest
Afebrile
P=105 regular, BP 104/59, RR 28
JVP 6 cm
No prosthetic click heard
Lungs bi-basal crepitations
Mild pedal oedema
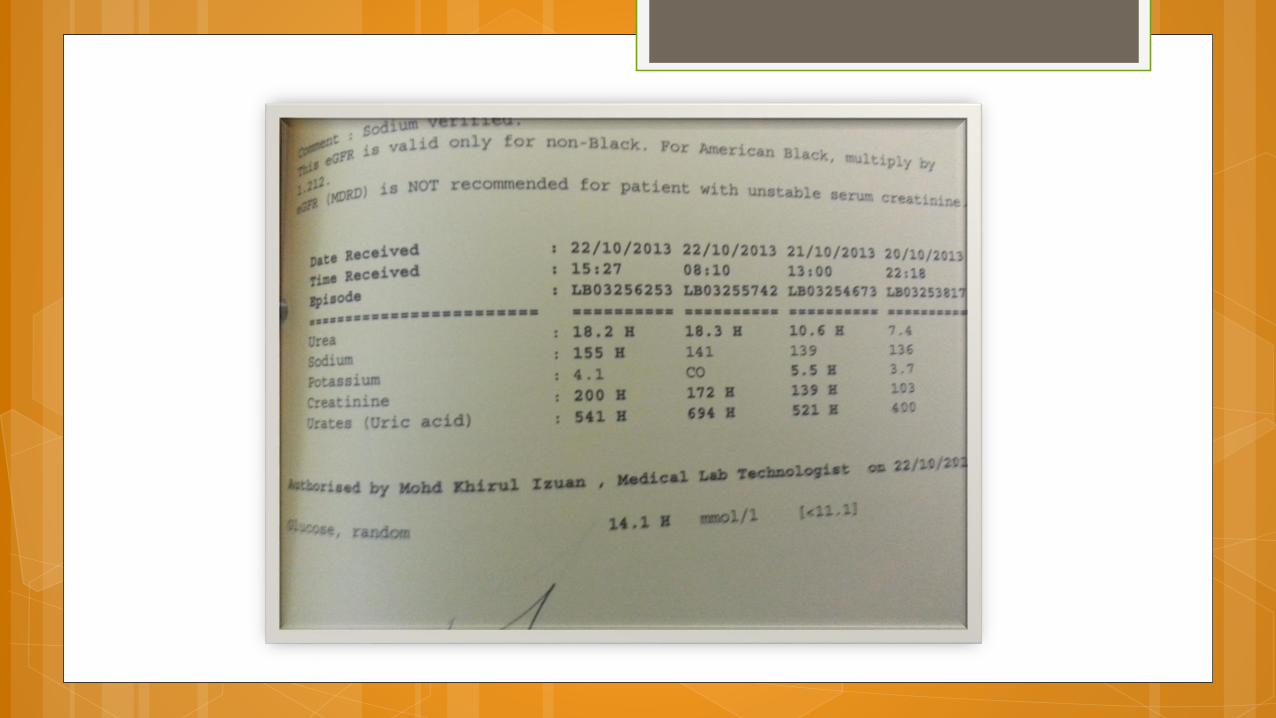
Blood test
Wcc 13.9x10 (neu 91), hb 17.4, plt 324
Lft ; normal, Rp; normal
Inr 4.1
Crp; 36.6 and ESR 13
Differential diagnosis




Transfer to CCU- for invasive monitoring
Refer to CTS for redo MV
Keep NBM
FFP x 2
IV Frusemide
IV Rocephine
4 am 21/10/2013
Worsening SOB
Already had 2 unit of FFP
P; 130 bpm, BP 130/80
JVP: 8cm
I/O: -200
Intubation

Post
Intubation
at 4 am

7.30 am 21/10/2013 Intubated ventilated sedated
P: 131 bpm Bp 83/59 CVP 18, sat 100% on Fio2 65%
Dobutamin 2.5 mcg/kg/min
INR 2.5
By 2 pm: maximun3 inotrope and milrenone
IABP was inserted
Aneuric with worsening renal profile and metabolic
acidosis
CVVH was started



22/10/2013
Redo MVR
Prosthetic Heart Valve
As early as 1960s
The ideal valve substitute should mimic the characteristics of a normal
native valve.
In particular, it should have excellent hemodynamics, long durability,
high thromboresistance, and excellent implantability
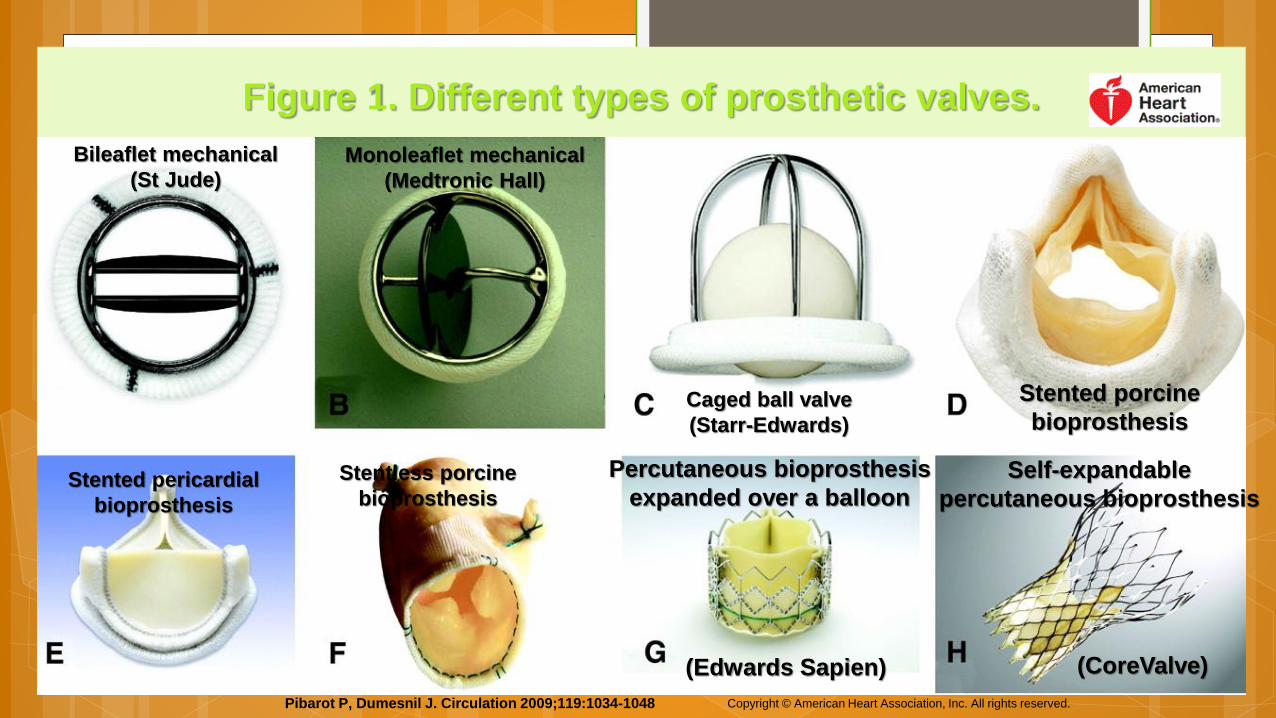
Figure 1. Different types of prosthetic valves.
Pibarot P, Dumesnil J. Circulation 2009;119:1034-1048 Copyright © American Heart Association, Inc. All rights reserved.
Bileaflet mechanical
(St Jude)Monoleaflet mechanical
(Medtronic Hall)
Caged ball valve
(Starr-Edwards)
Stented porcine
bioprosthesis
Stented pericardial
bioprosthesis
Stentless porcine
bioprosthesis
Percutaneous bioprosthesis
expanded over a balloon Self-expandable
percutaneous bioprosthesis
(Edwards Sapien) (CoreValve)
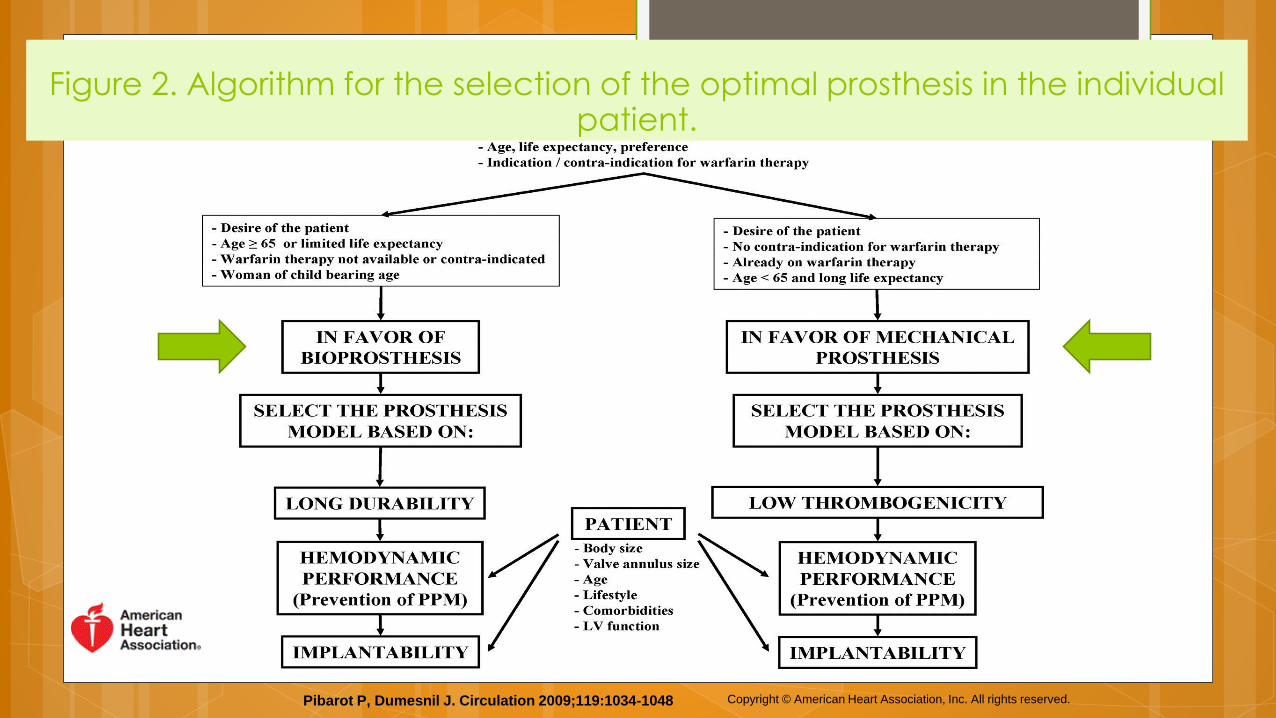
Figure 2. Algorithm for the selection of the optimal prosthesis in the individual patient.
Pibarot P, Dumesnil J. Circulation 2009;119:1034-1048 Copyright © American Heart Association, Inc. All rights reserved.

Long term managementAnti-thrombotic

Risk of Thromboembolic event
Mechanical > bioprosthetic valves
Mitral > aortic prosthetic valves
Early (<3 months)> late (> 3months)
Concomitant risk factors:
Atrial fibrillation
LV dysfunction
Left atrial dilation??
Previous thromboembolism
Hypercoagulable condition.
Aortic Valve
Mechanical
Mitral Valve
Bioprosthetic
< 3 months
> 3 months< 3 months
Mitral Valve +
Risk factor
Aortic Valve +
Risk factor
> 3 months
Aortic Valve
Mitral Valve

Figure 6. Prosthetic valves explanted for severe dysfunction.
Pibarot P, Dumesnil J. Circulation 2009;119:1034-1048 Copyright © American Heart Association, Inc. All rights reserved.
Obstructive thrombosis
Pannus ingrowth
Rupture of the outlet strut
and leaflet escape
Leaflet calcific degeneration and tear

Figure 7. Algorithm for the management of patients with left-sided prosthetic valve thrombosis.
Pibarot P, Dumesnil J. Circulation 2009;119:1034-1048 Copyright © American Heart Association, Inc. All rights reserved.
Thrombolysis:-
urokinase,
streptokinase,
Rtpa
Long term managementEndocarditis Prophylaxis

Patients with prosthetic valves are at high risk for endocarditis
because of the foreign valve surface and sewing ring.
Lifelong requirement for antibiotic prophylaxis
Dental
Endoscopic
surgical procedures
Patients and their treating physicians/dentists should be aware
of the importance of:
Dental hygiene
Blood cultures for any febrile illness before starting antibiotic therapy.

Long term managementProsthetic Valve Endocarditis

The incidence ≈0.5% per patient-year
High mortality rates (30% to 50%).
Diagnosis:
Positive blood cultures
Echocardiographic evidence of prosthetic infection:
Vegetations
Paraprosthetic abscesses
New paravalvular regurgitation
TEE is essential because of its greater sensitivity in detecting these
abnormalities.
Prosthetic valve endocarditis will eventually require surgery.
Case 3

42 years old Malay man Diagnosed with Non Ischemic Dilated Cardiomyopathy in
2005
CRT-D implanted in 2006
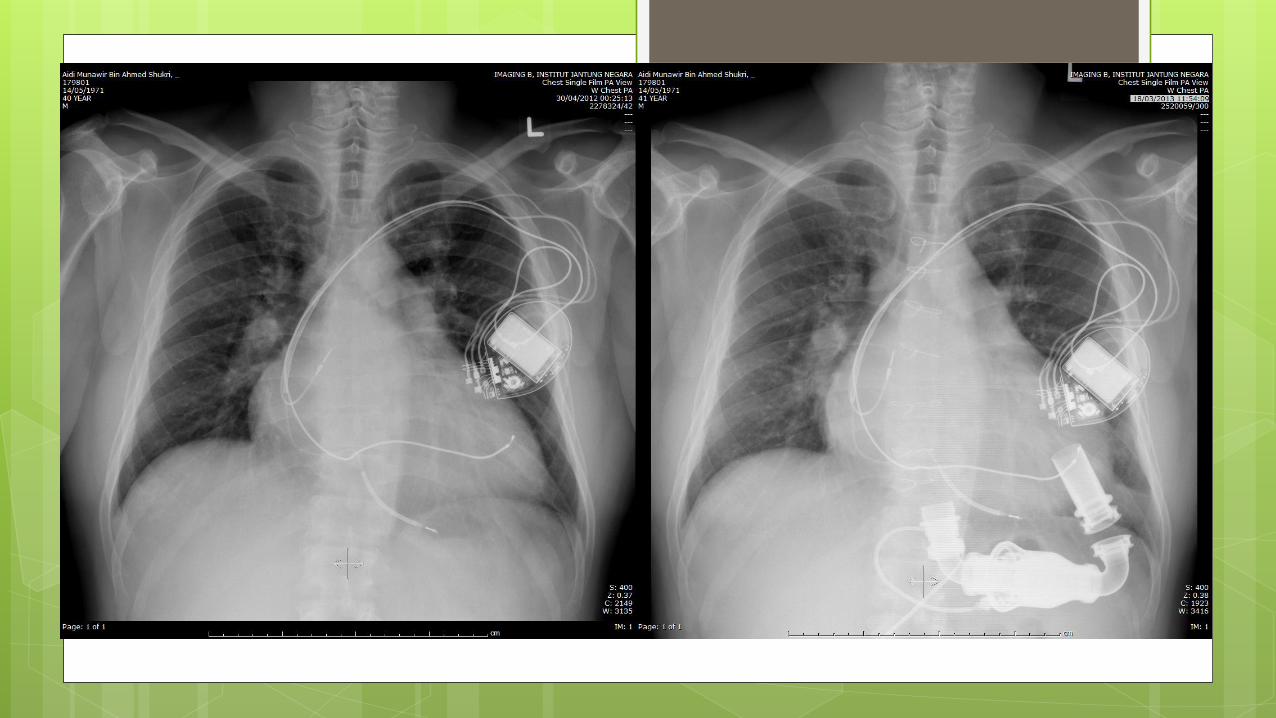
Ventricular Assist Device in planted July 2012
Well post Implantation. F class 1
End stage Heart Failure
Despite recent advancement in the management of heart failure, the quality of life and the survival rate of patients with severe heart failure remains limited.
The one-year mortality rate of those with advanced disease exceeded 50 % and the occurrence of sudden death is frequent.
For those patients who are suitable candidates, cardiac transplantation is the gold standard with proven benefit.
But worldwide shortages of donor hearts have resulted in the development of Ventricle Assist Device (VAD) to bridge patients to heart transplant.
Survival for the LVAD vs. OMM groups at 1 year were 52% vs. 25%, respectively.
Mechanical Circulatory Support as a Bridge to Transplant tor for Destination Therapy. Curr Heart Fail Rep (2010) 7:159–166..DOI 10.1007/s11897-010-0026-4
Long Term use of a left ventricular assist Device for End stage Heart Failure. N Engl J Med, Vol. 345, No. 20, November 15, 2001
Mechanical Cardiac Support Device Dream and Develish Detail N Engl J Med, Vol. 345, No. 20.November 15, 2001
ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult: Executive SummaryJ. Am. Coll. Cardiol. 2001;38;2101-2113
Long-Term Destination Therapy With the HeartMate XVE Left Ventricular Assist Device: Improved Outcomes Since the REMATCH Study Congestive Heart Failure.Volume 11, Issue 3, pages 133–138, May/June 2005
Since 2010, the smaller and streamlined design of axial (HM II) and centrifugal flow pumps
(Heartware) has been implanted instead of the pulsatile pumps (PVAD and IVAD) which were much larger.
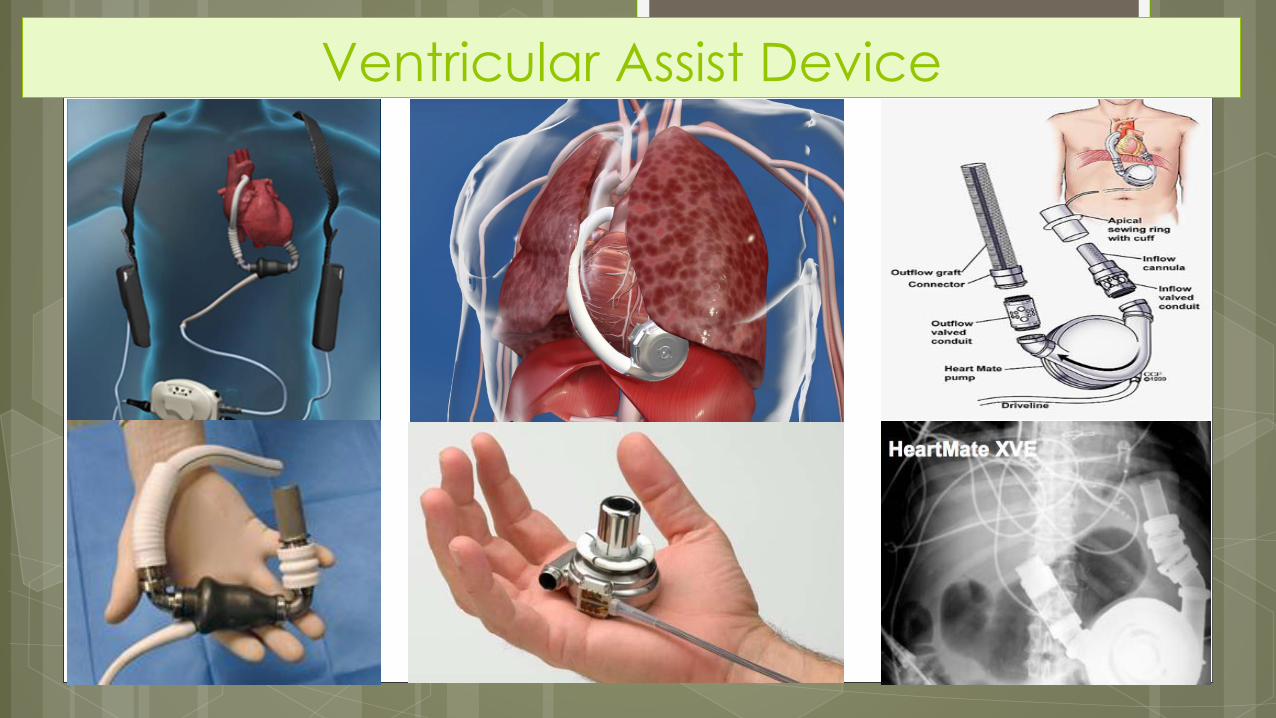
Ventricular Assist Device
Why Do We Need VADs?
Malaysia Data 1995-2014
90 people were waiting for a heart
23 received one
48 died waiting
19 were taken out
21 VAD implanted in 2005-2014
IJN Heart Transplant Data

0
2
4
6
8
10
12
14
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Chart Title
Listed Transplant

0
2
4
6
8
10
12
14
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Transplant and patient on waiting list
Listed Transplant

Indications for VAD
Bridge to transplant (BTT)
most common
allow rehab from severe CHF
while awaiting donor
Bridge to recovery (BTR)
unload heart, allow “reverse
remodeling”
can be short- or long-term
“Destination” therapy (DT)
permanent device, instead of transplant
currently only in transplant-
ineligible patients
Bridge to candidacy (BTC)/
Bridge to decision (BTD)
when eligibility unclear at implant
not true “indication” but true
for many pts
2009 Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults :
Circulation 2009, 119:1977-2016

21/06/2013
Worsening SOB and oedema
Admitted for decompensated heart failure
Respond to IV diuretic
Noted on echo:
Worsening LV dilatation
Worsening AR

25/06/2013
Sudden onset of SOB
Pulse: not palpable ( monitor 150 bpm )
BP: mean 45 mmhg
Sat 94% in RA
Chest: bibasal crepitation

CASE 4
23 y/o malay female
Diagnosed with idiopathic dilated cardiomyopathy
Had a heart transplant for six years previously.
Post-transplant course has previously been
uncomplicated.
Very compliant with medical follow up.
Last surveillance heart biopsy 3 months ago showed no
rejection
His last cath was 2 years ago and normal
2 day H/O generally feeling unwell with nausea and mild
dyspnea at rest.
Immunosuppressive regimen has been stable and
consists of cyclosporin and mycophenolate mofetil.
Other medications include Ramipril, ASA, pravastatin.
Clinical examination
On exam he appears restless,
BP 105/60, pulse 110 regular, O2 sat 99%.
No signs of CHF
Cardiac exam is only significant for an S3 gallop
Investigations CXR is unremarkable.
ECG reveals sinus tachycadia with IRBBB unchanged
from previous but new T inversion in the ant leads.
A bedside echocardiogram reveals mild generalized LV
hypokinesis.
Screening labs, including cardiac enzymes is
unremarkable
Differential diagnosis Early / Subclinical opportunistic pulmonary
infection.
Cardiac allograft rejection
.
Myocardial ischemia.
Anxiety.
Recurrent cardiomyopathy.

.
Myocardial ischemia
The transplanted heart remains denervated.
incapable of experiencing the subjective symptom of
angina pectoris.
The cardiac allograft is prone to develop a very diffuse
form of coronary vasculopathy
independent of the usual coronary risk factors
prevalent with time after transplantation, and can be
rapidly progressive.

Cardiac allograft rejection
A long-term transplant recipient who is on a stable low-
dose immunosuppressive regimen
Unlikely to develop allograft rejection or opportunistic
infection, although both are within the realm of possibility.

Anxiety
Patient is relatively hypotensive and to write his symptoms
off to anxiety or an upper respiratory infection would be
a great disservice.
Thank You
Dr Ika Faizura Bt Mohd Nor