Sports Medicine Fractures and Sprains
33
ACOFP 55th Annual Convention & Scientific Seminars 8 New Physicians and Residents: Sports Medicine - Fractures and Sprains Priscilla Tu, DO
Transcript of Sports Medicine Fractures and Sprains

ACOFP 55th Annual Convention & Scientific Seminars
8
New Physicians and Residents: Sports Medicine - Fractures and Sprains
Priscilla Tu, DO


3/14/2018
1
Sports Medicine
Fractures and Sprains
Priscilla Tu, DO, FAOASM, FAAFP
ACOFP New Physicians & Residents
March 23, 2018
Disclosures
• I have no financial
disclosures…unfortunately!
3/14/2018
2
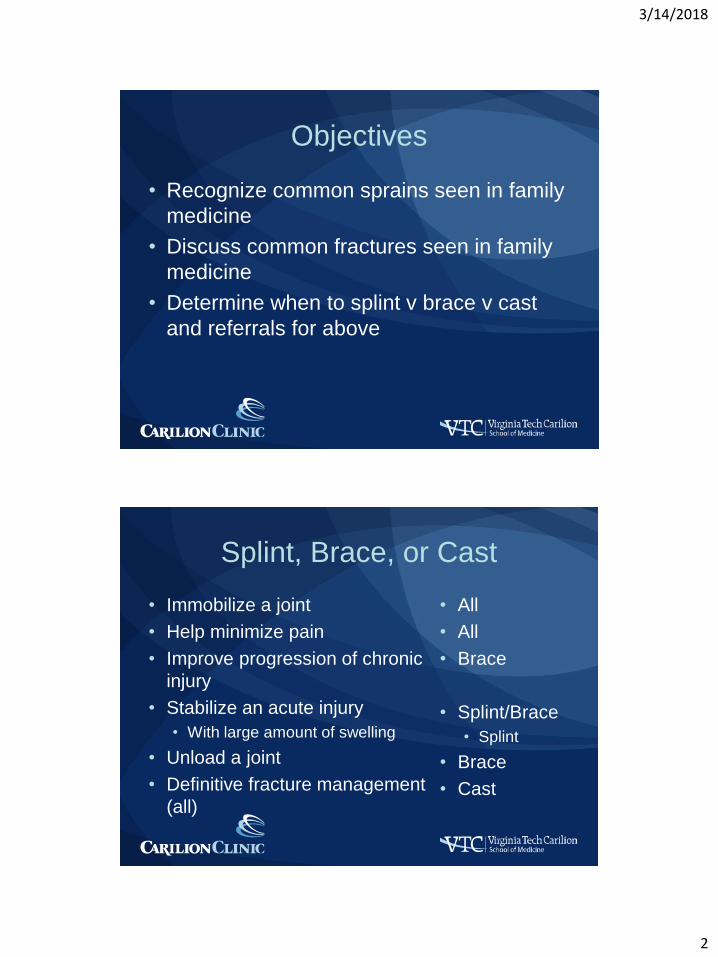
Objectives
• Recognize common sprains seen in family
medicine
• Discuss common fractures seen in family
medicine
• Determine when to splint v brace v cast
and referrals for above
Splint, Brace, or Cast
• Immobilize a joint
• Help minimize pain
• Improve progression of chronic
injury
• Stabilize an acute injury
• With large amount of swelling
• Unload a joint
• Definitive fracture management
(all)
• All
• All
• Brace
• Splint/Brace
• Splint
• Brace
• Cast

3/14/2018
3
Goals of Immobilization
• Decrease pain
• Provide stability – limit ROM
• Maintain alignment
• Promote healing
• Protect injury
• Help compensate for surrounding
muscular weakness
Bracing – When to Use
• Chronic injury
• Unload joint
• Must have accurate
diagnosis
• Worsening of injury
• Injury prevention

3/14/2018
4
Bracing – Fitting Brace
• BRACE MUST FIT
WELL
• Patient should know
how to put on brace
properly
• Watch them in clinic
before you let them
leave
Splint v Cast
• Stage and severity of injury
• Potential for instability
• Risk of complications
• Patient's functional requirements

3/14/2018
5
Splint versus Cast
• Fast and easy
• Can be static or
dynamic
• Allow for swelling
• Removed more easily
• Less risk
complications
• Soft tissue injuries
• Circumferential
• Superior
immobilization
• Complex fractures
• Definitive fracture
management
• Harder to remove
Case 1
• A 19yo F Longhorns volleyball player presents to clinic with ankle pain, swelling, and bruising after landing poorly during a game. She has a positive drawer sign and talar tilt. Xrays are negative, but patient is still having difficulty bearing weight.

3/14/2018
6
Ankle Sprain
Ankle Sprain
• Most common injury
in sports
• Lateral more common
than medial (85-90%)
• Usually <35yo
• Usually ligament
sprain or tear
• Occ fractures

3/14/2018
7
Ankle Sprain
• Medial Ankle
Ligament = Deltoid
Ligament
• Largest ankle ligament
• Broad, fan-like
• Prevents abduction /
eversion of ankle and
subtalar joint
Ankle Sprain – Treatment
• PRICE
• Control swelling
• Early ROM
• Stretching
• Proprioception / Balance
3/14/2018
8
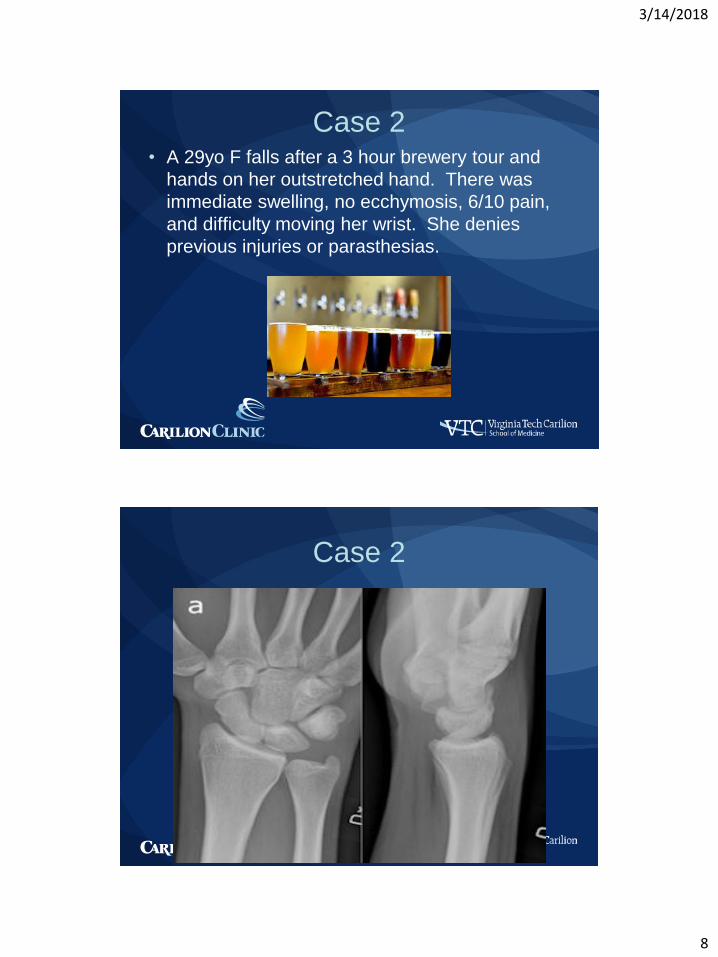
Case 2• A 29yo F falls after a 3 hour brewery tour and
hands on her outstretched hand. There was
immediate swelling, no ecchymosis, 6/10 pain,
and difficulty moving her wrist. She denies
previous injuries or parasthesias.
Case 2

3/14/2018
9
Wrist Sprain / Soft Tissue Injury
• PRICE
• Control swelling
• Early ROM
• Stretching
Case 3
• A 32yo M rodeo clown
presents with medial
knee pain after
distracting a bull the
night before. No pops.
Pain made worse
turning in bed and
getting out of car.
Positive Valgus stress
test and tenderness
medially.

3/14/2018
10
Medial Collateral Ligament
Sprain• Grade I, II, III
• Treatment
• PRICE
• Control swelling
• Early ROM
• Physical therapy
• RTP – depends on
grade
• Surgery – rare
• Same for LCL
Lateral Collateral Ligament
Sprain

3/14/2018
11
Fractures
Fractures – Most Common
• Phalanges (Fingers)
• Metacarpals
• Radius (Distal)
• Phalanges (Toes)
• Fibula
• Metatarsal
• Clavicle

3/14/2018
12
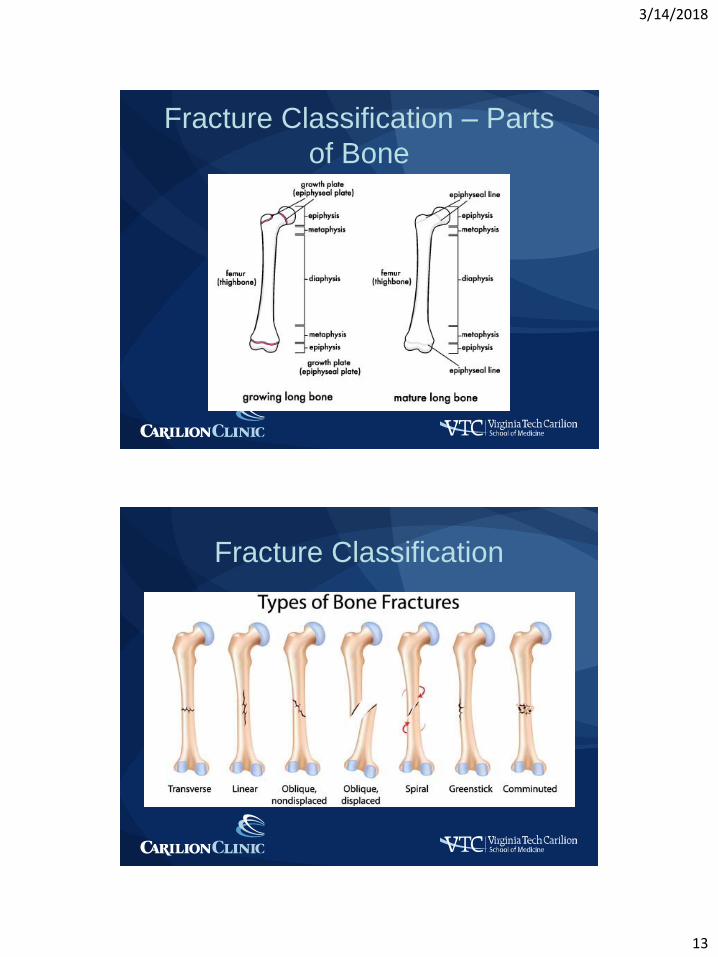
Fracture Classification /
Description• Open v closed
• Anatomic location
• Distal, mid, proximal
• Diaphysis,
epiphysis,
metaphysis
• Intra-articular
• Fracture line pattern
• Relationship of
fragments
• Angulated
• Displaced
• Rotated
• Dislocation
• Neurovascular
status
Fracture Classification
3/14/2018
13
Fracture Classification – Parts
of Bone
Fracture Classification

3/14/2018
14
Fracture Classification
Fracture Classification -
Pediatrics

3/14/2018
15
Fracture Assessment
History
• MOI
• Other injuries
• Previous injuries
• PMH
• Medications
• Menstrual cycle for
women
• Nutrition
• Allergies
Physical Exam
• On field
• ABCs
• Neurovascular, skin breaks
• Palpate entire bone
• Joint above and below
• Radiographs
• At least 2 differing by 90
degrees
• Put in order what you are
concerned about
Fracture Treatment
• Factors affecting healing
• Age
• Hormone balance / nutrition
• Medications – NSAIDS, corticosteroids, Abx
• Smoking / ETOH
• Diabetes
• Weight bearing
• Patient non-compliance

3/14/2018
16
Fracture Healing
• Most fractures heal in?
• 8 weeks
• How long before swelling resolve / patient
feel normal?
• A year or more
• If surgery needed, when?
• Within 2 weeks if possible
Fracture Treatment – Refer?
• Open or comminuted fractures• Tenting of skin concern for open fracture
• Arterial or nerve injury
• Intra-articular fractures
• Fracture dislocations
• Specifics for different body parts
• Compartment Syndrome• Elevated pressures in rigid fascial muscle
compartments
• 5 Ps – pain, pallor, paresthesias, pulselessness, paralysis

3/14/2018
17
Fracture Treatment – Refer?
• Calcaneus
• Talus
• Tibia shaft
• Femoral shaft
• Hip
• Humerus
• Ankle
Case 4
• A 19yo male Texas
Longhorn basketball
player noted a pop
and pain in his finger
after going for a loose
ball. Since then, the
distal end of his finger
cannot straighten.
You obtain an xray.

3/14/2018
18
Case 4
Mallet fracture
• Finger Splint (6-8 weeks)
3/14/2018
19
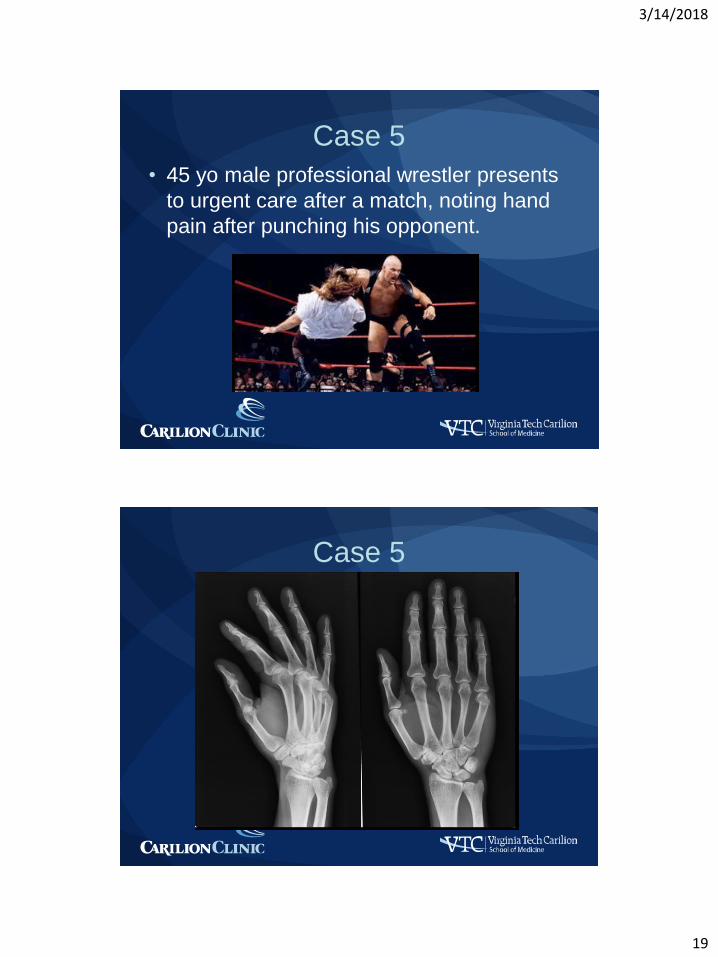
Case 5
• 45 yo male professional wrestler presents
to urgent care after a match, noting hand
pain after punching his opponent.
Case 5

3/14/2018
20
Boxer’s Fracture
• Most common hand fracture
• Check for rotation / angulation / dislocation refer
• Check for teeth marks• Abx if needed
• Ulnar Gutter Splint
• Heal Time: 4-6 wks
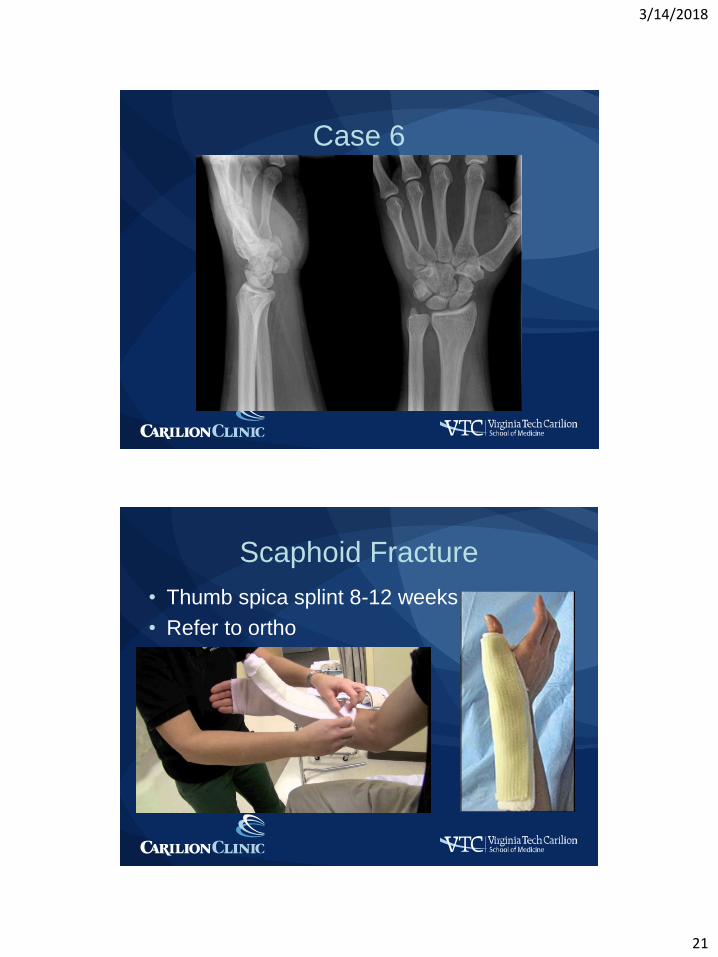
Case 6
• A 33yo M presents with
wrist pain with swelling
and ecchymosis. He
was riding a
mechanical bull and
was thrown off, landing
on his outstretched
hand. He has snuff box
tenderness on the
affected hand.
3/14/2018
21
Case 6
Scaphoid Fracture
• Thumb spica splint 8-12 weeks
• Refer to ortho

3/14/2018
22
Scaphoid Fracture?
• If initial xrays negative but snuffbox tender,
splint and re-xray in 10-14 days
• If still negative and pain, consider CT/MRI
• Refer to ortho
• Healing: 6-24 wks
• Complications
• Nonunion
• Avascular necrosis
Other Finger FracturesDiagnosis Exam Treatment Referral
PIP Dislocation
(Volar =
boutonniere)
Attempt reduction,
check NV status,
postreduction xray
Dorsal: splint; ROM
Volar: splint
extension if central
slip extensor tendon
disrupted
>30% intra-articular
surface; cannot
reduce; no full
extension after
reduction
MCP Dislocation
(esp thumb)
See above Splint; early ROM Open or hard
reductions
DIP Dislocation See above Splint; early ROM Complicated
Distal Phalanx
(Tuft Fracture)
Assess tenderness;
xray
Splint 2-4 weeks
then ROM
Rare
Mallet Fracture If unable to extend at
DIP, xray
Splint DIP in
extension 8 weeks
If large displaced
fragment; large
volar subluxation
FDP Avulsion
Fracture (Jersey)
If unable to flex at
DIP, xray
Refer for possible
FDP retraction
All
Middle/Proximal
Phalanx Fracture
Assess tenderness,
rotation, xray
Buddy tape, early
ROM
Displaced, oblique,
spiral fx

3/14/2018
23
Case 1
• A 19yo F Longhorns
volleyball player
presents to clinic with
ankle pain, swelling,
and bruising after
landing poorly during
a game. She has a
positive drawer sign
and talar tilt. Xrays…
Avulsion Fracture 5th MT
• Most common
fracture LE
• Peroneal brevis
tendon
• Firmed sole shoes for
4-8 weeks

3/14/2018
24
Case 1
• A 19yo F Longhorns volleyball player presents to clinic with ankle pain, swelling, and bruising after landing poorly during a game. She has a positive drawer sign and talar tilt. She also has tenderness lateral leg.
Maisonneuve Fracture
• Lateral ankle sprain
proximal fibula
fracture
• Non-weightbearing
bone
• Walking boot w
crutches
• Heal 6-8 weeks

3/14/2018
25
Case 7
• A 28 yo male Austin
Huns rugby player
presents with ankle
and foot pain with
inability to bear
weight after an injury
during a match. He
has pain and swelling
in lateral ankle and
foot.
Case 7

3/14/2018
26
Jones Fracture
• Cast for at least 6
weeks, up to 12
weeks
• Refer to ortho
• Poor blood supply
• If does not heal well
surgery needed
• May perform surgery
earlier if athlete or
concern for non-
healing
Other Foot FracturesFracture Type Treatment Radiographs Referral
First MT shaft Posterior splint;
NWB; f/u 3-5
days; short leg
walking cast or
boot; f/u q2-4 wks;
heal 6 wks
3-view foot;
repeat 1 wk and
4-6 wks
Open, fx-
dislocations; intra-
articular;
displacement or
angulation
Lesser MT shaft Posterior splint;
NWB; f/u 3-5
days; short leg
walking boot/cast
6wks; f/u q2-4
wks; heal 6 wks
3-view foot;
repeat 1 wk and
4-8 wks
Open,
fx/dislocations;
multiple; >3mm
displaced; >10deg
angulation
5th MT tuberosity Compressive
dressing; WBAT;
f/u 4-7 days
3-view foot attn
oblique; repeat 6-
8 wks
>3mm displaced;
>1mm stepoff;
fragment 60%
MT-cuboid joint

3/14/2018
27
Other Foot Fractures
Fracture Type Treatment Radiographs Referral
Prox 5th MT
(Jones)
Posterior splint;
NWB; f/u 3-5 days
3-view foot attn
oblique; repeat 1
wk and 4-6 wks
(10-12 wks if no
healing)
>2mm displaced;
nonunion after 12
wks; athletes
Great toe Short leg walking
boot; WBAT; f/u 4-
7 days
3-view foot or
phalanx; repeat 1
wk if IA or
reduced
Fx/dislocations;
intra-articular
displaced or
>25% joint; physis
Lesser toes Buddy tape, rigid
toe shoe; WBAT;
f/u 1-2 weeks
Same as great toe Displaced IA;
>20deg angled;
>20deg rotation;
>25% joint; physis
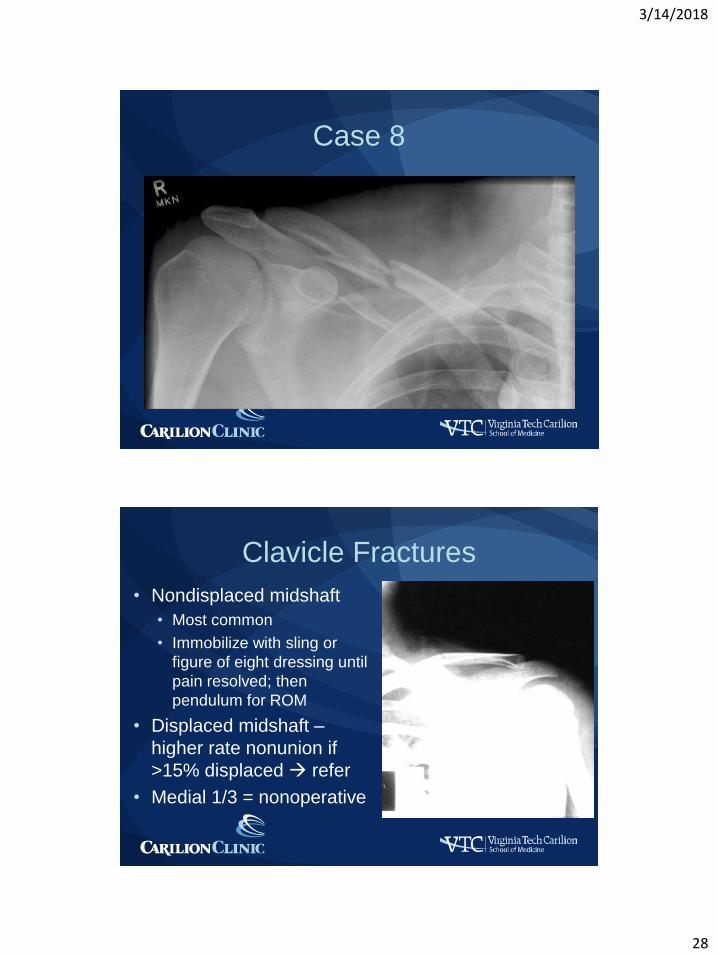
Case 8
• A 21yo male football
player presents to
urgent care with his arm
adducted close to body,
holding it up with the
other arm. MOI was
falling during a game
onto his shoulder. He
has shoulder pain and
swelling and bruising
noted.
3/14/2018
28
Case 8
Clavicle Fractures
• Nondisplaced midshaft
• Most common
• Immobilize with sling or
figure of eight dressing until
pain resolved; then
pendulum for ROM
• Displaced midshaft –
higher rate nonunion if
>15% displaced refer
• Medial 1/3 = nonoperative

3/14/2018
29
Clavicle Fractures – Distal
• 12-15% clavicle fx but
50% of nonunions
• Type 1:
coracoclavicular
ligaments intact;
minimal to no
displacement
nonoperative
Clavicle Fractures – Distal
• Type II
• Level of
coracoclavicular
ligament
• IIA – conoid and
trapezoid ligaments
intact; fracture medial
to ligaments
• IIB – disruption conoid
ligament
• Surgery recommended

3/14/2018
30
Clavicle Fractures – Distal
• Type III
• Distal to
coracoclavicular
ligaments and involve
AC joint
• Minimally or
nondisplaced usually
• Nonoperative
treatment
Questions?

3/14/2018
31
References
• Bica D, Sprouse RA, Armen J. Diagnosis and management of common foot fractures. AFP 2016; 93(3): 183-191.
• Borchers JR & Best TM. Common finger fractures and dislocations. AFP 2012; 85(8): 805-810.
• Boyd AS, Benjamin HJ, Asplund C. Principles of casting and splinting. AFP 2009; 79(1): 16-22.
• Boyd AS, Benjamin HJ, Asplund C. Splints and casts: Indications and methods. AFP 2009; 80(5): 491-499.
• Pecci M & Kreher JB. Clavicle fractures. AFP 2008; 77(1): 65-70.