Spinal Cord Stimulation for Patients with Critical Limb Ischemia: Immediate and Long-Term Clinical...
6
© 2004 International Neuromodulation Society, 1094-7159/04/$15.00/0 Neuromodulation, Volume 7, Number 2, 2004 97–102 Address correspondence and reprint requests to: Alessandra Tedesco, MD, Vascular Surgery Department, Azienda Ospedaliera S. Orsola Malpighi, Via Massarenti 9, Bologna 40100, Italy. Email: [email protected]. Blackwell Publishing, Ltd. Spinal Cord Stimulation for Patients with Critical Limb Ischemia: Immediate and Long-Term Clinical Outcome from the Prospective Italian Register Alessandra Tedesco, MD Massimo D’Addato, MD Vascular Surgery Department, Azienda Ospedaliera S. Orsola Malpighi, Bologna University, Bologna, Italy ABSTRACT The Prospective Italian Register of spinal cord stimula- tion (SCS) was designed to evaluate the clinical outcome of patients with severe peripheral arterial occlusive disease (PAOD) treated with SCS. Baseline data were collected for all patients with PAOD under- going SCS treatment (September 1998 to February 2001) at 34 participating centers. If, after a 2- to 3- week trial, SCS demonstrated significant clinical ben- efits, a permanent implantable pulse generator was implanted. Follow-up data were evaluated at 4, 8, and 12 months postimplantation. Overall, 250 patients (176 men, 74 women) were enrolled (mean age 72.6 ± 17 years) and classified by Fontaine stage. In total, 77.6% (194/250) of patients received a perma- nent implant and 43.6% (109/250) reached 1 year of follow-up. Fontaine stage, pain relief, free-walking interval, and drug intake improved significantly during follow-up. Age and Fontaine stage were significantly associated with major amputation. Cumulative limb survival at 1 year for the subgroup of Fontaine stage III patients was 82.2%. The mean number of hospital admissions and stay duration at 1 year postimplantation was significantly reduced compared with 1 year pre- implant: 1.5 vs. 0.6 admissions and 27 vs. 6 days, re- spectively. Among 109 patients evaluable at 12 months, 83 (76.1%) experienced ≥ 50% reduction in pain. All PAOD parameters improved significantly during follow-up. At 12 months postimplantation, 76.1% of patients were responsive to SCS therapy. The reduction in the use of analgesics and the number and duration of hospital stays offers clear economic advantages. KEY WORDS: critical limb ischemia, limb survival, peripheral arterial occlusive disease, register, spinal cord stimulation. INTRODUCTION Patients with peripheral arterial occlusive disease (PAOD), defined as persistent ischemic rest pain or ulcers requiring analgesics and accompanied by severely reduced peripheral blood pressure (1), have a high risk of amputation within 1 year (2).
-
Upload
alessandra-tedesco -
Category
Documents
-
view
212 -
download
0
Transcript of Spinal Cord Stimulation for Patients with Critical Limb Ischemia: Immediate and Long-Term Clinical...

© 2004 International Neuromodulation Society, 1094-7159/04/$15.00/0 Neuromodulation, Volume 7, Number 2, 2004 97–102
Address correspondence and reprint requests to: AlessandraTedesco, MD, Vascular Surgery Department, Azienda OspedalieraS. Orsola Malpighi, Via Massarenti 9, Bologna 40100, Italy. Email:[email protected].
Blackwell Publishing, Ltd.
Spinal Cord Stimulation for Patients with Critical Limb Ischemia: Immediate and
Long-Term Clinical Outcome from
the Prospective Italian Register
Alessandra Tedesco, MD
�
Massimo D’Addato, MD
Vascular Surgery Department, Azienda Ospedaliera S. Orsola Malpighi, Bologna University, Bologna, Italy
�
A
BSTRACT
The Prospective Italian Register of spinal cord stimula-tion (SCS) was designed to evaluate the clinicaloutcome of patients with severe peripheral arterialocclusive disease (PAOD) treated with SCS. Baselinedata were collected for all patients with PAOD under-going SCS treatment (September 1998 to February2001) at 34 participating centers. If, after a 2- to 3-week trial, SCS demonstrated significant clinical ben-efits, a permanent implantable pulse generator wasimplanted. Follow-up data were evaluated at 4, 8,and 12 months postimplantation. Overall, 250 patients(176 men, 74 women) were enrolled (mean age72.6
±
17 years) and classified by Fontaine stage. Intotal, 77.6% (194/250) of patients received a perma-nent implant and 43.6% (109/250) reached 1 yearof follow-up. Fontaine stage, pain relief, free-walkinginterval, and drug intake improved significantly duringfollow-up. Age and Fontaine stage were significantly
associated with major amputation. Cumulative limbsurvival at 1 year for the subgroup of Fontaine stageIII patients was 82.2%. The mean number of hospitaladmissions and stay duration at 1 year postimplantationwas significantly reduced compared with 1 year pre-implant: 1.5 vs. 0.6 admissions and 27 vs. 6 days, re-spectively. Among 109 patients evaluable at 12 months,83 (76.1%) experienced
≥
50% reduction in pain.All PAOD parameters improved significantly during
follow-up. At 12 months postimplantation, 76.1% ofpatients were responsive to SCS therapy. The reductionin the use of analgesics and the number and durationof hospital stays offers clear economic advantages.
�
K
EY
W
ORDS
:
critical limb ischemia, limb survival,peripheral arterial occlusive disease, register, spinalcord stimulation.
INTRODUCTION
Patients with peripheral arterial occlusive disease(PAOD), defined as persistent ischemic rest painor ulcers requiring analgesics and accompanied byseverely reduced peripheral blood pressure (1),have a high risk of amputation within 1 year (2).

98
�
TEDESCO
AND
D
’
ADDATO
The current treatment of choice is vascular recon-struction, but this is often inappropriate and istherefore not an option for a considerable numberof patients (40%) (3).
Spinal cord stimulation (SCS) is an alternativetreatment for patients with PAOD who are unsuit-able for revascularization with the aim of reducingpain, reducing limb amputation, and improvingpatients’ quality of life. Many authors have demon-strated that the beneficial effects of SCS lie in itsanalgesic and anti-ischemic properties, while effi-cacy in symptom resolution is reported to be inthe range of 47–85% (4–6).
However, up to now most published clinicalexperience comes from retrospectively gathereddata. Available data on the efficacy and safety ofSCS are limited and large prospective registersand randomized trials on large numbers of casehistories are still lacking.
The Prospective Italian Register of SCS wasdesigned to evaluate the immediate and long-termclinical outcome of patients suffering from severePAOD treated with SCS (evaluation scales applied:Fontaine stage, see Table 1; VAS scale; free walk-ing interval).
MATERIALS AND METHODS
Patient Inclusion
All patients who underwent SCS device implanta-tion to treat PAOD, from September 1998 to Feb-ruary 2001, at the 34 centers participating in theProspective Italian Register were enrolled in thestudy.
All the patients included in the register con-formed to the following selection criteria: PAOD;restricted pain-free walking interval or rest painwith or without lesions; unsuitable for eithersurgical or percutaneous revascularization foranatomic reasons or due to the presence of highanesthesiologic risk; no contraindications for
SCS; and written consent to undergo SCS deviceimplantation after being informed by a physicianof the technical aspects and clinical implicationsof the treatment, as well as of the possible sideeffects and complications.
Implantation Technique
The stimulation device was implanted using a ster-ile technique and X-ray guidance. The electrodewas inserted under local anesthesia in the epiduralspace and the tip of the electrode was positionedso that the patient felt paresthesia in the painfularea, usually at level T11–T12. The pulse generatorwas placed in a subcutaneous pocket in theabdominal region and connected to the electrodeby means of an extension. The implantation wasperformed in two stages. First, the electrode wasimplanted and connected to an external neuro-stimulator. This allowed a stimulation efficacy trialto be carried out, lasting for 2–3 weeks. If thetreatment was considered to have had significantclinical benefits during this trial phase by boththe patient and the attending physician, then apermanent implantable pulse generator ( IPG) wasimplanted.
Patient Assessment and Follow-Up
A form was generated and distributed to all partici-pating centers to obtain prospective data onpatients with PAOD treated with SCS. The baselineform was designed to obtain data on: the patient’smedical history, including general data, etiology ofthe disease, previous revascularization procedure,reasons why revascularization was impossible, thenumber of hospital admissions, and the total num-ber of days spent in hospital during the 12 monthspreceding implantation; assessments of Fontainestage, visual analog scale (VAS) score, and free-walking interval; the use of analgesic drugs; docu-mentation of nonrevascularization (angiography);and implantation and surgical complications.
The follow-up data were evaluated at 4, 8, and12 months after SCS device implantation. Com-plete clinical evaluation was performed at eachfollow-up visit and the same clinical parameters asthose collected at baseline were recorded, includ-ing Fontaine stage, VAS score, major amputations(defined as forefoot, below-knee or above-knee
Table 1. Fontaine Stages
Clinical Definition
Fontaine stage I AsymptomaticFontaine stage II Intermittent claudicationFontaine stage III Daily rest painFontaine stage IV Tissue necrosis

SCS for Critical Limb Ischemia
�
99
amputation), the number of hospital admissions,and the total number of days spent in hospital.
Statistical Analysis
All forms were collected by a monitor and thenanalyzed. Limb survival analysis was performed usingthe Kaplan–Meier method. Univariate Cox regressionanalysis was applied to identify any significantassociation between Fontaine stage and major limbamputation. Within-group comparisons of continuousvariables were performed by paired
t
-test, whilediscrete variables were analyzed by
χ
2
test.SCS was considered to be effective in each
patient if, at the last available visit, there was atleast 50% pain reduction with no major limbamputation. In patients who had major amputa-tion or who died, the clinical data obtained at thelast follow-up assessment before the event wereused in the analyses.
Data are expressed as means
±
standard devia-tion (SD), and a
p
-value of <0.05 was required forstatistical significance. Statistical analysis was carriedout using SPSS 10.07 software (Chicago, IL).
RESULTS
Main Clinical Features
Overall, 250 patients (176 men and 74 women)were enrolled in the register. The main clinicalcharacteristics are summarized in Table 2. The
mean age was 72.5
±
17.1 years. The majority ofpatients were classified as Fontaine stage IV(
n
= 124), while the others were Fontaine stage III(
n
= 95) and stage II (
n
= 31). The main causesof PAOD were arteriosclerosis (
n
= 146), diabeticarteriopathy (
n
= 81), Buerger’s disease (
n
= 13),and diabetic foot (
n
= 10). The mean VAS scorewas 63.3
±
30 and the mean free-walking intervalwas 43
±
7.1 m.In total, 77.6% (194/250) of patients received
a full IPG implant, whereas the electrode wasremoved after the trial screening period in theremaining 56 patients. The reasons for electroderemoval are listed in Table 3.
Clinical Events
The average follow-up period of the 194 patientswho underwent permanent IPG implantation was8.1 months; 109 of these patients reached 1 yearof follow-up; the remaining 85 withdrew fromthe register before the 1 year follow-up visit: thereasons for withdrawal were major amputation(
n
= 39), death (
n
= 25), and loss to follow-up(
n
= 21). Thirty-eight patients withdrew from theregister immediately after enrollment, thereforewithout receiving IPG implantation.
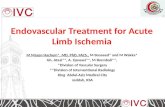
Among the baseline clinical variables, age andFontaine stage were significantly associated withmajor amputation according to Cox proportionalregression analysis (Fig. 1). We also assessed limbsurvival according to the baseline Fontaine stage
Table 2. Baseline Characteristics (N = 250)
Mean ± SD Range
Age, years 72.5 ± 17.1 28–97VAS score 63.3 ± 30 0–100Mean free-walking interval, m 43 ± 7.1 0–100
n %Sex (male/female) 176/74 70.4/29.6Dyslipidemia 69 27.6Hypertension 152 60.8Diabetes mellitus 83 33.2Smoking 85 34.0Previous myocardial infarction 66 26.4Previous transient ischemic attack 20 8.0Previous cardiovascular attack 10 4.0Fontaine stage IV 124 49.6Fontaine stage III 95 38.0Fontaine stage II 31 12.4Intake of analgesics 128 51.2
Table 3. Reason for Electrode Removal (N = 56) afterTrial Stimulation
Reason n %
Inefficacya 18 32.1Patient request 9 16.1Major amputation 8 14.3Death 6 10.7Infection 5 8.9Unable to manage stimulation 3 5.4Clinical presentation worsening 2 3.6Persistence of pain 1 0.2Decubitus 1 0.2Allergy 1 0.2Unable to manage the device 1 0.2Foot gangrene 1 0.2
a Cases of inefficacy, that is, incapability to get paresthesias and thus pain relief in the proper body areas, were randomly distributed over the participating centers

100
�
TEDESCO
AND
D
’
ADDATO
(II + III vs. IV) and we found a statistically signifi-cant difference between the two groups ofpatients (log rank test = 4.7,
p
= 0.03). Figure 2shows the corresponding Kaplan–Meier limbsurvival curves.
Clinical Effects of SCS Therapy
All indicators of peripheral arterial disease consid-ered in the register improved significantly during
follow-up, including Fontaine stage, pain relief,free-walking interval, and drug intake (Table 4).
Table 4 shows data for the 109 patients whoattended the 1-year follow-up visit. The meannumber of hospital admissions and stay durationas a result of peripheral arterial disease at 1 yearpostimplant was significantly reduced comparedwith 1 year preimplant: 1.5 vs. 0.6 admissions(
p <
0.0001) and 27 vs. 6 days (
p <
0.0001), re-spectively. Among the 109 patients, 83 (76.1%)experienced at least 50% reduction in pain and socan be considered responsive to the SCS therapy.
We also analyzed the 95 patients (38.0% of250) with rest pain (Fontaine stage III). For thesepatients, the overall number of major amputationswas 13/95 (13.7%). Figure 3 shows the limb sur-vival curve for this subgroup of patients. Thecumulative limb survival at 1 year for the Fontainestage III patients was 82.2%. In total, 44.2% (42/95)of patients completed the follow-up period in
Figure 1. Multivariate Cox analysis with major amputation asdependant variable. This figure analyzes the amputation riskby Proportional Hazards regression (Cox). Given amputationdata, final status (limb survival vs. major amputation), andcovariates — also called predictor’s coefficients — (sex, age,Fontaine stage), the analysis produces a baseline (average)limb survival curve (which conventionally starts at 1.0 at timeZero), risk ratios, 95% confidence intervals, and significancelevels. These last three data indicate the effect of eachcovariate on the baseline curve. Zero means that a variablehas no effect on the curve, therefore sex has no effect onlimb survival vs. amputation; a positive variable indicates thatlarger values of the variable are associated with greateramputation risk, an age >71 years predicts a higher risk ofamputation and so does a Fontaine stage equal to IV. Moreimportantly, the confidence intervals (represented by thelength of the interval related to each covariate) provide ameasure of the sampling error associated with eachpredictor’s coefficient: this allows us to assess which variablesare significantly related to limb survival/amputation. Age(>71) and Fontaine stage (IV), having confidence intervals inthe positive value horizontal bar, are significantly related tomajor amputation.
Table 4. Baseline and 12-Month Follow-Up Data (Homogeneous Population; N = 109)
Baseline 12 months t-test (p-value)
Fontaine stage (mean ± SD) 3.27 ± 0.74 2.40 ± 0.72 10.7 (p < 0.0001)VAS score (mean ± SD) 61.5 ± 3.1 15.9 ± 2.2 23.4 (p < 0.0001)Free-walking interval (mean ± SD), m 37 ± 34.9 264 ± 22.6 7.125 (p < 0.0001)Analgesic intake, n (%) 54 (49.5%) 18 (16.5%) 12.5 (p < 0.0001)
Figure 2. Kaplan–Meier limb survival curve according tobaseline Fontaine stage (log rank = 4.7; p = 0.03).

SCS for Critical Limb Ischemia
�
101
line with the protocol. Of these, 83.3% (35/42)improved by one Fontaine stage, 11.9% (5/42) re-mained at Fontaine stage III, and 4.8% (2/42)worsened to Fontaine stage IV. Among the remaining40/95 patients, 10 died, the SCS system was explantedin seven patients and 23 patients withdrew fromthe register, either because of lack of therapy effi-cacy or being lost to follow-up. Of the 42 patientswho completed the 1 year of follow-up, 38 (90.5%)had at least 50% reduction of pain and so can beconsidered responsive to the SCS therapy.
DISCUSSION
The lack of homogeneity in the clinical character-istics of the enrolled patients (eg, different Font-aine stages) imposes limits on the validity of theregister. However, the register has allowed us togather a variety of data and experience enablingthe evaluation of the different clinical approachesto the use of SCS in cases of PAOD that are unsuit-able for revascularization.
The results confirm those reported to date inliterature (7) with respect to the analgesic effectof SCS and the consequent improvement in thepatients’ quality of life. The reduction in the quantityof non-narcotic analgesics taken, along with thenumber and duration of hospital stays related tothe pathology, offers clear economic advantages.
The clinical results regarding the avoidance oflimb amputation at 12 months demonstrate theimportance of the timing of stimulator implanta-tion, as amputation seems to be significantlycorrelated to the clinical position at enrollment(Fig. 2). However, in order to confirm the efficacy
of SCS in terms of reducing limb amputation, itwould be necessary to compare the clinical resultsof SCS with those of the optimal medical therapyusing microcirculatory screening.
Indeed, the most recent publications (8) haveshown that there is no statistically significant dif-ference between SCS and a comparable treatmentwithout using basal transcutaneous oxygen pres-sure (9) as a predictive parameter of limb preser-vation. It is therefore to be hoped that the data inthe register can act as a starting point for random-ized and well-aimed studies to confirm the role ofSCS in saving limbs.
ACKNOWLEDGMENTS
This Register was supported and funded byMedtronic Italy.
The following centers participated in thisstudy. Azienda Ospedaliera S. Orsola-Malpighi,Chirurgia Vascolare (Prof. D’Addato), Bologna;Azienda Ospedaliera Umberto I Università di Ancona,Chirurgia Vascolare (Prof. Alò), Ancona; AziendaOspedaliera Ospedale Regionale della Valle D’Aosta,Unità Operativa di Chirurgia Vascolare e Angiologia(Dr. Peinetti), Aosta; Ospedale C. e G. Mazzone,Chirurgia Generale (Dr. Senati), Ascoli Piceno;Ospedali Moscati, Chirurgia Vascolare (Dr. Matulo),Avellino; Policlinico di Bari, Chirurgia Vascolare(Prof. Regina), Bari; Azienda Ospedaliera OspedaliCivili, Clinica Chirurgica (Prof. Giulini), Brescia;Azienda Ospedaliera di Caserta, Chirurgia Vascolare(Dr. Farina), Caserta; Azienda Ospedaliera S.S.Luigi e Currò, Terapia Antalgica (Dr. Mazzarino),Catania; Azienda Ospedaliera V. Emanuele, Fer-rarotto e S. Bambino, Angiologia (Dr. Di Salvo),Catania; Ospedali Bassini, Chirurgia Vascolare(Prof. Biasi), Cinisello Balsamo (Milano); OspedaliMaggiore di Crema, Chirurgia Vascolare (Dr. Farina),Crema (Cemona); Azienda Ospedaliera IstitutiOspitalieri di Cremona, Terapia Antalgica (Dr.S.S.A. Giannunzio), Cremona; Azienda OspedalieraS. Croce, Centro di Algologia (Dr. Menardo),Cuneo; Ospedali Civile di Feltre, Terapia Antalgica(Dr. Laterra), Feltre (Belluno); Azienda Ospedalieradi Ferrara, Chirurgia Vascolare (Dr. Mascoli), Ferrara;Azienda Ospedaliera G. Salvini, Terapia Antalgica (Dr.Zucco), Garbagnate Milanese (Milano); OspedaliCivile di Mestre, Terapia Antalgica (Dr. Pinato),Mestre (Venezia); Ospedali S. Carlo Borromeo,
Figure 3. Kaplan–Meier limb survival curve (patients withbaseline Fontaine stage III; N = 95).

102
�
TEDESCO
AND
D
’
ADDATO
Chirurgia Vascolare (Prof. Settembrini), Milano;Ospedali S. Paolo, Chirurgia Generale (Prof. Scorza),Milano; Azienda Ospedaliera Università PoliclinicoFederico II, Chirurgia Vascolare (Prof. Bracale),Napoli; Ospedali S. Antonio di Padova, Chirurgiad’Urgenza (Dr. Frasson), Padova; Azienda Osped-aliera Civico Benefratelli, Chirurgia Vascolare (Prof.Martino), Palermo; Azienda Ospedaliera PoliclinicoS. Matteo, Chirurgia Vascolare (Prof. Odero), Pavia;Azienda Ospedaliera Santa Maria degli Angeli,Terapia Antalgica (Dr. Bodi), Pordenone; AziendaOspedaliera di Reggio Calabria, Chirurgia Vasco-lare (Prof. Alberti), Reggio Calabria; AziendaOspedaliera Arcispedale S. Maria Nuova, Angiolo-gia (Dr. Paolicelli), Reggio Emilia; Ospedali degliInfermi, Terapia Antalgica (Dr. Raffaeli), Rimini;Ospedali Santa Barbara, Terapia Antalgica (Dr. Funari),Rogliano (CS); Istituto Dermopatico dell’Immaco-lata, Chirurgia Vascolare I (Prof. Camilli), ChirurgiaVascolare II (Dr. Bandiera), Roma; Ospedali Israel-itico, Angiologia (Dr. Murgiano), Roma; UniversitàCattolica, Neurochirurgia (Prof. Meglio), Roma;Azienda Ospedaliera S. Camillo, Chirurgia Vasco-lare (Prof. Rabitti), Roma; Azienda Ospedaliera Uni-versità Policlinico Umberto I, I Clinica Chirurgica(Prof. Sciacca), Chirurgia Vascolare (Prof. Fiorani),Roma; Ospedali Mauriziano Umberto I, ChirurgiaVascolare (Prof. Palombo), Torino; AziendaOspedaliera Ospedali S. Giovanni Battista, Chiru-gia Vascolare A (Prof. Ponzio), Torino; PoliclinicoG.B. Rossi, Chirurgia Vascolare (Prof. Vecchioni),Verona.
REFERENCES
1. Second European Consensus Document onchronic critical leg ischaemia.
Eur J Vasc Surg
1992;6(Suppl. A):1–32.
2. Dormandy J, Mahir M, Ascady G et al. Fate of thepatient with chronic leg ischaemia. A review article.
JCardiovasc Surg (Torino)
1989;30:50–57.3. Nachbur B, Gersbach P, Hasdemir M. Spinal
cord stimulation for unreconstructable chronic limbischaemia.
Eur J Vasc Surg
1994;8:383–388.4. Spincemaille GHJJ, de Vet HCW, Ubbink DT,
Jacobs MJHM. The results of spinal cord stimulation incritical limb ischaemia: a review.
Eur J Vasc EndovascSurg
2001;21:99–105.5. Augustinsson LE, Carlsson CA, Holm J, Jivegard
L. Epidural electric stimulation in severe limb ischemia.Pain relief, increased blood flow, and possible limb-saving effect.
Ann Surg
1985;202:104–110.6. Jacobs MJ, Jorning PJ, Beckers RCY et al. Foot
salvage and improvement of microvascular blood flowas a result of epidural spinal cord electrical stimulation.
J Vasc Surg
1990;12:354–360.7. Ubbink DT, Jacobs MJ. Spinal cord stimulation
in critical limb ischemia. A review.
Acta Chir Belg
2000;100:48–53.8. Klomp HM, Spincemaille GH, Steyerberg EW,
Habbema JD, van Urk H. Spinal-cord stimulation in crit-ical limb ischaemia: a randomised trial. ESES StudyGroup.
Lancet
1999;353:1040–1044.9. Ubbink DT, Spincemaille GHJJ, Prins MH,
Reneman RS, Jacobs MJHM. Microcirculatory investiga-tions to determine the effect of spinal cord stimulationfor critical leg ischemia: the Dutch multicenter random-ized controlled trial.
J Vasc Surg
1999;30:236–244.