
Acute Limb Ischemia. Acute Limb Ischemia: sudden decrease in or worsening of limp perfusion causing...
55
Acute Limb Ischemia
-
Upload
shanon-summers -
Category
Documents
-
view
246 -
download
3
Transcript of Acute Limb Ischemia. Acute Limb Ischemia: sudden decrease in or worsening of limp perfusion causing...

Acute Limb Ischemia
Acute Limb Ischemia:
sudden decrease in or worsening of limp perfusion causing a thread to extremity mobility and viability that has been present for less than 14 days.
There is no time for collaterals to form. may lead to irreversible tissue loss within
hours if rapid diagnosis and restoration of flow are not achieved.

Etiology:
Embolism * (the most common) Thrombsis Trauma Iatrogenic

Embolism
Translocation of material within the arterial stream to a more distal site.
80% of the emboli are cardiac in origin Or it may come from an Aneurysm Or Atherosclerotic plaques. Usually lodges at site of bifurication , most
commonly the femoral artery .
Sources of emboli:
Cardiac pathology. 80%
Atrial thrombus. (atrial fibrillation – atrial cardiac myxoma)
Ventricular thrombus. (following MI – ventricular aneurism)
Damaged valves . (RHD produce microemboli) Patent foramen ovale. (allow paradoxical
embolism to travel from venous into arterial circulation)

Proximal arterial pathology : (arterial –arterial embolism) Aneurysm (most commonly the infrarenal aorta or
popliteal arteries – may harbor a mural thrompus)
Atherosclerotic plaques. (serve as a nidus for thrombus or platelet aggregate that embolize distally – rupture discharging small debris.
In situ thrombosis:
Thrombosis of a chronically diseased vessel (most commonly SFA and popliteal A- may cause acute ischemia if collateral circulation is poorly developed )
Hypercoagulable states .(even if the arterial segment is normal – generally occurs in the more distal segments such as tibial vessels or pedal arches)

Clinical presentation: The “6 Ps” define this syndrome:
Paresthesias . The 1st to appear. (sever neural dysfunction –herald impending limp loss –an insensate limp is generally considered nonviable
Pain (acute onset – severe – unremitting-mainly unilateral )
Pallor (associated with coolness – occurs at one level below the occlusion)
Poikilothermia (coldness).
Plusless ( and usually will not have detectable Doppler signals distally because their collaterals may not be developed enough to support distal flow.
Paralysis (result as muscle function is severely compromised – heralds limp loss if blood flow is not restored promptly)

How to mange this patient:
History: Pain: onset, location, duration Hx of previous claudication Hx of cardiac disease: valvular HD, atrial fibrillation,
MI * (the commenest ptn. of acute limb ischemia) ,cardiomyopathy
Hx of recent trauma Risk factors of cardiovascular disease: (HTN – DM –
hyperlipidemia – smoking – family history)
Physical examination: Compare with contralateral extremity
involving:- Level of pulslesness .- Temperature .- Mottling .
Motor and sensory examination Cardiac Ex :rhythm , murmurs

Investigations:
Non invasive examinations:- Doppler signals .Other non invasive Ex generally are not
performed at the interest of time. Invasive procedures :
- Arteriography : to define the level of occlusion and distal reconstitution.

Treatment :
Goals : rapid restoration of blood in order to save the limb , but not on expense of life.
Strategies: ABCs Heparin: to prevent further propagation of the
thrombus. Thrombolytic therapy in selected patients. Rapid surgical restoration(revascularaization)
: thrombectomy.
Heparin therapy : initial therapy for patient with AAI, unless there is contraindication – 100 u/kg bolus then continued empirically at 1000 u/hr up to the time of surgery
Hydration : to maintain adequate urine output . Alklinazation of urine and osmotic diuresis are used to protect the kidney from damage by myoglobinuria in patient with prolonged sever ischemia

Revascularization :
Definite treatment – ideally is performed within 6h of the onset to avoid irreparable nerve and muscle damage.
Surgical therapy :the patient should be taken directly to OR following heparinization especially if motor and sensory changes are present.
Embolectomy (the procedure of choice for macroembolism to a large artery)
Bypass ( thrombosis – when adequate thromboembolectomy can not be performed)

Thrombolytic therapy:
In selected patients such as those with prior vascular intervention.
Tissue plasmiogen activator and urokinase have been used to dissolve acutely formed thrombus.
Contraindications include :Prescience of sensory and motor changes on
presentation (it requires 24h of treatment Recent surgery Known intracranial pathology

Complication of revascularization:Reperfusion injury, which has two effects:
local effect : compartment syndrome .For that reason ,fasciotomy is done with thrombectomy as
prophylactic.
Systemic effect: release of K & myoglobin.
This will lead to cardiac arrest & ARF.
Compartment syndrome:
Reperfusion injery to the muscle may result in swelling and increased compartment pressure within the facial spaces of the calf .
Pathophysiology:
Endothelial cell injury during ischemia
capillary permeability and edema
Tissue swelling after reperfusion
intracompartment pressure (more than capillary perfusion pressure – 30 mmhg)
decrease perfusion
Ischemia and myonecrosis

Clinical features:
Pain :after passive movement of the foot
Paralysis
Parasthesia
Pallor
Pulse usualy present
Diagnosis:
History
Suspicion
Measuring compartment pressure
Management :
Prevention : low threshould for faciotomy
Treatment : opening compartments via bilateral calf incision


Leg Ulceration

What is ulcer ?
Ulcer is a break through an epithelial surface .
Types of lower limb ulceration : Vascular *** Venous 70% Arterial 10% Mixed 10%
Neuropathic DM Alcohol Spina bifida
Infective Fungal TB Syphilis Leprosy
Iatrogenic Bandaging ,Casts
Neoplastic 2%BCC , SCCMelanomaMarjolin’s
LymphoedemaTraumaticVasculiticRA ,PAN
MetabolicPyoderma gangrenosum Pretibial myxoedema
Cryopathic

Venous ulcer :
The most common cause of leg ulceration is venous disease .
Two third of all leg ulcers are caused by venous disease.
Pathophysiology: Reflux (90%) Obstruction (10%)


Pathophysiology:
Reflux of venous blood will lead to venous hypertention
This in turn leads to edema and leakage of blood cells and fibrin into the tissues
This will cause discoloration and hardening of the tissues (lipodermatoscelerosis)
These tissues are then prone to injury

Pathophysiology:

Valvular incompetence resulting in reflux may occur in either :
- spuerficial veins resulting in varicose veins , or
- deep veins (e.g. DVT is a cause of deep vein incompetence)

Causes of obstruction : Pregnancy Fibroids/ovarian cysts Abdominal lymphadenopathy Pelvic cancer Iliac vein thrombosis

Evaluation
History Physical Examination Investigations
Non-invasive (Doppler/Duplex)
Invasive ( Venography)
History
History : age , sex, occupation History of leg ulcer : duration , No. of ulcers
or episodes , pain, discharge Vascular history: Hx of DVT, venous surgery,
sclerotherapy , Hx of claudication and IHD, CVA ...

Examination
Local : The leg: varicose veins , arteries and nerves the ulcer: site ( gaiter area = above the medial
malleolus), shape , size, edge (sloping), base ( usually covered with granulation tissue, depth ( usually shallow), discharge.
the surrounding tissues : usually show signs of chronic venous hypertentsion – induration and pigmentation, warmth, redness, tenderness.
General : examine the abdomen, the other leg , local lymph nodes
Investigations
Non-invasive :
Doppler ( augmentation, phasic movement), ABI (Ankle-Brachial Index)
Duplex ( compressibility, valve incompetence) Invasive :
venogram

Keys to management:
Elevation of Feet at right atrial level Dressings Compression +/- surgery
Management
In patient with venous ulcer due to superficial incompetence varicose vein surgery is effective .
In deep venous incompetence :
- local ulcer management
- application of compression

Local ulcer management
Clean the ulcer by soaking it in tap water Debride the ulcer to remove any slough no role for topical antibiotics or topical
drugs to speed the healing The most important factor in achieving
healing is the use of high levels of compression

Compression
Dressing alone is not enough It has been found that pressures of 30-45
mmHg applied to the ulcer are much more effective than lower level of compression
These can be achieved by - Compression stocking or by bandaging ( e.g.
four-layer bandaging technique)

Four- layer bandaging
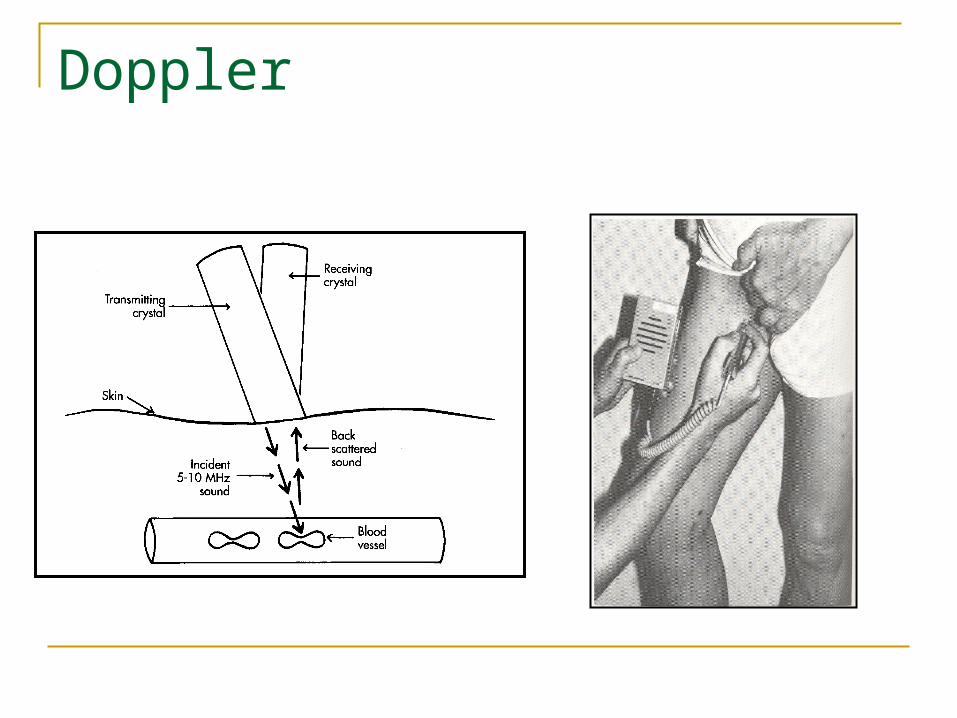
Doppler

Duplex

Compression stocking

Sclerotherapy, endovenous laser therapy (EVLT),
endovenous ablation therapy and surgery are other option to treat the
underlying cause.

surgery

Arterial Ulcers(ischemic)

Neuropathic ulcer
Occur over pressure areas Usually are deep penetrating ulcers The surrounding tissues are healthy and
have a good circulation Painless

Diabetic Neuropathic ulcer
It result from a combination of factors peripheral polyneuropathy ischemic changes due to arterial disease retardation of wound healing infection

Management
General measures : control diabetes stop smoking lose weight refer to chiropodistLocal : Treat infection with antibiotics Antiseptic and dressings Remove necrotic tissues Amputations with debridement of dead tissues until
healthy bleeding tissue is obtained

Malignant ulcers:
BCC SCC Melanoma Marjolin’s

Basal cell carcinoma ( rodent ulcer)- Locally invasive- rarely metastasizes- Found in skin exposed to sunlight- It has rolled edge- Rx : surgical excision or radiotherapy


Squamous cell carcinoma:
- It metastasize via lymphatics- Caused by exposure to sun light- Marjolin’s ulcer ?(commonly present in the context of chronic wounds including burns, venous
ulcer, ulcers from osteomyelitos, and post radiotherapy scars. )
Rx : wide excision or radiptherapy

Thank you


















