Spinal Cord Injury
37
B E T M S SPINAL CORD INJURY
description
Spinal Cord Injury Presentation
Transcript of Spinal Cord Injury
-
B E T M S
SPINAL CORD INJURY
-
Spinal Cord Anatomy and Structural Changes with SCI SCI events and natural recovery Clinical Assessment of SCI SCI Therapy
OUTLINE
-
M SPINAL CORD STRUCTURE &
FUNCTION
-
WHAT: Forms part of CNS Elongated cylinder of nervous tissue and support cells 45cm long and varying width (2 enlargements) LOCATION: Extends from the medulla oblongata of the brain Down the vertebral canal (surrounded/protected by vertebrae) Ends at 1st lumbar vertebrae (2/3 of canal) FUNCTION: Transmits sensory input from body to the brain Conducts motor impulses from brain to muscles and organs Reflex center
Intercepts sensory signals and initiates a reflex signal
SPINAL CORD
-
31 Segments: gives rise to 31 pairs of spinal nerves 4 Regions: cervical, thoracic, lumbar, and sacral 2 Enlargements: cervical, and lumbar (tapers to conus medullaris, then cauda equina) 3 meninges (fibrous CT): pia, arachnoid, dura mater
GROSS ANATOMY
-
CROSS-SECTION
Grey Matter White Matter
Neurons: cell bodies, dendrites, proximal axons Dorsal Horn: sensory neurons Interneurons: forms reflex arc Lateral Horn (T2-L1): sympathetic nervous system Ventral Horn: somatic motor neurons Central canal: ependymal cells CSF
Tracts: bundles of myelinated axons Bundles 3 pairs = columns/funiculi:
dorsal, lateral, ventral each have subdivisions = tracts/fasciculi
-
Ascending Tracts Descending Tracts Carry sensory information from the body, upwards to the brain Touch Skin temperature Pain Joint position
Carry information from the brain downwards: Initiate movement Control body functions.
-
VASCULATURE
Arteries Veins Single anterior spinal a.
Paired posterior spinal a. Arterial vasocorona (anastomoses)
Segmental/radicular a.
Anterior & posterior spinal veins Anterior & posterior radicular veins
-
SCI: LATE CHANGES IN STRUCTURE
Macroscopic Changes Microscopic Changes Lesion Reduction in spinal cord
diameter (spinal atrophy, neurodegeneration)
Formation of cysts Formation of syrinx
Loss of white matter integrity: o Wallerian degeneration: axonal degeneration, tract
demyelination o Astroglial scar o Schwannosis o Mesenchymal scar (esp. after laceration)
-
B SCI EVENTS & HEALING
-
Definition: Damage to the vertebrae, ligaments or disks of the spinal column or to the spinal cord itself.
Results nerve fibres transection and damage to surrounding tissues via secondary injury
Secondary injury responsible for continued cell death in intact tissue surrounding the site of injury
Cascade of events A. Increased activation of neuronal glutamate receptors B. Increase in calcium influx, protease activity C. Loss of mitochondrial function D. Increased free radical oxidative stress with ischaemia
and haemorrhage
LETS DEFINE SPINAL CORD INJURY!
-
Extensive loss of oligodendrocytes (following days & weeks) Via necrosis, apoptosis, and autophagy Oligodendrocyte loss and demyelination => loss of function
+ impacts functional recovery Typical of traumatic CNS lesion: Exacerbation of primary lesion
12
SPINAL CORD INJURY
-
Damage to blood vessels -> Microhemorrhage in the central gray matter
Hypoxia and ischaema -> Deprive grey and white matter of oxygen and nutrients necessary for neural cell survival and function.
Swelling rapidly occurs at the injury level, and because the bony spinal canal has a fixed diameter, pressure on the cord climbs higher than venous blood pressure.
Immediate effect = spinal shock Continued and selective cell death and demyelination in
previously intact tissue adjacent to the injury epicentre (Silver & Miller, 2004; Donnelly & Popovich, 2008)
13
SCI EVENTS AFFECTING HEALING
-
Post SCI - Inflammatory environment Causes destruction of tissue surrounding the injury Some have neuro-protective effects
Microglia and macrophages can produce protective growth factors and cytokines Limits oligodendrocyte toxicity CNS macrophages -> axon growth and regeneration.
Chronic phase of injury - loss of central grey matter in surrounding segments
Fluid-filled cyst with cerebrospinal fluid -> cavitation and cord collapse Rim of white matter surrounding injury epicentre - Accounts for
functional recovery Extent of white matter rim Remaining axonal connections (Tang et. al., 2003; Silver and Miller,
2004)
SCI EVENTS AFFECTING HEALING
-
Dural scarring - Microinjury and impaired functional recovery
Highly inflammatory environment - Glial scar formation
Majority of astrocytes hypertrophy to bolster surrounding intact neural circuits from worsening damage
Astrocytic or glial scar - limits growth of regenerating axons and can persist for extended periods depending on injury severity (Tang et. al., 2003)
Within region of forming scar tissue, axons unable to continue extending swell and distort into growth cones that can exist for years within axon tracts
Axonal connections cannot be as effectively reformed (Silver and Miller, 2004; Kwon et. al., 2002)
15
SCI EVENTS AFFECTING HEALING
-
Determined following clinical examination according to the International Standards for Neurological Classification of SCI
General prognostic indicators: Extent of injury, age and the amount of preserved spinal cord function
Greater functional preservation => Better prognosis for recovery
16
FACTORS AFFECTING PROGNOSIS
-
Of patients who present in the first 72 hours > 80% with distal
movement > 70% with no motor
strength but sensory ability (B) were able to recover to walk again (Masri, 2010)
Patients with A (Complete injury) but with pin prick sensation in a partial preservation zone recover some functional myotomes (Consortium for Spinal Cord Medication, 1999)
17
FACTORS AFFECTING PROGNOSIS
-
E CLINICAL ASSESSMENT
OF SCI
-
Prognoses based on neurological exam done by clinician 2 types of SCI Complete no motor and sensory function in sacral segments S4-5 Incomplete partial preservation of sensory and/or motor function at
S4-5 Assessment important for determining long-term prognosis
CLINICAL ASSESSMENT OF SCI
-
CLINICAL ASSESSMENT OF SCI
(Burns et al, 2011)
-
Light touch and pinprick assessed bilaterally at 28 dermatomes 0-3
Motor function assessed by bringing patients through 5 key muscle actions 0-5
CLINICAL ASSESSMENT OF SCI
-
Grade Definition
A Complete. No sensory or motor function is preserved in the sacral segments S4-5
B Incomplete. Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-5
C Incomplete. Motor function is preserved below the neurological level, and less than half of key muscles below the neurological level have a muscle grade greater than or equal to 3
D Incomplete. Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade greater than or equal to 3
E Normal. Sensory and motor functions are normal.
CLINICAL ASSESSMENT OF SCI
(Burns et al, 2011)
-
RELATIONSHIP BETWEEN TIMING OF ASSESSMENT AND PROGNOSIS
(Goodwin-Wilson, Watkins, Gardner-Elahi, 2010)
-
Evidence-based process maps for SCI rehabilitation Patient activity matched with ASIA impairment scale Shown to provide better insight to patient rehabilitation process
(Goodwin-Wilson, Watkins, Gardner-Elahi, 2010)
RELATIONSHIP BETWEEN TIMING OF ASSESSMENT AND PROGNOSIS
-
T S
THERAPY FOR SPINAL CORD INJURY
-
BONE MARROW-DERIVED MESENCHYME STEM CELLS
-
BONE MARROW-DERIVED MESENCHYME STEM CELLS
Capable of directly differentiating into neurons
Able to migrate to areas of injury and inflammation
A study of 20 SCI patients who were administrated BMMSC showed improvement in motor and sensory function in 5 out of 7 patients with acute SCI and 1 out of 13 chronic SCI patients
Not as effective in chronic spinal cord injuries and is associated with chondroitin sulfate proteoglycans
-
NEUROTROPHIN-3
-
NEUROTROPHIN-3
Useful in modulating neuronal survival, axonal growth and synaptic plasticity
It works through interaction with trk receptors
Enhancing the regeneration of damaged tissue
and is used combination with stem cell transplantation
-
Another possible avenue of treatment of spinal cord injury (SCI) involves the modification of extracellular matrix
ECM creates an environment less than optimal during SCI through the restriction of plasticity and regeneration
Chondroitin sulphate proteoglycans (CSPGs) are a component of the ECM which are detrimental to the repair of the CNS
Administration of chondroitinase ABC (ChABC), an enzyme which inhibits CSPGs has clinical potential
Genetic evidence of this was in a study involving ChABC transgenic mice with dorsal root injuries who exhibited improved function through repair of nociceptive axons
EXTRACELLULAR MATRIX MODIFICATION
-
Stem Cell: Also In a systematic review of in-vivo models only 19 out of 162
studies involved human cells, with the majority utilizing rat models (Tetzlaff et al., 2011)
NGF: No single experimental treatment can tackle all of these factors
limiting ability to augment axonal regeneration Modification of ECM: The delivery of ChABC to the CNS still has issues in its safety,
biodistribution, and thermal stability Another pitfall is the lack of larger mammals as test subjects with
the majority being rodent models.
LIMITATIONS
-
M TEAMWORK
-
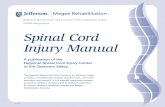
First and second years We did Belbin for personal assessment to understand the roles we
play in our group and discover any aspects we could improve.
BELBIN MODEL
Member Before After
B Team Worker, Completer Finisher Coordinator, Completer Finisher
E Monitor Evaluator, Team Worker, Shaper
Implementer, Resource Investigator, Monitor Evaluator, Team Worker
M Implementer, Team Worker, Completer Finisher
Implementer, Team Worker
S Implementer, Team Worker, Shaper, Resource Investigator
Implementer, Completer Finisher, Plant
T Plant, Team Worker, Coordinator Plant, Team Worker, Implementer, Shaper
-
Strong Team Workers and Implementers Versatile, efficient in carrying
out practical plans Consistency; the team having
a variety of roles to balance each others weaknesses
BELBIN MODEL ANALYSIS
0
10
20
30
40
50
60
70
80Implementer
Coordinator
Shaper
Plant
Resource Investigator
Monitor Evaulator
Team Worker
Completer Finisher
Before
After
-
Challenges: Getting organised, deadlines Positive: Good teamwork dynamics, efficient meetings, effective task
distribution and feedback, helping each other with understanding difficult tasks
CHALLENGES AND STRENGTHS
-
Dasari, V. R., Veeravalli, K. K., & Dinh, D. H. (2014). Mesenchymal stem cells in the treatment of spinal cord injuries: A review. World journal of stem cells,6(2), 120.
Jones, L. L., Oudega, M., Bunge, M. B., & Tuszynski, M. H. (2001). Neurotrophic factors, cellular bridges and gene therapy for spinal cord injury.The Journal of physiology, 533(1), 83-89.
Satake, K., Lou, J., & Lenke, L. G. (2004). Migration of mesenchymal stem cells through cerebrospinal fluid into injured spinal cord tissue. spine, 29(18), 1971-1979.
Skaper, S. D. (2012). The neurotrophin family of neurotrophic factors: an overview. In Neurotrophic Factors (pp. 1-12). Humana Press.
Ichim, T. E., Solano, F., Lara, F., Paris, E., Ugalde, F., Rodriguez, J. P., ... & Riordan, N. H. (2010). Feasibility of combination allogeneic stem cell therapy for spinal cord injury: a case report. Int Arch Med, 3, 30.
Burns, A. S., Marino, R. J., Flanders, A. E., & Flett, H. (2012). Clinical diagnosis and prognosis following spinal cord injury. Verhaagen, J. and mcdonald, J. W. III.(eds) handbook of clinical neurology (pp. Chapter 3) Elsevier BV
Goodwin-Wilson, C., Watkins, M., & Gardner-Elahi, C. (2009). Developing evidence-based process maps for spinal cord injury rehabilitation. Epub, 48(2), 122-127.
REFERENCES
-
Dont be spineless
Q&A
Spinal Cord InjuryOutlineSpinal Cord Structure & FunctionSpinal CordGross AnatomyCross-sectionSlide Number 7VascuLatureSCI: Late Changes in StructureSCI EVENTS & HEALINGLets define Spinal Cord Injury!SPINAL cord injurysci events affecting healingSCI EVENTS AFFECTING HEALINGSCI Events Affecting HealingFACTORS AFFECTING PROGNOSISFACTORS AFFECTING PROGNOSISClinical Assessment of SCIClinical Assessment of SCIClinical Assessment of SCIClinical Assessment of SCIClinical Assessment of SCIRelationship between timing of assessment and prognosisRelationship between timing of assessment and prognosisTherapy for Spinal Cord InjuryBone marrow-derived mesenchyme stem cells Bone marrow-derived mesenchyme stem cells Neurotrophin-3Neurotrophin-3Extracellular matrix ModificationLimitations TeamworkBelbin ModelBelbin Model AnalysisChallenges and StrengthsREFERENCEsQ&A