Special Education Department Teacher Handbook · 4 Updating and Closing IEPS on SEAS Flowchart 5...
178
Weslaco Independent School District Special Education Department Teacher Handbook Policies and Procedures
Transcript of Special Education Department Teacher Handbook · 4 Updating and Closing IEPS on SEAS Flowchart 5...

Weslaco Independent School District
Special Education Department
Teacher Handbook
Policies and Procedures

TABLE OF CONTENTS
Section Topic
1 Starting the New School Year (Beginning of the school year procedures)
Teacher Checklist Where do I Begin?
• Getting Started • Coordination of Services
2 ARD / IEP Procedures/Description
Notice of Procedural Safeguards Notice of ARD Meetings ARD meeting without parents Member of ARD Committee Timelines Requirements for Annual ARD Meetings ARDs by Special Education Teachers / ARDs by
Educational Diagnosticians ARD Committee Meeting Agenda Introductions Checklist Purpose of IEP PEIMS Sheet Present Level of Performance of Academic Achievement
and Functional Performance (PLAAFP) Goals & Objectives Components of a Measurable Goal Assessment Decision Determination of Placement Assurances Read and Approve Minutes / Conclusion Prior Written Notice / Notice of Proposal/Refusal Procedures to Follow During Non-Consensus ARD
10 Day ARD 3 Updating Goals, Objectives, and IEP Progress Report / Closing IEPS
4 Updating and Closing IEPS on SEAS Flowchart
5 Extended School Year (ESY) Services
Extended School Year Services for Students with Disabilities
ARD/IEP Supplement – Extended School Year Services Found on SEAS

6 Modified Exit Criteria from Bilingual or ESL Services Process for Considering Special Exit Criteria from
Bilingual/English as a Second Language (ESL) Services WISD – Review and Recommendation of Exit Criteria
7 Secondary Student Education Needs
Transition Planning/Services Transfer of Rights Secondary Graduation Plan Graduation ARD Summary of Academic Achievement and Functional
Performance Secondary Functional Vocational Evaluation
8 Amendments to ARD Meetings (Agreement to Change) 9 Implementation of Accommodations/Modification Coordination with Regular Teacher
10 Procedures for Transfer Students
11 Request to Exit Student from Special Education Program
12 Parent / Student Rights (Confidentiality)
Confidentiality Memorandum Discussing Confidentiality Parents/Student Right
13 Functional Behavior Assessment
14 SHARS (School Health and Related Services) SHARS Procedures Consent to Release Personally Identifiable Information & Access
Medicaid Reimbursement (English and Spanish) Annual Notice of Intent to Access Medicaid Reimbursement Evaluation Report: School Health Services (SEAS)
15 Child Find Overview 16 Related Services 17 Assistive Technology 18 Private School Consultation

19 Procedures for Independent Educational Evaluation 20 Foster Parent/ Surrogate Parents 21 Food Preparation 22 Purchasing Material 23 Terminology
Common Acronyms Used in Special Education Glossary of Special Education Terms Glossary of Special Education Personnel
24 Attachments
***Attachments can be downloaded from the Weslaco ISD Website and found at the end of this manual.

Section 1

Revised 8/1/16
Teacher Checklist
CALENDAR OF COMPLETION DATES FOR THE FOLLOWING
FORMS AND ATTACHMENTS
Form / Attachment Completion Date Submit To
Teacher’s Student Folder Monitoring List (Attachment C) August 31st Ed. Diag.
Student Information/PEIMS Verification (Attachment R) September 30th Ed. Diag.
Receipt of Required Special Education Documentation September 16th Ed. Diag. (Procedural Safeguards - April 2016 - SEAS) * Medicaid Forms - refer to Medicaid Procedures Consent to Release Personally Identifiable *September 16th Information & Access Medicaid Reimbursement Only For Notices Ed Diag. (Must be provided in Parent Language) not secured and all New to District, & Initials OR Annual Notice of Intent to Access Medicaid *September 16th Ed Diag. Reimbursement Copy of Annual Notice (Must be provided in Parent Language)
Parent Language Preference (Attachment A) September 16th Filed in Campus Folder
Accommodations Folder Beginning of Year Stored at Campus
Verification of Receipt (Attachment N) Beginning of Year
Coordination Cover Sheet (Attachment L) Beginning of Year
Coordination of Services (Attachment M) Every 6 Weeks (EOY – campus folder)
Content Mastery Log (Attachment E) Ongoing - School Year Filed in Campus Folder
Inclusion Log (Attachment E) Ongoing - School Year Filed in Campus Folder
ARD Progress Report (Attachment B) Prior to ARD Turn in with ARD

Revised 8/1/16
Teacher Checklist
Transition (Secondary) – Forms will be submitted with ARD Packet
Form / Attachment Due Date/Timeline
Consent for Disclosure of Confidential Information To be submitted with annual
for Transition (Attachment Fc) paperwork
Receipt of Brochures (Attachment F) Beginning of Year (updated annually)
Student Interview (Attachment G) Prior to age of 14 (updated annually)
Functional Vocational Assessment/Teacher Obs. Checklist Prior to age of 14 (updated annually)
(Attachment H)
Invitation to Agency (Attachment I) Send out after the Consent for
Disclosure of Confidential Information
for Transition services has been
secured.
Information Regarding Transfer of Parental Rights at age Prior to turning 18 (secured during 9th
of Majority (SEAS) grade - updated annually)
Notification of Transfer of Parental Rights at Age of Majority After age 18 – (updated annually)
(SEAS)

WHERE DO I BEGIN??
A. Getting Started
1. Pick up a campus roster from your educational diagnostician. (Refer to Section 3 to help you understand disability and instructional setting codes)
2. After determining monitoring special education teacher for all students on the roster, the Monitoring teachers will complete the Student Information/PEIMS Verification form (Attachment R).
• Monitor teacher is responsible for maintaining the student's folder and making sure student has a current annual at all times, including current IEP(s), modifications, BIP, schedule of services, etc.
• Review each student folder, including the additional comments page of last two ARDs for any pending assessments, and/or additional information as indicated by the previous ARD committee members
• Notify diagnostician of any discrepancies/ problems so that corrections can be made accordingly.
• Refer to the projected calendar due date contained in this section as to when this form must be given to the Educational Diagnostician.
3. Get an alpha list of your students on your campus from the campus attendance clerk.
• Look for each student on your roster and note who his/her homeroom teacher is. • Ensure that necessary special education services are provided immediately. • Ensure you have the correct student by checking his date of birth and/or ID number.
4. Ask each student's homeroom teacher for his/her daily schedule (Attachment J). It will probably be tentative, but so will your schedule at this point. You may need to move students around when you find out what time works best for the student, teacher, and you.
5. Take the general education teacher schedules and fit-in students on the Daily Schedule form (Attachment K). Schedule the student for the subject(s) he/she is to be served. This schedule should also include students who are to be served in a content mastery or mainstream arrangement.
6. Create a coordination folder for each student. (See Part B, next page)
7. Ensure that each student's special education folder has a contact log (Attachment P) and Record of Confidentiality (Attachment Q). • Use the Contact Log to document each time you contact parents: For Example: home visit,
telephone calls, notices, etc. At the end of the year, the original contact logs will be picked up and filed in the student’s eligibility folder at the Special Education Office.
• The Record of Confidentiality needs to be signed by any person who has a legitimate educational reason to view the student’s information. Form will be filed remain in the student folder.

B. COORDINATION OF SERVICES
1. Create a Coordination Folder for each of your students with a copy of Attachments L and M.
2. Each of the student's general education/electives teachers who need to modify instruction will need to be provided with a coordination folder. You will need to include in this folder:
• A copy of Coordination of Service form (Attachment L & M) • Copies of current Modifications • Copies of current IEPs • The Additional Comments page if it contains pertinent information (use your judgment) • Behavior Intervention Plan (BIP) if necessary. Give a copy of the BIP to the
administrator(s).
3. Arrange to meet with each general education teacher (or cluster of special education teachers) give them their Coordination Folder. Each general education teacher receiving a folder must sign Attachment N – Verification of Receipt. Keep Attachment N in safe place as it may need to be referred to at a later date.
• Communication is the key for working with general education teachers to meet students' special needs.
• Item #2 and #3 above will be repeated each time the ARD committee changes any of the items in #2.
*Please complete Coordination of Services Attachment M at the end of each six weeks grading period. Review it to make sure the student is making progress both in his/her special education and general education classes. If student is NOT showing adequate progress, consult with your Diagnostician. Attachment M will be picked up at the end of the school year.

Section 2

Notice of Procedural Safeguards
We are required to provide parents with a copy of the Notice of Procedural Safeguards only one time a school year, except that the school must provide the copy of the document upon initial referral or the parent/adult student’s request for evaluation; upon receipt of the first special education complaint filed with the TEA; upon receipt of the first due process hearing complaint in a school year; when a decision is made to take disciplinary action that constitutes a change of placement; or upon the request of the parent or adult student. The requirement to provide the Notice of Procedural Safeguards on an annual basis can be met in one of two manners. Teachers who are the case managers can opt to send the parent/adult student a copy of the Procedural Safeguards at the beginning of the year, or the teachers can opt to provide a copy at the Annual ARD Meeting. In addition to the outlined instances, it is best practice to provide a copy of the Procedural Safeguards when a non-consensus ARD Meeting is held or upon parental request to exit the student from the Special Education Program.

Notice of ARD Meetings
• ARD meetings must be set up at a mutually convenient time for the school and the parent.
• It is understood, that when an ARD meeting cannot be attended by the parent during the regular school hours that school personnel try, within reason, accommodating the parent.
• Notice of ARD meetings must be accompanied with a notice of procedural safeguards.
• Notice of ARD meetings must be received by the parent at least 5 school days prior to the scheduled ARD meeting. This will allow for parents to make arrangements to attend.
• Always keep a copy of the ARD notice, as one must be turned in with the ARD paperwork.
• ARD meetings cannot be held without the parent being provided with a notice of an ARD meeting at least five school days prior to the meeting. The exception to this is when parents waive their right to receive this notice within the required time frame. In this event, the parent must indicate in writing on the notice of ARD, that they are waiving their right to receive the notice five school days prior to the meeting. This should be the rule rather than the exception.

ARD Meetings without Parents
• The following procedure is recommended in order to help ensure parental participation at an ARD meeting: Parents must receive notice at least five school days prior to the meeting; Send a copy of the ARD notice with the student; Send a copy of the ARD notice through the mail; Follow up with a phone call; if needed, follow up with a home visit.
• Always document on the ARD notice all of the methods utilized to convince the parent to attend the ARD meeting.
• If the parent has indicated to have the meeting without them, make sure that a signed invitation has been secured and indicates in writing that the parent has requested that the meeting be held without them.
• If you do not hear back from the parent by the time of the ARD meeting, strongly consider rescheduling the meeting. Meetings can be held without parents only when we are certain that they were properly notified. In this event the law requires us to document our efforts to convince the parent to attend the ARD meeting.
• If rescheduling the meeting, another notice of ARD meeting must be sent. Once again, the parent must receive the notice at least five school days prior to the meeting.
• The same procedures to ensure parental participation as stated above should be followed and documented.
• A viable option for obtaining parental participation could include participation via conference call.
Members of the ARD Committee
The following are the members of the ARD committee:
• Representative of the Local Education Agency (Principal, or Assistant Principal)
• Parent/Adult Student • Representative of Regular Education Instruction • Representative of Special Education Instruction • Someone who can interpret the instructional implications of assessment (the person
who fills this role is contingent upon the nature of the assessment being reviewed)
• LP AC representative (if student is receiving bilingual instruction, or being monitored by the bilingual program)
• Career and Technology representative (if the student is in, or being considered for enrollment in a CATE course)
• Any individual that the district distinguished as having any special knowledge or expertise regarding the child, such as a service provider.
• Any individual invited by the parent. • Student of any age (whose ARD committees are discussing the provision of
transition services).
• Some individuals may serve dual roles on the ARD committee. For instance, a representative of special education instruction can also double as the individual who can interpret the instructional implications of assessment Again this depends on the nature of the assessment being discussed.
• It is important to remember to ensure that all required members are present and sign the ARD document.

Timeline Requirements for Annual ARD Meetings
• As per state and federal regulations, annual ARD meetings must be held at least once a year. A year is defined as 365 days.
• All annuals must be held on or before the anniversary date of the previous year’s meeting.
• In order to ensure compliance that timeline requirements are met, it is recommended that Annual ARD meetings be scheduled at least four to six weeks prior to the anniversary date.

SPECIAL EDUCATION TEACHERS MAY CONDUCT THE FOLLOWING ARDS
These include: • Annual ARD • Change of Instructional Arrangement ARDs (long ARD must be used to discuss
LRE) For example: resource to self-contained, mainstream to resource, etc. • Brief ARD
Examples when to use a Brief Form may include:
• Developing and implementing new lEP's • Transportation • Change of Schedule or Services (without changing instructional arrangement) • Add/Drop Modifications • Address issues affecting student progress • State Assessment • FBA / BIP development • Vocational IEP • Transition
Note: if you have any questions, please do not hesitate to contact your diagnostician
DIAGNOSTICIANS ARE REQUIRED TO PRESENT AT THE FOLLOWING ARDs
• Initials • 3 year re-evaluations • Manifestation, including change of placement
• Dismissals • Graduation • Temporary Placement ARDs (Transfers) • Permanent Placement ARDs • And any other ARD where formal evaluations will be discussed
8/12

ADMISSION, REVIEW, & DISMISSAL (ARD) MEETING AGENDA
1. Introductions 2. Statement of Confidentiality and Conduct:
All information concerning a student with disabilities is confidential and may not be discussed with anyone except those who have a legitimate educational interest in the student with disabilities. Consistent with school board policy, persons participating in the ARD meeting will refrain from making any personal attacks on school staff, students, or parents. All participants are expected to speak in a courteous manner and in a conversational tone. This expectation must be followed in order to facilitate a safe, collaborative environment focused on the development of appropriate educational plans for this student.
3. Purpose of ARD Meeting
4. Review of Assessment Data to include performance on state mandated tests such as STAAR, STAAR-A, STAAR Alt. etc.
5. Determination of Eligibility 6. Consideration of Special Factors: Limited English Proficient, Blind or Visual Impairment, Assistive Technology, Deaf or Hard of Hearing, Autism. 7. Review of Present Level of Academic Achievement and Functional Performance (PLAAFPs)
8. Develop Goals & Objectives based on PLAAFPs. 9. Accommodations/Modifications
10. Assessment recommendations for benchmark and state mandated tests to include TELPAS as well as allowable accommodations.
11. LRE; Determination of Placement; Services to be provided to include related services. 12. ESY Determination
13. Administrator Assurances 14. Read and Approve Minutes.
15. Signatures ** All steps may not apply to every ARD Meeting 7/16

Introductions Checklist
Who is chairing the ARD?
Have everyone introduce themselves
Pass around a sign in sheet to get everyone's name and position.
Will parent be taping the ARD? Will school be taping the ARD?
Remind everyone that the minutes are being taken and not everyone can talk at one time.
Is there a time limit?
Note for the record one of the following:
a. Parent received notice of the ARD timely, agreed to attend and is
present at the ARD. b. Parent waived 5 days notice requirement, agreed to attend and is
present at the ARD. b. Parent was notified, could not attend, yet gave permission for the
committee to convene. A copy of the ARD paperwork and Notice of Proposal/Refusal is sent toParent/guardian/adult student, who is advised to review the action proposed and contact the school immediately if there is a question. If Change of Placement is initiated, a copy of the Procedural Safeguards will also be attached.
c. Participated in the ARD via conference call or telephone call from representative at the meeting.
e. Was notified _______ times yet did not respond. List dates of ARD Notices. With documentation of reasonable notice, the committee convened in the absence of the Parent/guardian/adult student. A copy of the ARD is being sent to the Parent/guardian/adult student, who is advised to review the action proposed and contact the school immediately if there is a question. If Change of Placement is initiated, a copy of the Procedural Safeguards will also be attached.
Parent received a copy of the due process rights booklet
8/12

PEIMS SHEET
PURPOSE:
The PEIMS sheet is a concise way of reporting the special education service(s) to be provided to a student eligible to receive such services. The information that you include on the PEIMS sheet is inputted into the school district's computer system (SunGard) by the Special Education PEIMS (Public Education Information Management System) Clerk. The information is then used to generate:
• Campus rosters • Special Education class rosters
NOTE: Rosters contain information pertaining to the student's handicapping conditions, instructional arrangements, related services, etc.
PEIMS REPORTS:
• are submitted to the Texas Education Agency for compliance monitoring and as basis for funding.
• are reported to the Federal Government (which in turn brings in federal funding).
All of the information that is submitted on the PEIMS sheet must be accurate. Refer to the ensuing pages for information regarding disability and instructional settings codes.
8/12

Present Level of Performance of Academic Achievement and Functional Performance (PLAAFP)
• All IEPs must contain a statement about the child’s present levels of academic achievement and functional performance. The PLAAFP is a statement of how the child’s disability affects the child’s involvement and progress in the general education setting; or how the disability affects the preschool child’s participation in appropriate activities.
• The PLAAFP must be a narrative statement. It must include supports/accommodations/
modifications that the child may need. The statement should also include some of the competencies that the student possesses.
• The PLAAFP statement must address any academic and/or non-academic area that is being
impacted by the student’s disability.
• When writing a PLAAFP do not forget to include information regarding a student’s functional performance.
• Include things the student is able to do for themselves, as well as things that they may not be
able to do for themselves.
• For some students, statements could be written about the punctuality of the student in attending class, whether the student brings their materials to class, whether the student participates in class, whether the student is able to advocate for himself/herself, whether the student is able to stay on task, how the student gets along with others, etc.
• Sources of data for the PLAAFP statements may include, but are not limited to observations,
work samples, teacher information, review of test scores, progress reports from regular education teachers, etc.
• When completed, check the PLAAFP for the following:
1. Is it a narrative statement? 2. Did it include competencies as well as areas of concern for the student in academic
and functional areas? 3. Did it include supports/accommodations/modifications needed by the student? 4. Did it include a statement of the student’s functional performance?
• There must be a correlation between the PLAAFP, the goals and objectives, recommended
assessments, and the special education service(s) that the student receives. Areas of concern noted on the PLAFFP should be addressed as a goal/objective.
7/16
Goals and Objectives
Note: In this section, IEP refers to the individualized goals and objectives, not to the entire ARD packet
Definition
A statement of measurable annual goals, including academic and functional goals designed to...
• Meet the child's needs that result from the child's disability to enable the child to be involved in and progress in and progress in the general curriculum;
• And meet each of the child's other educational needs that result from the child's disability.
IDEA-IA of 2004
The special education teacher will present to the ARD committee proposed goals and objectives for the members to consider. At the ARD meeting the drafted goals and objectives will be edited and/or rewritten to reflect the parents' and other committee members concerns about the student's educational needs.
Annual Goals
Annual goals are to be written in measurable and observable terms in the area of educational needs to determine educational priorities which the student may reasonably be expected to accomplish/master.
Annual goals are to be individualized to meet each student's needs.
Goals are to reflect TEKS Objectives, or in the case of a very small number of individuals with significant cognitive disabilities, pre-requisites to TEKS objectives.
Short Term Objectives
Short term objectives are required for students who take assessments based on alternate achievement standards.
Reminder: Progress of students on goals and objectives must be monitored and updated as often as determined by ARD committee.
8/12

Components of a Measurable Goal
All written goals and any short-term objectives must be written in a measurable manner. To be measurable one must be able to observe and or count the behavior that we is expected. For instance if it is stated that a student will solve single digit addition problems, the student can be provided with single digit addition problems and observe whether the problems were solved. Contrast that with writing a goal that states that a student will improve a skill or will show appreciation for something. The behavior of improving or showing appreciation cannot be measured. For a goal to be measurable it must include the following components:
1. Time Frame – within 36 instructional weeks
2. Condition – the circumstance and or support to be provided to the student. a. For example: when provided with a calculator
and a set of problems.
3. Behavior – What we expect the student to accomplish. b. For example: Solve a problem, read a
paragraph, write an essay.
4. Criterion – the expected that we have. c. For example:
complete with 70% master . complete 7 out of 10 trials.
Example of a Measurable Goal Within 36 instructional weeks when provided with a word list and a word bank, Johnny will write a three paragraph essay on eight out of ten occasions.
8/12

Assessment Decisions
All assessment decisions are to be made in accordance with the policies, procedures and criteria outlined by the Texas Education Assessment Agency. Participation of students with disabilities on all district and state-mandated assessments must be considered. If students will not be participating on certain assessments, ARD Committees must provide a rationale for non-participation, as well as selecting the manner in which the student will be assessed and providing a reason as to why that assessment is most appropriate. Once students are in 3rd grade and beyond, the assessment options available are the following: STAAR, STAAR-A, and STAAR Alternate. The first consideration for participation always begins with the regular assessment either with or without accommodations. The only students who are to take either a STAAR Alternate assessment are those that meet every single outlined participation criteria. It is the student’s ARD committee, taking into account the type of instruction and supports that the student is receiving, that determines the assessment which the student will be participating on. If the student’s ARD committee determines that the student will be participating on an assessment based on alternate achievement standards, the IEP must provide written confirmation that the student meets all of the participation criteria for that particular assessment. In addition, the IEP must contain evidence that the student is receiving instruction based on pre-requisite skills and based on an alternate curriculum. This evidence must be contained in the Present Levels of Academic Achievement and Functional Performance (PLAAFP) statement, which must clearly establish that the student is receiving instruction based on pre-requisite skills/alternate curriculum. In addition, the PLAAFP statement should clearly spell out the supports needed by the students which necessitate them taking a test based on alternate achievement standards. If the student will be participating on an alternate test, there must be goals and short-term objectives in that particular subject area which clearly delineate the pre-requisite skills that the student is receiving instruction in. To ensure that appropriate assessment decisions are being made, Special Education personnel will provide annual training on the ARD Decision Making Process. Currently, the Every Student Succeeds Act (ESSA), only allows for 1 percent of District’s eligible test takers to take a STAAR-Alt.

7/16
Determination of Placement
The student's instructional arrangement is largely based on a comparison of regular vs. special education time. **** Get acknowledgement from parent and committee that the committee including the parents agrees with placement. (40) Mainstream (no scheduled pull-out services) (41) Resource room/service - less than 21% (42) Resource room/service - more than 21% but less than 50% (43) Self Contained, mild and moderate, regular campus - at least 50% and not more than 60% (44) Self Contained, mild and moderate, regular campus- more than 60% (45) Full Time Early Childhood
(0) Speech (1) Homebound (2) Hospital class
(8) Vocational Adjustments class (9) Community Class Off home campus Residential Other For a more detailed explanation of instructional arrangements please contact Educational Diagnostician assigned to your campus, Orfelinda Tamez (PEIMS Clerk) or Neil D. Garza (Special Education Director).
08/12

ASSURANCES
The representative of the Local Education Agency, either the principal or assistant principal must read the assurances.
8/12

READ AND APPROVE MINUTES
Ask the diagnostician to read the minutes and we can correct them as necessary.
• Correct anything that needs to be changed as the scribe is reading the minutes.
• Enter into the minutes that changes were made and minutes were approved.
CONCLUSIONS
• Make sure parents have signed any other forms - like consents, etc.
• Check if consensus was reached with parent. If not a 10 day recess must he offered.
• Make sure everyone signed the IEP. Also check to see if anyone disagreed. If there is any disagreement among anyone other than the parents, the member of the ARD who is not in agreement must provide a written statement indicating why they disagree.
8/12

Prior Written Notices / Notice of Proposal/Refusal
The law calls for Prior Written Notices to be sent under the following circumstances
• Before proposing to initiate or change the identification of the child; • Before proposing to initiate or change the evaluation of the child; • Before proposing or refusing to initiate or change the provision of FAPE to the child; • Before ceasing the provision of special education and related services due to the
parent’s revocation of consent for services; or • Before implementing an IEP with which the parent or adult student disagrees; • Before convening an ARD Meeting (This is accomplished through the notice of ARD
meeting). Prior written notice must be sent regardless of whether the parent agreed to the change or requested the change. After the completion of an ARD meeting, a Prior Written Notice must be provided to the parent informing them of the proceedings and decisions of the ARD committee. The Prior Written Notice will inform the parents of what was proposed or rejected, why the action was proposed or rejected, which options were considered as well as why those options were rejected, the sources of data that helped the ARD committee in reaching their determination and any other relevant factors to the proposal. Prior to the ARD recommendations being carried out, the parents must receive written notification of the proposed changes five school days before the actual change, unless the parents agree otherwise.
8/12

Procedures to follow for a Non-Consensus ARD
• Should an ARD Meeting end in non-consensus attempt to clarify all the points of agreement (this should be documented in the deliberations)
• The deliberations should also document the point(s) with which there is non-consensus.
• Offer the parent the ability to provide a written statement outlining what forms the basis for their disagreement.
• Offer and document that a ten day recess was offered to the parent. The parent does not have to accept the offer to recess and reconvene the ARD within ten business days. The recess is meant to allow each party to consult with additional resources, as well as to allow for reconsideration on both parts.
• Both the parent and the Local Education Agency (LEA) can mutually agree to reconvene the ARD Committee after ten business days. If the parent decides to accept and reconvene the ARD Committee, make certain to document the agreed time, date and location of when the ARD Committee will be reconvened.
• Document on the deliberations that a ten day recess was offered. • Provide and document that Procedural Safeguards was provided by the
parent. • Should the parent opt not to recess the ARD Meeting, which is their right,
explain that the LEA will implement the IEP as determined by the majority of the ARD Committee. A Notice of Proposal/Refusal must then be sent to the parent informing them of the proposed or refused action that the ARD will be following/implementing.
7/16
Section 3

Updating of Goals/Objectives and IEP Progress Reports
• All teachers and service providers are responsible for updating progress on student’s goals and objectives pages. The law requires for Districts to report to parents the progress that students are making toward meeting their annual goals. This must occur on the same timely basis that is provided to parents of non-disabled children and may occur con-currently with report cards.
• This will be done by sending to the parent a copy of the student’s goals/objectives page which contains a brief written statement indicating the progress that the student has made towards meeting the annual goal.
• A brief statement will be written in the boxes located at the right hand portion of the goals and objectives page indicating student progress made towards the annual goal.
• The monitoring teacher is responsible for securing the IEP Progress Reports from other special education and the related service providers and sending home a copy.
• An original of the progress noted on the goals and objectives page must be kept as proof that progress reports have been sent.
• Remember to also complete the portion at the bottom of the goals/objectives page indicating whether the progress that the student is making to date is sufficient to enable him/her to achieve their measureable goal(s) by the end of the IEP year. Also, indicate on the Parental Notification Statement (also located at the bottom portion of the goals/objectives page) how often written IEP progress reports will be provided to the parent.

Closing IEPs (Goals and Objectives)
1. When closing goals and objectives at the end of the IEP year, mastery or non-mastery of goals and objectives can be documented in the following manner:
a) If mastered, write Mastered. b) If not mastered, and the teacher chooses to continue teaching the objective,
write Continued. c) If not mastered, and the teacher feels the objective is inappropriate to
continue teaching, write Discontinued.
Periodic Reports on the progress the child is making toward meeting the annual goals must be provided to parents. This is done as often as determined appropriate by ARD committee.

Section 4

UPDATING AND CLOSING IEP’s/PROGRESS REPORTS
RELATED SERVICE STAFF AND TEACHERS WILL FILE THEIR OWN IEP’S. There are two options for closing IEP’s which option you select depends on the information that is currently in SEAS. Please read these steps carefully and select the appropriate option.
Step 1: Go to MAIN MENU and select File/Archive Documents. Step 2: Search for Student using the search tools at top of page. Step 3: Once student’s filed and archived records appear look for a FILED IEP Goal Only Pages or IEP
Goals and Objectives Pages. If a FILED goal page does exist then go to Step 4 (A) and FOLLOW (A) UNTIL STEPS ARE COMPLETED. If a FILED goal page does not exist then go to Step 4 (B) and FOLLOW (B) UNTIL STEPS ARE COMPLETED.
(A) (B)
Step: 4 Open the FILED Goal Only or Goals and Objectives page
Step: 4 Go to Main Menu and Select IEP
Step 5: Review IEP’s complete progress report sections.
Step 5: Go to Create/Update Goal Only or Goal and Objectives as needed per student.
Step 6: Click on SAVE and Review the name and date of the FILED/ARCHIVE List follow Step 7 (A) for correct format for name and date of closed IEP.
Step 6: If not already in students file search for student name using search tools at top of screen.
Step 7: Click on FILE: Closed IEPs should be NAMED in this format “CLOSED IEPs, TYPE OF ARD, ARD DATE” Example: CLOSED IEPS ANNUAL 9/24/2011. Closed IEPs should be DATED on the date of the ARD.
Step 7: Click on View previous Goal Areas and Open IEP to Update and or Close IEP/Progress Reports
Step 8: Teachers will notify diagnostician via email when ARD packets are complete and include statement when the IEPs/ Progress reports have been updated and closed.
Step 8: Click on FILE: Closed IEPs should be NAMED in this format “CLOSED IEPs, TYPE OF ARD, ARD DATE” Example: CLOSED IEPS ANNUAL 9/24/2011. Closed IEPs should be DATED on the date of the ARD.
Step 9: Diagnosticians will ARCHIVE.
Step 9: Verify that Goal/Progress is Successfully filed at bottom of page in BLUE.
Step 10: Click on EXIT.
Step 11: Go to MAIN MENU and select File/Archive Documents.
Step 12: Search for Student using the search tools at top of page.
Step 13: Open the FILED Goal Only or Goals and Objectives page.
Step 14: Review IEPs complete progress report sections.
Step 15: Click on FILE: Closed IEPs should be NAMED in this format “CLOSED IEPs, TYPE OF ARD, ARD DATE” Example: CLOSED IEPS ANNUAL 9/24/2011. Closed IEPs should be DATED on the date of the ARD.
Step 16: Teachers will notify diagnostician via email when ARD packets are complete and include statement when the IEPs/ Progress reports have been updated and closed.
Step 17: Diagnosticians will ARCHIVE.
IEP may have been accepted in another ARD besides the Annual.
IEP may have been accepted in another ARD besides the Annual.

MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Rectangle
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
of ARD
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text
Section 5

Extended School Year Services for Students with Disabilities
Background
Since 2000, Texas bas followed the OSEP Continuous Improvement Monitoring Process (CIMP), which is designed to assess, on an ongoing basis, the impact and effectiveness of state and local efforts in providing early intervention services to infants and toddlers with disabilities and their &milies, and a fiee appropriate public education to children and youth with disabilities. During the spring of 2002, the U.S. Department of Education Office of Special Education Programs (OSEP) monitored the state of Texas.
In 2003, the Texas Education Agency received the OSEP Monitoring Report which outlined the specific areas of noncompliance, strengths, and suggested areas of improvement for the Individuals with Disabilities Education Act (IDEA)-B (ages 3-21) and IDEA-C (ages o-3) programs in the state of Texas. The provision of extended school year (ESY) services was identified . as an area of noncompliance for the State.
An Improvement Pbmning Task Force met to review the State's current guidance reganling ESY services and determine a desired result. Additicmally, this task force discussed the action needed by the State to achieve tbis result.
The ongoing improvement and planning activities, in response to the federal monitoring process, is referred to as the Texas Continuous Improvement Process (TCIP). Using the TCIP, the State submitted an Improvement Plan in response to the OSEP Monitoring Report. It addresses areas of improvement identified during the self-assessment, validation planning (public meeting), and validation data collection ( onsite visit) phases of the process.
An overview of the CIMP, TCIP, the Self Assessment, the Texas Monitoring Report and the Improvement Plan may be found on the web at:
http://www .tea.state.tx.us/special.edlcimp/
Texas Education A/;ltJnc'/ 1 Spedal Education Sprlng2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

One of the greatest challenges currently facing Texas in regard to the delivery of services for students with disabilities is the prevalence of inconsistent and inaccurate information. The purpose of this document is to provide information and guidance to parents, district staff; and other interested stakeholders regarding the provision of extended school year (ESY) services. It is intended to address the identified Improvement Area in the State.
The document includes:
• A Definition ofESY Services
• Legal References Regarding ESY Services (Federal and State)
• Areas oflmprovement Identified for ESY Through the OSEP Continuous Improvement Monitoring Process
• State Result Developed Through the Texas Continuous Improvement Process
• Action Needed to Ensure the State Meets the Identified Result
Definition of ESY Services
Esteadecl School Year Servlces-iiD individualized instructional progmm for eligible students with disabilities that are provided beyond the regulai school year. The need for ESY services must be determined on an individual basis by the admission, review, and dismissal (ARD) committee.
Some students with disabilities have difficulty retaining skills dming long school holidays and/or summer. If a student requires a significant amount of time to recoup mastered skills, then the ARD committee should discuss whether the student needs extended educational and/or related services during school breaks.
The determination of whether a child will receive ESY services will be made by the ARD committee; and the individualized education program (IEP) developed for ESY must include goals and objectives.
TEA I Special Education tdlp:l/wWW tea.stata.tx.uslapedal.edl
2 State Rasaurca: ESY Services Sprtng2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle
e Legal References Regarding ESY Services I Federal Regnlations
e
e
. IDdlviduals with DlsabUltla Edueatloa Aet (34 CF'R Part 300)
§300.309. Extended Hllool year semees.
(a) General.
(1) Each public agency shall ensure that extended school year services are available as necessary to provide F APE, consistent with paragraph (aX2) oftbis section.
(2) Extended school year services must be provided only if a child's IEP team detennines, on aa individual basis, in accordance with §§300.340-300350, that the services are necessary for the provision ofF APE to the child
(3) In implementing the requirements oftbis section, a public agency may not--
(i) Limit extended school year services to particular categories of disability; or
(ii) Unilataally limit the type, amount, or duration of those services.
(b) Definition. As used in this section, the term extended school year services means special education and related services tbat-
(1) An: provided to a child with a disab~-
(i) Beyond the normal school year of the public agc:ncy;
(ii) In acccmlaDce with the child's IEP; and
(iii) At-no cost to the panmts of the child; and
(2) Meet the standards of1he SEA.
§300.24. Related servlces. (aeerpt)
(a) Oeneml. As used in this part, the term related services means 1raDspottation and such developmental, corrective, and other supportive services as are required to assist a child witb a disability to benefit fiom special education, and includes speech-language pa1hology and audiology services, psychological services, physical and occupational therapy, mnation, including therapeutic recreation, early identification and assessment of disabilities in children, counseling services, includiDg rehabilitation counseling, orientation aud mobili11 services, and medical services for diagnostic or evaluation purposes. 'lbc tenD also includes sdaool health services, social work services in schoo~ and parent counseling and training.
(b) Individual terms defined. The terms usccl in this definition are defined as follows:
(IS) Transportation include&-
(i) Travel to and &om school and between schools;
(ii) Travel in and around school buildings; and
(iii) Specialized equipment (such as special or adapted buses, lifts, and ramps), if required to provide special transportation for a child with a disability.
'lbc docmnent Tems SpecitJI Edtlcatlon Rules tmd Regulations, which includes special education related federal regulations, state laws and rules,
can be found on the Web at:
httpllwww.tea.state.tx.uslspecial.edlruleslsbs.html
TEA I Special Education htlp:J/www.taa.atata.tx.UIIipeCial.fJAJJ
3 S1at8 Relourat: ESY ServlcDs Sprtng2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

- Legal References Regarding ESY Services I State Rules
Teus Admllllstntive Code (fAC) Title 19, Cbapter 89. Adaptations for Special Populations, Subebapter AA: Commissioner's Rules ConeeraiDg Speelal Education Services
§89.1065. Emaded Sdlool Year Services (ESY Services).
Extended school year (ESY) services are defined as individualized instructional programs beyond the regular school year for eligible students with disabilities.
(I) The need for ESY services must be determined on an individual student basis by the admission, review, and dismissal (ARD) COJiliDittee in acconlance with 34 Code ofFederal Regulations (CFR.), §300.309, and the provisions of this section. In detamining the need for and in providing ESY services, a school district may not
(A) limit ESY services to particular categories of disability; or
(B) unilaterally limit the type, amomt, or duration ofESY services.
(2) The need for ESY services must be documented ftom formal and/or informal evaluations provided by the district or the parents. The documentation sball demonstrate that in one or more critical areas addressed in the c:urrent individualized education program (IEP) objectives, the student bas exhibited, or reasonably may be expected to exhibit, severe or subslantial regression that cmmot be recouped within a reasonable period of time. Severe or substantial regression means that the student bas been, or will be, uuable to maintain one or more acquired critical skills in the absence ofESY services.
(3) 1be reasonable period of time for recoupment of acquired critical skills shall be determined on the basis of needs identified in each student's IEP .If the loss of acquired critical skills would be particularly severe or substantial, or if such loss n:su1ts, or reasonably may be expected to result, in immediate physical harm to the student or to others, ESY services may be justified without consideration of the period of time for~ of such sldlls.ID any case, the period of time for recoupment sball not exceed eight weeks.
(4) A skill is critical when the loss of that skill n:su1ts, or is reasonably expected to result, in any of the following occum:nccs cluriDg tbe first eight weeks ofdle next regular school year:
(A) placemeDt in a more restrictive iDstructional ammgement;
(B) sigoificant loss of acquired skills necessary for the student to appropriately progress in the geueral curriculmn;
(C) significaDt loss of self-suflicieacy in self-help skill areas as evidenced by an increase in the number of direct service saaff' and/or amount of time required to provide special education or related services;
(D) loss of access to coJ111111111ity-based independent living skills iDstruction or an illdcpmdent living environment provided by noneducational sources as a result of regression in skills; or
(E) loss of access to on-the-job training or productive employment as a result of regression in skills.
(S) lfdle district does not propose ESY services for discussion at the amwal review of a student's IEP, the parent may request that the ARD committee discuss ESY services pursuant to 34 CFR, §300.344.
(6) If a student for whom ESY services were considered and rejected loses critical skills because of the decision not to provide ESY services, and if those skills are not regained after the reasonable period of time for recoupment, the ARD committee shall reconsider the current IEP if the student's loss of critical skills interferes with the implementation of the studart's IEP.
(7) For students emolling in a district cluriDg the school year, iDfonnation obtained fiom the prior school district as well as iDfonnation collected during the curratt year may be used to determine the need for ESY services.
(8) 1be provision ofESY services is limited to the educational needs of the student and shall not supplant or limit the responsibility of other public agencies to continue to provide care and treatment services pursuant to policy or practice, even when 1hose services are similar to, or the same as, the services addressed in the student's IEP. No student sball be denied ESY services because the student receives care and treatment services under the auspices of other agencies.
(9) Districts are not eligible for reimbursement for ESY services provided to students for reasons other than those set forth in this section.
TEA I Spacial Education htlp://Www.tsa.stata.tx.usllpedal.edl
4 State Reaourca: ESY Sanricas Sprtng2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

, What were tbe CONCERNS
identified?
Bow did the State address the
CONCERNS?
ldeatified Result
Texas Continuous Improvement Process ·Extended School Year Services
......... _. Areas of Improvement Identified for ESY Through the IIIII"" OSEP ContiDuous Improvement Monitorillg Proeess
• Decisions to provide ESY services may be based on the student's category of disability rather than the individual needs of each student.
• Transportation, as a related service, is not always provided to students with disabilities participating in extended school year programs.
• In some districts, ESY services are not discussed during ARD meetings or provided to students, and the criteria used for determining eligibility varies across districts/schools.
• There is much variation across districts/schools in terms of what and how ESY services are provided. In many cases, the timing and amount ofESY services are inflexible, and services do not always address all needed and relevant goals for students.
http://www.tea.state.tx.us/special.edltcip/fape.html
to Address State Result Developed Through the CONCERNS Tesas Continuous 1m provemeat Process
~
.. • __ ....... Each district must ensure that extended school year services are ...... available as necessary to provide a free appropriate public
education.
TEA I Special Education htlp:llwww.tea.stata.tx.uslapedal.edl
• ESY services are determined by the student's ARD committee.
• ESY services are not limited to particular categories of disability.
• ESY services are not unilaterally limited as to the type, amount, or duration.
• Transportation, as a related service, is considered and offered to students with disabilities who need this service to benefit from ESY services.
5 State Rasaurcll: ESY Servk:es Spring 2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

How will the State achieve the
RESULT?
Texas Continuous Improvement Process Extended School Year Services
....... Action Needed to Ensure tbe State Meets tbe Identified Result
DISTRICT ACTION
Distrlets should examine their current guidelines/framework used to determiDe and provide ESY serviees to ensure that the following eoaslderatioas are Ia plaee:
ESY Services are considered and determined by the student's ARD committee.
District has and disseminates specific written guidelines and procedures pertaining to the provision ofESY.
• Guidelines/Procedures include a timeline for planning.
• Guidelines/Procedures include an evaluation of the effectiveness of the program.
• Guidelines/Procedures include consideration of ESY services for students tnmsferring to the district from other districts or Early Childhood Intervention (ECI) programs.
All district s1aff are informed of and understand the purpose of ESY services and the role staff play in the consideration and delivery ofESY services.
• District staff refers to administrators, supervisors, teachers, related service personnel, and teaching assistants.
• District staff participate in the considetation of ESY services discussion.
• District staff involved in the pmvision ofESY services are informed of the student's goals and other information ~elated to ensuring the effectiveness of the services.
Parents of students with disabilities receive an explanation of the purpose for ESY services. Additionally, parents are informed of the role they play in the consideration and delivery of the ESY services.
Districts consider and determine a variety of options for the delivery ofESY services including amounts of time and duration of services.
• Services are student need driven and include a variety of options.
• Consideration of service delivery includes community options/services.
• ESY Goals/Activities are reflected in the student's current IEP.
Districts consider ESY services for c~dren in all disability categories.
• District information reflects that all disability categories are considered for ESY.
• Considemtion is by individual student need.
TEAl Spedal Education http://wwW.taa.atate.tx.usllpedaJ.edl
8 State Ralourca: ESY Services Spring 2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

HowwUlthe State aebieve the
RESULT?
Texas Continuous Improvement Process Extended School Year Services
Aetioa Needed to Easare tbe State Meets the Ideatified Result
DISTRICT ACTION (eontinued)
Districts should eumiae their eurreat guideliDeslfnmework used to determiae and provide ESY services to easure the foUowiag eoasideratioas are in place:
ESY Services are connected to previous and future school year services.
• A communication system is in place that defines roles and responsibilities for ESY documentation to flow between and among district staff.
• Sending and receiving teachers provide information and feedback regarding the provision and etJectiveness of the ESY services.
• Framework for the ESY program includes a process for planning prior to the initiation of and following the end ofESY services.
Districts consider and detennine related services, including transportation, needed for the student to benefit from ESY services.
Each district ensures that ESY services are available as necessary to provide a free appropriate public education.
ESY services are effective in maintaining identified critical skills.
PARENT ACTION
Parents understand information provided to them in regard to the purpose and intent ofESY services.
When parents have questions regarding this service, they know who to ask for further discussion and/or explanation of the process.
Parents participate in the ARD committee discussion regarding the consideration ofESY services.
When needed or appropriate, parents provide documentation to the ARD committee for use in the determination ofESY eligt"bility.
Parents communicate with district staff and participate in the ESY services as they would for their child's school year services.
TEA I Special EdUcatfon htlp:llwww.tea.stata.tx.ualapec:ial.edl
7 State Relaurca: ESY SeMcea Sprfng2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

Resources
Additional information ftom the State regarding the provision ofESY services will be available on the TEA Special Education web page:
http://www.tea.state.tx.uslspecial.edl
·For technical assistance and training in regard to ESY and other aspects of the provision of services for students with disabilities; contact your regional education service center (see the web page listed below for education service center locations and contact information).
TEA I Special Educatlan htlp:l/www.tea.llats.tx.ulllpeclal.edl
http://www.tea.state.tx.us/ESC
8 State Rasource: ESY Services Spttng2004
MGARCIA
Rectangle
MGARCIA
Rectangle
MGARCIA
Rectangle

Extended School Year Services
• At each student's Annual ARD meeting, Extended School Year Services (ESY) will be considered. If it is determined that ESY services are needed, ARD/IEP SUPPLEMENT EXTENDED SCHOOL YEAR SERVICES (SEAS) will need to be completed.
• If the Annual Meeting was already held, and it was determined at the time that the student was not in need of ESY services, but at the end of the year personnel working with the student, or the parent later believe that the student may be in need of ESY services, an ARD committee meeting will be reconvened to consider the need for ESY services.
• If all stakeholders (parent and school) are in agreement that ESY is needed and this determination was not made at the annual ARD meeting, an amendment to the IEP can be developed to reflect this determination, as long as the parents are in agreement for this change without an ARD meeting.
• Whether a determination for ESY services was made through an ARD meeting or an amendment, the ESY supplement must be completed and the goals and objectives to be worked on during the summer must also be completed.
• In considering whether ESY services are needed, the ARD committee will review progress reports, updated goals and objectives, information provided by the parent and teacher, and any other evaluation data in order to discern whether a significant amount of time is needed in order for the student to recoup mastered skills after long school holidays and/or summer. Please refer to attached guidance from TEA in determining the need for ESY services.

Section 6

Modified Exit Criteria from Bilingual or ESL Services
Under certain circumstances, state law allows for exit criteria from Bilingual or ESL services to be modified for some students who receive special education services. Caution should be exercised when choosing to modify exit criteria and consideration should be limited to students in 3rd grade or higher who are taking the alternate version of the state mandated assessment. Discussion should begin at or near the beginning of the year when key members of the LPAC and ARD Committee (need not be every member) begin to examine whether a student, because of reasons related to their disability, may never be able to meet state required exit criteria. In addition, both formal and informal data to include teacher input is examined in determining whether the student continues to need second language support. If deciding to modify the exit criteria, key members of the ARD and LPAC will document their decision to do so on the attached document titled Review and Recommendation of Exit Criteria. In modifying the exit criteria, modifications of performance standards on academic content assessments (Reading and Writing) are not permitted. State established standards must be used. For English language proficiency assessments, modification of assessment standards may be allowable on a domain by domain basis provided that evidence exists that the students, because of reasons related to their disability, may never meet state established standards and it is determined that the student no longer appears to benefit from second language support When the form Review and Recommendation of Exit Criteria is completed, an ARD Committee Meeting must be held in order to review the documentation and determine whether the Committee is in agreement with modifying the LEP exit criteria. The meeting must occur prior to the student’s participation in the identified assessment. As the year progresses, the student will then participate in the assessment that was recommended. Near the end of the year, when assessment results are received by the district, the key members of the ARD and LPAC meet within the context of an LPAC meeting to review whether established standards were met and to determine whether exit of the student will occur. If after this process, it is determined that exit will occur, a formal ARD Committee meeting will then occur to finalize and document the change in placement or program. Attached you will find of copy, made available by the state, outlining the steps to take in this process for consideration of Special Exit Criteria from Bilingual or ESL services. These steps are to be followed.

1
Process for Considering Special Exit Criteria
from Bilingual/English as a Second Language (ESL) Services Under 19 TAC §89.1225(k)1
2015–2016 School Year
Grades 1–12
Under Texas Administrative Code (TAC) §89.1225(h), districts are required to use the exit criteria represented in the chart titled 2015-2016 English Proficiency Exit Criteria Chart found at http://tea.texas.gov/bilingual/esl/education/to exit English language learners (ELLs) from bilingual/ESL programs. The exit criteria under TAC §89.1225(h) apply to the vast majority of ELLs who receive special education services. In rare cases, an ELL receiving special education services may qualify to be exited using criteria permitted under TAC §89.1225(k), which give special consideration to an ELL for whom assessments and/or standards under TAC §89.1225(h) are not appropriate because of the nature of a student’s particular disabling condition. Students considered for special exit criteria under TAC §89.1225(k) should only be only those designated to take STAAR Alternate 2, as determined by the ARD committee in conjunction with the LPAC. This document outlines the process to follow when considering whether a student qualifies to exit using the criteria authorized by TAC §89.1225(k).
Step 1: Schedule Meeting to Evaluate Whether Student Potentially Qualifies for Exit At or near the beginning of the school year, a meeting is to be scheduled between key admission, review, and dismissal (ARD) committee and language proficiency assessment committee (LPAC) members to discuss whether the student qualifies to exit using criteria under §TAC 89.1225(k). o Through this process, a determination is made about the assessments and/or English language proficiency
assessment standards to be used in the exiting process. o This process applies ONLY when one or more assessments and/or English language proficiency
assessment standards under TAC §89.1225(h) are not appropriate for the student in a particular language domain for reasons directly associated with the student’s disability. In following this process, refer also to the document titled Guidance Related to ARD Committee and LPAC Collaboration found at http://tea.texas.gov/index2.aspx?id=2147496923.
o This process is to be used to address the needs of an individual student, not groups of students. Very few students qualify to exit using the TAC §89.1225(k) criteria.
o This process must be conducted by key admission, review, and dismissal (ARD) committee members (including a diagnostician when applicable) and key language proficiency assessment committee (LPAC) members who are familiar with the student’s current progress and needs, including one or more teachers with in-depth knowledge of the student’s second language acquisition and academic achievement.
Step 2: Discuss Evidence of Need for Use of §89.1225(k) Exit Criteria At the meeting, the participants discuss the second language acquisition of the student within the context of the individual student’s disability to consider whether the TAC §89.1225(k) exit criteria are warranted. o Consideration must be IEP-based and must include documented evidence that, because of the nature of
the student’s disability, the student is not expected to be able to attain English language proficiency in one or more domains and no longer appears to benefit from second language acquisition support in English to address second language acquisition cognitive, linguistic, and affective needs (or is expected to reach that point during the school year).
o Evidence must include both historical formal and informal assessment data and direct teacher input. Ongoing informal assessment data may come from checklists, inventories, and other formative evaluations designed to identify the levels of academic functioning and English language proficiency of the student. The
1 Title 19 Texas Administrative Code Chapter 89 Adaptations for Special Populations; Subchapter BB. Commissioner’s Rules Concerning
State Plan for Educating Limited English Proficient Students

2
input of a diagnostician may be requested, as necessary, to help determine whether the TAC §89.1225(k) exit criteria are warranted. Direct teacher input should provide further insight into the student’s classroom performance and needs, and should include, if applicable, documentation of response to intervention, anecdotal notes, and other evidence drawn from sources such as classroom-based observations and classroom activities.
Step 3: Specify Assessments and English Language Proficiency Test Standards
If, after reviewing the evidence, the meeting participants conclude that the student no longer benefits from second language acquisition support in English (or is expected to reach that point during the school year), the participants review the assessment information in the IEP and make exit criteria recommendations based on the information below. Caution should be exercised when considering exit of students in Grades 1-2. It may be premature in these grades to consider program exit due to developmental factors related to emergent language and literacy. Additionally, in early grades it is often difficult to know the effect of the student’s disability on long-term prospects for second language acquisition.
ACADEMIC CONTENT ASSESSMENTS OF READING AND WRITING IN GRADES 1-2
o Norm-referenced standardized achievement tests are not required for students in grades 1-2 eligible under TAC §89.1225(k).
ACADEMIC CONTENT ASSESSMENTS OF READING AND WRITING IN GRADES 3-12
o Selection of appropriate academic content assessments Students considered for exit criteria under TAC §89.1225(k) should be only those designated to STAAR Alternate 2, as determined by the ARD committee in conjunction with the LPAC. Reminder: State-established standards must be used for all state assessments.
o Modification of performance standards on academic content assessments not permitted
STAAR Alternate 2 is an assessment based on alternate academic achievement standards. Further modification of performance standards on academic content assessments is not permitted. State-established standards must be used for all state assessments.
ENGLISH LANGUAGE PROFICIENCY ASSESSMENTS IN GRADES 1-12
o Modification of English language proficiency assessment standards on a domain-by-domain basis Any modified standards must be supported by historical data and evidence that the student is not expected to be able to attain English language proficiency because of factors directly related to the student’s disability and that the student no longer appears to benefit from second language acquisition support in English to address second language acquisition cognitive, linguistic, and affective needs (or is expected to reach that point during the school year).
o Selection of appropriate English language proficiency assessments − Listening: TELPAS listening or other OLPT from state-approved list − Speaking: TELPAS speaking or other OLPT from state-approved list − Reading: TELPAS reading or other English language reading proficiency test from state-approved list − Writing: TELPAS writing or other English language writing proficiency test from state-approved list
Step 4: Prepare Documentation Key members of the ARD committee and LPAC document the evidence, recommendation, assessments, and any modified English language proficiency test standards.
Step 5: Discuss Recommended Exit Criteria in Formal ARD Committee Meeting Key members of the ARD committee and LPAC present the documentation at a formal ARD committee meeting.

3
o The meeting should take place as early in the current school year as possible or at the end of the year to be applied the next school year. The meeting must occur prior to the student’s participation in the identified assessments.
o Based on discussion at the formal ARD committee meeting, the IEP is updated with documentation of the modified exit criteria if the committee as a whole determines that exit is anticipated.
Step 6: Determine and Document Whether Student Has Met Modified Exit Criteria At the end of the year, the ARD committee, with key LPAC members, meets to review the assessment results and subjective teacher evaluation required under TAC §89.1225(h) to determine whether the student has met the modified exit criteria. o The subjective teacher evaluation must reflect the status of the student following the administration of the
assessments. o This meeting is to be held at the end of the school year, as required by TAC Section 89.1220(g). This means
that an additional ARD committee meeting is necessary for students whose annual ARD committee meeting is held at a different time.
o If the decision is made to exit the student based on the assessment results and subjective teacher evaluation, the ARD committee finalizes and documents the change in placement or program and delineates instructional services including the monitoring period for exited students. Furthermore, as required under TAC §89.1220(l)(1)(H) relating to exit from bilingual education or ESL services, the LPAC also documents the exit decision in the student’s permanent record file.

Weslaco Independent School District Review and Recommendation of Exit Criteria
Student Name __________________________ Student ID# ___________________________ DOB ________ Grade __________Campus ____________
Placement:
Classification □ English Language Learners (LEP) □ Parent Denial (PD) _____ Total no. of years provided special language services
Bilingual /ESL Category: □ Beginner □ Intermediate □ Advanced □ Advanced High □ Elementary Bilingual/ESL Program □ Middle School Placement: □ ESL □ English □ High School Placement: □ ESOL I □ ESOL II □ English
Proposed LEP Exit Criteria: Based on documented IEP evidence, the following was determined: □ YES □ No Due to the nature of the student’s disability, is the student expected to be able to attain English language proficiency in one or more domains? □ YES □ No Does the student appear to benefit from second language acquisition support in English? If both are answered “No”, then it may be permissable to modify the 2016-2017 LEP Exit Criteria. Please indicate what evidence, both historical formal and informal assessment data to include direct teacher input was utilized in order to make the decision that modification of LEP Exit Criteria is needed. ______________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ Discuss the state assessment testing expectations for this student as they are outlined in the IEP. Note: Students taking the state assessment are most likely eligible for the Special Exit Criteria.
Check the test the student is expected to take and master.
State Assessment Reading Expectation Alternate
State Assessment Writing Expectation Alternate Discuss the TELPAS testing expectations for this student as they are outlined in the IEP.
Check one.
TELPAS Listening Expectation B I A AH
TELPAS Speaking Expectation B I A AH
TELPAS Reading Expectation B I A AH
TELPAS Writing Expectation B I A AH
____________ Administrator
______________ Counselor
______________ Bilingual/ESL Teacher
______________ Special Ed. Teacher
______________ Other
______________ Other
Date of Collaboration: _______________

Exit Documentation: At the end of the year, key members of the ARD committee and LPAC meet to review the assessment results and subjective teacher evaluation to determine if the student has met exit criteria. If the student has met exit criteria, an additional ARD will need to be scheduled.
Student’s name:
End-of-year ARD meeting date:
The assessment results reviewed at the ARD were:
State Assessment Reading Modified Alternate State Assessment Writing Modified Alternate Results TELPAS Listening B I A AH TELPAS Speaking B I A AH TELPAS Reading B I A AH TELPAS Writing B I A AH Summarize subjective teacher evaluation and attach documentation.
End-of-year LPAC date:
A decision was made to exit from the Bilingual/ESL program based on the comprehensive review of the ARD/LPAC Committee.
will be reclassified as Non-LEP and will be monitored for two school years.
Attach a copy of the documentation to the LPAC folder.
Notify parents of student’s reclassification.
Document on the student’s permanent record folder.
Recommendation: Signatures:
□ LEP (student did not meet exit criteria) □ Bilingual Program □ Elementary ESL Program □ Secondary ESL Program □ Monitored: Exit Bilingual/ESL Program (met exit criteria Exit Date: ____________________ (Day after last day of school enrollment for the year)
___________________ Administrator ___________________ Counselor ___________________ Bilingual/ESL Teacher ___________________ Special Education Teacher ___________________ Other ___________________ Other Date of Discussion/Collaboration: ___________________

Section 7

TRANSITION PLANNING / SERVICES
• A separate Individual Transition Plan Meeting is no longer required. • In-spite of this, Transition planning is alive and well and must be done within the
context of an ARD Meeting.
• Federal law requires that a student of any age must be invited to the ARD meeting, if the purpose of the meeting is to discuss transition services.
• If this is the case, remember to indicate on the notice of ARD that one of the purposes of the meeting will be to discuss transition services. Also remember to indicate on the ARD notice that the student is being invited to the meeting.
• If the purpose of the meeting is to discuss transition services and the student does not attend, paperwork must indicate the steps that were taken to consider the interests of the student.
• By age 14 (before student turns 14) state law requires that nine elements related to transition be considered / reviewed by the ARD committee. These elements are embedded within the Middle and High School ARD packet.
• Beginning at age 13 and thereafter, transition brochures should be given to the parents and/or the adult student at the annual meeting. The transition brochure can be obtained from your educational diagnostician.
• By age 16 (before student turns 16), federal law requires that the ARD Committee identify the transition services needed by the student. The transition services are to be incorporated throughout the ARD document. The elements to be addressed are embedded within the Middle and High School ARD packets.
• Federal law requires the school to invite any agency that is providing Transition Services, or may be responsible in providing or paying for transition services.
• Prior to inviting any agency representatives, a Consent for Disclosure of Confidential Information is needed from the parent or adult student.
• Refer to the Transition Services Checklist which is found on the
Sp. Ed. Website.
8/12

Transfer of Rights
• In accordance with federal law, students IEPs must contain a statement that the rights afforded to the parents under IDEA 2004 will transfer to the adult student once the student turns 18 years of age.
• This statement must be addressed at least a year before the student turns 18.
• As a result, whenever an ARD meeting is being held for a student that is 16, the transfer of rights must be addressed at that point. If an ARD meeting was being held during the year that the student had already turned 17 and we waited until then to address the fact that the student's rights would be transferring at 18, then we would not be in compliance, as the law specifically states that this must be addressed a year before the student turns 18.
• The form on the ensuing page titled Information Regarding Transfer of Parental Rights at Age Majority, must be completed and a copy of the procedural safeguards must be sent to the parents and provided to the student. Please keep a copy of this form and send it with a copy of the annual ARD to the special education office.
• Upon the student turning 18, the parents and student must now receive a notice indicating that the student has turned 18 and unless guardianship was obtained by the parent, all rights afforded to the parent under IDEA 2004 have now transferred to the student. A separate notice along with the procedural safeguards must be provided to the parents and student. The notice can be found after the form titled Information Regarding Transfer of Parental Rights at Age of Majority, and is titled Notification of Transfer of Parental Rights at Age of Majority.
• It is expected that each person at the High Schools monitor their own caseload and send these notices as soon as any individual on their caseload turns 18. Keep a copy of the notice that is sent and turn it in to your assigned Educational Diagnostician, who will then provide a copy to the special education office, which will then be filed in the student's eligibility folder.
8/12

SECONDARY GRADUATION PLAN
• A graduation plan is necessary for all students beginning at least in the 9th grade.
• The school counselor develops the graduation plan according to the student's academic needs and keeps it in their active folder.
• The special education teacher also duplicates the graduation plan using the special
education form and uses it during ARD meeting. It is filed in the eligibility folder with the ARD packet
• The graduation plan must be revised as classes are dropped or added.
• A copy of the graduation plan is placed in the student folder and reviewed at each
annual.
• Each plan has a district code that is entered by the Data Entry Clerk for accounting purposes.
• A Graduation Supplement form is completed and signed at the graduation ARD.
8/12

Graduation ARDs
Prior to the graduation of a student who receives special education services, the law calls for the student's ARD committee to identify the method of graduation. This is typically referred to as a graduation ARD. The graduation ARD will typically be convened one to two months prior to the student's anticipated graduation date. The documentation of the method of graduation can be found on the ensuing page. In instances where students are graduating because they are aging out, or have completed all of the curricular and credit requirements as all other students (without substitutions), graduation constitutes a change in placement and terminates a student's eligibility for special education services. Under this circumstance, the notice of ARD meeting for the graduation ARD must include the following statement: Graduation constitutes a change in placement and terminates the student's eligibility for special education services. In addition, a Notice of Proposal/Refusal must be sent to the parent notifying them of this.

Summary of Functional Performance and Academic Achievement
• A new provision from IDEA 2004 requires that prior to graduation, student's receiving a regular diploma must receive a summary of academic achievement and functional performance that includes recommendations for meeting post-secondary goals. The form on the ensuing page will be utilized for meeting this new requirement.
• The Summary of Academic Achievement and Functional Performance can be completed at the student's designated graduation ARD. A copy of this form should be provided to the adult/student and/or parent who may have obtained guardianship of the student.
• A copy of the Summary of Academic Achievement and Functional Performance must be included as part of the student's graduation ARD.

Secondary Functional Vocational Evaluation
A Functional Vocational Evaluation is a tool to facilitate individual transition planning at the secondary level.
The Student Interview and Functional Vocational Assessment–Teacher Observation should be administered beginning at age 14 to all students to ensure that student preferences are driving the development of transition services.
8/12
Section 8

Amendments to ARD Meetings (Agreement to Change IEP)
• Federal Law allows, in certain cases, for changes to be made to a student's IEP after Annual ARD meetings without an IEP meeting, provided that the parent/adult student and school agree not to convene an IEP meeting for the purpose of those changes and instead develop a written document to modify the child's current IEP.
• The AGREEMENT TO CHANGE CURRENT IEP with signature found on SEAS may be used, in
certain circumstances in order to make minor changes to the Annual ARD meeting provided that the parent is in agreement.
• These provisions were made in order to help with the reduction of paperwork. • The AGREEMENT TO CHANGE CURRENT IEP form is not to be used in instances
where ARD meetings must be held, such as, but not limited to the following occasions: Manifestation ARD meetings, any changes that will result in a change of placement for a student, review of formal evaluation such as Psychological, FIEs, etc.; .
• Instances in which IEPs can be changed through the amendment process might include: Adding or deleting of goals and objectives; schedule changes that do not result in a change of instructional arrangement; change to a behavior intervention plan; adding of modifications/accommodations. These are just some examples, again as questions arise, please consult with your educational diagnostician.
• In instances where it is believed that changes to an IEP can be made through the amendment process, please consult with the educational diagnostician assigned to your campus.
• If it is determined that the change can be made through the amendment process, the educational
diagnostician will provide you with the necessary paperwork.
• Additional signatures are required on the AGREEMENT TO CHANGE CURRENT IEP form in order to safeguard that important decisions are not being made solely at the whim of one person.
• When the AGREEMENT TO CHANGE CURRENT IEP is completed, it is then either sent to the parent, or a meeting can be scheduled with the parent to explain the changes.
• If parents do not agree with the action being proposed on the amendment, an ARD meeting must be held to discuss the matter further.
Section 3 7/16

Section 9

Implementation of Accommodations/Modifications and Coordination With Regular Education Teachers
Special Education teachers must in a timely manner provide pertinent sections of a student's IEP to regular education teachers, to include a copy of needed accommodations/modifications and a copy of a behavioral intervention plan (should one exist.) In order to document that the regular education teacher received a copy of the accommodations/modifications as recommended by the ARD committee, the special education teacher should ensure that a signed Verification of Receipt of modifications (See attachment N) is obtained from the regular education teacher. In addition, the special education teacher is responsible for coordinating with regular education teachers to ensure that regular education teachers are aware of what the recommended accommodations/modifications are and more importantly understands how to implement them. At least once a six weeks, the special education teacher must provide and obtain from the regular education teacher a Coordination of Services Sheet (Attachment M). The Coordination of Services Sheet will ensure that students are receiving the proper supports in the regular education setting. Please stress to the regular education teachers that they have a legal and ethical obligation to provide accommodations/modifications as recommended by the ARD committee. It is important that the regular education teachers have proof of accommodations/modifications that are being provided. Proof of provided accommodations/modifications can be documented on weekly lesson plans, or on assignments themselves. For instance, if a particular test was read orally to the student, the regular education teacher can simply write on the test itself, Test Was Orally Administered. In addition, on a homework assignment, the teacher can write, Provided Extra Time for Completion, at the top of the assignment.
8/12

Section 10

Procedures for Transfer Students
• Upon the notification from the parent that a student transferring into the district was receiving services previously from another district, the special education teacher will inform the educational diagnostician of this development.
• The campus personnel will ask the parent whether they have any documentation in the way of a copy of the latest assessment and/or ARD paperwork.
• If the parent and/or adult student does not have any paperwork to confirm that they were previously receiving special education services, the campus personnel will call the previous school district and verify the following: 1 .Was the student receiving special education services? 2. What was the category of eligibility? 3. What educational as well as related services was the student receiving? 4. What are the dates of the student's evaluations?
• Upon confirmation of information from the previous district, the parent and/or adult student will be asked to waive their right to receive the ARD notice at least 5 school days prior to the meeting, and a transfer ARD meeting will be held immediately.
• If the scenario exists in which the student was receiving services from a public school district in the state of Texas and the district has a copy of the student's IEP, and it is current, a temporary transfer meeting is not needed. In this case, the district must determine that the IEP is appropriate and will be implemented as written by the previous district. There must be written agreement between the parent and the district representative. The form titled Agreement to Implement In-State or Out of State IEP found on SEAS will be utilized to document that the aforementioned criteria has been met and a temporary meeting is not needed. In any case an ARD meeting must be held within 30 school days to finalize the IEP.
• If a student transferred from out of state, a transfer meeting must be held immediately. In addition, at the meeting, most likely a recommendation for further evaluation will be made, as the eligibility criteria for some states may not match that of Texas. In this event, do not forget to provide the parent with a notice of evaluation, obtain consent for evaluation, and provide the parent with a copy of the procedural safeguards.
• It is important to note that there should never be a cessation in services, and transfer meetings must occur immediately.
8/12

Section 11

Request to Exit Student from Special Education Program
In the event that a parent/adult student requests to be exited from the special education program, the following procedures will occur:
• Ask the parent to provide a written statement requesting that their child be exited from the special education program.
• Inform your Educational Diagnostician of the parent request. • The Educational Diagnostician will then consult with the Special Education
Director. The two will collaboratively write a Prior Written Notice outlining the services and supports that the student will no longer be entitled to receive should the student be exited from the Special Education Program.
• The notice will explain that unless communicated otherwise from the parent/adult student within five school days of receipt of the Prior Written Notice, that the student will then be exited from the program.
Section 12

Parent/Student Rights
PARENTS & STUDENT RIGHTS
A. CONFIDENTIALITY
PURPOSE:
The purpose of confidentiality of personally identifiable information is to ensure that the student's rights to privacy are implemented. Confidentiality is a professional, ethical, and legal issue and must be adhered to within the confines of the law.
These are the operating procedures regarding confidentiality in reference to:
STUDENT FOLDERS / ELGIBILITY FOLDERS:
• To ensure confidentiality of student records, a Record of Confidentiality (Attachment Q) must be kept in each student's folder.
• The Record of Confidentiality must be signed by anyone reviewing the folder.
• All the required information on process record must be filled out.
SPECIAL EDUCATION TEACHERS:
• All student folders should have one Record of Confidentiality in place. Please use (Attachment Q) to make more copies as needed.
8/12



Section 13

Functional Behavioral Assessment (FBA)
• FBAs are assessments that gather information for the purpose of attempting to determine why certain behaviors are occurring. Specifically the assessment aims to pinpoint potential triggers, and cause and effect relationships.
• FBAs may consist of informal measures such as repeated observations of the student in various environments, as well as anecdotal information from individuals familiar with the student. FBAs may also consist of more formal measures such as questionnaires.
• FBAs are required when there is a disciplinary change in placement. • FBAs may also be needed when in spite of the consideration of
positive behavioral interventions and supports; and other strategies to address the behavior that is impeding the student’s learning and that of others, the behavior continues to be a concern.
• An FBA should be requested through an ARD meeting and written consent must be obtained.
• FBAs can be conducted by the student’s special education teacher in consultation with other individuals such as, but not limited to Educational Diagnostician, Special Education Counselors, and Licensed Specialist in School Psychology.

Section 14

SHARS (School Health and Related Services)
• In an effort to help offset the costs of special education programming, school districts are allowed and highly encouraged to obtain reimbursement for certain services listed on a student’s individual education plan.
• Some of the services for which School Districts can obtain reimbursement include: Occupational Therapy, Physical Therapy, Speech Therapy, Nursing (requires Evaluation Report: School Health Service – SEAS), Special Transportation, Counseling Services provided by certain individuals, Nurse, Personal Care Services (Personal Care Supplement must be included as part of IEP).
• All services must be clearly delineated within the student’s IEP document. Such documentation can be included in student’s PLAAFPs statement, Goals and Objectives, deliberations, various ARD supplements such as Personal Care Supplements, Transportation, and Evaluation Report: School Health Service, etc.
• School Districts must have a signed consent parental consent to release personally identifiable information and accessing Medicaid reimbursement.
• After signed parental consent is obtained to release personally identifiable information and accessing Medicaid reimbursement, Districts are required to provide to parents notice of intent to access Medicaid reimbursement is required.

SHARS Procedures
• For students who do not have on file the following form: Consent to Release Personally Identifiable Information & Access Medicaid Reimbursement, Special Education teachers will secure this form within the first six weeks of school. The consents are to then be provided to the campus Educational Diagnostician who will submit the forms to Araceli Rodriguez (SHARS Clerk).
• For any initial referrals where students qualify for special education services, secure a Consent to Release Personally Identifiable Information & Access Medicaid Reimbursement at the initial ARD meeting. Form must be forwarded to Araceli Rodriguez.
• For any students who transfer from another school district, a Consent to Release Personally Identifiable Information & Access Medicaid Reimbursement must be secured at Transfer ARD meeting and forwarded to Araceli Rodriguez.
• Once the Consent to Release Personally Identifiable Information &Access Medicaid Reimbursement is secured, consent is only required to be obtained once, unless the frequency, duration and type of service is changed. In this event, a new written parental consent is needed.
• After obtaining consent, school districts are required to notify parents on an annual basis of the intent to access reimbursement for services provided under the SHARS program. Teachers and service providers are to use the form titled Notice of Intent to Access Medicaid Reimbursement.
• Special Education Teachers are to send to parents the Notice of Intent to Access Medicaid Reimbursement within the first six weeks of school. A copy of this form is to be sent to Araceli Rodriguez no later than the first six weeks of each school year. Teachers are to keep a copy of this notice in the campus student folder.
• For all students, ARD paperwork must clearly document the service that the student is receiving. Remember to include Personal Care Supplement for all students who receive personal care services.
• All forms to be utilized are included.

Weslaco Independent School District Special Education Department
Consent to Release Personally Identifiable Information & Access Medicaid Reimbursement Name: DOB: ID:
School: Grade: Medicaid #:
Your child’s Individualized Education Program (IEP) includes special education and related services provided by the Weslaco Independent School District (Weslaco ISD) Special Education staff. One or more of the school-based services included on your child’s IEP may be eligible for Medicaid reimbursement to Weslaco ISD. Medicaid is a public insurer that the Weslaco ISD routinely accesses to assist the school district in meeting the cost of providing special education and related services.
This form is requesting permission to release student information so the District may apply for Medicaid reimbursement under the School Health and Related Services (SHARS) program for designated services listed in the student’s Individualized Education Program (IEP). Schools are required by the Individuals with Disabilities Education Act (IDEA) and the Family Education Rights and Privacy Act (FERPA) to obtain parental consent before disclosing information about a student. * This includes providing the following personally identifiable information to state and/or federal Medicaid agency/ representative and any third party billing company contracted by WISD, including but not limited to student name, date of birth, Social Security number, Medicaid number, date of service, service type, service duration, student eligibility and information regarding student’s disability and health condition.
This form is also requesting permission for WISD to access you/your child’s Medicaid benefits to file for reimbursement for SHARS services provided to your child.
Once the Weslaco ISD obtains this one-time consent, the district will not be required to obtain any further parental consent in the future before it accesses your or your child’s public benefits or insurance regardless of whether there is any change in the type, amount, or cost of services to be billed to the public benefits or insurance program (e.g. Medicaid). However, Weslaco ISD will annually thereafter provide you with written notification that it will access your or your child’s public benefits or insurance.
The district may not 1) require parents to incur out-of-pocket expenses or sign up for public benefits in order for their child to receive services; 2) use benefits that would decrease a child’s lifetime coverage or result in the family paying for services that would otherwise be covered, or 3) use benefits if that use would increase premiums, lead to the discontinuation of benefits or risk loss of eligibility for home and community-based waivers as described in section 300.154.
Weslaco ISD ensures that your child will be provided the services specified in the IEP at no cost to you regardless of whether you consent to Weslaco ISD billing Medicaid for reimbursement; however; your consent will greatly assist the district in providing the highest quality of services to the children served by Weslaco ISD. The money collected from Medicaid is used to expand and enhance medical and related services for children. Your consent is voluntary and may be revoked at any time. Accordingly, the revocation is not retroactive and does not negate reimbursements that may have been received prior to your revocation.
Please check by each statement, sign your name, insert date, and return this form to: at as soon as possible. School / Department Staff School / Department
YES NO I give consent for Weslaco ISD to release personally identifiable information for my child which is outlined and bolded in the above
notice regarding School Health and Related Services (SHARS) my child receives at school to state and/or federal Medicaid agency/ representative and any third party billing company contracted by WISD to determine eligibility and/or to file claims for Medicaid reimbursement. This consent will be effective for the duration of the time that your child is receiving School Health and Related Services (SHARS).
YES NO I acknowledge that I have been fully informed and understand the request for the District to file for reimbursement with the state’s School-based Medicaid Program for my child/me.
YES NO I give consent for Weslaco ISD to file for reimbursement for School Health and Related Services (SHARS) provided for my child/me.
YES NO I have been informed in my native language or other mode of communication.
YES NO I understand that my consent for release of information and for Weslaco ISD to file for reimbursement for (SHARS) is voluntary and can be revoked at any time. However, the revocation is not retroactive.
YES NO I give consent for the filing for reimbursement to begin immediately by waiving the required five (5) school day waiting period between notice of intent to file SHARS and initiation of the filing of SHARS.
_________________________________________________________________ ______________________________________ SIGNATURE OF PARENT, ADULT STUDENT, GUARDIAN, OR SURROGATE PARENT DATE
_________________________________________________________________ ______________________________________ SIGNATURE OF INTERPRETER, IF NEEDED DATE
* If you have any questions, please contact: Neil D. Garza, Director or Araceli Rodriguez, SHARS at 956-969-6822 School / Department Staff Phone#
Or Texas Health and Human Services Commission Medicaid Client Hotline at 1-800-252-8263
Revised 7/8/15

Distrito Escolar Independiente de Weslaco Departamento de Educación Especial
Consentimiento para Divulgar Información de Identificación y Acceso al Reembolso de Medicaid
Nombre: Fecha de Nacimiento
No. de Identificación
Escuela Grado: Medicaid #:
El Plan Individual de Educación (Individual Education Plan o IEP) de su hijo(a) incluye servicios de educación especial y otra asistencia relacionada que son proveídos por el personal del Departamento de Educación Especial del Distrito Escolar Independiente de Wéslaco (Weslaco Independent School District o WISD). Uno o más de los servicios incluidos en el IEP de su hijo califican para que WISD obtenga reembolso de Medicaid. Medicaid es una institución pública de seguros médicos a la cual el Distrito accede rutinariamente para enfrentar los gastos de educación especial y otros servicios relacionados.
Este formulario está solicitando permiso para divulgar la información del estudiante por lo que el Distrito puede solicitar el reembolso de Medicaid bajo del Programa de Servicios Relacionados (SHARS) del programa de servicios designados que se mencionan en el Programa de Educación Individualizada (IEP). Las escuelas están obligadas por la Ley de Discapacidades (IDEA) y los Derechos Educativos de la Familia y la Ley de Privacidad (FERPA) con obtener consentimiento de los padres antes de divulgar información sobre un estudiante. *Esto incluye el suministro de información a la agencia pública y cualquier otra compañía de cobros facturación de los terceros contratada por WISD , incluyendo pero no limitado a, nombre, fecha de nacimiento, número de Seguro Social, número de Medicaid, fecha de servicio, tipo de servicio y duración del servicio.
Este formulario también está solicitando permiso para que WISD acceda a los beneficios de Medicaid suyos o de su hijo para solicitar reembolso por los servicios de SHARS proveídos a su hijo.
Después que WISD obtenga su consentimiento, el distrito no va a requerir en el futuro obtener más consentimientos de los padres antes de acceder beneficios públicos o seguro independientemente de su hijo(a) o de usted, no importa si hay algún cambio en el tipo, cantidad, o costo de los servicios que se facturan a los beneficios públicos o programa de seguros (p. ej. Medicaid). Sin embargo, WISD, anualmente le proporcionara una notificación por escrito de que se tendrá acceso a los beneficios públicos o seguros de su hijo(a) o de usted.
El distrito no podrá 1) requerir que los padres incurren gastos de bolsillo o registrarse para beneficios públicos para que su hijo reciba los servicios, 2) utilizar los beneficios que disminuiría cobertura de por vida de un niño o dar lugar a que la familia pague por servicios que de otra manera estarían cubiertos, o 3) utilizar los beneficios si ese uso sería aumentar las primas, dar lugar a la suspensión de los beneficios o riesgos de pérdida de la elegibilidad de exención en el hogar y en la comunidad, como se describe en la sección 300.154.
WISD le asegura que su hijo(a) recibirá los servicios especificados en el plan individual de educación en forma gratuita, independientemente que el Distrito envíe la cuenta a Medicaid o no; sin embargo, su consentimiento asistirá a WISD a brindarles a los estudiantes servicios de alta calidad. El reembolso recibido de Medicaid se usa para expandir y mejorar la asistencia médica y otros servicios relacionados con los estudiantes. Su consentimiento es voluntario y puede ser revocado en cualquier momento.
Por favor seleccione la respuesta apropiada en cada declaración, firme y escriba la fecha y envié este formulación a:
en lo más pronto posible. Personal de la Escuela/Departamento Escuela/Departamento
SI NO Doy mi consentimiento a Wéslaco ISD a entregar información de identificación personal para mi hijo que se describe y en molde en el aviso anterior sobre Salud Escolar y Servicios Relacionados (SHARS) mi niño recibe en la escuela a otro y / o agencia / representante federal Medicaid y cualquier tercero empresa factura correspondiente contratada por WISD para determinar la elegibilidad y / o presentar las solicitudes de reembolso de Medicaid. Esta autorización será efectiva mientras dure el tiempo que su hijo está recibiendo Salud Escolar y Servicios Relacionados (SHARS).
SI NO Roconozco que he sidoplenamente informado y entiendo la solicitud por medio del Districto a presentar para el reembolso con el Programa de Medicaid en las escuelas del estada para mi hijo/mi.
SI NO Doy mi consentimiento para que el Distrito Escolar de Wéslaco solicite el reembolso de Salud Escolar y Servicios Relacionados (SHARS) previstos para mi hijo.
SI NO He sido informado de todo en mi idioma natal u otro tipo de comunicación.
SI NO Entiendo que mi consentimiento para autorizar entrega de información y para que el Distrito Escolar de Wéslaco solicite el reembolso de Salud Escolar y Servicios Relacionados (SHARS) es voluntario. Si decido revocar mi consentimiento, esto no niega una acción que haya ocurrido después que haya dado el consentimiento y antes que haya sido revocado.
SI NO Doy mi consentimiento para la presentación de reembolso para comenzar de inmediato mediante la renuncia de los cinco requerido (5) días escolares plazo entre la notificación de la intención de presentar SHARS y el inicio de la presentación de SHARS _________________________________________________________________ ______________________________________ FIRMA DEL PADRE, ALUMNO ADULTO, TUTOR LEGAL O SUBSTITUTO (circule el apropiado) FECHA
_________________________________________________________________ ______________________________________ FIRMA DEL INTERPRETE SI SE USO DICHO SERVICIO FECHA Si tiene alguna pregunta, llame a:
Neil D. Garza, Director o Araceli Rodriguez, SHARS At 956-969-6822 Personal de la Escuela/Departamento TELEPHONO #
O llamar a la Comisión de Tejas de Servicios Humanos y Salud al Cliente de Medicaid al 1-800-252-8263
Revised 7/8/15

Weslaco Independent School District Special Education Department
Annual Notice of Intent to Access Medicaid Reimbursement
Name: DOB: ID:
School: Grade: Date Sent:
Your child’s/Your Individualized Education Program (IEP) includes Special Education and Related Services provided by Weslaco ISD Special Education staff. One or more of the school-based services included in your child’s/your IEP may be eligible for federal Medicaid reimbursement to the Weslaco Independent School District. Medicaid is a public insurer that the school district routinely accesses to assist the school district in meeting the cost of providing special education and related services. Funding may be sought for reimbursement for the following services if they are provided to your child/you who is/are eligible for the Medicaid Program:
Personal Care Counseling Psychological Services School Health Services Transportation Services
Speech Therapy Occupational Therapy Physical Therapy Assessment Audiology Our records indicate that you have already provided written consent for WISD to apply for reimbursement under the SHARS program. It is the districts intent to access Medicaid Reimbursement. In accordance with federal regulations 34 CFR§300.154(d)(2)(iv)(A)-(B), you will be provided this Annual Notice of Intent to Access Medicaid Reimbursement on an annual basis and:
• Personally identifiable information related to your child/you regarding eligibility and services may be released to the state’s school-based Medicaid program for reimbursement including, but not limited to, Student name, Date of Birth, Social Security number, Medicaid number, Date of Service, Service type, Service duration, Student eligibility and information regarding student’s disability and health condition.
• You will be requested to give a one-time consent for the district to access these benefits.
• Refusal to give permission to access public benefits does not relieve the District of its responsibility to
ensure that all required services are provided at no cost to the parent. SHARS is filed monthly for eligible students.
• The district is required to provide you this notice in language that is easily understood by the general
public.
• The district is required to provide you this notice in your native language or other mode of communication if feasible to do so.
• You are notified that you may revoke your consent at any time; however, the revocation is not retroactive.
The district may not 1) require parents to incur out-of-pocket expenses or sign up for public benefits in order for their child to receive services; 2) use benefits that would decrease a child’s lifetime coverage or result in the family paying for services that would otherwise be covered, or 3) use benefits if that use would increase premiums, lead to the discontinuation of benefits or risk loss of eligibility for home and community-based waivers as described in section 300.154. *Please note that the state’s school-based Medicaid Program does not affect an individual’s personal lifetime benefits. If you have any questions regarding the Texas Medicaid Program please contact: TX Health and Human Services Commission Medicaid Client Hotline @ 1.800.252.8263 or * If you have any questions or wish to revoke this consent, please contact:
Neil D. Garza, Special Education Director or Araceli Rodriguez, SHARS at 956-969-6822 School / Department Staff Phone#

Distrito Escolar Independiente de Weslaco Departamento de Educación Especial
Notificación anual de ARD/IEP para acceder a reembolso de Medicaid
Nombre: Fecha de Nacimiento
No. de Identificación
Escuela Grado:
Fecha de Envio
Su Programa de Educación Individualizada (IEP) o de su hijo/a incluye la educación especial y servicios relacionados proporcionados por el personal de Educación Especial del Distrito Escolar de Wéslaco. Uno o más de los servicios basados en las escuelas incluidas en la de su hijo / a o su IEP puede ser elegible para el reembolso federal de Medicaid para el Distrito Escolar Independiente de Wéslaco. Medicaid es un asegurador público que el distrito escolar accede habitualmente a asistir al distrito escolar en el cumplimiento de los costos de proveer educación especial y servicios relacionados. El financiamiento puede ser indagado para el reembolso de los siguientes servicios si son proveídos a su hijo/a o a ustedes que es/son elegibles para el programa de Medicaid: Cuidado Personal Consejería Servicios Psicológicos Servicios de Salud Escolar Servicios de Transportación Terapia del Habla Terapia Ocupacional Terapia Física Evaluación Audiología Nuestros registros indican que usted ya ha dado su consentimiento a WISD para solicitar el reembolso bajo el programa SHARS. Es la intención del Distrito de Wéslaco de acceder el reembolso de Medicaid. De conformidad con las regulaciones federales 34 CFR§300.154 (d) (2) (iv) (A) - (B), se le proporcionará esta Notificación Anual de Intención de Acceso Medicaid reembolso sobre una base anual y: De conformidad con las regulaciones federales 34 CFR§300.154 (d) (2) (iv) (A) - (B), se le proporcionará esta Notificación Anual de Intención de Acceso de reembolso de Medicaid sobre una base anual y:
• Información de identificación personal relacionada con su hijo /usted con respecto a la elegibilidad y los servicios puede ser liberado al programa de Medicaid en las escuelas del estado para el reembolso, incluyendo, pero no limitado a, nombre del estudiante, fecha de nacimiento, número de Seguro Social, número de Medicaid, fecha del servicio , tipo de servicio, duración de servicio, la elegibilidad del estudiante y la información con respecto a la discapacidad del estudiante y condición de salud.
• Se le pedirá a dar un consentimiento de una sola vez para el distrito para acceder a estos beneficios. • Rehusarse a dar permiso para acceder a los beneficios públicos no libera al Distrito de su responsabilidad de
garantizar que todos los servicios requeridos sean proporcionados sin costo alguno para los padres. SHARS se presenta mensualmente para los estudiantes elegibles.
• El distrito está obligado a proporcionarle este aviso en un lenguaje que sea fácilmente entendido por el público en general.
• El distrito está obligado a proporcionarle este aviso en su idioma nativo u otro modo de comunicación de ser posible hacerlo.
• Se le notifica que usted puede revocar su consentimiento en cualquier momento; Sin embargo, la revocación no es retroactiva.
El distrito no puede 1) requerir que los padres incurren gastos directos de su bolsillo o registrarse para obtener beneficios públicos para que su hijo reciba los servicios; 2) utilizar los beneficios que disminuirían cobertura de por vida de un niño o resultar en que la familia pague por servicios que de otra forma estarían cubiertos, o 3) utilizar los beneficios si ese uso aumentaría las primas, conducir a la suspensión de los beneficios o pérdida de elegibilidad para el hogar y exenciones basados en la comunidad, como se describe en la sección 300.154. * Tenga en cuenta que el programa de Medicaid en las escuelas del estado no afecta a los beneficios de por vida personales de un individuo. Si usted tiene alguna pregunta relacionada con el programa de Medicaid de Texas por favor póngase en contacto con: Comisión de TX de Salud y Servicios Humanos Medicaid @ 1.800.252.8263 o
Si tiene alguna pregunta o desea revocar este consentimiento, llame a:
Neil D. Garza, Director o Araceli Rodriguez, SHARS at 956-969-6822 Personal de la Escuela/Departamento TELEFONO #

Section 15

CHILD FIND / CHILD SERVE
6/01
Weslaco Independent School District Child Find Training
Early identification is critical to a child's success in education. Child Find is a system which provides for the early identification of children who may have disabilities and may need Special Education and related services. Special Education services are at no cost to the family and are available to any eligible individual from 3 through 21 years of age. Students with Visual and/or Auditory Impairments may be eligible for services from birth. Educational programs are designed to provide educational benefit for individuals. Types of disabilities include: Physical
may have uneven or no movement may be either physically overactive or passive may be clumsy or make lots of mistakes may have limited strength, vitality or alertness
Deaf or hard of hearing
may have inappropriate response or no response to sound may have chronic middle ear infections may pull at ears
Visual Impairment
may be unable to see things close up and/or far away may avoid eye contact may be unable to follow or focus on objects may be unable to recognize objects/people may squint eyelids together may rub eyes often
Deaf/Blind
no speech or response to sound(s) at an age when speech and hearing would normally be expected
little or no reaction to visual and/or auditory stimuli
CHILD FIND / CHILD SERVE
6/01
Intellectual Disability
does not understand directions or instruction may not play or relate well to others does not identify common objects displays little or no independence depends on others to care for personal and social needs
Learning Disability
may have difficulty learning concepts may have difficulty remembering academic tasks may have difficulty with reading, listening comprehension, spelling, and/or
mathematical tasks
Speech and/or language
may have difficulty pronouncing words may have difficulty being understood by others may have limited speaking skills may have difficulty responding to others may not babble, coo, or talk
Autism
may exhibit repetitive activities and stereotyped movements may not enjoy being touched or cuddled may be resistant to environmental change or changes in daily routines may exhibit unusual responses to sensory experiences
Other Health Impairment
may have learning problems due to health issues may have had an accident or head injury which resulted m a loss of previous learning may experience limited strength, vitality, or alertness, due to chronic or acute
health problems
Traumatic Brian Injury
loss of previous learning as result of a closed or open head injury (loss of learning can be social, educational, physical, or cognitive)

CHILD FIND / CHILD SERVE
6/01
Emotional or Behavioral
may have difficulty learning which cannot be explained by intellectual sensory, or health factors
may exhibit an inability to build or maintain relationships with others may exhibit a pervasive mood of unhappiness or depression may exhibit inappropriate behaviors or have drastic mood swings may have little or no understanding of real dangers may have a need for constant movement
Referral for assessment can be made by the parent, doctor, teacher, family member or other concerned adults. Those who spend time with the child will probably recognize areas of concern that others may not. STEP BY STEP What do I do? 1. Remember it is your responsibility as a district employee to report any student, 3 (Possibly from birth if identified as having a Visual and/or Auditory Impairment) through 21 years of age , who has, or is suspected of having, a disability. 2. Reporting procedures may vary depending on the age and the circumstance of the
student. In all cases documentation must be maintained regarding the referral. 3. Reporting procedures:
a. not currently enrolled in school (0-2 years of age): • initiate referral by calling Region One Service Center (984-0000) and ask for Early Childhood Intervention (ECI). • be prepared to give child's name, phone number and address and reason for
referral
b. currently enrolled in school (3 to 21 years): • initiate referral by contacting child's home campus counselor to assess need
for SHARE Process
4. If you have any questions, contact the Special Education department at (956) 969-6822.

Section 16

RELATED SERVICES
As defined by federal law, the term related service means transportation and such development, corrective, and other supportive services as are required to assist a child with a disability to benefit from special education.
Examples of Related Services include, but are not limited to:
Audiology Counseling Services Early identification and assessment of disabilities Medical services (only to diagnose or evaluate a student's disability) Occupational Therapy Orientation and Mobility Services Parent Counseling and Training Physical Therapy Psychological Services Recreation Rehabilitation Counseling Services School health services Social Work Services in School Transportation

Procedures for Requesting Evaluation for Related Services
As part of the evaluation process (initial FIE or re-evaluation), the evaluations will be comprehensive enough to indicate the need for a related service. In the event that a student's evaluation has occurred and at that time, the evaluation data did not point out a need for related services, but later there is a change in the student's functioning that might point out the need for a related service, the student's regular and or special education teachers will consult with the campus Educational Diagnostician, the student's parent and any other personnel that could provide pertinent information. After this consultation, should it appear that there might be a need for the student to receive related services, an ARD meeting will be convened and a recommendation for an evaluation to determine the need for a related service will be made. At that point, notice and consent for assessment will be obtained from the parent and or adult student. Next, the ARD paperwork will be forwarded to the Educational Diagnostician who is assigned to that campus. The Educational Diagnostician will then complete a request for an evaluation and forward it to the appropriate related service provider so that the evaluation can be completed on a timely basis. Upon completion of the evaluation, an ARD committee will be convened in order to review the results of the evaluation. If the evaluation report indicates that the student qualifies for related services, the services will begin immediately. Please refer to attached guidance from TEA.











Section 17

Assistive Technology
• Assistive Technology Device is defined by IDEA-IA as any item, piece of equipment, or product system, whether acquired commercially, off the shelf, modified or customized, that is used to increase, maintain or improve functional capabilities of a child with a disability.
• Assistive Technology Service is defined as any service that directly assists a child with a disability in the selection, acquisition, or use of an assistive technology device.
• Each student’s ARD committee will determine whether a student needs assistive technology in order for a student to receive a Free Appropriate Public Education.
• For each initial evaluation and three-year re-evaluation, a multidisciplinary team will consider the student’s need for assistive technology. The multi-disciplinary team will be comprised of special education assessment personnel, general education instructor(s) and special education instructor(s). Other related service personnel and/or service providers may be invited to provide input.
• As part of each FIE evaluation report, an Assistive Technology Consideration Form will be completed and included as part of the report.
• If it is determined that a formal Assistive Technology Assessment is needed in order to further determine the needs of any student, special education evaluation personnel will contact the District’s Assistive Technology Team Leader .
• In the event of a need for a formal Assistive Technology Evaluation, Special Education Assessment Personnel will provide the parent with a Notice of Assessment and ensure that written consent is secured. This information will then be turned over to the District Assistive Technology Team Leader.

Procedures for Requesting Assistance from District Assistive Technology Team
1) In order to assist you with an AT evaluation, your campus team must have already collected some evidence of an AT evaluation with the student for whom you request assistance. (It is helpful to remember that AT evaluations are often ongoing and not a one time occurrence.)
2) A completed Student Referral Guide (see attachment) must be submitted to Edna Perez at [email protected] or in person to the WISD Sp Ed Office.
3) After receiving the request for assistance, we will schedule a date and time to come to the student's campus to provide the AT team with on-site technical assistance as they work with the student. (We will not be conducting the evaluation, but will be providing support and recommendations.)
4) Individuals who typically work with the student should be present for the entire evaluation session. This includes teaching assistants, related service personnel, and teachers working with the student. We encourage parents or guardians to provide input as well.
5) The campus team should designate one individual to be the note taker for the evaluation so that all pertinent evaluation data is collected and recorded.
6) We will require 30 minutes before the evaluation to review the student's folder on-site.

Region One VI/Assistive Technology Project (2001) 1
Weslaco Independent School District VI/Assistive Technology Project
Student Referral Guide
Student Name ____________________ DOB __/__/__ Age_______ Grade_______ School __________________________ Teacher ____________________________ Date of ARD requesting Assistive Technology Evaluation _____________________ Disability: (Check all that apply)
Auditory Impairment Autism Deaf-Blind Emotional Disturbance Learning Disability Intellectual Disability Multiple Disabilities Non-Categorical Orthopedic Impairment Other Health Impaired Speech Impairment Traumatic Brain Injury Visual Impairment
Related Services Received:
Occupational Therapy Physical Therapy Other ______________ Check the areas of concern and complete the appropriate sections of the guide.
Mechanics of Writing (Pages 6-7) Math (Page 9) Computer/Device Access (Pages 4-5) Recreation and Leisure (Pages 3-4) Composing Written Material (Pages 7-8) Seating and Positioning (Page 3) Communication (Pages 5-6) Mobility (Page 3) Reading (Page 8) Vision (Page 2) Study Skills (Page 8-9) Hearing (Page 2)
Current Technology: List any assistive technology (including computer hardware and software) being currently used by the student:________________________________________________________ ________________________________________________________________________ What type of computer is available for student use? ______________________________ Typical school platform: ___________________________________________________ Additional Information: __________________________________________________ _______________________________________________________________________ Person completing form: __________________________________________________

Region One VI/Assistive Technology Project (2001) 2
Current Student Status Vision (Should be completed by Vision Teacher)
Acuities if known: __________________ Eye Condition: ________________________________________________________ Visual Abilities: (Check all that apply)
Can read standard textbook print Reads large print in ______ size font Requires special lighting such as __________ Requires specialized positioning of materials such as__________________________ Currently uses a Closed Circuit Television Currently uses a magnification software: _____________________ at ___________X Currently uses a screen reader software: ____________________________________
Current Technology:
Currently uses taped materials versus print or Braille Currently uses Perkins Brailler Currently uses Braille note taking device: ___________________________________
Summary of student’s abilities and concerns related to vision: ________________________________________________________________________________________________________________________________________________ Hearing (Should be completed by Auditorially Impaired Teacher) Hearing Loss identified: Right ear Mild Moderate Severe Profound
Left ear Mild Moderate Severe Profound Hearing Abilities: (Check all that apply)
Attends to sound high pitch low pitch voices background noises Discriminates environmental vs. non-environmental sounds Turns toward sound Can hear some speech sounds Can understand synthesized speech
Student Communication Mode: (Check all that apply)
Speech Gestures Signs Picture Cues Speech and sign together Written messages
Is there a discrepancy between receptive and expressive abilities? Yes No If yes, describe further: _____________________________________________

Region One VI/Assistive Technology Project (2001) 3
Summary of hearing abilities and concerns: ___________________________
_________________________________________________________________
Seating and Positioning: Student’s current seating and positioning: (Check all that apply)
Sits in regular chair Uses tray on wheelchair
Sits in adapted chair Uses adapted table Sits in wheelchair Maintains head control
Uses regular desk Spends part of day out of chair for prescribed Uses desk with height adjusted positioning
Summary of student’s abilities and concerns related to seating and positioning:
___________________________________________________________________ ___________________________________________________________________
___________________________________________________________________
Mobility Student’s current mobility abilities: (Check all that apply):
Walks independently Uses manual wheelchair, independently
Walks with assistance Uses power wheelchair, independently Has difficulty walking Walks with appliance
Is pushed in manual wheelchair
Summary of student’s abilities and concerns related to mobility: _____________________________________________________________________
_____________________________________________________________________ _____________________________________________________________________

Region One VI/Assistive Technology Project (2001) 4
Recreation and Leisure: (Check all that apply) Handles/manipulates objects
Throws/catches objects Operates TV, VCR, Computer, CD Player, etc.
What activities does the student enjoy? ___________________________________
_____________________________________________________________________ Current technology: (Check all that apply)
Toys adapted with Velcro, magnets, etc. Modified utensils, e.g Brushes Switch operated toys Universal cuff or strap
Adaptive sporting equipment Software on computer
Summary of student’s abilities and concerns in the area of Recreation and Leisure: ______________________________________________________________________
______________________________________________________________________
Computer/Device Access: Current fine motor abilities: Observe the student with paper and pencil, computer, switches, etc. Look at the movements as well as the activities and environment. Does the student have voluntary, isolated, controlled movement using: (Check all that apply)
Left hand Right hand Eye(s) Left arm Right arm Head
Left leg Right leg Mouth Left foot Right foot Tongue
Finger(s) Eyebrows Other: ______________
Briefly describe the activities observed: ___________________________________ ___________________________________________________________________
Range of Motion: Student has limitations in range of motion: Yes No
If yes, describe specific range in which the student has the most motor control: ___________________________________________________________________

Region One VI/Assistive Technology Project (2001) 5
___________________________________________________________________
Abnormal reflexes and muscle tone: Student has abnormal reflexes or muscle tone: Yes No If yes, describe the abnormal reflex patterns or patterns of low or high
muscle tone: _________________________________________________________ ____________________________________________________________________
Accuracy: Student has difficulty with accuracy: Yes No
If yes, describe the difficulties with accuracy: _______________________________ ____________________________________________________________________
Fatigue: Student fatigues easily: Yes No
Direct Selection Method: (Check those that apply) Finger Head pointer/stick, mouth stick
Hand Light beam/laser Pointers, hand grips, splints, etc. Eye Gaze
Grid size that student is able to access accurately: 1” 2” 3” 4”
Number of squares across _____________ Number of squares down ___________
Scanning: If student cannot direct select, does the student use scanning?
Yes No If yes: Step Automatic Inverse Preferred control site (body) ____________________________________________
Type of switch: The following switches have been tried: (Check all that apply) Plate Wobble Rocker Joystick
Eyebrow Sip/Puff Flex Mercury (tilt) Other: ____________________________________
Summary of student’s abilities and concerns related to computer/device access: ____________________________________________________________________ ____________________________________________________________________

Region One VI/Assistive Technology Project (2001) 6
Communication Student’s present means of communication: (Check all that apply)
Changes in breathing patterns Body position changes Eye-gaze/eye movement Facial Expressions
Gestures Pointing Sign language approximations Sign language (# signs ____)
Vocalizations, examples ________________ Single words, examples _________________
Yes/No 2 –3 words Examples _________________
Intelligible Speech ___________________ Unintelligible Speech _________________
Communication board (# of symbols____________) See comment on page 10 Voice Output Device (Name of device ________________ # symbols ________)
Writing
Current level of receptive language ______________________________________ Current level of expressive language _____________________________________ Summary of student’s abilities and concerns related to communication:
_____________________________________________________________________ _____________________________________________________________________
_____________________________________________________________________
Mechanics of Writing Current writing ability: (Check all that apply)
Uses regular pencil Can copy words Uses adapted pencil Can copy from board
Can print name Uses regular paper Can print a few words Uses special paper (Example _________)
Can write cursive Writes independently and legibly Fatigues easily when writing Uses Perkins brailler
Writing is slow

Region One VI/Assistive Technology Project (2001) 7
Current keyboarding ability: (Check all that apply)
Does not type Uses portable word processor for typing Types with one finger
Requires wrist or hand support to write Uses adapted keyboard to type ( Name ___________________)
Can perform 10 finger typing (wpm ____________________) Uses switch for typing ( Name ______________________)
Uses adapted software ( Name ______________________)
Summary of student’s ability and concerns related to writing: _______________
____________________________________________________________________ ____________________________________________________________________
Written Composition Student’s present writing is: (Check all that apply)
Single words Paragraphs
Phrases Essays Sentences
Student has difficulty with: (Check all that apply)
Getting started on a sentence or story Using a variety of vocabulary Generating ideas Summarizing information
Adding information to a topic Planning content
Sequencing information
Aids or assistive technology currently used: (Check all that apply) Word cards/books Word Processing Software
Word Wall Talking Word Processing Software Dictionary Abbreviation/Expansion Software
Electronic dictionary Word Processing with Word Prediction

Region One VI/Assistive Technology Project (2001) 8
Talking dictionary Multimedia Software Symbol based software Voice Recognition Software
Portable word processor
Summary of student’s abilities and concerns related to composing written material: ______________________________________________________________________
______________________________________________________________________ ______________________________________________________________________
Reading Student reads at ___________ grade level orally. Student reads at ___________ grade level silently.
Aids or assistive technology currently used: (Check all that apply)
Smaller amount of text on paper Highlighting Enlarged text Talking Dictionary
Lowered reading level Electronic books Audio tapes Books on computer
Reduced length of assignment Computer with talking word processor Colored filters Computerized reading system
Typoscope
Summary of student’s abilities and concerns related to reading: _____________ ____________________________________________________________________
____________________________________________________________________
Study Skills Student has difficulties in: (Check all that apply)
Remembering assignments Remembering steps of assignments/tasks
Taking notes during lecture Reviewing lecture notes

Region One VI/Assistive Technology Project (2001) 9
Organizing notes Turning in assignments
Aids or assistive technology currently being used: ( Check all that apply) Print schedule Palm computers
Low tech aids to find materials (Example _______________________) Highlighting
Voice output reminders Software for manipulation of objects and concepts
Organizational software
Summary of student’s abilities and concerns in the area of learning and studying: _____________________________________________________________________ _____________________________________________________________________
_____________________________________________________________________
Math Student has difficulty with: (Check all that apply)
Legibly writing numbers Understanding math vocabulary Understanding meaning of numbers Understanding place value
Understanding simple math facts Understanding measurement Solving story problems Graphing
Aids or assistive technology currently being used: (Check all that apply)
Abacus Computer calculator Math line Scanning calculator
Enlarged worksheet Alternate keyboards Money calculator/Coinulator Math worksheet software
Tactile/Voice measurement devices Software for manipulation of objects Calculator
Talking calculator
Summary of student’s abilities and concerns related to math:

Region One VI/Assistive Technology Project (2001) 10
_____________________________________________________________________ _____________________________________________________________________
_____________________________________________________________________ General Information
1. Are there any behaviors (positive and negative) that significantly impact the
student’s performance? _________________________________________________________________
_________________________________________________________________ 2. Are there any other factors about the student that the assistive technology
team should consider? ________________________________________________________________
________________________________________________________________
***** Please attach a copy of the student’s communication boards if that area has been checked in the communication section.*****
Campus should plan to have the student folder available for reviewing prior to the assessment. The folder will be reviewed upon arrival at the campus, so time will need to be allowed for this function.

Section 18

Private School Consultation
At the beginning of each school year, Special Education Administration will consult with the representatives of each of the Private Schools that are located within Weslaco ISD boundaries. These consultations will most likely occur through a face to face meeting. In addition, for any students with disabilities that are being home-schooled, the Special Education Administration will place phone calls and/or send written correspondence to the parents of any of these students. The purpose of these phone calls/written correspondence will be to provide the meaningful consultation as required by federal and state law. After the meaningful consultation is completed, Special Education Administration will consider the needs of all of the students and a determination will then be made as to the proportionate share of services to be provided. For students who will be receiving a proportionate share of services, a Services Plan will be developed. Should the parents of the child who resides within the boundary of the District be undetermined as to whether they may want to enroll the child in a WISD school, an ARD Meeting for the purpose of developing an IEP, to offer a Free Appropriate Public Education (FAPE) will be conducted. ARD meetings are not necessary in cases where parents have indicated that they have no intention of having their child attend public school. Students who are 3-5 years old are allowed to be dually enrolled and may be serviced through an IEP even if the parent selects this option.

Section 19

Independent Educational Evaluations & Outside Evaluations brought in by Parents
• Whenever formal evaluations being completed by the district are reviewed at an ARD meeting and parents are not in agreement with the results, they have the right to request an Independent Educational Evaluation (IEE) at the district's expense.
• In instances where this may occur, always ascertain the reason for the
disagreement and document in ARD.
• In instances where an IEE is requested because a parent disagreed with one of the district's evaluations, the educational diagnostician and or speech therapist will immediately inform the Special Education Director so that steps can be taken to provide the parent with information where an IEE can be obtained.
• The district currently maintains of list of qualified evaluators for Full Initial
Evaluations.
• All evaluators utilized for IEEs must have proper certification and or licenses as required by relevant state and federal laws as well as the Texas Education Agency, the State Board of Educator Certification and any boards that may govern that particular profession.
• Upon requests for IEEs from parents who request specific evaluators not
commonly utilized, the district will consider these requests, but will impose a criteria that the evaluator be located within a 250 mile radius of the district.
• In instances when parents present the results of any outside evaluations to the
school staff an ARD meeting must be convened so that the committee can review and consider the results & recommendations of the outside evaluation.
• The ARD committee must review and consider the recommendations and results of IEEs.
• WISD maintains the right to conduct our own evaluation.

Section 20

FOSTER PARENTS/SURROGATE PARENTS
In accordance with state law, whenever a foster parent is representing a student with disabilities, a surrogate parent must be assigned. Primary consideration should be given to assigning the Foster Parent as the Surrogate Parent. The following documents (Designation of Surrogate Parent and Determination of Conflict of Interest) must be completed. These forms are located on SEAS. In the event that a foster parent is representing a student who is receiving special education services, please inform the educational diagnostician and/or speech therapist assigned to your campus. The evaluation and/or campus personnel will consult and make a determination as to whether the foster parent can be assigned as the surrogate parent. If assigned as the surrogate parent, the evaluation personnel will inform the special education director, who will make arrangements to conduct the required training.
8/12

Section 21



Section 22



Section 23

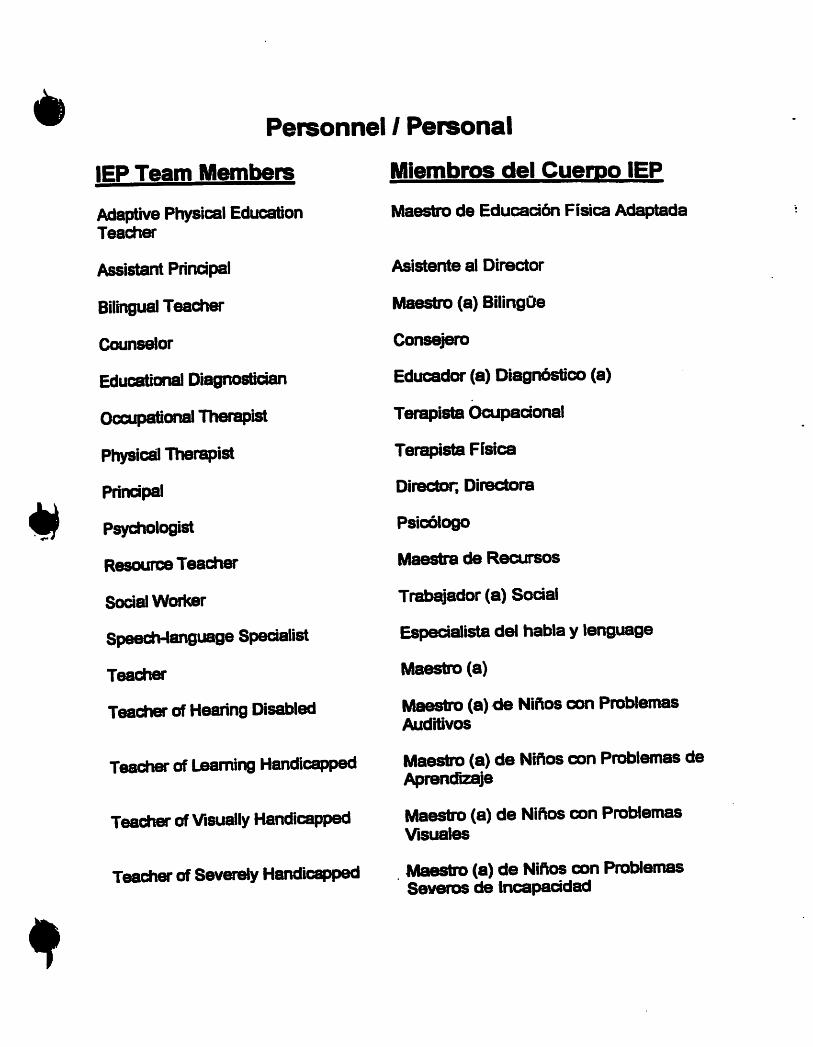

















Section 24

Attachment Index
Attachment Attachment Name
A Parent Language Preference
B Progress Report
C Teacher Student Folder Monitoring List
E Content Mastery Log
E Inclusion Log
F Receipt of Transition Brochure
Fa Transition Planning – Brochure – English
Fb Transition Planning – Brochure - Spanish
FF Transition Checklist
G Student Interview
H Functional Vocational Assessment Teacher Observation Form
I Notice of Agency
J Daily Schedule
K Daily Schedule Planner
L Coordination Cover Sheet
M Coordination of Services
N Verification of Receipt
O Staffing Documentation
P Contact Log
Q Record of Confidentiality
R Student Information PEIMS Verification Sheet
T Counselor Evaluation Referral Form
U Counseling Service Checklist
W Evaluation Report: School Health Service – Example (SEAS form)
X SHARS Transportation Log
Z OT/PT/Speech Request Form

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment A
Parent Language Preference/Lenguaje Preferido por los Padres
Student/Estudiante: D.O.B./Fecha de Nacimiento:
ID# Campus/Escuela:
Dear Parents:
To better serve your needs, we are asking that you please inform us of the language preference in which you would like to receive all correspondence. Please sign the following line if you would like all correspondence in English. This correspondence includes all notices and consents from our department.
Parents
Date
Estimados padres,
Para major servirles, quisieramos que nos informaran de la preferencia de idioma en la que prefieren recibir nuestra correspondencia. Porfavor firme abajo si prefiere recibir nuestra correspondencia en Español. Notificaciones y consentimientos esta incluidos en esta correspondencia.
Padres
Fecha

Weslaco Independent School District Special Education Department
306 N. Bridge Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment B
Attachment B Aug. 2016
ARD Progress Report Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
TEACHER: SUBJECT/AREA: GRADE:
A. Information needed for the ARD Committee C. Information needed for assessment purposes B. Information needed for progress review D. Other:
FROM/RETURN TO: DATE SENT: DATE DUE: ***************************************************************************** PLEASE NOTE: THIS FORM WILL BE A PERMANENT PART OF THE STUDENT’S OFFICIAL SPECIAL EDUCATION FOLDER. Grade Average(s) to date:
Attendance: Tardies Excused Absences ____ Unexcused Absences
I. Check all that apply: 6. Needs to bring material
1. An excellent student 7. Missing assignments/homework 2. Class work is satisfactory 8. Poor class participation 3. Cooperates and works well 9. Needs to study for tests/quizzes 4. Is well behaved and pleasant 10. Becomes easily distracted 5. Exhibits positive attitude 11. Sent to office time(s) for (specify)___
II. Academic Competencies: III. TEKS Objective Weakness (es): Please specify per Subject Area:e.g., (Math, add 2 digits #’s) Please write TEK obj. indicator (e.g.: Alg.1-(4).A, (3).C ) (Reading:Identifies main idea) IV. Modifications appear to be appropriate for this student: YES NO Not Applicable If NO, explain:
V. COMMENTS:
SIGNATURE OF TEACHER/SERVICE PROVIDER DATE
Thank you for your continued commitment to ensure learning for all students.
C O N F I D E N T I A L

Attachment C
Attachment C updated 8/21/12
Weslaco Independent School District Special Education Department 700 S. Bridge, Weslaco TX 78596
Phone (956)969-6822 Fax (956)969-6966
Teacher’s Student Folder Monitoring List
Special Education Teacher: School
Ed. Diagnostician:
Student I.D. D.O.B.

Weslaco Independent School District Special Education Department
700. S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment E
Attachment E 8/12
Content Mastery Log
Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
CODES
R=Reading E=English S=Science M=Math W=Writing / Composition SS=Social Studies Other:
Date Code Time-In Time-Out Total Time Student Signature
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment E
Attachment E 8/12
Inclusion Log
Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
CODES
R=Reading E=English S=Science M=Math W=Writing / Composition SS=Social Studies Other:
Date Code Time-In Time-Out Total Time Student Signature
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -

WESLACO INDEPENDENT SCHOOL DISTRICT Attachment F Special Education Department
700 S. Bridge Weslaco, TX 78596 Phone: (956) 969-6822 Fax: (956) 969-6965
"SUCCESS FOR ALL"
RECEIPT OF TRANSITION BROCHURE / RECIBO DE INFORMACION DE SERVICIO DE TRANSICION
To the parents of/ Para los padres de: Student/Estudiante: D.O.B./Fecha de Nacimiento: Campus/Grade/Escuela/Grado: Re: TRANSITOIN PLANNING/ SERVICES
This notice is to inform you about the Transition Planning. The information in this packet informs you about some of the different services that will be available to your child when he/she turns of age. I would appreciate your signature as an acknowledgement that you have received the packet. Thank you very much for your time. If I can be of any service, please contact me at (956) .
___________________________________________ _____________________ Parent/Guardian/Adult Student Signature Date Re: Plan de Transition/ Servicio's de Transicion
Esta noticia es para informarle del Plan De Transicion. Este paquete es para informarle de varios de los diferentes servicios que van a ser accesibles para su hijo/hija al momento en que tenga la edad apropiada. Le agradezco su firma como reconocimiento que recibio el paquete. Muchas gracias por su tiempo. Si puedo servirle en algo, favor de llamarme al (956) .
_____________________________________________ __________________ Firma de Padre/Estudiante Adulto Fecha





TRANSITION SERVICES CHECKLIST
Student Name: DOB:
P
COMPLETED
Updated 8/17/16
High School - Notification of Transfer of Parental Rights at Age of Majority (turned
18) - Secure at the beginning of the school year.
Receipt of Transition Brochures (signed by parents/adult student)
Individual Transition Plan Meeting Brochure (in parent's language)
Student Interview
Functional Vocational Evaluation (Ex. Functional Vocational: Teacher Observation)
Transition Needs (on or before 14 years of age) on SEAS 2 pg.
High School - Information Regarding Transfer of Parental Rights of Age of Majority (will turn 18) - completed during the 9th grade
ITEM
Notice of ARD (check off R development of transition services…… )
Letter to Parents (list of agencies available) request from Campus Diagnostion.
Consent for Disclosure of Confidential Information For Transition Service (parent's
signature must be secured before sending out the Notice to Agency)
Notice to Agency: Transition Planning/Services Meeting (date sent must be after the
parent's date of Consent for Disclosure)

Page 1 of 3 8/12
WESLACO INDEPENDENT SCHOOL DISTRICT Special Instructional Services
Transition Planning Student Interview
Please Print Date:
Name: _________________________ Male Female
Address: ________________________________________________________________________________________ Street City State Zip Code Home Telephone:__________________________________ Age: _________ Birthdate: __________________ Parent(s)/Guardian(s): _________________________________________________________________ Current School ___________________________________________ Previous School Attended ________________________
Social Security Number: _____-___-_____ How many days of school have you missed in the past years? Please check the appropriate box. Grade: _______________ 0-5 6-10 11-15 16 or over
Home Living What work or chores do you do at home?
If you had to prepare a meal for your family, what would it be?
Do you help with family grocery shopping (yes or no)?
What is your favorite home activity?
Where do you plan to live after graduation?
Are you able to save money to use at a later time (yes or no)?
Who would you contact if there was a serious accident in your home?
Recreation & Leisure
What are your hobbies and spare time activities?
What sports do you play? Where do you play?
Do you read/look at the newspaper? YES NO
Do you like to do things alone or with others? ALONE WITH OTHERS BOTH
Where do you go for fun (i.e. Boys & Girls Club, Youth Group Activities, shopping center, mall)?

Page 2 of 3 8/12
Community Participation Do you have a Texas ID, drivers permit, or license? YES NO
If not, would you like to get one? YES NO
If you are a male and are over the age of 18, have you registered for Selective Service? YES NO
Have you registered to vote? YES NO
If not, do you know how to register to vote?
Where is your favorite place to visit or go shopping?
What are the "Yellow Pages" of the telephone book used for?
Jobs and Job Training
Have you ever been involved in any school/work vocational programs? YES NO
If yes, please list these experiences:
Have you ever filled out a job application? YES NO
If yes, where?
Have you ever had a job interview? YES NO
If yes, where?
Would you like help to improve your job interviewing skills? YES NO
List different jobs/volunteer experiences you have had (paid/Unpaid/volunteer):
1. 2. 3. 4.
Which of the above jobs did you like best?
Are you working now? YES NO
List your job related strengths
List your job related weaknesses:
What do you think would be a good job for you right now?
What kinds of work do you like best?
What annual or hourly wage would you need to make a living?

Page 3 of 3 8/12
Post-Secondary Education
Would you like help in discovering your career interests/abilities? YES NO
What are your favorite classes in school?
What classes would you like to try that you haven't taken yet?
What are things in school that are difficult for you? Circle that apply Students Teachers Lunch Attendance Bus Rides Activities
Which classes are most difficult for you?
After high School, What type of training plans do you have? Specify below your area of interest. For example, auto mechanics, truck driving, secretary, education, etc.
College - Name of the College and area of interest: Technical School - Name of the school and area of interest Military/Branch - Work Force: (Area of Interest?) Stay at Home Other:
What career would you like to have five years from now?
What kind of help do you need to be successful in learning?

Weslaco Independent School District Special Education Department
Functional Vocational Assessment: Teacher Observation Form
Student: _________________________ DOB: _____________ Campus/Gr.: ___________________
Usually Sometimes Never Clean and appropriately dressed Interacts appropriately w/ peers Interacts appropriately w/ adults Follows oral instructions Follows written instructions Is considerate of others Works independently w/ little help Initiates activities/tasks
Assumes responsibility for work Adheres to rules/directions Is able to transfer learning Adapts to changes
Maintains focus/undistracted Remains on task until completion Works at an adequate rate Strives for quality performance
Responds positively to corrections Improves production with instruction Is calm, even tempered Has good self-control
Shows pride in accomplishments Attends school regularly Is punctual
Above Below Avg. Avg. Avg.
Fine motor speed Endurance Comments:
Teacher(s) Completing form Date
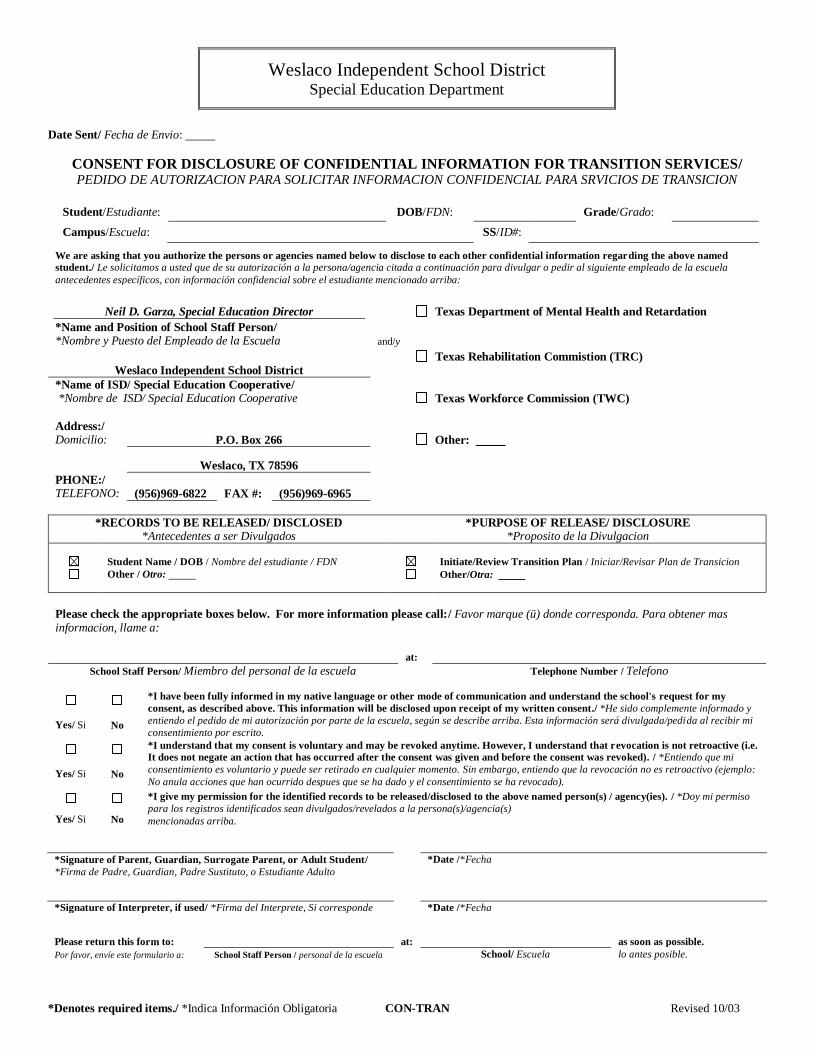
Weslaco Independent School District Special Education Department
*Denotes required items./ *Indica Información Obligatoria CON-TRAN Revised 10/03
Date Sent/ Fecha de Envio:
CONSENT FOR DISCLOSURE OF CONFIDENTIAL INFORMATION FOR TRANSITION SERVICES/ PEDIDO DE AUTORIZACION PARA SOLICITAR INFORMACION CONFIDENCIAL PARA SRVICIOS DE TRANSICION
Student/Estudiante: DOB/FDN: Grade/Grado:
Campus/Escuela: SS/ID#:
We are asking that you authorize the persons or agencies named below to disclose to each other confidential information regarding the above named
student./ Le solicitamos a usted que de su autorización a la persona/agencia citada a continuación para divulgar o pedir al siguiente empleado de la escuela
antecedentes específicos, con información confidencial sobre el estudiante mencionado arriba:
Neil D. Garza, Special Education Director Texas Department of Mental Health and Retardation
*Name and Position of School Staff Person/ *Nombre y Puesto del Empleado de la Escuela and/y
Texas Rehabilitation Commistion (TRC)
Weslaco Independent School District
*Name of ISD/ Special Education Cooperative/ *Nombre de ISD/ Special Education Cooperative Texas Workforce Commission (TWC)
Address:/ Domicilio: P.O. Box 266 Other:
Weslaco, TX 78596
PHONE:/ TELEFONO: (956)969-6822 FAX #: (956)969-6965
*RECORDS TO BE RELEASED/ DISCLOSED *Antecedentes a ser Divulgados
*PURPOSE OF RELEASE/ DISCLOSURE *Proposito de la Divulgacion
Student Name / DOB / Nombre del estudiante / FDN Initiate/Review Transition Plan / Iniciar/Revisar Plan de Transicion
Other / Otro: Other/Otra:
Please check the appropriate boxes below. For more information please call:/ Favor marque (ü) donde corresponda. Para obtener mas informacion, llame a:
at:
School Staff Person/ Miembro del personal de la escuela Telephone Number / Telefono
*I have been fully informed in my native language or other mode of communication and understand the school's request for my
consent, as described above. This information will be disclosed upon receipt of my written consent./ *He sido complemente informado y
entiendo el pedido de mi autorización por parte de la escuela, según se describe arriba. Esta información será divulgada/pedida al recibir mi
consentimiento por escrito. Yes/ Si No
*I understand that my consent is voluntary and may be revoked anytime. However, I understand that revocation is not retroactive (i.e.
It does not negate an action that has occurred after the consent was given and before the consent was revoked). / *Entiendo que mi
consentimiento es voluntario y puede ser retirado en cualquier momento. Sin embargo, entiendo que la revocación no es retroactivo (ejemplo:
No anula acciones que han ocurrido despues que se ha dado y el consentimiento se ha revocado). Yes/ Si No
*I give my permission for the identified records to be released/disclosed to the above named person(s) / agency(ies). / *Doy mi permiso
para los registros identificados sean divulgados/revelados a la persona(s)/agencia(s)
mencionadas arriba. Yes/ Si No
*Signature of Parent, Guardian, Surrogate Parent, or Adult Student/
*Firma de Padre, Guardian, Padre Sustituto, o Estudiante Adulto
*Date /*Fecha
*Signature of Interpreter, if used/ *Firma del Interprete, Si corresponde *Date /*Fecha
Please return this form to: at: as soon as possible.
Por favor, envíe este formulario a: School Staff Person / personal de la escuela School/ Escuela lo antes posible.

WESLACO INDEPENDENT SCHOOL DISTRICT Special Education Department
700 S. Bridge Weslaco, TX 78596
Phone: (956) 969-6822 Fax: (956) 969-6965
NOTICE TO AGENCY: TRANSITION PLANNING/SERVICE MEETING
Agency: Date Sent: Student: D.O.B.: Meeting Date: Time: Location: RM#: The purpose of the meeting is to: The following individuals/agencies are invited to attend and have been notified:
Initiate or Change Transition Planning/Services
Review or discuss Transition Planning/Services
The following areas will be reviewed/discussed:
Instruction Related Services Community Experiences Employment Objectives Post-School Adult Living Objectives Daily Living Skills, if appropriate Functional Vocational Evaluation, if appropriate
Student Parent/Guardian/Surrogate School Administrator .Special Education Teacher .General Education Teacher(s) Vocational Education Teacher Tropical Texas Behavioral Health Supplemental Security Income (SSI) Texas Workforce Solutions Dept. of Assistive and Rehabilitative Services Dept. of Assistive and Rehabilitative Services –
Division for Deaf and Hard of Hearing Dept. of Assistive and Rehabilitative Services –
Division for Blind Service Texas Department of Health & Human
Resources Other: Other:
Please INITIAL the space indicating your response to our invitation to attend this meeting
I will be able to attend the meeting as scheduled.
I would like to attend the meeting, but will be unable to attend as scheduled. Please contact me to discuss re-scheduling.
I will be unable to attend the meeting and ask that you conduct the meeting without me. If the meeting is re-scheduled, please conduct the meeting without me.
For School Use Only:
ITP Meeting Re-scheduled for Date: Time:
Attachment I

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment J
Attachment J 8/12
Dear , I will be working with this school year. Please give me your daily schedule so that I can schedule this student’s special education class(es). You may bring it to room or put it in my box in the workroom. I am looking forward to working with you. Thank you, Your Name Here Special Education Teacher
PERIOD / TIME SUBJECT
General Education Teacher conference time: Special Education Teacher conference time:

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment K
Attachment K 8/12
DAILY SCHEDULE
Teacher: Campus: Setting:
Time: Time: Time: Time: Time: Time: Subject: Subject: Subject: Subject: Subject: Subject:
Time: Time: Time: Time: Time: Time: Subject: Subject: Subject: Subject: Subject: Subject:

Weslaco Independent School District Special Education Department
103 S. IOWA Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment L
Attachment L AUGUST 2010
Coordination Cover Sheet To: ,General Education Teacher From: , Special Education Teacher Date: Subject: Coordination of Services Included in this folder is a copy of (check all that apply): Modifications IEP(s) Behavior Intervention Plan Additional Comments Page (if pertinent) from last annual ARD meeting. The ARD committee determined that these modifications/decisions are necessary for this student to succeed. Please be advised that State and Federal Special Education regulations state that these modifications must be provided. Contact me if you need assistance (or would like additional information) in order to ensure that these modifications are provided in your classroom, or if you have any questions regarding any of the decisions made for this student. My conference period is Refer to the enclosed Coordination of Services (Attachment M) form. This form will need to be submitted to me 3 weeks prior to the ending of each six weeks in order to address any concerns with student progress before report cards are issued.

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment M
Attachment M 8/12
COORDINATION OF SERVICES Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
To: ,General Education Teacher
From: , Special Education Teacher Subject(s):
According to Chapter 75.4 ( ) and (d), the monitoring of special education students needs to occur and be documented to ensure coordination between General and Special Teachers. This form will ensure that coordination effort. *Please notify the Special Education Teacher immediately if at any time you feel this student's progress is unsatisfactory in any subject area.
Form Codes: S = Satisfactory N = Needs Improvement U = Unsatisfactory
1st Six Wks
2nd Six Wks
3rd Six Wks
4th Six Wks
5th Six Wks
6th Six Wks
Student… S N U S N U S N U S N U S N U S N U is maintaining a passing grade, level or levels of mastery. attends school regularly. gets to school on time. brings supplies to class. completes assignments. turns in completed homework. follows directions. keeps up in class with extra help and/or modifications.
maintains appropriate behavior. is cooperative with teachers. is cooperative with fellows students.
Initials of person coordinating Support I may need (Please check those that would best help you in your particular situation.) Help in modifying. Suggestions for behavior management.
Weekly or biweekly conference with special education instructor
regarding student program(s). Reading grade:
Phonics Level: Math grade: English / Writing grade:

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment N
Attachment N 8/12
Verification of Receipt of (check those that apply):
Instructional Modifications IEP BIP STAAR/TAKS Information/District-Wide Assessment Behavioral Medical Concerns
Teacher:
I acknowledge that I have received the above as designated by the ARD Committee on: for
Date of ARD student
I understand that I will receive updated copies as this information changes.
I also acknowledge that:
1. The modifications were explained to me by . Special Education Teacher
2. I understand how to implement the modifications.
3. I can contact at ext. if I need further clarification. Educational Diagnostician
Signature of General Education Teacher Date

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment O
Attachment O 8/12
STAFFING DOCUMENTATION
Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
Staffing Date: Eligibility: REASON FOR STAFFING: Failure Discipline Related Services Other: DISCUSSION: RECOMMENDATIONS:
Signature of Special Ed. Teacher Signature of General Education Teacher
Signature of Other (Specify) Signature of Administrator **Not to be filed in eligibility folder

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment P
Attachment P 8/12
CONTACT LOG
SCHOOL YEAR: -
Student: Campus: Parents: Phone: Person Making Contact: Position: Contact Codes: NF Notification Form TC Telephone Call PC Parent Conference HV Home Visit W Writing (Letter/Note)
DATE CODE COMMENTS / RESULTS

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment Q
Attachment Q 8/12
RECORD OF CONFIDENTIALITY
PERSON REVIEWING FILE MUST HAVE A LEGITIMATE EDUCATIONAL REASON AND MUST SIGN RECORD OF CONFIDENTIALITY FOR: Student’s Full Name:
Birth Date: Address: Home Telephone#: City, Zip:
(If Rural, Specify Location and Description):
Father’s Name: Work#:
Mother’s Name: Work #:
SIGNATURE OF PERSON
DATE
REASON FOR REVIEWING INFORMATION

Weslaco Independent School District Special Education Department
700 S. Bridge / P.O. Box 266 Phone (956)969-6822 Fax (956) 969-6965
Attachment R
Updated 8/12
STUDENT INFORMATION / PEIMS VERIFICATION Teacher name & e-mail: Campus: Date: Page of Diagnostician: Please indicate on the first column by each student if a discrepancy exists between PEIMS Reports and campus folder information. If a discrepancy exists then provide corrected information under the appropriate category. If NO discrepancy exists, you need only to include student’s name, ID, and answer yes/no questions about Sp. Ed. Transportation and Assistive Technology.
Discrepancy? Student' s Name ID#
Disability/ Related Services
Date of Last Annual
FIE Date
*Instructional Arrangement
Code
Sp. Ed. Trans.
Assistive
Technology
YES NO YES NO YES NO

Weslaco Independent School District Special Education Department
Consent to Release Personally Identifiable Information & Access Medicaid Reimbursement Name: DOB: ID:
School: Grade: Medicaid #:
Your child’s Individualized Education Program (IEP) includes special education and related services provided by the Weslaco Independent School District (Weslaco ISD) Special Education staff. One or more of the school-based services included on your child’s IEP may be eligible for Medicaid reimbursement to Weslaco ISD. Medicaid is a public insurer that the Weslaco ISD routinely accesses to assist the school district in meeting the cost of providing special education and related services.
This form is requesting permission to release student information so the District may apply for Medicaid reimbursement under the School Health and Related Services (SHARS) program for designated services listed in the student’s Individualized Education Program (IEP). Schools are required by the Individuals with Disabilities Education Act (IDEA) and the Family Education Rights and Privacy Act (FERPA) to obtain parental consent before disclosing information about a student. * This includes providing the following personally identifiable information to state and/or federal Medicaid agency/ representative and any third party billing company contracted by WISD, including but not limited to student name, date of birth, Social Security number, Medicaid number, date of service, service type, service duration, student eligibility and information regarding student’s disability and health condition.
This form is also requesting permission for WISD to access you/your child’s Medicaid benefits to file for reimbursement for SHARS services provided to your child.
Once the Weslaco ISD obtains this one-time consent, the district will not be required to obtain any further parental consent in the future before it accesses your or your child’s public benefits or insurance regardless of whether there is any change in the type, amount, or cost of services to be billed to the public benefits or insurance program (e.g. Medicaid). However, Weslaco ISD will annually thereafter provide you with written notification that it will access your or your child’s public benefits or insurance.
The district may not 1) require parents to incur out-of-pocket expenses or sign up for public benefits in order for their child to receive services; 2) use benefits that would decrease a child’s lifetime coverage or result in the family paying for services that would otherwise be covered, or 3) use benefits if that use would increase premiums, lead to the discontinuation of benefits or risk loss of eligibility for home and community-based waivers as described in section 300.154.
Weslaco ISD ensures that your child will be provided the services specified in the IEP at no cost to you regardless of whether you consent to Weslaco ISD billing Medicaid for reimbursement; however; your consent will greatly assist the district in providing the highest quality of services to the children served by Weslaco ISD. The money collected from Medicaid is used to expand and enhance medical and related services for children. Your consent is voluntary and may be revoked at any time. Accordingly, the revocation is not retroactive and does not negate reimbursements that may have been received prior to your revocation.
Please check by each statement, sign your name, insert date, and return this form to: at as soon as possible. School / Department Staff School / Department
YES NO I give consent for Weslaco ISD to release personally identifiable information for my child which is outlined and bolded in the above
notice regarding School Health and Related Services (SHARS) my child receives at school to state and/or federal Medicaid agency/ representative and any third party billing company contracted by WISD to determine eligibility and/or to file claims for Medicaid reimbursement. This consent will be effective for the duration of the time that your child is receiving School Health and Related Services (SHARS).
YES NO I acknowledge that I have been fully informed and understand the request for the District to file for reimbursement with the state’s School-based Medicaid Program for my child/me.
YES NO I give consent for Weslaco ISD to file for reimbursement for School Health and Related Services (SHARS) provided for my child/me.
YES NO I have been informed in my native language or other mode of communication.
YES NO I understand that my consent for release of information and for Weslaco ISD to file for reimbursement for (SHARS) is voluntary and can be revoked at any time. However, the revocation is not retroactive.
YES NO I give consent for the filing for reimbursement to begin immediately by waiving the required five (5) school day waiting period between notice of intent to file SHARS and initiation of the filing of SHARS.
_________________________________________________________________ ______________________________________ SIGNATURE OF PARENT, ADULT STUDENT, GUARDIAN, OR SURROGATE PARENT DATE
_________________________________________________________________ ______________________________________ SIGNATURE OF INTERPRETER, IF NEEDED DATE
* If you have any questions, please contact: Neil D. Garza, Director or Araceli Rodriguez, SHARS at 956-969-6822 School / Department Staff Phone#
Or Texas Health and Human Services Commission Medicaid Client Hotline at 1-800-252-8263
Revised 7/8/15

Distrito Escolar Independiente de Weslaco Departamento de Educación Especial
Consentimiento para Divulgar Información de Identificación y Acceso al Reembolso de Medicaid
Nombre: Fecha de Nacimiento
No. de Identificación
Escuela Grado: Medicaid #:
El Plan Individual de Educación (Individual Education Plan o IEP) de su hijo(a) incluye servicios de educación especial y otra asistencia relacionada que son proveídos por el personal del Departamento de Educación Especial del Distrito Escolar Independiente de Wéslaco (Weslaco Independent School District o WISD). Uno o más de los servicios incluidos en el IEP de su hijo califican para que WISD obtenga reembolso de Medicaid. Medicaid es una institución pública de seguros médicos a la cual el Distrito accede rutinariamente para enfrentar los gastos de educación especial y otros servicios relacionados.
Este formulario está solicitando permiso para divulgar la información del estudiante por lo que el Distrito puede solicitar el reembolso de Medicaid bajo del Programa de Servicios Relacionados (SHARS) del programa de servicios designados que se mencionan en el Programa de Educación Individualizada (IEP). Las escuelas están obligadas por la Ley de Discapacidades (IDEA) y los Derechos Educativos de la Familia y la Ley de Privacidad (FERPA) con obtener consentimiento de los padres antes de divulgar información sobre un estudiante. *Esto incluye el suministro de información a la agencia pública y cualquier otra compañía de cobros facturación de los terceros contratada por WISD , incluyendo pero no limitado a, nombre, fecha de nacimiento, número de Seguro Social, número de Medicaid, fecha de servicio, tipo de servicio y duración del servicio.
Este formulario también está solicitando permiso para que WISD acceda a los beneficios de Medicaid suyos o de su hijo para solicitar reembolso por los servicios de SHARS proveídos a su hijo.
Después que WISD obtenga su consentimiento, el distrito no va a requerir en el futuro obtener más consentimientos de los padres antes de acceder beneficios públicos o seguro independientemente de su hijo(a) o de usted, no importa si hay algún cambio en el tipo, cantidad, o costo de los servicios que se facturan a los beneficios públicos o programa de seguros (p. ej. Medicaid). Sin embargo, WISD, anualmente le proporcionara una notificación por escrito de que se tendrá acceso a los beneficios públicos o seguros de su hijo(a) o de usted.
El distrito no podrá 1) requerir que los padres incurren gastos de bolsillo o registrarse para beneficios públicos para que su hijo reciba los servicios, 2) utilizar los beneficios que disminuiría cobertura de por vida de un niño o dar lugar a que la familia pague por servicios que de otra manera estarían cubiertos, o 3) utilizar los beneficios si ese uso sería aumentar las primas, dar lugar a la suspensión de los beneficios o riesgos de pérdida de la elegibilidad de exención en el hogar y en la comunidad, como se describe en la sección 300.154.
WISD le asegura que su hijo(a) recibirá los servicios especificados en el plan individual de educación en forma gratuita, independientemente que el Distrito envíe la cuenta a Medicaid o no; sin embargo, su consentimiento asistirá a WISD a brindarles a los estudiantes servicios de alta calidad. El reembolso recibido de Medicaid se usa para expandir y mejorar la asistencia médica y otros servicios relacionados con los estudiantes. Su consentimiento es voluntario y puede ser revocado en cualquier momento.
Por favor seleccione la respuesta apropiada en cada declaración, firme y escriba la fecha y envié este formulación a:
en lo más pronto posible. Personal de la Escuela/Departamento Escuela/Departamento
SI NO Doy mi consentimiento a Wéslaco ISD a entregar información de identificación personal para mi hijo que se describe y en molde en el aviso anterior sobre Salud Escolar y Servicios Relacionados (SHARS) mi niño recibe en la escuela a otro y / o agencia / representante federal Medicaid y cualquier tercero empresa factura correspondiente contratada por WISD para determinar la elegibilidad y / o presentar las solicitudes de reembolso de Medicaid. Esta autorización será efectiva mientras dure el tiempo que su hijo está recibiendo Salud Escolar y Servicios Relacionados (SHARS).
SI NO Roconozco que he sidoplenamente informado y entiendo la solicitud por medio del Districto a presentar para el reembolso con el Programa de Medicaid en las escuelas del estada para mi hijo/mi.
SI NO Doy mi consentimiento para que el Distrito Escolar de Wéslaco solicite el reembolso de Salud Escolar y Servicios Relacionados (SHARS) previstos para mi hijo.
SI NO He sido informado de todo en mi idioma natal u otro tipo de comunicación.
SI NO Entiendo que mi consentimiento para autorizar entrega de información y para que el Distrito Escolar de Wéslaco solicite el reembolso de Salud Escolar y Servicios Relacionados (SHARS) es voluntario. Si decido revocar mi consentimiento, esto no niega una acción que haya ocurrido después que haya dado el consentimiento y antes que haya sido revocado.
SI NO Doy mi consentimiento para la presentación de reembolso para comenzar de inmediato mediante la renuncia de los cinco requerido (5) días escolares plazo entre la notificación de la intención de presentar SHARS y el inicio de la presentación de SHARS _________________________________________________________________ ______________________________________ FIRMA DEL PADRE, ALUMNO ADULTO, TUTOR LEGAL O SUBSTITUTO (circule el apropiado) FECHA
_________________________________________________________________ ______________________________________ FIRMA DEL INTERPRETE SI SE USO DICHO SERVICIO FECHA Si tiene alguna pregunta, llame a:
Neil D. Garza, Director o Araceli Rodriguez, SHARS At 956-969-6822 Personal de la Escuela/Departamento TELEPHONO #
O llamar a la Comisión de Tejas de Servicios Humanos y Salud al Cliente de Medicaid al 1-800-252-8263
Revised 7/8/15

Weslaco Independent School District Special Education Department
Annual Notice of Intent to Access Medicaid Reimbursement
Name: DOB: ID:
School: Grade: Date Sent:
Your child’s/Your Individualized Education Program (IEP) includes Special Education and Related Services provided by Weslaco ISD Special Education staff. One or more of the school-based services included in your child’s/your IEP may be eligible for federal Medicaid reimbursement to the Weslaco Independent School District. Medicaid is a public insurer that the school district routinely accesses to assist the school district in meeting the cost of providing special education and related services. Funding may be sought for reimbursement for the following services if they are provided to your child/you who is/are eligible for the Medicaid Program:
Personal Care Counseling Psychological Services School Health Services Transportation Services
Speech Therapy Occupational Therapy Physical Therapy Assessment Audiology Our records indicate that you have already provided written consent for WISD to apply for reimbursement under the SHARS program. It is the districts intent to access Medicaid Reimbursement. In accordance with federal regulations 34 CFR§300.154(d)(2)(iv)(A)-(B), you will be provided this Annual Notice of Intent to Access Medicaid Reimbursement on an annual basis and:
• Personally identifiable information related to your child/you regarding eligibility and services may be released to the state’s school-based Medicaid program for reimbursement including, but not limited to, Student name, Date of Birth, Social Security number, Medicaid number, Date of Service, Service type, Service duration, Student eligibility and information regarding student’s disability and health condition.
• You will be requested to give a one-time consent for the district to access these benefits.
• Refusal to give permission to access public benefits does not relieve the District of its responsibility to
ensure that all required services are provided at no cost to the parent. SHARS is filed monthly for eligible students.
• The district is required to provide you this notice in language that is easily understood by the general
public.
• The district is required to provide you this notice in your native language or other mode of communication if feasible to do so.
• You are notified that you may revoke your consent at any time; however, the revocation is not retroactive.
The district may not 1) require parents to incur out-of-pocket expenses or sign up for public benefits in order for their child to receive services; 2) use benefits that would decrease a child’s lifetime coverage or result in the family paying for services that would otherwise be covered, or 3) use benefits if that use would increase premiums, lead to the discontinuation of benefits or risk loss of eligibility for home and community-based waivers as described in section 300.154. *Please note that the state’s school-based Medicaid Program does not affect an individual’s personal lifetime benefits. If you have any questions regarding the Texas Medicaid Program please contact: TX Health and Human Services Commission Medicaid Client Hotline @ 1.800.252.8263 or * If you have any questions or wish to revoke this consent, please contact:
Neil D. Garza, Special Education Director or Araceli Rodriguez, SHARS at 956-969-6822 School / Department Staff Phone#
Distrito Escolar Independiente de Weslaco Departamento de Educación Especial
Notificación anual de ARD/IEP para acceder a reembolso de Medicaid
Nombre: Fecha de Nacimiento
No. de Identificación
Escuela Grado:
Fecha de Envio
Su Programa de Educación Individualizada (IEP) o de su hijo/a incluye la educación especial y servicios relacionados proporcionados por el personal de Educación Especial del Distrito Escolar de Wéslaco. Uno o más de los servicios basados en las escuelas incluidas en la de su hijo / a o su IEP puede ser elegible para el reembolso federal de Medicaid para el Distrito Escolar Independiente de Wéslaco. Medicaid es un asegurador público que el distrito escolar accede habitualmente a asistir al distrito escolar en el cumplimiento de los costos de proveer educación especial y servicios relacionados. El financiamiento puede ser indagado para el reembolso de los siguientes servicios si son proveídos a su hijo/a o a ustedes que es/son elegibles para el programa de Medicaid: Cuidado Personal Consejería Servicios Psicológicos Servicios de Salud Escolar Servicios de Transportación Terapia del Habla Terapia Ocupacional Terapia Física Evaluación Audiología Nuestros registros indican que usted ya ha dado su consentimiento a WISD para solicitar el reembolso bajo el programa SHARS. Es la intención del Distrito de Wéslaco de acceder el reembolso de Medicaid. De conformidad con las regulaciones federales 34 CFR§300.154 (d) (2) (iv) (A) - (B), se le proporcionará esta Notificación Anual de Intención de Acceso Medicaid reembolso sobre una base anual y: De conformidad con las regulaciones federales 34 CFR§300.154 (d) (2) (iv) (A) - (B), se le proporcionará esta Notificación Anual de Intención de Acceso de reembolso de Medicaid sobre una base anual y:
• Información de identificación personal relacionada con su hijo /usted con respecto a la elegibilidad y los servicios puede ser liberado al programa de Medicaid en las escuelas del estado para el reembolso, incluyendo, pero no limitado a, nombre del estudiante, fecha de nacimiento, número de Seguro Social, número de Medicaid, fecha del servicio , tipo de servicio, duración de servicio, la elegibilidad del estudiante y la información con respecto a la discapacidad del estudiante y condición de salud.
• Se le pedirá a dar un consentimiento de una sola vez para el distrito para acceder a estos beneficios. • Rehusarse a dar permiso para acceder a los beneficios públicos no libera al Distrito de su responsabilidad de
garantizar que todos los servicios requeridos sean proporcionados sin costo alguno para los padres. SHARS se presenta mensualmente para los estudiantes elegibles.
• El distrito está obligado a proporcionarle este aviso en un lenguaje que sea fácilmente entendido por el público en general.
• El distrito está obligado a proporcionarle este aviso en su idioma nativo u otro modo de comunicación de ser posible hacerlo.
• Se le notifica que usted puede revocar su consentimiento en cualquier momento; Sin embargo, la revocación no es retroactiva.
El distrito no puede 1) requerir que los padres incurren gastos directos de su bolsillo o registrarse para obtener beneficios públicos para que su hijo reciba los servicios; 2) utilizar los beneficios que disminuirían cobertura de por vida de un niño o resultar en que la familia pague por servicios que de otra forma estarían cubiertos, o 3) utilizar los beneficios si ese uso aumentaría las primas, conducir a la suspensión de los beneficios o pérdida de elegibilidad para el hogar y exenciones basados en la comunidad, como se describe en la sección 300.154. * Tenga en cuenta que el programa de Medicaid en las escuelas del estado no afecta a los beneficios de por vida personales de un individuo. Si usted tiene alguna pregunta relacionada con el programa de Medicaid de Texas por favor póngase en contacto con: Comisión de TX de Salud y Servicios Humanos Medicaid @ 1.800.252.8263 o
Si tiene alguna pregunta o desea revocar este consentimiento, llame a:
Neil D. Garza, Director o Araceli Rodriguez, SHARS at 956-969-6822 Personal de la Escuela/Departamento TELEFONO #

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment T
Attachment T 8/12
Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
COUNSELOR’S EVALUATION REFERRAL FORM Monitoring Teacher: Impairment /Setting:
Reason(s) for Referral
Self-Blame Poor Impulse Control
Anxiety Poor Reality Contact
Withdrawal Poor Sense of Identity
Poor Attention Excessive Aggression
Other
Diagnostician/Special Education Counselor Signature: _________________________________
Date:
To be completed by the Special Education Counselor:
Date Referral Form was received
Date of ARD
Counselor’s Report is Due
Special Education Counselor’s Signature: ___________________________Date: __________ NOTE: Special Education Counselor will file this completed form in office records. Do not include thisin student’s eligibility folder. No other copies should be made of this page.
Director of Special Education

Weslaco Independent School District Special Education Department
700 S. Bridge, Weslaco, TX 78596 Phone (956)969-6822 Fax (956) 969-6965
Attachment U
Attachment U 8/12
Counseling Services Checklist Student/Estudiante: D.O.B./Fecha de Nacimiento: ID #: Campus/ Escuela:
*To be completed by ARD Committee
ATTEMPTED CAMPUS INTERVENTIONS: Y or N RESULTS
Individual Counseling
Group Counseling
Parent Intervention
Teacher/Staff Training
Administrative Conferences
Specific Student Interventions:
*Attendance *Retreats
*CARS
*BIP
*Ropes
*Project Pass *Contract
*Other_________________
Additional Strategies
Note: At least 5 strategies listed should have occurred before student is eligible for referral Comments: Person completing form: ______________________________ Date:__________________

Full and Individual Evaluation Report Information from Licensed Physician (Order or Prescription)
NAME OF PHYSICIAN RECOMMENDING, ORDERING, OR PRESCRIBING HEALTH SERVICES
DIAGNOSTIC IMPRESSION: LEARNING COMPETENCIES:
Good general health Documented hearing loss vision loss Fine Motor Skills are appropriate delayed Gross Motor Skills are appropriate delayed Difficulty maintaining attention Uses Mobility Aids walker wheelchair Wears hearing aids corrective lenses Student is medically fragile Requires special health procedure catheterization suctioning gastrostomy feeding toileting activities of daily living
SPECIFIC HEALTH SERVICES REQUIRED: Dispensing of Prescribed Medication in School
Medication: When Given? Medication: When Given? Training and Supervision of Health Procedures related to: catheterization gastrostomy feeding tracheostomy monitoring suctioning seizures
Monitoring Equipment/Environmental Needs wheelchair braces hearing aids heat/coolness of environment Monitoring: special diet rest periods positioning Periodic Assessment of Medical Condition in Instructional Setting Screening and Referral for Health Needs Consultation with the Physician and parents regarding the effects of medication Counseling with students and their families concerning health care practices and services Training in Emergency Care for Staff and/or Parents
SERVICE RECOMMENDATIONS: Based on the information reported, it is the professional opinion of the school nurse/licensed health professional that this student needs does not need the provision or supervision of the indicated School Health Services by an RN, LVN or Delegated Nursing Services Provider in the school setting, in order to receive education benefit from his/her special education.
Amount of Time: Frequency: daily weekly monthly Duration of Service:
__________________________________________ _______________________ Signature of School Nurse/Licensed Health Professional Date of Report
FIE: Related Service/School Health
Date of Report Initial Evaluation Re-Evaluation
Special Request by ARD CommitteeEVALUATION REPORT: SCHOOL HEALTH SERVICES
Student: Birthdate: Age:Student #: Campus: Grade:
PROFESSIONAL EVALUATOR: School Nurse/Licensed Health Professional
SOURCE OF DATA DATE SOURCE OF DATA DATE
Phone:Fax:
An ARD committee made up of a group of qualified professionals and the parent of the student will complete final determination of eligibility for special education based upon disability and educational need(s).
●
Weslaco Independent School DistrictSpecial Education Department
700 S. Bridge/ P.O. Box 266Weslaco, TX 78596
(956) 969-6822(956) 969-6965
MGARCIA
Typewritten Text
Example of Form
MGARCIA
Typewritten Text
Access in SEAS
MGARCIA
Typewritten Text
MGARCIA
Typewritten Text

Teacher's Name: Month: Year:
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
a.m.S.S. # - - p.m.
1. Please mark an X in the specific box to indicate if the student rode the bus to school and home.2. Please use the following when needed: A=Absent, D=Dropped off, P=Picked Up, W=Weekend.3. Please use the comment lines provided to explain why boxes are left blank (include student's name in case there is more than one student you are referring to.4. The names on this form should only be of those students that are in your class. Please do not include the names of other students not in your class.5. Before submitting this form be sure that all the information is provided accurately. (teacher name, student's name, date of birth, and teacher signature). **Any incomplete forms will be returned.
Teacher's Signature: Date:
Comments:
7/06
School Code:
SHARS Special Transportation LogSpecial Education Department / Fax # (956) 969-6965
Weslaco Independent School District Attachment X
15 MSCS Use Only
16 2524 3130299 10 11 12 191817 23 285 6 7 8 222120 27Student's Name D.O.B. 1 2 3
If you have a special situation or have any questions regarding SHARS procedures on special transportation, please contact Paula Delgadillo 969-6918 ext. 302.
13 144 26

Attachment Z
WESLACO INDEPENDENT SCHOOL DISTRICT SPECIAL EDUCATION DEPARTMENT
Occupational Therapy / Physical Therapy / Speech Therapy
Request Form
Date Requested: Date Needed: (To Be Completed By ): Student Name: D.O.B.: Identification #: School: Parent Name: Home #: Address: Physician Name / Phone & Fax # (Required if requesting evaluation): Diagnostician Ext.
Type of Request
Initial Evaluation 3 Year Re-evaluation
Annual Review Discharge
Equipment Evaluation ARD Meeting
IEP Request Parent Concern
Home Visit Documentation
Progress Reports Closed IEPs Other: .
Comments / Main Concerns---(Specify Interventions Attempted by Teacher):
*ATTACH CONSENT FORM (if applicable) *ALL ITEMS MUST BE ADDRESSED BEFORE PROCESSING