Special Considerations in PRESCRIBING OPIOIDS
42
Information for Prescribers Special Considerations in PRESCRIBING OPIOIDS for Older Adults: Division of Aging, Adult and Behavioral Health Services O F F I C E O F D R U G D I R E C T O R S T A T E O F A R K A N S A S P r e v e n tio n T r e a t m e n t E n fo rc e m e n t This education was made possible by Grant Number 1H79T108700-01 from the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Arkansas Department of Human Services Division of Aging, Adult and Behavioral Health Services (DAABHS).
Transcript of Special Considerations in PRESCRIBING OPIOIDS

Information for Prescribers
Special Considerations in PRESCRIBING OPIOIDS for Older Adults:
Division of Aging, Adult and Behavioral Health Services
OFFIC
E OF DRUG DIRECTO
R
STATE OF ARKANSAS
Prev
entio
n Treatment
Enforcement
This education was made possible by Grant Number 1H79T108700-01 from the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Arkansas Department of Human Services Division of Aging, Adult and Behavioral Health Services (DAABHS).


Opioid Prescribing | 1
Special Considerations in PRESCRIBING OPIOIDS for Older Adults: Information for Prescribers
TABLE OF CONTENTSOpioid Stewardship 3
Special Consideration In Prescribing Opioids For Older Adults 4Older Individuals With Chronic Pain 5Medication Assisted Treatment (MAT) 10
FDA Has Approved The Following Buprenorphine Products 12Co-Occurring Psychiatric Disorders 14
State Prescription Drug Monitoring Programs 15Select An Appropriate Medication 16Execute The Prescription Order 16
Pain Contract: Educate The Patient And Obtain Informed Consent 17
Monitor The Patient’s Response To Treatment 18
Consider Prescribing Naloxone Along With The Initial Opioid Prescription 19Current Naloxone Formulations 20• Evzio• Narcan Injection 0 4mg/mL• Narcan Nasal Spray• Narcan Injection 1 mg/mL

2 | Opioid Prescribing
Summary Of Product Availability And Dosing 22Talking To The Patient About Naloxone 23Starting the Conversation About Naloxone 24
Decide Whether And When To End Opioid Therapy 25
Diagnosing Opioid Use Disorder 26Table 1: Common signs of opioid intoxication and WithdrawalTable 2: Related physical exam findings in substance use disorders Figure 1: Identify and refer urgent problems
Tapering Opioids 30
Treating Opioid Overdose 31Figure 2: Opioid Overdose
Claims Coding And Billing 34Arkansas State Medical Board Rules And Regulations On Opioid Prescribing For Chronic Non-malignant Pain 34
Chronic Non-malignant Pain Opioid Prescribing Checklist 36
MATRIARC 37CAST 37Abbreviations 38References/Resources 39

Opioid Prescribing | 3
OPIOID STEWARDSHIP Opioid overdose is a major public health problem that affects men and women of all ages, ethnicities, and income levels, and involve both illicit drugs such as heroin and prescription opioid analgesics such as hydrocodone, oxycodone and morphine
When treating new patients, a thorough assessment of prior treatment and medications is necessary Obtaining a history of the patient’s past use of medication and checking the Arkansas Prescription Drug Monitoring Program (PDMP) is essential
In emergency situations, doctors should use the smallest dose for pain, not exceed a 3-day supply, and schedule a follow-up visit for the next day In non-emergency situations, only a minimal amount of an opioid analgesic should be prescribed to meet the patient’s needs until the next appointment

SPECIAL CONSIDERATION IN PRESCRIBING OPIOIDS FOR OLDER ADULTSThe conditions below can be precipitated or become worse with opioid use in older adults• Delirium or Acute Changes in Mental Status
(AMS)• High risk for sudden death• Serious drug interaction & serious side
effects secondary to altered metabolism• Cardiac depression with arrhythmias and
heart failure • Respiratory depression• Cognitive impairment/dementia• Anxiety/depression• Fatigue• Gait and balance issues• Sedentary behavior• Sarcopenia• Sleep apnea• Driving difficulties• Severe constipation• Urinary retention• Nausea and/or vomiting• Hypersomnolence• Fall and fall-related injuries with premature
nursing home placement or disability• Serious side-effects of age-associated
reduction in metabolism and reduced creatinine clearance
• Drug interactions with other CNS active drugs
4 | Opioid Prescribing

OLDER INDIVIDUALS WITH CHRONIC PAIN• For all individuals with pain, it is important
that the correct diagnosis is made and that a target suitable for treatment is identified
• In all cases a candid discussion needs to be initiated with patient and/or caregivers about pain relief, functional limitations and quality of life The expectation that pain will be zero with therapy might not always be achievable and realistic
• Emphasis should be on maintaining function and quality of life
• Non-pharmacological therapies should be tried first Physical therapy can be very helpful and has an array of modalities including exercises, ultrasound, dry needling, and other therapies
• Integrative therapy should also be tried and could include: Tai Chai, standard yoga or chair yoga, dance, Pilates, acupuncture, aromatherapy, essential oils, hot or cold therapy, over-the-counter muscle gels/creams, etc
• Age-associated changes in metabolism of drugs: The distribution, metabolism, and excretion of drugs is significantly altered with age In addition, pharmacodynamic variations in elderly patients may increase or decrease sensitivity to a medication independent of pharmacokinetic changes Opioid metabolism is an important safety consideration in older patients with
Opioid Prescribing | 5

complex co-morbidities or inflammation, impaired renal and hepatic function, and impaired immunity Polypharmacy can also lead to drug competition for cytochrome P450 (CYP 450) hepatic enzymes, resulting in increased half-lives of hepatically metabolized drugs Methadone is metabolized mainly by the liver and not removed by dialysis Fentanyl is metabolized and eliminated almost exclusively by the liver
In renal insufficiency, accumulation of metabolites of morphine such as glucuronides can cause intoxication with respiratory depression, sedation, nausea, and vomiting Oxycodone level can increase by approximately 50% in renal insufficiency Oxycodone concentrations are also approximately 25% higher in women vs men after controlling for differences in body weight Regular monitoring of renal and liver function is important in patients on opioids
• Non-narcotic medications such as acetaminophen and NSAIDS should be tried first NSAIDS can have a synergistic effect with acetaminophen for relief of pain Exercise caution for reduced renal function and potential for gastric ulceration in older adults with NSAIDs Limit total dose of acetaminophen to less than 4gms per day and avoid with liver dysfunction
6 | Opioid Prescribing

• Gabapentin is often used, especially for neurogenic pain but needs renal dosing Also exercise caution about increasing the dosage of Gabapentin because it can potentiate the effect of opioids Gabapentin can also increase somnolence and paradoxically increase agitation in some adults
• The same precautions apply to pregablin (Lyrica) as for Gabapentin Pregablin is more potent than gabapentin, hence the CNS side-effects can be more severe
• Cymbalta is also used as a pain modifying drug but special precaution is recommended in older adults because of its side effects of tachycardia, hypertension and vasoconstriction It should be dosed carefully with CAD or tachyarrhythmias and the dose should preferably not exceed more than 30mg daily
• Try extra strength acetaminophen (500mg) or Tylenol arthritis (650mg) bid/tid, or diclofenac (Voltaren) 1% gel, tid/qid
• Low dose muscle relaxants can be used as adjuvant therapy These include cyclobenzaprine, tizanidine and baclofen Use the lowest dose possible because these can cause dizziness and pre-syncope/falls
• Optimize sleep Poor sleep exacerbates pain Use non-pharmacological therapies and instruct on sleep hygiene Simple measures such as eliminating noise or light in the room (e g TV) or a change in mattress or pillow might be helpful Refer to sleep clinic if needed
Opioid Prescribing | 7

• Optimize mood Anxiety and depression can increase pain Antidepressants might be helpful and/or counseling Antidepressants may increase the risk of hyponatremia Avoid benzodiazepines and hypnotics There is a high risk of delirium and falls in older adults taking these Anti-psychotics are sometimes employed in agitated delirium when non-pharmacological methods are not effective In general, quetiapine and olanzapine have less side-effects However, all anti-psychotics carry risks of extra-pyramidal symptoms and prolongation of QT interval with potential torsades de pointes and require careful monitoring
• Optimize social conditions if possible Review history for domestic violence/abuse, nutrition, finances, living situation, alcohol or other substance abuse Refer to a social worker or a nurse care manager
• Other appropriate referrals include those to Physical Medicine and Rehabilitation and Interventional Pain therapy
• Injection therapies might include: steroid injections, radiofrequency ablations or implantable intrathecal pain pump for pain control, or delivering small dosages of morphine or baclofen The intrathecal pain pump can be refilled every 6 weeks to 6 months, depending on the device capacity and requirement
• Nerve/cord compression or other bone related etiologies might require neurosurgery or orthopedic referral
8 | Opioid Prescribing

• OPIOID PAIN MEDICATIONS ARE ONLY TO BE USED AS A LAST RESORT FOR SEVERE PAIN IN OLDER INDIVIDUALS, except in patients suffering from cancer pain and in a palliative care/hospice patient
• Use the lowest dose and least potent opioid, for e g Tylenol # 3
• If the individual is using potent opioid preparations (e g oxycodone), try to gradually reduce to the least potent such as Tylenol # 3
• Opioid Use Disorder (OUD) also occurs in older adults Learn to recognize the signs and symptoms
• Pharmacotherapy in conjunction with psychosocial treatment should be considered for patients with pain who have OUD
Opioid Prescribing | 9

MEDICATION-ASSISTED TREATMENT (MAT)MAT is the use of FDA-approved medications in combination with counseling and behavioral therapies, to provide a “whole-patient” approach to the treatment of substance use disorders Combining medications used in MAT with anxiety treatment medications can be fatal The half-life of anxiolytics such as diazepam is significantly prolonged in older adults MAT should only be provided by physicians trained in the use of the medications for Opioid Treatment Programs (OTP) Medications used for MAT include: methadone, naltrexone or buprenorphine
10 | Opioid Prescribing

• Methadone is quite effective at decreasing cravings for opioids Its use for OUD treatment is limited to specially licensed clinics and pharmacies
• Patients on methadone for the treatment of OUD will require doses of opioids in addition to their regular daily dose of methadone to manage acute pain o The dosing of pain relievers prescribed
may be higher due to tolerance • Patients on methadone for the treatment of
OUD and who are admitted for surgery may require additional short-acting opioid pain relievers
• Buprenorphine or Suboxone has the advantage that it can be prescribed by any physician, nurse practitioner, or physician assistant who has completed eight hours of Suboxone training and has received a DEA-X-waiver Under this waiver they are eligible to administer and/or prescribe buprenorphine medication-assisted therapy to treat OUD An emergency medical technician can also give Buprenorphine in an overdose situation
Opioid Prescribing | 11

FDA HAS APPROVED THE FOLLOWING BUPRENORPHINE PRODUCTS:• Generic Buprenorphine/naloxone sublingual
tablets• Buprenorphine sublingual tablets (Subutex)• Buprenorphine/naloxone sublingual films
(Suboxone)• Buprenorphine/naloxone) sublingual tablets
(Zubsolv)• Buprenorphine/naloxone buccal film
(Bunavail)• Buprenorphine implants (Probuphine)• Buprenorphine extended-release injection
(Sublocade)• For severe acute pain, discontinuing
buprenorphine and commencing on a high potency opioid (such as fentanyl) is advisable o Monitor patients closely and consider
additional intervention such as regional anesthesia
• The decision to discontinue buprenorphine prior to an elective surgery should be made in consultation with the attending surgeon and anesthesiologist o If it is decided that buprenorphine should
be discontinued prior to surgery, this should occur 24-36 hours in advance of surgery and restarted post-operatively when the need for full opioid agonist analgesia has passed
12 | Opioid Prescribing

• Buprenorphine and methadone help reduce cravings by activating opioid receptors
• Naltrexone reduces cravings but blocks opioid receptors There is no abuse and diversion potential with naltrexone
• Naltrexone is available in three forms: tablet (ReVia and Depade), injectable form (Vivitrol) and an implant The pills are 50mg, once daily
• The IM injection, 360mg, is given once a month
• Naltrexone implants are shaped like small pellets and are inserted into the lower abdominal wall Insertion is completed with a local anesthetic Once implanted, the device releases a consistent amount of naltrexone in the body for approximately 3-6 months Currently, implants are only available in an inpatient treatment setting in order to monitor potential side effects
• Using naltrexone together with buprenorphine is not recommended
• Naltrexone will trigger withdrawal symptoms if you are currently physically dependent on opioids It’s important to refrain from taking opioids for a minimum of 7-10 days before taking naltrexone to reduce the risk of a withdrawal
Opioid Prescribing | 13

• Patients on naltrexone will not respond to opioid analgesics in the usual manner Therefore, it is recommended that mild pain be treated with NSAIDS and moderate to severe pain be treated with ketorolac on a short-term basis
• Oral naltrexone should be discontinued 72 hours prior to surgery and extended- release injectable naltrexone should be discontinued 30 days prior to an anticipated surgery
CO-OCCURRING PSYCHIATRIC DISORDERS• A comprehensive assessment, including
determination of mental health status, should evaluate whether the patient is stable o Patients with suicidal or homicidal
ideation should be considered immediately for treatment and possibly hospitalization
• Management of patients at risk for suicide should include:a) Reducing immediate riskb) Managing underlying factors associated
with suicidal intentc) Monitoring and follow-up
• All patients at risk for suicide should be asked about suicidal ideation and behavior
14 | Opioid Prescribing

o Patient with a history of suicidal ideation or attempts should have OUD and psychiatric medication use monitored
• Assessments for psychiatric disorder should occur at the onset of agonists or antagonist treatment o Reassessment using a detailed mental
status examination should occur after stabilization with methadone, buprenorphine, or naltrexone
• Pharmacotherapy in conjunction with psychosocial treatment should be considered for patients with OUD and a co- occurring psychiatric disorder
• Clinicians should be aware of potential interactions between medications used to treat co-occurring psychiatric conditions and OUD
STATE PRESCRIPTION DRUG MONITORING PROGRAMS (PDMP)Prescribers need to enroll in the PDMP and monitor whether a patient is filling prescriptions provided and/or obtainingprescriptions for the same or similar drug from multiple providers Providers can also appoint a delegate to check on the patient’s prescriptions
Opioid Prescribing | 15

SELECT AN APPROPRIATE MEDICATIONThe drug selected should be one that is efficacious, safe, and relevant for the patient’s disease or disorder Physicians should consider the severity of the symptoms, the patient’s reliability in taking medications, the dependence-producing potential of the medication, as well as the side effects - especially in the older population When prescribing, also consider reduced renal and hepatic function in older adults In renal failure, fentanyl and methadone are safer alternatives, but in liver failure, fentanyl might be the only relatively safe option
EXECUTE THE PRESCRIPTION ORDERTo prevent falsification, federal law requires that prescription orders for controlled substances be:• signed and dated on the day they are issued• include patient demographics, physician
demographics, DEA registration number, and MD signature
• specify name and quantity of drug, directions for use, refill information and effective date for filling the prescription
Use the opioid conversion table and reduce dose 30-50% when switching from one opioid to another
16 | Opioid Prescribing

PAIN CONTRACT: EDUCATE THE PATIENT AND OBTAIN INFORMED CONSENT
Ideally, a patient taking an opioid for chronic pain should sign a pain contract with the provider The pain contract should clearly outline the risks and benefits of opioid therapy, the opioid regimen agreed upon, and the name of the pharmacy and treating provider If the patient is not cognitively intact, the pain contract will need to be between the caregiver(s) and provider Patient and care provider(s) need to be informed about the requirements for random drug screens The pain contract should be updated periodically as the treatment plan changes Violations of the pain contract might result in dismissal of the patient from the clinic or from the provider’s practice Providing informed consent educates the patient about the risks and benefits of opioid therapy and the legal and ethical obligations of both the patient and physician Informed consent should specifically address the potential for physical dependence and cognitive impairment as side effects of opioid analgesics Patients should be educated on how to take opioids and when to not take them Patient education improves medication use and adherence Patients and caregivers need to be educated about naloxone therapy for overdose
Opioid Prescribing | 17

MONITOR THE PATIENT’S RESPONSE TO TREATMENTMonitor patients and document for drug efficacy, safety, compliance, and potential development of tolerance Consider both subjective and objective symptoms that may serve as early signs of therapeutic failure or unacceptable adverse drug reactions that may indicate a modification of the treatment plan Giving patients the task of keeping a log to monitor symptoms provides them with a sense of participation In addition, patients should be informed that pain medication is only part of an overall treatment plan In patients taking opioids, it is important to do a:• cognitive history• driving evaluation• psychiatric evaluation• polypharmacy evaluation
18 | Opioid Prescribing

CONSIDER PRESCRIBING NALOXONE ALONG WITH THE INITIAL OPIOID PRESCRIPTIONWith proper instructions on use, a naloxone kit is recommended for patients who are:• Taking high doses of opioids for long-term
management of chronic pain (> 50 MMEs) morphine mg equivalent
• Discharged from emergency medical care after opioid intoxication/poisoning
• At high risk for overdose because of a legitimate medical need for analgesia and with a suspected history of substance use disorder
• On certain opioids (extended release/ long acting) or benzodiazepines that may increase the risk for overdose
• Have completed a mandatory opioid detoxification or abstinence program
• Have recently been released from incarceration with a history of opioid use disorder
• Overdose plan for at-risk patient to share with family, friends, or significant others regarding signs of overdose,
and how to give naloxone, or to call 911
Opioid Prescribing | 19

CURRENT NALOXONE FORMULATIONSEvzio:• Approved by the FDA in 2014• 1 box contains two, single-use naloxone
auto injection devices• Electronic, voice-directed• 2mg/0 4mL• Injects 2 mg naloxone either IM or SubQ• Hold to person’s thigh-- even over clothing
Cost:Expensive ($4,000-$4,500 out of
pocket)Not well covered yetCommunity pharmacies not stocking in
most cases
Naloxone Injection 0.4mg/mL:• Generally administered by a healthcare
professionalOr must sell syringe and needle
• Comes in 1 ml vials, 10 per package• Administer 1 ml IV, IM SubQ• Have the trust of the patient/family/friend
to administer correctly Cost:0 4 mg/ml is affordable (need out-of-
pocket cost for 0-4mg/ml & 1,g/ml)Many pharmacies do not stock
20 | Opioid Prescribing

Narcan Nasal Spray:• Approved as a 4 mg dose in 2015• Approved as a 2 mg dose in 2017
Not yet available• 2 nasal spray bottles per box• 1 applicator per nostril
Cost:$140-$150 out-of-pocket for patient
$0 co-pay for Medicaid Less than $15 from other insurers
Naloxone usually stocked as Narcan by pharmacies
Narcan Injection 1 mg/mL:• Comes in 2 ml pre-filled Luer-Lock Syringe• Packaged as an injection but can administer
intranasal• Requires nasal atomizer device• Administer ½ syringe (1 ml) in each nostril
Naloxone products should be kept at room temperature and protected from light Make sure the product is not expired Naloxone will not be effective in overdose from cocaine, benzodiazepines, or alcohol
Opioid Prescribing | 21

SUMMARY OF PRODUCT AVAILABILITY AND DOSING1 Narcan® Nasal Spray (naloxone HCl)
4mg/0 1ml Nasal Spray• Directions for use: Administer one (1)
spray of Narcan® in one nostril Repeat after three (3) minutes if no response
2 Naloxone HCl Solution 1 mg/ml in a 2 ml pre-filled Luer-Lock Syringe• Directions for use: Spray 1 ml (1/2 of
syringe into each nostril Repeat after three (3) minutes if no response
3 Evzio® (naloxone HCI injection) 2 mg/0 4 auto injector
• Directions for use: Follow audio instruction from device Place on thigh and inject 0 4 ml Repeat after three (3) minutes if no response
22 | Opioid Prescribing
You can download the “Narcansas” app on your cellphone, tablet or computer. It is free. This App provides for life saving information
and resources on opioids. The NARCANsas app will provide you with resources, links, and tools that will help you administer the drug
naloxone in the moment of an opioid overdose and provide steps on how to save a person’s life. The app also has information for
treatment, prevention and recovery. FOR ANDROID USERS: Google Play: https://bit.ly/2VYcpq8
FOR APPLE USERS: I-Tunes: https://itunes.apple.com/us/app/narcansas/id1460163807?mt=8

Opioid Prescribing | 23
TALKING TO THE PATIENT ABOUT NALOXONE AT THE PHARMACY
Scenario: Patient picking up a prescription for an opioid medication such as Percocet or Norco
New Prescription Chronic UseTechnician: I see that this is a new prescription for you. The pharmacist will be over in just a moment to talk to you about your prescription. Are you familiar with naloxone?
Technician: I see that you have been taking a Percocet prescription for some time. I know you may or may not have any new questions about this for the pharmacist, but are you familiar with naloxone?
Patient: No, I’ve never heard of it.
Technician: Naloxone is a medication that can be used in case of a serious side effect to your new medication. It is a similar concept to having an Epipen® in case of an allergic reaction. If you are interested I can provide you with information to look at while you wait for the pharmacist who will be happy to go through all the details and answer any questions you might have. If you are interested, it won’t require a visit to your doctor. We will be able to initiate everything here and process it through your insurance so you can take it home with you today.
Patient: Sure, I will look at the information and talk to the pharmacist. Thank you for letting me know about it.

24 | Opioid Prescribing
STARTING THE CONVERSATION ABOUT NALOXONEStarting a conversation about naloxone can help initiate a general dialogue on opioid-use disorder (OUD) with a patient or caregiver who had been reluctant to discuss it before Wider availability and use of the opioid overdose antidote naloxone, can lower the deadly toll of the opioid epidemic When talking with patients or caregivers about naloxone, physicians need to be ready to answer patients’ questions, respond to any resistance, and work to reduce the stigma that is still often attached to opioid-use disorder and its treatments Having a naloxone kit at home is like having easy access to a fire extinguisher Tell the patient that all that is cared about is their safety and health and that naloxone can save their life or potentially save a friend’s life Naloxone will not do any good if it sits in a drawer and nobody knows where it is, so discuss it with a family member or trusted friend so they will be able to administer it if the need arises In addition, physicians need to counter the notion that providing naloxone is enabling drug abuse Greater awareness about the potential for overdoses and how naloxone can reverse them has led to people taking less offense at bringing this up Physicians must be both tactful and frank, even if the patient is initially offended The overall objective is to see naloxone made available a lot more often, especially for those who are at risk

Opioid Prescribing | 25
DECIDE WHETHER AND WHEN TO END OPIOID THERAPYOut-of-control behaviors may warrant immediate cessation of prescribing This includes altering or selling prescriptions, accidental or intentional overdose, multiple episodes of running out early (due to excessive use), and doctor shopping or engaging in threatening behaviors In all cases, patients should be given the benefit of the physician’s concern and attention Even drug- seeking patients often have very real medical problems that demand and deserve the same quality medical care offered to any patient Hence, it is good to have an opioid contract with every patient that both patient/caregiver(s), and provider(s) sign

26 | Opioid Prescribing
DIAGNOSING OPIOID USE DISORDER (OUD)Other clinicians may diagnose OUD, but confirmation of the diagnosis by the provider with prescribing authority and who recommends medication use, must be obtained before pharmacotherapy for OUD commences OUD is primarily diagnosed based on the history provided and a comprehensive assessment that includes a physical examination Validated clinical scales that measure withdrawal symptoms may be used to assist in evaluation Urine drug testing is recommended during the comprehensive assessment and frequently during treatment Determine the frequency of urine drug testing by assessing the stability of the patient, the type of treatment, and the treatment setting In tables 1 and 2, respectively, are common signs of opioid intoxication, withdrawal scales, and related physical exam findings in substance use disorders

Opioid Prescribing | 27
Table 1. Common Signs of Opioid Intoxication and withdrawal
Signs of Opioid Intoxication
• Drooping eyelids• Constricted pupils• Reduced respiratory rate
• Scratching (due to histamine release)• Head nodding
Signs of Opioid Withdrawal
OOWS (objective opioid Withdrawal scale)
SOWS (subjective opioid withdrawal scale)
COWS (clinical opioid withdrawal scale)
• Yawning• Rhinorrhea• Piloerection (observe arm)• Perspiration• Lacrimation• Tremor (hand)• Mydriasis• Hot and cold flushes• Restlessness• Muscle twitches• Abdominal cramps• Anxiety
• I feel anxious.• I feel like yawning.• I’m perspiring.• My eyes are tearing.• My nose is running.• I have goose flesh • I am shaking.• I have hot flashes.• I have cold flashes.• My bones and muscles ache.• I feel restless.• I feel nauseous.• I feel like vomiting.• My muscles twitch.• I have cramps in my stomach.• I feel like shooting up now.
• Pulse• Sweating• Restlessness• Pupil size• Bone or joint aches• Rhinorrhea• Tearing• GI upset• Tremor of out-
stretched hands• Yawning• Anxiety or irritability• Gooseflesh skin

28 | Opioid Prescribing
Table 2. Related Physical Exam Findings in Substance Use Disorders
System Findings
Dermatologic Abscess, rashes, cellulitis, thrombosed veins, jaundice, scars, track marks, pock marks from skin popping
Ear, nose, throat and eyes
Pupils pinpoint or dilated, yellow sclera, conjunctivitis, rhinorrhea, rhinitis, excoriation or perforation of nasal septum, epistaxis, sinusitis, hoarseness or laryngitis
Mouth Poor dentition, gums disease, abscesses
Cardiovascular Murmurs, arrhythmias
Respiratory Asthma, dyspnea, rales, chronic cough, hematemesis
Musculoskeletal and extremities
Pitting edema, broken bones, traumatic amputations, burns on fingers
Gastrointestinal Hepatomegaly, hernias

Opioid Prescribing | 29
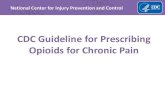
Figure 1. Evaluation and Treatment
Identify and refer urgent problems
History• Concomitant medical
conditions (hepatitis, HIV, TB, acute trauma)
• Other substance use including tobacco
Mental Health Status• (See Co-Occurring
Psychiatric Disorders)
Laboratory• CBC, LFTs, HIV, hepatitis
A, B & C• Urine drug testing
(frequently)• STDs (?)
Physical
Social and Environmental Factors
• Offer hepatitis B vaccine (?)• Withdrawal management (WM)
LEGENDDiagnosis/EvaluationTreatmentResults, Notes, Status
Select treatment site
Level 1Outpatient,
general medical or
addiction/WM
Level 2Specialty addiction
intensive out-patient/WM
Level 3Residential/
WM
Level 4Hospital/WM
Procedure1. Change in
treatment plan - focus on medication adherence
2. Consideration of intensity of care
3. Switch Medications
To address withdrawal symptoms, add:• Clonidine • Other ancillary medications
NaltrexoneMethadoneBuprenorphinea
Painrefer to the page(s) in this
document that address pain
Psychosocial treatment
Relapse Relapse prevention Switch medications

30 | Opioid Prescribing
TAPERING OPIOIDSReduce opioids by 5-10% every visit and taper over several months
TREATING OPIOID OVERDOSEIt is possible to reverse respiratory depression of opioids through respiratory support to include emergency resuscitation and giving the opioid antagonist – naloxone The safety of this drug is high, and it is approved by the FDA Naloxone can trigger unpleasant withdrawal symptoms Therefore, some persons may become agitated or even combative and will need help to remain calm (SAMHSA, 2016) The American Society of Addiction Medicine (ASAM) provides specific steps for opioid overdose
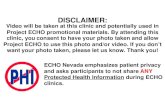
Figure 2. Overdose
Step 2: Recognize Overdose• Extreme sleepiness, inability to awaken
verbally or upon sternal rub • Breathing problems can range from slow
to shallow breathing in a patient that cannot be awakened
Step 1: Call for Help (Dial 911)AN OPIOID OVERDOSE NEEDS
IMMEDIATE MEDICAL ATTENTION.

Opioid Prescribing | 31
Step 3: Support Respiration• Verify that the airway is clear • With one hand on the patient’s chin, tilt the
head back and pinch the nose closed • Place your mouth over the patient’s mouth
to make a seal and give 2 slow breaths (the patient’s chest should rise, but not the stomach)
• Follow up with one breath every 5 seconds
Step 4: Administer Naloxone• For the initial treatment of opioid
intoxication of a patient, the American Heart Association recommends, after initiation of CPR, the use of intranasal or IM naloxone If there is an initial patient response (i e , purposeful movement, regular breathing, moan, or other response), but the patient then stops responding, begin CPR again, repeat naloxone dose and provide external oxygen support if available If no initial response, continue CPR If in the field, use an automated external defibrillator (AED) as appropriate
Step 2: Recognize Overdose (cont.)• Fingernails or lips turning blue/purple• Extremely small pupils - “pinpoint pupils”• Slow heartbeat and/or low blood pressure

32 | Opioid Prescribing
Step 4: Administer Naloxone (cont.)• IV, IM, SQ: Initial: 0 4 to 2 mg; may need
to repeat doses every 2 to 3 minutes A lower initial dose (0 1 to 0 2 mg) should be considered for patients with opioid dependence to avoid acute withdrawal or if there are concerns regarding concurrent stimulant overdose IM and SQ naloxone have a slower onset of action compared to IV injection but have a prolonged effect After reversal, one may need to re-administer dose(s) at a later interval (i e 20 to 60 minutes) depending on type/duration of action of opioid (e g , methadone) If no response is observed after 10mg total, consider other causes of respiratory depression Injection solution can also be sprayed into the nostril Spray 1 ml (1/2 of syringe) into each nostril This can be repeated after 2-3 minutes if no response
• IM, SQ naloxone (Evzio): This is available as a 2-pack with two auto-injectors of 2 mg (1 prefilled auto-injector) When activated, the device provides verbal instructions for IM or SQ injections Give as a single dose of 2 mg; may be repeated every 2 to 3 minutes until emergency medical assistance becomes available (no assembly required, can be used by non-medical personnel)

Step 4: Administer Naloxone (cont.)• Intranasal naloxone spray (Narcan): Onset
of action is slightly delayed compared to IM or IV routes Give 4 mg (contents of 1 nasal spray) as a single dose in one nostril; may be repeated every 2 to 3 minutes in alternating nostrils until medical assistance becomes available, or if respiratory depression persists (no assembly required, can be used by non-medical personnel)
Step 5: Monitor the Patient’s Response• Most patients respond to naloxone by
returning to spontaneous breathing, with mild withdrawal symptoms The response generally occurs within 3-5 minutes of nalozone administration (Rescue breathing and/or oxygen support should continue while waiting for the naloxone to take effect )
• The duration of effect of naloxone is 30-90 minutes depending on dose and route of administration Patients should be observed after that time for re-emergence of overdose symptoms More than one dose of naloxone may be required to revive the patient
• The goal of naloxone therapy should be restoration of adequate spontaneous breathing, but not necessarily complete arousal.
Opioid Prescribing | 33

CLAIMS CODING AND BILLINGMost insurance plans, including Medicare and Medicaid, cover the cost of naloxone The codes for Screening, Brief Intervention and Referral to Treatment (SBIRT) can be used to counsel a patient on recognizing opioid overdose and how to administer Naloxone The Centers for Medicare and Medicaid Services (CMS) Medicare Learning Network (MLN) provides a printer-friendly booklet for SBIRT that contains information regarding eligible providers under Medicare, Medicaid and dual eligibles that may be found at https://www cms gov/Outreach-and- Education/Medicare- Learning-Network-MLN/ MLNProducts/Downloads/SBIRT_ Factsheet_ICN904084 pdf
ARKANSAS STATE MEDICAL BOARD RULES AND REGULATIONS ON OPIOID PRESCRIBING FOR CHRONIC NONMALIGNANT PAINArkansas State Medical Board has rules and regulations for licensed prescribers who prescribe opioids and/or benzodiazepines for chronic nonmalignant pain • Prescriber or prescriber’s designated
delegate must check the information in the Prescription Drug Monitoring Program (PDMP) every time when prescribing a Schedule II or Schedule III opioid and the first time a benzodiazepine is prescribed to a patient
34 | Opioid Prescribing

Opioid Prescribing | 35
Prescriber must document in the patient record that the PDMP was checked before prescribing
• Written informed consent must be obtained from patients with a risk of substance abuse and the risk and benefits of opioids must be discussed with the patient, guardian, or authorized representative
• A signed pain contract must be obtained with the expectations for the behavior of the patient, which may include random urine drug screens and random pill counts
• Patient must be evaluated at least once every six months by a physician who is licensed by the Arkansas State Medical Board
• Periodical reviews of the schedule drug treatment should be conducted with the patient and any new information about etiology
• Accurate records should be kept of medical history physical examination, evaluations and consultations, treatment plan objectives, informed consents, agreements, and medication prescribed

36 | Opioid Prescribing
Check the PDMP before prescribing any controlled substances.
CHRONIC NONMALIGNANT PAIN OPIOID PRESCRIBING CHECKLIST
• Check PDMP every time when prescribing a Schedule II or Schedule III opioid and the first time a benzodiazepine is prescribed
• Document in the patient record that the PDMP was checked
• Consider multimodal therapies such as superficial cold/heat therapy, spinal manipulation, physical therapy, psychotherapy, acupuncture, massage, etc
• Get informed consent with discussion of benefits and risks of opioid therapy noted in the patient record
• Get a signed pain contract and baseline urine drug screen
• Use the lowest effective dose of opioids Use caution and reassess before increasing dosage to > 50 morphine milligram equivalent (MME) per day Avoid increasing dosage to > 90 MME/day
• Conduct random urine drug screens and pill counts
• Evaluate the patient ideally every three months
• Review treatment plan with assessment of appropriateness

Opioid Prescribing | 37
• Document medical history, physicals, evaluations and consultations, treatment plan, informed consents, agreements, and prescribed medications in the patient record
• Co-prescribe naloxone when clinically appropriate and when on >_ 50 MME per day of opioids
• Advise how to properly secure all medications
• Advise where and how to safely dispose of all unused, unwanted or expired medications
Note:MATRIARC (Medication Assisted Treatment Recovery Initiative for Arkansas Rural Communities) is a partnership with the Psychiatric Research Institute and the Arkansas Department of Human Services designed to expand evidence-based treatment for opioid use disorder The service is available Monday through Friday, from 8:30 a m to 4:30 p m excluding state holidays Call (501) 526-8459 or (833) 82-7404 to speak with a trained addiction specialist
The Psychiatric Center for Addiction Services and Treatment (CAST) provides medication assisted treatment (MAT) to treat opioid use disorders A handbook outlining all of the criteria for admission as well as the details of the program and a fee schedule is available upon request To get help, contact CAST at (501) 526-8400 and request Suboxone information

38 | Opioid Prescribing
ABBREVIATIONS:AFMC – Arkansas Foundation for Medical Care
ASAM – American Society of Addiction Medicine
COWS – Clinical Opioid Withdrawal Scale
FDA – Food and Drug Administration
MME – Morphine Milligram Equivalent
NSAID – Non-Steroidal Anti-inflammatory Drug
OOWS – Objective Opioid Withdrawal Scale
OUD – Opioid Use Disorder
PDMP – Prescription Drug Monitoring Program
SAMHSA – Substance Abuse and Mental Health Services Administration
SOWS – Subjective Opioid Withdrawal WM – Withdrawal Management

Opioid Prescribing | 39
REFERENCES/RESOURCES:1 The ASAM National Practice Guideline for
the Use of Medications in the Treatment of Addiction Involving Opioid Use Available at http://www asam org/docs/default-source/ practice-support/guidelines-and-consensus-docs/national-practice-guideline pdf
2 http://afmc org/opioids
3 http://www artakeback org/
4 https://arkansaspmp com
5 https://www armedicalboard org/Professionals/pdf/mpa pdf
6 http://www asam org/docs/default-source/ practice-support/quality-improvement/ asam-standards-of-care pdf
7 http://www asam org/publications/ the-asam-criteria
8 ASAM GuidelineCentral com for calculators
9 Hayes, Cory PharmD, MPH Naloxone: Formulations, Cost, and When to Talk to the Patient UAMS Geriatric Grand Rounds March 3, 2020
10 Naloxone: 5 tips on talking with patients, families Andis Robeznieks August 2018 https://www ama-assn org/delivering-care/opioids/naloxone-5-tips-talking-patients-families

OFFIC
E OF DRUG DIRECTO
R
STATE OF ARKANSAS
Prev
entio
n Treatment
Enforcement
Disclaimer:Information provided in this booklet should only be used as a guideline. Initial judgment concerning any course of action should be made by the health care professional after careful consideration of the individual patient. Neither the University of Arkansas for Medical Sciences (UAMS) Reynolds Institute on Aging (RIOA), the Department of Human Services (DHS) Division of Aging and Adult Behavioral Health Services (DAABHS), nor the authors endorse any product or services associated with this clinical reference tool or information contained in this booklet.