Prescribing Opioids in the ED
48
American College of Emergency Physicians Clinical Policy: http://www.acep.org/clini calpolicies/ Critical Issues in the Prescribing of Opioids for Adult Patients in the Emergency Department Created by Danielle S. Campbell, Project Coordinator Subject Expert: Knox Todd, MD
-
Upload
danielle-campbell -
Category
Documents
-
view
35 -
download
1
Transcript of Prescribing Opioids in the ED
American College of Emergency Physicians Clinical Policy:
http://www.acep.org/clinicalpolicies/
Critical Issues in the Prescribing of Opioids for Adult Patients in the Emergency Department
Created by Danielle S. Campbell, Project CoordinatorSubject Expert: Knox Todd, MD
*This photo is used as a courtesy from Johns Hopkins Medicine.7/24/2013
High Pain Prevalence
Press Ganey
Prescription Opioid Abuse
The Joint Commission
Pain Management in the Emergency Department
ED Physicians Must Balance
undertreatment
misuse
with
Unintended Consequences
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Prop
ortio
n rece
iving op
ioids
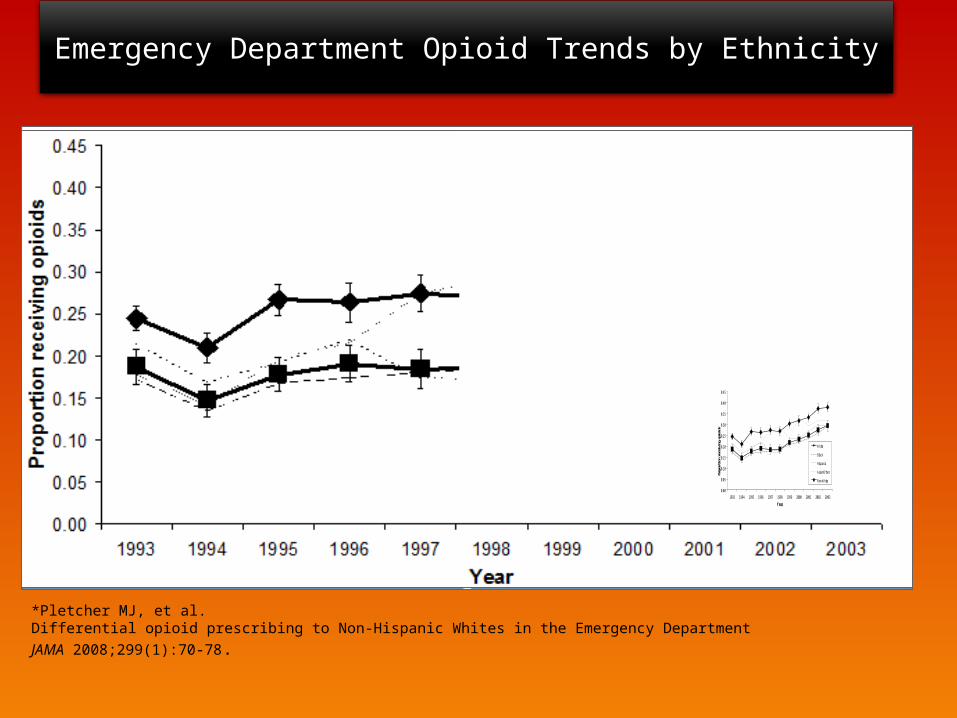
White
Black
Hispanic
Asian/Other
Non-White
*Pletcher MJ, et al. Differential opioid prescribing to Non-Hispanic Whites in the Emergency DepartmentJAMA 2008;299(1):70-78.
Emergency Department Opioid Trends by Ethnicity
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Prop
ortio
n rece
iving op
ioids
White
Black
Hispanic
Asian/Other
Non-White
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Prop
ortio
n rece
iving op
ioids
White
Black
Hispanic
Asian/Other
Non-White
*Slide used as a curtsey from pinterest
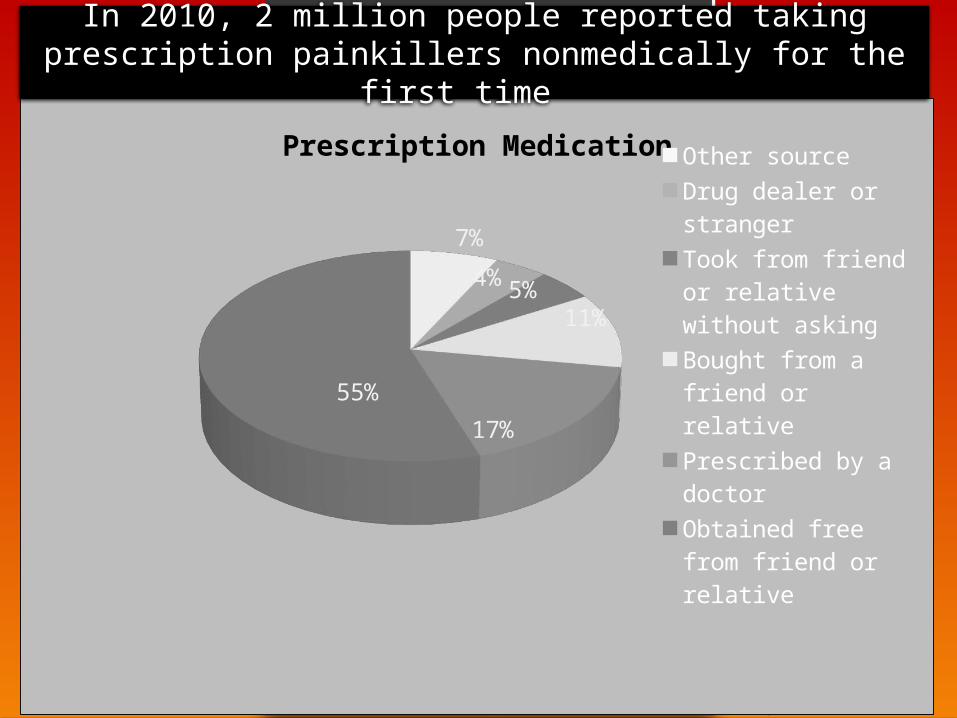
7%
4%5%11%
17%55%
Prescription MedicationOther source
Drug dealer or stranger
Took from friend or relative without asking
Bought from a friend or relative
Prescribed by a doctor
Obtained free from friend or relative
In 2010, 2 million people reported taking prescription painkillers nonmedically for the first time

Risky Patients
Risky Pills
Emergency Department Opioid Prescribing
http://www.acep.org/clinicalpolicies/
Emergency Physicians, as a specialty, are higher prescribers of opioids for patients between the ages of 10 to 40 years.
American College of Physicians Progression of Public Policies
PROPERTIESAllow user to leave interaction: After viewing all the stepsShow ‘Next Slide’ Button: Show upon completionCompletion Button Label: Next Slide
Stephen V. Cantrill, MDMichael D. Brown, MD, MSCRussell J. Carlisle, MDKathleen A. Delaney, MDLewis S. Nelson, MDRobert E. O’Connor, MD, MPH Ann Marie Papa, DNP, RN, CEN, NE-BC Karl A. Sporer, MDKnox H. Todd, MD, MPHRhonda R. Whitson, RHIADaniel P. Hays, PharmD
Leonard J. Paulozzi, MD, MPHNational Center for Injury Prevention and Control, CDC
Chet Pogostin, DMV, MPHNational Center for Injury Prevention and Control, CDC
Bob A. Rappaport, MDCenter for Drug Evaluation and Research, FDA
Jacqueline Spaulding, MDCenter for Drug Evaluation and Research, FDA
Writing Panel Technical Panel
American College of Emergency Physicians Opioid Guideline Writing Panel
2. Expert review
3. PICO format
Development of Recommendations
1. Literature reviewpatient
intervention
comparison
outcome
PICO
What does PICO stand for?
http://www.acep.org/clinicalpolicies/
Strength of Clinical Findings
Level A High degree
Level C Other strategiesLevel C
Level B Moderate degree
Disclaimer:
This policy is not intended to be a complete manual on the evaluation and management of adult ED patients with painful conditions where prescriptions for opioids are being considered, but rather a focused examination of critical issues that have particular relevance to the current practice of emergency medicine.
It is the goal of the ACEP Opioid Guideline Panel to provide an evidence-based recommendation when the medical literature provides enough quality information to answer a critical question. When the medical literature does not contain enough quality information to answer a critical question, the members of the ACEP Opioid Guideline Panel believe that it is equally important to alert emergency physicians to this fact.
Recommendations offered in this policy are not intended to represent the only management options that the emergency physician should consider. ACEP clearly recognizes the importance of the individual physician’s judgment. Rather, this guideline defines for the physician those strategies for which medical literature exists to provide support for answers to the critical questions addressed in this policy.
Limited
Evidence based
Judgment
1. Compare prescription drug monitoring programs.
2. Describe an ideal prescription monitoring program.
3. Register for the prescription monitoring program (PAT) in Texas.
4. Obtain opioid risk screening tools.
5. Recognize the need for quality research.
OBJECTIVES
“A mature person is one who does not think only in absolutes,who is able to be objective even when deeply stirred emotionally,who has learned that there is both good and bad in all people and in all things,and who walks humbly and deals charitably with the circumstances of life, knowing that in this world no one is all knowing and therefore all of us need both love and charity.” -Eleanor Roosevelt, It seems to Me: Selected Letterswww.goodreads.com
1st Critical Question
In the adult ED patient with non cancer pain for whom opioid prescriptions are considered, what is the utility of state prescription drug monitoring programs in identifying patients who are at high risk for opioid abuse?
Level A: None specified.
Level B: None specified.
Recommendations:
Level C: The use of a state prescription monitoring program may help identify patients who are at high risk for prescription opioid diversion or doctor shopping.
critical question #1
PDMPS may help identify high risk patients
Is this statement True or False?“Only Physicians can access data from the prescription monitoring program.”
TRUE FALSE
“Most states allow health care providers and pharmacists to access the programs for patients under their care. Other groups such as law enforcement and regulatory boards may also have access. One program tracks only schedule II drug prescriptions, whereas most track drug prescriptions of schedule II to IV or II to V drugs.”
http://www.acep.org/clinicalpolicies/
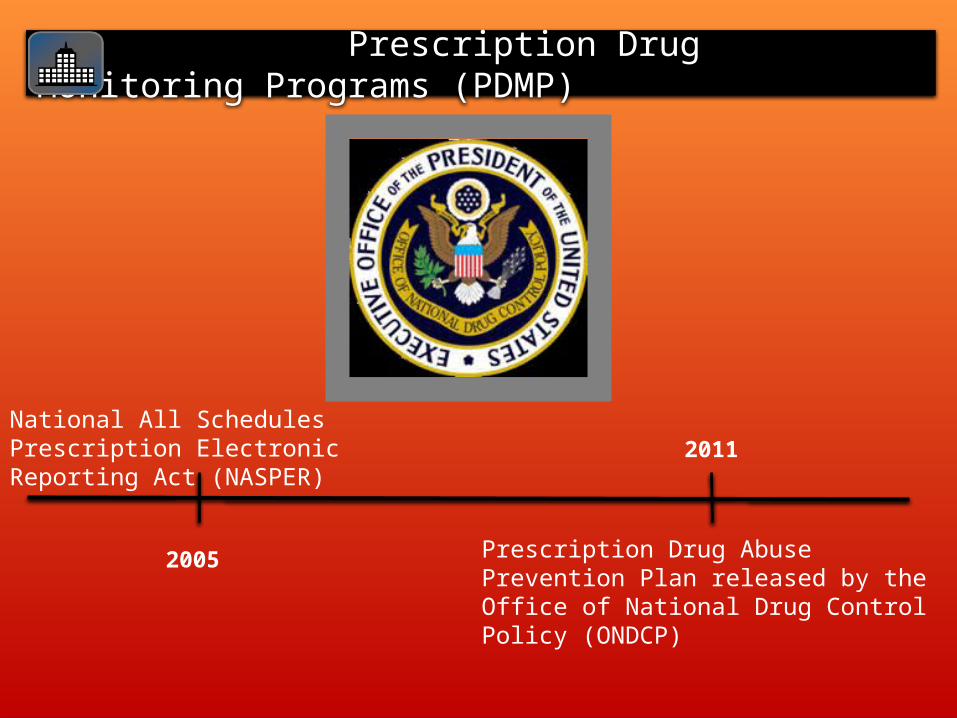
Prescription Drug Monitoring Programs (PDMP)
2011
2005
National All Schedules Prescription Electronic Reporting Act (NASPER)
Prescription Drug Abuse Prevention Plan released by the Office of National Drug Control Policy (ONDCP)
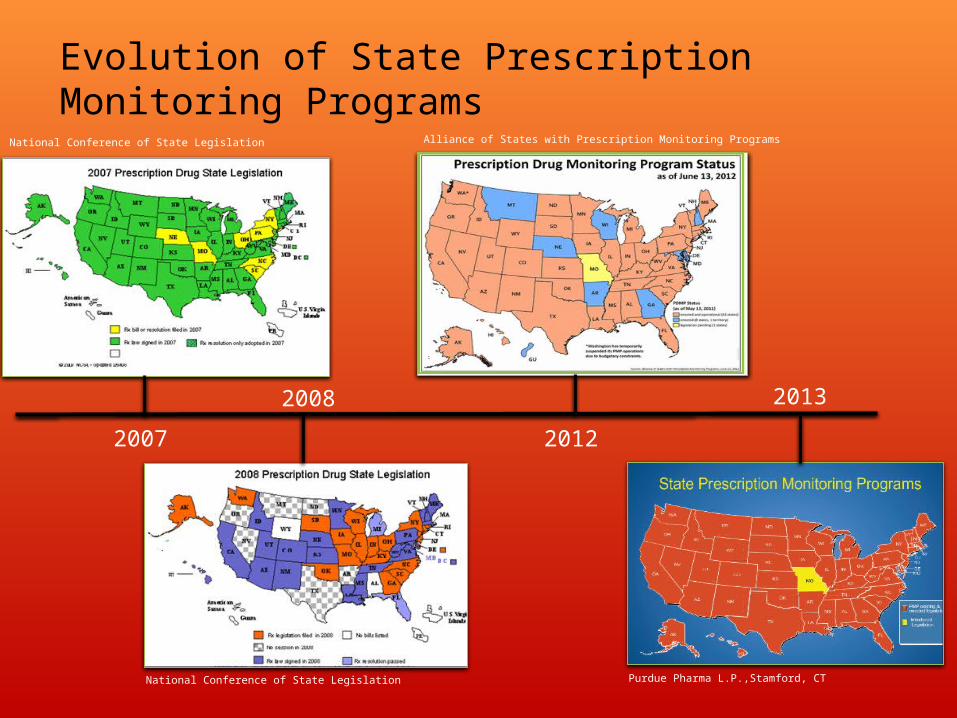
Evolution of State Prescription Monitoring Programs
Purdue Pharma L.P.,Stamford, CT
2007
2008
2012
2013
National Conference of State Legislation
National Conference of State Legislation
Alliance of States with Prescription Monitoring Programs
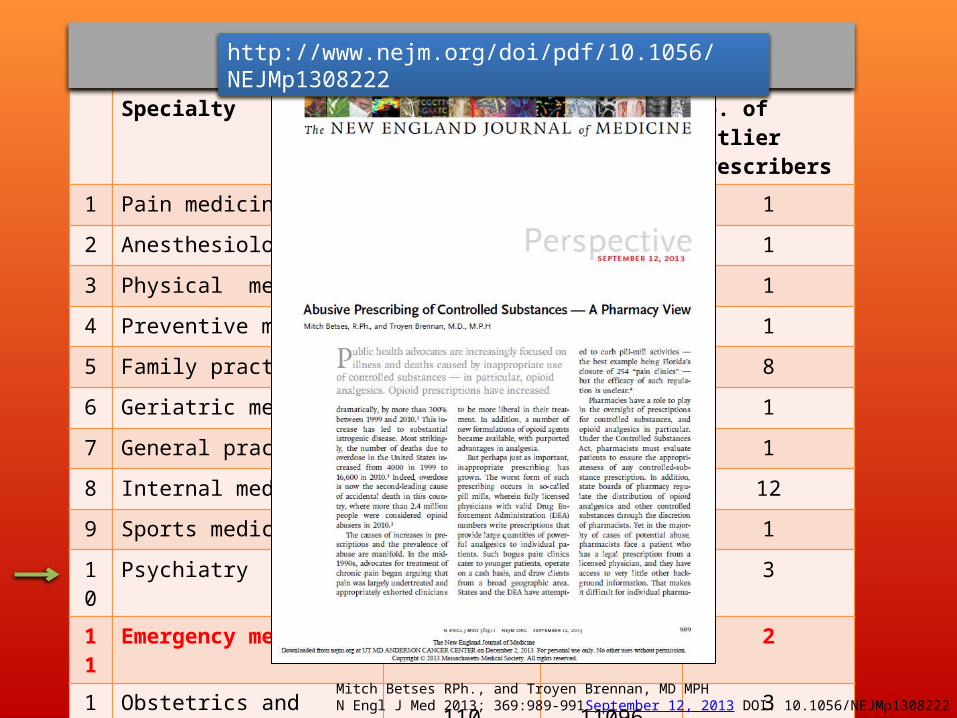
Specialty Nonoutlier Prescribers
Outlier Prescribers
No. of Outlier Prescribers
1 Pain medicine 3813 8811 1
2 Anesthesiology 1749 8128 1
3 Physical medicine 916 5599 1
4 Preventive medicine 662 44,397 1
5 Family practice 575 12903 8
6 Geriatric medicine 493 15544 1
7 General practice 462 24502 1
8 Internal medicine 422 11314 12
9 Sports medicine 387 7025 1
10 Psychiatry 213 18757 3
11 Emergency medicine 203 7935 2
12 Obstetrics and gynecology 110 11096 3
13 Pediatrics 31 5524 2
Average Monthly Doses of High-Risk Drugs Prescribed
Mitch Betses RPh., and Troyen Brennan, MD MPHN Engl J Med 2013; 369:989-991September 12, 2013 DOI: 10.1056/NEJMp1308222
http://www.nejm.org/doi/pdf/10.1056/NEJMp1308222
Help identify patients who engage in doctor shopping.
May identify providers or pharmacists who engage in diversion of controlled substances.
Provide information about prescribing trends for surveillance and evaluation purposes.
Functions of PDMPs
Data interpretation
Improved legislation
Interstate communication
Access issues
Improvements Needed
What does an ideal prescription monitoring program look like?
Are you registered for the PAT?
Prescription Access in Texas (PAT)
texaspatx.com/TXNewRegistration.aspx
PAT Registration Process
To register for the PAT you will need:
• Drivers license number• Social security number• DEA number• Practitioner board license number • DPS number

Texas DPS Homepage
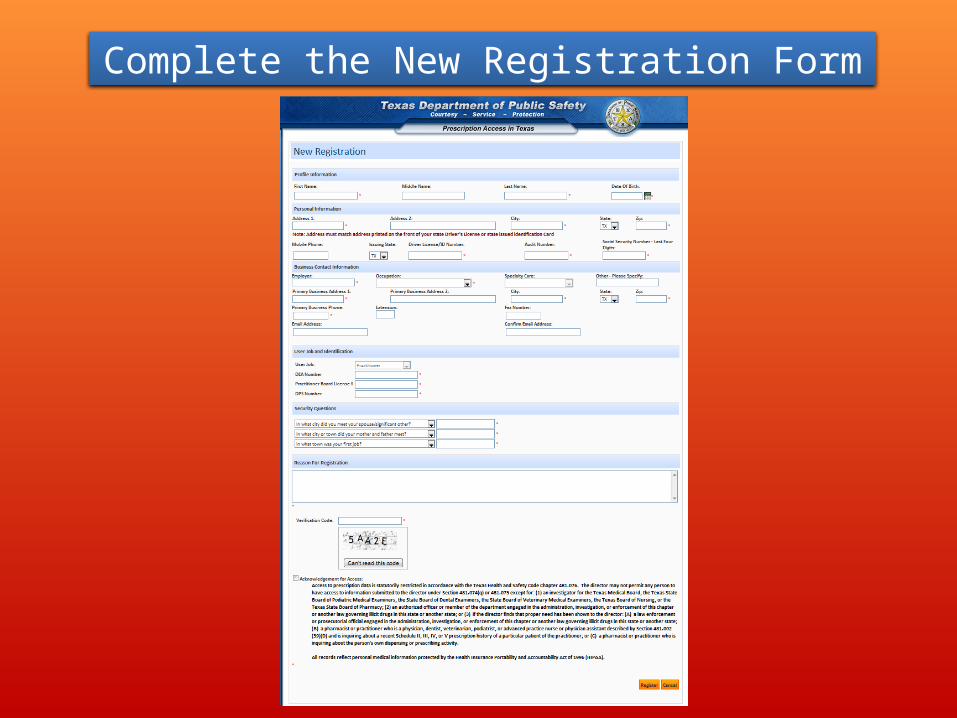
Complete the New Registration Form
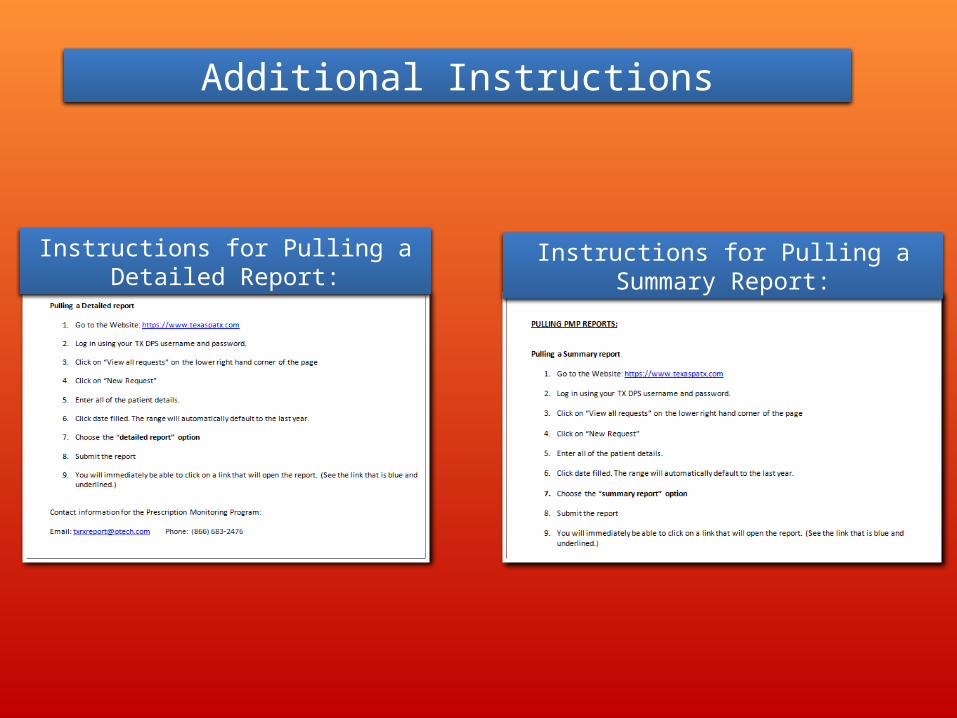
Instructions for Pulling a Detailed Report:
Additional Instructions
Instructions for Pulling a Summary Report:
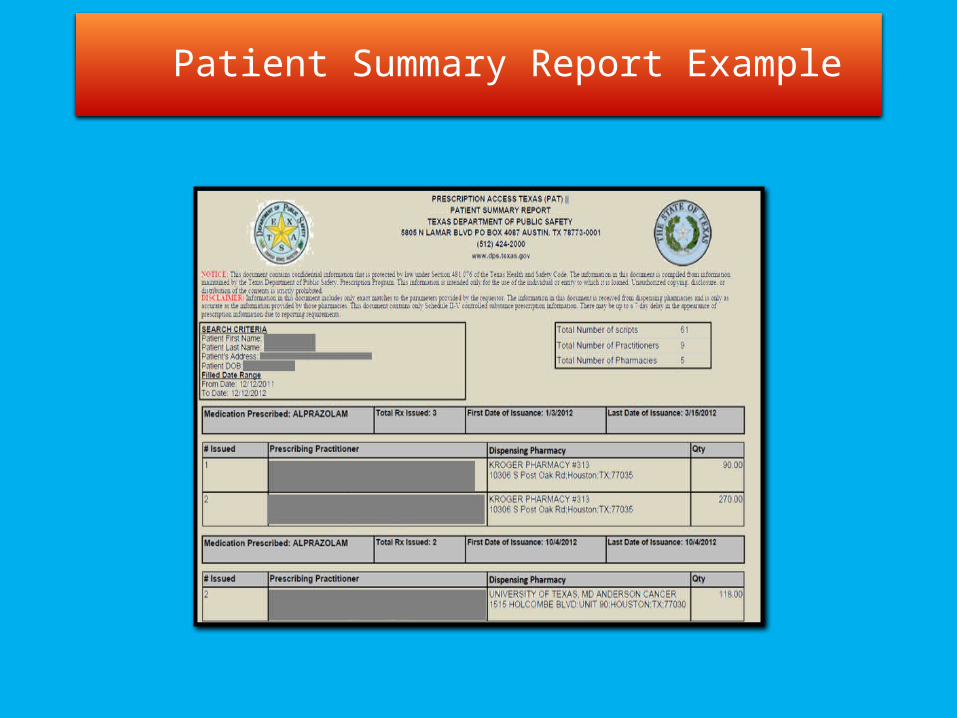
Patient Summary Report Example

4TH Critical Question
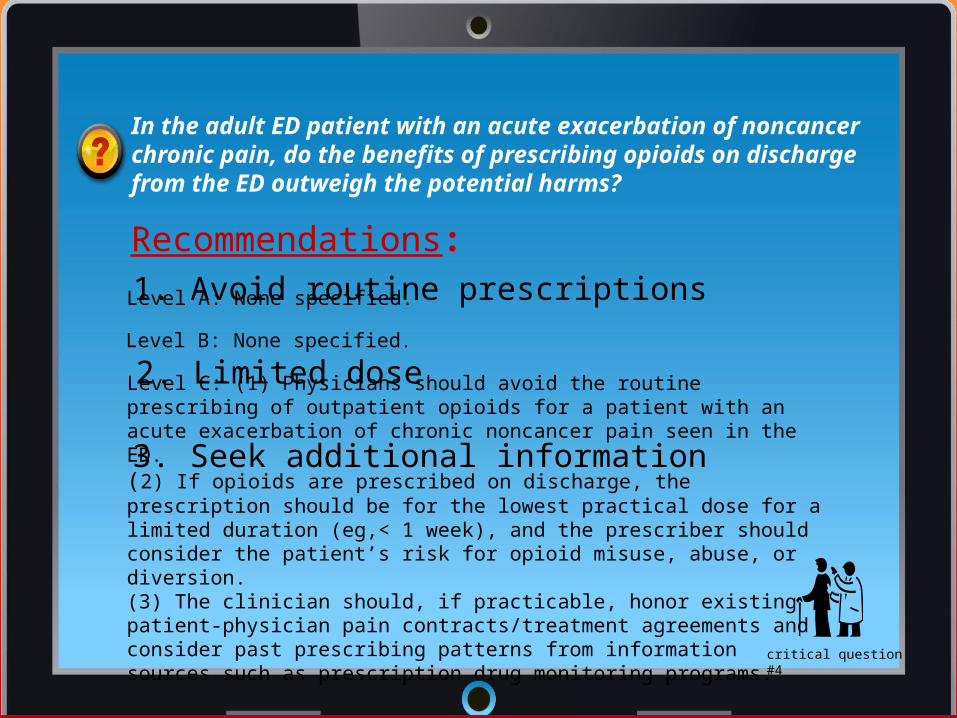
Recommendations:
Level C: (1) Physicians should avoid the routine prescribing of outpatient opioids for a patient with an acute exacerbation of chronic noncancer pain seen in the ED.(2) If opioids are prescribed on discharge, the prescription should be for the lowest practical dose for a limited duration (eg,< 1 week), and the prescriber should consider the patient’s risk for opioid misuse, abuse, or diversion.(3) The clinician should, if practicable, honor existing patient-physician pain contracts/treatment agreements and consider past prescribing patterns from information sources such as prescription drug monitoring programs.
In the adult ED patient with an acute exacerbation of noncancer chronic pain, do the benefits of prescribing opioids on discharge from the ED outweigh the potential harms?
Level A: None specified.
Level B: None specified.
critical question #4
1. Avoid routine prescriptions
2. Limited dose
3. Seek additional information
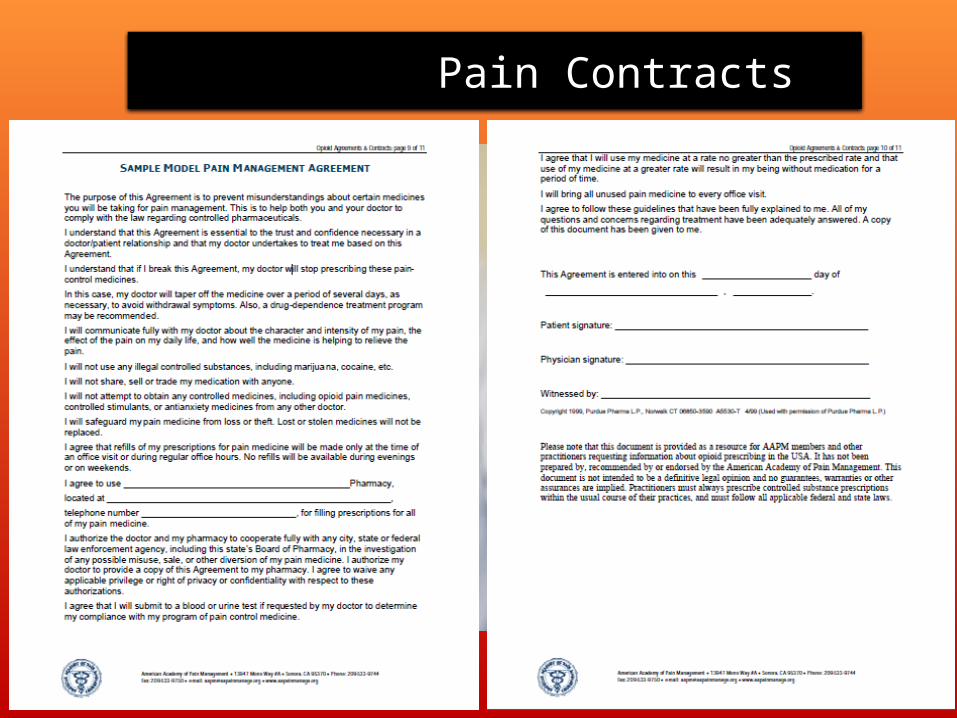
Pain Contracts

Best Use of Opioids
Reduce variability
• ORT: Opioid Risk Tool• SOAPP-R: Screener and Opioid Risk Assessment Tool• DIRE: Diagnosis Intractability Risk and Efficacy score• BPI: Brief Pain Inventory• Patient Pain Contracts• Prescription Pain Medication Safe Storage and Disposal
What is in your toolbox?

3rd Critical Question
In the adult ED patient for whom opioid prescription is considered appropriate for treatment of new-onset acute pain, are short-acting schedule II opioids more effective than short-acting schedule III opioids?
Level C: Research evidence to support superior pain relief for short-acting schedule II over schedule III opioids is inadequate.
Level B: For the short-term relief of acute musculoskeletal pain, emergency physicians may prescribe short-acting opioids such as oxycodone or hydrocodone products while considering the benefits and risks for the individual patient.
Level A: None specified.
critical question #3
1.Two studies
Recommendations:
2. No differences found

Schedule II Opioids:1. oxycodone combination products 2. hydromorphone (eg, Dilaudid 3. oxycodone (eg, Roxicodone) and oxycodone combination products 4. morphine (eg, MS Contin),
oxymorphone (eg, Opana),morphine (eg, MS Contin), oxycodone (eg, Roxicodone) oxycodone combination products (eg, Percocet, Percodan), and fentanyl (eg, Duragesic patch, Actiq).
Schedule III Opioids:1. hydrocodone combination products2. codeine combination products
Controlled Substance Scheduling
What are the schedule II and schedule III opioids?
Calls to Reclassify Hydrocodone
http://www.fda.gov/drugs/drugsafety/ucm372089.htm

2nd Critical Question
In the adult ED patient with acute low back pain, are prescriptions for opioids more effective during the acute phase than other medications?
Level A: None specified.
Level B: None specified.
Level C: (1) For the patient being discharged from the ED with acute low back pain, the emergency physician should ascertain whether nonopioid analgesics and nonpharmacologic therapies will be adequate for initial pain management.
(2) Given a lack of demonstrated evidence of superior efficacy of either opioid or nonopioid analgesics and the individual and community risks associated with opioid use, misuse, and abuse, opioids should be reserved for more severe pain or pain refractory to other analgesics rather than routinely prescribed.
(3) If opioids are indicated, the prescription should be for the lowest practical dose for a limited duration (eg, <1 week), and the prescriber should consider the patient’s risk for opioid misuse, abuse, or diversion.
Recommendations:
critical question #2
1. Consider nonpharmacologic and nonopioid therapies
2. Avoid routine opioid prescribing
3. Lowest dose and duration
Low Back Pain in the Emergency Department
19% reported opioid use at 3 month follow up
Reoccurrence Rate of Low Back Pain
50-80%Symptoms
Opioids
Low Back Pain
Abuse
Reference:42. United States Government Accountability Office Instances of Questionable Access to Prescription Drugs. GAO-11-699.Washington, DC: Government Accountability Office;2011.
Questionable Access to Prescription Drugs
• Federal Guidelines on Proper Disposal of Prescriptions: www.fda.gov/forconsumers/consumerupdates
• Office of National Drug Control Policy: www.whitehouse.gov/nidamed
• NIDA: The National Institute on Drug Abuse: www.drigabuse.gov • SAMHSA: The Substance Abuse and Mental Health Services Administration
www.samhsa.gov
• DAWN: Drug Abuse Warning Network: www.dawn.gov
Additional Resources
Baehren DF, Marco CA, Droz DE, et al. A statewide prescription monitoring program affects emergency department prescribing behaviors.Ann Emerg Med. 2010;56:19-23.
Cantrill SV, et alClinical Policy-Critical Issues in the Prescribing of Opioids for Adult Patients in the Emergency DepartmentAnn Emerg Med. 2012;60:499-525.
Devulder J, Jacobs A, Richarz U, et al. Impact of opioid rescue medication for breakthrough pain on the efficacy and tolerability of long-acting opioids in patients with chronic non-malignant pain.Br J Anaesth. 2009;103:576-585.
Friedman BW, Chilstrom M, Bijur PE, et al. Diagnostic testing and treatment of low back pain in US emergency departments. A national perspective. Spine. 2010;35:E1406-E1411.
Hall AJ, Logan JE, Toblin RL, et al. Patterns of abuse among unintentional pharmaceutical overdose fatalities. JAMA. 2008;300:2613-2620.
Holmes CP, Gatchel RJ, Adams LL, et al. An opioid screening instrument: long-term evaluation of the utility of the Pain Medication Questionnaire. Pain Pract. 2006;6:74-88.
Marco CA, Plewa MC, Buderer N, et al. Comparison of oxycodone and hydrocodone for the treatment of acute pain associated with fractures: a double-blind, randomized, controlled trial. Acad Emerg Med. 2005;12:282-288.
McIntosh G, Hall H.Low back pain (acute). Clin Evid (Online).2011;05:1102.
References
Palangio M, Morris E, Doyle RT Jr., et al. Combination hydrocodone and ibuprofen versus combination oxycodone and acetaminophen in the treatment of moderate or severe acute low back pain. Clin Ther. 2002;24:87-99
Passik SD, Kirsh KL, Casper D. Addiction-related assessment tools and pain management: instruments for screening, treatmentplanning, and monitoring compliance. Pain Med. 2008;9(suppl2):S145-S166
Pradel V, Frauger E, Thirion X, et al. Impact of a prescriptionmonitoring program on doctor-shopping for high dose buprenorphine. Pharmacoepidemiol Drug Saf. 2009;18:36-43.
Rockett IRH, Putnam SL, Jia H, et al. Assessing substance abuse treatment need: a statewide hospital emergency department study. Ann Emerg Med. 2003;41:802-813.
Roelofs PDDM, Deyo RA, Koes BW, et al. Non-steroidal anti-inflammatory drugs for low back pain. Cochrane Database SystRev. 2008;(1):CD000396. doi:10.1002/14651858.CD000396.pub3.
Simpson DM, Messina J, Xie F, et al. Fentanyl buccal tablet for the relief of breakthrough pain in opioid-tolerant adult patients withchronic neuropathic pain: a multicenter, randomized, double-blind,placebo-controlled study. Clin Ther. 2007;29:588-601.
Tamayo-Sarver JH, Dawson NV, Cydulka RK, et al. Variability in emergency physician decision making about prescribing opioid analgesics. Ann Emerg Med. 2004;43:483-493.
References
Email us:
Knox H. Todd, MD, MPHProfessor and ChairDepartment of Emergency Medicine MD [email protected]
Danielle S. CampbellProgram CoordinatorDepartment of Emergency MedicineMD [email protected]
Zeena ShelalResearch InterviewerDepartment of Emergency MedicineMD [email protected]
Questions