
Sonographic Changes of the Gallbladder Wall in Cholecystitis · 2016-12-27 · - Jae Hoon Lim, et...
8
3 pp. 384 - 391 , 1986 Journal of Kore an Radiological Society , Vo 1. 22 , No.3, 1986 Sonographic Changes of the Gallbladder Wall in Cholecystitis - A Sonographic-Pathological Correlation - Jae Hoon lim, M.D., Young Tae Ko , M.D. , and 500n Yong Kim, M.D.* 01 Radiology, K yung Hee Universi/)’ Hosþita/ * Presen/ Adres s: 01 Ha n Yang Ull iversi/y Hosþila/ - - 17 1) 2) 3) 3 To asse ss the pathologica l basis of the son ographic changes of the gal lbladder wall in cholecystitis , the sonographic appearances of the gallbladder wall we re analysed in 17 patients with acute cholec ys titis and 27 patients with chronic cholecystitis , and correlated with the pathological specirnens rernoved at su rgery In aCllte cholecystitis, a thin sonol ucent layer within the ec hogenic gal lbladder wall co rr esponds to subse rosa l edell1 a, hell1 0rrhage an d inflall1 rna to ry cell in filtrati on; in chronic cholecystitis it corresponds to rnu scu lar hypertrophy. Indistinctness and/ or a low echogenicity rind along the inner ll1argin refl ec ts rnucosal sloughing ob literation of the ll1 ucosal folds. Unifor ll1 ly decreased echogenicity of the wall is ca used by severe infla ll1 - ll1 atory cell in filtration with sloughing of the ll1 ucosa or oblit eration of the ll1 ucosal folds. Th ese so nograp hic signs are cO l1 sid ered 1' 0 be va lllable Sigl1 5 of cholecystitis Recei vecl A pri l 19, 1986; acceptecl M ay 17, 1986 384 -
Transcript of Sonographic Changes of the Gallbladder Wall in Cholecystitis · 2016-12-27 · - Jae Hoon Lim, et...
-
太 ~;~IjJ(~‘t~↓협쩡짤표‘ 찌'í 22 양 第 3 ~Æ pp. 384 - 391, 1986 Journal of Korean Radiological Society, Vo1.22, No.3, 1986
〈 국문초록〉
Sonographic Changes of the Gallbladder Wall
in Cholecystitis
- A Sonographic-Pathological Correlation -
Jae Hoon lim, M.D., Young Tae Ko, M.D., and 500n Yong Kim, M.D.*
Depar/Jηen/ 01 Diagηosl1‘c Radiology, Kyung Hee Universi/)’ Hosþita/ * Presen/ Adress: Deþartmeη t 01 R,αdiology, Ha n Yang Ull iversi/y Hosþila/
H홈킹훌싹에 있어서 擔훌훌의 超音波 所見
- 超音波所見과 病理組織所見의 .It較 -
g얄熙大쌓!校 짧科大學 放射線科웰敎室
林在勳·高永泰·金짧鋼
a홉않t~時 뼈察되는 超흡波所見의 病理學的 根題을 究明하기 위하여 수울로 切除한 急性體짧~ 17
例와 ↑성性廳짧~ 27 例의 廳짧慶을 組織學的으로 觀察하고 이를 超룹波所見파 各各 比較하여 마음
과 같은 結폐을 얻었마.
1) 超흡波所見上 廳製훨 自體內의 低에코혐 은 急性觸짧~인 경우는 類陳下層의 F¥種, 出血 또는
~j[쩌flH댐용뼈等에 의하고 ↑상性願짧췄인 경우는 觸肉혐의 nEJl길에 의한마.
2) 不解明한 內測 廳짧훨 혹운 內떼의 低에코輪은 챔廳의 l뾰짧이나 *퍼願주릉의 消失에 의한다.
3) 觸製훨에코의 全般的인 減少는 以上의 두가지, 즉 짧l않下혐의 ~j[性 짧化와 *김願脫落 또는
*6 1l1윗주릉消失에 의한다.
著者들은 이 3 가지 超륨波檢효所見 즉, 1!1쩔웰t용훌 自體內의 低에코햄, 不解明한 內에 廳製용훌 또는
低에코輪, 그러고 m쩔짧툴풍에코의 全般的 減少等은 擔製찢 該斷에 매우 有用한 所見임을 彈調한마.
To assess the pathologica l basis of the sonograph ic changes of the gal lbladder wall in cho lecystiti s, the
sonographic appearances of the gall bladder wall were analysed in 17 patients with acute cholecys titi s and
27 patients with chronic cholecystitis, and co rrelated wi th the pathological specirnens rernoved at su rgery
In aCllte cho lecystitis, a thin sonol ucent layer within the echogenic gal lbladder wall corresponds to subserosal
edell1a, hell10rrhage and inflall1 rna to ry ce ll infiltration; in chronic cho lecystitis it corresponds to rnuscular
hypertrophy. Ind istinctness and/or a low echogenicity rind along the inner ll1argin reflec ts rnucosal sloughing
。 r ob literation of the ll1 ucosal folds. Unifor ll1 ly decreased echogenicity of the wall is caused by severe infla ll1 -
ll1 atory cell infiltration w ith sloughing of the ll1 ucosa or obliteration of the ll1 ucosa l folds . These sonographic
signs are cO l1sidered 1'0 be va lllabl e Sigl1 5 of cholecystit is
Receivecl A pri l 19, 1986; acceptecl M ay 17, 1986
384 -
-
- Jae Hoon Lim , et al.: Sonographic Changes of the Gallbladder Wall in Cholecystitis -
Introduction Materials and Methods
The role of ultrasound in the diagnosis of ga llstone The st udy populalion COnSiSled of 17 patients with
is well estab !ished but its role in the diagnosis 0 1' acute cholecyst itis and 27 patients with chronic
cholecystitis remains cont ro vers ia l. U ltrason ic cholecystitis who were referred for abdo minal
demonstration of ga ll stones is a supporti ve sig n of sonography before su rgery. At the time of sonography
cholecystitis in the appropriate clinical sett ings , 1 ) but each patient had appropr iate clinical evidence of in-
its mere ex istence does not necessarily indicate inflam- flammation o f the ga llbladder and there was no in-
mation of the gallb ladde r. Ga llbladder wall th icken- dication of other diseases which might cause
ing has been described as a s ign of cho lecys titis ,2-7 sonographic changes of the gallbladder wal l. The pa-
but it is a lso seen in disease s other tha n tients who had acute c holecyst itis superimposed on
cholecystiti s.Ó - 1" ) c hron c c h o lecystitis we re classified as acute
There have been several papers concerned with the c hol ecyst iti s , as acute inflammatory changes
sonograp hic changes 0 1' the ga llbl adder wa ll in pa- predominated in the pathological findin gs and clinical
tients wit h cholecystitis , (for example , so nolu ce ncy signs and symptoms were those of acute cholecystitis.
surrounding the gallbladder waI1. 3 1
-
- The Journal of the Korean Radiological Society, Vo l. 22 , No. 3, 1986
of the gaIlbladder waIl echoes. The sonographer tried
to maintain the incident beam perpendicular to the Results
gallbladder waIl and longitudinal views were usuaIly
obtained in left lateral decubitus position. The seg- Sixteen of the 17 patients with acute cholecystitis
ment of the gaIlbladder waIl in contact with the liver and 14 of the 27 patients with chronic cholecystitis
was chosen for sonographic analysis. showed one or two sonographic abnormalities (Table
Sonograms were analysed for the presence of the 1).
fo Ilowing: The sonographic-pathological correlation may be
1. a sonolucent layer within the hyperechoic summerized as fo Ilows:
gaIlbladder waIl which divided it into two layers (Fig. 1. The sonolucent layer was proven to represent
l-A) , edema, hemorrhage and inflmmatory ceIl infiltration 2. indistinctness and/ or a low echogenicity rind in the subserosal (perimuscular) layer in acute
a long the inner aspect of the wa Il (Fig. 2-A) , and cholecystitis (Fig. l-A ,B) and moderate to severe 3. alteration of the overaIl wa Il echogenicity with muscular hypertrophy in chronic cholecystitis
reference to the hepatic echogenicity (Fig. 3-A). (Fig .4-A ,B).In 14 cases of acute cholecystitis superim-On histological examination , the fo Ilowing were posed on chronic cholecystitis both of these
recorded: pathological findings were observed in the same
1. integrity of the mucosa , gallbladder. 2. presence of subserosal edema , hemorrhage and 2. GaIlbladders showing an indistinctness and/ or
inflammatory ceIl infiltration , and low echogenicity rind along the inner aspect of the 3. muscular hypertrophy. gaIlbladder on sonography had sloughed mucosa and
A direct correlation between the sonographic and obliteration or loss of the mucoosal folds (Fig.2-A ,B). pathological findings of the gaIlbladder was then at- Gallbladders showing both a sonolucent layer with
tempted. indistinctness and/ or a low echogenicity rind show-
A . 향쩔얀짧향협聊f"~웠 깅I흩흩~ ,톨톨l1li tf.. -- B
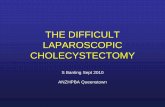
Fig. 2. A 67-year-old man with acute cholecystitis superimposed on chronic cholecystit is A. Transverse ultrasonogram of the gallbladder wall (between arrows) shows a low echogenicity rind alo l1g
the il1ner sid e of the outer hyperechoic layer. NOl1shadowing echogenic foci occupy the clepenclant part of the gallbladder lumen . Note indistinct inner margin. G Gallblaclcler lumen
B. Low-power micrograph of the gallblaclcler wall (HE stain , 5X magnification) cliscloses slollghi ng of the ITI lICOSa , cell infiltration , ancl necrosis (between arrows). Debris , tiny stones ancl epithelial cells fill the 11ll11en Fibrosis of subserosal layer (between open arrows) corresponcl to hyperechoic ollter layer ancl cell infilt ra-tion and necrosis corresponcl to low echogenicity ri ncl of inner layer 011 50no15ra l11 . MlIcosa l sloll15hi ng ex-plains inclist inctness of inner surface of the gallbladcler on sono15ra l11
- 386-
-
Jae Hoon Lim , et a1.: Sonographic Changes of the Gallbladder Wall in Cholecystitis-
ed both the subserosal and mucosal changes describ- to our parameters on sonography showed minimal
ed above (Fig.5-A,B) . inflammatory changes , fibromuscular thickening or 3. Gallbladders showing uniformly decreased wall fat cell infiltration.
echoes had a severe inflammatory cell infiltration in
the entire wall as well as sloughing of the mucosa Discussion
or obliteration of the mucosal folds (Fig .3-A ,B) . 4 . Gallbladders showing no abnormality according The pathological change of the gallbladder wall
Table 1. Summary of Sonographic Findings
No. of Patients Sonographic Parameters
Acute Cholecystitis Chronic Cholecystitis
Sonolucent layer within hyper-
echoic wall
Indistinctness and/or low
echogenicity rind
Sonolucent layer and indistinct-
ness and/or low echogenicity rind
Uniformaly decreased wall
echogenicity
No abnormality
Total
A
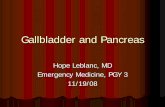
Fig. 3. A 74.year-old woman with chronic cholecystit is .
7 6
5 3
3 4
13
17 27
A. lJ ltrasonogrilm shows uniformly decreased gallbladder wall echo. Echo from the gallbladder wall is the same as that of the liver, and thus the gallbladder \Vall is not separable from adjacent liver
ß. L。이 power micrograph of the gallbladder wall (HE sta in , 5X magnification) shows diffuse inflammatory ce ll infiltration as well as dense fibrosis in the subserosallayer ancl muscular hypertrophy. Arrows point patch y areas of mucosal fol c\ obliteration. Diffuse inflam l11i1 tory cell infiltration , fib rosis ancl ll1uscular hypenrophy ex plain uniform clecrease of the gallblacl c1 er \\'all echo . an c1 piltchy ll1 ucosal folcl obliteration explains the lack of sharp echogenic inner margin 0 1' the gallblacl c1 er wall on sonogram. Note cholesterolosis :vlU :\1ucosal surface . SE Serosal surface
387 -
B
-
- The Journal of the Korean Radiological Society, Vo l. 22 , No. 3, 1986 -
MU
Fig. 4. A 65-year-old man with chronic cholecystit is A. U ltrasonogram for the gallbladder wa ll (between a rrows) shows a hypoechoic layer between two sharply
defined hyperechoic laye rs . A large shadowing stone seen B. Low-power micrograph of the gallb ladclel ψall (HE stain , 5X Illagnification). There is severe subserosal
edema with minimal infla lll ll1atory cell infil tration and sOllle fibrosis . Note in tact Illucosa ancl Illuscular hypertrophy. [nner echogenic layer on sonogram corresponcls to in tact Illucosa and outer echogenic laye r corresponcls to fibrosi s of the subserosal laye r. Subserosal eclerna ancl Ill uscular hyper trophy between them a re responsible for the hypoechoic layer between two hyperechoic wall echoes . SE Serosal Sllr-face. M U Mucosal sur face
MU
Fig. 5_ A 53-year-old man with aCllte cholecyst itis s lIperilllposecl on chronic cholecyst itis A. Ult rasonogram shows two hypoechoic la yers in the t hickenecl gallb lac\c\ er \Vall (between alTO\\’ S). ln ne l
Illargin is no 1' sharply c1 efinec\ ancl less echogenic B. Low-power l11 icrograph of I'he gallblaclclel 、\'all (HE stain , 5X Illagnification) discloses sc\'ere lhickenin니
0 1' the \Vall up to 11 111111. Localizecl abscess (AB) ancl inflanllnatorv ccll infillral ion are re、]lOllsihk for Ihe hypoechoic layers ancl fibrosis (F) of the 、\'all is responsible fo r the hyperechoic layers. i\ il:cosal sloll미 ll J1g (arrows) e:ψlains the indistinct inner Illargin on sonogra111. MU ;Vlllcosal surface
- 388 -
B
B
-
- Jae Hoon Lim , et a1. : Sonographic Changes of the Gallhlaclclel 씨! all in Cholecyst itis -
in acute cholecystitis is thickening 01‘ th e ga llbl adder cho lecyst it iSl7 15 . ' 시 a nd peric holecys ti c a bscess 2 2 ) has
wa ll which is caused b y spread ing of t he t iss ue been documented . Marc ha l et a l. described a sono lu-
elem ents and filling of the these spaces by edem a cent a rea within the wa ll as being a speciric sign fo r
fluid , blood and in rIammatory cells. 20 ) These in rI am- aCllt e cho lecystiti s a nd a ttribllt ed it to sllbserosal
m atory changes a re most severe in the sllbserosa llayer ede ma. 17 ) Raghave nd ra et a l. desc ribed ga llbl add er
as it is no rma lly composed o f loose co nnecti ve wa ll a nec ho icit y in 17 0 1' 24 pa ti ents with aCllte
ti ssue. 21 ) The mucosa may be either shed o r mi ssing cho lecyst itis a nd considered it represen ted inflam-
in som e areas a nd prese rved in o thers. In ch ro nic mato ry cha nges s lIch as ede m a , blood a nd celllllar
cholecystiti s, the muscular layer Illay be greatly hyper- inriltra tio n occurring predo minently in the slI bserosa l
trophied with increased co nnecti ve ti ss lle between th e (pcri m ll scllla r) loose connecti ve ti ss ll e spaces .' ")
muscJe bundles in the lamina propria a nd sllbserosa l J oseph desc ribed the “ dOllble wa ll sig n ' ’ in acute layer. The epithelium is lIs lla lly in tact bll t the m llcosa l cho lecys titi s a nd co n firmed that it was produced by
fo lds may be o blitera ted 0 1' absent in ad vanced stages. edern a occ llrring in th e subserosa l laye r. He a lso
At int ervals, rnllcosa l o llt po llchin gs penetra te th e o bserved th e sign in chronic ch o lecys titis and
thick ened mu scllla r coat to va rying depths towa rd s postulated it was dlle to p oor echoes a rJ Slllg from
the externa l layer (Rok it a nsky-Asc ho ff sin llses). A II a thick , fibro lls layer la id dow n uniform a nd display-
th e co nnecti ve ti ss ue is infilt rated with IYll1 phocytes , ing relat ive aco ustic hOlll ogeni city with few int er-pl as ll1 a cell s , large mo no nllclea r ce ll s a nd cos inp hili c ph ases. ' 9)
g ra nlll ocytes . In chron ic c h o l cιys titi s with s lI pc ri ll1 - In thi s series , the a llth o rs o bse rvecl thi s so no lu-
posed aC lI te cho lecyst itis , th ese infla ll1l11 atory cha nges cent layer in t he ga ll b lacl derwa ll in 12 0 1' th e 17 cases
0 1' aCllte a nd ch ronic cho lecyst it is occ ur a t the sa ll1 e (7 10/0) or aC lI te cho lecys ti t is a nd 9 01‘ the 27 cases
t ime ancl grossly , sllch a ga ll b laclde r d iffe rs little 1‘ rom ( 33ψ'0 ) 0 1' chro ni c cho lecyst iti s. These layers we re
o ne with aC ll te cho lecyst iti s excep t for th e prcse ncc a nec ho ic 0 1' hypoec hoic , co ntinll o ll s 0 1' in te rrll pted 0 1' ca lc llli . 2띠 11‘ th ese pat
- 389-
-
- The Journal of the Korean Radiological Society, Vo l. 22 , No. 3, 1986 -
is contradiction with the observation of Joseph.1 9) are more or less subjective and one-to-one comparison
However , several diseases that produce thicken- between the observed sonographic findings and ing of the gallbladder wall may also cause a sonolu- histologic findings is very difficult. Authors were
cent layer. 14 .19) We have seen this sonolucent layer aware of this fact and tried to lessen this effect at
in pa tients with ascites , hypoalbuminemia , cirrhosis the time of sonography and review of pathology of the liver and hepatitis . Although there has been specimens.
no pathological confirmation , the mechanism of this In summary , it is concluded that 1) a thin sonolu-layer in these patients may be similar to that in cent layer within the echogenic gallbladder wall repre-
cholecystitis , i.e. , subserosal edema. sents subserosal edema , hemorrhage and inflam-
Indistinct ness of the inner margin of the gallblad- matory cell infiltration or muscu1ar hypertrophy,>)
der wall has been regarded as sign of acute indistinctness and/ or a low echogenicity rind along
cholecystitis by several authors. 17 ) Schneider et a l. the inner aspect reflect sloughing of the mucosa or
described a halo of low level echoes between the echo- obliteration of the mucosal folds and3 ) uniformly
free gallbladder lumen and the confluent high level decreased wall echogenicity represents severe inflam
echoes that surround it and called it the “ halo sign". 7) matory cell infiltration of the entire wall with
This halo of low level echoes correspo nds exactly to sIoughing of the mucosa or obliteration of the
the low echogenicity rind in our series. However, there mucosal folds. Some diseases other than cholecystitis
has been no pathological confirmation of these may results in a sonolucent layer within the ga llblad
so nographic signs. der wall and thus it is not. specific for cholecystitis
In our se rie s , indi st in ctn ess and / or lo w but indist inctness and / or a low echogenicity rind of
echogenicity rind along th e inner aspect of the the inner aspect and uniformly decreased wall
gallbladder wall was observed ll1 6 of 17 cases (35 % ) echogenicity ma y be co nsidered specific fOI
of acute cholecystitis and 4 of 27 cases (15 070) of cholecystitis.
chronic cholecystitis. Pathology specimens showed a
partially or tota lly sloughed mucosa 0 1' obliteration Acknowledgement
of the mucosal fold s (Fi g .2-a ,b and Fig.5-a ,b). Con sidering the distinct hi
ed in 7 patients is considered to represent diffuse
severe inflammatory cell infiltration of the entire 、vall 1. Cinto ra 1, Ben.Ora A, MacNe il R, Gils cl orf RB
as well as sloughing of mucosa or obliteration o f the Cholecystosonography for the deísíon to operate when
mucosal folds (Fig.3-A ,B). Hypertrophied muscle is acute cholecystítís ís suspected. A/ll 1 SurglY79. believed to be responsible for the decreased wall echo ηδ δ 18.820
on sonogram. 2. Hanclle r 51: Ullrasound of gallbladder wall thíckeníng and
The authors admit that sonographic observations íts rclalíon 10 cholecystítís . Alk 7') 7
-
Jae Hoon Lim. et al.: Sonograph ic Changes of the Gallbladder Wall in Cholecystitis -
3. Mindel Hj, Ring A: Callbladder wall thickening: u/trasonic
findings. Radiology 1979; 133:699-701
4. Finberg Hj, Bi rnho lz JC: Ultrasound evaluation of the gallbladder wall. Radiology 1979; 133:693-698
S. Engel jM , Deitch EA, Sikkerna W: Callbladder wall
thickness: 50nographic accuracy and relation to disease
AjR 1 98α 134:907-909
6. 5anders RC: The s igniηcance of sonographic gallbladder
wall thickening. j CU 198α 8:743-146
7. 5chneider M , Rubenstein 、VA, Auh YH, Kazam E
Ultrasonography and computed tomography in the evalua-
tion of biliary tract disease. In: Thorbjarnarson 8 ed. Surgery
of the biliary tract. Philadelphia, Londoπ Toronto, ιlex
ico city, Rio de janeiro, 5ydneκ Tokyo : ,ν B. 5aunders
Company. 1982; 79-60
8. Fiske CE, Laing FC, Brow n TW: Ultrasonographic evidence
of a gallbladdel νV.δ 11 rhickening in association wirh
hypoalbuminemia. Radiology 1980; 13.5:713-716
9. 5hlaer W j, Leopold CR, 5cheible FW: 50nography of the
thickened gallbladder νV긴 11: a nonspecific finding. AjR
7981;136:337-33 9
10. Yum HY, Fink AH: 5ol1 ographic findings in primary car-
cinoma of the gallbladder‘ Radiology 1980; 134:693-696
11. Ralls I'W , Quinn tv\F , juttner H-U, Halls jM , Boswell WD
Callbladder νvall thickening: Patients without intrinsic
gallbladder disease. AjR 1981; 137:6.5-68
12. juttner H-U, Ra lls I'W, Q uinn MF, jenny jM: Thickening
of the gallbladder wall in acute hepatitis: ultrasound
demonstration. Radiology 1982; 1-+2:-+65-466
-13. I'at ri gui HB, Dipietro M , Barber FE, Tce le RL: 50nogr따Jhy
of thickened gallbladder wall: Causes in children. AjR 1983,
141:.57-60.
14. Maudgal D, Wansbrough-jones MH, joseph AEA Callblad
der abnormalities of acute infectious hepatitis. A prospec-
tive study. Oig Ois 5ci 1984; 29:257-260.
15. Creenberg M , Kangarloo H, Cochran 5t, 5amp le WF: The
Ultrasonographic diagno sis of cho lecysti tis and
cholelithiasis in children. Radiology 1980; 137 ’ 745-749
16. Kane RA: Ultrasonographic diagnosis of gangrenous
cholecystitis and empyema of the gallbladder. Radiology
1980; 134: 191-194
17. Marchal GjF, Casaer ι1, Baert AL, Goddeeris I'G, Kerremans
R, Fevery j : Callbladder wall sonolucency in acute
cholecystitis . Radiology 1979;133.429-433
18. Raghavendra BN, Feiner HD, 5ubramanyam BR, Ranson
jHC, T oder 51', Horii 5C, Madamba MR: Acute cholecystitis:
sonographic-pathologic anaylysis. AjR 1981; 137:327-332
19. joseph AEA: The gallbladder. In: joseph AEA, Consgrove
00 eds. Ultrasound in inflammatory disease. New York,
Edinburgh, London, ι1elbourne: Churchill Livingstone,
1983, 761-183
20. Halpert B: Callbladder and biliary ducts. In: Anderson
WAO, Kissane j,ι1 eds. Pathology. 5t Louis: Mosby. 1977;
1439-14.56
21 Thomas CG, Wonack NA: Acute cholecystitis, its
pathogenesis and repair. Arch 5urg 19.52; 64:590-600
22 . Bergman AB, Neiman, HL, Kraut ß: U/trasonographic
evalua l'ion of pericholecystic abscesses. AjR 1979;
132:201-203
- 391-






![Chronic Cholecystitis which Mimics Gallbladder Cancer: a ......malignant gallbladder disorders from benign ones [1-3]. We describe a case of chronic cholecystitis that showed focal](https://static.fdocuments.net/doc/165x107/5e9edb35d364e168286b9adc/chronic-cholecystitis-which-mimics-gallbladder-cancer-a-malignant-gallbladder.jpg)



![FSU 2017 MCQ-2.pptx [Read-Only] - Radiological Society of · PDF file · 2017-09-20estimated at up to 25% higher than with ... B. Acute cholecystitis with gallbladder stoneAcute cholecystitis](https://static.fdocuments.net/doc/165x107/5aa37d2c7f8b9a80378e4f52/fsu-2017-mcq-2pptx-read-only-radiological-society-of-2017-09-20estimated.jpg)




