
Gallbladder and Pancreas - USF Health | Education...
52
Gallbladder and Pancreas Gallbladder and Pancreas Hope Leblanc, MD Hope Leblanc, MD Emergency Medicine, PGY 3 Emergency Medicine, PGY 3 11/19/08 11/19/08
Transcript of Gallbladder and Pancreas - USF Health | Education...

Gallbladder and PancreasGallbladder and Pancreas
Hope Leblanc, MDHope Leblanc, MDEmergency Medicine, PGY 3Emergency Medicine, PGY 3
11/19/0811/19/08

ObjectivesObjectives
GallbladderGallbladderCholelithiasis/BiliaryCholelithiasis/Biliary coliccolicCholecystitisCholecystitisAcalculousAcalculous cholecystitischolecystitisCholangitisCholangitisComplications of Complications of cholecystitischolecystitisTumorsTumors
PancreasPancreasAcute versus Chronic PancreatitisAcute versus Chronic PancreatitisTumorsTumors

Risk Factors for GallstonesRisk Factors for Gallstones
““FortyForty””““FemaleFemale””““FertileFertile””““FatFat””MedicationsMedicationsPregnancyPregnancyEthnicityEthnicityProfound weight lossProfound weight lossProlonged fastingProlonged fasting
TPNTPNHigh spinal cord High spinal cord injuryinjuryChronic intravascular Chronic intravascular hemolysishemolysisLiver diseaseLiver diseaseCystic fibrosisCystic fibrosisHypertriglyceridemiaHypertriglyceridemiaChronic parasitic Chronic parasitic infectionsinfections

Anatomy 101Anatomy 101
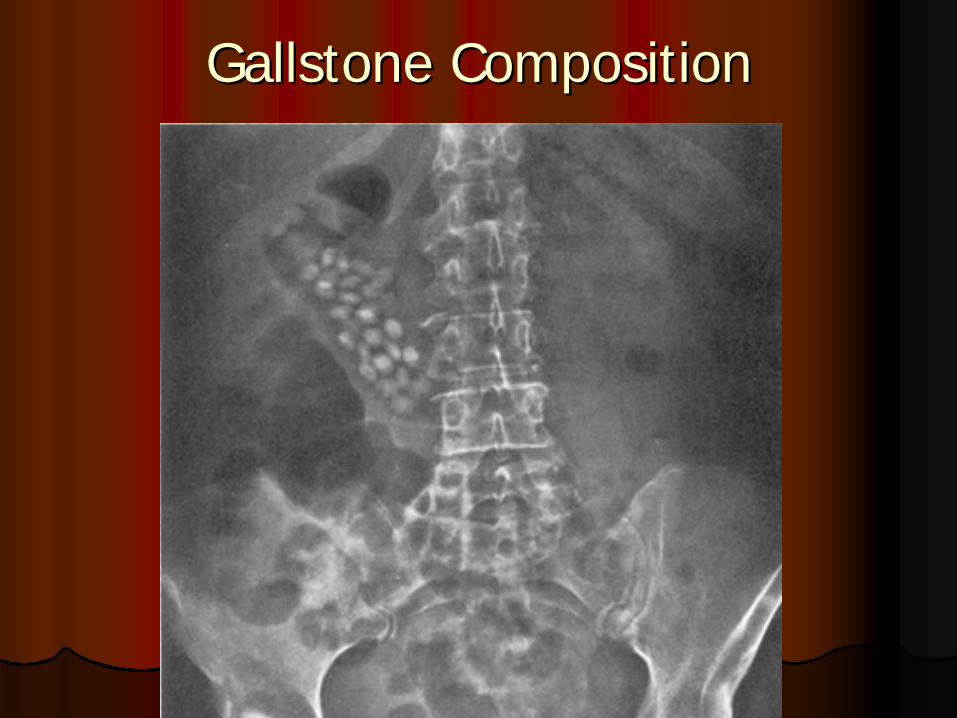
Gallstone CompositionGallstone Composition
Gallbladder DiseaseGallbladder Disease
Cholecystitis
Cholangitis
Biliary Colic
Empyema or Gangrenous Gallbladder
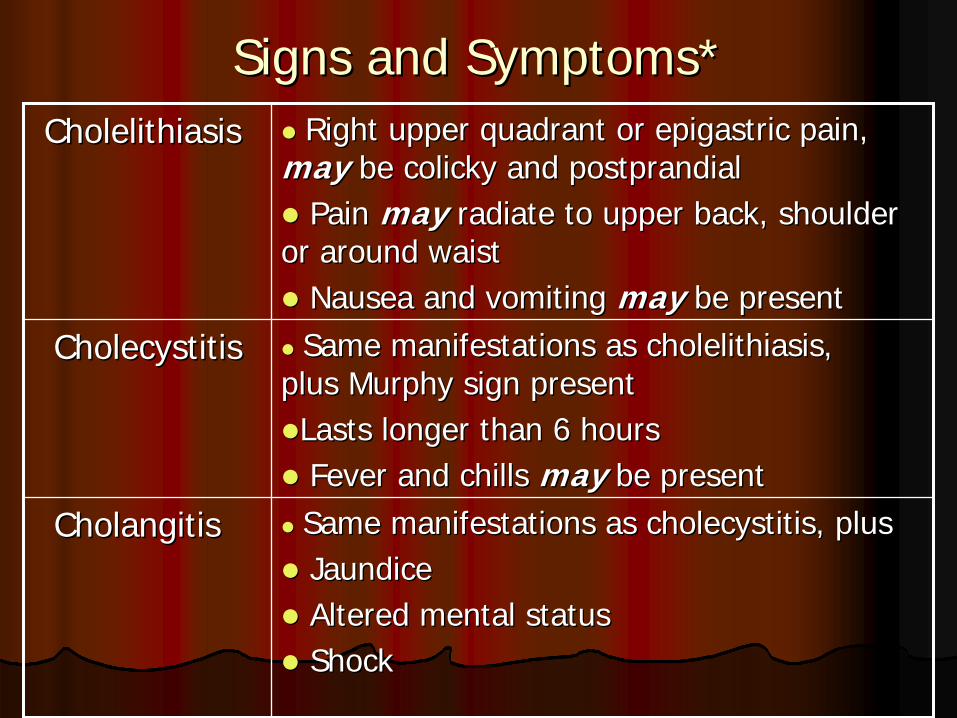
Signs and Symptoms*Signs and Symptoms*CholelithiasisCholelithiasis Right upper quadrant or Right upper quadrant or epigastricepigastric pain, pain,
maymay be colicky and postprandialbe colicky and postprandialPain Pain maymay radiate to upper back, shoulder radiate to upper back, shoulder
or around waistor around waistNausea and vomiting Nausea and vomiting maymay be presentbe present
CholecystitisCholecystitis Same manifestations as Same manifestations as cholelithiasischolelithiasis, , plusplus Murphy sign presentMurphy sign presentLasts longer than 6 hoursLasts longer than 6 hoursFever and chills Fever and chills may may be presentbe present
CholangitisCholangitis Same manifestations as Same manifestations as cholecystitischolecystitis, plus, plusJaundiceJaundiceAltered mental statusAltered mental statusShockShock

AcalculousAcalculous CholecystitisCholecystitis
10% of patients with 10% of patients with acute acute cholecystitischolecystitis
Indistinguishable with Indistinguishable with 2 exceptions:2 exceptions:
patients frequently are patients frequently are gravely ill gravely ill Is a complication from Is a complication from another processanother process
Risk factors:Risk factors:elderly elderly DMDMmultiple traumamultiple traumaextensive burn injuryextensive burn injuryprolonged laborprolonged labormajor surgerymajor surgerygallbladder torsiongallbladder torsionsystemic systemic vasculiticvasculiticinfections of infections of biliarybiliary tract tract
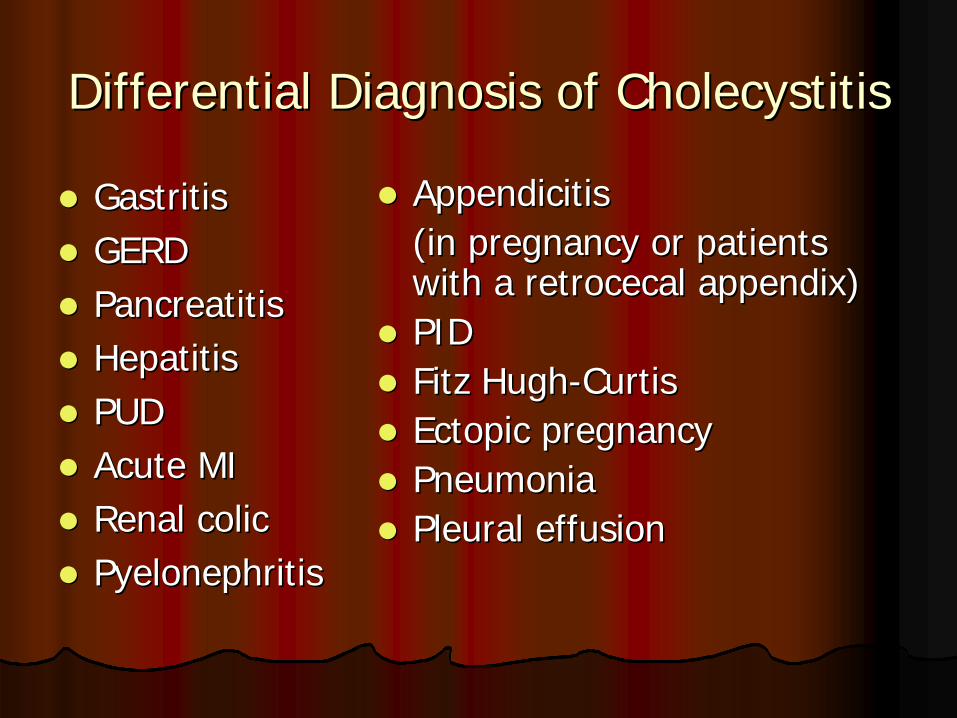
Differential Diagnosis of Differential Diagnosis of CholecystitisCholecystitis
GastritisGastritisGERDGERDPancreatitisPancreatitisHepatitisHepatitisPUDPUDAcute MIAcute MIRenal colic Renal colic PyelonephritisPyelonephritis
Appendicitis Appendicitis (in pregnancy or patients (in pregnancy or patients with a with a retrocecalretrocecal appendix) appendix) PIDPIDFitz HughFitz Hugh--Curtis Curtis Ectopic pregnancyEctopic pregnancyPneumoniaPneumoniaPleural effusionPleural effusion

DiagnosisDiagnosis
Poor predictive valuePoor predictive valueHistoryHistoryPhysicalPhysicalLabsLabs
UltrasoundUltrasoundSensitivity 94%Sensitivity 94%Specificity 78%Specificity 78%
HIDA scanHIDA scanSensitivity 97%Sensitivity 97%Specificity 90%Specificity 90%



TreatmentTreatmentBiliaryBiliary ColicColic Supportive careSupportive care
Possible ED dischargePossible ED dischargeElective surgeryElective surgery
CholecystitisCholecystitis Surgery within 1Surgery within 1--3 days3 daysSupportive careSupportive careSingleSingle--coverage antibioticscoverage antibiotics
CholangitisCholangitis and other and other complicated diseasecomplicated disease
Aggressive resuscitationAggressive resuscitationBroadBroad--spectrum antibiotics spectrum antibiotics Immediate surgeryImmediate surgery
Antibiotics in Complicated InfectionAntibiotics in Complicated Infection
Ampicillin, Ampicillin, gentamicingentamicin, and , and metronidazolemetronidazoleCiprofloxacinCiprofloxacin and and metronidazolemetronidazoleZosynZosynUnasynUnasynTicarcillinTicarcillin--clavulanateclavulanateImipenemImipenemThirdThird--generation cephalosporin and generation cephalosporin and metronidazolemetronidazole or or clindamycinclindamycinAztreonamAztreonam and and clindamycinclindamycin
ComplicationsComplications
Ascending Ascending CholangitisCholangitisGallstone PancreatitisGallstone PancreatitisGallstone Gallstone IleusIleusGallbladder EmpyemaGallbladder EmpyemaEmphysematous (Gangrenous) Emphysematous (Gangrenous) CholecystitisCholecystitisPorcelain GallbladderPorcelain Gallbladder
Gallstone Gallstone IleusIleus
Gallstone erodes into the bowelGallstone erodes into the bowelFistula forms between Fistula forms between biliarybiliary tract and intestinetract and intestineElderly and femalesElderly and femalesIntestinal obstruction if stone > 2 cmIntestinal obstruction if stone > 2 cmMechanical obstruction not an Mechanical obstruction not an ileusileusMay be intermittent: May be intermittent: ““tumbling phenomenontumbling phenomenon””

Gallstone Gallstone IleusIleus
NauseaNauseaVomitingVomitingPain Pain ConstipationConstipationHistory of History of biliarybiliary diseasediseaseRarely have Rarely have biliarybiliary symptoms directly symptoms directly before episodebefore episode

Gallstone Gallstone IleusIleus
RiglerRigler’’ss TriadTriadPartial or complete obstructionPartial or complete obstructionPneumobiliaPneumobiliaEctopic gallstone in intestineEctopic gallstone in intestine
CT scan up to 93% sensitive in diagnosing CT scan up to 93% sensitive in diagnosing gallstone gallstone ileusileusUrgent Urgent LaparotomyLaparotomy

Ascending Ascending CholangitisCholangitis
Complete Complete biliarybiliary obstruction + bacterial obstruction + bacterial infectioninfectionCharcot triad (25%)Charcot triad (25%)ReynoldReynold’’ss pentadpentadMortality approaches 100% if untreatedMortality approaches 100% if untreatedFluids, Fluids, VasopressorsVasopressors, IV antibiotics and , IV antibiotics and Surgical decompressionSurgical decompression

Gallbladder EmpyemaGallbladder Empyema
Complete cystic duct obstruction + Complete cystic duct obstruction + bacterial infection + abscess formationbacterial infection + abscess formationReynoldReynold’’ss pentadpentadRisk Factors: elderly, DM, trauma, burns, Risk Factors: elderly, DM, trauma, burns, vasculitisvasculitisFrequently develop gramFrequently develop gram--negative sepsisnegative sepsisFluids, Fluids, VasopressorsVasopressors, IV antibiotics and , IV antibiotics and Surgical decompressionSurgical decompression

Gangrenous Gangrenous CholecystitisCholecystitis
Focal or diffuse gangrene Focal or diffuse gangrene Gallbladder wall becomes ischemic, then develop Gallbladder wall becomes ischemic, then develop bacterial infection and gangrenebacterial infection and gangrene1% of 1% of cholecystitischolecystitis ptpt’’s, but 30% of these are s, but 30% of these are acalculousacalculousReynoldReynold’’ss pentadpentadKUB may demonstrate KUB may demonstrate pneumobiliapneumobiliaRecommend CT scanRecommend CT scanSimilar treatmentSimilar treatment

Porcelain GallbladderPorcelain Gallbladder
Incidence 0.6Incidence 0.6--0.8% 0.8% Pathological finding of a brittle gallbladder with Pathological finding of a brittle gallbladder with bluish discoloration resulting from extensive bluish discoloration resulting from extensive calcification of the gallbladder wallcalcification of the gallbladder wallRelevance is based on high association between Relevance is based on high association between gallbladder cancer and porcelain gallbladdergallbladder cancer and porcelain gallbladderDiagnosis:Diagnosis:
hard mass in the RUQ hard mass in the RUQ incidental findings on KUB, US, or CT incidental findings on KUB, US, or CT
Prophylactic Prophylactic cholecystectomycholecystectomy

TumorsTumors
CholangiocarcinomaCholangiocarcinomaPrimary Gallbladder Primary Gallbladder CancerCancer

CholangiocarcinomaCholangiocarcinoma
Neoplasm from intraNeoplasm from intra-- or or extrahepaticextrahepaticbile duct epitheliumbile duct epitheliumSecond most common primary hepatic Second most common primary hepatic tumortumorAverage age 50 yrsAverage age 50 yrsIncreasing incidence in USIncreasing incidence in US1 case per 100,000 per year1 case per 100,000 per yearRisk factor: primary Risk factor: primary sclerosingsclerosingcholangitischolangitis
CholangiocarcinomaCholangiocarcinoma
Most Most cholangiocarcinomascholangiocarcinomas remain clinically silent remain clinically silent until advanced stagesuntil advanced stages
ExtrahepaticExtrahepatic: : biliarybiliary obstruction results in painless obstruction results in painless jaundicejaundiceIntrahepaticIntrahepatic: RUQ pain and : RUQ pain and cachexiacachexia and malaiseand malaise
CT and MRI with MRCP help with diagnosis and CT and MRI with MRCP help with diagnosis and stagingstagingSurgical resection or liver transplantation and Surgical resection or liver transplantation and chemotherapychemotherapyOverall survival 6 months in 90% of ptOverall survival 6 months in 90% of pt’’ss

Primary Gallbladder CancerPrimary Gallbladder Cancer
Incidence 0.8% to 1.2%Incidence 0.8% to 1.2%Female: Male, 3:1Female: Male, 3:1Aged 62Aged 62--66yrs66yrsHighest in American Indians and Hispanic Highest in American Indians and Hispanic Most patients not diagnosed until advanced Most patients not diagnosed until advanced disease as no specific signs or symptomsdisease as no specific signs or symptomsRisk factor is chronic inflammationRisk factor is chronic inflammation
>75 % inflammation is cholesterol gallstones>75 % inflammation is cholesterol gallstones
Signs and SymptomsSigns and Symptoms
Similar symptoms of gallstones and Similar symptoms of gallstones and biliarybiliary coliccolicAbdominal pain may be of a more diffuse and Abdominal pain may be of a more diffuse and persistent naturepersistent natureCourvoisier sign: Palpable mass in the RUQCourvoisier sign: Palpable mass in the RUQSister Mary Joseph nodes: Sister Mary Joseph nodes: PeriumbilicalPeriumbilical LADLADVirchow node: Left Virchow node: Left supraclavicularsupraclavicular adenopathyadenopathyPelvic seeding: Mass is palpated on DREPelvic seeding: Mass is palpated on DRE

Diagnosis and TreatmentDiagnosis and Treatment
May see elevated alkaline May see elevated alkaline phosphatasephosphatase and and bilirubinbilirubin levelslevelsUS or CT scan completed due to RUQ painUS or CT scan completed due to RUQ pain1010--20% of patients present with tumor confined20% of patients present with tumor confinedComplete surgical resection in early diseaseComplete surgical resection in early diseaseGallbladder replaced by the cancerGallbladder replaced by the cancer50% of patients have lymph node 50% of patients have lymph node metsmetsAdvanced disease, palliative treatment onlyAdvanced disease, palliative treatment only55--year survival rates of 15year survival rates of 15--20%20%
PancreasPancreas
Acute PancreatitisAcute PancreatitisChronic PancreatitisChronic PancreatitisPancreatic CancerPancreatic Cancer
PathophysiologyPathophysiology of Acute Pancreatitisof Acute Pancreatitis
A stress/trigger starts the activation of A stress/trigger starts the activation of proenzymesproenzymes and digestive zymogensand digestive zymogensResults in Results in autodigestionautodigestion of the pancreasof the pancreasCauses edema, interstitial hemorrhage, Causes edema, interstitial hemorrhage, vascular damage, coagulation, and cellular vascular damage, coagulation, and cellular necrosisnecrosisMay get extension of the localized process May get extension of the localized process into a generalized systemic inflammatory into a generalized systemic inflammatory responseresponse

Acute PancreatitisAcute Pancreatitis
United StatesUnited States90% due to alcohol abuse or 90% due to alcohol abuse or cholelithiasischolelithiasis5% due to medications5% due to medicationsRemaining due to infection, inflammation, Remaining due to infection, inflammation, trauma, and metabolic disturbances trauma, and metabolic disturbances
Etiology different in other countriesEtiology different in other countriesPrevalence is 0.5%Prevalence is 0.5%
Medications Associated with PancreatitisMedications Associated with PancreatitisAntiarrhythmicsAntiarrhythmics:: AmiodaroneAmiodarone, , amlodipineamlodipineAntiasthmaticAntiasthmatic:: MontelukastMontelukastAntibiotics:Antibiotics: ErythromycinErythromycin, , azithromycinazithromycin, , clarithromycinclarithromycin, , sulfamethoxazolesulfamethoxazole, , quinolonesquinolones, , pentamidinepentamidine, , paromomycinparomomycin, , rifampinrifampin, , dalfopristindalfopristin--quinupristinquinupristinAntiepilepticsAntiepileptics: : CarbamazepineCarbamazepine, , valproicvalproic acidacid, , topiramatetopiramateAntifungals:Antifungals: MetronidazoleMetronidazoleAntihypertensivesAntihypertensives:: DiazoxideDiazoxide, , indapamideindapamide, , methyldopamethyldopaAntilipemicAntilipemic agents:agents: All typesAll typesAntineoplasticAntineoplastic agents:agents: LL--AsparaginaseAsparaginase, , pegaspargasepegaspargase, , cytarabinecytarabine, , tamoxifentamoxifen, , mycophenolatemycophenolate, , vinorelbinevinorelbine, , anagrelideanagrelide, interleukin2 , interleukin2 ((ILIL--22) analogues, ) analogues, interferonsinterferons
AntipsychoticsAntipsychotics: : RisperidoneRisperidoneAntiretroviralsAntiretrovirals: All types: All types
DiphenoxylateDiphenoxylate (opiate agonist) (opiate agonist) Diuretics:Diuretics: ThiazidesThiazides, , furosemidefurosemide, , ethacrynicethacrynic acidacid, , metolazonemetolazoneErgotaminesErgotaminesEstrogensEstrogens: All types: All typesEtanerceptEtanercept (anti(anti--TNF) TNF) EthanolEthanolGastrointestinal agentsGastrointestinal agents: : CholestyramineCholestyramine, , cimetidinecimetidine, , octreotideoctreotide, , ranitidineranitidine, proton pump inhibitors, proton pump inhibitorsGlucocorticoidsGlucocorticoids:: All typesAll typesHydroxyureaHydroxyureaNonsteroidalNonsteroidal antianti--inflammatory agents:inflammatory agents: All All typestypesRetinoic acidRetinoic acid derivativesderivativesSalicylatesSalicylatesSomatropinSomatropin ((growth hormonegrowth hormone))

Signs and SymptomsSigns and SymptomsMidepigastricMidepigastric or LUQ or LUQ pain pain Constant, boring pain Constant, boring pain Radiates to back, Radiates to back, flanks, chest, or lower flanks, chest, or lower abdomen abdomen Worse in supine Worse in supine position position Relieved by sitting, Relieved by sitting, knees flexed knees flexed Nausea and vomitingNausea and vomitingAbdominal bloatingAbdominal bloating
LowLow--grade fevers grade fevers Tachycardia Tachycardia Hypotension Hypotension Cullen sign Cullen sign Grey Turner signGrey Turner signHypovolemicHypovolemic shock shock Multisystem organ Multisystem organ failurefailure

Complications of Acute PancreatitisComplications of Acute Pancreatitis
PulmonaryPulmonaryL Pleural effusionsL Pleural effusionsAtelectasisAtelectasisHypoxemiaHypoxemiaARDS (>50% mortality)ARDS (>50% mortality)
MetabolicMetabolicHypocalcemiaHypocalcemiaHyperglycemiaHyperglycemiaHyperlipidemiaHyperlipidemiaCoagulopathyCoagulopathyDIC DIC
CardiovascularCardiovascularMyocardial depressionMyocardial depressionHemorrhageHemorrhageHypovolemiaHypovolemia
OtherOtherHemorrhageHemorrhageColonic perforationColonic perforationRenal failureRenal failureErythemaErythema--nodosumnodosumArthritisArthritisPseudocystPseudocystAbscessAbscess
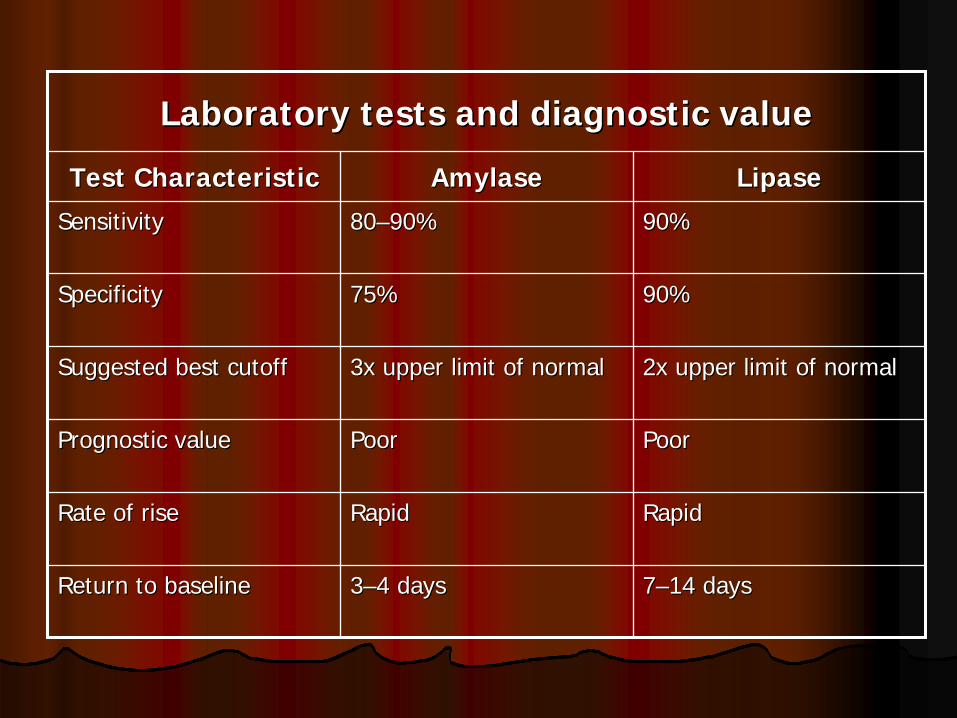
Laboratory tests and diagnostic valueLaboratory tests and diagnostic value
Test CharacteristicTest Characteristic AmylaseAmylase LipaseLipase
SensitivitySensitivity 8080––90%90% 90%90%
SpecificitySpecificity 75%75% 90%90%
Suggested best cutoffSuggested best cutoff 3x upper limit of normal3x upper limit of normal 2x upper limit of normal2x upper limit of normal
Prognostic valuePrognostic value PoorPoor PoorPoor
Rate of riseRate of rise RapidRapid RapidRapid
Return to baselineReturn to baseline 33––4 days4 days 77––14 days14 days
DiagnosisDiagnosis
ALT: 3 X upper limit of normalALT: 3 X upper limit of normalPositive predictive value 95% for gallstone etiologyPositive predictive value 95% for gallstone etiology
FilmFilmRules out other diseaseRules out other disease
UltrasoundUltrasoundImportant in ruling out gallstones as etiologyImportant in ruling out gallstones as etiologyMay visualize pancreatic edema or May visualize pancreatic edema or pseudocystspseudocysts
CT scanCT scanInsensitive in early or mild diseaseInsensitive in early or mild diseasePhlegmonsPhlegmons, abscesses, or , abscesses, or pseudocystspseudocysts

Prognostic Markers?Prognostic Markers?
RansonRanson’’ss CriteriaCriteriaAPACHE IIAPACHE IILevel of amylase or lipaseLevel of amylase or lipase

RansonRanson’’ss CriteriaCriteria
At admission:At admission:Age > 55 years Age > 55 years WBC > 16000WBC > 16000Glucose > 200Glucose > 200serum serum ASTAST > 250> 250serum serum LDHLDH > 350> 350
After 48 hours:After 48 hours:Calcium < 8.0 Calcium < 8.0 HHCT drop > 10% CT drop > 10% Oxygen PO2 < 60 Oxygen PO2 < 60 BUNBUN increased by 5increased by 5Base deficit > 4Base deficit > 4Fluid Sequestration > Fluid Sequestration > 6 L6 L

Treatment Mild to Moderate Treatment Mild to Moderate PancreatitisPancreatitis
90%90%"rest the pancreas" "rest the pancreas" IV fluid resuscitationIV fluid resuscitationClear liquidsClear liquidsUOP = 100 ml/hrUOP = 100 ml/hrIV narcotics and IV narcotics and antiemeticsantiemeticsBiliaryBiliary etiology: elective etiology: elective vsvs urgent surgeryurgent surgery


Treatment of Severe PancreatitisTreatment of Severe Pancreatitis
1010--20% develop necrosis or systemic 20% develop necrosis or systemic complicationscomplicationsSupportive careSupportive careNPONPOIV antibioticsIV antibiotics
PolymicrobialPolymicrobialImipenemImipenem (or FQ) + (or FQ) + metronidazolemetronidazole
VasopressorsVasopressorsConsider surgical interventionConsider surgical intervention
DispositionDisposition
Level of disease, PO tolerance, follow upLevel of disease, PO tolerance, follow up
HomeHomeMedical floorMedical floorICUICUConsider Surgical consultConsider Surgical consult
Chronic PancreatitisChronic Pancreatitis
Prevalence from 0.04 to 5 %Prevalence from 0.04 to 5 %Irreversible damage to pancreatic Irreversible damage to pancreatic structure and functionstructure and function
Interstitial inflammation with duct obstruction Interstitial inflammation with duct obstruction and dilatation leads to and dilatation leads to parenchymalparenchymal loss and loss and fibrosisfibrosisResults in impairment of both exocrine and Results in impairment of both exocrine and endocrine pancreatic functionsendocrine pancreatic functionsEndocrine impairment occurs much laterEndocrine impairment occurs much later

Etiology of Chronic PancreatitisEtiology of Chronic Pancreatitis
Alcohol abuseAlcohol abuseIdiopathicIdiopathicMalnutrition Malnutrition HyperparathyroidismHyperparathyroidismPancreas Pancreas divisumdivisumAmpullaryAmpullary stenosisstenosisCystic fibrosisCystic fibrosisHereditaryHereditaryTraumaTrauma

Signs and SymptomsSigns and Symptoms
Similar to acute pancreatitisSimilar to acute pancreatitisProgresses from discrete attacks to no Progresses from discrete attacks to no pain free periodspain free periodsAppear chronically illAppear chronically ill
Weight lossWeight lossSteatorrheaSteatorrheaClubbingClubbingPolyuriaPolyuriaMay have stigmata of liver diseaseMay have stigmata of liver disease
DiagnosisDiagnosis
Amylase and Lipase may be elevated or Amylase and Lipase may be elevated or normalnormalUS or CTUS or CT
Consider when pain increasing and intractableConsider when pain increasing and intractableCheck for complications (abscess, Check for complications (abscess, pseudocystpseudocyst))Rule out pancreatic cancerRule out pancreatic cancer

Short and Long Term TreatmentShort and Long Term Treatment
Supportive careSupportive careTreat complicationsTreat complications
Relieve mechanical obstructionRelieve mechanical obstructionCorrect Correct malabsorptionmalabsorptionAlteration of the disease course Alteration of the disease course
Pancreatic extractsPancreatic extractsAlcohol abstinenceAlcohol abstinenceCeliac plexus nerve blockCeliac plexus nerve block

DispositionDisposition
HomeHomeRuled out complicationsRuled out complicationsClose followClose follow--upupPain under controlPain under control
AdmissionAdmissionComplicationsComplicationsPain reliefPain relief

Pancreatic CancerPancreatic Cancer
Incidence has increased over the last decadesIncidence has increased over the last decades1010thth most common cancer in the USmost common cancer in the USPoor overall 5Poor overall 5--year survival rate of 5%year survival rate of 5%Why prognosis so poorWhy prognosis so poor
lack of early symptomslack of early symptomsearly and frequent vessel wall involvementearly and frequent vessel wall involvementhigh incidence of liver metastaseshigh incidence of liver metastasesonly 7% are localized to the organ without only 7% are localized to the organ without spreading or distant spreading or distant metsmetspain, jaundice, weight loss, and obstruction are late pain, jaundice, weight loss, and obstruction are late symptomssymptoms
Pancreatic CancerPancreatic Cancer
Cancer screening in general population:Cancer screening in general population:Low incidenceLow incidenceLack of accurate, inexpensive, and Lack of accurate, inexpensive, and noninvasive diagnostic tests for early diseasenoninvasive diagnostic tests for early disease
Screening in highScreening in high--risk populations:risk populations:Strong family history pancreatic cancerStrong family history pancreatic cancerPancreatitisPancreatitisHereditary cancer syndromesHereditary cancer syndromes

SummarySummary
1.1. Stop DrinkingStop Drinking2.2. Learn how to do gallbladder ultrasounds.Learn how to do gallbladder ultrasounds.3.3. If youIf you’’re feeling fine, you may have re feeling fine, you may have
cancer!cancer!

ReferencesReferencesAttasaranyaAttasaranya S. S. CholedocholithiasisCholedocholithiasis, ascending , ascending cholangitischolangitis, and gallstone pancreatitis. , and gallstone pancreatitis. Medical Medical Clinics North AmClinics North Am Volume 92 Issue 4 (July 2008) 925Volume 92 Issue 4 (July 2008) 925--60. 60. BlechaczBlechacz, B. R., Gores, G. J. , B. R., Gores, G. J. CholangiocarcinomaCholangiocarcinoma. . Clinics in Liver DiseaseClinics in Liver Disease, Volume 12, Issue 1 , Volume 12, Issue 1 (February 2008) (February 2008) 131–150.Chen, E. L. LongLong--term survival after pancreatic cancer treatmentterm survival after pancreatic cancer treatmentAmerican Journal of Surgery Volume 194, Issue 4(October 2007) 12American Journal of Surgery Volume 194, Issue 4(October 2007) 1277--30.30.Elwood, D. R. Cholecystitis. Surg Clin N Am Volume 88 (2008) 1241-1252.Gordon, F. D. Primary sclerosing cholangitis. Surgical Clinics of North America, Volume 88, Issue 6 (December 2008).Gourgiotis, S. et al. Gallbladder cancer. American Journal of Surgery, VolS. et al. Gallbladder cancer. American Journal of Surgery, Volume 196, Issue 2 ume 196, Issue 2 (August 2008) (August 2008) 252–264.HelmstaedterHelmstaedter, L. Endoscopic ultrasound and early diagnosis of pancreatic can, L. Endoscopic ultrasound and early diagnosis of pancreatic cancer. American cer. American Journal of Surgery, Volume 194, Issue 4 (October 2007) 87Journal of Surgery, Volume 194, Issue 4 (October 2007) 87--90.90.Acute and Chronic Pancreatitis. Acute and Chronic Pancreatitis. In In TintinalliTintinalli J.E. J.E. TintinalliTintinalli’’ss Emergency Medicine., 6Emergency Medicine., 6thth edition. The edition. The McgrawMcgraw--Hill Companies, Inc. 2004: Chapter 87.Hill Companies, Inc. 2004: Chapter 87.CholecystitisCholecystitis and and BiliaryBiliary Colic: Introduction. Colic: Introduction. In In TintinalliTintinalli J.E. J.E. TintinalliTintinalli’’ss Emergency Medicine., 6Emergency Medicine., 6thth
edition. The edition. The McgrawMcgraw--Hill Companies, Inc. 2004: Chapter 85.Hill Companies, Inc. 2004: Chapter 85.Zaliekas, J. Complications of gallstones: The Mirizzi Syndrome, gallstone ileus, gallstone pancreatitis, complications of “lost” gallstones. Surg Clin N Am Volume 88 (2008) 1345-1368.EmedicineEmedicine. Porcelain Gallbladder. . Porcelain Gallbladder. Article Last Updated: Feb 12, 2008 Article Last Updated: Feb 12, 2008


















