Social Media - A Connected Way of Life: Lessons from using social media to advance personal and...
51
-
Upload
sarah-amani -
Category
Career
-
view
262 -
download
0
Transcript of Social Media - A Connected Way of Life: Lessons from using social media to advance personal and...


Lessons from using social media to advance personal and collective growth
A Connected Way of Life
15th January 2015
Sarah Amani
@S_Amani #SeacoleScholar
www.ehealthconsultant.org

1 Background
2 Discovery
3 The journey so far
4 Challenges and woes
Overview
5 Growth

What is Social Media?Social media refers to the means of
interactions among people in which they create, share, and exchange information
and ideas in virtual communities and networks.

Facebook = Friend Builder
Twitter = Community Builder
YouTube = Broadcast Content to the World
Flickr = Photographs to Inspire
LinkedIn = Professional Connections
Blogs = Your Own Online Newspaper
Tumblr = Sharing Information

“The impact of social media on the balance of power and knowledge between patient and professional is
enormously significant...”
Disruptive Technologies Report


Tracing my Roots,Malawi, 2010
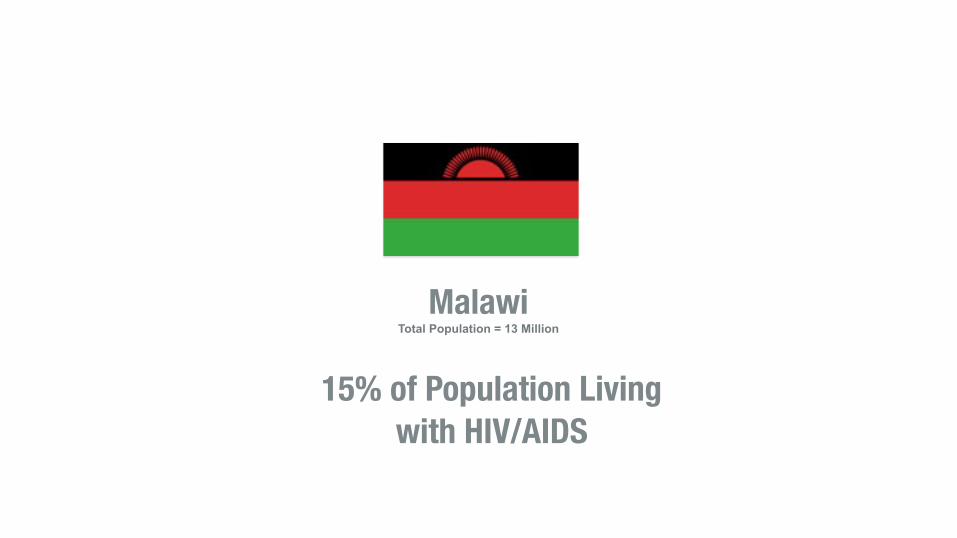
Malawi Total Population = 13 Million
15% of Population Living with HIV/AIDS


Moyo = Life

15% of Secondary School Age
Girls Attend School
30% of Secondary School
Age Boys Attend School
Nkhota-Kota, Malawi 13,000 Children aged 14-17
29 Secondary Schools 1:63 Teacher - Pupil Ratio

2008 2012 20132009 2010 2011
Started work at EIP + University of Surrey
Vision Unclear
Noted frequent Staff turnover
Poor pt satisfaction Poor staff morale Poor clinical outcomes
Manager left Staff posts cut Staff sickness rocketed
PIER Project awarded £10,000 (National Leadership Council)
Took up management of team Began developing a vision
Completed Transformational Leadership Programme
Reach Out Project awarded £12,500 Mary Seacole Award (DoH)
Youth Mental Health Network Project (YMHN) awarded £20, 000 for My Journey app (SHA)
Started Proactive Intervention to Enhance Recovery (PIER) project
YMHN awarded £35, 000 for YMH economic evaluation by LSE (NHS Confed)
After numerous rejected proposals My Journey App awarded £40,000 for evaluation (Burdett Trust)
2014
Moyo Project

Success is an Iceberg


1. Create a youth orientated & accessible online resource for first episode psychosis & mental health.
2. Raise awareness & reduce Duration of Untreated Psychosis & enhance Recovery.
3. Embed leadership, innovation & service user involvement in EIP.
Triple Aim

Released: 1998 CPU: 233 MHz RAM: 32 MB (512 MB max) Storage: 4 GB (+ optical drive) Display: 38.1 cm Millions of colours Dimensions: 40.1 x 38.6 x 44.7 cm Weight: 17.3 kgs
Released: 2007CPU: 412 MHzRAM: 128 MBStorage: 4 GB (8 GB max)Display: 8.9 cm Millions of coloursDimensions: 11.4 x 6.1 x 1.2 cmWeight: 135 g
This was ‘portable’...
<10 years...


23
Engaging young people with familiar tools
92% of 14-25 year olds own a smartphone
Sensors, devices, networks, software, sensors
and data
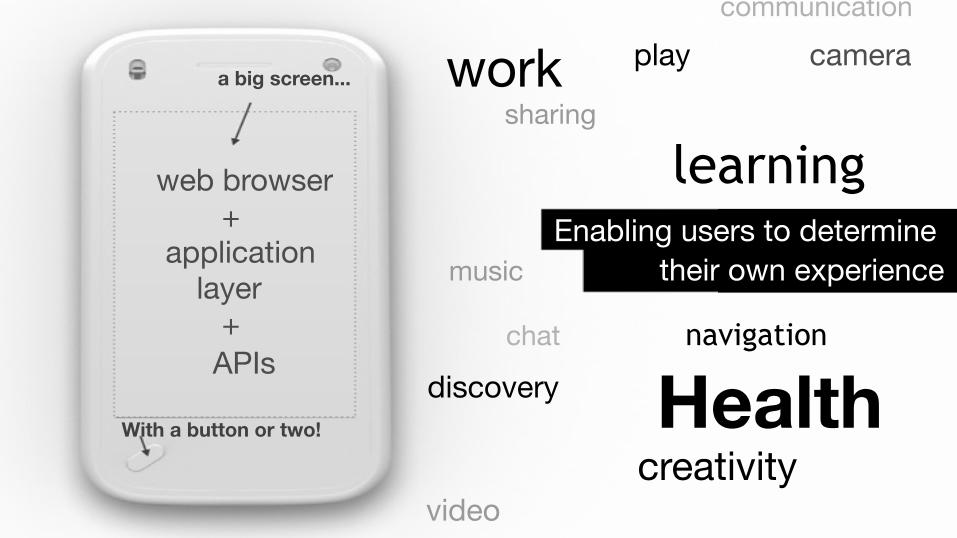
work
learning
navigation
discovery With a button or two!
creativity video
a big screen...
web browser + application layer + APIs
communication play camera
sharing
Enabling users to determine music their own experience
chat
Health




Community Health Ambassadors should be members of the communities where they live, work, study, play… should be selected by their communities, should be answerable to the communities for their activities, should be supported by the health system but not necessarily a part of its organization,
and have shorter training than professional workers.
World Health Organization (2007)
“
”
Community Health Ambassadors (CHAs)

The Wisdom of Crowds?

“A lie can travel halfway around the world while the truth is putting on its shoes.”
Mark Twain
Tracking Anti-Vaccination Sentiment in Europe Using Social Media. Unicef, April 2013
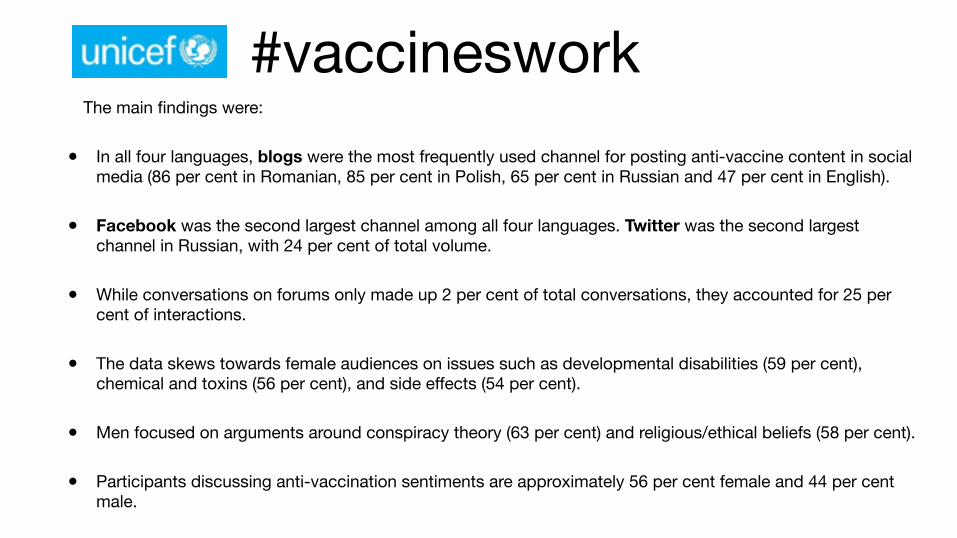
#vaccinesworkThe main findings were:
• In all four languages, blogs were the most frequently used channel for posting anti-vaccine content in social media (86 per cent in Romanian, 85 per cent in Polish, 65 per cent in Russian and 47 per cent in English).
• Facebook was the second largest channel among all four languages. Twitter was the second largest channel in Russian, with 24 per cent of total volume.
• While conversations on forums only made up 2 per cent of total conversations, they accounted for 25 per cent of interactions.
• The data skews towards female audiences on issues such as developmental disabilities (59 per cent), chemical and toxins (56 per cent), and side effects (54 per cent).
• Men focused on arguments around conspiracy theory (63 per cent) and religious/ethical beliefs (58 per cent).
• Participants discussing anti-vaccination sentiments are approximately 56 per cent female and 44 per cent male.

Implications
• Majority do vaccinate & immunize themselves & their children
• But many have concerns over safety
• They are seeking information online & via social media
• How reliable is this information?


BME NetworksUnited for Equality
Where are we now?• ‘Subtle’ incidents of intentional and non intentional disadvantaging of minorities - that can
not be proven
• Disproportionate repercussions with BME people being more likely to face hearings but many cases reversed by registering bodies e.g NMC, GMC etc
• Many of these events have ‘unspoken’ outcomes (Non Disclosure Agreements)
• Secrecy means contributory factors + facts are hidden and therefore lessons are not learnt*
*A basic definition of madness is: Doing the same and expecting different results….

Knowledge is Power• Do you know enough about the status quo?
• Where does race equality sit your organisation’s current priority list?
• Who are your sponsors and detractors?
• Who is being real and who is pretending?

Where are you going?




The digital revolution
Advances in technology and particularly mobile digital informationand communication technology continue at an exponential rate,making it possible to communicate, obtain information and accessand buy goods and services in new ways. In 2013, 36 millionadults in the UK (73%) accessed the internet every day and72% of all adults bought goods or services online.1 Access tothe internet using a mobile phone more than doubled between2010 and 2013 to 53%. In total, 51% of UK adults now own asmartphone (almost doubled from 2011) and 24% own a tablet.Also, 43% of adults now use the internet to seek health-relatedinformation, an increase from 18% in 2007.1 Significant sectionsof society are becoming increasingly familiar and comfortablewith using technology for a wide range of transactions.
E-health and m-health (increasingly collectively referred to as‘connected health’, see Appendix) describe the delivery of health-care by electronic means via the internet using a variety of devicesincluding mobile phones, remote monitoring devices and otherwireless devices. These digital technologies can greatly improveaccess to mental healthcare and treatment adherence by enablingservices to be delivered more flexibly and tailored to individualpatient needs. Recent developments in sensor technology, onlinepsychological therapy and remote video consultation, mobileapplications (‘apps’) and gaming all present real opportunitiesto engage and empower patients and create novel approaches toboth assessment and intervention for mental health problems.
The drivers for technological transformationin mental health services
The growth in demand for mental healthcare exceeds available UKNational Health Service (NHS) resources, and this gap is likely toincrease up to 2020. Cost pressures require that more is done forless and providers therefore must find innovative ways to deliverservices. The UK Government’s mental health strategy ‘No healthwithout mental health’2 recommends the increased use ofinformation and communication technology (ICT) to improvecare and access to services. UK Government initiatives such as‘Digital First’ aim to reduce unnecessary face-to-face contactbetween patients and healthcare professionals with NHS trustsencouraged to replace these unnecessary face-to-face contacts withvideo-based remote consultations. However, service usersconsistently report dissatisfaction with a ‘top–down’ one-size-fits-all approach. Connected health innovations have the potentialto offer great flexibility and to be more patient-centred.
Digital mental healthcare
E-mental health is not just about technology, but represents acultural change in mental healthcare by empowering patients toexercise greater choice and control. For example, the provisionof online psychological interventions, potentially accessible 24 hat day, 7 days a week, is increasing rapidly using synchronousvideo/voice or asynchronous text communication. Examples ofproviders to the NHS include Xenzone (www.xenzone.com),
1
AUTHOR’S PROOF
Technological innovations in mentalhealthcare: harnessing the digital revolutionChris Hollis, Richard Morriss, Jennifer Martin, Sarah Amani, Rebecca Cotton,Mike Denis and Shon Lewis
SummaryDigital technology has the potential to transform mentalhealthcare by connecting patients, services and health datain new ways. Digital online and mobile applications can offerpatients greater access to information and services andenhance clinical management and early intervention throughaccess to real-time patient data. However, substantial gapsexist in the evidence base underlying these technologies.Greater patient and clinician involvement is needed toevaluate digital technologies and ensure they target unmetneeds, maintain public trust and improve clinical outcomes.
Declaration of interestC.H. receives research funding from Shire Pharmaceuticalspaid to his employing institution. R.C. reports that JanssenCilag Ltd have provided a grant to support an upcomingMental Health Network event on the subject of technologyand mental health services. S.L. is chief investigator on theClintouch project. C.H., R.M. and J.M. are all involved in theNational Institute of Health Research (NIHR) MindTechHealthcare Technology Co-operative.
The British Journal of Psychiatry (2015)206, 1–3. doi: 10.1192/bjp.bp.113.142612
Editorial
Chris Hollis (pictured) is Professor of Child and Adolescent Psychiatry at theUniversity of Nottingham, and Director of the National Institute of HealthResearch (NIHR) MindTech Healthcare Technology Co-operative (HTC), hisresearch interests are in attention-deficit hyperactivity disorder,neurodevelopmental disorders and the evaluation and implementation ofdigital technologies in mental healthcare. Richard Morriss is Professor ofPsychiatry at the University of Nottingham, Mood Disorders lead for the NIHRMindTech HTC, Director of Research for NIHR CLAHRC East Midlands andleads externally funded research in randomised controlled trials of video-based psychological treatment for health anxiety and self-harm, internetprogrammes for managing early warning signs of bipolar disorder and facialrecognition to objectively measure the severity of depression. Jennifer Martinis NIHR MindTech HTC programme manager, prior to joining MindTech shewas a senior research fellow in human factors at the University of Nottinghamwhere her research was focused on the development and evaluation ofhealthcare technology. Sarah Amani is a mental health nurse with a specialinterest in early intervention and youth mental health. Her recent workincludes the co-development of mobile health apps, telehealth solutions andpiloting the use of social media in mental health services. Rebecca Cotton isDirector of Policy for the Mental Health Network, part of the NHSConfederation. She has a strong interest in e-health and has previouslywritten on the subject. Mike Denis has recently joined Oxford AcademicHealth Science Centre/Network bringing successful experience in electronicmedical records and patient health records design and leading an Oxford,Cambridge, London research informatics programme. Shon Lewis is Directorof the Institute of Brain, Behaviour and Mental Health at the University ofManchester and Mental Health Academic Lead for the Manchester AcademicHealth Sciences Centre. He leads an European Union- and Medical ResearchCouncil-funded programme of connected health research for people withsevere mental illness.
Author:Please supply aphoto of thefirst author(AQ1)
Author:Please note wehave separatedoff some ofthe materialfrom thissection andplaced it in theFundingsection instead– please checkthe changesare acceptable.Also pleasecheck that thelast sentence,which we haveadded, isappropriateand amend asnecessary(included hereas the co-operative ismentioned inthe articlealong with theClintouchproject).(AQ2)

Q & A
Thank You
Sarah Amani
@S_Amani #SeacoleScholar
www.ehealthconsultant.org