
Small Business Group Benefits Guide - Rogers Benefit · Health Net built our small business group...
56
Small Business Group Jesus Hao, Health Net We keep members informed. Benefits Guide Choice made simple Effective September 1, 2011 Commercial
Transcript of Small Business Group Benefits Guide - Rogers Benefit · Health Net built our small business group...

Small Business Group
Jesus Hao,
Health Net
We keep members
informed.
Benefits GuideChoice made simple
Effective September 1, 2011
Commercial


1
Choice Made Simple
Keeping small business growing with the coverage/cost combinations
that fit just right.
Choices for every business, every budgetHealth Net built our small business group
plan portfolio to meet the diverse and growing
needs of your clients. With several price points
and coverage options, we make it simple to
get maximum value for every health care
plan purchase.
• Standard – This line of well-priced,
comprehensive benefit plans gives your
clients the most for their money.
• Value – The Value plans enable clients
to stretch their health care budget with
more employee cost-sharing.
• Health Net Advantage – Our most
economical line is the optimal solution
for clients who haven’t been able to
provide health benefits, as well as those
who need to trim costs.
Have your pick of Standard, Value or
Advantage in HMO, EOA or PPO design.
Our portfolio also offers Standard and
Value HSA-compatible, HRA-eligible
and POS plans.
Tailored network optionsBuilding accessible, quality networks is one
of the things we do best. We’ve translated that
expertise into tailored network options that
give you the most value for the money.
We started with our full HMO network –
one of California’s largest – and created two
subsets: Silver Network and Bronze Network.
By partnering with select providers, our
tailored networks create value and lower
costs for employers. Plus, they give employees
access to trusted health care resources.
Consumer-directed plansWe’re also the one-stop source for your
clients who want to increase employee
involvement in the way they use and pay for
health care services. We offer both Health
Savings Account (HSA)-compatible health
insurance plans and Health Reimbursement
Arrangement (HRA)-eligible plans.
With Health Net, small business owners have
more budget-friendly options to choose from,
which means that more can buy. And when
more clients are buying, you can do more
selling. Turn the page to see how easy it is!
With several price
points and coverage
options, we make
it simple to get
maximum value for
every health care
plan purchase.

2
1 Health Net HMO, EOA, POS and Salud con Health Net HMO plans are offered by Health Net of California, Inc., a subsidiary of Health Net, Inc. Health Net PPO, HSA-compatible PPO insurance plans, HRA-eligible PPO insurance plans, Flex Net and Salud con Health Net PPO and EPO insurance plans are underwritten by Health Net Life Insurance Company.
2 15, 25, 35 and 45 plans are only available with PPO.
Portfolio at a GlanceOur Standard and Value portfolio features
the complete collection of health plan designs:
HMO, Elect Open Access (EOA), PPO,
HSA-compatible PPO and HRA-eligible
PPO insurance plans and POS.1
Price Levels that
Meet Every BudgetOur plans cover a range of price and benefit
levels, so your clients can get the value they
want and deserve. Plan levels are arranged in
decrements of $5 copay levels with percentages
indicating estimated savings between plans.
Plan type
Average savings between copay plans
Average savings between standard & value plans
Average savings between value & advantage plans
Standard HMO 6%12%
Value HMO 10%6%Advantage
HMO 9%
Standard EOA 6%12%
Value EOA 10%6%Advantage
EOA 7%
Standard PPO 10%20%
Value PPO 11%29%Advantage
PPO 12%
Rich Benefits Less rich
Hea
lth N
et
Adv
anta
ge
$$
$
Po
tent
ial s
avin
gs
$
Valu
e2St
anda
rd
t
10
t
15
t
20
t
50
t
25
t
30
t
35
t
40
t
45
10 15 20
50
t
25 30
t
35 40
t
45
2535
45
Standard Value
Co
pay
HMO EOA PPO HMO EOA PPO POS10 • • • • • • •15 • • • – – • –20 • • • • • • •25 • • • – – • –30 • • • • • • –35 • • • – – • –40 • • • • • • –45 – – • – – • –50 • • – • • – –
Health Net Advantage
Co
pay
HMO EOA PPO25 • • –35 • • •45 • • •
Standard Value
Ded
ucti
ble
HSA-compatible PPO1500 – •2500 – •3500 – •4000 • –4500 – •
HRA-eligible PPO3000 •5000 •

3
3 References are to federal taxes only. State taxes may apply. Tax information is for general purposes only. For more detailed information about the tax implications of an HSA, please contact a professional tax advisor. The HSA component of our HSA-compatible PPO plans is offered by Bank of America, N.A., as trustee of the HSA. Health Net is not affiliated with Bank of America, N.A.
Finding
the Perfect FitStep 1: Choose a plan designHMO – Plans that require members to
select a primary care physician (PCP). The
PCP coordinates all care and referrals for
the member.
EOA (Elect Open AccessSM) – Our EOA
plans work like an HMO plan with the added
flexibility for members to self-refer to select
providers in our statewide PPO network for
professional services.
PPO – These give insureds the choice of going
to a doctor or hospital in our PPO network
– one of the largest in California with over
63,000 physicians, practitioners and health
professionals and 302 hospitals. Or they can
see a provider not in our network. In general,
insureds get more for less when they use our
PPO network.
POS (Point-of-Service) – Members select a
primary physician like they would in an HMO,
but can choose between two tiers of benefits –
HMO or PPO – each time they access covered
services. Out-of-pocket costs are less when
members use their HMO benefits.
Health Savings Account (HSA)-compatible
PPO plans (part of the Standard-Value
portfolio) – These are a great way for your
clients to give their employees the ability
to use their health care dollars in ways that
work best for them while enjoying tax-
saving opportunities. These plans include
access to our full PPO provider network.
Plus, Health Net has partnered with Bank of
America to offer our members an HSA that’s
easy to administer, quick to set up, and that
comes with a convenient Bank of America
VISA® debit card for account access.3
HRA-eligible (Health Reimbursement
Arrangement) PPO insurance plans – A choice
of two high-deductible PPO health insurance
plans that can be used for self-funding or
wrapping purposes, giving small business
owners even more control over their health
care budget. Among the employer advantages
are no third-party administrator (TPA)
restrictions or limits to the plans clients wrap.
Step 2: Select Standard, Value or AdvantageChoose between Standard, Value and
Advantage for an HMO, EOA or PPO plan.
This choice applies to most of our plan
designs except for HRA-eligible and POS.
Here’s how it works:
• MostbenefitsarethesameforStandard,
Value and Health Net Advantage.
• Thevariablebenefitsare:copayamount,
hospital services, PPO plan deductibles,
prescription brand deductibles and
out-of-pocket maximums.
• Thevariablebenefitsadjustinconsistent
increments with the increase in copay
amounts.
Variable benefits
• Copay (professional services)
• Out-of-pocket maximum
• Hospital services
• Deductibles (PPO only)
• Prescription – brand deductibles

4
Step 3: Pick a deductible or copay• ForourStandardHSA-compatiblePPO
plan, we offer a deductible amount of
$4,000. The plan features 100 percent
in-network coverage for covered services
after the annual deductible is met. And if
the Standard plan doesn’t meet your clients’
needs, we also have Value HSA-compatible
PPO plans at $1,500, $2,500, $3,500 and
$4,500 deductible levels.
• OurHRA-eligiblePPOinsuranceplansare
great cost-saving solutions for your clients
who wish to self-fund or wrap benefit
plans. Groups can pick from two deductible
amounts, $3,000 or $5,000.
• Forallofourotherplans,groupshavea
choice of copay (see the “Portfolio at a glance”
section and plan grids for the options).
Step 4: Pick a network• HMO network – provides over 46,500
physicians and 5,500 pharmacies
across California.
• Silver Network – a select subset of our
regular HMO network offers up to a 25%
savings in parts of our service area. In this
service area, members have access to more
than 6,600 primary care physicians and
14,300 specialists.
• HMO Bronze Network – a select subset
of our Silver Network offers up to a 14%
savings in parts of our service area. In this
service area, members have access to more
than 1,600 primary care physicians and
3,200 specialists.
• PPO network – includes more than
63,000 physicians and 5,500 pharmacies
across California.
Silver Network service areaAvailable in all or parts of Kern, Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Francisco, Santa Clara, Stanislaus and Ventura counties.
Bronze Network service areaAvailable in parts of Los Angeles, San Bernardino and San Diego counties.
Herminia Escobedo,
Health Net
We get members
what they need.

5
4Available in Orange and select ZIP codes of Los Angeles, Riverside, San Bernardino and San Diego counties.
5Available in Los Angeles, Orange and Ventura counties.
6Available in Mexicali, Rosarito, Tecate and Tijuana.
Package deals: Tailored for choice
Enhanced Choice, Silver Choice, Bronze Choice
With the Choice packages, members receive
the same high quality of care, but at an even
lower price. Employers pay one fixed premium
amount while giving employees the option of
choosing from any of the plans in the small
group portfolio.
Hn Options, Hn Options + Silver, Hn Options + Bronze
The Hn Options packages give employees
a choice of 12 (for five to nine employees)
or 17 (for 10 to 50 employees) Health Net
plans that may be offered alongside another
carrier, including Kaiser Permanente, as long
as the employer meets a few participation
requirements.
See our Underwriting Guidelines for
package specifics.
Cross-border coverage: SaludOur affordable and innovative cross-border
plan continues to bring an affordable health
care option tailored to the unique needs of
the Latino community. Salud plans feature:
• Accesstomorethan3,600doctorsand
specialists in our Salud HMO Network.4
Or, there are also more than 1,300
physicians and specialists in our Salud
PPO Network5 and more than 200 doctors
in the SIMNSA Network6 in México.
• Cross-borderaccesstocarewithouta
referral via the Sistemas Médicos Nacionales,
S.A. de C.V. (SIMNSA) network of providers
in Mexico (Tijuana, Mexicali, Rosarito
and Tecate).
• Coverageforeligibledependentslivingin
Mexico, within 50 miles of the California
border, who may enroll and receive care
exclusively from SIMNSA providers.
• Urgentcarefacilitiesforafter-hourscare
(in select medical groups).
• Ratesrunapproximately30–40percentlower
than similar commercial plans in the market
that don’t offer cross-border coverage.
The Salud plans are a great way to attract new
group clients in the counties of Los Angeles,
Orange and San Diego, plus select ZIP codes
in San Bernardino and Riverside counties. Call
your Health Net sales representative to get
service area ZIP codes.
Dual Network option: Mix and matchPick any number of Silver Choice or Bronze Choice tailored network plans. Clients first select Silver or Bronze and then offer as many plans as they’d like within that portfolio.
Offer up to four specially designed full network HMO plans alongside. Each one comes with the familiar HMO benefits, full network access,
health-promoting wellness resources, and more. So all your clients have to do is pick the one – or ones – that fits their business best.
To qualify for Dual Network, clients need to have 2–50 employees and 75 percent participation with a minimum of two employees enrolled.
1
2
6
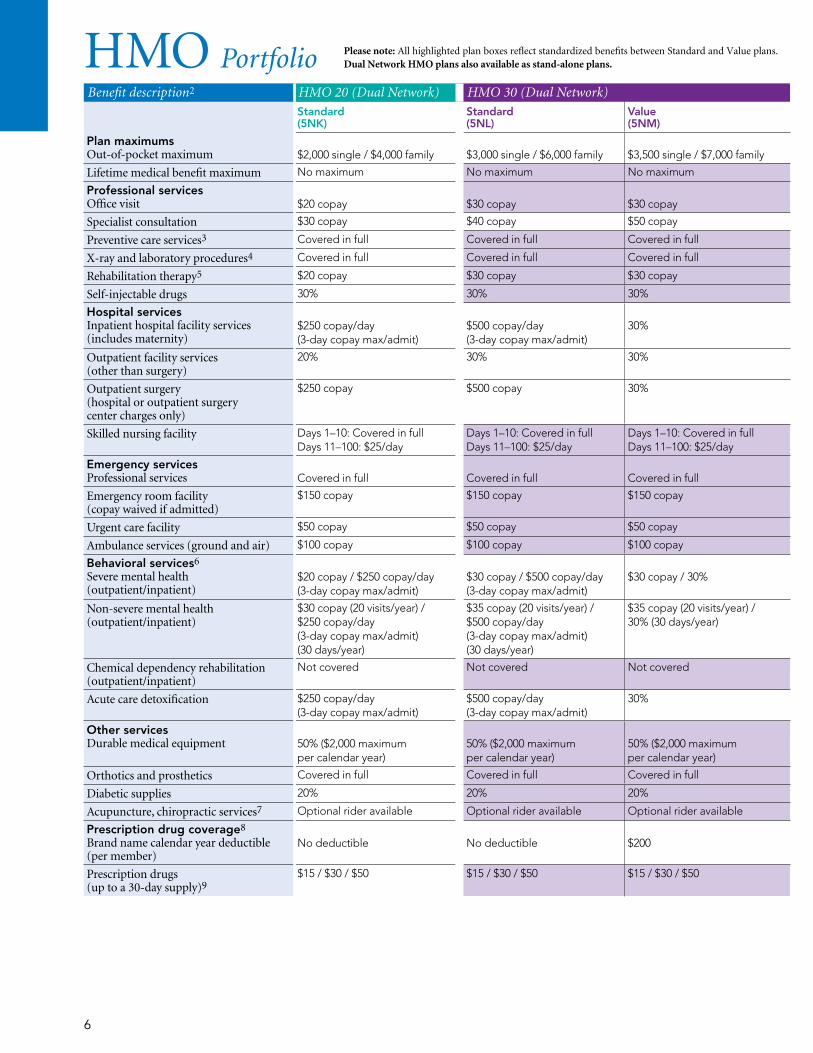
HMO PortfolioBenefit description2 HMO 20 (Dual Network) HMO 30 (Dual Network) HMO 40 (Dual Network)
Standard (5NK)
Standard (5NL)
Value (5NM)
Value (5NJ)
Plan maximumsOut-of-pocket maximum
$2,000 single / $4,000 family
$3,000 single / $6,000 family
$3,500 single / $7,000 family
$4,500 single / $9,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$20 copay
$30 copay
$30 copay
$40 copay
Specialist consultation $30 copay $40 copay $50 copay $60 copay
Preventive care services3 Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy5 $20 copay $30 copay $30 copay $40 copay
Self-injectable drugs 30% 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
$250 copay/day (3-day copay max/admit)
$500 copay/day (3-day copay max/admit)
30%
40%
Outpatient facility services (other than surgery)
20% 30% 30% 40%
Outpatient surgery (hospital or outpatient surgery center charges only)
$250 copay $500 copay 30% 40%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$150 copay $150 copay $150 copay $150 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air) $100 copay $100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$20 copay / $250 copay/day (3-day copay max/admit)
$30 copay / $500 copay/day (3-day copay max/admit)
$30 copay / 30%
$40 copay / 40%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/year) / 30% (30 days/year)
$40 copay (20 visits/year) / 40% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered
Acute care detoxification $250 copay/day (3-day copay max/admit)
$500 copay/day (3-day copay max/admit)
30% 40%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
No deductible
No deductible
$200
$250
Prescription drugs (up to a 30-day supply)9
$15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50
Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans. Dual Network HMO plans also available as stand-alone plans.

7
HM
O
Plan footnotes found on pages 50–53.
Benefit description2 HMO 20 (Dual Network) HMO 30 (Dual Network) HMO 40 (Dual Network)
Standard (5NK)
Standard (5NL)
Value (5NM)
Value (5NJ)
Plan maximumsOut-of-pocket maximum
$2,000 single / $4,000 family
$3,000 single / $6,000 family
$3,500 single / $7,000 family
$4,500 single / $9,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$20 copay
$30 copay
$30 copay
$40 copay
Specialist consultation $30 copay $40 copay $50 copay $60 copay
Preventive care services3 Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy5 $20 copay $30 copay $30 copay $40 copay
Self-injectable drugs 30% 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
$250 copay/day (3-day copay max/admit)
$500 copay/day (3-day copay max/admit)
30%
40%
Outpatient facility services (other than surgery)
20% 30% 30% 40%
Outpatient surgery (hospital or outpatient surgery center charges only)
$250 copay $500 copay 30% 40%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$150 copay $150 copay $150 copay $150 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air) $100 copay $100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$20 copay / $250 copay/day (3-day copay max/admit)
$30 copay / $500 copay/day (3-day copay max/admit)
$30 copay / 30%
$40 copay / 40%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/year) / 30% (30 days/year)
$40 copay (20 visits/year) / 40% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered
Acute care detoxification $250 copay/day (3-day copay max/admit)
$500 copay/day (3-day copay max/admit)
30% 40%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
No deductible
No deductible
$200
$250
Prescription drugs (up to a 30-day supply)9
$15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50

8
HMO Portfolio Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans. All HMO plans available in the full, Silver or Bronze Networks.1
Benefit description2 HMO 10 HMO 15 HMO 20 HMO 25
Standard (1EJ) (1FV) (1GE)
Value (1EN) (1FZ) (1GJ)
Standard (5SG) (5SN) (5SU)
Standard (1EK) (1FW) (1GF)
Value (1EP) (1GB) (1GK)
Standard (5SH) (5SP) (5SV)
Plan maximumsOut-of-pocket maximum
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$2,500 single / $5,000 family
$2,000 single / $4,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$10 copay
$10 copay
$15 copay
$20 copay
$20 copay
$25 copay
Preventive care services3 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy5 $10 copay $10 copay $15 copay $20 copay $20 copay $25 copay
Self-injectable drugs 30% 30% 30% 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
10%
$250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20%
$500 copay/day (3-day copay max/admit)
Outpatient facility services (other than surgery)
Covered in full 10% 15% 20% 20% 25%
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 10% $250 copay $250 copay 20% $500 copay
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $150 copay $100 copay $100 copay $150 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$10 copay / Covered in full
$10 copay / 10%
$15 copay / $250 copay/day (3-day copay max/admit)
$20 copay / $250 copay/day (3-day copay max/admit)
$20 copay / 20%
$25 copay / $500 copay/day (3-day copay max/admit)
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / Covered in full (30 days/year)
$30 copay (20 visits/year) / 10% (30 days/year)
$15 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 20% (30 days/year)
$25 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered Not covered
Acute care detoxification Covered in full 10% $250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20% $500 copay/day (3-day copay max/admit)
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
No deductible
$100
No deductible
No deductible
$150
No deductible
Prescription drugs (up to a 30-day supply)9
$10 / $25 / $50 $10 / $25 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50

9
HM
O
Plan footnotes found on pages 50–53.
Benefit description2 HMO 10 HMO 15 HMO 20 HMO 25
Standard (1EJ) (1FV) (1GE)
Value (1EN) (1FZ) (1GJ)
Standard (5SG) (5SN) (5SU)
Standard (1EK) (1FW) (1GF)
Value (1EP) (1GB) (1GK)
Standard (5SH) (5SP) (5SV)
Plan maximumsOut-of-pocket maximum
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$2,500 single / $5,000 family
$2,000 single / $4,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$10 copay
$10 copay
$15 copay
$20 copay
$20 copay
$25 copay
Preventive care services3 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy5 $10 copay $10 copay $15 copay $20 copay $20 copay $25 copay
Self-injectable drugs 30% 30% 30% 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
10%
$250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20%
$500 copay/day (3-day copay max/admit)
Outpatient facility services (other than surgery)
Covered in full 10% 15% 20% 20% 25%
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 10% $250 copay $250 copay 20% $500 copay
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $150 copay $100 copay $100 copay $150 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$10 copay / Covered in full
$10 copay / 10%
$15 copay / $250 copay/day (3-day copay max/admit)
$20 copay / $250 copay/day (3-day copay max/admit)
$20 copay / 20%
$25 copay / $500 copay/day (3-day copay max/admit)
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / Covered in full (30 days/year)
$30 copay (20 visits/year) / 10% (30 days/year)
$15 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 20% (30 days/year)
$25 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered Not covered
Acute care detoxification Covered in full 10% $250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20% $500 copay/day (3-day copay max/admit)
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
No deductible
$100
No deductible
No deductible
$150
No deductible
Prescription drugs (up to a 30-day supply)9
$10 / $25 / $50 $10 / $25 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50

10
HMO Portfolio Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans. All HMO plans available in the full, Silver or Bronze Networks.1
Benefit description2 HMO 30 HMO 35 HMO 40 HMO 50
Standard (1EL) (1FX) (1GG)
Value (1EQ) (1GC) (1GL)
Standard (5SJ) (5SQ) (5SW)
Standard (1EM) (1FY) (1GH)
Value (1ER) (1GD) (1GM)
Standard (5NS) (5BP) (5PD)
Value (5NT) (5PC) (5PE)
Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$3,500 single / $7,000 family
$3,000 single / $6,000 family
$4,000 single / $8,000 family
$4,500 single / $9,000 family
$4,500 single / $9,000 family
$5,750 single / $11,500 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$30 copay
$30 copay
$35 copay
$40 copay
$40 copay
$50 copay
$50 copay
Preventive care services3 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy5 $30 copay $30 copay $35 copay $40 copay $40 copay $50 copay $50 copay
Self-injectable drugs 30% 30% 30% 30% 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
$500 copay/day (3-day copay max/admit)
30%
$750 copay/day (3-day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40%
$1,500 copay/day (3-day copay max/admit)
50%
Outpatient facility services (other than surgery)
30% 30% 35% 40% 40% 50% 50%
Outpatient surgery (hospital or outpatient surgery center charges only)
$500 copay 30% $750 copay $1,000 copay 40% $1,500 copay 50%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $150 copay $100 copay $100 copay $200 copay $300 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$30 copay / $500 copay/day (3-day copay max/admit)
$30 copay / 30%
$35 copay / $750 copay/day (3-day copay max/admit)
$40 copay / $1,000 copay/day (3-day copay max/admit)
$40 copay / 40%
$50 copay / $1,500 copay/day (3-day copay max/admit)
$50 copay / 50%
Non-severe mental health (outpatient/inpatient)
$35 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/year) / 30% (30 days/year)
$35 copay (20 visits/year) / $750 copay/day (3-day copay max/admit) (30 days/year)
$40 copay (20 visits/year) / $1,000 copay/day (3-day copay max/admit) (30 days/year)
$40 copay (20 visits/year) / 40% (30 days/year)
$50 copay (20 visits/year) / $1,500 copay/day (3-day copay max/admit) (30 days/year)
$50 copay (20 visits/year) / 50% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered Not covered Not covered
Acute care detoxification $500 copay/day (3-day copay max/admit)
30% $750 copay/day (3-day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40% $1,500 copay/day (3-day copay max/admit)
50%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
No deductible
$200
No deductible
No deductible
$250
No deductible
$250
Prescription drugs (up to a 30-day supply)9
$15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50

11
HM
O
Plan footnotes found on pages 50–53.
Benefit description2 HMO 30 HMO 35 HMO 40 HMO 50
Standard (1EL) (1FX) (1GG)
Value (1EQ) (1GC) (1GL)
Standard (5SJ) (5SQ) (5SW)
Standard (1EM) (1FY) (1GH)
Value (1ER) (1GD) (1GM)
Standard (5NS) (5BP) (5PD)
Value (5NT) (5PC) (5PE)
Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$3,500 single / $7,000 family
$3,000 single / $6,000 family
$4,000 single / $8,000 family
$4,500 single / $9,000 family
$4,500 single / $9,000 family
$5,750 single / $11,500 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$30 copay
$30 copay
$35 copay
$40 copay
$40 copay
$50 copay
$50 copay
Preventive care services3 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy5 $30 copay $30 copay $35 copay $40 copay $40 copay $50 copay $50 copay
Self-injectable drugs 30% 30% 30% 30% 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
$500 copay/day (3-day copay max/admit)
30%
$750 copay/day (3-day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40%
$1,500 copay/day (3-day copay max/admit)
50%
Outpatient facility services (other than surgery)
30% 30% 35% 40% 40% 50% 50%
Outpatient surgery (hospital or outpatient surgery center charges only)
$500 copay 30% $750 copay $1,000 copay 40% $1,500 copay 50%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $150 copay $100 copay $100 copay $200 copay $300 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$30 copay / $500 copay/day (3-day copay max/admit)
$30 copay / 30%
$35 copay / $750 copay/day (3-day copay max/admit)
$40 copay / $1,000 copay/day (3-day copay max/admit)
$40 copay / 40%
$50 copay / $1,500 copay/day (3-day copay max/admit)
$50 copay / 50%
Non-severe mental health (outpatient/inpatient)
$35 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/year) / 30% (30 days/year)
$35 copay (20 visits/year) / $750 copay/day (3-day copay max/admit) (30 days/year)
$40 copay (20 visits/year) / $1,000 copay/day (3-day copay max/admit) (30 days/year)
$40 copay (20 visits/year) / 40% (30 days/year)
$50 copay (20 visits/year) / $1,500 copay/day (3-day copay max/admit) (30 days/year)
$50 copay (20 visits/year) / 50% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered Not covered Not covered
Acute care detoxification $500 copay/day (3-day copay max/admit)
30% $750 copay/day (3-day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40% $1,500 copay/day (3-day copay max/admit)
50%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
No deductible
$200
No deductible
No deductible
$250
No deductible
$250
Prescription drugs (up to a 30-day supply)9
$15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50

12
HMO Portfolio Please note: All highlighted plan boxes reflect standardized benefits between Advantage plans. All HMO plans available in the full, Silver or Bronze Networks.1
Benefit description2 Advantage HMO 25 (1JZ) (1JV) (1JT) Advantage HMO 35 (1KB) (1JW) (1JU) Advantage HMO 45 (1JY) (1JR) (1JS)Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family
$5,000 single / $10,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$25 copay
$35 copay
$45 copay
Preventive care services3 Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full
Rehabilitation therapy5 $25 copay $35 copay $45 copay
Self-injectable drugs 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
25%
35%
45%
Outpatient facility services (other than surgery)
25% 35% 45%
Outpatient surgery (hospital or outpatient surgery center charges only)
25% 35% 45%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $100 copay
Urgent care facility $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$25 copay / 25%
$35 copay / 35%
$45 copay / 45%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / 25% (30 days/year) $35 copay (20 visits/year) / 35% (30 days/year) $45 copay (20 visits/year) / 45% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered
Acute care detoxification 25% 35% 45%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
$200
$250
$300
Prescription drugs (up to a 30-day supply)9
$15 / $40 / $60 $15 / $40 / $60 $15 / $40 / $60

13
HM
O
Plan footnotes found on pages 50–53.
Benefit description2 Advantage HMO 25 (1JZ) (1JV) (1JT) Advantage HMO 35 (1KB) (1JW) (1JU) Advantage HMO 45 (1JY) (1JR) (1JS)Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family
$5,000 single / $10,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$25 copay
$35 copay
$45 copay
Preventive care services3 Covered in full Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full Covered in full
Rehabilitation therapy5 $25 copay $35 copay $45 copay
Self-injectable drugs 30% 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
25%
35%
45%
Outpatient facility services (other than surgery)
25% 35% 45%
Outpatient surgery (hospital or outpatient surgery center charges only)
25% 35% 45%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $100 copay
Urgent care facility $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$25 copay / 25%
$35 copay / 35%
$45 copay / 45%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / 25% (30 days/year) $35 copay (20 visits/year) / 35% (30 days/year) $45 copay (20 visits/year) / 45% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered
Acute care detoxification 25% 35% 45%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
$200
$250
$300
Prescription drugs (up to a 30-day supply)9
$15 / $40 / $60 $15 / $40 / $60 $15 / $40 / $60

14
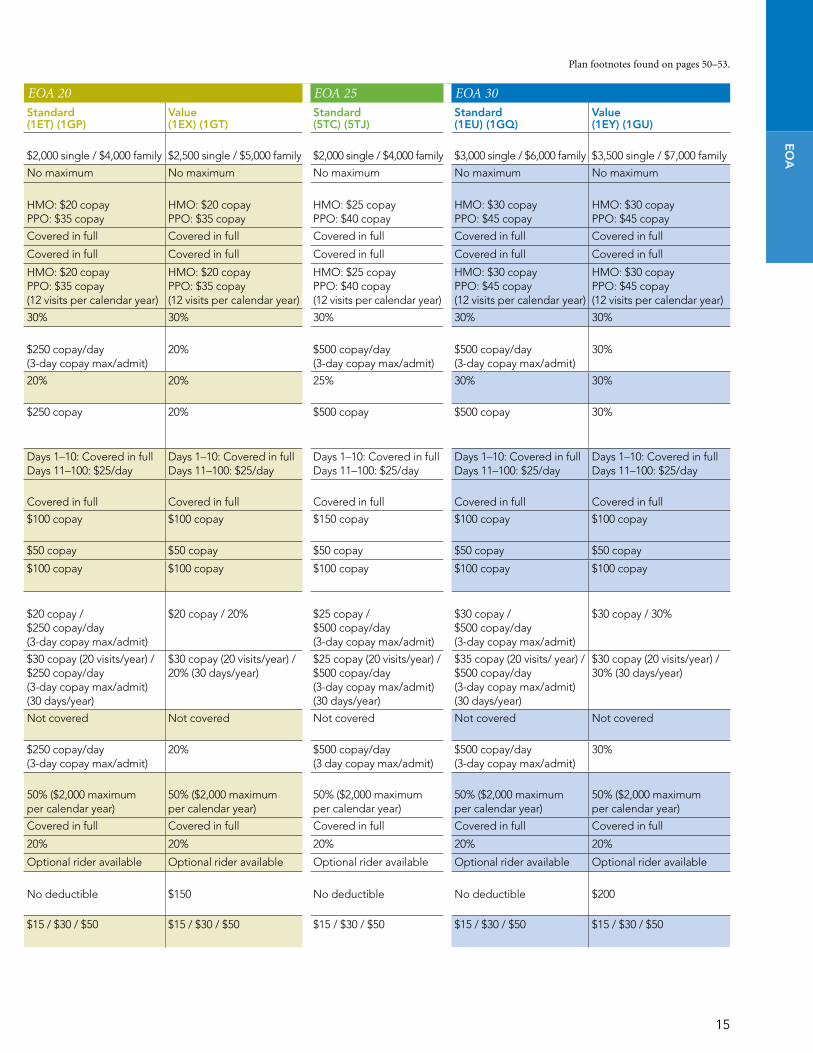
EOA Portfolio Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans. All EOA plans available in Silver Network.1
Benefit description2 EOA 10 EOA 15 EOA 20 EOA 25 EOA 30
Standard (1ES) (1GN)
Value (1EW) (1GS)
Standard (5TB) (5TH)
Standard (1ET) (1GP)
Value (1EX) (1GT)
Standard (5TC) (5TJ)
Standard (1EU) (1GQ)
Value (1EY) (1GU)
Plan maximumsOut-of-pocket maximum
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$2,500 single / $5,000 family
$2,000 single / $4,000 family
$3,000 single / $6,000 family
$3,500 single / $7,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum No maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $10 copay PPO: $25 copay
HMO: $10 copay PPO: $25 copay
HMO: $15 copay PPO: $30 copay
HMO: $20 copay PPO: $35 copay
HMO: $20 copay PPO: $35 copay
HMO: $25 copay PPO: $40 copay
HMO: $30 copay PPO: $45 copay
HMO: $30 copay PPO: $45 copay
Preventive care services4 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy7 HMO: $10 copay PPO: $25 copay (12 visits per calendar year)
HMO: $10 copay PPO: $25 copay (12 visits per calendar year)
HMO: $15 copay PPO: $30 copay (12 visits per calendar year)
HMO: $20 copay PPO: $35 copay (12 visits per calendar year)
HMO: $20 copay PPO: $35 copay (12 visits per calendar year)
HMO: $25 copay PPO: $40 copay (12 visits per calendar year)
HMO: $30 copay PPO: $45 copay (12 visits per calendar year)
HMO: $30 copay PPO: $45 copay (12 visits per calendar year)
Self-injectable drugs 30% 30% 30% 30% 30% 30% 30% 30%
Hospital services8
Inpatient hospital facility services (includes maternity)
Covered in full
10%
$250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20%
$500 copay/day (3-day copay max/admit)
$500 copay/day (3-day copay max/admit)
30%
Outpatient facility services (other than surgery)
Covered in full 10% 15% 20% 20% 25% 30% 30%
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 10% $250 copay $250 copay 20% $500 copay $500 copay 30%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $150 copay $100 copay $100 copay $150 copay $100 copay $100 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services9
Severe mental health (outpatient/inpatient)
$10 copay / Covered in full
$10 copay / 10%
$15 copay / $250 copay/day (3-day copay max/admit)
$20 copay / $250 copay/day (3-day copay max/admit)
$20 copay / 20%
$25 copay / $500 copay/day (3-day copay max/admit)
$30 copay / $500 copay/day (3-day copay max/admit)
$30 copay / 30%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/ year) / Covered in full (30 days/year)
$30 copay (20 visits/year) / 10% (30 days/year)
$15 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 20% (30 days/year)
$25 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/ year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 30% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered Not covered Not covered Not covered
Acute care detoxification Covered in full 10% $250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20% $500 copay/day (3 day copay max/admit)
$500 copay/day (3-day copay max/admit)
30%
Other servicesDurable medical equipment8
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20% 20% 20% 20%
Acupuncture, chiropractic services10 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage11
Brand name calendar year deductible (per member)
No deductible
$100
No deductible
No deductible
$150
No deductible
No deductible
$200
Prescription drugs (up to a 30-day supply)12
$10 / $25 / $50 $10 / $25 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50
15
Plan footnotes found on pages 50–53.
Benefit description2 EOA 10 EOA 15 EOA 20 EOA 25 EOA 30
Standard (1ES) (1GN)
Value (1EW) (1GS)
Standard (5TB) (5TH)
Standard (1ET) (1GP)
Value (1EX) (1GT)
Standard (5TC) (5TJ)
Standard (1EU) (1GQ)
Value (1EY) (1GU)
Plan maximumsOut-of-pocket maximum
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$1,500 single / $3,000 family
$2,000 single / $4,000 family
$2,500 single / $5,000 family
$2,000 single / $4,000 family
$3,000 single / $6,000 family
$3,500 single / $7,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum No maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $10 copay PPO: $25 copay
HMO: $10 copay PPO: $25 copay
HMO: $15 copay PPO: $30 copay
HMO: $20 copay PPO: $35 copay
HMO: $20 copay PPO: $35 copay
HMO: $25 copay PPO: $40 copay
HMO: $30 copay PPO: $45 copay
HMO: $30 copay PPO: $45 copay
Preventive care services4 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy7 HMO: $10 copay PPO: $25 copay (12 visits per calendar year)
HMO: $10 copay PPO: $25 copay (12 visits per calendar year)
HMO: $15 copay PPO: $30 copay (12 visits per calendar year)
HMO: $20 copay PPO: $35 copay (12 visits per calendar year)
HMO: $20 copay PPO: $35 copay (12 visits per calendar year)
HMO: $25 copay PPO: $40 copay (12 visits per calendar year)
HMO: $30 copay PPO: $45 copay (12 visits per calendar year)
HMO: $30 copay PPO: $45 copay (12 visits per calendar year)
Self-injectable drugs 30% 30% 30% 30% 30% 30% 30% 30%
Hospital services8
Inpatient hospital facility services (includes maternity)
Covered in full
10%
$250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20%
$500 copay/day (3-day copay max/admit)
$500 copay/day (3-day copay max/admit)
30%
Outpatient facility services (other than surgery)
Covered in full 10% 15% 20% 20% 25% 30% 30%
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 10% $250 copay $250 copay 20% $500 copay $500 copay 30%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $150 copay $100 copay $100 copay $150 copay $100 copay $100 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services9
Severe mental health (outpatient/inpatient)
$10 copay / Covered in full
$10 copay / 10%
$15 copay / $250 copay/day (3-day copay max/admit)
$20 copay / $250 copay/day (3-day copay max/admit)
$20 copay / 20%
$25 copay / $500 copay/day (3-day copay max/admit)
$30 copay / $500 copay/day (3-day copay max/admit)
$30 copay / 30%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/ year) / Covered in full (30 days/year)
$30 copay (20 visits/year) / 10% (30 days/year)
$15 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / $250 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 20% (30 days/year)
$25 copay (20 visits/year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$35 copay (20 visits/ year) / $500 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 30% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered Not covered Not covered Not covered
Acute care detoxification Covered in full 10% $250 copay/day (3-day copay max/admit)
$250 copay/day (3-day copay max/admit)
20% $500 copay/day (3 day copay max/admit)
$500 copay/day (3-day copay max/admit)
30%
Other servicesDurable medical equipment8
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20% 20% 20% 20%
Acupuncture, chiropractic services10 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage11
Brand name calendar year deductible (per member)
No deductible
$100
No deductible
No deductible
$150
No deductible
No deductible
$200
Prescription drugs (up to a 30-day supply)12
$10 / $25 / $50 $10 / $25 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50
EO
A

16
EOA Portfolio Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans. All EOA plans available in Silver Network.1
Benefit description2 EOA 35 EOA 40 EOA 50
Standard (5TD) (5TK)
Standard (1EV) (1GR)
Value (1EZ) (1GV)
Standard (5NX) (5PL)
Value (5NW) (5PK)
Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family
$4,500 single / $9,000 family
$4,500 single / $9,000 family
$5,750 single / $11,500 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $35 copay PPO: $50 copay
HMO: $40 copay PPO: $55 copay
HMO: $40 copay PPO: $55 copay
HMO: $50 copay PPO: $65 copay
HMO: $50 copay PPO: $65 copay
Preventive care services4 Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy7 HMO: $35 copay PPO: $50 copay (12 visits per calendar year)
HMO: $40 copay PPO: $55 copay (12 visits per calendar year)
HMO: $40 copay PPO: $55 copay (12 visits per calendar year)
HMO: $50 copay PPO: $65 copay (12 visits per calendar year)
HMO: $50 copay PPO: $65 copay (12 visits per calendar year)
Self-injectable drugs 30% 30% 30% 30% 30%
Hospital services8
Inpatient hospital facility services (includes maternity)
$750 copay/day (3-day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40%
$1,500 copay/day (3-day copay max/admit)
50%
Outpatient facility services (other than surgery)
35% 40% 40% 50% 50%
Outpatient surgery (hospital or outpatient surgery center charges only)
$750 copay $1,000 copay 40% $1,500 copay 50%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$150 copay $100 copay $100 copay $200 copay $300 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services9
Severe mental health (outpatient/inpatient)
$35 copay / $750 copay/day (3-day copay max/admit)
$40 copay / $1,000 copay/day (3-day copay max/admit)
$40 copay / 40%
$50 copay / $1,500 copay/day (3-day copay max/admit)
$50 copay / 50%
Non-severe mental health (outpatient/inpatient)
$35 copay (20 visits/year) / $750 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / $1,000 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 40% (30 days/year)
$50 copay (20 visits/year) / $1,500 copay/day (3-day copay max/admit) (30 days/year)
$50 copay (20 visits/year) / 50% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered
Acute care detoxification $750 copay/day (3 day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40% $1,500 copay/day (3 day copay max/admit)
50%
Other servicesDurable medical equipment8
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20%
Acupuncture, chiropractic services10 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage11
Brand name calendar year deductible (per member)
No deductible
No deductible
$250
No deductible
$250
Prescription drugs (up to a 30-day supply)12
$15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50

17
Plan footnotes found on pages 50–53.
Benefit description2 EOA 35 EOA 40 EOA 50
Standard (5TD) (5TK)
Standard (1EV) (1GR)
Value (1EZ) (1GV)
Standard (5NX) (5PL)
Value (5NW) (5PK)
Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family
$4,500 single / $9,000 family
$4,500 single / $9,000 family
$5,750 single / $11,500 family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $35 copay PPO: $50 copay
HMO: $40 copay PPO: $55 copay
HMO: $40 copay PPO: $55 copay
HMO: $50 copay PPO: $65 copay
HMO: $50 copay PPO: $65 copay
Preventive care services4 Covered in full Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full Covered in full Covered in full Covered in full
Rehabilitation therapy7 HMO: $35 copay PPO: $50 copay (12 visits per calendar year)
HMO: $40 copay PPO: $55 copay (12 visits per calendar year)
HMO: $40 copay PPO: $55 copay (12 visits per calendar year)
HMO: $50 copay PPO: $65 copay (12 visits per calendar year)
HMO: $50 copay PPO: $65 copay (12 visits per calendar year)
Self-injectable drugs 30% 30% 30% 30% 30%
Hospital services8
Inpatient hospital facility services (includes maternity)
$750 copay/day (3-day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40%
$1,500 copay/day (3-day copay max/admit)
50%
Outpatient facility services (other than surgery)
35% 40% 40% 50% 50%
Outpatient surgery (hospital or outpatient surgery center charges only)
$750 copay $1,000 copay 40% $1,500 copay 50%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$150 copay $100 copay $100 copay $200 copay $300 copay
Urgent care facility $50 copay $50 copay $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay $100 copay $100 copay
Behavioral services9
Severe mental health (outpatient/inpatient)
$35 copay / $750 copay/day (3-day copay max/admit)
$40 copay / $1,000 copay/day (3-day copay max/admit)
$40 copay / 40%
$50 copay / $1,500 copay/day (3-day copay max/admit)
$50 copay / 50%
Non-severe mental health (outpatient/inpatient)
$35 copay (20 visits/year) / $750 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / $1,000 copay/day (3-day copay max/admit) (30 days/year)
$30 copay (20 visits/year) / 40% (30 days/year)
$50 copay (20 visits/year) / $1,500 copay/day (3-day copay max/admit) (30 days/year)
$50 copay (20 visits/year) / 50% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered Not covered Not covered
Acute care detoxification $750 copay/day (3 day copay max/admit)
$1,000 copay/day (3-day copay max/admit)
40% $1,500 copay/day (3 day copay max/admit)
50%
Other servicesDurable medical equipment8
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20% 20% 20%
Acupuncture, chiropractic services10 Optional rider available Optional rider available Optional rider available Optional rider available Optional rider available
Prescription drug coverage11
Brand name calendar year deductible (per member)
No deductible
No deductible
$250
No deductible
$250
Prescription drugs (up to a 30-day supply)12
$15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50 $15 / $30 / $50
EO
A

18
EOA Portfolio Please note: All highlighted plan boxes reflect standardized benefits between Advantage plans. All EOA plans available in Silver Network.1
Benefit description2 Advantage EOA 25 (1KD) (1KH) Advantage EOA 35 (1KE) (1KJ) Advantage EOA 45 (1KC) (1KG)
Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family $5,000 single / $10,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $25 copay PPO: $45 copay
HMO: $35 copay PPO: $55 copay
HMO: $45 copay PPO: $65 copay
Preventive care services4 Covered in full Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full Covered in full
Rehabilitation therapy7 HMO: $25 copay / PPO: $45 copay(12 visits per calendar year)
HMO: $35 copay / PPO: $55 copay(12 visits per calendar year)
HMO: $45 copay / PPO: $65 copay(12 visits per calendar year)
Self-injectable drugs 30% 30% 30%
Hospital services8
Inpatient hospital facility services (includes maternity)
25%
35%
45%
Outpatient facility services (other than surgery)
25% 35% 45%
Outpatient surgery (hospital or outpatient surgery center charges only)
25% 35% 45%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $100 copay
Urgent care facility $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay
Behavioral services9
Severe mental health (outpatient/inpatient)
$25 copay / 25% $35 copay / 35% $45 copay / 45%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / 25% (30 days/year) $35 copay (20 visits/year) / 35% (30 days/year) $45 copay (20 visits/year) / 45% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered
Acute care detoxification 25% 35% 45%
Other servicesDurable medical equipment8 50% ($2,000 maximum per calendar year) 50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20%
Acupuncture, chiropractic services10 Optional rider available Optional rider available Optional rider available
Prescription drug coverage11
Brand name calendar year deductible (per member)
$200 $250
$300
Prescription drugs (up to a 30-day supply)12
$15 / $40 / $60 $15 / $40 / $60 $15 / $40 / $60

19
Plan footnotes found on pages 50–53.
Benefit description2 Advantage EOA 25 (1KD) (1KH) Advantage EOA 35 (1KE) (1KJ) Advantage EOA 45 (1KC) (1KG)
Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family $5,000 single / $10,000 family
Lifetime medical benefit maximum No maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $25 copay PPO: $45 copay
HMO: $35 copay PPO: $55 copay
HMO: $45 copay PPO: $65 copay
Preventive care services4 Covered in full Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full Covered in full
Rehabilitation therapy7 HMO: $25 copay / PPO: $45 copay(12 visits per calendar year)
HMO: $35 copay / PPO: $55 copay(12 visits per calendar year)
HMO: $45 copay / PPO: $65 copay(12 visits per calendar year)
Self-injectable drugs 30% 30% 30%
Hospital services8
Inpatient hospital facility services (includes maternity)
25%
35%
45%
Outpatient facility services (other than surgery)
25% 35% 45%
Outpatient surgery (hospital or outpatient surgery center charges only)
25% 35% 45%
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Days 1–10: Covered in full Days 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay $100 copay
Urgent care facility $50 copay $50 copay $50 copay
Ambulance services (ground and air)
$100 copay $100 copay $100 copay
Behavioral services9
Severe mental health (outpatient/inpatient)
$25 copay / 25% $35 copay / 35% $45 copay / 45%
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits/year) / 25% (30 days/year) $35 copay (20 visits/year) / 35% (30 days/year) $45 copay (20 visits/year) / 45% (30 days/year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered Not covered
Acute care detoxification 25% 35% 45%
Other servicesDurable medical equipment8 50% ($2,000 maximum per calendar year) 50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full Covered in full
Diabetic supplies 20% 20% 20%
Acupuncture, chiropractic services10 Optional rider available Optional rider available Optional rider available
Prescription drug coverage11
Brand name calendar year deductible (per member)
$200 $250
$300
Prescription drugs (up to a 30-day supply)12
$15 / $40 / $60 $15 / $40 / $60 $15 / $40 / $60
EO
A

20
POS PortfolioBenefit description1 POS 10 (1FB) POS 20 (1FC)
Plan maximumsCalendar year deductible
HMO PPO2 Out-of-network3.4 HMO PPO2 Out-of-network3.4
No deductible
$250 single / $500 family
$500 single / $1,000 family
No deductible
$500 single / $1,000 family
$1,000 single / $2,000 family
Out-of-pocket maximum $1,500 single / $3,000 family $3,000 single / 2 per family $6,000 single / 2 per family $2,000 single / $4,000 family $3,500 single / 2 per family $7,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$10 copay
$20 copay
50%
$20 copay
$30 copay
50%
Preventive care services5 Covered in full Covered in full Not covered Covered in full Covered in full Not covered
X-ray and laboratory procedures Covered in full 10% 50% Covered in full 20%7 50%7
Rehabilitation therapy6 $10 copay 10% 50% $20 copay 20%7 50%7
(12 visits per calendar year, PPO and OON combined) (12 visits per calendar year, PPO and OON combined)
Self-injectable drugs 30% 30% 50% 30% 30%7 50%7
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
10%7
50% ($600 maximum allowable/day)7
$250 copay/day (3-day copay maximum)
20%7
50% ($600 maximum allowable/day)7
($250 deductible per calendar year, PPO and OON combined)8 ($250 deductible per calendar year, PPO and OON combined)8
Outpatient facility services (other than surgery)
Covered in full 10%7 50% (50% maximum allowable)7 20% 20%7 50% (50% maximum allowable)7
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 10%7 50% (50% maximum allowable)7 $250 copay 20%7 50% (50% maximum allowable)7
($250 deductible per calendar year, PPO and OON combined)8 ($250 deductible per calendar year, PPO and OON combined)9
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
10%7 50% ($250 maximum allowable/day)7
Days 1–10: Covered in full Days 11–100: $25/day
20%7 50% ($250 maximum allowable/day)7
($250 deductible per calendar year, PPO and OON combined)9 ($250 deductible per calendar year, PPO and OON combined)8
Emergency servicesProfessional services
Covered in full
10%
Covered in full
20%
50%
Emergency room facility (copay waived if admitted)
$100 copay $100 copay + 10% $100 copay $100 copay + 20% $100 + 50%
Urgent care facility $50 copay $50 copay + 10% $50 copay $50 copay + 20% $50 + 50%
Ambulance services (ground and air) $100 copay $50 copay + 10%7 $50 copay + 50%7 $100 copay $50 copay + 20%7 $50 copay + 50%7
Behavioral services10
Severe mental health (outpatient/inpatient)
$10 copay / Covered in full
Not covered
$20 copay / $250/day (3-day copay max/admit)
Not covered
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits per calendar year) / Covered in full (30 days per calendar year)
Not covered $30 copay (20 visits per calendar year) / $250/day (3-day copay max/admit) (30 days per calendar year)
Not covered
Chemical dependency rehabilitation (outpatient/inpatient)
$30 copay (20 visits per calendar year) / Covered in full (30 days per calendar year)
Not covered Not covered / Not covered Not covered
Acute care detoxification Covered in full Not covered $250 copay/day (3-day copay max/admit)
Not covered
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50%7 ($2,000 maximum per calendar year,
PPO and OON combined)
50% ($2,000 maximum per calendar year)
50%7 ($2,000 maximum per calendar year,
PPO and OON combined)
Orthotics Covered in full 10%7 50%7 Covered in full 20%7 50%7
Prosthetics Covered in full 10%7 50%7 Covered in full 20%7 50%7
Diabetic supplies 20% 20%7 50%7 20% 20%7 50%7
Chiropractic services11 $10 copay $20 copay (12 visits per calendar year)
Not covered $20 copay $30 copay (12 visits per calendar year)
Not covered
Acupuncture11 $10 copay Not covered $20 copay Not covered Not covered
Prescription drug coverage12
Calendar year deductible (per member) No deductible
No deductible
$100
No deductible
No deductible
$100
Prescription drugs (up to a 30-day supply)13
$10 / $25 / $50 50% $15 / $30 / $50 50%

21
PO
SP
OS
Plan footnotes found on pages 50–53.
Benefit description1 POS 10 (1FB) POS 20 (1FC)
Plan maximumsCalendar year deductible
HMO PPO2 Out-of-network3.4 HMO PPO2 Out-of-network3.4
No deductible
$250 single / $500 family
$500 single / $1,000 family
No deductible
$500 single / $1,000 family
$1,000 single / $2,000 family
Out-of-pocket maximum $1,500 single / $3,000 family $3,000 single / 2 per family $6,000 single / 2 per family $2,000 single / $4,000 family $3,500 single / 2 per family $7,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$10 copay
$20 copay
50%
$20 copay
$30 copay
50%
Preventive care services5 Covered in full Covered in full Not covered Covered in full Covered in full Not covered
X-ray and laboratory procedures Covered in full 10% 50% Covered in full 20%7 50%7
Rehabilitation therapy6 $10 copay 10% 50% $20 copay 20%7 50%7
(12 visits per calendar year, PPO and OON combined) (12 visits per calendar year, PPO and OON combined)
Self-injectable drugs 30% 30% 50% 30% 30%7 50%7
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
10%7
50% ($600 maximum allowable/day)7
$250 copay/day (3-day copay maximum)
20%7
50% ($600 maximum allowable/day)7
($250 deductible per calendar year, PPO and OON combined)8 ($250 deductible per calendar year, PPO and OON combined)8
Outpatient facility services (other than surgery)
Covered in full 10%7 50% (50% maximum allowable)7 20% 20%7 50% (50% maximum allowable)7
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 10%7 50% (50% maximum allowable)7 $250 copay 20%7 50% (50% maximum allowable)7
($250 deductible per calendar year, PPO and OON combined)8 ($250 deductible per calendar year, PPO and OON combined)9
Skilled nursing facility Days 1–10: Covered in full Days 11–100: $25/day
10%7 50% ($250 maximum allowable/day)7
Days 1–10: Covered in full Days 11–100: $25/day
20%7 50% ($250 maximum allowable/day)7
($250 deductible per calendar year, PPO and OON combined)9 ($250 deductible per calendar year, PPO and OON combined)8
Emergency servicesProfessional services
Covered in full
10%
Covered in full
20%
50%
Emergency room facility (copay waived if admitted)
$100 copay $100 copay + 10% $100 copay $100 copay + 20% $100 + 50%
Urgent care facility $50 copay $50 copay + 10% $50 copay $50 copay + 20% $50 + 50%
Ambulance services (ground and air) $100 copay $50 copay + 10%7 $50 copay + 50%7 $100 copay $50 copay + 20%7 $50 copay + 50%7
Behavioral services10
Severe mental health (outpatient/inpatient)
$10 copay / Covered in full
Not covered
$20 copay / $250/day (3-day copay max/admit)
Not covered
Non-severe mental health (outpatient/inpatient)
$30 copay (20 visits per calendar year) / Covered in full (30 days per calendar year)
Not covered $30 copay (20 visits per calendar year) / $250/day (3-day copay max/admit) (30 days per calendar year)
Not covered
Chemical dependency rehabilitation (outpatient/inpatient)
$30 copay (20 visits per calendar year) / Covered in full (30 days per calendar year)
Not covered Not covered / Not covered Not covered
Acute care detoxification Covered in full Not covered $250 copay/day (3-day copay max/admit)
Not covered
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50%7 ($2,000 maximum per calendar year,
PPO and OON combined)
50% ($2,000 maximum per calendar year)
50%7 ($2,000 maximum per calendar year,
PPO and OON combined)
Orthotics Covered in full 10%7 50%7 Covered in full 20%7 50%7
Prosthetics Covered in full 10%7 50%7 Covered in full 20%7 50%7
Diabetic supplies 20% 20%7 50%7 20% 20%7 50%7
Chiropractic services11 $10 copay $20 copay (12 visits per calendar year)
Not covered $20 copay $30 copay (12 visits per calendar year)
Not covered
Acupuncture11 $10 copay Not covered $20 copay Not covered Not covered
Prescription drug coverage12
Calendar year deductible (per member) No deductible
No deductible
$100
No deductible
No deductible
$100
Prescription drugs (up to a 30-day supply)13
$10 / $25 / $50 50% $15 / $30 / $50 50%

22
PPO PortfolioBenefit description1 PPO 10 PPO 15
Plan maximumsCalendar year deductible
Standard (1FN) Value (1KK) Standard (5QH) Value (5QJ)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
No deductible
$500 single / $1,000 family
$1,000 single / $2,000 family
$2,000 single / $4,000 family
$250 single / $500 family
$500 single / $1,000 family
$750 single / $1,500 family
$1,500 single / $3,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$2,500 single / 2 per family
$5,000 single / 2 per family
$2,500 single / 2 per family
$5,000 single / 2 per family
$3,000 single / 2 per family
$6,000 single / 2 per family
$4,000 single / 2 per family
$8,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$10 copay
40%
$10 copay
40%
$15 copay
50%
$15 copay
50%
Specialist consultation $10 copay 40% $10 copay 40% $25 copay 50% $25 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 10% 40% 20% 40% 15% 50% 25% 50%
Rehabilitation therapy5,6 10% 40% 20% 40% 15% 50% 25% 50%(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
10%
40%
20%
40%
15%
50% ($600 maximum allowable per day)
25%
50%
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
10% 40% 20% 40% 15% 50% 25% 50%
Outpatient surgery (hospital or outpatient surgery center charges only)
10% 40% 20% 40% 15% 50% 25% 50%
Skilled nursing facility 10% 40% ($250 maximum allowable per day)
20% 40% ($250 maximum allowable per day)
15% 50% ($250 maximum allowable per day)
25% 50% ($250 maximum allowable per day)
Emergency servicesProfessional services
$10 copay
$10 copay
$15 copay
$15 copay
Emergency room facility (copay waived if admitted)
$100 copay + 10% $100 copay + 20% $200 copay + 15% $250 copay + 25%
Urgent care facility $50 copay + 10% $50 copay + 20% $50 copay + 15% $50 copay + 25%
Ambulance services (ground and air)5 $50 copay + 10% $50 copay + 40% $50 copay + 20% $50 copay + 40% $50 copay + 15% $50 copay + 50% $50 copay + 25% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$10 copay / 10%
40%
$10 copay / 20%
40%
$15 copay / 15%
50%
$15 copay / 25%
50%
Non-severe mental health (outpatient/inpatient)9
10% 40% 20% 40% 15% 50% 25% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
10% 40% 20% 40% 15% 50% 25% 50%
Acute care detoxification 10% 40% 10% 40% 15% 50% 25% 50%($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)
Other servicesDurable medical equipment5
10%
40%
20%
40%
15%
50%
25%
50%
($3,000 maximum per calendar year, PPO and OON combined)
($3,000 maximum per calendar year, PPO and OON combined)
($3,000 maximum per calendar year, PPO and OON combined)
($3,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 10% 40% 20% 40% 15% 50% 25% 50%
Diabetic supplies 10% 40% 20% 40% 15% 50% 25% 50%
Chiropractic services $10 copay (12 visits per calendar year)
Not covered $10 copay (12 visits per calendar year)
Not covered $15 copay (12 visits per calendar year)
Not covered $15 copay (12 visits per calendar year)
Not covered
Acupuncture 10% 40% 20% 40% 15% 50% 25% 50%(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$100 brand deductible
$100
No deductible
$100
$100 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$10 / $25 / $50 50% $10 / $25 / $50 50% $10 / $25 / $50 50% $10 / $25 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered
Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans.

23
PP
O
Plan footnotes found on pages 50–53.
Benefit description1 PPO 10 PPO 15
Plan maximumsCalendar year deductible
Standard (1FN) Value (1KK) Standard (5QH) Value (5QJ)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
No deductible
$500 single / $1,000 family
$1,000 single / $2,000 family
$2,000 single / $4,000 family
$250 single / $500 family
$500 single / $1,000 family
$750 single / $1,500 family
$1,500 single / $3,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$2,500 single / 2 per family
$5,000 single / 2 per family
$2,500 single / 2 per family
$5,000 single / 2 per family
$3,000 single / 2 per family
$6,000 single / 2 per family
$4,000 single / 2 per family
$8,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$10 copay
40%
$10 copay
40%
$15 copay
50%
$15 copay
50%
Specialist consultation $10 copay 40% $10 copay 40% $25 copay 50% $25 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 10% 40% 20% 40% 15% 50% 25% 50%
Rehabilitation therapy5,6 10% 40% 20% 40% 15% 50% 25% 50%(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
10%
40%
20%
40%
15%
50% ($600 maximum allowable per day)
25%
50%
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
10% 40% 20% 40% 15% 50% 25% 50%
Outpatient surgery (hospital or outpatient surgery center charges only)
10% 40% 20% 40% 15% 50% 25% 50%
Skilled nursing facility 10% 40% ($250 maximum allowable per day)
20% 40% ($250 maximum allowable per day)
15% 50% ($250 maximum allowable per day)
25% 50% ($250 maximum allowable per day)
Emergency servicesProfessional services
$10 copay
$10 copay
$15 copay
$15 copay
Emergency room facility (copay waived if admitted)
$100 copay + 10% $100 copay + 20% $200 copay + 15% $250 copay + 25%
Urgent care facility $50 copay + 10% $50 copay + 20% $50 copay + 15% $50 copay + 25%
Ambulance services (ground and air)5 $50 copay + 10% $50 copay + 40% $50 copay + 20% $50 copay + 40% $50 copay + 15% $50 copay + 50% $50 copay + 25% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$10 copay / 10%
40%
$10 copay / 20%
40%
$15 copay / 15%
50%
$15 copay / 25%
50%
Non-severe mental health (outpatient/inpatient)9
10% 40% 20% 40% 15% 50% 25% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
10% 40% 20% 40% 15% 50% 25% 50%
Acute care detoxification 10% 40% 10% 40% 15% 50% 25% 50%($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)
Other servicesDurable medical equipment5
10%
40%
20%
40%
15%
50%
25%
50%
($3,000 maximum per calendar year, PPO and OON combined)
($3,000 maximum per calendar year, PPO and OON combined)
($3,000 maximum per calendar year, PPO and OON combined)
($3,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 10% 40% 20% 40% 15% 50% 25% 50%
Diabetic supplies 10% 40% 20% 40% 15% 50% 25% 50%
Chiropractic services $10 copay (12 visits per calendar year)
Not covered $10 copay (12 visits per calendar year)
Not covered $15 copay (12 visits per calendar year)
Not covered $15 copay (12 visits per calendar year)
Not covered
Acupuncture 10% 40% 20% 40% 15% 50% 25% 50%(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$100 brand deductible
$100
No deductible
$100
$100 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$10 / $25 / $50 50% $10 / $25 / $50 50% $10 / $25 / $50 50% $10 / $25 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered

24
PPO PortfolioBenefit description1 PPO 20 PPO 25
Plan maximumsCalendar year deductible
Standard (1FP) Value (1FS) Standard (5QD) Value (5QE)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
$250 single / $500 family
$500 single / $1,000 family
$1,250 single / $2,500 family
$2,500 single / $5,000 family
$500 single / $1,000 family
$1,000 single / $2,000 family
$1,000 single / $2,000 family
$2,000 single / $4,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$3,000 single / 2 per family $6,000 single / 2 per family $3,500 single / 2 per family $7,000 single / 2 per family $3,500 single / 2 per family $7,000 single / 2 per family $5,000 single / 2 per family $10,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$20 copay
50%
$20 copay
50%
$25 copay
50% $25 copay
50%
Specialist consultation $20 copay 50% $20 copay 50% $35 copay 50% $35 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 10% 50% 20% 50% 25% 50% 35% 50%
Rehabilitation therapy5,6 10% 50% 20% 50% 25% 50% 35% 50%(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
10%
50% ($600 maximum allowable/day)
20%
50% ($600 maximum allowable/day)
25% 50% ($600 maximum allowable/day)
35% 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
10% 50% (50% maximum allowable)
20% 50% (50% maximum allowable)
25% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
10% 50% (50% maximum allowable)
20% 50% (50% maximum allowable)
25% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 10% 50% ($250 maximum allowable/day)
20% 50% ($250 maximum allowable/day)
25% 50% ($250 maximum allowable/day)
35% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$20 copay
$20 copay $25 copay $25 copay
Emergency room facility (copay waived if admitted)
$100 copay + 10% $100 copay + 20% $200 copay + 25% $250 copay + 35%
Urgent care facility $50 copay + 10% $50 copay + 20% $50 copay + 25% $50 copay + 35%
Ambulance services (ground and air)5 $50 copay + 10% $50 copay + 50% $50 copay + 20% $50 copay + 50% $50 copay + 25% $50 copay + 50% $50 copay + 35% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$20 copay / 10%
50% / 50% ($600 maximum allowable/day)
$20 copay / 20%
50% / 50% ($600 maximum allowable/day)
$25 copay / 25%
50% / 50% ($600 maximum allowable/day)
$25 copay / 35% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
10% 50% 20% 50% 25% 50% 35% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
10% 50% 20% 50% 25% 50% 35% 50%
Acute care detoxification 10% 50% 20% 50% 25% 50% 35% 50%($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
10%
50%
20%
50%
25%
50%
35%
50%
($2,000 maximum per calendar year, PPO and OON combined)
($2,000 maximum per calendar year, PPO and OON combined)
($2,000 maximum per calendar year, PPO and OON combined)
($2,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 10% 50% 20% 50% 25% 50% 35% 50%
Diabetic supplies 10% 50% 20% 50% 25% 50% 35% 50%
Chiropractic services $20 copay (12 visits per calendar year)
Not covered $20 copay (12 visits per calendar year)
Not covered $25 copay (12 visits per calendar year)
Not covered $25 copay (12 visits per calendar year)
Not covered
Acupuncture 10% 50% 20% 50% 25% 50% 35% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$150 brand deductible
$100 No deductible
$100
$150 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered
Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans.

25
PP
O
Benefit description1 PPO 20 PPO 25
Plan maximumsCalendar year deductible
Standard (1FP) Value (1FS) Standard (5QD) Value (5QE)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
$250 single / $500 family
$500 single / $1,000 family
$1,250 single / $2,500 family
$2,500 single / $5,000 family
$500 single / $1,000 family
$1,000 single / $2,000 family
$1,000 single / $2,000 family
$2,000 single / $4,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$3,000 single / 2 per family $6,000 single / 2 per family $3,500 single / 2 per family $7,000 single / 2 per family $3,500 single / 2 per family $7,000 single / 2 per family $5,000 single / 2 per family $10,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$20 copay
50%
$20 copay
50%
$25 copay
50% $25 copay
50%
Specialist consultation $20 copay 50% $20 copay 50% $35 copay 50% $35 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 10% 50% 20% 50% 25% 50% 35% 50%
Rehabilitation therapy5,6 10% 50% 20% 50% 25% 50% 35% 50%(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
10%
50% ($600 maximum allowable/day)
20%
50% ($600 maximum allowable/day)
25% 50% ($600 maximum allowable/day)
35% 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
10% 50% (50% maximum allowable)
20% 50% (50% maximum allowable)
25% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
10% 50% (50% maximum allowable)
20% 50% (50% maximum allowable)
25% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 10% 50% ($250 maximum allowable/day)
20% 50% ($250 maximum allowable/day)
25% 50% ($250 maximum allowable/day)
35% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$20 copay
$20 copay $25 copay $25 copay
Emergency room facility (copay waived if admitted)
$100 copay + 10% $100 copay + 20% $200 copay + 25% $250 copay + 35%
Urgent care facility $50 copay + 10% $50 copay + 20% $50 copay + 25% $50 copay + 35%
Ambulance services (ground and air)5 $50 copay + 10% $50 copay + 50% $50 copay + 20% $50 copay + 50% $50 copay + 25% $50 copay + 50% $50 copay + 35% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$20 copay / 10%
50% / 50% ($600 maximum allowable/day)
$20 copay / 20%
50% / 50% ($600 maximum allowable/day)
$25 copay / 25%
50% / 50% ($600 maximum allowable/day)
$25 copay / 35% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
10% 50% 20% 50% 25% 50% 35% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
10% 50% 20% 50% 25% 50% 35% 50%
Acute care detoxification 10% 50% 20% 50% 25% 50% 35% 50%($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
10%
50%
20%
50%
25%
50%
35%
50%
($2,000 maximum per calendar year, PPO and OON combined)
($2,000 maximum per calendar year, PPO and OON combined)
($2,000 maximum per calendar year, PPO and OON combined)
($2,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 10% 50% 20% 50% 25% 50% 35% 50%
Diabetic supplies 10% 50% 20% 50% 25% 50% 35% 50%
Chiropractic services $20 copay (12 visits per calendar year)
Not covered $20 copay (12 visits per calendar year)
Not covered $25 copay (12 visits per calendar year)
Not covered $25 copay (12 visits per calendar year)
Not covered
Acupuncture 10% 50% 20% 50% 25% 50% 35% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$150 brand deductible
$100 No deductible
$100
$150 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered
Plan footnotes found on pages 50–53.

26
PPO PortfolioBenefit description1 PPO 30 PPO 35
Plan maximumsCalendar year deductible
Standard (1FQ) Value (1FT) Standard (5QG) Value (5QB)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
$500 single / $1,000 family
$1,000 single / $2,000 family
$1,500 single / $3,000 family
$3,000 single / $6,000 family
$750 single / $1,500 family
$1,500 single / $3,000 family
$1,250 single / $2,500 family
$2,500 single / $5,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$3,500 single / 2 per family $7,000 single / 2 per family $4,500 single / 2 per family $9,000 single / 2 per family $4,000 single / 2 per family $8,000 single / 2 per family $6,000 single / 2 per family $12,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$30 copay 50%
$30 copay 50%
$35 copay
50%
$35 copay
50%
Specialist consultation $30 copay 50% $30 copay 50% $45 copay 50% $45 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 20% 50% 30% 50% 35% 50% 45% 50%
Rehabilitation therapy5,6 20% 50% 30% 50% 35% 50% 45% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
20% 50% ($600 maximum allowable/day)
30%
50% ($600 maximum allowable/day)
35%
50% ($600 maximum allowable/day)
45%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 20% 50% ($250 maximum allowable/day)
30% 50% ($250 maximum allowable/day)
35% 50% ($250 maximum allowable/day)
45% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services $30 copay $30 copay $35 copay $35 copay
Emergency room facility (copay waived if admitted)
$100 copay + 20% $100 copay + 30% $200 copay + 35% $250 copay + 45%
Urgent care facility $50 copay + 20% $50 copay + 30% $50 copay + 35% $50 copay + 45%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 50% $50 copay + 30% $50 copay + 50% $50 copay + 35% $50 copay + 50% $50 copay + 45% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$30 copay / 20% 50% / 50% ($600 maximum allowable/day)
$30 copay / 30%
50% / 50% ($600 maximum allowable/day)
$35 copay / 35% 50% / 50% ($600 maximum allowable/day)
$35 copay / 45% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
20% 50% 30% 50% 35% 50% 45% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
20% 50% 30% 50% 35% 50% 45% 50%
Acute care detoxification 20% 50% 30% 50% 35% 50% 45% 50%($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
20%
50%
30%
50%
35%
50%
45%
50%
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 20% 50% 30% 50% 35% 50% 45% 50%
Diabetic supplies 20% 50% 30% 50% 35% 50% 45% 50%
Chiropractic services $30 copay (12 visits per calendar year)
Not covered $30 copay (12 visits per calendar year)
Not covered $35 copay (12 visits per calendar year)
Not covered $35 copay (12 visits per calendar year)
Not covered
Acupuncture 20% 50% 30% 50% 35% 50% 45% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$200 brand deductible
$100
No deductible
$100
$200 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered
Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans.

27
PP
O
Benefit description1 PPO 30 PPO 35
Plan maximumsCalendar year deductible
Standard (1FQ) Value (1FT) Standard (5QG) Value (5QB)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
$500 single / $1,000 family
$1,000 single / $2,000 family
$1,500 single / $3,000 family
$3,000 single / $6,000 family
$750 single / $1,500 family
$1,500 single / $3,000 family
$1,250 single / $2,500 family
$2,500 single / $5,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$3,500 single / 2 per family $7,000 single / 2 per family $4,500 single / 2 per family $9,000 single / 2 per family $4,000 single / 2 per family $8,000 single / 2 per family $6,000 single / 2 per family $12,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$30 copay 50%
$30 copay 50%
$35 copay
50%
$35 copay
50%
Specialist consultation $30 copay 50% $30 copay 50% $45 copay 50% $45 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 20% 50% 30% 50% 35% 50% 45% 50%
Rehabilitation therapy5,6 20% 50% 30% 50% 35% 50% 45% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
20% 50% ($600 maximum allowable/day)
30%
50% ($600 maximum allowable/day)
35%
50% ($600 maximum allowable/day)
45%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
35% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 20% 50% ($250 maximum allowable/day)
30% 50% ($250 maximum allowable/day)
35% 50% ($250 maximum allowable/day)
45% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services $30 copay $30 copay $35 copay $35 copay
Emergency room facility (copay waived if admitted)
$100 copay + 20% $100 copay + 30% $200 copay + 35% $250 copay + 45%
Urgent care facility $50 copay + 20% $50 copay + 30% $50 copay + 35% $50 copay + 45%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 50% $50 copay + 30% $50 copay + 50% $50 copay + 35% $50 copay + 50% $50 copay + 45% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$30 copay / 20% 50% / 50% ($600 maximum allowable/day)
$30 copay / 30%
50% / 50% ($600 maximum allowable/day)
$35 copay / 35% 50% / 50% ($600 maximum allowable/day)
$35 copay / 45% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
20% 50% 30% 50% 35% 50% 45% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
20% 50% 30% 50% 35% 50% 45% 50%
Acute care detoxification 20% 50% 30% 50% 35% 50% 45% 50%($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
20%
50%
30%
50%
35%
50%
45%
50%
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 20% 50% 30% 50% 35% 50% 45% 50%
Diabetic supplies 20% 50% 30% 50% 35% 50% 45% 50%
Chiropractic services $30 copay (12 visits per calendar year)
Not covered $30 copay (12 visits per calendar year)
Not covered $35 copay (12 visits per calendar year)
Not covered $35 copay (12 visits per calendar year)
Not covered
Acupuncture 20% 50% 30% 50% 35% 50% 45% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$200 brand deductible
$100
No deductible
$100
$200 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered
Plan footnotes found on pages 50–53.
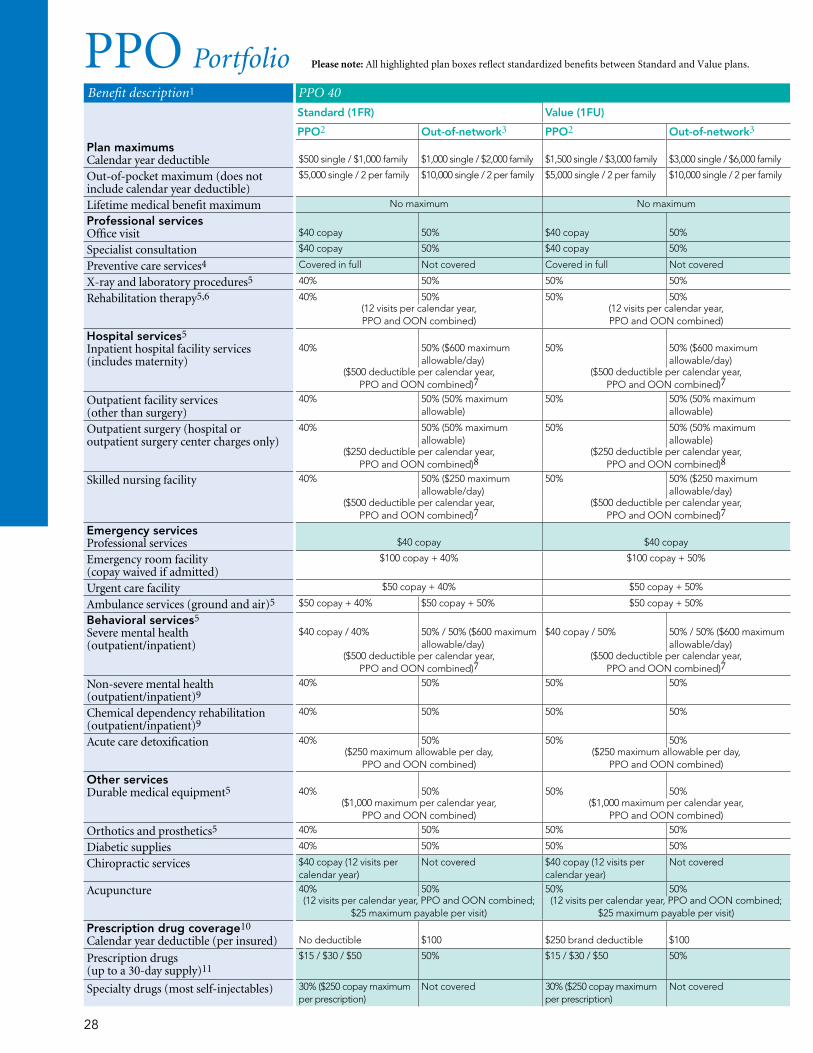
28
PPO PortfolioBenefit description1 PPO 40 PPO 45
Standard (1FR) Value (1FU) Standard (5QF) Value (5QC)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
Plan maximumsCalendar year deductible
$500 single / $1,000 family
$1,000 single / $2,000 family $1,500 single / $3,000 family
$3,000 single / $6,000 family
$1,000 single / $2,000 family
$2,000 single / $4,000 family
$1,500 single / $3,000 family
$3,000 single / $6,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$5,000 single / 2 per family $10,000 single / 2 per family $5,000 single / 2 per family $10,000 single / 2 per family $5,000 single / 2 per family $10,000 single / 2 per family $7,000 single / 2 per family $14,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$40 copay 50%
$40 copay 50%
$45 copay
50%
$45 copay
50%
Specialist consultation $40 copay 50% $40 copay 50% $55 copay 50% $55 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 40% 50% 50% 50% 45% 50% 50% 50%
Rehabilitation therapy5,6 40% 50% 50% 50% 45% 50% 50% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
40% 50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
45%
50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
40% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
40% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 40% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
45% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services $40 copay $40 copay $45 copay $45 copay
Emergency room facility (copay waived if admitted)
$100 copay + 40% $100 copay + 50% $200 copay + 45% $250 copay + 50%
Urgent care facility $50 copay + 40% $50 copay + 50% $50 copay + 45% $50 copay + 50%
Ambulance services (ground and air)5 $50 copay + 40% $50 copay + 50% $50 copay + 50% $50 copay + 45% $50 copay + 50% $50 copay + 50% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$40 copay / 40% 50% / 50% ($600 maximum allowable/day)
$40 copay / 50%
50% / 50% ($600 maximum allowable/day)
$45 copay / 45% 50% / 50% ($600 maximum allowable/day)
$45 copay / 50% 50% / 50% ($600 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
40% 50% 50% 50% 45% 50% 50% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
40% 50% 50% 50% 45% 50% 50% 50%
Acute care detoxification 40% 50% 50% 50% 45% 50% 50% 50%($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)
Other servicesDurable medical equipment5
40%
50%
50%
50%
45%
50%
50%
50%
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 40% 50% 50% 50% 45% 50% 50% 50%
Diabetic supplies 40% 50% 50% 50% 45% 50% 50% 50%
Chiropractic services $40 copay (12 visits per calendar year)
Not covered $40 copay (12 visits per calendar year)
Not covered $45 copay (12 visits per calendar year)
Not covered $45 copay (12 visits per calendar year)
Not covered
Acupuncture 40% 50% 50% 50% 45% 50% 50% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$250 brand deductible
$100
No deductible
$100
$250 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered
Please note: All highlighted plan boxes reflect standardized benefits between Standard and Value plans.

29
PP
O
Plan footnotes found on pages 50–53.
Benefit description1 PPO 40 PPO 45
Standard (1FR) Value (1FU) Standard (5QF) Value (5QC)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
Plan maximumsCalendar year deductible
$500 single / $1,000 family
$1,000 single / $2,000 family $1,500 single / $3,000 family
$3,000 single / $6,000 family
$1,000 single / $2,000 family
$2,000 single / $4,000 family
$1,500 single / $3,000 family
$3,000 single / $6,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$5,000 single / 2 per family $10,000 single / 2 per family $5,000 single / 2 per family $10,000 single / 2 per family $5,000 single / 2 per family $10,000 single / 2 per family $7,000 single / 2 per family $14,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit
$40 copay 50%
$40 copay 50%
$45 copay
50%
$45 copay
50%
Specialist consultation $40 copay 50% $40 copay 50% $55 copay 50% $55 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 40% 50% 50% 50% 45% 50% 50% 50%
Rehabilitation therapy5,6 40% 50% 50% 50% 45% 50% 50% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
40% 50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
45%
50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
40% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
40% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 40% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
45% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services $40 copay $40 copay $45 copay $45 copay
Emergency room facility (copay waived if admitted)
$100 copay + 40% $100 copay + 50% $200 copay + 45% $250 copay + 50%
Urgent care facility $50 copay + 40% $50 copay + 50% $50 copay + 45% $50 copay + 50%
Ambulance services (ground and air)5 $50 copay + 40% $50 copay + 50% $50 copay + 50% $50 copay + 45% $50 copay + 50% $50 copay + 50% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$40 copay / 40% 50% / 50% ($600 maximum allowable/day)
$40 copay / 50%
50% / 50% ($600 maximum allowable/day)
$45 copay / 45% 50% / 50% ($600 maximum allowable/day)
$45 copay / 50% 50% / 50% ($600 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
40% 50% 50% 50% 45% 50% 50% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
40% 50% 50% 50% 45% 50% 50% 50%
Acute care detoxification 40% 50% 50% 50% 45% 50% 50% 50%($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)($250 maximum allowable per day,
PPO and OON combined)
Other servicesDurable medical equipment5
40%
50%
50%
50%
45%
50%
50%
50%
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 40% 50% 50% 50% 45% 50% 50% 50%
Diabetic supplies 40% 50% 50% 50% 45% 50% 50% 50%
Chiropractic services $40 copay (12 visits per calendar year)
Not covered $40 copay (12 visits per calendar year)
Not covered $45 copay (12 visits per calendar year)
Not covered $45 copay (12 visits per calendar year)
Not covered
Acupuncture 40% 50% 50% 50% 45% 50% 50% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) No deductible
$100
$250 brand deductible
$100
No deductible
$100
$250 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered

30
PPO Portfolio Plan footnotes found on pages 50–53.
Benefit description1 Advantage PPO 35 (5ZQ) Advantage PPO 45 (5ZR)PPO2 Out-of-network3 PPO2 Out-of-network3
Plan maximumsCalendar year deductible $3,000 single / $6,000 family
$4,000 single / $8,000 family
Out-of-pocket maximum(includes calendar year deductible)
$6,500 single / 2 per family
$13,000 single / 2 per family
$8,000 single / 2 per family
$16,000 single / 2 per family
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit
$35 copay 50%
$45 copay 50%
Specialist consultation $45 copay 50% $55 copay 50%
Preventive care services4 Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 40% 50% 50% 50%
Rehabilitation therapy5,6 40% 50% 50% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
40% 50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
Outpatient facility services (other than surgery)
40% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
Outpatient surgery (hospital charges only)
40% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
Outpatient surgery (ambulatory surgery center charges only)
35% 50% (50% maximum allowable)
45% 50% (50% maximum allowable)
Skilled nursing facility 40% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
Emergency servicesProfessional services $35 copay $45 copay
Emergency room facility (copay waived if admitted)
$150 copay + 40% $150 copay + 50%
Urgent care facility $50 copay + 40% $50 copay + 50%
Ambulance services (ground and air)5 $50 copay + 40% $50 copay + 50% $50 copay + 50% $50 copay + 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$35 copay / 40% 50% / 50% ($600 maximum allowable/day)
$45 copay / 50%
50% / 50% ($600 maximum allowable/day)
Non-severe mental health (outpatient/inpatient)9
40% 50% 50% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
40% 50% 50% 50%
Acute care detoxification 40% 50% 50% 50%($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
40%
50%
50%
50%
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 40% 50% 50% 50%
Diabetic supplies 40% 50% 50% 50%
Chiropractic services $35 copay (12 visits per calendar year)
Not covered $45 copay (12 visits per calendar year)
Not covered
Acupuncture 40% 50% 50% 50%(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Brand name calendar year deductible (per insured)
$250 brand deductible
$100
$250 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription)
Not covered 30% ($250 copay maximum per prescription)
Not covered

31
Standard HSA Portfolio Plan footnotes found on pages 50–53.
Benefit description1 Standard HSA 4000 (1FJ)PPO2 Out-of-network3
Plan maximumsCalendar year deductible (For family coverage, the enrolled employee and dependents must collectively pay the family amount before Health Net begins to pay.)
$4,000 single (employee-only coverage) /$8,000 family (employee and dependent coverage)
Out-of-pocket maximum (includes deductible and copays)
$5,950 single (employee-only coverage) / $11,900 family (employee and dependent coverage)
$10,000 single (employee-only coverage) / $20,000 family (employee and dependent coverage)
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$0 copay (deductible not waived) 50%
Preventive care services4 Covered in full Not covered
X-ray and laboratory procedures5 0% 50%
Rehabilitation therapy5,6 0% 50%
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
0% 50% ($600 maximum allowable/day)
Outpatient facility services (other than surgery)
0% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
0% 50% (50% maximum allowable)
Skilled nursing facility 0% 50% ($250 maximum allowable/day)
Emergency servicesProfessional services $0 copay (deductible not waived)
50%
Emergency room facility 0% 50%
Urgent care facility 0% 50%
Ambulance services (ground and air)5 0% 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
0% 50% ($600 maximum allowable/day)
Non-severe mental health (outpatient/inpatient)7
0% 50%
Chemical dependency rehabilitation (outpatient/inpatient)7
0% 50%
Acute care detoxification 0% 50%
($250 maximum allowable/day)
Other servicesDurable medical equipment5
0%
50%
($2,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 0% 50%
Diabetic supplies 0% 50%
Chiropractic services $0 copay (deductible not waived, 12 visits per calendar year)
Not covered
Acupuncture 0% 50%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage8
Calendar year deductible (per insured) Subject to annual deductible
Prescription drugs (up to a 30-day supply)9
$10 / $25 / $50 50%
Specialty drugs (most self-injectables) 30% Not covered
STAN
DA
RD
HSA

32
Value HSA PortfolioBenefit description1 Value HSA 1500 (1FD) Value HSA 2500 (1FF) Value HSA 3500 (1FH) Value HSA 4500 (1FK)
Plan maximumsCalendar year deductible (For family coverage, the enrolled employee and dependents must collectively pay the family amount before Health Net begins to pay.)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
$1,500 single (employee-only coverage) /
$3,000 family (employee and dependent coverage)
$2,500 single (employee-only coverage) /
$5,000 family (employee and dependent coverage)
$3,500 single (employee-only coverage) /
$7,000 family (employee and dependent coverage)
$4,500 single (employee-only coverage) /
$9,000 family (employee and dependent coverage)
Out-of-pocket maximum (includes deductible)
$3,000 single (employee-only coverage) / $6,000 family (employee and dependent coverage)
$6,000 single (employee-only coverage) / $12,000 family (employee and dependent coverage)
$4,000 single (employee-only coverage) / $8,000 family (employee and dependent coverage)
$8,000 single (employee-only coverage) / $16,000 family (employee and dependent coverage)
$5,000 single (employee-only coverage) / $10,000 family (employee and dependent coverage)
$10,000 single (employee-only coverage) / $20,000 family (employee and dependent coverage)
$5,950 single (employee-only coverage) / $11,900 family (employee and dependent coverage)
$10,000 single (employee-only coverage) / $20,000 family (employee and dependent coverage)
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$10 copay (deductible not waived)
40% $20 copay (deductible not waived)
50% $30 copay (deductible not waived)
50%
$40 copay (deductible not waived)
50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 20% 40% 20% 50% 30% 50% 50% 50%
Rehabilitation therapy5,6 20% 40% 20% 50% 30% 50% 50% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
20% 40%
20%
50% ($600 maximum allowable/day)
30%
50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
20% 40% 20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 40% 20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 20% 40% ($250 maximum allowable/day)
20% 50% ($250 maximum allowable/day)
30% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$10 copay (deductible not waived)
40% $20 copay
(deductible not waived)
50% $30 copay
(deductible not waived)
50% $40 copay
(deductible not waived)
50%
Emergency room facility (copay waived if admitted)
$100 copay + 20% $100 + 40% $100 copay + 20% $100 + 50% $100 copay + 30% $100 + 50% $100 copay + 50%
Urgent care facility $50 copay + 20% $50 + 40% $50 copay + 20% $50 + 50% $50 copay + 30% $50 + 50% $50 copay + 50%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 40% $50 copay + 20% $50 copay + 50% $50 copay + 30% $50 copay + 50% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$10 copay / 20% 40% / 40%
$20 copay / 20%
50% / 50% ($600 maximum allowable/day)
$30 copay / 30% 50% / 50% ($600 maximum allowable/day)
$40 copay / 50% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
20% 40% 20% 50% 30% 50% 50% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
20% 40% 20% 50% 30% 50% 50% 50%
Acute care detoxification 20% 40% 20% 50% 30% 50% 50% 50%($250 maximum allowable/day) ($250 maximum allowable/day) ($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
20%
40%
20%
50%
30%
50%
50%
50%
($3,000 maximum per calendar year,PPO and OON combined)
($2,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 20% 40% 20% 50% 30% 50% 50% 50%
Diabetic supplies 20% 40% 20% 50% 30% 50% 50% 50%
Chiropractic services $10 copay (deductible not waived, 12 visits per calendar year)
Not covered $20 copay (deductible not waived, 12 visits per calendar year)
Not covered $30 copay (deductible not waived, 12 visits per calendar year)
Not covered $40 copay (deductible not waived, 12 visits per calendar year)
Not covered
Acupuncture 20% 40% 20% 50% 30% 50% 50% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured)
Subject to annual deductible
Subject to annual deductible
Subject to annual deductible
Subject to annual deductible
Prescription drugs (up to a 30-day supply)11
$10 / $25 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% Not covered 30% Not covered 30% Not covered 30% Not covered

33
Plan footnotes found on pages 50–53.
VA
LUE
HSA
Benefit description1 Value HSA 1500 (1FD) Value HSA 2500 (1FF) Value HSA 3500 (1FH) Value HSA 4500 (1FK)
Plan maximumsCalendar year deductible (For family coverage, the enrolled employee and dependents must collectively pay the family amount before Health Net begins to pay.)
PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3 PPO2 Out-of-network3
$1,500 single (employee-only coverage) /
$3,000 family (employee and dependent coverage)
$2,500 single (employee-only coverage) /
$5,000 family (employee and dependent coverage)
$3,500 single (employee-only coverage) /
$7,000 family (employee and dependent coverage)
$4,500 single (employee-only coverage) /
$9,000 family (employee and dependent coverage)
Out-of-pocket maximum (includes deductible)
$3,000 single (employee-only coverage) / $6,000 family (employee and dependent coverage)
$6,000 single (employee-only coverage) / $12,000 family (employee and dependent coverage)
$4,000 single (employee-only coverage) / $8,000 family (employee and dependent coverage)
$8,000 single (employee-only coverage) / $16,000 family (employee and dependent coverage)
$5,000 single (employee-only coverage) / $10,000 family (employee and dependent coverage)
$10,000 single (employee-only coverage) / $20,000 family (employee and dependent coverage)
$5,950 single (employee-only coverage) / $11,900 family (employee and dependent coverage)
$10,000 single (employee-only coverage) / $20,000 family (employee and dependent coverage)
Lifetime medical benefit maximum No maximum No maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$10 copay (deductible not waived)
40% $20 copay (deductible not waived)
50% $30 copay (deductible not waived)
50%
$40 copay (deductible not waived)
50%
Preventive care services4 Covered in full Not covered Covered in full Not covered Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 20% 40% 20% 50% 30% 50% 50% 50%
Rehabilitation therapy5,6 20% 40% 20% 50% 30% 50% 50% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
20% 40%
20%
50% ($600 maximum allowable/day)
30%
50% ($600 maximum allowable/day)
50%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
20% 40% 20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 40% 20% 50% (50% maximum allowable)
30% 50% (50% maximum allowable)
50% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 20% 40% ($250 maximum allowable/day)
20% 50% ($250 maximum allowable/day)
30% 50% ($250 maximum allowable/day)
50% 50% ($250 maximum allowable/day)
($500 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$10 copay (deductible not waived)
40% $20 copay
(deductible not waived)
50% $30 copay
(deductible not waived)
50% $40 copay
(deductible not waived)
50%
Emergency room facility (copay waived if admitted)
$100 copay + 20% $100 + 40% $100 copay + 20% $100 + 50% $100 copay + 30% $100 + 50% $100 copay + 50%
Urgent care facility $50 copay + 20% $50 + 40% $50 copay + 20% $50 + 50% $50 copay + 30% $50 + 50% $50 copay + 50%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 40% $50 copay + 20% $50 copay + 50% $50 copay + 30% $50 copay + 50% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$10 copay / 20% 40% / 40%
$20 copay / 20%
50% / 50% ($600 maximum allowable/day)
$30 copay / 30% 50% / 50% ($600 maximum allowable/day)
$40 copay / 50% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
($500 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
20% 40% 20% 50% 30% 50% 50% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
20% 40% 20% 50% 30% 50% 50% 50%
Acute care detoxification 20% 40% 20% 50% 30% 50% 50% 50%($250 maximum allowable/day) ($250 maximum allowable/day) ($250 maximum allowable/day,
PPO and OON combined)($250 maximum allowable/day,
PPO and OON combined)
Other servicesDurable medical equipment5
20%
40%
20%
50%
30%
50%
50%
50%
($3,000 maximum per calendar year,PPO and OON combined)
($2,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 20% 40% 20% 50% 30% 50% 50% 50%
Diabetic supplies 20% 40% 20% 50% 30% 50% 50% 50%
Chiropractic services $10 copay (deductible not waived, 12 visits per calendar year)
Not covered $20 copay (deductible not waived, 12 visits per calendar year)
Not covered $30 copay (deductible not waived, 12 visits per calendar year)
Not covered $40 copay (deductible not waived, 12 visits per calendar year)
Not covered
Acupuncture 20% 40% 20% 50% 30% 50% 50% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured)
Subject to annual deductible
Subject to annual deductible
Subject to annual deductible
Subject to annual deductible
Prescription drugs (up to a 30-day supply)11
$10 / $25 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% Not covered 30% Not covered 30% Not covered 30% Not covered

34
HRA PortfolioBenefit description1 HRA 3000 (5UG) HRA 5000 (5UH)
PPO2 Out-of-network3 PPO2 Out-of-network3
All benefits including Rx are subject to the deductible
Plan maximumsCalendar year deductible (For family coverage, the enrolled employee and dependents must collectively pay the family amount before Health Net begins to pay.)
$3,000 single (employee-only coverage) /
$6,000 family (employee and dependent coverage)
$5,000 single (employee-only coverage) /
$10,000 family (employee and dependent coverage)
Out-of-pocket maximum (includes deductibles, coinsurance and copays)
$4,000 single (employee-only coverage) / $8,000 family (employee and dependent coverage)
$6,000 single (employee-only coverage) / $12,000 family (employee and dependent coverage)
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
50% (deductible not waived) Not covered 50% (deductible not waived)
Not covered
Preventive care services4 Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 20% 40% 20% 40%
Rehabilitation therapy5,6 20% 40% 20% 40%
(12 visits per calendar year, PPO and OON combined) (12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity) 20% 40% ($600 maximum allowable/day)
20%
40% ($600 maximum allowable/day)
Outpatient facility services (other than surgery) 20% 40% (50% maximum allowable) 20% 40% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 40% (50% maximum allowable) 20% 40% (50% maximum allowable)
Skilled nursing facility 20% 40% ($250 maximum allowable/day) 20% 40% ($250 maximum allowable/day)
Emergency servicesProfessional services
$10 copay (deductible not waived)
40% $10 copay (deductible not waived)
40%
Emergency room facility (copay waived if admitted) $100 copay + 20% $100 + 40% $100 copay + 20% $100 + 40%
Urgent care facility $50 copay + 20% $50 + 40% $50 copay + 20% $50 + 40%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 40% $50 copay + 20% $50 copay + 40%
Behavioral services5
Severe mental health (outpatient/inpatient) 20% Not covered 20% Not covered
Non-severe mental health (outpatient/inpatient) 20%7 Not covered 20%7 Not covered
Chemical dependency rehabilitation (outpatient/inpatient)
20%7 Not covered 20%7 Not covered
Acute care detoxification 20% ($250 maximum allowable/day) Not covered 20% ($250 maximum allowable/day) Not covered
Other servicesDurable medical equipment and orthotics5
20%
40%
20%
40%
($3,000 maximum per calendar year, PPO and OON combined) ($3,000 maximum per calendar year, PPO and OON combined)
Diabetic supplies 20% 40% 20% 40%
Chiropractic services $20 (12 visits per calendar year) Not covered $20 (12 visits per calendar year) Not covered
Acupuncture 20% 40% 20% 40%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage8 Subject to calendar year medical deductible (per insured) Subject to calendar year medical deductible (per insured)
Prescription drugs (up to a 30-day supply)9 $10 / $25 / $50 50% $10 / $25 / $50 50%
Specialty drugs (most self-injectables) 30% Not covered 30% Not covered

35
Plan footnotes found on pages 50–53.
Benefit description1 HRA 3000 (5UG) HRA 5000 (5UH)PPO2 Out-of-network3 PPO2 Out-of-network3
All benefits including Rx are subject to the deductible
Plan maximumsCalendar year deductible (For family coverage, the enrolled employee and dependents must collectively pay the family amount before Health Net begins to pay.)
$3,000 single (employee-only coverage) /
$6,000 family (employee and dependent coverage)
$5,000 single (employee-only coverage) /
$10,000 family (employee and dependent coverage)
Out-of-pocket maximum (includes deductibles, coinsurance and copays)
$4,000 single (employee-only coverage) / $8,000 family (employee and dependent coverage)
$6,000 single (employee-only coverage) / $12,000 family (employee and dependent coverage)
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
50% (deductible not waived) Not covered 50% (deductible not waived)
Not covered
Preventive care services4 Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 20% 40% 20% 40%
Rehabilitation therapy5,6 20% 40% 20% 40%
(12 visits per calendar year, PPO and OON combined) (12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity) 20% 40% ($600 maximum allowable/day)
20%
40% ($600 maximum allowable/day)
Outpatient facility services (other than surgery) 20% 40% (50% maximum allowable) 20% 40% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 40% (50% maximum allowable) 20% 40% (50% maximum allowable)
Skilled nursing facility 20% 40% ($250 maximum allowable/day) 20% 40% ($250 maximum allowable/day)
Emergency servicesProfessional services
$10 copay (deductible not waived)
40% $10 copay (deductible not waived)
40%
Emergency room facility (copay waived if admitted) $100 copay + 20% $100 + 40% $100 copay + 20% $100 + 40%
Urgent care facility $50 copay + 20% $50 + 40% $50 copay + 20% $50 + 40%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 40% $50 copay + 20% $50 copay + 40%
Behavioral services5
Severe mental health (outpatient/inpatient) 20% Not covered 20% Not covered
Non-severe mental health (outpatient/inpatient) 20%7 Not covered 20%7 Not covered
Chemical dependency rehabilitation (outpatient/inpatient)
20%7 Not covered 20%7 Not covered
Acute care detoxification 20% ($250 maximum allowable/day) Not covered 20% ($250 maximum allowable/day) Not covered
Other servicesDurable medical equipment and orthotics5
20%
40%
20%
40%
($3,000 maximum per calendar year, PPO and OON combined) ($3,000 maximum per calendar year, PPO and OON combined)
Diabetic supplies 20% 40% 20% 40%
Chiropractic services $20 (12 visits per calendar year) Not covered $20 (12 visits per calendar year) Not covered
Acupuncture 20% 40% 20% 40%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage8 Subject to calendar year medical deductible (per insured) Subject to calendar year medical deductible (per insured)
Prescription drugs (up to a 30-day supply)9 $10 / $25 / $50 50% $10 / $25 / $50 50%
Specialty drugs (most self-injectables) 30% Not covered 30% Not covered
HR
A

36
Salud con Health Net PortfolioBenefit description1 Salud HMO y Más 15 (1HT)
SIMNSA Network2
(Mexico members)Salud network(California members)
SIMNSA Network2
(self-referral for California members)
Plan maximumsOut-of-pocket maximum3
$1,500 single / $3,000 two-party / $4,500 family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$5 copay
$15 copay $5 copay
Preventive care services4 Covered in full Covered in full Covered in full
X-ray and laboratory procedures Covered in full Covered in full Covered in full
Rehabilitation therapy6 $5 copay $15 copay $5 copay
Self-injectable drugs Covered in full Covered in full Covered in full
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
$250 per admission copay
Covered in full
Outpatient facility services (other than surgery)
Covered in full 20% Covered in full
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 20% Covered in full
Skilled nursing facility(100 days per calendar year)
Covered in full 20% Covered in full
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$10 copay $50 copay $10 copay
Urgent care facility $10 copay $15 copay $10 copay
Ambulance services (ground and air) Covered in full $50 copay Covered in full
Behavioral services5
Severe mental health (outpatient/inpatient)
$5 copay / Covered in full7 $15 copay / Covered in full
$5 copay / Covered in full7
Non-severe mental health (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (20 days/year)7
$15 copay / Covered in full $5 copay (20 visits/year) / Covered in full (20 days/year)7
Chemical dependency rehabilitation (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
$20 copay (20 visits/year) / Covered in full (30 days/year)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
Acute care detoxification 20%7 Covered in full 20%7
Other servicesDurable medical equipment
Covered in full
Covered in full
Covered in full
Orthotics and prosthetics Covered in full Covered in full Covered in full
Diabetic supplies Covered in full Covered in full Covered in full
Acupuncture, chiropractic services Not covered Optional rider available8 Not covered
Prescription drug coverage
Brand name calendar year deductible (per insured)
No deductible
No deductible
No deductible
Prescription drugs (up to a 30-day supply)9
$5 copay $5 / $15 / $35 $5 copay

37
Benefit description1 Salud HMO y Más 25 (1HU)SIMNSA Network2
(Mexico members)Salud network (California members)
SIMNSA Network2
(self-referral for California members)
Plan maximumsOut-of-pocket maximum3
$1,500 single / $3,000 two-party / $4,500 family
$3,500 single / $7,000 family
$1,500 single / $3,000 two-party / $4,500 family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$5 copay
$25 copay $5 copay
Preventive care services4 Covered in full Covered in full Covered in full
X-ray and laboratory procedures Covered in full Covered in full5 Covered in full
Rehabilitation therapy6 $5 copay $25 copay $5 copay
Self-injectable drugs Covered in full Covered in full Covered in full
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
$250/day (4-day copay maximum)
Covered in full
Outpatient facility services (other than surgery)
Covered in full 20% Covered in full
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 20% Covered in full
Skilled nursing facility(100 days per calendar year)
Covered in full 20% Covered in full
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$10 copay $100 copay $10 copay
Urgent care facility $10 copay $25 copay $10 copay
Ambulance services (ground and air) Covered in full $100 copay Covered in full
Behavioral servicesSevere mental health (outpatient/inpatient)
$5 copay / Covered in full7 $25 copay / Covered in full
$5 copay / Covered in full7
Non-severe mental health (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (20 days/year)7
$25 copay / Covered in full $5 copay (20 visits/year) / Covered in full (20 days/year)7
Chemical dependency rehabilitation (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
$25 copay (20 visits/year) / Covered in full (30 days/year)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
Acute care detoxification 20% (20 days per year)7 Covered in full 20% (20 days per year)7
Other servicesDurable medical equipment
Covered in full
30%
Covered in full
Orthotics and prosthetics Covered in full Covered in full Covered in full
Diabetic supplies Covered in full Covered in full Covered in full
Acupuncture, chiropractic services Not covered Optional rider available8 Not covered
Prescription drug coverage
Brand name calendar year deductible (per insured)
No deductible
$250
No deductible
Prescription drugs (up to a 30-day supply)9
$5 copay $10 / $35 / $50 $5 copay
SALU
D C
ON
H
EA
LTH N
ET
Plan footnotes found on pages 50–53.
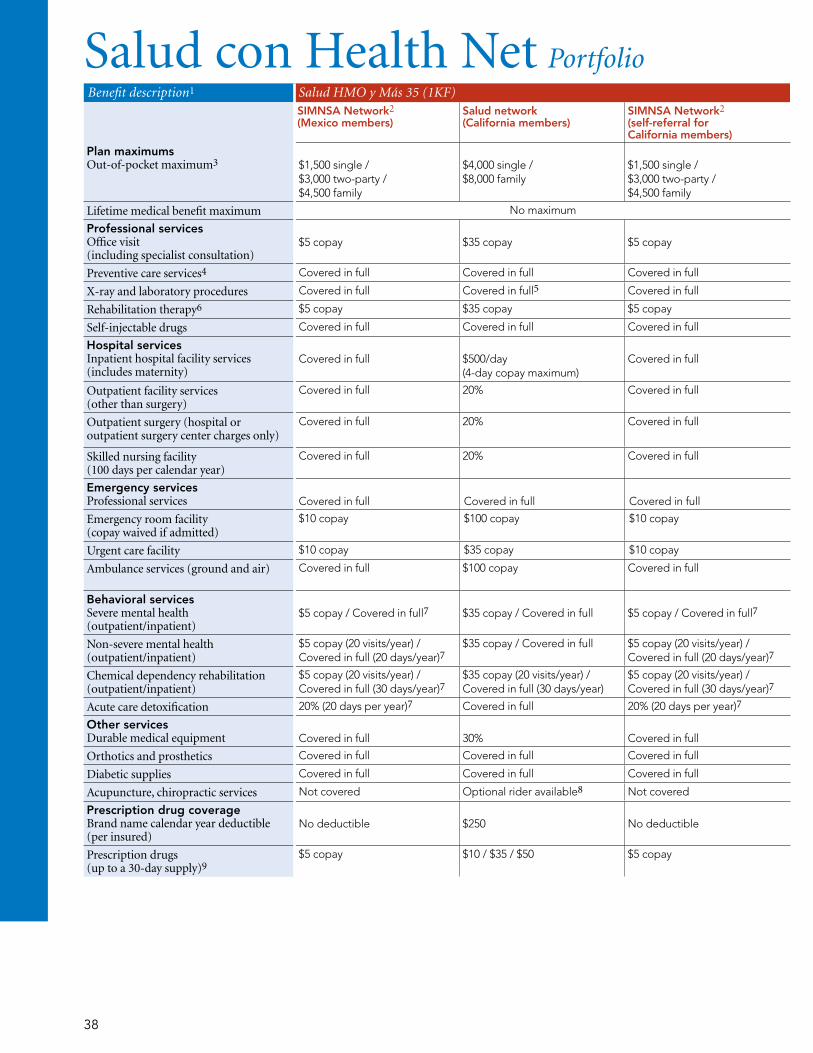
38
Benefit description1 Salud HMO y Más 35 (1KF) Salud Mexico HMO (1HX)SIMNSA Network2 (Mexico members)
Salud network(California members)
SIMNSA Network2
(self-referral for California members)
SIMNSA Network only2
Plan maximumsOut-of-pocket maximum3
$1,500 single / $3,000 two-party / $4,500 family
$4,000 single / $8,000 family
$1,500 single / $3,000 two-party / $4,500 family
$1,500 single / $3,000 two-party / $4,500 family
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$5 copay
$35 copay $5 copay
$5 copay
Preventive care services4 Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures Covered in full Covered in full5 Covered in full Covered in full
Rehabilitation therapy6 $5 copay $35 copay $5 copay $5 copay
Self-injectable drugs Covered in full Covered in full Covered in full Covered in full
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
$500/day (4-day copay maximum)
Covered in full
Covered in full
Outpatient facility services (other than surgery)
Covered in full 20% Covered in full Covered in full
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 20% Covered in full Covered in full
Skilled nursing facility(100 days per calendar year)
Covered in full 20% Covered in full Covered in full
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$10 copay $100 copay $10 copay $10 copay (in Mexico) /$50 copay (outside Mexico)
Urgent care facility $10 copay $35 copay $10 copay $10 copay
Ambulance services (ground and air) Covered in full $100 copay Covered in full Covered in full (air ambulance not covered)
Behavioral servicesSevere mental health (outpatient/inpatient)
$5 copay / Covered in full7 $35 copay / Covered in full
$5 copay / Covered in full7
$5 copay / Covered in full7
Non-severe mental health (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (20 days/year)7
$35 copay / Covered in full $5 copay (20 visits/year) / Covered in full (20 days/year)7
$5 copay (20 visits/year) / Covered in full (20 days/year)7
Chemical dependency rehabilitation (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
$35 copay (20 visits/year) / Covered in full (30 days/year)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
$5 copay (20 visits/year) / Covered in full (30 days/year)7
Acute care detoxification 20% (20 days per year)7 Covered in full 20% (20 days per year)7 20%7
Other servicesDurable medical equipment
Covered in full
30%
Covered in full
Covered in full
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full
Diabetic supplies Covered in full Covered in full Covered in full Covered in full
Acupuncture, chiropractic services Not covered Optional rider available8 Not covered Not covered
Prescription drug coverage
Brand name calendar year deductible (per insured)
No deductible
$250
No deductible
No deductible
Prescription drugs (up to a 30-day supply)9
$5 copay $10 / $35 / $50 $5 copay $5 copay
Salud con Health Net Portfolio

39
Benefit description1 Salud HMO y Más 35 (1KF) Salud Mexico HMO (1HX)SIMNSA Network2 (Mexico members)
Salud network(California members)
SIMNSA Network2
(self-referral for California members)
SIMNSA Network only2
Plan maximumsOut-of-pocket maximum3
$1,500 single / $3,000 two-party / $4,500 family
$4,000 single / $8,000 family
$1,500 single / $3,000 two-party / $4,500 family
$1,500 single / $3,000 two-party / $4,500 family
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$5 copay
$35 copay $5 copay
$5 copay
Preventive care services4 Covered in full Covered in full Covered in full Covered in full
X-ray and laboratory procedures Covered in full Covered in full5 Covered in full Covered in full
Rehabilitation therapy6 $5 copay $35 copay $5 copay $5 copay
Self-injectable drugs Covered in full Covered in full Covered in full Covered in full
Hospital servicesInpatient hospital facility services (includes maternity)
Covered in full
$500/day (4-day copay maximum)
Covered in full
Covered in full
Outpatient facility services (other than surgery)
Covered in full 20% Covered in full Covered in full
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 20% Covered in full Covered in full
Skilled nursing facility(100 days per calendar year)
Covered in full 20% Covered in full Covered in full
Emergency servicesProfessional services
Covered in full
Covered in full
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$10 copay $100 copay $10 copay $10 copay (in Mexico) /$50 copay (outside Mexico)
Urgent care facility $10 copay $35 copay $10 copay $10 copay
Ambulance services (ground and air) Covered in full $100 copay Covered in full Covered in full (air ambulance not covered)
Behavioral servicesSevere mental health (outpatient/inpatient)
$5 copay / Covered in full7 $35 copay / Covered in full
$5 copay / Covered in full7
$5 copay / Covered in full7
Non-severe mental health (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (20 days/year)7
$35 copay / Covered in full $5 copay (20 visits/year) / Covered in full (20 days/year)7
$5 copay (20 visits/year) / Covered in full (20 days/year)7
Chemical dependency rehabilitation (outpatient/inpatient)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
$35 copay (20 visits/year) / Covered in full (30 days/year)
$5 copay (20 visits/year) / Covered in full (30 days/year)7
$5 copay (20 visits/year) / Covered in full (30 days/year)7
Acute care detoxification 20% (20 days per year)7 Covered in full 20% (20 days per year)7 20%7
Other servicesDurable medical equipment
Covered in full
30%
Covered in full
Covered in full
Orthotics and prosthetics Covered in full Covered in full Covered in full Covered in full
Diabetic supplies Covered in full Covered in full Covered in full Covered in full
Acupuncture, chiropractic services Not covered Optional rider available8 Not covered Not covered
Prescription drug coverage
Brand name calendar year deductible (per insured)
No deductible
$250
No deductible
No deductible
Prescription drugs (up to a 30-day supply)9
$5 copay $10 / $35 / $50 $5 copay $5 copay
Plan footnotes found on pages 50–53.
Josefina Bravo,
Health Net
We’re dedicated
to member health
and wellness.
SALU
D C
ON
H
EA
LTH N
ET

40
Benefit description1 Salud PPO (1HW)SIMNSA Network2 (Mexico members)
Salud network(California members)
Out-of-network3
(self-referral for California members)
Plan maximumsCalendar year deductible
Not applicable
$100 single / 2 per family
$1,000 single / 2 per family
Out-of-pocket maximum $1,000 single / $2,000 family $2,000 single / $4,000 family $10,000 single / $10,000 family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$5 copay
$15 copay 50%
Preventive care services4 Covered in full Covered in full 50%
X-ray and laboratory procedures5 10% 20% 50%
Rehabilitation therapy5,6 10% 20% ($25 maximum per visit) 50% ($25 maximum per visit)
Self-injectable drugs5 $5 copay See Specialty drugs See Specialty drugs
Hospital services5
Inpatient hospital facility services (includes maternity)
10% $250 per admission deductible9 + 20%
$250 per admission deductible9 + 50% ($380 maximum/day)
Outpatient facility services (other than surgery)
10% $250 deductible9 + 20% $250 deductible9 + 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
10% $250 deductible9 + 20% $250 deductible9 + 50% (50% maximum allowable)
Skilled nursing facility Not covered $250 deductible9 + 20% $250 deductible9 + 50% ($150 maximum allowable/day)
Emergency servicesProfessional services
10%
20%
50%
Emergency room facility (copay waived if admitted)
$25 deductible + 10% $50 deductible + 20% $100 deductible + 50%
Urgent care facility $25 deductible + 10% $50 deductible + 20% $100 deductible + 50%
Ambulance services (ground and air)5 $20 deductible + 10% (air not covered)
$50 deductible + 20% 50%
Behavioral services5
Severe mental health (outpatient/inpatient)
$5 copay / 10% $15 copay / $2509 + 20% 50% / $2509 + 50% ($380 maximum allowable/day)
Non-severe mental health (outpatient/inpatient)7
$5 copay + 10% / 10%8 $30 copay + 20% / 20% $30 copay + 50% / 50%8
Chemical dependency rehabilitation (outpatient/inpatient)7
$5 copay + 10% / Not covered8 $30 copay + 20% / Not covered $30 copay + 50% / Not covered8
Acute care detoxification 10% 20% + $250 per admit9 50% + $250 per admit9
($380 max allowable/day)
Other servicesDurable medical equipment5
10%
20%
50%
Orthotics and prosthetics 10% 20% 50%
Diabetic supplies 10% 20% 50%
Acupuncture, chiropractic services Not covered
Prescription drug coverage
Prescription drugs dispensed by SIMNSA
$5 copay
Not applicable
$5 copay
Prescription drugs dispensed by a Health Net participating pharmacy10
Not applicable $10 / $35 / 50% Not covered
Specialty drugs (most self-injectables) Not covered 30% ($250 copay maximum per prescription)
Not covered
Salud con Health Net Portfolio
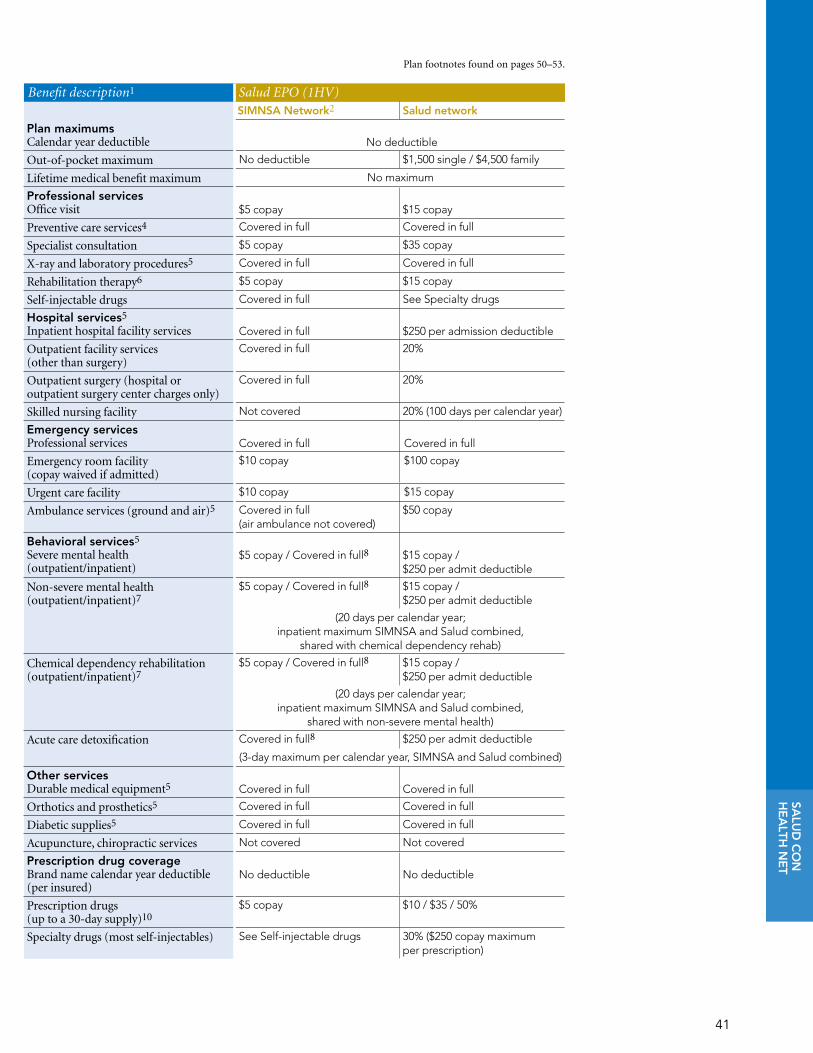
41
Benefit description1 Salud EPO (1HV)SIMNSA Network2 Salud network
Plan maximumsCalendar year deductible No deductible
Out-of-pocket maximum No deductible $1,500 single / $4,500 family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit
$5 copay $15 copay
Preventive care services4 Covered in full Covered in full
Specialist consultation $5 copay $35 copay
X-ray and laboratory procedures5 Covered in full Covered in full
Rehabilitation therapy6 $5 copay $15 copay
Self-injectable drugs Covered in full See Specialty drugs
Hospital services5
Inpatient hospital facility services Covered in full $250 per admission deductible
Outpatient facility services (other than surgery)
Covered in full 20%
Outpatient surgery (hospital or outpatient surgery center charges only)
Covered in full 20%
Skilled nursing facility Not covered 20% (100 days per calendar year)
Emergency servicesProfessional services
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$10 copay $100 copay
Urgent care facility $10 copay $15 copay
Ambulance services (ground and air)5 Covered in full (air ambulance not covered)
$50 copay
Behavioral services5
Severe mental health (outpatient/inpatient)
$5 copay / Covered in full8
$15 copay / $250 per admit deductible
Non-severe mental health (outpatient/inpatient)7
$5 copay / Covered in full8 $15 copay / $250 per admit deductible
(20 days per calendar year; inpatient maximum SIMNSA and Salud combined,
shared with chemical dependency rehab)
Chemical dependency rehabilitation (outpatient/inpatient)7
$5 copay / Covered in full8 $15 copay / $250 per admit deductible
(20 days per calendar year; inpatient maximum SIMNSA and Salud combined,
shared with non-severe mental health)
Acute care detoxification Covered in full8 $250 per admit deductible
(3-day maximum per calendar year, SIMNSA and Salud combined)
Other servicesDurable medical equipment5
Covered in full
Covered in full
Orthotics and prosthetics5 Covered in full Covered in full
Diabetic supplies5 Covered in full Covered in full
Acupuncture, chiropractic services Not covered Not covered
Prescription drug coverage
Brand name calendar year deductible (per insured)
No deductible
No deductible
Prescription drugs (up to a 30-day supply)10
$5 copay $10 / $35 / 50%
Specialty drugs (most self-injectables) See Self-injectable drugs 30% ($250 copay maximum per prescription)
Plan footnotes found on pages 50–53.
SALU
D C
ON
H
EA
LTH N
ET

42
Flex Net Portfolio Plan footnotes found on pages 50–53.
Benefit description1 Flex Net Indemnity2 (1KL)
Plan maximumsCalendar year deductible $300 single / $900 family
Out-of-pocket maximum (does not include calendar year deductible)
$1,500 single / $4,500 family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
20%
Preventive care services3 Covered in full
X-ray and laboratory procedures4 20%
Rehabilitation therapy4,5 20% (60 visits per calendar year)
Hospital services4
Inpatient hospital facility services (includes maternity)
20%
Outpatient facility services (other than surgery)
20%
Outpatient surgery (hospital or outpatient surgery center charges only)
20%
Skilled nursing facility 20% (60 days per calendar year)
Emergency servicesProfessional services
20%
Emergency room facility 20%
Urgent care facility 20%
Ambulance services (ground and air) 20% (Ground: max distance 75 miles per incident / Air: $750 max per incident)
Behavioral servicesSevere mental health (outpatient/inpatient)
20% / 20%
Non-severe mental health6 (outpatient/inpatient)
50% / 50%
Chemical dependency rehabilitation (outpatient/inpatient)6
50% / 50%
Acute care detoxification 50% (3 days per calendar year)
Other servicesDurable medical equipment4
20%
Orthotics and prosthetics4 20%
Diabetic supplies 20%
Chiropractic services 20% (15 visits per calendar year, $25 maximum payable per visit)
Acupuncture Not covered
Prescription drug coverageCalendar year deductible (per insured) $75 brand-name deductible
Prescription drugs (up to a 30-day supply)
20%
Specialty drugs (most self-injectables) 20% ($250 copay maximum per prescription)

43
Benefit description2 Options HMO 25 (1HY) (1HZ) (1JB) Options HMO 35 (1JC) (1JD) (1JE)Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$25 copay
$35 copay
Preventive care services3 Covered in full Covered in full
X-ray and laboratory procedures4 Covered in full Covered in full
Rehabilitation therapy5 $25 copay $35 copay
Self-injectable drugs 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
20%
30%
Outpatient facility services (other than surgery)
20% 30%
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 30%
Skilled nursing facility Days 1–10: Covered in fullDays 11–100: $25/day
Days 1–10: Covered in fullDays 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay
Urgent care facility $50 copay $50 copay
Ambulance services (ground and air) $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$25 copay / 20% $35 copay / 30%
Non-severe mental health (outpatient/inpatient)
$30 (20 visits per calendar year) /20% (30 days per calendar year)
$40 (20 visits per calendar year) /30% (30 days per calendar year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered
Acute care detoxification 20% 30%
Other servicesDurable medical equipment
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics Covered in full Covered in full
Diabetic supplies 20% 20%
Acupuncture, chiropractic services7 Optional rider available Optional rider available
Prescription drug coverage8
Brand name calendar year deductible (per member)
$150
$200
Prescription drugs (up to a 30-day supply)9
$15 / $30 / $50 $15 / $30 / $50
Options HMO PortfolioPlease note: HMO plans are available with Silver Network and Bronze Network.1
Plan footnotes found on pages 50–53.
Hn O
PTIO
NS H
MO

44
Please note: EOA plans are available with Silver Network.1
Plan footnotes found on pages 50–53.Options EOA PortfolioBenefit description2 Options EOA 25 (1JF) (1JG) Options EOA 35 (1JH) (1JJ)Plan maximumsOut-of-pocket maximum
$3,000 single / $6,000 family
$4,000 single / $8,000 family
Lifetime medical benefit maximum No maximum No maximum
Professional services3
Office visit (including specialist consultation)
HMO: $25 copay PPO: $40 copay
HMO: $35 copay PPO: $50 copay
Preventive care services4 Covered in full Covered in full
X-ray and laboratory procedures5,6 Covered in full Covered in full
Rehabilitation therapy7 HMO: $25 copay PPO: $40 copay (12 visits per calendar year)
HMO: $35 copay PPO: $50 copay (12 visits per calendar year)
Self-injectable drugs 30% 30%
Hospital servicesInpatient hospital facility services (includes maternity)
20%
30%
Outpatient facility services (other than surgery)8
20% 30%
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 30%
Skilled nursing facility Days 1–10: Covered in fullDays 11–100: $25/day
Days 1–10: Covered in fullDays 11–100: $25/day
Emergency servicesProfessional services
Covered in full
Covered in full
Emergency room facility (copay waived if admitted)
$100 copay $100 copay
Urgent care facility $50 copay $50 copay
Ambulance services (ground and air) $100 copay $100 copay
Behavioral services6
Severe mental health (outpatient/inpatient)
$25 copay / 20% $35 copay / 30%
Non-severe mental health (outpatient/inpatient)
$35 (20 visits per calendar year) /20% (30 days per calendar year)
$40 (20 visits per calendar year) /30% (30 days per calendar year)
Chemical dependency rehabilitation (outpatient/inpatient)
Not covered Not covered
Acute care detoxification 20% 30%
Other servicesDurable medical equipment8
50% ($2,000 maximum per calendar year)
50% ($2,000 maximum per calendar year)
Orthotics and prosthetics8 Covered in full Covered in full
Diabetic supplies 20% 20%
Acupuncture, chiropractic services9 Optional rider available Optional rider available
Prescription drug coverage10
Brand name calendar year deductible (per member)
$150
$200
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 $15 / $30 / $50
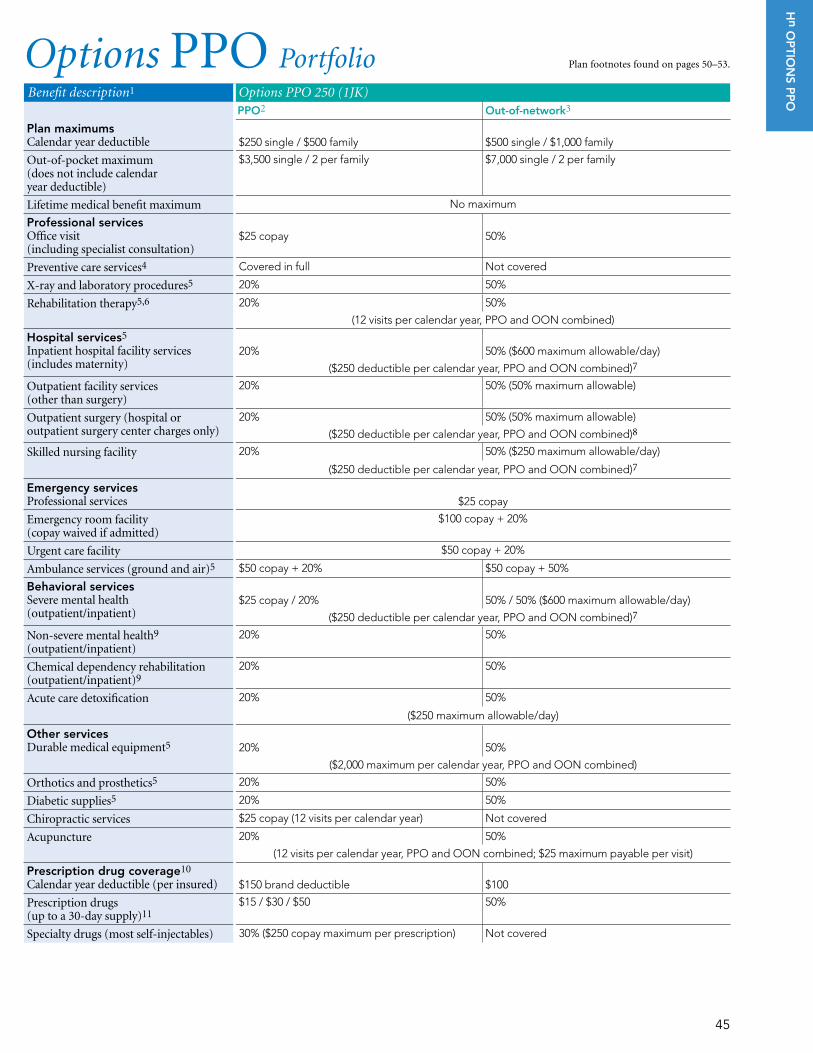
45
Options PPO Portfolio Plan footnotes found on pages 50–53.
Benefit description1 Options PPO 250 (1JK)PPO2 Out-of-network3
Plan maximumsCalendar year deductible
$250 single / $500 family
$500 single / $1,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$3,500 single / 2 per family $7,000 single / 2 per family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$25 copay 50%
Preventive care services4 Covered in full Not covered
X-ray and laboratory procedures5 20% 50%
Rehabilitation therapy5,6 20% 50%
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
20% 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
20% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
20% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 20% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$25 copay
Emergency room facility (copay waived if admitted)
$100 copay + 20%
Urgent care facility $50 copay + 20%
Ambulance services (ground and air)5 $50 copay + 20% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$25 copay / 20% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health9 (outpatient/inpatient)
20% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
20% 50%
Acute care detoxification 20% 50%
($250 maximum allowable/day)
Other servicesDurable medical equipment5
20%
50%
($2,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 20% 50%
Diabetic supplies5 20% 50%
Chiropractic services $25 copay (12 visits per calendar year) Not covered
Acupuncture 20% 50%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) $150 brand deductible $100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription) Not covered
Hn O
PTIO
NS P
PO

46
Plan footnotes found on pages 50–53.Options PPO PortfolioBenefit description1 Options PPO 500 (1JL)
PPO2 Out-of-network3
Plan maximumsCalendar year deductible
$500 single / $1,000 family
$1,000 single / $2,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$4,000 single / 2 per family $8,000 single / 2 per family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$35 copay 50%
Preventive care services4 Covered in full Not covered
X-ray and laboratory procedures5 30% 50%
Rehabilitation therapy5,6 30% 50%
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
30%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
30% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
30% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 30% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services $35 copay
Emergency room facility (copay waived if admitted)
$100 copay + 30%
Urgent care facility $50 copay + 30%
Ambulance services (ground and air)5 $50 copay + 30% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$35 copay / 30% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health9 (outpatient/inpatient)
30% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
30% 50%
Acute care detoxification 30% 50%
($250 maximum allowable/day)
Other servicesDurable medical equipment5
30%
50%
($1,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 30% 50%
Diabetic supplies5 30% 50%
Chiropractic services $35 copay (12 visits per calendar year) Not covered
Acupuncture 30% 50%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) $200 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription) Not covered

47
Options PPO PortfolioBenefit description1 Options PPO 1500 (1JM)
PPO2 Out-of-network3
Plan maximumsCalendar year deductible
$1,500 single / $3,000 family
$3,000 single / $6,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$4,000 single / 2 per family $8,000 single / 2 per family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$25 copay 50%
Preventive care services4 Covered in full Not covered
X-ray and laboratory procedures5 30% 50%
Rehabilitation therapy5,6 30% 50%
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
30% 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
30% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
30% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 30% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$25 copay
Emergency room facility (copay waived if admitted)
$100 copay + 30%
Urgent care facility $50 copay + 30%
Ambulance services (ground and air)5 $50 copay + 30% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$25 copay / 30% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health9 (outpatient/inpatient)
30% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
30% 50%
Acute care detoxification 30% 50%
($250 maximum allowable/day)
Other servicesDurable medical equipment5
30%
50%
($2,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 30% 50%
Diabetic supplies5 30% 50%
Chiropractic services $25 copay (12 visits per calendar year) Not covered
Acupuncture 30% 50%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) $150 brand deductible $100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription) Not covered
Plan footnotes found on pages 50–53.
Hn O
PTIO
NS P
PO

48
Options PPO Portfolio Plan footnotes found on pages 50–53.
Benefit description1 Options PPO 1750 (1JN)PPO2 Out-of-network3
Plan maximumsCalendar year deductible
$1,750 single / $3,500 family
$3,500 single / $7,000 family
Out-of-pocket maximum (does not include calendar year deductible)
$5,000 single / 2 per family $10,000 single / 2 per family
Lifetime medical benefit maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$35 copay 50%
Preventive care services4 Covered in full Not covered
X-ray and laboratory procedures5 40% 50%
Rehabilitation therapy5,6 40% 50%
(12 visits per calendar year, PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
40%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
40% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
40% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 40% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services $35 copay
Emergency room facility (copay waived if admitted)
$100 copay + 40%
Urgent care facility $50 copay + 40%
Ambulance services (ground and air)5 $50 copay + 40% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$35 copay / 40% 50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health9 (outpatient/inpatient)
40% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
40% 50%
Acute care detoxification 40% 50%
($250 maximum allowable/day)
Other servicesDurable medical equipment5
40%
50%
($1,000 maximum per calendar year, PPO and OON combined)
Orthotics and prosthetics5 40% 50%
Diabetic supplies5 40% 50%
Chiropractic services $35 copay (12 visits per calendar year) Not covered
Acupuncture 40% 50%
(12 visits per calendar year, PPO and OON combined; $25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured) $200 brand deductible
$100
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% ($250 copay maximum per prescription) Not covered

49
Options PPO Portfolio Plan footnotes found on pages 50–53.
Benefit description1 Options PPO 3000 (HSA-compatible) (1JP) Options PPO 4000 (HSA-compatible) (1JQ)
Plan maximumsCalendar year deductible (For family coverage, the enrolled employee and dependents must collectively pay the family amount before Health Net begins to pay.)
PPO2 Out-of-network3 PPO2 Out-of-network3
$3,000 single (employee-only coverage) /
$6,000 family (employee and dependent coverage
$4,000 single (employee-only coverage) /
$8,000 family (employee and dependent coverage)
Out-of-pocket maximum (includes calendar year deductible)
$4,000 single (employee-only coverage) /$8,000 family (employee and dependent coverage)
$5,000 single (employee-only coverage) /$10,000 family (employee and dependent coverage)
Lifetime medical benefit maximum No maximum No maximum
Professional servicesOffice visit (including specialist consultation)
$25 copay (deductible not waived)
50% $35 copay (deductible not waived)
50%
Preventive care services4 Covered in full Not covered Covered in full Not covered
X-ray and laboratory procedures5 30% 50% 40% 50%
Rehabilitation therapy5,6 30% 50% 40% 50%(12 visits per calendar year,PPO and OON combined)
(12 visits per calendar year,PPO and OON combined)
Hospital services5
Inpatient hospital facility services (includes maternity)
20% 50% ($600 maximum allowable/day)
40%
50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Outpatient facility services (other than surgery)
30% 50% (50% maximum allowable)
40% 50% (50% maximum allowable)
Outpatient surgery (hospital or outpatient surgery center charges only)
30% 50% (50% maximum allowable)
40% 50% (50% maximum allowable)
($250 deductible per calendar year, PPO and OON combined)8
($250 deductible per calendar year, PPO and OON combined)8
Skilled nursing facility 30% 50% ($250 maximum allowable/day)
40% 50% ($250 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Emergency servicesProfessional services
$25 copay (deductible not waived)
50% $35 copay
(deductible not waived)
50%
Emergency room facility (copay waived if admitted)
$100 copay + 30% $100 + 50% $100 copay + 40% $100 + 50%
Urgent care facility $50 copay + 30% $50 + 50% $50 copay + 40% $50 + 50%
Ambulance services (ground and air)5 $50 copay + 30% $50 copay + 50% $50 copay + 40% $50 copay + 50%
Behavioral servicesSevere mental health (outpatient/inpatient)
$25 / 30% 50% / 50% ($600 maximum allowable/day)
$35 / 40%
50% / 50% ($600 maximum allowable/day)
($250 deductible per calendar year, PPO and OON combined)7
($250 deductible per calendar year, PPO and OON combined)7
Non-severe mental health (outpatient/inpatient)9
30% 50% 40% 50%
Chemical dependency rehabilitation (outpatient/inpatient)9
30% 50% 40% 50%
Acute care detoxification 30% 50% 40% 50%($250 maximum allowable/day) ($250 maximum allowable/day)
Other servicesDurable medical equipment5
30%
50%
40%
50%
($2,000 maximum per calendar year,PPO and OON combined)
($1,000 maximum per calendar year,PPO and OON combined)
Orthotics and prosthetics5 30% 50% 40% 50%
Diabetic supplies5 30% 50% 40% 50%
Chiropractic services $25 copay (deductible not waived, 12 visits per calendar year)
Not covered $35 copay (deductible not waived, 12 visits per calendar year)
Not covered
Acupuncture 30% 50% 40% 50%(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)(12 visits per calendar year, PPO and OON combined;
$25 maximum payable per visit)
Prescription drug coverage10
Calendar year deductible (per insured)
Subject to annual deductible
Subject to annual deductible
Prescription drugs (up to a 30-day supply)11
$15 / $30 / $50 50% $15 / $30 / $50 50%
Specialty drugs (most self-injectables) 30% Not covered 30% Not covered
Hn O
PTIO
NS P
PO

50
HMO 1 The Silver Network is an affordable network alternative offered in all or parts of Kern, Los Angeles, Orange, San Bernardino,
San Diego, San Francisco, Santa Clara, Stanislaus, Riverside and Ventura counties. The Bronze Network is a network alternative offered in parts of Los Angeles, San Bernardino and San Diego counties. Ask if these networks are available in your area.
2 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Evidence of Coverage for terms and conditions of coverage. The three plan codes are: Full network; Silver Network; Bronze Network.
3 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 4 Complex radiology (includes CT, SPECT, PET and MRI) requires a $100 copay. 5 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 6 All mental health and chemical dependency services are provided or contracted through Managed Health Network (MHN).
Please contact MHN for details. 7 Chiropractic and/or acupuncture rider coverage is available as an optional benefit with the HMO plan shown above. Features of
Health Net’s chiropractic coverage include a $10 per visit copay and up to 20 visits per calendar year. 8 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific
drug, go to www.healthnet.com. 9 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
EOA 1 The Silver Network is an affordable network alternative offered in all or parts of Kern, Los Angeles, Orange, San Bernardino,
San Diego, San Francisco, Santa Clara, Stanislaus, Riverside and Ventura counties. Ask if this network is available in your area. 2 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Evidence of Coverage for
terms and conditions of coverage. The two plan codes are: Full network; Silver Network. 3 For the PPO level, self-referral to a PPO network physician. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Complex radiology (includes CT) requires a $100 copay under HMO and PPO. MRI, MUGA, PET and SPECT services are not
covered through PPO level. 6 Under Elect Open Access, radiographic X-ray and laboratory services will be covered only when provided or coordinated by your
primary care physician and approved by the PPG/IPA, except when provided at a PPO physician’s office or contracted PPO lab or facility. 7 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 8 Under Elect Open Access, inpatient hospital and professional services, durable medical equipment and orthotics and prosthetics
are covered when provided or coordinated by the primary care physician only and approved by the PPG/IPA. Inpatient care and outpatient services are not covered on the PPO level.
9 All mental health and chemical dependency services are provided or contracted through Managed Health Network (MHN). Please contact MHN for details.
10 Chiropractic and/or acupuncture rider coverage is available as an optional benefit with the EOA plan shown above. Features of Health Net’s chiropractic coverage include a $10 per visit copay and up to 20 visits per calendar year.
11 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific drug, go to www.healthnet.com.
12 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
POS 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Evidence of Coverage for
terms and conditions of coverage. 2 Member pays the negotiated rate, which is the rate the participating or preferred providers have agreed to accept for providing a
covered service.
3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology.
4 The 50% coinsurance through the OON level will apply towards the member’s out-of-pocket maximum.
5 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services.
6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy.
7 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%. 8 This deductible is required only for the first inpatient hospital or skilled nursing facility admission each calendar year. Once the
deductible is satisfied, no deductible is required for subsequent admissions in the same calendar year. This deductible is in addition to the plan calendar year deductible.
9 Once the outpatient surgery deductible is satisfied, no deductible is required for subsequent outpatient surgeries in the same calendar year. This deductible is in addition to the plan calendar year deductible.
10 All mental health and chemical dependency services are provided or contracted through Managed Health Network (MHN). Please contact MHN for details.
11 Chiropractic and/or acupuncture rider coverage is available as an optional benefit with the POS plan shown above through the HMO level. Features of Health Net’s chiropractic coverage include a $10 per visit copay and up to 20 visits per calendar year.
12 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific drug, go to www.healthnet.com.
13 The three prescription drug tiers are: Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Note: Health Net’s 2010 ratio of premium costs to health services paid for Small Business HMO and PPO health plans were 76.3% and 92.8% respectively.Footnotes
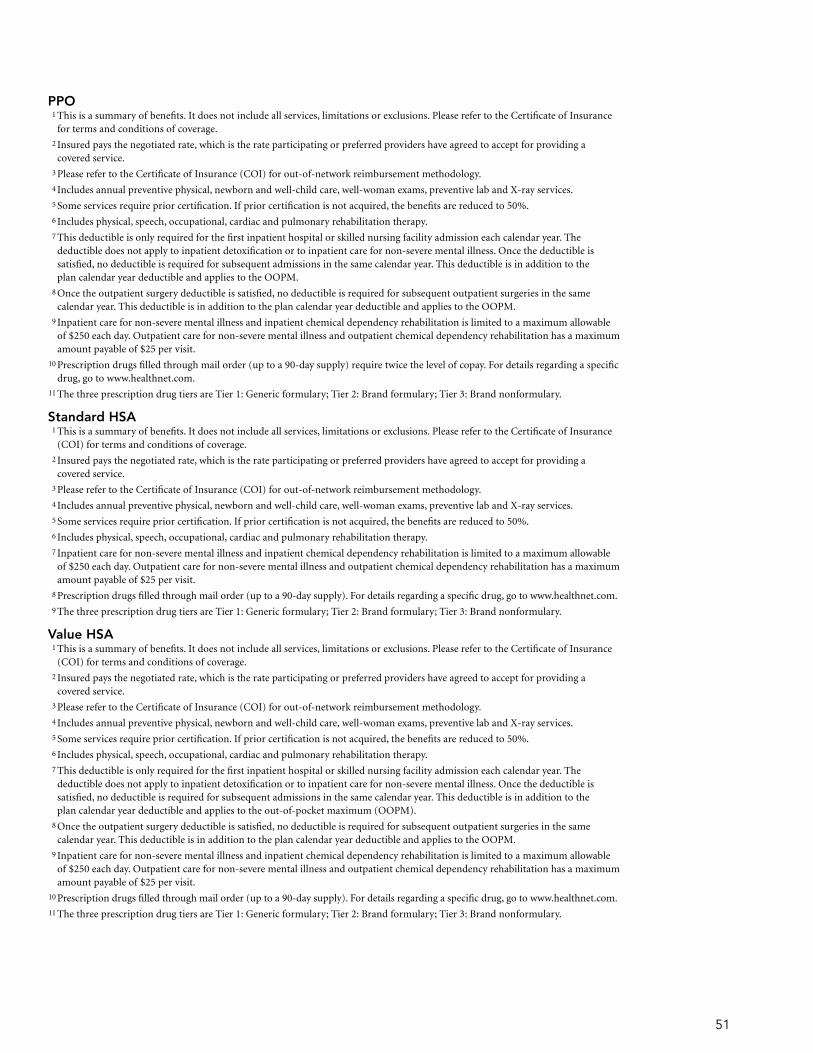
51
PPO 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
for terms and conditions of coverage. 2 Insured pays the negotiated rate, which is the rate participating or preferred providers have agreed to accept for providing a
covered service. 3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%. 6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 7 This deductible is only required for the first inpatient hospital or skilled nursing facility admission each calendar year. The
deductible does not apply to inpatient detoxification or to inpatient care for non-severe mental illness. Once the deductible is satisfied, no deductible is required for subsequent admissions in the same calendar year. This deductible is in addition to the plan calendar year deductible and applies to the OOPM.
8 Once the outpatient surgery deductible is satisfied, no deductible is required for subsequent outpatient surgeries in the same calendar year. This deductible is in addition to the plan calendar year deductible and applies to the OOPM.
9 Inpatient care for non-severe mental illness and inpatient chemical dependency rehabilitation is limited to a maximum allowable of $250 each day. Outpatient care for non-severe mental illness and outpatient chemical dependency rehabilitation has a maximum amount payable of $25 per visit.
10 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific drug, go to www.healthnet.com.
11 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Standard HSA 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
(COI) for terms and conditions of coverage. 2 Insured pays the negotiated rate, which is the rate participating or preferred providers have agreed to accept for providing a
covered service. 3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%. 6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 7 Inpatient care for non-severe mental illness and inpatient chemical dependency rehabilitation is limited to a maximum allowable
of $250 each day. Outpatient care for non-severe mental illness and outpatient chemical dependency rehabilitation has a maximum amount payable of $25 per visit.
8 Prescription drugs filled through mail order (up to a 90-day supply). For details regarding a specific drug, go to www.healthnet.com. 9 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Value HSA 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
(COI) for terms and conditions of coverage. 2 Insured pays the negotiated rate, which is the rate participating or preferred providers have agreed to accept for providing a
covered service. 3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%. 6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 7 This deductible is only required for the first inpatient hospital or skilled nursing facility admission each calendar year. The
deductible does not apply to inpatient detoxification or to inpatient care for non-severe mental illness. Once the deductible is satisfied, no deductible is required for subsequent admissions in the same calendar year. This deductible is in addition to the plan calendar year deductible and applies to the out-of-pocket maximum (OOPM).
8 Once the outpatient surgery deductible is satisfied, no deductible is required for subsequent outpatient surgeries in the same calendar year. This deductible is in addition to the plan calendar year deductible and applies to the OOPM.
9 Inpatient care for non-severe mental illness and inpatient chemical dependency rehabilitation is limited to a maximum allowable of $250 each day. Outpatient care for non-severe mental illness and outpatient chemical dependency rehabilitation has a maximum amount payable of $25 per visit.
10 Prescription drugs filled through mail order (up to a 90-day supply). For details regarding a specific drug, go to www.healthnet.com. 11 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.

52
HRA 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
for terms and conditions of coverage. 2 Insured pays the negotiated rate, which is the rate participating or preferred providers have agreed to accept for providing a covered service. 3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Some services require prior certification. Without prior certification, the benefits are reduced to 50%. An additional $250 penalty
deductible is applied for each inpatient admit that does not receive prior certification and an additional $50 penalty deductible is applied for outpatient visits for specified services. Refer to your Certificate of Insurance (COI) for additional information.
6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 7 Inpatient care for non-severe mental illness and inpatient chemical dependency rehabilitation is limited to a maximum allowable
of $250 each day. Outpatient care for non-severe mental illness and outpatient chemical dependency rehabilitation has a maximum amount payable of $25 per visit.
8 Prescription drugs filled through mail order (up to a 90-day supply). For details regarding a specific drug, go to www.healthnet.com. 9 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Salud con Health Net HMO y Más and Salud Mexico 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Evidence of Coverage for
terms and conditions of coverage. 2 Out-of-network providers, facilities or pharmacies in Mexico (other than those in the SIMNSA Network) are not covered by
this plan. 3 The OOPM is combined for SIMNSA networks in Mexico and California. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Complex radiology (includes CT, SPECT, PET and MRI) requires a $100 copay. 6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 7 Mental health and substance abuse services must be provided by a SIMNSA provider. 8 Chiropractic and/or acupuncture rider coverage is available as an optional benefit with the HMO plan shown above. Features of
Health Net’s chiropractic coverage include a $10 per visit copay and up to 20 visits per calendar year. 9 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Salud con Health Net PPO/EPO 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
(COI) for terms and conditions of coverage. 2 Out-of-network providers, facilities or pharmacies in Mexico (other than those in the SIMNSA Network) are not covered by
this plan.
3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services.
5 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%.
6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy.
7 For non-severe inpatient services, there is a $250 maximum allowable through Health Net Salud Network and OON. Outpatient mental health care and outpatient chemical dependency rehabilitation are limited to 20 visits for each member in a calendar year through SIMNSA, PPO and OON combined.
8 Mental health and substance abuse services must be provided by a SIMNSA provider.
9 A $250 deductible is required for each inpatient hospital admission and each outpatient service, including surgery. The deductible will apply when emergency services are performed.
10 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Hn HMO Options 1 The HMO Silver Network is an affordable network alternative offered in all or parts of Kern, Los Angeles, Orange, San Bernardino,
San Diego, San Francisco, Riverside, Santa Clara, Stanislaus and Ventura counties. The Bronze Network is a network alternative offered in parts of Los Angeles, San Bernardino and San Diego counties. Ask your employer if these networks are available to you.
2 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Evidence of Coverage for terms and conditions of coverage. The three plan codes are: Full network; Silver Network; Bronze Network.
3 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 4 Complex radiology (includes CT, SPECT, PET, MUGA and MRI) requires a $100 copay. 5 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 6 All mental health and chemical dependency services are provided or contracted through Managed Health Network (MHN).
Please contact MHN for details. 7 Chiropractic and/or acupuncture rider coverage is available as an optional benefit with these HMO plans. Features of Health Net’s
chiropractic coverage include a $10 per visit copay and up to 20 visits per calendar year. 8 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific
drug, go to www.healthnet.com. 9 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.

53
Hn EOA Options 1 The EOA Silver Network is an affordable network alternative offered in all or parts of Kern, Los Angeles, Orange, San Bernardino,
San Diego, San Francisco, Riverside, Santa Clara, Stanislaus and Ventura counties. Ask your employer if this network is available to you.
2 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Evidence of Coverage for terms and conditions of coverage. The two plans codes are: Full network; Silver Network.
3 For the PPO level, self-referral to a PPO network physician. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Under Elect Open Access, radiographic X-ray and laboratory services will be covered only when provided or coordinated by
your primary care physician and approved by the PPG/IPA, except when provided at a PPO physician’s office or contracted PPO lab or facility.
6 Complex radiology (includes CT) requires a $100 copay under HMO and PPO. MRI, MUGA, PET and SPECT services are not covered through PPO level.
7 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 8 Under Elect Open Access, inpatient hospital and professional services, durable medical equipment and orthotics and prosthetics
are covered when provided or coordinated by the primary care physician only and approved by the PPG/IPA. Inpatient care and outpatient services are not covered on the PPO level.
9 Chiropractic and/or acupuncture rider coverage is available as an optional benefit with the EOA plan shown above. Features of Health Net’s chiropractic coverage include a $10 per visit copay and up to 20 visits per calendar year.
10 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific drug, go to www.healthnet.com.
11 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Hn PPO OPTIONS 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
(COI) for terms and conditions of coverage. 2 Insured pays the negotiated rate, which is the rate participating or preferred providers have agreed to accept for providing a
covered service. 3 Please refer to the Certificate of Insurance (COI) for out-of-network reimbursement methodology. 4 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 5 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%. 6 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 7 This deductible is only required for the first inpatient hospital or skilled nursing facility admission each calendar year. The
deductible does not apply to inpatient detoxification or to inpatient care for non-severe mental illness. Once the deductible is satisfied, no deductible is required for subsequent admissions in the same calendar year. This deductible is in addition to the plan calendar year deductible.
8 Once the outpatient surgery deductible is satisfied, no deductible is required for subsequent outpatient surgeries in the same calendar year. This deductible is in addition to the plan calendar year deductible.
9 Inpatient care for non-severe mental illness and inpatient chemical dependency rehabilitation is limited to a maximum allowable of $250 each day. Outpatient care for non-severe mental illness and outpatient chemical dependency rehabilitation has a maximum amount payable of $25 per visit.
10 Prescription drugs filled through mail order (up to a 90-day supply) require twice the level of copay. For details regarding a specific drug, go to www.healthnet.com.
11 The three prescription drug tiers are Tier 1: Generic formulary; Tier 2: Brand formulary; Tier 3: Brand nonformulary.
Flex Net 1 This is a summary of benefits. It does not include all services, limitations or exclusions. Please refer to the Certificate of Insurance
(COI) for terms and conditions of coverage. Flex Net is only available to out-of-area (OOA) subscribers, subject to standard OOA guidelines. Health Net must be the sole carrier.
2 Please refer to the Certificate of Insurance (COI) for reimbursement methodology. 3 Includes annual preventive physical, newborn and well-child care, well-woman exams, preventive lab and X-ray services. 4 Some services require prior certification. If prior certification is not acquired, the benefits are reduced to 50%. 5 Includes physical, speech, occupational, cardiac and pulmonary rehabilitation therapy. 6 Inpatient mental health and inpatient chemical dependency rehabilitation are limited to a combined maximum of 30 days for each
member in a calendar year. Outpatient mental health and outpatient chemical dependency rehabilitation has a maximum amount payable of $50 per visit.

6025248 CA82560 (7/11) Health Net of California, Inc., Health Net Life Insurance Company and Managed Health Network are subsidiaries of Health Net, Inc. Health Net, Health Net Elect and Salud con Health Net are registered service marks of Health Net, Inc. All other identified trademarks/service marks remain the property of their respective companies. All rights reserved.
For more information please contact
Health Net
PO Box 9103
Van Nuys, CA 91409-9103
Broker Services
1-800-448-4411, option 4
Small Business Group Sales and Service Administration
1-800-447-8812 (English)
1-877-891-9050 (Cantonese)
1-877-339-8596 (Korean)
1-877-891-9053 (Mandarin)
1-800-331-1777 (Spanish)
1-877-891-9051 (Tagalog)
1-877-339-8621 (Vietnamese)
Telecommunications device for the hearing and speech impaired
1-800-995-0852
Other optionsCoverage for individuals and families
1-800-909-3447
Coverage for family members over 65 years of age
1-800-944-7287
Coverage for children in a low-income household
1-800-327-0502
Coverage for businesses with 50+ employees
1-800-448-4411, option 4
www.healthnet.com


















