Sloft in ischio rectal abscess
15
SLOFT IN THE MANAGEMENT OF ISCHIO-RECTAL ABSCESS Dr D.U.Pathak MS FACRSI Shalby Hospital Jabalpur India
-
Upload
dilip-pathak -
Category
Health & Medicine
-
view
76 -
download
4
Transcript of Sloft in ischio rectal abscess
SLOFT IN THE MANAGEMENT OFISCHIO-RECTAL ABSCESS
Dr D.U.PathakMS FACRSI
Shalby Hospital Jabalpur India
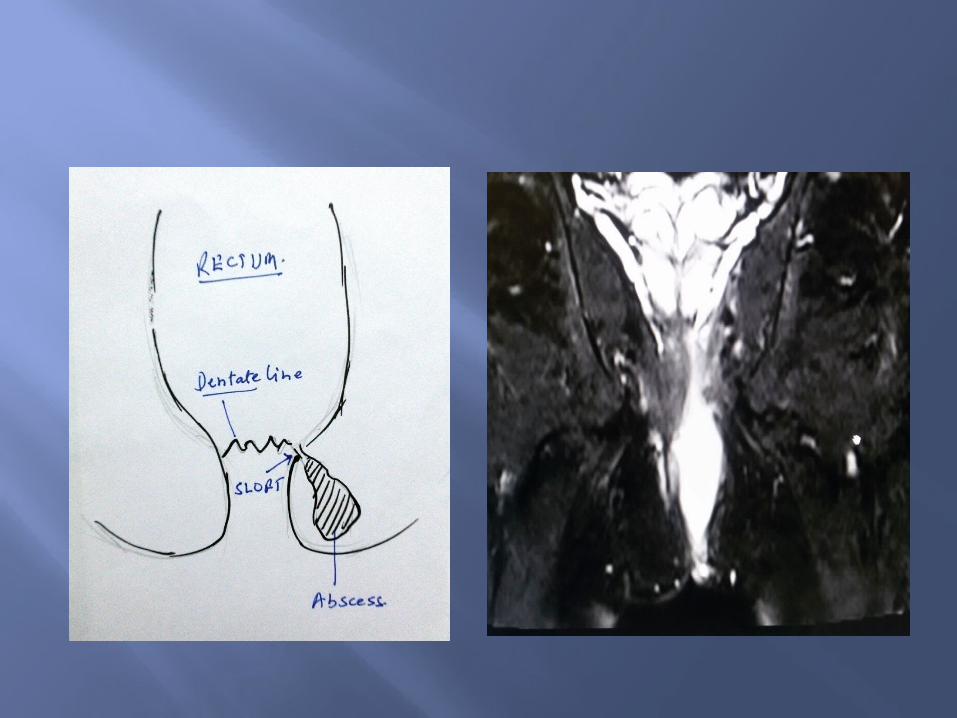
59 yrs Non diabetic male with clinically and on MRI detected as a case of acute Ischio-rectal abscess.

Treatment choices
I&D with de-roofing of the abscess cavity
Leaving internal opening with chances of Fistula formation later on in 50% of cases
Dealing with internal opening
Lay open Put in a Seton Ayurvedic kshar
sutra
Do nothing – with 50% chances of Fistula formation later on
LIFT not possible
Where LIFT is not possible ...
I&D and dealing internal opening with SLOFT effectively prevents fistula formation.
SLOFT is possible because the inherent anal duct, is transacted, near to the internal opening at dentate line .
With this breach in communication, de-roofing of the abscess cavity and wide excision of skin is un-necessary

Ischio-rectal abscess Abscess drained
near anal verge. Incision is cruciate
and small No de-roofing done Curettage done Pus sent for culture
sensitivity

Probing
Every Ischio-rectal abscess has an internal opening at dentate line
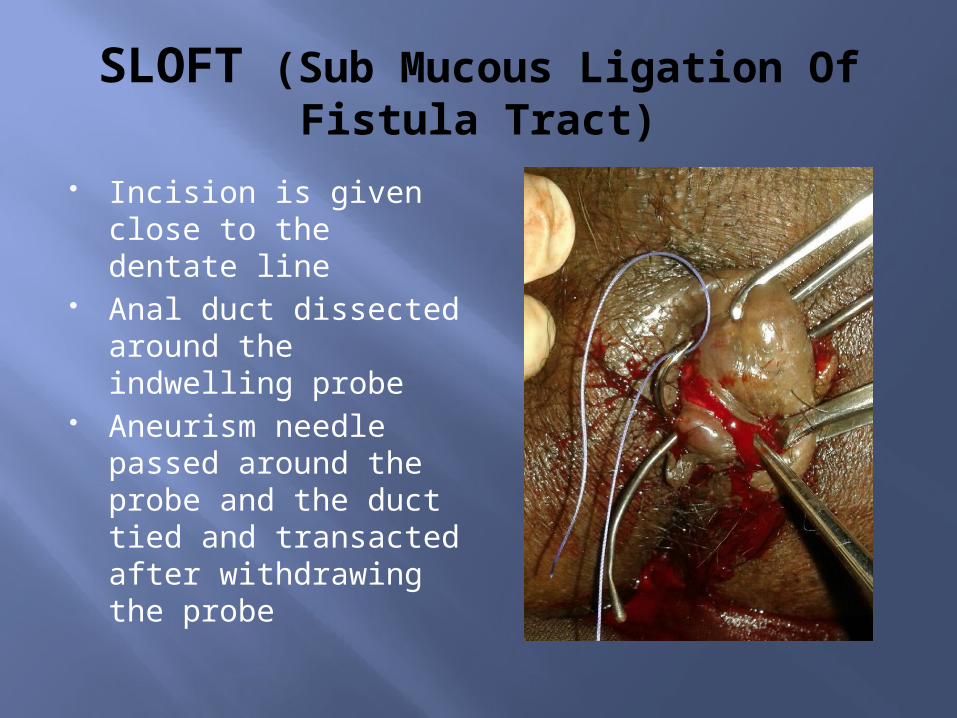
SLOFT (Sub Mucous Ligation Of Fistula Tract)
Incision is given close to the dentate line
Anal duct dissected around the indwelling probe
Aneurism needle passed around the probe and the duct tied and transacted after withdrawing the probe
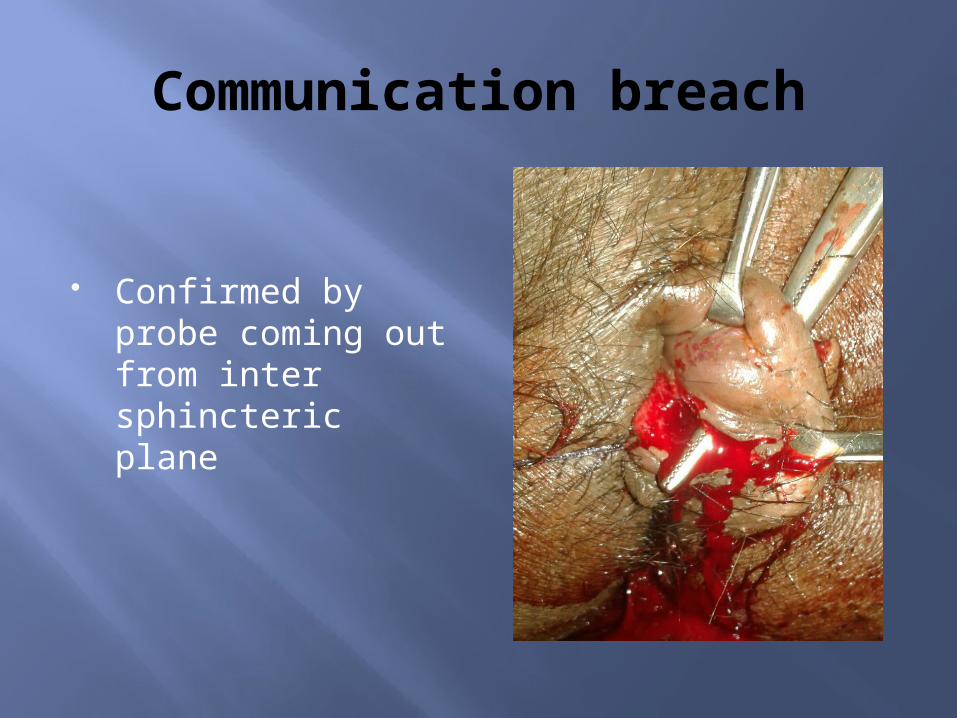
Communication breach
Confirmed by probe coming out from inter sphincteric plane
Post operative care
No dressings or packing of the wound
Only regular sitz bath and hygiene
Weekly follow ups

Conclusion
The SLOFT is an easy way to deal with the internal opening rather than to leave is and accepting the risk of 50% chances of Fistula formation
Normally the wound heals in 15-20 days

Post operative result after 48 hours
The cavity is collapsed.
Patient has no pain. Incision is almost
invisible. It is obvious that
there is no need of any post op care or follow up.
ThanksDr D.U.Pathak
(Cell and WhatsappNo - 94251-52747)