
Single Implant Supported Cantilever Prosthesis in the...
22
1 Single Implant Supported Cantilever Prosthesis in the esthetic zone – A new treatment approach. Mauricio Barreto, DDS, DMD, MSc 1 Carlos Eduardo Francischone, DDS, MSc, PhD 2 Hugo Nary Filho, DDS, MSc, PhD 3 1 Doctorate Student, Course on Implantology, Sagrado Coração University, Bauru, São Paulo, Brazil. 2 Titular Professor, Coordinator, Master of Science Degree Course on Implantology, Sagrado Coração University, Bauru, São Paulo, Brazil. 3 Assistant Professor, Coordinator, Master of Science Degree Course on Oral and Maxillofacial Surgery, Sagrado Coração University, Bauru, São Paulo, Brazil. Correspondence to: MAURICIO ANDRADE BARRETO AV.ACM,585 ED. ODONTOMEDICO LJ 35 SALVADOR, Bahia 41850-000 Telephone: (71) 3354 - 3344 e-mail – [email protected] www.implo.com.br
Transcript of Single Implant Supported Cantilever Prosthesis in the...

1
Single Implant Supported Cantilever Prosthesis in the esthetic zone –
A new treatment approach.
Mauricio Barreto, DDS, DMD, MSc1
Carlos Eduardo Francischone, DDS, MSc, PhD2
Hugo Nary Filho, DDS, MSc, PhD3
1Doctorate Student, Course on Implantology, Sagrado Coração University, Bauru, São Paulo, Brazil.
2Titular Professor, Coordinator, Master of Science Degree Course on Implantology, Sagrado
Coração University, Bauru, São Paulo, Brazil.
3Assistant Professor, Coordinator, Master of Science Degree Course on Oral and Maxillofacial
Surgery, Sagrado Coração University, Bauru, São Paulo, Brazil.
Correspondence to:
MAURICIO ANDRADE BARRETO
AV.ACM,585 ED. ODONTOMEDICO LJ 35
SALVADOR, Bahia 41850-000
Telephone: (71) 3354 - 3344
e-mail – [email protected]
www.implo.com.br

2
ABSTRACT
Background: Esthetic complications due to non harmonious periimplant soft tissue profiles
are common in the anterior maxilla, especially when two adjacent implants are found. This
controlled clinical studies evaluatied soft and hard tissue stability of a ten single implant supported
cantilever prosthesis.
Methods: Ten patients, 5 men e 5 women, with absence of the maxillary central and lateral
incisors were treated with a single implant supported cantilever prosthesis. The soft peri- implants
tissues were assessed using the Pink Esthetic Score (PES) described by Fürhauser et al. Assessment
of the level of peri- implant bone support were performed on radiographs taken 4 months after
implant placement, but immediately before implant exposition (baseline), and at the 6-months
follow-up (immediately after seating definitive prosthesis).
Results: The Pink Esthetic Score (PES) based on clinical photographs obtained 1 week after
seating definitive prosthesis is 9,22 (SD = 0,63). The crestal bone loss was - 0, 92 mm (SD = 0,8) at
6-moth follow-up (immediately after seating definitive prosthesis). The crestal bone level changes
for time interval was 1,42 mm (SD = 0,7).
Conclusions: The insertion of a single implant to replace two maxillary anterior teeth can
provide a more acceptable esthetic appearance of the periimplant soft tissue profile. The single
implant supported cantilever prosthesis was not able to prevent crestal bone loss More controlled
clinical studies are necessary to address soft and hard tissue stability in this treatment modality, as
well as studies to evaluate the mechanical performance of a single implant supported cantilever
prosthesis.
Keywords : dental papilla, gingival tissue, titanium implants, esthetic zone, implant-supported
prosthesis, cantilever

3
INTRODUCTION
Presence or absence of papillary tissue between adjacent teeth,1 implants or tooth-implant
interface2 has received a great deal of attention from clinicians over the last 15 years, since filling
most of the interproximal embrasure space by papillae is fundamental for achieving a pleasant
dentogingival composition3.
Reformation of natural-appearing sulcular and papilla anatomy between adjacent implants in
the esthetic zone presents a complex challenge for the implant team. The replacement of multiple
adjacent missing teeth in the anterior maxilla with fixed implant restorations is poorly documented.
In this context, esthetic restoration is not predictable, particularly regarding the contours of the
interimplant soft tissue4.
Tarnow et al.2 measured papillary height between adjacent implants and found an average of
3.4mm, ranging from 1 to 7mm. When these results are compared with the papillary height between
natural teeth (5mm)1, this represents a lack of 1-2mm, which leads to important esthetic issues in the
anterior maxillary zone2.
To overcome this problem, several suggestions have been made for preserving or regaining
soft tissue integrity in the esthetic zone, through surgical5-8 or prosthetic9,10 procedures. However,
there is still an increasing demand for scientific investigation in this area.
The clinical situation in this article refers to the absence of two contiguous teeth in the
esthetic zone: the upper central and lateral incisors (Figs 1a and b). The therapeutic suggestion is to
insert two implants, but keeping the implant from the upper lateral incisor submerged and unloaded
prosthetics. The hypothesis to be proved is that this procedure can generate a better clinical
performance.
The biological rationale for this recommendation is based on the understanding of the
formation of the biologic space around titanium implants11. It is known that after the titanium
implant is exposed to the oral medium, a rapid reabsorption of the bone crest around the platform is
observed. Therefore, the exposure to the oral environment of single implant supported cantilever
prosthesis could make it possible to preserve the interdental papilla and gingival outline, there would
be at the crest bone reabsorption around the platform of the second implant.

4
a b
Figs 1a and 1b - Treatment of the absence of two adjacent teeth in the anterior maxilla, with
titanium implants. In the clinical case on the left (a) two contiguous implants were inserted and a
deficiency of the interdental papilla was observed. In the clinical case on the right (b) a single
implant exposed to the oral cavity and the presence of interdental papilla and a more harmonious
gingival outline were observed.
Therefore, clinicians must be careful during implant treatment planning in partially
edentulous patients, because two adjacent implants pose a greater esthetic risk due to gingival tissue
contours being less predictable.
The aim of this article is evalue soft/ hard implant tissue of a ten single implant supported
cantilever prosthesis in the anterior maxilla.
M ATERIAL AND METHODS
Clinical procedures
Ten patients, 5 men e 5 women, with absence of the maxillary central and lateral incisors are
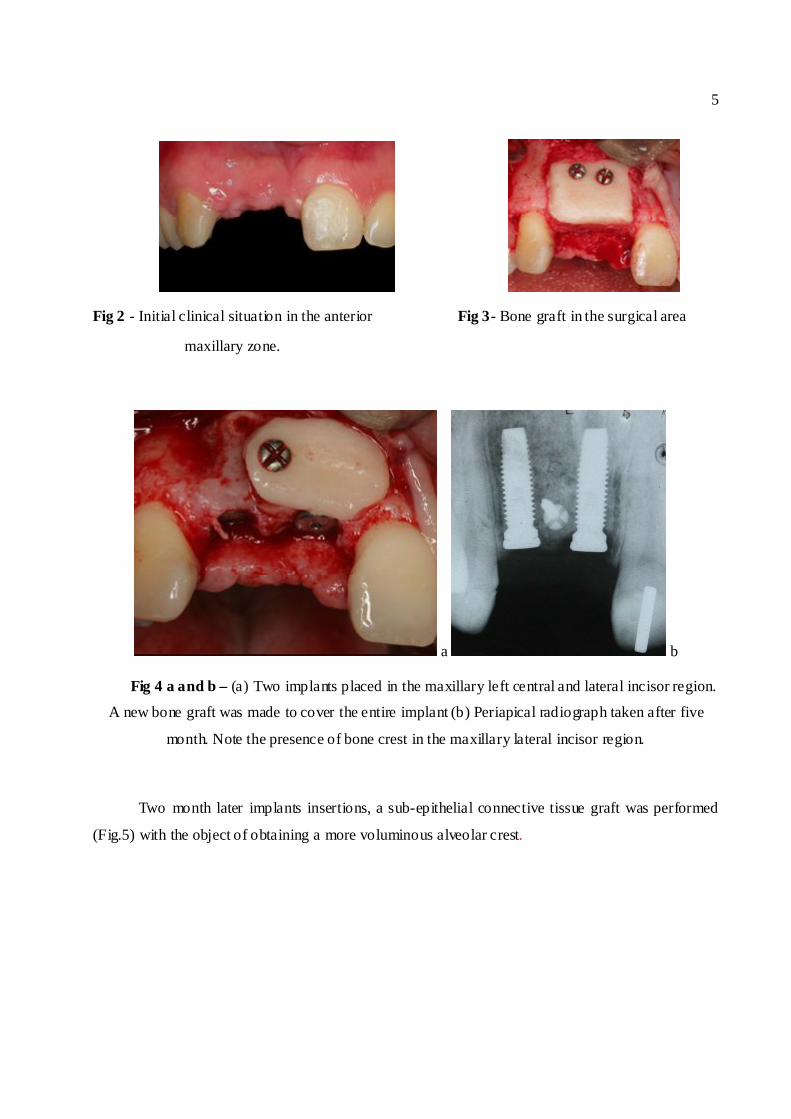
randomly select (Fig 2). After adequate surgical and prosthetic planning, a bone graft was made to
augment the width of the alveolar bone crest, using the mandibular ramus as a donor site (Fig 3).
Four months later, a commercially pure titanium implant (PI Philosophy™, São Paulo, Brazil) was
placed in the maxillary central and lateral incisor region (Fig 4). The average distance between the
implants installed is of 3.58 mm (SD = 0.62).
The implant complied with the following specifications: platform diameter: 4.1mm, external
hexagon width: 2.7mm, external hexagon height: 0.71mm.
5
Fig 3- Bone graft in the surgical area
a b
Fig 4 a and b – (a) Two implants placed in the maxillary left central and lateral incisor region.
A new bone graft was made to cover the entire implant (b) Periapical radiograph taken after five
month. Note the presence of bone crest in the maxillary lateral incisor region.
Two month later implants insertions, a sub-epithelial connective tissue graft was performed
(Fig.5) with the object of obtaining a more voluminous alveolar crest.
Fig 2 - Initial clinical situation in the anterior
maxillary zone.

6
a b c
Four months later, the implant in the maxillary central incisor region was exposed and a
provisional cantilever fixed partial denture (FPD) (Fig 6) was made, using a titanium prosthetic
component screwed into the implant platform (UCLA Titanium, PI Philosophy ™ , São Paulo,
Brazil) and self-polymerizable acrylic (Jet Classic, São Paulo- Brazil). To obtain the plaster model, a
mold was made using a polyether based material (3M ESPE Impregum Soft), and a personalized
individual mold made of self-polymerizable acrylic (Jet Classic, São Paulo- Brazil). The opposing
dentition impression was made using an irreversible hydrocolloid. The soft tissue was conditioned
by means of successive compression cycles by adding self-polymerizable acrylic resin to the cervical
portion of the FPD (Fig 7).
a b c
Fig. 6 a to c- Clinical photograph showing the implant exposed (a), a fabricated FDP (b and c) in
a laboratory situation.
Fig. 5 a to c. Sub-epithelial connective tissue graft procedure performed
with the object of obtaining a more voluminous alveolar crest.

7
a b c
When a period of 90 days after performing the subepithelial connective tissue graft had
elapsed, procedures to make the definitive denture were started. Thus a new polyether mold (3M
ESPE Impregum Soft) of the maxillary arch and a personalized individual mold were made. For
correct molding of the peri-implant soft tissue, the provisional denture was used to personalize an
impression coping with self-polymerizable acrylic (Duralay II, Reliance, Worth, IL) (Fig 8).
a b
Figs 7a and b – Clinical photographs showing the emergency profile in the central incisor
region (a) and a fabricated FDP inserted (b). Periapical radiograph taken 3 months after the FDP
was inserted. Note the presence of bone crest in the maxillary lateral incisor region (c).
Fig. 8a and b - Molding for making the definitive denture. Observe that the correct
molding of the peri- implant soft tissue was obtained by means of personalizing the
molding component.

8
A screw retained zirconia metal- free framework was made (ZircozanT M Italy) (Fig 9). The
screw retained definitive prosthesis (Fig. 10) was inserted 5 months after the surgical procedures.
Occlusal adjustment was made in order to maintain a slight occlusal contact in the maximum
intercuspation position, and an anterior guide with concomitant contacts on the two central incisors.
An endeavor was made to avoid occlusal contacts on the maxillary left lateral incisor (cantilever).
a b
Figs 10a and b – Final prosthesis inserted. Note that the interdental papilla is more coronal in
relation to the contra lateral counterpart.
Fig. 9 - All-ceramic zirconia framework in position.

9
Fig 11 - Periapical radiograph taken 1 immediately after the definitive prosthesis was inserted. Note
the presence of bone crest in the maxillary lateral incisor region.
Evaluation of soft peri-implants tissues:
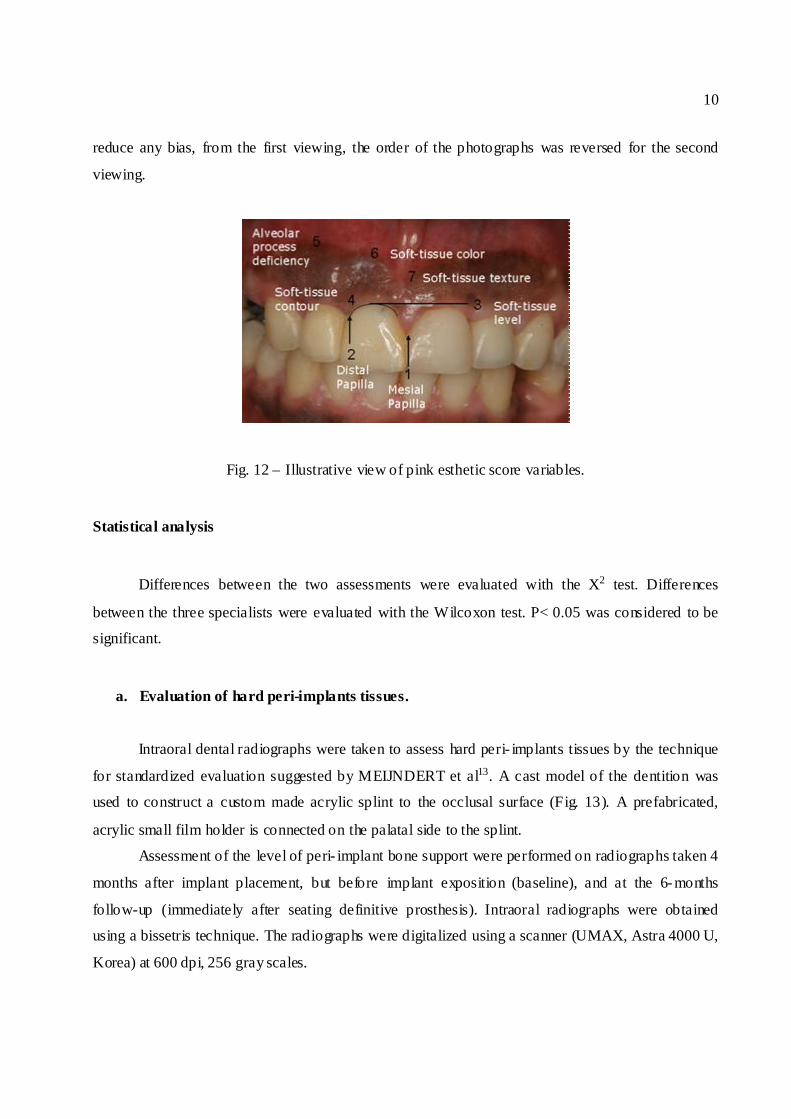
The soft peri- implants tissues were assessed using the Pink Esthetic Score (PES) described
by Fürhauser et al12. The PES is based on seven variables: mesial papilla, distal papilla, soft-tissue
level, soft-tissue contour, alveolar process deficiency, soft-tissue color and texture (Fig. 12). Each
variable was assessed with a 2-1-0 score, with 2 being the best and 0 the poorest score. Clinical
photographs (20 D digital camera, Cannon, 100 mm lens and circular flashes) of ten single implant
supported cantilever prosthesis in the anterior maxilla were evaluated. All of them replaced central
and lateral incisor. Photographs were obtained 1 week after seating definitive prosthesis (10
photographs). For assessing anterior teeth replacements, the contra lateral reference teeth had to be
visible well enough to ensure comparability. The photographs were magnified to twice the original
size, printed out on A4 sheets together with the list of variables. Implant-supported crows were
marked by arrows. All photographs were developed and processed by the same person. Blinded
evaluation of clinical photographs was carried out by specialists who had not been involved in the
treatment. The questionnaire was handed to 3 individuals of variable specialization (1 prosthodontist,
1 oral surgeon and 1 dental student). Assessments were made twice at an interval of 4 weeks. To
10
reduce any bias, from the first viewing, the order of the photographs was reversed for the second
viewing.
Fig. 12 – Illustrative view of pink esthetic score variables.
Statistical analysis
Differences between the two assessments were evaluated with the X2 test. Differences
between the three specialists were evaluated with the Wilcoxon test. P< 0.05 was considered to be
significant.
a. Evaluation of hard peri-implants tissues.
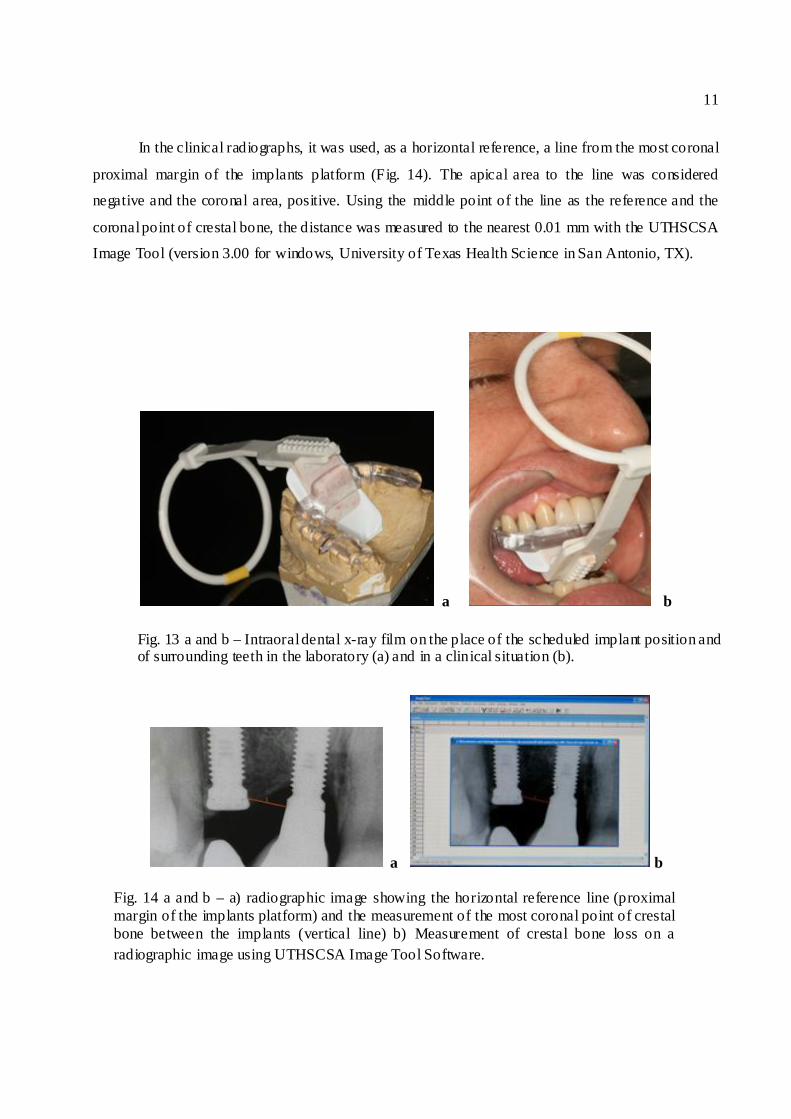
Intraoral dental radiographs were taken to assess hard peri- implants tissues by the technique
for standardized evaluation suggested by MEIJNDERT et al13. A cast model of the dentition was
used to construct a custom made acrylic splint to the occlusal surface (Fig. 13). A prefabricated,
acrylic small film holder is connected on the palatal side to the splint.
Assessment of the level of peri- implant bone support were performed on radiographs taken 4
months after implant placement, but before implant exposition (baseline), and at the 6-months
follow-up (immediately after seating definitive prosthesis). Intraoral radiographs were obtained
using a bissetris technique. The radiographs were digitalized using a scanner (UMAX, Astra 4000 U,
Korea) at 600 dpi, 256 gray scales.
11
In the clinical radiographs, it was used, as a horizontal reference, a line from the most coronal
proximal margin of the implants platform (Fig. 14). The apical area to the line was considered
negative and the coronal area, positive. Using the middle point of the line as the reference and the
coronal point of crestal bone, the distance was measured to the nearest 0.01 mm with the UTHSCSA
Image Tool (version 3.00 for windows, University of Texas Health Science in San Antonio, TX).
a b
a b
Fig. 13 a and b – Intraoral dental x-ray film on the place of the scheduled implant position and of surrounding teeth in the laboratory (a) and in a clinical situation (b).
Fig. 14 a and b – a) radiographic image showing the horizontal reference line (proximal margin of the implants platform) and the measurement of the most coronal point of crestal bone between the implants (vertical line) b) Measurement of crestal bone loss on a radiographic image using UTHSCSA Image Tool Software.
12
RESULTS
Soft peri- implants tissues:
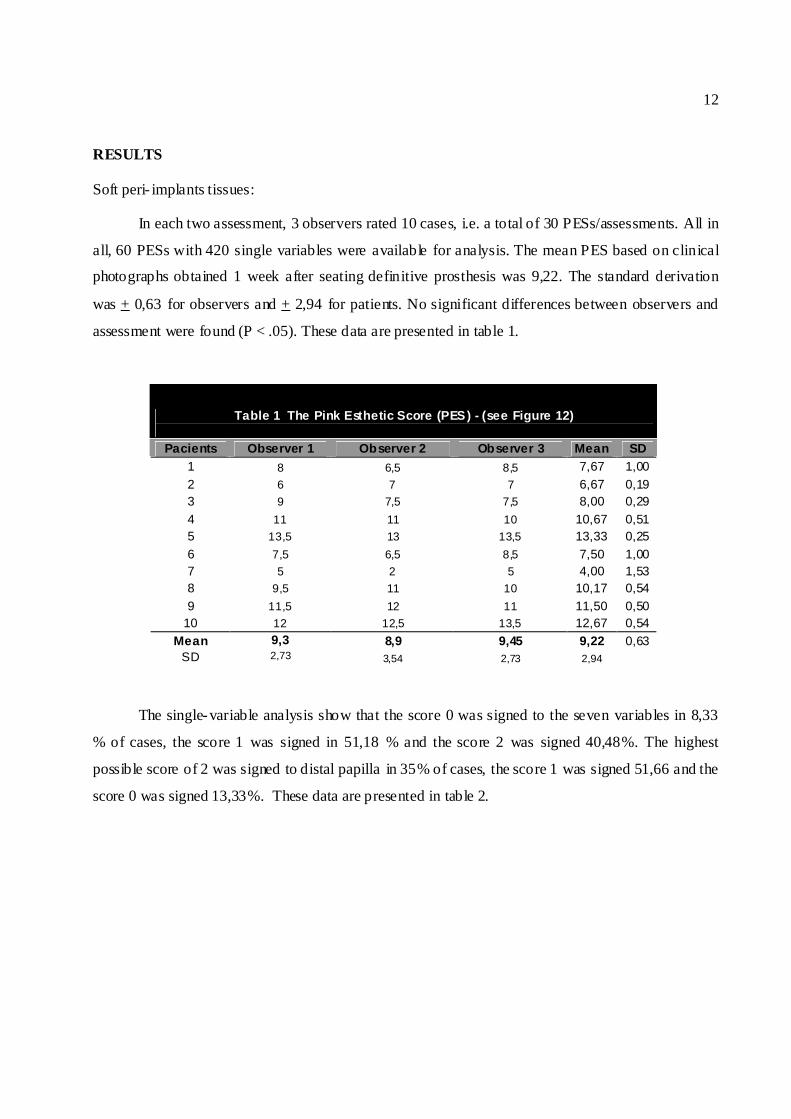
In each two assessment, 3 observers rated 10 cases, i.e. a total of 30 PESs/assessments. All in
all, 60 PESs with 420 single variables were available for analysis. The mean PES based on clinical
photographs obtained 1 week after seating definitive prosthesis was 9,22. The standard derivation
was + 0,63 for observers and + 2,94 for patients. No significant differences between observers and
assessment were found (P < .05). These data are presented in table 1.
Table 1 The Pink Esthetic Score (PES) - (see Figure 12)
Pacients Observer 1 Observer 2 Observer 3 Mean SD 1 8 6,5 8,5 7,67 1,00 2 6 7 7 6,67 0,19 3 9 7,5 7,5 8,00 0,29 4 11 11 10 10,67 0,51 5 13,5 13 13,5 13,33 0,25 6 7,5 6,5 8,5 7,50 1,00 7 5 2 5 4,00 1,53 8 9,5 11 10 10,17 0,54 9 11,5 12 11 11,50 0,50
10 12 12,5 13,5 12,67 0,54 Mean 9,3 8,9 9,45 9,22 0,63
SD 2,73 3,54 2,73 2,94
The single-variable analysis show that the score 0 was signed to the seven variables in 8,33
% of cases, the score 1 was signed in 51,18 % and the score 2 was signed 40,48%. The highest
possible score of 2 was signed to distal papilla in 35% of cases, the score 1 was signed 51,66 and the
score 0 was signed 13,33%. These data are presented in table 2.

13
Table 2 Frequency of variable assessment of score s 0, 1 and 2.
Variable Score 0 Score 1 Score 2 No. % No. % No. %
Mesial papilla 10 16,66 26 43,33 24 40 Distal Papilla 8 13,33 31 51,66 21 35
Alveolar process 5 8,33 19 31,66 36 60 Soft-tissue texture 5 8,33 34 56,66 21 35 Soft-tissue contour 5 8,33 31 51,66 24 40 Soft-tissue collor 0 0 37 61,66 23 38,33
Level of Soft-tissue margin 2 3,33 37 61,66 21 35 Mean 5,00 8,33 30,71 51,18 24,29 40,48
SD 3,37 5,61 6,45 10,75 5,35 8,91
b. Hard peri-implants tissues.
The crestal bone loss was - 0, 92 mm (+ 0,8 SD) at 6-moth follow-up (immediately after
seating definitive prosthesis). The crestal bone level changes for time interval was 1,42 mm (+ 0,7
SD). These data are presented in table 3. ,
Table 3 Crestal Bone Level (mm) Changes for Different Time Interval (see Figure 14)
Pacients Baseline Follow-up 6-month Difference 1 1,27 -1,18 2,45 2 0,98 0,88 0,1 3 0,54 -1,06 1,6 4 0,27 -0,58 0,85 5 0 -1,12 1,12 6 0,7 -1,6 2,3 7 1,39 -0,42 1,81 8 0 -0,93 0,93 9 -0,53 -2,19 1,66
10 0,41 -1 1,41 Mean 0,50 -0,92 1,42 SD 0,6 0,8 0,7

14
DISCUSSION
Soft tissue behavior
The soft tissue profile is a fundamental factor in the esthetic appearance of implant
prostheses. But how can a single implant replacing two adjacent teeth contribute to stabilizing the
gingival tissue contours? This explanation is perhaps found when one understands the biologic width
around implants.11 It is well known that bone loss near the implant platform is observed just after the
second stage surgery.14 The bone resorption process takes place in an apical and lateral direction15;
magnitude of bone loss is dependent on several factors, among others, the periodontal biotypes 16,
prosthetic load17 implant type14 and initial implant position18.
Why is the gingival contour difficult to maintain in the presence of two adjacent implants
exposed? First, we have to consider that the edentulous alveolar ridge is flat and no bone crest is
observed under the gingival papilla, as seen between two adjacent natural teeth. Thus, a second
exposed adjacent implant is problematic, because it contributes to the lateral bone loss in the implant
platform, thus decreasing the bone crest height between the implants even further15. In the single-
implant technique, the chance of a more stable alveolar ridge increases.
In the present study, the evaluation of ten single implant supported cantilever prosthesis in
the anterior maxilla, there was a PES average of 9.22 (+ 2.94 SD). In 2000, Fürhauser et all12
showed the mean PES at first assessment (n = 600) was 9.46 (+ 3.81 SD) and 9.24 (+ 3.8 SD) at the
second one to assess 30 single-tooth implant crows. Thus we can conclude, based on the sample
submitted, that insertion of one implant to replace two adjacent teeth demonstrates the same effects
as those observed at implant-supported single-tooth replacements. This hypothesis, if proved
scientifically in the future based on more randomized controlled clinical studies, could represent a
new esthetic parameter for the treatment of absence of two contiguous teeth in the anterior maxilla.
The single-variable analysis showed the lowest possible score of 0 was assigned to the mesial
papilla in 16.66% of cases and to the distal papilla in 13.33%. These data are in agreement with
other publications19, 20 that reported the achievement of gingival papilla as the major obstacle of
osseointegration. However, in this study, most patients received scores 1 and 2 in the gingival
papillae, demonstrating that a single implant supported cantilever prosthesis can provide satisfactory
cosmetic results.

15
Hard tissue behavior
The crestal bone loss was - 0, 92 mm (+ 0.8 SD) at 6-moth follow-up (immediately after
seating definitive prosthesis) and the crestal bone level changes for time interval was 1,42 mm (+ 0.7
SD). Based on these data, we can say that single implant supported cantilever prosthesis was not able
to prevent crestal bone loss. It is important to emphasize that the second implant installed in the
upper lateral incisor was kept covered by gingival tissue, and is not therefore subject to load
prosthetics.
These data are consistent to those seen by Tarnow et all15 in 2000 that assessed the effect of
inter- implant distance on height of inter- implant bone crest when we have two adjacent implants
exposed to the oral cavity. In Tarnow’s study, the crestal bone loss for implants with a greater than 3
mm distance between them was 0,45mm, while the implants that had a distance of 3mm or less
between them had a crestal bone loss of 1.04 mm. Therefore, we can say that single implant
supported cantilever prosthesis made a crestal bone loss similar to that observed when two implants
had a distance of 3 mm or less between them. How to explain this fact? Firstly, it is important to
remember that most patients were subjected to increased bone vertical through autogenous bone
graft. For the concept of vertical ridge augmentation to enable dental implant placement, there are
clinical and histological data supporting its potential use. However, this procedure in order to
improve the aesthetics is poorly documented21, 22. Another possibility is bacterial contamination of
the implant covered by gingival tissue23. Furthermore, the surgical trauma of insertion of the second
implant may explain the crestal bone loss.
Despite the crestal bone loss observed, this study showed that the aesthetic end of treatment
was satisfactory. To speculate that it may, under the conditions of the study, the implant installed in
the upper lateral Incisor played the mechanical support of soft tissue, thus keeping the volume of soft
tissue compatible with an aesthetically pleasing result.
The validity of the use of the second implant submerged
In the present study, 2 implants were installed: one in the upper central incisor and another in
the region of upper lateral incisor. The second implant was left submerged and unloaded prosthetics.
It is the use of the implant submerged for two reasons: first, by a lack of scientific evidence to
recommend the use of single implant supported cantilever prosthesis in humans, during a

16
complication of biomechanics, we would have the second available to support prosthetic implant.
The second justification is based on clinical observation: It is observed that around fixing screws
bone graft, bone has a lower degree of bone resorption (Fig.15). Thus, it was this same effect with
the implant submerged. In the present study, bone loss occurred around the implant covered by
gingival tissue in some patients (Fig. 16).
a b
Fig . 15 - Clinical photographs showing bone graft surgery. b) Upon the establishment of the graft.
b) After 4 months. Note the large bone resorption and maintenance of bone tissue around the screws
for fixing the graft.
Fig 16. Periapical radiograph taken immediately after the definitive prosthesis was inserted. Note
bone loss around the implant in the left lateral incisor.

17
Thus, one can say that the implant not exposed to the oral cavity was not effective in
preventing bone resorption. Moreover, as discussed earlier, the final aesthetic result of the treatment
was satisfactory. It is speculated, then, that the submerged implant may play the role of mechanical
support of soft tissues. If this hypothesis is proven in the future, you can construct solid cylinders of
titanium for mechanical support of soft tissues, which in theory would be less susceptible to bacterial
contamination.
Implant connection type
In the periapical radiographs of the two clinical cases described in this article, it was possible
to observe a circumferential radiolucent area close to the implant platform, compatible with the
biologic width around titanium implants11. Several advances have been described to maintain the
bone crest around implants by macro and microanatomic implant modifications.24, 25, 26.
Several implant manufacturers evoke their clinical superiority for maintaining optimal bone
crest levels, but there is a lack of extensive clinical documentation on this topic.27 Despite this, it is
expected that new designs will be able to keep desirable bone levels around the implant platforms.
Thus, unless new implant designs demonstrate the same bone crest/coronal root portion
relationships, the clinician should consider the use of a single implant to replace two lost adjacent
teeth in the anterior maxilla, because it is thought that this procedure could result in better clinical
performance.
Framework
High-strength all-ceramic systems for fixed partial dentures (FPDs) are available for
replacing missing teeth. New core/framework materials have been developed and have evolved in
the last decade28. All-ceramic systems are a focus of interest, because they offer aesthetic results
that may be difficult to achieve with metal-ceramic systems. Nowadays, the new ceramics associate
good esthetic and mechanical qualities, biocompatibility and accurate marginal fit.29, 30. But what is
the best material for making the framework of single implant supported cantilever prosthesis? From
the mechanical point of view, one could speculate that metal-ceramic bridges are preferably
indicated due to their predictable characteristics of long-term strength. All-ceramic systems can be
recommended for anterior bridges, especially if highly satisfactory esthetic results are required.

18
There are no studies that make reference to the use of implant-supported all-ceramic restorations
applied in a single implant supported cantilever prosthesis. Further studies should be conducted for
detailed evaluation of the clinical performance of all-ceramic systems for fixed partial dentures
(FPDs)31 and single implant supported cantilever prosthesis.
Biomechanical risks
The number of implants and their length, as well as bone quality, occlusal pattern and
prosthesis design are fundamental to the biomechanical integrity of an implant prosthesis.32 With
regard to the possible biomechanical risks, is it safe to plan a single implant supported cantilever
prosthesis in the anterior maxilla?
Barreto et al33 assess the unscrewing and alignment torque of the screw of an implant
supported denture with pillar and cantilever by means of a fatigue test. Torque and detorque were
measured before cycling fatigue three times, with intervals of two minutes between measurements
and a single time after cycling. In the screwed group, the mean initial detorque value was 25.2 +
2.9N/cm and final detorque value was 22.7 ± 0.9N/cm (p=0.049 Wilcoxon Test). In the cemented
group, the mean initial detorque value was 27.67 + 1.92N/cm and final detorque value was 24.7 +
1.55N/cm. (p=0.002 paired t-Test). Significant difference was observed between the pre-fatigue
mean detorque values and the post-fatigue detorque value in both groups. No significant alterations
were found in the denture screw alignment. In spite of the reduction in the unscrewing torque, there
was no slackening and loosening of screws.
Even with the lack of scientific evidences, some factors point out to a favor their treatment
option: The occlusal forces in the anterior region are less than half the value observed in the
posterior region;34 manufacturers constantly seek to develop implants that present more bone to
implant contact, which could increase due to their anchorage35; a thorough occlusal adjustment with
slight contact in the maximum intercuspation, with unimpeded lateral and protrusive excursive
movements around the implant; and excluding patients with parafunctional habits and class II and
class III malocclusion36 from this type of treatment, are factors that can determine the
biomechanical longevity of single implant supported cantilever prosthesis.

19
CONCLUSION
The insertion of a single implant to replace two maxillary anterior teeth can provide a more
acceptable esthetic appearance of the periimplant soft tissue profile. The single implant supported
cantilever prosthesis was not able to prevent crestal bone loss More controlled clinical studies are
necessary to address soft and hard tissue stability in this treatment modality, as well as studies to
evaluate the mechanical performance of a single implant supported cantilever prosthesis.
REFERENCES
1. Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the
crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol
1992;63: 995-996.
2. Tarnow DP, Elian N, Fletcher P, Froum S, Magner AW, Cho S et al. Vertical distance from
the crest of bone to the height of the interproximal papilla between adjacent implants. J
Periodontol 2003;74:1785-1788.
3. Leblebicioglu B, Rawal S, Mariotti A. A review of the functional and esthetic requirements
for dental implants. J Am Dent Assoc. 2007 Mar;138(3):321-9. Review.
4. Belser UC, Schmid B, Higginbottom F, Buser D. Outcome analysis of implant restorations
located in the anterior maxilla: a review of the recent literature. Int J Oral Maxillofac
Implants. 2004;19 Suppl:30-42. Review.
5. Steigmann M, Wang HL. Esthetic buccal flap for correction of buccal fenestration defects
during flapless immediate implant surgery. J Periodontol;77:517-22, 2006.
6. Oh TJ, Shotwell JL, Billy EJ, Wang HL. Effect of flapless implant surgery on soft tissue
profile: a randomized controlled clinical trial. J Periodontol;77:874-82, 2006.
7. Nasr HF. Current methods for soft tissue enhancement of the esthetic zone. Atlas Oral
Maxillofac Surg Clin North Am 2006;14:39-49.
8. Scarso J, Barreto M, Tunes U. Planejamento estético, cirúrgico e protético em
implantodontia. Ed. Artes Médicas, 2001.
9. Lesage BP. Improving implant aesthetics: prosthetically generated papilla through tissue
modeling with composite. Pract Proced Aesthet Dent 2006;18:257-63.
20
10. Donitza A. Prosthetic procedures for optimal aesthetics in single-tooth implant restorations: a
case report. Pract Periodontics Aesthet Dent 2000;12:347-52.
11. Hermann JS, Buser D, Schenk RK, Higginbottom FL, Cochran DL. Biologic width around
titanium implants. A physiologically formed and stable dimension over time. Clin Oral
Implants Res 2000;11:1-11.
12. Fürhauser R, Florescu D, Benesch T, Haas R, Mailath G, Watzek G. Evaluation of soft tissue
around single-tooth implant crowns: the pink esthetic score. Clin Oral Implants Res 2005
Dec; 16(6) :639-44.
13. Meijndert L, Meijer HJ, Raghoebar GM, Vissink A. A technique for standardized evaluation
of soft and hard peri- implant tissues in partially edentulous patients. J Periodontol. 2004
May;75(5):646-51.
14. Hermann JS, Buser D, Schenk RK, Schoolfield JD, Cochran DL. Biologic Width around one-
and two-piece titanium implants. Clin Oral Implants Res. 2001 Dec;12(6):559-71.
15. Tarnow DP, Cho SC, Wallace SS. The effect of inter- implant distance on the height of inter-
implant bone crest. J Periodontol. 2000 Apr;71(4):546-9.
16. Sanavi F, Weisgold AS, Rose LF. Biologic width and its relation to periodontal biotypes. J
Esthet Dent. 1998;10(3):157-63.
17. Duyck J, Rønold HJ, Van Oosterwyck H, Naert I, Vander Sloten J, Ellingsen JE. The
influence of static and dynamic loading on marginal bone reactions around osseointegrated
implants: an animal experimental study. Clin Oral Implants Res. 2001 Jun;12(3):207-18.
18. Hartman GA, Cochran DL. Initial implant position determines the magnitude of crestal bone
remodeling. J Periodontol. 2004 Apr;75(4):572-7.
19. Pradeep AR, Karthikeyan BV. Peri- implant papilla reconstruction: realities and limitations. J
Periodontol. 2006 Mar;77(3):534-44
20. Elian N, Jalbout ZN, Cho SC, Froum S, Tarnow DP. Realities and limitations in the
management of the interdental papilla between implants: three case reports.. Pract Proced
Aesthet Dent. 2003 Nov-Dec;15(10):737-44; quiz 746. Review
21. Clinical outcomes of vertical bone augmentation to enable dental implant placement: a
systematic review. Rocchietta I, Fontana F, Simion M. J Clin Periodontol. 2008 Sep;35(8
Suppl):203-15. Review.

21
22. Esposito M, Grusovin MG, Coulthard P, Worthington HV. The efficacy of various bone
augmentation procedures for dental implants: a Cochrane systematic review of randomized
controlled clinical trials.. Int J Oral Maxillofac Implants. 2006 Sep-Oct;21(5):696-710.
Review
23. Barboza EP, Caúla AL, Carvalho WR. Crestal bone loss around submerged and exposed
unloaded dental implants: a radiographic and microbiological descriptive study. Implant
Dent. 2002;11(2):162-9.
24. Holt RL, Rosenberg MM, Zinser PJ, Ganeles J. A concept for a biologically derived,
parabolic implant design. Int J Periodontics Restorative Dent. 2002 Oct;22(5):473-81
25. Glauser R, Schüpbach P, Gottlow J, Hämmerle CH. Periimplant soft tissue barrier at
experimental one-piece mini- implants with different surface topography in humans: A light-
microscopic overview and histometric analysis. Clin Implant Dent Relat Res. 2005;7 Suppl
1:S44-51.
26. Hermann F, Lerner H, Palti A. Factors influencing the preservation of the periimplant
marginal bone. Implant Dent. 2007 Jun;16(2):165-75.
27. Eckert SE, Choi YG, Sánchez AR, Koka S. Comparison of dental implant systems: Quality
of clinical evidence and prediction of 5-year survival. Int J Oral Maxillofac Implants
2005;20:406-415.
28. Raigrodski AJ. Contemporary materials and technologies for all-ceramic fixed partial
dentures: a review of the literature. J Prosthet Dent. 2004 Dec;92(6):557-62. Review
29. Sadan A, Blatz MB, Lang B. Clinical considerations for densely sintered alumina and
zirconia restorations: Part 1. Int J Periodontics Restorative Dent. 2005 Jun;25(3):213-9.
30. Sadan A, Blatz MB, Lang B. Clinical considerations for densely sintered alumina and
zirconia restorations: part 2. Int J Periodontics Restorative Dent. 2005 Aug;25(4):343-9.
31. Wassermann A, Kaiser M, Strub JR. Clinical long-term results of VITA In-Ceram Classic
crowns and fixed partial dentures: A systematic literature review. Int J Prosthodont. 2006 Jul-
Aug;19(4):355-63. Review.
32. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants
in the treatment of the edentulous jaw. Int J Oral Surg, 1981;10:387-416.
33. Barreto M, Francischone CE, Rosseti P, Laurenti JA. Mechanical evaluation of an single
implant supported cantilever prosthesis by a cyclic load test. Quintecensse Int. In press.

22
34. Gibbs CH, Mahan PE, Mauderli A, Lundeen HC, Walsh EK. Limits of human bite strength.J
Prosthet Dent. 1986 Aug;56(2):226-9.
35. Albrektsson T, Wennerberg A. Oral implant surfaces: Part 1--review focusing on topographic
and chemical properties of different surfaces and in vivo responses to them. Int J
Prosthodont. 2004 Sep-Oct;17(5):536-43.
36. Kim Y, Oh TJ, Misch CE, Wang HL. Occlusal considerations in implant therapy: clinical
guidelines with biomechanical rationale. Clin Oral Implants Res. 2005 Feb;16(1):26-35.
Review


















