Simultaneous surgical repair of post-infarct ventricular septal … · 2017-10-17 · 3 weeks...
4
Case Report 70 Journal-Cardiovascular Surgery 2015:3(3):70-73 doi; 10.5455/jcvs.20142x20 Yucel et al. Simultaneous surgical repair of post-infarct ventricular septal defect, left ventricular aneurysm and coronary artery disease Simultaneous surgical repair of post-infarct ventricular septal defect, left ventricular aneurysm and coronary artery disease Ertan Yucel 1 , Kanat Ozisik 2 , Ozgur Ersoy 3 , Omer Ulular 3 , Zeki Temizturk 3 , Kasım Karapinar 3 1 Department of Cardiovascular Surgery, Diskapi Yildirim Beyazid Training & Research Hospital, Ankara, Turkey, 2 Department of Cardiovascular Surgery, Kafkas University Medical School, Kars, Turkey, 3 Department of Cardiovascular Surgery, Diskapi Yildirim Beyazid Training & Research Hospital, Ankara, Turkey *Corresponding Author: Kanat Özışık, Department of Cardiovascular Surgery, Kafkas University Medical School, Kars, Turkey. e-mail: [email protected] Key words: Coronary artery disease; heart aneurysm; heart septal defects, ventricular Received: 20.07.2014 Accepted: 16.09.2014 e-published: 18.12.2014 Abstract A 52-year-old patient was admitted in our hospital for postinfarction ventricular septal defect (VSD), left ventricular aneurysm and coronary artery disease. He was investigated by echocardiography and coronary angiography and proposed for operation. In the light of the patient’s stable hemodynamic condition, surgical intervention was delayed. 3 weeks following the acute myocardial infarction open heart surgery was performed and had been managed just pre-operatively with an intra-aortic balloon pumping. The patient underwent successful VSD closure with a patch. The repair involves VSD closure and infarct exclusion technique. The patient discharged 10 days postoperatively. We consider that this modification is a simple and effective way to decrease the surgical risk of postinfarction VSD. Introduction Postinfarction ventricular septal defect (VSD) and left ventricular aneurysm (LVA) are highly lethal complications of acute myocardial infarction (MI) with an incidence of 1-2% and 8-10%, respectively [1-3]. The surgical repair of postinfarction VSD is mandatory. After confirming diagnosis and evaluation of coronary arteries prompt attempts should be done to stabilize the patient since postinfarction VSD clo- sure should be performed 4-5 weeks after MI. Surgical repair of VSD is accompanied by technical difficulties due to the weakness and unclear border of infarcted myocardial tissue. Although numerous techniques and materials have been used to close postinfarction VSDs, the best technique has not yet been settled upon [4,5]. We present the case of a patient who underwent success- ful correction of postinfarction VSD and LVA using the one patch technique and coronary artery by-pass (CABG). Case Presentation A 52-year-old man was referred for a postinfarction VSD occurring after an acute MI. Echocardiography demonstrated significant shunt flow through the ruptured anterior ventricu- lar septum (Figure 1). Emergency cardiac catheterization was performed. Cineangiography revealed a shunt flow through the anterior VSD with 2.1 Qp/Qs ratio and triple-vessel dis- ease. In the light of the patient’s stable hemodynamic condi- tion, surgical intervention was delayed. 3 weeks following the acute MI open heart surgery was performed and had been managed just pre-operatively with an intra-aortic balloon pumping (IABP). A midline sternotomy was performed under general anes- thesia. Total cardiopulmonary bypass (CPB) with bicaval drainage was established and cooled to 28°C. A cross-clamp was applied. Crystalloid cardioplegia was administered into the aortic root with topical cooling using ice slush. The infarcted area was seen along the left anterior descending artery (LAD). A longitudinal transinfarction incision was made in the left ventricular myocardium parallel to and 15 mm away from the LAD. There was a twenty mm diame- ter VSD with fibrotic margins in the anterior part of the sep- tum (Figure 2). A Dacron patch was inserted into the left ventricular cavity and placed on the anterior septum and a series of pledgeted interrupted mattress sutures were placed around the perime- ter of the VSD and then into the patch (Figure 3). The second group of sutures passed through the anterior septum about 3 cm away from the VSD into the right ventricular cavity
Transcript of Simultaneous surgical repair of post-infarct ventricular septal … · 2017-10-17 · 3 weeks...

Case Report 70Journal-Cardiovascular Surgery 2015:3(3):70-73doi; 10.5455/jcvs.20142x20
Yucel et al.Simultaneous surgical repair of post-infarct ventricular septal defect,
left ventricular aneurysm and coronary artery disease
Simultaneous surgical repair of post-infarct ventricular septal defect, left ventricular aneurysm and coronary artery disease
Ertan Yucel1, Kanat Ozisik2, Ozgur Ersoy3, Omer Ulular3, Zeki Temizturk3, Kasım Karapinar3
1Department of Cardiovascular Surgery, Diskapi Yildirim Beyazid Training & Research Hospital, Ankara, Turkey, 2Department of Cardiovascular Surgery, Kafkas University Medical School, Kars, Turkey, 3Department of Cardiovascular Surgery, Diskapi Yildirim Beyazid Training & Research Hospital, Ankara, Turkey*Corresponding Author: Kanat Özışık, Department of Cardiovascular Surgery, Kafkas University Medical School, Kars, Turkey. e-mail: [email protected] words: Coronary artery disease; heart aneurysm; heart septal defects, ventricularReceived: 20.07.2014 Accepted: 16.09.2014 e-published: 18.12.2014
Abstract
A 52-year-old patient was admitted in our hospital for postinfarction ventricular septal defect (VSD), left ventricular aneurysm and coronary artery disease. He was investigated by echocardiography and coronary angiography and proposed for operation. In the light of the patient’s stable hemodynamic condition, surgical intervention was delayed. 3 weeks following the acute myocardial infarction open heart surgery was performed and had been managed just pre-operatively with an intra-aortic balloon pumping. The patient underwent successful VSD closure with a patch. The repair involves VSD closure and infarct exclusion technique. The patient discharged 10 days postoperatively. We consider that this modification is a simple and effective way to decrease the surgical risk of postinfarction VSD.
Introduction
Postinfarction ventricular septal defect (VSD) and left ventricular aneurysm (LVA) are highly lethal complications of acute myocardial infarction (MI) with an incidence of 1-2% and 8-10%, respectively [1-3]. The surgical repair of postinfarction VSD is mandatory. After confirming diagnosis and evaluation of coronary arteries prompt attempts should be done to stabilize the patient since postinfarction VSD clo-sure should be performed 4-5 weeks after MI. Surgical repair of VSD is accompanied by technical difficulties due to the weakness and unclear border of infarcted myocardial tissue. Although numerous techniques and materials have been used to close postinfarction VSDs, the best technique has not yet been settled upon [4,5].
We present the case of a patient who underwent success-ful correction of postinfarction VSD and LVA using the one patch technique and coronary artery by-pass (CABG).
Case Presentation
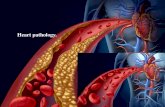
A 52-year-old man was referred for a postinfarction VSD occurring after an acute MI. Echocardiography demonstrated significant shunt flow through the ruptured anterior ventricu-lar septum (Figure 1). Emergency cardiac catheterization was
performed. Cineangiography revealed a shunt flow through the anterior VSD with 2.1 Qp/Qs ratio and triple-vessel dis-ease. In the light of the patient’s stable hemodynamic condi-tion, surgical intervention was delayed. 3 weeks following the acute MI open heart surgery was performed and had been managed just pre-operatively with an intra-aortic balloon pumping (IABP).
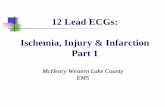
A midline sternotomy was performed under general anes-thesia. Total cardiopulmonary bypass (CPB) with bicaval drainage was established and cooled to 28°C. A cross-clamp was applied. Crystalloid cardioplegia was administered into the aortic root with topical cooling using ice slush. The infarcted area was seen along the left anterior descending artery (LAD). A longitudinal transinfarction incision was made in the left ventricular myocardium parallel to and 15 mm away from the LAD. There was a twenty mm diame-ter VSD with fibrotic margins in the anterior part of the sep-tum (Figure 2).
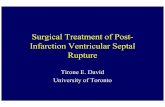
A Dacron patch was inserted into the left ventricular cavity and placed on the anterior septum and a series of pledgeted interrupted mattress sutures were placed around the perime-ter of the VSD and then into the patch (Figure 3). The second group of sutures passed through the anterior septum about 3 cm away from the VSD into the right ventricular cavity

Yucel et al.Simultaneous surgical repair of post-infarct ventricular septal defect, left ventricular aneurysm and coronary artery disease
71Journal-Cardiovascular Surgery 2015:3(3):70-73doi; 10.5455/jcvs.20142x20
and came out through the right ventricle free wall. The rest of the Dacron patch was placed on the epicardial site covering the infarcted area was used as a support for the suture on the other and hence the running suture is easy, fast and, as it is achieved very far away from the necrosed area, has little tendency to tear. The infarcted myocardium with VSD and ventriculotomy was sandwiched between one Dacron patch in a double manner without infarctectomy. The curve of the patch reinforce the fragile wall of the intraventricular septum (Figure 4). The ventriculotomy closed over the patch with 3-0 polypropylene suture, buttressed with 2 strips of Teflon (Figure 5).
The left internal thoracic artery was grafted to LAD, and saphenous veins were grafted to right and diagonal coronary arteries. The heart was rewarmed after a cross-clamp time of 83 min. The patient was weaned from CPB after a total pump
Figure 1: Pre-operative echocardiography of the patient shows the postinfarction ventricular septal defect.
Figure 2: Intra-operative photograph of postpostinfarction ventricular septal defect.
Figure 3: Operative photograph shows repair of postinfarction ventricular septal defect using the single patch technique.
Figure 4: The curve of the patch reinforce the fragile wall of the intraventricular septum.
Figure 5: The ventriculotomy was closed in two layers of sutures buttressed on strips of pericardium or Teflon felt.

Yucel et al.Simultaneous surgical repair of post-infarct ventricular septal defect, left ventricular aneurysm and coronary artery disease
72Journal-Cardiovascular Surgery 2015:3(3):70-73doi; 10.5455/jcvs.20142x20
time of 125 min on dopamin 7, 5 mcg/kg/min as continuous infusion.
The patient tolerated the procedure well and returned to the intensive care unit in a stable condition. He was weaned off the IABP on the 5th post-operative day. The patient dis-charged 10 days postoperatively and there were no signs of residual VSD on echocardiography. At the last follow-up visit 3 months after operation, he was in New York Heart Association class I with no signs of residual VSD.
Discussion
Cooley et al. reported the 1st surgical repair of postinfarc-tion VSD in 1957 [6]. From that time, surgical correction has been accepted as the preferred therapy in this difficult group of patients. Subsequently, the improvements in myocardial pro-tection and the design and refinement of surgical techniques, improved prosthetic grafts, and widespread use of echocar-diography to permit the earlier diagnosis of postinfarction VSD have all contributed to making earlier successful repair of this entity a possibility. However, technical difficulty in managing the fragile myocardium is often encountered while repairing postinfarction VSD. This problem becomes greater if the patient is old, if myocardial necrosis is fresh, or if the MI is extensive in the endocardium [7]. The decision, to operate a patient who is in cardiogenic shock should be tailored for each patient individually. Repair of postinfarc-tion VSD 2-3 weeks or more after septal rupture is relatively safe. By then the edges of the VSD have become tougher and repair is more securely and safely accomplished. Therefore when the patient presents with a stable hemodynamic state, repair can be delayed like our patient. Percutaneous closure of VSD has become a widely accepted alternative to surgical repair [8]. The placement of the device greatly improved the patient’s clinical condition allowing the delay of the surgical procedure. However, until date our knowledge postinfarction VSD closure with percutaneous technique still remains lim-ited. Furthermore, there are no data about long-term efficacy, which could compare the results of surgical closure.
Some studies showed no benefit of CABG while others found evidence for concomitant CABG to be advantageous. It has been shown that concomitant myocardial revascular-ization decreases operative mortality and improves long-term survival [9]. We could not prove any influence of concomi-tant CABG on late survival of our patient, but we believe that patients who have multivessel disease should be routinely revascularized.
Balkanay and co-authors [10] described a technique with two autologous pericardial patches to repair postinfarction VSD. We modified the classical Balkanay’s technique using
a single patch in a double manner. The observations made by David et al. [11] demonstrate the technique of endocar-dial patch with infarct exclusion should enhance operative survival because it leaves the right ventricle undisturbed and restores the geometry the left ventricle in these patients with acute MI and ruptured septum. Infarct expansion is common after transmural MI and patients in whom a VSD develops often have an acute ventricular aneurysm. Restoration of left ventricular geometry has been shown to be important for left ventricular function [12,13].
Due to of necrotic myocardium and friable endocardial tissue, the suture of the Dacron patch is difficult with a high risk of recurrence of the VSD and subsequent mortality [14]. The single Dacron patch placed on the left side of the intra-ventricular septum, which covers the anterior VSD and ven-triculotomy from the inside in a double layer, sticks to the endocardium tightly due to the high blood pressure of the left ventricle. Furthermore, the curve of the patch reinforce the fragile wall of the intraventricular septum. We consider that this modification is a simple and effective way to decrease the surgical risk of postinfarction VSD. In patients without cardiogenic shock urgent operation becomes unnecessary and the choice of surgical technique and surgical timing as well as pre-operative management should be tailored for each patient individually.
References
1) Glower D, Lowe J. Left ventricular aneursym. In: Cohn L, editor. Cardiac Surgery in the Adult. 3rd ed., Vol. 31. New York: Mc Graw-Hill; 2008. p. 803-822.
2) Agnihotri AK, Madsen JC, Daggett WM. Surgical treatment of complications of acute myocardial infarction: Postinfarction ventricular septal defect and free wall rupture. In: Cohn L, editor. Cardiac Surgery Surgery in the Adult. 3rd ed., Vol. 29. New York: Mc Graw-Hill; 2008. p. 753-754.
3) Senocak H, Atesal S, Karakelleoglu S, Sahin M, Alp N. Akut Miyokard infarktüsü sonucu oluşan ventriküler septal defektv. Turkiye Klinikleri J Cardiol 1992;3:190-192.
4) Ito T, Hagiwara H, Maekawa A. Entire septal patch technique for postinfarction ventricular septal rupture. Ann Thorac Surg 2000;70:273-274.
5) Tabuchi N, Tanaka H, Arai H, et al. Double-patch technique for postinfarction ventricular septal perforation. Ann Thorac Surg 2004;77:342-343.
6) Cooley DA, Belmonte BA, Zeıs LB, Schnur S. Surgical repair of ruptured interventricular septum following acute myocardial infarction. Surgery 1957;41:930-937.
7) Skillington PD, Davies RH, Luff AJ, et al. Surgical treatment for infarct-related ventricular septal defects. Improved

Yucel et al.Simultaneous surgical repair of post-infarct ventricular septal defect, left ventricular aneurysm and coronary artery disease
73Journal-Cardiovascular Surgery 2015:3(3):70-73doi; 10.5455/jcvs.20142x20
early results combined with analysis of late functional status. J Thorac Cardiovasc Surg 1990;99:798-808.
8) Hijazi ZM. Catheter closure of atrial septal and ventricular septal defects using the Amplatzer devices. Heart Lung Circ 2003;12 Suppl 2:S63-S72.
9) Jeppsson A, Liden H, Johnsson P, Hartford M, Rådegran K. Surgical repair of post infarction ventricular septal defects: A national experience. Eur J Cardiothorac Surg 2005;27:216-221.
10) Balkanay M, Eren E, Keles C, Toker ME, Guler M. Double-patch repair of postinfarction ventricular septal defect. Tex Heart Inst J 2005;32:43-46.
11) David TE, Dale L, Sun Z. Postinfarction ventricular septal rupture: Repair by endocardial patch with
infarct exclusion. J Thorac Cardiovasc Surg 1995;110:1315-1322.
12) David TE. Surgery for postinfarction ventricular septal defect. In: David TE, editor. Mechanical Complications of Myocardial İnfarction. Austin, Texas: RG Landes; 1993. p. 175-191.
13) Di Donato M, Barletta G, Maioli M, et al. Early hemodynamic results of left ventricular reconstructive surgery for anterior wall left ventricular aneurysm. Am J Cardiol 1992;69:886-890.
14) Labrousse L, Choukroun E, Chevalier JM, et al. Surgery for post infarction ventricular septal defect (VSD): Risk factors for hospital death and long term results. Eur J Cardiothorac Surg 2002;21:725-731.