
Session 69X Using Innovative Technology to Drive · PDF fileSession 69X Using Innovative...
27
Prepared for the Foundation of the American College of Healthcare Executives Session 69X Using Innovative Technology to Drive Value Presented by: Barton Sachs, MD, FACHE
Transcript of Session 69X Using Innovative Technology to Drive · PDF fileSession 69X Using Innovative...

Prepared for the Foundation of the American College of Healthcare Executives
Session 69X Using Innovative Technology to
Drive Value
Presented by: Barton Sachs, MD, FACHE


1
Barton L. Sachs, M.D., MBAChief of Staff & Special Assistant to CEOCo‐Director MUSC Innovation Center
Professor of Orthopaedics ‐‐Medical University of South Carolina
Using Innovative Technology to Drive Value
T 42
Disclosure of RelevantFinancial RelationshipsThe following faculty of this continuing education activity has financial relationships with commercial interests to disclose:
Barton Sachs, MD, FACHE
• APP Squared LLC – Investor– Founder/CMO
• Globus Medical – Royalty- Consultant
2

2
Barton L. Sachs
M.D., MBA
Chairman, CMO, Founder
Chief of Staff, Professor Orthopedics MUSC and BioEng.
Clemson; 3x Serial Founder
Matt Weismiller
CEO
Stryker Berchtold: CEO/GM; Hill-Rom: CTO,
CMO, Founder/SVP IT Division; 2x Turnaround-To-
Sale
Michael McEvoy
Dir. Product Development
Founder MustardSeed Software Agency; 16 yrs. Mobile App Development; Ten Commercial Healthcare
Apps
Nick Hofmeister
Co-Founder
5x serial founder; Triton, Sapphire; PSS; $250mm
raised: biotech, industrials, energy; Bain; MIT
Daniel Sachs
Co-Founder
4x serial founder; Triton Health, DECA Co; $250mm raised;
Majestic Realty; Harvard
70+ years healthcare industry
50+ years med device/life science
40+ years information technology
40+ years founding startups
45+ patents awarded
TEAMSeasoned healthcare entrepreneurial team with decades of success
3
Learning Objectives• Attendees will understand issues related
to inability to track & monitor APP work activity.
• Attendees will learn some basic benchmark data referenced to APPs documented work.
• Attendees will hear of an innovative software system used to capture unforeseen institutional employer revenue in range of $ 6 million.
4

3
• Introduction / Background
– Changes in Healthcare create needs & opportunity
• System Software Solution to meet need
• Snapp description
• Three components of “value position”
• Clinical trial data results – generated at AMC
• Value proposition confirmed
• Summary
Agenda
5
Background Issues“Burning Platform”• We currently live in a market age of unstable
/disruptive healthcare.• Financial reductions
– CMS: Medicaid & Medicare
– Accountable Care Act (Insurance exchanges)
– Sequestration reductions
• Regulatory requirements to:
– maintain & advance quality of clinic care
– Reduce clinical service work hours of house-staff
• Government & Payer expectations for increased open patient access for care
6

4
Triple Aim: How Do We Respond? • Meet situational requirements of:
– Expanding patient access to care
– Advancing & Improving Quality of service
– Reducing cost per unit of patient care
7
New Age Healthcare Market Conditions
• Strategy Drivers– “can not win by simply becoming more
disciplined with current strategy of all patients seen by a physician at each patient encounter”
ref. “The Discipline of Market Leaders”. HBR. M.Treacy & F. Wiersema (1995)
• Focus on “game-changing innovation” (GCI)ref. “Big-Bang Disruption: A New Kind of Innovator”. L. Downes & P.F.
Nunes. HBR. Mar.2013; 44-56
8

5
“Big Bang” Disruption• “Game-Changing Innovation” referred to
as “Big Bang Disruption” (BBD)• BBD holds immense potential for those
who can quickly learn new rules & manage service work in unstable market:– apply an undisciplined strategy,– respond to unconstrained market growth, &– apply new unencumbered developments.Ref. “Big-Bang Disruption: A New Kind of Innovator”. L. Downes & P.F.
Nunes. HBR. Mar.2013; 44-56
9
MUSC Strategy Response
• Response to unstable & changing healthcare market
• MUSC needed to become a “Big Bang Disrupter” by applying:– Innovation
– Patient / Customer intimacy
– Operational excellence
10
6
MUSC Opportunity for BBD APPs - Central Common Focus
• Solution to complex issues resides in expanding healthcare provider work force with:– Advanced Practice Providers (APPs)
• Nurse Practitioners (N.P.s)
• Physician Assistants (P.A.s)
11
Current APP Utilization - Outpatient1. Independent Patient Schedule
• APP has their own schedule template of patients• Supervising MD is not present• APP should bill independently
2. APP working with physician in outpatient clinic and seeing own patients on own schedule profile
• Supervising physician is present in clinic• APP can bill independently or under the supervising MD
3. APP working with physician in outpatient clinic and seeing patients from the physician profile
• APP initiates the visit (history, physical); MD performs a problem focused exam• Visit is billed under the attending physician
4. Global Surgical Specialties• Work efforts are non-billable based on global service coverage
*APP should always record their clinical work effort in the EHR
12

7
Current APP Utilization - Inpatient1. Acting as surrogate or extender for patient care in place of physician (attending
of record) -- this service may include global part of surgical service follow up care or daily administrative work for patient care such as discharge summaries, daily care rounds, etc.
• APP would not bill or invoice for clinical service provided
2. Providing clinical service care for patient in hospital such as: admission; daily care visit rounds (non-surgical patients); interventions, &/or procedures (e.g. line insertions, etc.)
• APP may bill for clinical care service if not employed by hospital
• Reference compliance algorithms
*APP should always record their clinical work effort in the EHR
13
100806040200
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Q and A Percentile Rank
Pro
duct
ivit
y
50
0.8A V G
HighHigh
Low
Below
BelowBelow
High
A V G
High
A bov e
A V G
High
Below
A V G
High
Low
A bov e
Below
A V GA V G
A V GA bov e
Below
A bov e
Low
Matrix Plot of Productivity vs Q and A Percentile Rank
Quality and Accountability Domain Metric WeightMortality Mortality Index 30%
Effectiveness Readmissions 25%Safety Complications 25%
Patient Centered Service Score 5%Efficiency Cost Index 10%Efficiency LOS Index 5%
14

8
Snapp SummarySoftware to coordinate workflow of Advanced Practice Providers (APPs)
PERFORMANCE WORK MANAGEMENT
For hospitals and APPs
Captures billings, improves efficiencies,and reduces regulatory risk
$4B lost from Skilled
Nurses and Physician
Assistants’ (APPs)
inefficiencies and
missed billings
15
APPs* (NPs + PAs) bridge our the increasing demand for healthcare services
Physician Provider
Supply
Healthcare Service Demand
Rapid increase in Advanced Practice Providers* to meet demand
*APPs; Nurses and Physicians Assistants
=
16
9
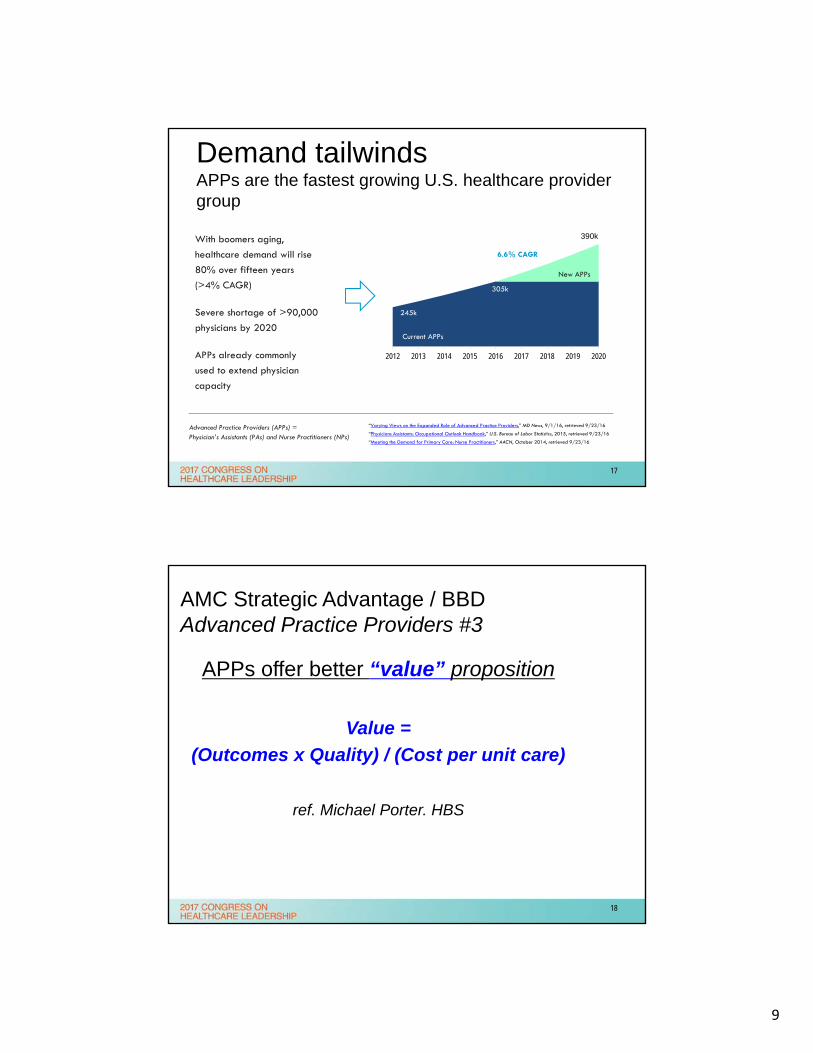
Demand tailwinds APPs are the fastest growing U.S. healthcare provider group
Current APPs
With boomers aging,
healthcare demand will rise
80% over fifteen years
(>4% CAGR)
Severe shortage of >90,000
physicians by 2020
APPs already commonly
used to extend physician
capacity
305k
2012 2013 2014 2015 2016 2017 2018 2019 2020
245k
Current APPs
6.6% CAGR
390k
New APPs
Advanced Practice Providers (APPs) = Physician’s Assistants (PAs) and Nurse Practitioners (NPs)
“Varying Views on the Expanded Role of Advanced Practice Providers,” MD News, 9/1/16, retrieved 9/23/16
“Physicians Assistants: Occupational Outlook Handbook,” U.S. Bureau of Labor Statistics, 2015, retrieved 9/23/16
“Meeting the Demand for Primary Care: Nurse Practitioners,” AACN, October 2014, retrieved 9/23/16
305k
17
AMC Strategic Advantage / BBD Advanced Practice Providers #3
APPs offer better “value” proposition
Value =
(Outcomes x Quality) / (Cost per unit care)
ref. Michael Porter. HBS
18

10
Clinical Areas of Utilization of APPs• Outpatient
– Provide access for new (NP) & follow-up (FU) patients
– Improve flow of patients through clinic– Provide oversight of process continuum clinical care
• Inpatient– Provide improved continuum of care for patients– Improve discharge (D/C) planning & process time– Decrease re-admission after discharge– Improve clinical documentation & assure quality
19
APP Re-Organization Advantages
• Develop new model for institutional clinical care & productivity
• Assures APPs working at high level of practice license & state standards
• Cultural shift of institutional perceptions for APP practice
• Advance “concept of team care” for patients: docs; house-staff; APPs; nurses; students; assoc. healthcare prof. (P.T.; O.T.; R.T.; dietary; Pharm.D.; etc.)
20

11
Inefficiency> 50% of time is spent on administrative non-billable activities
Lost Billings
> 12% of billings are uncaptured due to documentation errors
Legal Risk
> Common practice for APPs to bill activities under physicians; a significant regulatory risk with potential for steep fines (CMS/OIG)
Hospitals can’t fix these
issues because there is
no system to track
and manage APP
activity
Economic losses are
huge: lost revenue is
$1.5 mm per hospital*,
and $4B nationally
*Assumes hospital = 100 APPs
ProblemCurrent practices leave revenue on the table and expose hospitals to risk of fines
21
Three issues relative to APPs:Opportunity & Unmet Need in Healthcare
Lack of Benchmark Info -APP Staffing Management Lack of Benchmark Info -
APP Staffing Management
Lost or Misapplied Financial RevenueLost or Misapplied Financial Revenue
Employer Organization LacksCompliance Record
Employer Organization LacksCompliance Record
22

12
Simple mobile app for rapid + easy APP data entry and
charge capture
Eliminates lost billings, cuts charting time, and reduces
coding issues
Data management, analytics, and reporting tools. Visual Dashboard
Enables supervisors to track performance, set targets/quotas,
and improve efficiency
SolutionSoftware for APP task entry, charge capture, and coding compliance
Providers (APPs) Managers
Winner 2016
Innovation Excellence Award
23
Market sizingPotential financial benefit
$ 43 M / yr.
value created
$15,000 per APP/yr in value
1% utilization = ~2,900 APPs
(~30 hospitals, @ 100 APPs / hospital)
~ 288,000 APPs licensed in U.S.
5,600 hospitals in U.S.
24

13
Architecture of the platform
Snapp iOS (#4)Snapp Android (#5)
Azure SQLDatabase (#1)Azure Mobile
Services (#2/#6)
Windows DesktopQuestion Generator(#3)
App Steps 4 & 5:Decision Engine LogsAPP/Physician Patient Encounter
Windows DesktopData Tools(#7)
Android: mobile “front‐end” collection iOS: mobile “front‐end” collection
Snapp database
“back‐end” reportcustomization
25
Enter basic info for task as it is completed
Answer a few simple questions
System renders coding decision; APP approves.
Done in 7 seconds
SUBMIT CHARGE85% of Usual/Customary
Nurse Practitioner
TRICARE
Michael McEvoy
MUSC Tax ID.
Billing Level: 1
Billing Code: 99238
APP user interface:Easy, accessible, effective
26
14
Demo Video
27
Backend: admin userPowerful data analytics and visual management
Dashboard
• Track APP daily performance and take action as needed
• Views are by user, task, billing and compliance
• Drive achievement and teamwork through public display of performance
Admin Interface
• Set and achieve billing, productivity, and compliance targets
• Generate analytics, reports, and notifications
• Support auditing, internal and external
28

15
Value StreamsSnapp’s pilot verifies the scale of inefficiencies, resulting in major opportunities
Reduce Lost Billings >12% of billable tasks not captured
DEMONSTRATED
Reduce Admin Overhead >50% of time spent on administration
DEMONSTRATED
Reduce Compliance Risk >11% of APP tasks incorrectly billed by MD
DEMONSTRATED
29
Value creationPilot demonstrates Snapp creates ~$14,000 per APP in value for a user hospital
$ per APP/yr
$1.4 Million Revenue Per
Hospital*
> $4 BillionNationally
(*Assumes Hospital = 100 APPs)
6,200
5,500
2,000
13,700
Billings slippage TotalComplianceAdministrative inefficiency
Based on initial pilot product using only 36 codes; current product has over 600 codes results in higher
charge capture value
30

16
Pilot trial objectives• Demonstrate that the issue exists and is
significant
• Quantify the opportunity for improvement
• Demonstrate that APPs do not document all their work in the EHR, and/or they do not capture all of the tasks and billing codes fully and accurately.
• Demonstrate that Snapp prevents compliance errors
31
Pilot trial design
Term 30-60 days, depending on department
Departments additional depts = Endocrinology, Heme-Oncology, Pediatric Surgery, Neurosurgery, Orthopaedics
# of APPs 23 APPs enrolled in the trial use
Data set Encounters = 1,667Time = 1,472 hours (234 workdays)
Reconciliation Compared results of Snapp collections to Epic datafile for APPs (in each dept. of Ortho, Endo, and Heme-Onco)
32

17
First step: market survey(75% response rate)
150 APPs MUSC
Outpat. Clinic
50% unbilled100% admin.
support service unbilled
In-Hosp.
90% unbilled
33
Encounters
APP-BilledEncounters
Physician-BilledEncounters
UnbilledEncounters
Time
APP-BilledTime
Physician-Billed Time
Unbilled Time
Pilot data overview(5 departments – e.g. med. & surg.; in & out-pat.)
34
40% 48%
12%
34%
15%
51%

18
4%
6%
6%1%
2%2%
EncountersNon-Clinical
Un-Billable
Global
No Charge
Other Insurance
Clinical Phone Call
AdministrativePhone CallUpdate Hx/ExamPaperworkFMLA Paperwork
4%
1% 4%7%
2%1%
TimeNon-Clinical Time
Un-Billable Time
Global Time
No Charge Time
Other Insurance Time
Clinical Phone CallTimeAdministrative PhoneCall TimeUpdate Hx/ExamPaperwork TimeFMLA PaperworkTime
Detailed data5 depts
35
12%
16%
51%
81%
23.5%
6.6%
15.6%
54%
Billed ‐‐ APP
Billed ‐‐ Physician
Unbilled ‐ APP w/ patients
Unbilled ‐ APP admin activity
Results: APP time spent
Total Time = 1,472 hours (234 workdays)
Encounters Time
Billed ‐‐ APP 47.2% 23.5%
Billed ‐‐ Physician 10.4% 6.6%
Unbilled ‐ APP w/ patients 42.5% 15.6%
Unbilled ‐ APP admin activity 54.4%
Total 100.0% 100.0%
Problem identified
• 70% of all APP time is spent on non‐billed activities
• ~54.5% of all APP time is spent on administrative tasks
Opportunity for Snapp
• Track efficiency metrics for performance management of APPs
• Increase efficiency = reducing non‐billable time by speeding up APP processes
Time spent by avg. APP
Administration is >50% of APP workload
36

19
Problem identified
• Admin time ~55% of all APP activities
• If only 3% of total time were used for clinical/billable activities, it would be worth $6,200 in revenues per year per APP on average (10% increase)
• Top performing APPs spend the same amount of time on admin tasks as lesser performing APPs
Opportunity for Snapp
• Managers can shift APP time away from admin tasks and generate 10%+ increase in collections
3% efficiency gains are worth >$6,200/APP per year
Value of reducing admin time
$60,070
$99,827
$6,214
$10,877
Average APP Top APP
Actual collections Efficiency improvement
37
312
28
Billable encounters
Snapp, additional
Epic
Billings slippage
Problem identified
• EPIC does not capture all APP billable events
• Some APPs are missing 16% of their billable events
• Average slippage is 9%
• Annualized, this is 85 total encounters / 72 hours per APP, or $16,333 per year
• Collections rate is 33%, therefore lost revenue is ~$5,500 per year
Snapp Opportunity:
• Capture all billable events and eliminate slippage
340 9% of APP billings are not captured by Epic
• Lost billings 9% of total, loss of >$16k per APP annually
• With 33% collections rate, lost revenue is ~$5,500 per year
38

20
Compliance risk
Problem identified
• In normal departments, 11% of APP encounters are misbilled to physicians
• Certain APPs bill all (100%) of their encounters under a physician's name
• This represents a major compliance hazard for the hospital, and could result in multi‐million dollar fines
Opportunity for Snapp
• Allocate billings to the correct provider, avoiding compliance risks
• >10% of APP encounters are incorrectly billed by physicians
• Estimated cost of this risk is ~$2,000/APP per year
352 40
APP encounters tracked
by SnApp
Encounters misbilled to
physician in Epic
39
MedAptus1Ingenious
MedicalPMD ZirMed MD Tech
2patientkeeper
Solution for APPs Experienced healthcare IT startup team Drives all three improvement levers Hospital earns majority of financial benefit
Simplicity of implementation and use
National selling partnerships
Competitive landscapeIndirectDirect
Little direct competition; Snapp is a superior, full‐spectrum solution
1Acquired by North Bridge Oct. 20142Acquired by HCA Sept. 2014
40

21
Compliance ConsiderationsSnapp is designed to improve compliance, not encourage misuse and fraud
Snapp uses a number of mechanisms to prevent errors and fraud
• The application engine matches encounters, payors, and APPs in legitimate combinations only to reduce errors and false coding.
• The engine checks for and eliminates keystroke errors and double entries.
• The application produces a summary report on the users mobile device so that each APP can check their daily entries for accuracy and completeness and against the data in the electronic health record.
• Most importantly, the application produces a comprehensive detail time‐stamped record that is easily audited with internal resources to identify potential fraud. The auditable information is not currently available without the application.
• The application cannot prevent all billing errors. If a physician instructs an APP to not bill an encounter that the APP completed, the system cannot prevent that fraud. An audit will likely be able to identify this fraud after the fact.
41
Client ROI of 300% = $1.05 million in margin (per 100 APPs)
Compliance
Admin
Billing
Cost Value
$3,500
$14,000
330% ROI
$ Per APP/Yr
Client Return300% makes Snapp a clear-cut purchase decision for hospitals
Highly Attractive Purchase
• High ROI > 250%
• Low entry fee, costs are
primarily monthly expense
• Simple SaaS implementation
• Small # of users
• Low maintenance
42

22
MedAptus1Ingenious
MedicalPMD ZirMed MD Tech
2patientkeeper
Solution for APPs Experienced healthcare IT startup team Drives all three improvement levers Hospital earns majority of financial benefit
Simplicity of implementation and use
National selling partnerships
Competitive LandscapeIndirectDirect
Little direct competition; Snapp is a superior, full‐spectrum solution
1Acquired by North Bridge Oct. 20142Acquired by HCA Sept. 2014
43
MarketLarge market, strong interest, immediate access
~5,600 hospitals in the U.S., with 305,000 APPs
Estimated 1,400 hospitals (22%) with >100 APPs
Advanced discussions with healthcare national aggregators to regional network organizations
Potential to deploy to >400 hospitals, representing a $250 mm revenue opportunity
Management team has direct relationships with >25 major hospitals / networks
Represents $50+ mm revenue opportunity
Current engaged 4-5 initial partnerships
Next target acute care facilities deploying 25-100 APPs
Quickly extend sales efforts to very large institutions with >200 APPs
44

23
New CEO (Matt Weismiller)
• 35 years in health IT / med. devices:
management, strategy, R&D, and sales
• Led two successful exits, including
recent $172 mm sale to Stryker
Successful Live Customer
Pilot at MUSC
Multiple customers
engaged for early
partner implementations
Mobile app v5.0, web
interface/dashboard
v2.0 in development
Seed Round Anchor
($200k) Committed,
Closed mid November
Product Developed
v1.0-v4.0
TractionMajor milestones met over two years; progressing rapidly
Winner of 2016 Vizient Innovation Excellence
Award; visibility/access to 3,000+ hospitals
45
Seasoned healthcare
entrepreneurial team with decades
of success
$1 billion and growing market
Powerful and differentiated
solution drives improvement in
all three value streams
Hospitals realize $ millions in
new revenue and margin
SnappTHE FIRST PERFORMANCE WORK MANAGEMENT SOLUTION FOR APPs
46

24
Barton L. Sachs, M.D., MBA, FAAPL, FACHEMedical University of South Carolina
Bart Sachs, M.D. is the Director of Medical University of South Carolina Health System
Innovation Center (MUHIC.) He holds fellowship in American College of Physician
Executives and American Assoc. Physician Executives. As an Orthopaedic spine
surgeon, he maintains fellowship status in American Academy of Orthopaedic
Surgeons, American College of Surgeons, and American College of Spine Surgeons.
Dr. Sachs received the South Carolina ACHE Regents Award for 2015 Senior Leader.
Under his leadership, MUHIC at MUSC received Vizient's 2016 Top Award for
Innovation Excellence from their 3,000 hospital membership. He has promoted
innovative ways to reshape MUSC health provider workforce, thru more efficient use
of Advanced Practice Providers. Dr. Sachs has been instrumental in leading MUSC
through many innovations and improvements in access, quality, cost effectiveness,
safety, efficiency, and supply chain management. One project demonstrated $5.5m
savings over five years for surgical spine implants.
SnApp ‐‐ [email protected]
47
Bibliography/References• Optimizing Advanced Practitioner Charge Capture in High-Acuity Surgical
Intensive Care Units. Butler KL, Calabrese R, Tandon M, Kirton OC. Arch. Surg./Vol.146 (#5), May 2011; 552-555
• Avoiding Charges of Fraud & Abuse: Developing & Implementing an Effective Compliance Program. Bolin JN, Clark LS. J.Nursing Admin.; Vo.34, #12; Dec.2004, 546-550
• The Productivity of Physician Assistants 7 Nurse Practioners & Health Work Force Policy in the Era of Managed Health Care. Scheffler RM, Waitzman NJ, Hillman JM. J. Allied Health. Sum. 25(3), 1996, 207-17
• State False Claims Act Reviews. An Official Website of U.S. Gov. effective Mar. 15, 2013 https;//oig.hhs.gov/fraud/state-false-claims-act-reviews/index.asp
• Physician Assistant & Nurse Practitioner Utilization in Academic Medical Centers. Moote M, Krsek C, Kleinpell R, Todd B. Am. J. Med, Quality. Pub. May 9, 2011
• Effective Utilization of Physician Assistants (PAs) & Best Practice in Billing & Reimbursement. Pagel JK, Powe, M. white-paper report. June 16-18, 2014
• Big-Bang disruption: A New Kind of Innovator. Downes L & Nunes PF. HBR. Mar. 2013; 44-56
48

25
Thank you
49


















