Sedation Dentistry: An Application of Medical Histories ... · 4. Malamed, SF. (2010) Sedation: a...
1
Sedation Dentistry: An Application of Medical Histories and Observation Records to Create A Protocol Aimed at Identifying High-Risk Patients Ma#hew S. Bright 1 , James Cur6s, D.M.D. 2 , Mar6n Durkin, M.D., M.P.H. 3 , David Hicklin, D.M.D. 2 , Cynthia Nichols, D.M.D., M.S. 2 References: 1. Dionne RA. Raise the bar for safe sedation, not barriers for access to care. JADA. 2017;148(3):133-137. 2. “Guidelines for the Use of Sedation and General Anesthesia by Dentists” American Dental Association. 2007. 3. Goodchild JH, Donaldson M. New sedation and general anesthesia guidelines. JADA. 2017;148(3):138-141. 4. Malamed, SF. (2010) Sedation: a guide to patient management. St. Louis, Missouri: Mosby Elsevier. • This study aimed to assess patient outcomes when treated with the sedative medications, midazolam, fentanyl, diazepam, and meperidine, in the hope of identifying high-risk markers that will guide patient selection for in-of<ice sedation procedures Objective • A series of logistical regression models presenting odds ratios based on a dichotomized variable for length of recovery <20 min. or >20 min. resulted in the selected model that included BMI, Co- morbidities (>1), Age, and Morphine Equivalents chosen by the Akaike Information Criterion • A series of linear regression models based on a continuous variable for length of recovery (minutes) resulted in the selected model that included Gender (Male), Co-morbidities (>1), Age, Drug Combination (Versed), Drug Combination (Other), and Morphine Equivalents per Kilogram chosen by an adjusted R 2 value of (0.1018) Analysis • Prospective studies related to the administration, effectiveness, and safety of parenteral administered sedation have been called for as early as 1986 by the National Institute of Health Consensus Conference on Anesthesia and Sedation 1 • Since 2007, the American Dental Association requires the following from dentists practicing moderate sedation: 2 • At least 60 hours of didactic instruction coupled with the supervised management of 20 sedation patients via the intravenous route during the course • Basic Life Support Training for Healthcare Professionals Certi<ication obtained by the dentist, their assistants, and any auxiliary staff • Advanced Cardiac Life Support Certi<ication obtained by the dentist • In October 2016, Resolution 37 of the American Dental Association was approved by the House of Delegates in which more stringent requirements were suggested for all types of sedation provided in a dental setting including CO 2 end tidal monitoring 3 • This monitoring tool was already utilized at the Palmetto Health USC Department of Dentistry • There is still a need for evidence supported guidelines that account for variations in individual patients as well as identi<ied variables that impact sedation outcomes the most Introduction • All procedures were: • Performed at Palmetto Health USC Medical Group, Department of Dentistry • Between the dates of: 07/01/2013-06/30/2016 • Age ≥ 15 years at time of procedure • 298 procedures were included in this study • Linear regression models and logistical regression models with odds ratios were created to investigate the relationship between sedative drugs and demographic factors on a patient’s length of recovery following moderate sedation Materials and Methods 1 The University of South Carolina, South Carolina Honors College, Columbia, SC, USA 2 Palme#o Health USC Medical Group, Department of Den6stry, Columbia, SC, USA 3 Prisma Health Research Compliance, Columbia, SC, USA Table 1 Summary of Linear Regression Analysis for Variables Predicting Length of Recovery (Continuous Variable, Minutes) Coefficients Estimate Std. Error T-Value Pr(>|T|) Gender (Male) 1.69478 1.02872 1.647 0.1008 Co-morbidities (>1) 3.97855 0.99248 4.009 <.0001* Age 0.06519 0.03351 1.945 0.0529 ! Drug Combination Fentanyl - Versed -1.70116 1.65944 -1.025 0.3063 Drug Combination Other -4.25424 2.34289 -1.816 0.0707 ! Morphine Milligram Equivalents per Kilogram 14.87925 7.95897 1.869 0.0628 ! * if p < 0.05 ● if p < 0.1 Residual Standard Error = 7.021 Degrees of Freedom = 236 Adjusted R 2 = 0.1018 P-Value = 2.015e-05 • Moderate sedation for dental practice is a safe and effective modality for providing dental treatment in a regulated and controlled environment • Quantitative data analysis can guide the implementation of practice protocol for patient selection and management of moderate sedation procedures Conclusion Table 2 Summary of Logistical Regression Model for Variables Predicting Length of Recovery (Dichotomized Variable, <20 and >20 Minutes) Variables Odds Ratio -95% CI +95% CI P Value BMI 1.033 0.991 1.076 0.127 Co-morbidities (>1) 1.890 1.011 3.533 0.046* Age 1.023 0.999 1.047 0.057 ! Morphine Equivalents * if p < 0.05 ● if p < 0.1 1.052 0.984 1.124 0.141 • Although neither model alone is of suf<icient quality to explain the correlation between the chosen variables and the patient’s length of recovery, when compared, speci<ic variables are of signi<icant interest and warrant further study • Variables that are signi<icant in both models include the patient’s age and number of co-morbidites associated with their overall health • The morphine equivalents (associated with BMI) a patient receives was found to be an indicator of extended lengths of recovery • The speci<ic drug combination, (associated with morphine equivalents per kilogram), was also found to be an indicator of extended lengths of recovery in the linear regression model Discussion n= Figure 1. Scatter plots relating variables of Length of Procedure (min) and Length of Recovery (min). Each data point represents one sedation. • Fentanyl, although more potent than other sedative drugs, allows for shorter durations and increased clinical control, resulting in a more predictable, shorter recovery time 4 • Diazepam and Meperidine represent sedative drugs with longer durations and therefore decreased clinical control, yet are still viable options for moderate sedation Drug Combinations
Transcript of Sedation Dentistry: An Application of Medical Histories ... · 4. Malamed, SF. (2010) Sedation: a...

Sedation Dentistry: An Application of Medical Histories and Observation Records to Create A Protocol Aimed at Identifying High-Risk Patients
Ma#hewS.Bright1,JamesCur6s,D.M.D.2,Mar6nDurkin,M.D.,M.P.H.3,DavidHicklin,D.M.D.2,CynthiaNichols,D.M.D.,M.S.2
References: 1. Dionne RA. Raise the bar for safe sedation, not barriers for access to care. JADA. 2017;148(3):133-137. 2. “Guidelines for the Use of Sedation and General Anesthesia by Dentists” American Dental Association. 2007. 3. Goodchild JH, Donaldson M. New sedation and general anesthesia guidelines. JADA. 2017;148(3):138-141. 4. Malamed, SF. (2010) Sedation: a guide to patient management. St. Louis, Missouri: Mosby Elsevier.
• Thisstudyaimedtoassesspatientoutcomeswhentreatedwiththesedativemedications,midazolam,fentanyl,diazepam,andmeperidine,inthehopeofidentifyinghigh-riskmarkersthatwillguidepatientselectionforin-of<icesedationprocedures
Objective
• Aseriesoflogisticalregressionmodelspresentingoddsratiosbasedonadichotomizedvariablefor
lengthofrecovery<20min.or>20min.resultedintheselectedmodelthatincludedBMI,Co-
morbidities(>1),Age,andMorphineEquivalentschosenbytheAkaikeInformationCriterion
• Aseriesoflinearregressionmodelsbasedonacontinuousvariableforlengthofrecovery(minutes)
resultedintheselectedmodelthatincludedGender(Male),Co-morbidities(>1),Age,Drug
Combination(Versed),DrugCombination(Other),andMorphineEquivalentsperKilogramchosen
byanadjustedR2valueof(0.1018)
Analysis
• Prospectivestudiesrelatedtotheadministration,effectiveness,andsafetyofparenteraladministeredsedationhave
beencalledforasearlyas1986bytheNationalInstituteofHealthConsensusConferenceonAnesthesiaand
Sedation1
• Since2007,theAmericanDentalAssociationrequiresthefollowingfromdentistspracticingmoderatesedation:2
• Atleast60hoursofdidacticinstructioncoupledwiththesupervisedmanagementof20sedation
patientsviatheintravenousrouteduringthecourse
• BasicLifeSupportTrainingforHealthcareProfessionalsCerti<icationobtainedbythedentist,their
assistants,andanyauxiliarystaff
• AdvancedCardiacLifeSupportCerti<icationobtainedbythedentist
• InOctober2016,Resolution37oftheAmericanDentalAssociationwasapprovedbytheHouseofDelegatesin
whichmorestringentrequirementsweresuggestedforalltypesofsedationprovidedinadentalsettingincluding
CO2endtidalmonitoring3
• ThismonitoringtoolwasalreadyutilizedatthePalmettoHealthUSCDepartmentofDentistry
• Thereisstillaneedforevidencesupportedguidelinesthataccountforvariationsinindividualpatientsaswellas
identi<iedvariablesthatimpactsedationoutcomesthemost
Introduction
• Allprocedureswere:• PerformedatPalmettoHealthUSCMedicalGroup,DepartmentofDentistry• Betweenthedatesof:07/01/2013-06/30/2016• Age≥15yearsattimeofprocedure
• 298procedureswereincludedinthisstudy• Linearregressionmodelsandlogisticalregressionmodelswithoddsratioswerecreatedtoinvestigatetherelationship
betweensedativedrugsanddemographicfactorsonapatient’slengthofrecoveryfollowingmoderatesedation
Materials and Methods
1TheUniversityofSouthCarolina,SouthCarolinaHonorsCollege,Columbia,SC,USA2Palme#oHealthUSCMedicalGroup,DepartmentofDen6stry,Columbia,SC,USA
3PrismaHealthResearchCompliance,Columbia,SC,USA
Table 1
Summary of Linear Regression Analysis for Variables Predicting Length of Recovery (Continuous Variable, Minutes)
Coefficients Estimate Std. Error T-Value Pr(>|T|)
Gender (Male) 1.69478 1.02872 1.647 0.1008
Co-morbidities (>1) 3.97855 0.99248 4.009 <.0001*
Age 0.06519 0.03351 1.945 0.0529!
Drug Combination Fentanyl - Versed -1.70116 1.65944 -1.025 0.3063
Drug Combination Other -4.25424 2.34289 -1.816 0.0707!
Morphine Milligram Equivalents per
Kilogram14.87925 7.95897 1.869 0.0628!
* if p < 0.05● if p < 0.1
Residual Standard Error = 7.021
Degrees of Freedom = 236 Adjusted R2 = 0.1018 P-Value = 2.015e-05
• Moderatesedationfordentalpracticeisasafeandeffectivemodalityforprovidingdental
treatmentinaregulatedandcontrolledenvironment• Quantitativedataanalysiscanguidetheimplementationofpracticeprotocolforpatientselectionandmanagementofmoderatesedationprocedures
Conclusion
Table 2
Summary of Logistical Regression Model for Variables Predicting Length of Recovery (Dichotomized Variable, <20 and >20 Minutes)
Variables Odds Ratio -95% CI +95% CI P Value
BMI 1.033 0.991 1.076 0.127
Co-morbidities (>1) 1.890 1.011 3.533 0.046*
Age 1.023 0.999 1.047 0.057!
MorphineEquivalents
* if p < 0.05● if p < 0.1
1.052 0.984 1.124 0.141
• Althoughneithermodelaloneisofsuf<icientqualitytoexplainthecorrelationbetweenthechosenvariablesandthepatient’slengthofrecovery,whencompared,speci<icvariablesareofsigni<icant
interestandwarrantfurtherstudy• Variablesthataresigni<icantinbothmodelsincludethepatient’sageandnumberofco-morbidites
associatedwiththeiroverallhealth• Themorphineequivalents(associatedwithBMI)apatientreceiveswasfoundtobeanindicatorofextendedlengthsofrecovery
• Thespeci<icdrugcombination,(associatedwithmorphineequivalentsperkilogram),wasalsofoundtobeanindicatorofextendedlengthsofrecoveryinthelinearregressionmodel
Discussion
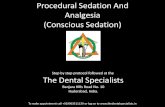
n=
Figure 1. Scatter plots relating variables of Length of Procedure (min) and Length of Recovery (min). Each data point represents one sedation.
• Fentanyl,althoughmorepotentthanothersedativedrugs,allowsforshorterdurationsandincreasedclinicalcontrol,resultinginamorepredictable,shorterrecoverytime4
• DiazepamandMeperidinerepresentsedativedrugswithlongerdurationsandthereforedecreasedclinicalcontrol,yetarestillviableoptionsformoderatesedation
Drug Combinations