Section 8 Liver and Gallbladder - Indiana University...
21
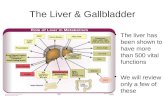
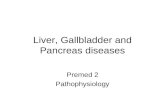
General and Systemic Histopathology C601 and C602 Section 8 Liver and Gallbladder As we will see in this unit, the liver is subject to many types of injury. Additionally, many systemic diseases have a liver component and sometimes it's hard to know what might have started a particular problem. We will be studying examples of infectious, vascular, nutritional, obstructive, neoplastic and iatrogenic injury of the liver. It's going to be very important to know the micro architecture of the liver. The liver is an organ that has a remarkable capacity for regeneration, assuming the underlying reticular (lobular) framework is intact Unfortunately, in the case of chronic and ongoing injury, complicated by loss of the basic reticular architecture, the drive to repair substantially misses the mark. In this connection, we are going to look at a number of examples and causes of cirrhosis and it's complications. Additionally, the study of hepatitis is going to be very important, but don't make the mistake of thinking that all cases of hepatitis are viral in nature, or for that matter, have a microbiological etiology. Many medications cause liver cell injury that can lead to overt hepatitis. And, as I am sure everyone knows, ethanol has rather marked liver toxic properties. One of the leading causes of acute hepatitis is acute alcohol injury. We will see others as well.
Transcript of Section 8 Liver and Gallbladder - Indiana University...
General and Systemic HistopathologyC601 and C602
Section 8 Liver and GallbladderAs we will see in this unit, the liver is subject to many types of injury. Additionally, many systemic diseases have a livercomponent and sometimes it's hard to know what might have started a particular problem. We will be studying examplesof infectious, vascular, nutritional, obstructive, neoplastic and iatrogenic injury of the liver. It's going to be very importantto know the micro architecture of the liver.
The liver is an organ that has a remarkable capacity for regeneration, assuming the underlying reticular (lobular)framework is intact Unfortunately, in the case of chronic and ongoing injury, complicated by loss of the basic reticulararchitecture, the drive to repair substantially misses the mark. In this connection, we are going to look at a number ofexamples and causes of cirrhosis and it's complications. Additionally, the study of hepatitis is going to be very important,but don't make the mistake of thinking that all cases of hepatitis are viral in nature, or for that matter, have amicrobiological etiology. Many medications cause liver cell injury that can lead to overt hepatitis. And, as I am sureeveryone knows, ethanol has rather marked liver toxic properties. One of the leading causes of acute hepatitis is acutealcohol injury. We will see others as well.

117General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 4: Liver with fatty metamorphosis
The mottled staining pattern of the tissue isquite evident in this slide. This tells us thereis a lot of something that doesn't actually belong here. Basically something of anon-water soluble nature.
This condition goes by several names. Bysome authors it is called fatty metamorphosisand by others fatty change. The former is themost widely used. It is a rather nonspecificalteration, but one we see commonly inbiopsies of the liver. The fat vacuoles arewithin the hepatocytes. There is no"invasion" of the liver with lipocytes. In thisslide there is little inflammation and thearchitecture of the liver is well preserved.The tissue is most likely from a diabetic patient, although the changes are common inalcoholics, those with various nutritionaldeficiencies and many other metabolic problems.
Your observations

118General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 27: Gallbladder with acute and chronicinflammation
This section represents only a small slice outof a dilated, inflamed (and no doubt painful)gallbladder. Undoubtedly there were stones present as well, but we don't have any directmicroscopic evidence for them. Find themucosa and then work your way through thewall to the serosa. Pay attention to theinflammatory cells and where you see them. What about the lamina propria?
Find the lumen and try to have yourselforiented before looking for the infiltrate. Youwill see a mixed inflammatory infiltrate consisting of both "acute" and "chronic"inflammatory cells, again lymphocytes are tobe expected in the submucosa of a structure associated with the gastrointestinal system.You will see a large amount of granulationtissue on the serosal surface.
Your observations
119General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
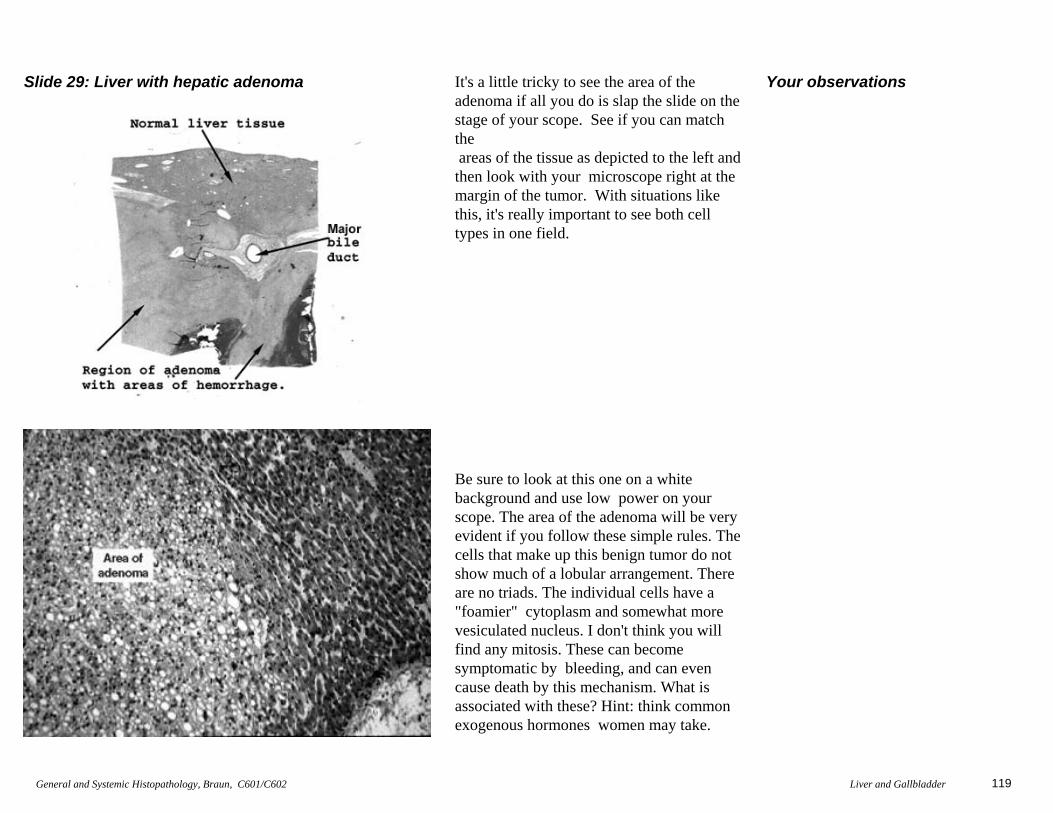
Slide 29: Liver with hepatic adenoma It's a little tricky to see the area of theadenoma if all you do is slap the slide on thestage of your scope. See if you can matchthe areas of the tissue as depicted to the left andthen look with your microscope right at themargin of the tumor. With situations likethis, it's really important to see both celltypes in one field.
Be sure to look at this one on a whitebackground and use low power on yourscope. The area of the adenoma will be very evident if you follow these simple rules. Thecells that make up this benign tumor do notshow much of a lobular arrangement. Thereare no triads. The individual cells have a"foamier" cytoplasm and somewhat morevesiculated nucleus. I don't think you willfind any mitosis. These can becomesymptomatic by bleeding, and can evencause death by this mechanism. What is associated with these? Hint: think commonexogenous hormones women may take.
Your observations
120General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
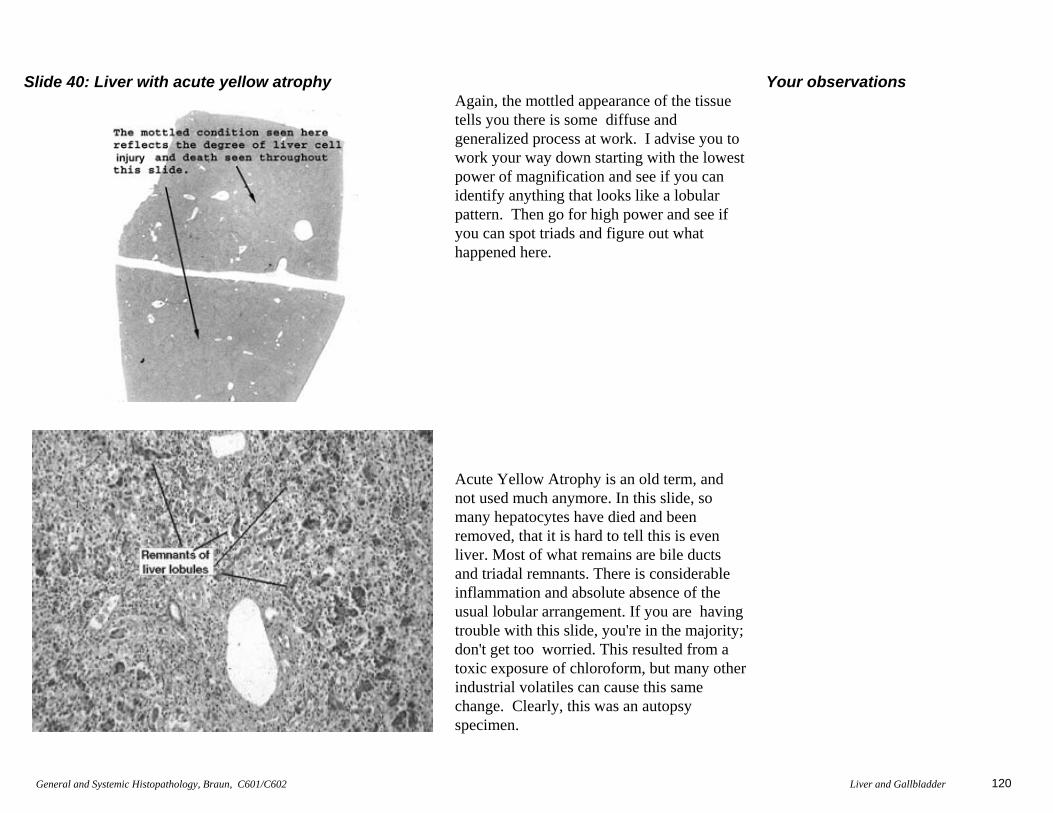
Slide 40: Liver with acute yellow atrophyAgain, the mottled appearance of the tissuetells you there is some diffuse andgeneralized process at work. I advise you towork your way down starting with the lowestpower of magnification and see if you canidentify anything that looks like a lobularpattern. Then go for high power and see ifyou can spot triads and figure out whathappened here.
Acute Yellow Atrophy is an old term, andnot used much anymore. In this slide, somany hepatocytes have died and beenremoved, that it is hard to tell this is evenliver. Most of what remains are bile ductsand triadal remnants. There is considerableinflammation and absolute absence of theusual lobular arrangement. If you are havingtrouble with this slide, you're in the majority;don't get too worried. This resulted from atoxic exposure of chloroform, but many otherindustrial volatiles can cause this samechange. Clearly, this was an autopsyspecimen.
Your observations
121General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
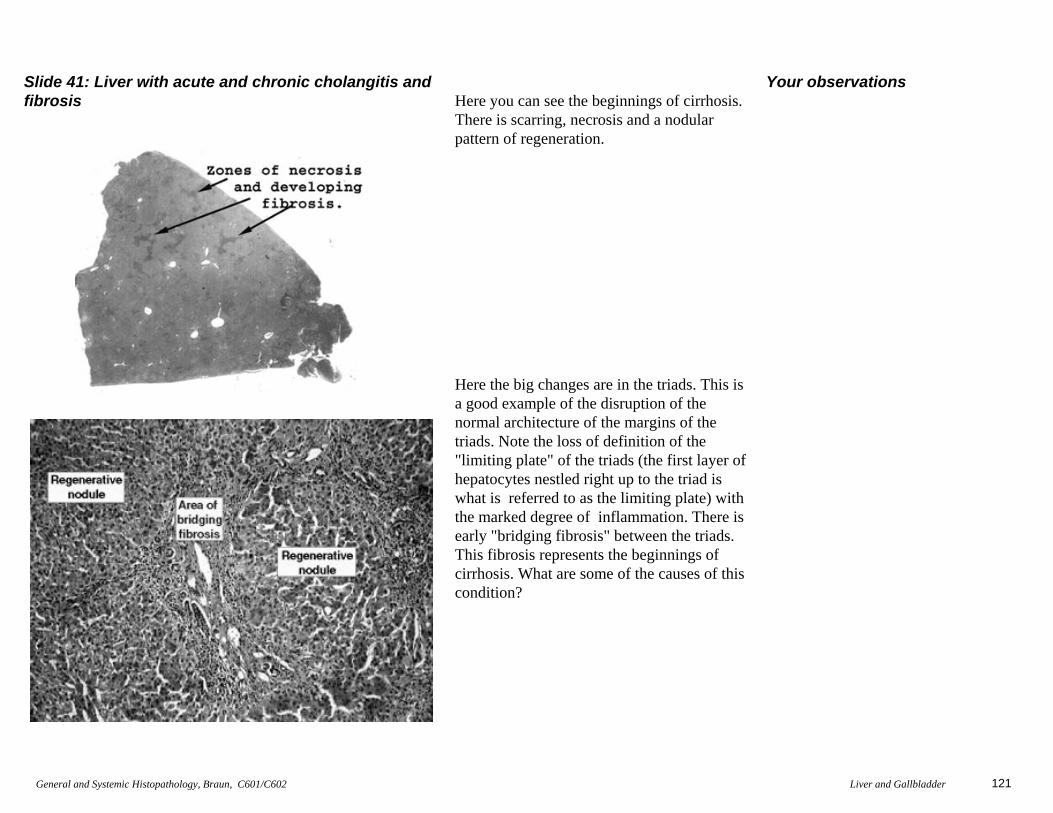
Slide 41: Liver with acute and chronic cholangitis andfibrosis Here you can see the beginnings of cirrhosis.
There is scarring, necrosis and a nodularpattern of regeneration.
Here the big changes are in the triads. This isa good example of the disruption of thenormal architecture of the margins of the triads. Note the loss of definition of the"limiting plate" of the triads (the first layer ofhepatocytes nestled right up to the triad iswhat is referred to as the limiting plate) withthe marked degree of inflammation. There isearly "bridging fibrosis" between the triads.This fibrosis represents the beginnings ofcirrhosis. What are some of the causes of thiscondition?
Your observations
122General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
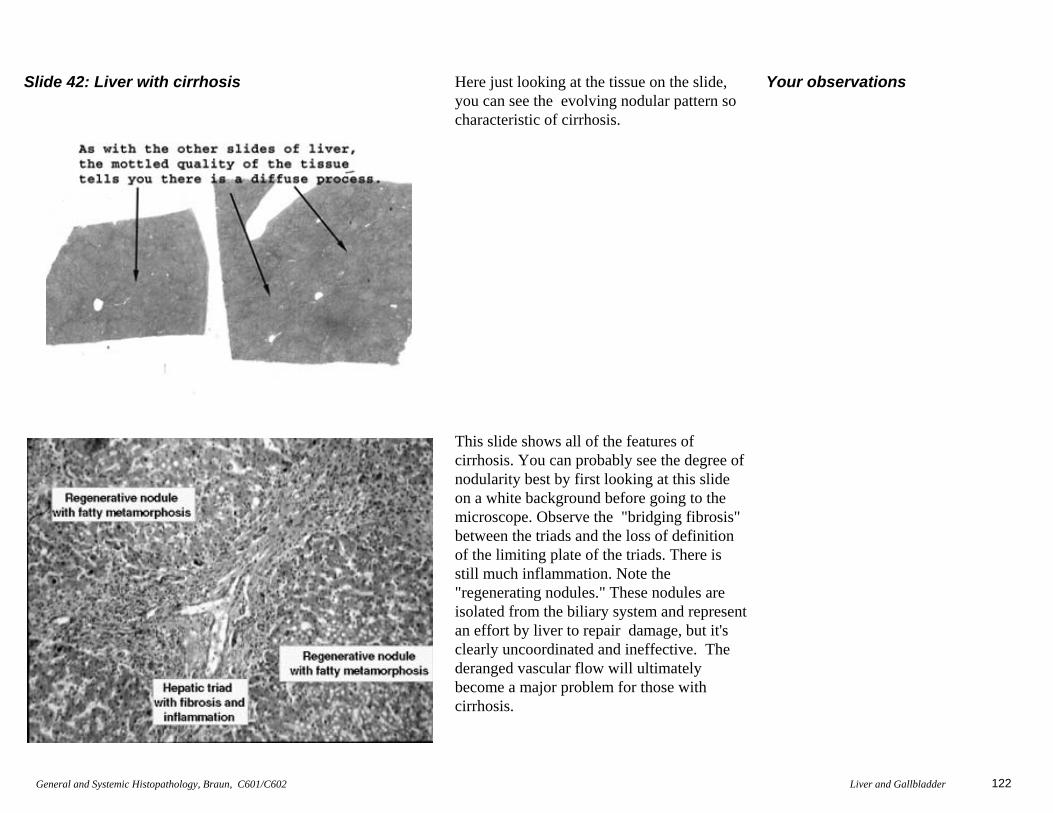
Slide 42: Liver with cirrhosis Here just looking at the tissue on the slide,you can see the evolving nodular pattern socharacteristic of cirrhosis.
This slide shows all of the features ofcirrhosis. You can probably see the degree ofnodularity best by first looking at this slideon a white background before going to themicroscope. Observe the "bridging fibrosis"between the triads and the loss of definitionof the limiting plate of the triads. There isstill much inflammation. Note the"regenerating nodules." These nodules areisolated from the biliary system and representan effort by liver to repair damage, but it'sclearly uncoordinated and ineffective. The deranged vascular flow will ultimatelybecome a major problem for those withcirrhosis.
Your observations

123General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 45: Liver with post necrotic cirrhosis I'll bet you can't miss the nodularity andscarring in this example of cirrhosis.
Here you will see large bands of scar tissuethroughout the liver, and this feature is thehallmark of post necrotic cirrhosis. There is profound disruption of the expected lobulararchitecture, and some inflammatory cellsshould still be seen. But again, the vascularderangement will play havoc in this situation.What does the term "bile duct duplication"really refer to? Be sure you understand whatis meant be the term "post necrotic" cirrhosis.
Your observations
124General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
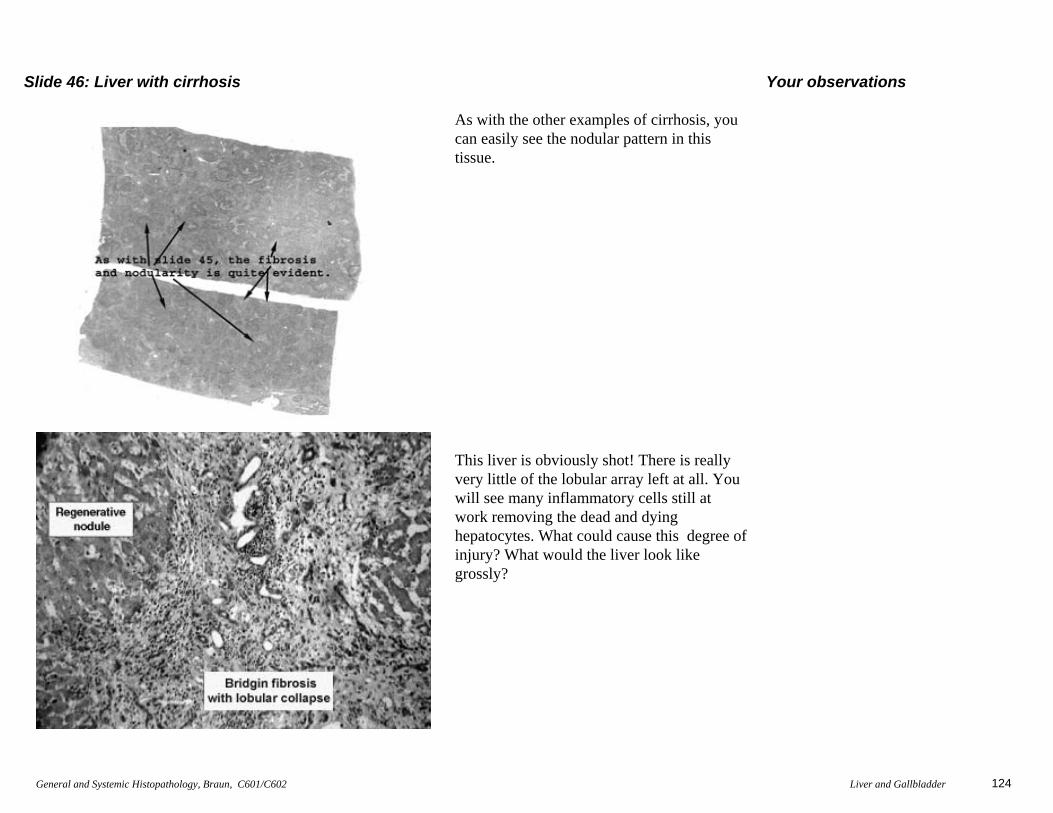
Slide 46: Liver with cirrhosis
As with the other examples of cirrhosis, youcan easily see the nodular pattern in thistissue.
This liver is obviously shot! There is reallyvery little of the lobular array left at all. Youwill see many inflammatory cells still atwork removing the dead and dyinghepatocytes. What could cause this degree ofinjury? What would the liver look likegrossly?
Your observations

125General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 47: Liver with metastatic cancer
As with slides of this sort, look at theuninvolved liver first and then move to theregion of pathology. The metastatic focus ispretty easy to recognize. See if you candetect a glandular or "Indian file" pattern.
Again, looking at this slide on a whitebackground will show the areas of cancerquite nicely. I believe this is an example of metastatic breast cancer. You will seerudimentary attempts to form glands by themalignant cells. Observe the advancing margins of the tumors. Compare the cytologyof the foreign malignant cells to that of thesurrounding healthy liver cells. Do you seevacuoles in the metastatic malignant cells?
Your observations
126General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
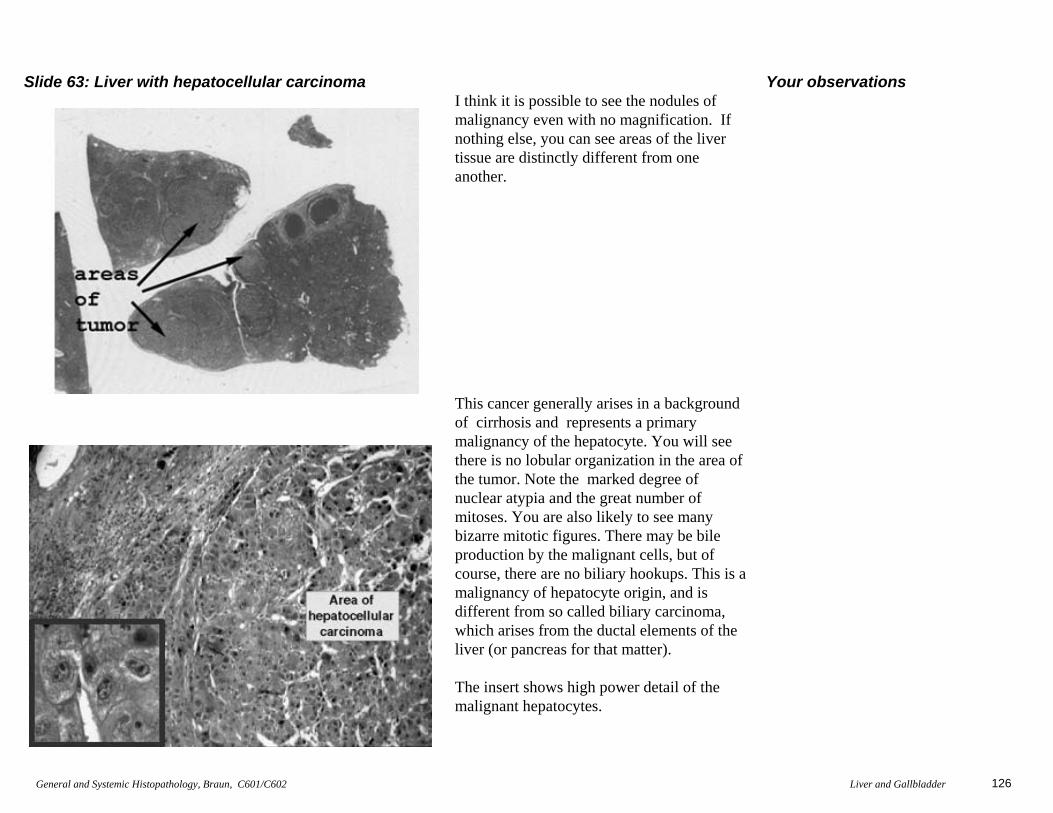
Slide 63: Liver with hepatocellular carcinoma I think it is possible to see the nodules ofmalignancy even with no magnification. Ifnothing else, you can see areas of the livertissue are distinctly different from oneanother.
This cancer generally arises in a backgroundof cirrhosis and represents a primarymalignancy of the hepatocyte. You will seethere is no lobular organization in the area ofthe tumor. Note the marked degree ofnuclear atypia and the great number ofmitoses. You are also likely to see manybizarre mitotic figures. There may be bileproduction by the malignant cells, but ofcourse, there are no biliary hookups. This is amalignancy of hepatocyte origin, and isdifferent from so called biliary carcinoma,which arises from the ductal elements of theliver (or pancreas for that matter).
The insert shows high power detail of themalignant hepatocytes.
Your observations
127General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 69: Liver with chronic lymphocytic leukemia
Can't really see much at this power ofmagnification. Look in the triads for thelymphocytic infiltrate.
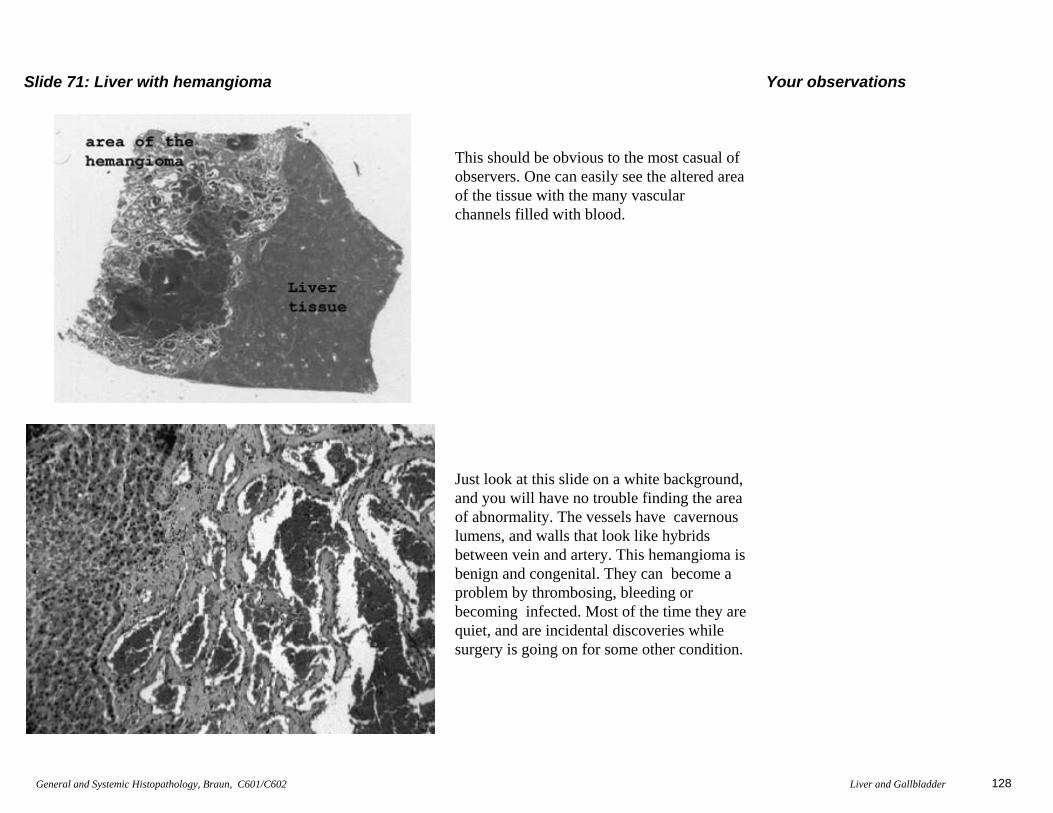
The changes here are subtle. You will see aninfiltrate of, quite frankly benign looking,lymphocytes in the triads. We call this a"cold infiltrate" because the lymphocytes donot have a "stimulated" appearance and arenot there as a response to some inflammatory process. These lymphocytesmay lack the classical cytologic features ofmalignancy, but they are indeed malignant.
Your observations
128General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
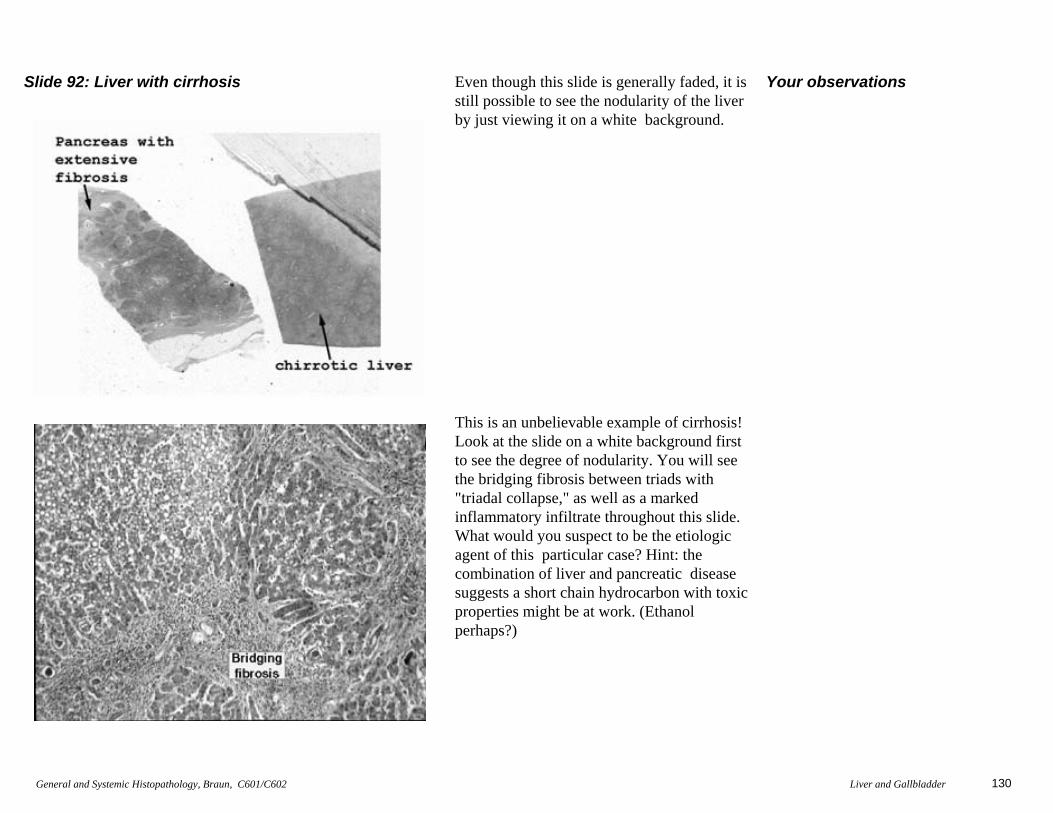
Slide 71: Liver with hemangioma
This should be obvious to the most casual ofobservers. One can easily see the altered areaof the tissue with the many vascular channels filled with blood.
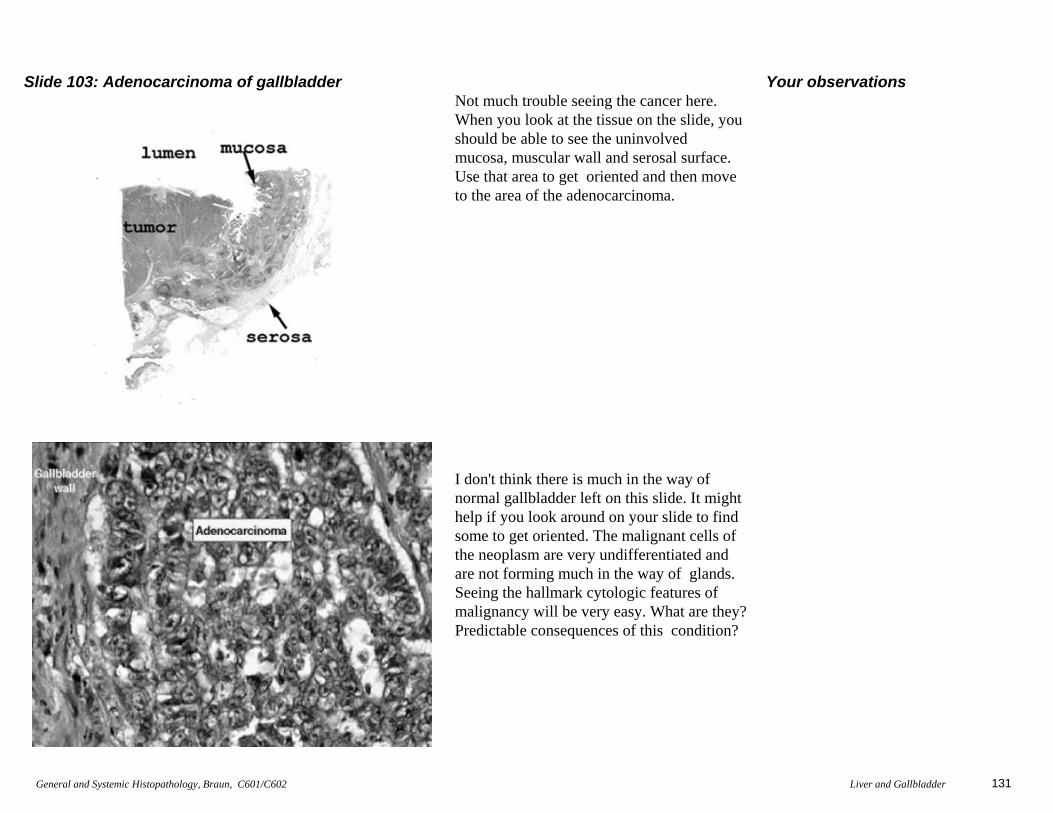
Just look at this slide on a white background,and you will have no trouble finding the areaof abnormality. The vessels have cavernouslumens, and walls that look like hybridsbetween vein and artery. This hemangioma isbenign and congenital. They can become aproblem by thrombosing, bleeding orbecoming infected. Most of the time they arequiet, and are incidental discoveries whilesurgery is going on for some other condition.
Your observations

129General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 75: Fatty infiltration of pancreas
The changes of importance here are probablybetter seen in this scan of the tissue than byuse of the microscope. Here you can see the"infiltration" of benign fat cells into thepancreas. That's all there is here.
This is hard to pick up, because what ispresent in the pancreas is what is normallythere; just more than usual. You should see mature fatty tissue extending into the lobulesof the pancreas. The fat cells are notmalignant, and this is not particularly pathological. We see this change in obesepeople. This condition is quite different fromfatty metamorphosis which occurs in theliver. In fatty metamorphosis we see theeffected cell accumulating a large lipiddroplet. Slide #4 in your set shows a niceexample. The main purpose here is to be sureyou know the difference between fattyinfiltration and fatty metamorphosis. Do you?
Your observations
130General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 92: Liver with cirrhosis Even though this slide is generally faded, it isstill possible to see the nodularity of the liverby just viewing it on a white background.
This is an unbelievable example of cirrhosis!Look at the slide on a white background firstto see the degree of nodularity. You will seethe bridging fibrosis between triads with"triadal collapse," as well as a markedinflammatory infiltrate throughout this slide.What would you suspect to be the etiologicagent of this particular case? Hint: thecombination of liver and pancreatic diseasesuggests a short chain hydrocarbon with toxicproperties might be at work. (Ethanolperhaps?)
Your observations
131General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 103: Adenocarcinoma of gallbladder Not much trouble seeing the cancer here. When you look at the tissue on the slide, youshould be able to see the uninvolved mucosa, muscular wall and serosal surface. Use that area to get oriented and then moveto the area of the adenocarcinoma.
I don't think there is much in the way ofnormal gallbladder left on this slide. It mighthelp if you look around on your slide to findsome to get oriented. The malignant cells ofthe neoplasm are very undifferentiated andare not forming much in the way of glands.Seeing the hallmark cytologic features ofmalignancy will be very easy. What are they?Predictable consequences of this condition?
Your observations
132General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
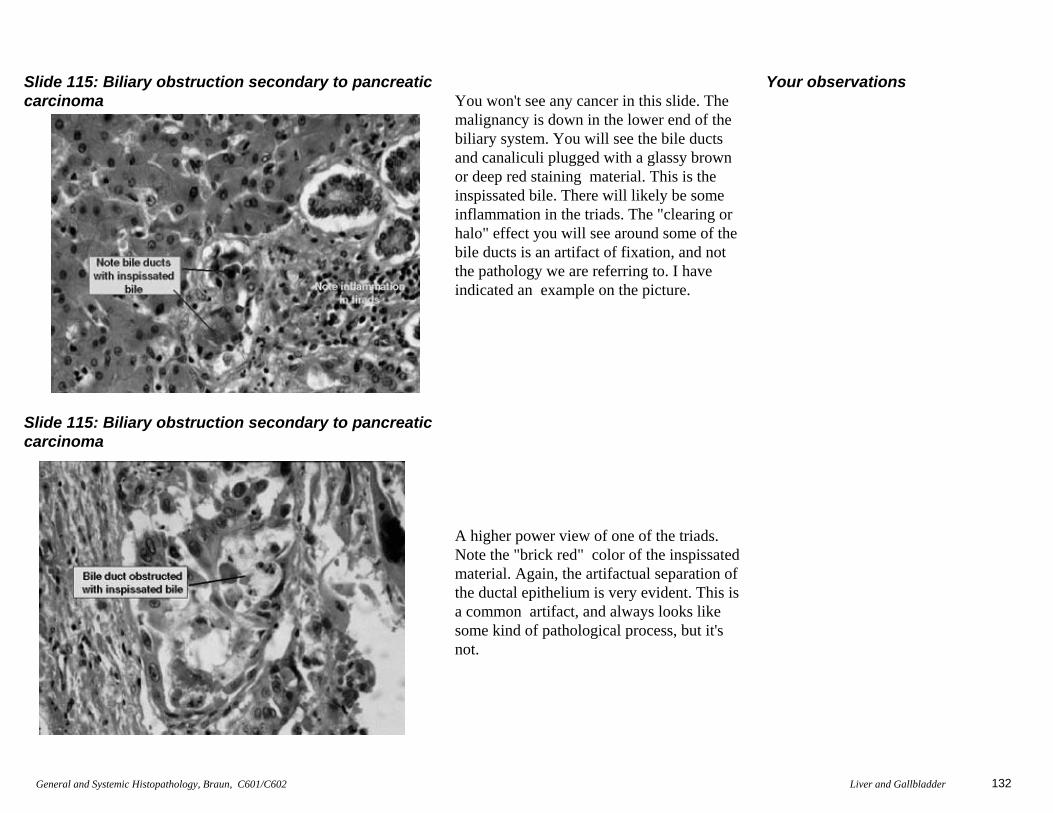
Slide 115: Biliary obstruction secondary to pancreaticcarcinoma
Slide 115: Biliary obstruction secondary to pancreaticcarcinoma
You won't see any cancer in this slide. Themalignancy is down in the lower end of thebiliary system. You will see the bile ductsand canaliculi plugged with a glassy brownor deep red staining material. This is theinspissated bile. There will likely be some inflammation in the triads. The "clearing orhalo" effect you will see around some of thebile ducts is an artifact of fixation, and notthe pathology we are referring to. I haveindicated an example on the picture.
A higher power view of one of the triads.Note the "brick red" color of the inspissatedmaterial. Again, the artifactual separation ofthe ductal epithelium is very evident. This isa common artifact, and always looks likesome kind of pathological process, but it'snot.
Your observations
133General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
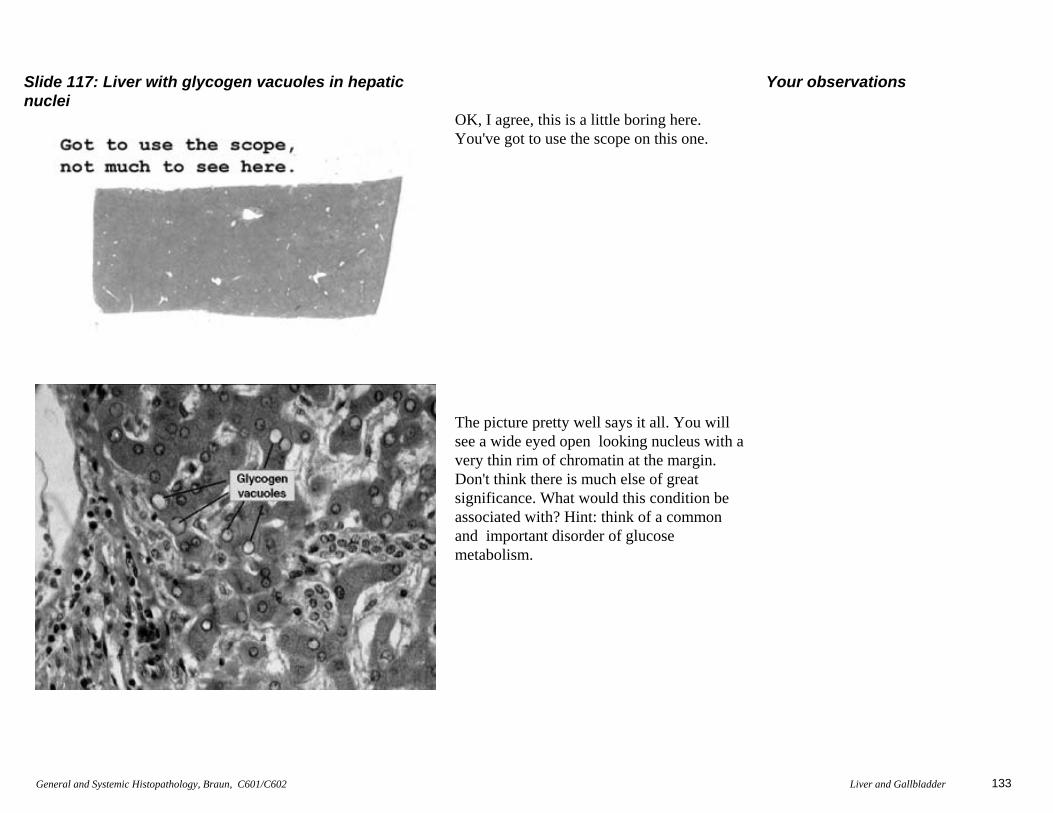
Slide 117: Liver with glycogen vacuoles in hepaticnuclei
OK, I agree, this is a little boring here.You've got to use the scope on this one.
The picture pretty well says it all. You willsee a wide eyed open looking nucleus with avery thin rim of chromatin at the margin. Don't think there is much else of greatsignificance. What would this condition beassociated with? Hint: think of a commonand important disorder of glucosemetabolism.
Your observations
134General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
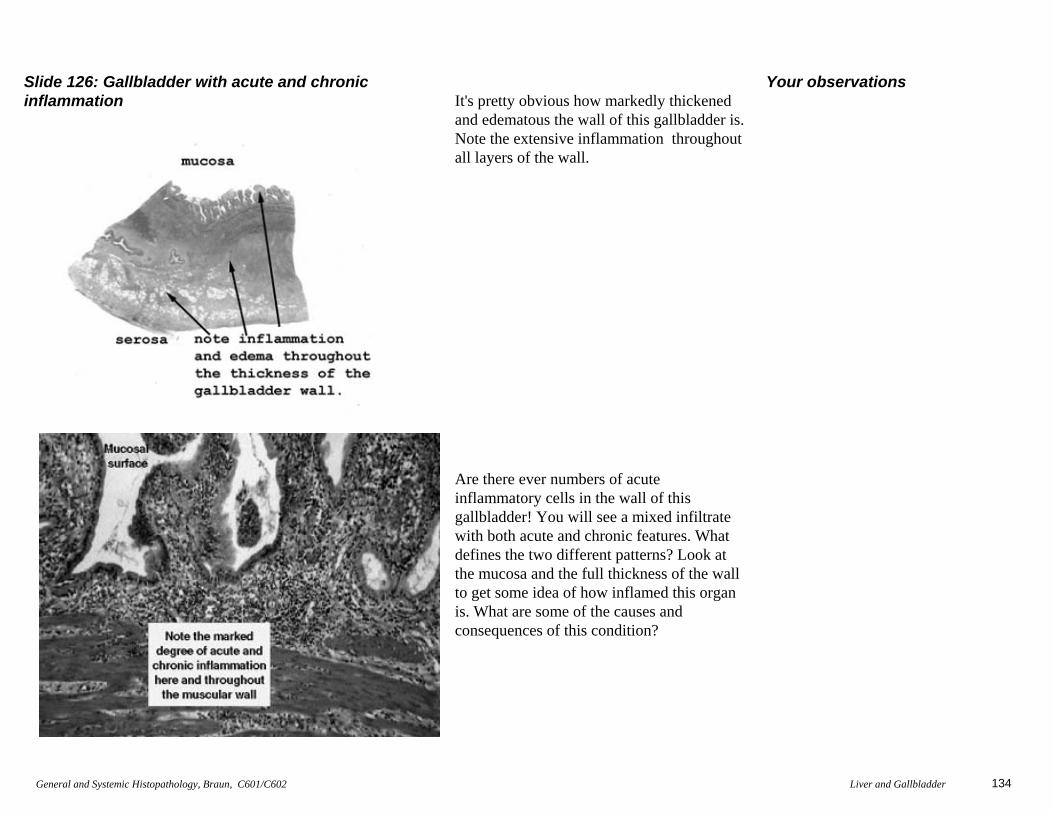
Slide 126: Gallbladder with acute and chronicinflammation It's pretty obvious how markedly thickened
and edematous the wall of this gallbladder is. Note the extensive inflammation throughoutall layers of the wall.
Are there ever numbers of acuteinflammatory cells in the wall of thisgallbladder! You will see a mixed infiltratewith both acute and chronic features. Whatdefines the two different patterns? Look atthe mucosa and the full thickness of the wallto get some idea of how inflamed this organis. What are some of the causes andconsequences of this condition?
Your observations

135General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
Slide 132: Acute viral hepatitis
Normal liver for comparison
There are a number of features we look for tomake the diagnosis of acute hepatitis, andthis slide has them all. Note the "piecemeal(focal ) necrosis" of the hepatocytes in thelobules. You will see little clusters of acuteinflammatory cells in the lobules and in thetriads. There may be some disruption of the "limiting plate" of the triads too. The limitingplate refers to the junctional zone (i.e. firstlayer of hepatocytes) between the triad andthe liver lobules. You should also see someKupffer cell hyperplasia, again a commonfinding in hepatitis, especially viral hepatitis.What exactly are the Kupffer cells? Hint:think reticuloendothelial system.
This is it. You know, normal liver.
Your observations
136General and Systemic Histopathology, Braun, C601/C602 Liver and Gallbladder
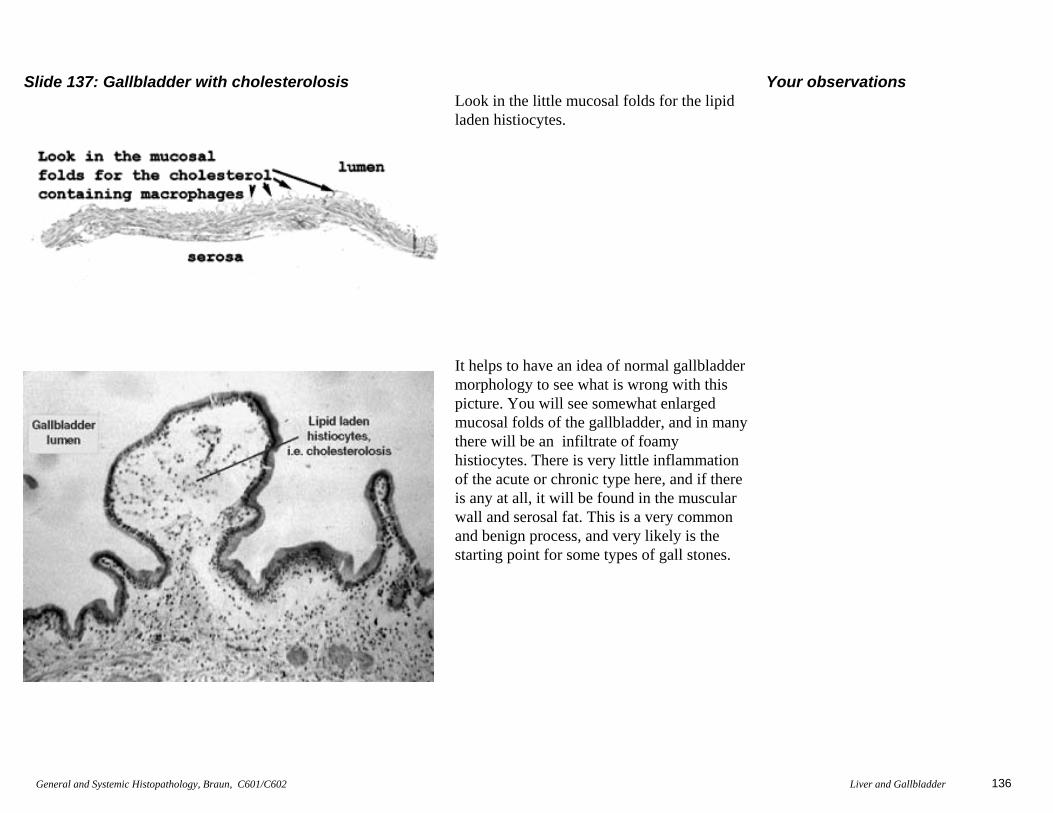
Slide 137: Gallbladder with cholesterolosisLook in the little mucosal folds for the lipidladen histiocytes.
It helps to have an idea of normal gallbladdermorphology to see what is wrong with thispicture. You will see somewhat enlarged mucosal folds of the gallbladder, and in manythere will be an infiltrate of foamyhistiocytes. There is very little inflammationof the acute or chronic type here, and if thereis any at all, it will be found in the muscularwall and serosal fat. This is a very commonand benign process, and very likely is thestarting point for some types of gall stones.
Your observations