PHTHISIOLOGY. Lecture 5 CLINICAL FORMS OF TUBERCULOSIS: Primary tuberculosis Secondary tuberculosis.
description

SECONDARY SECONDARY TUBERCULOSISTUBERCULOSIS
LECTURELECTURE
docdoc. . Kravchenko N.S.Kravchenko N.S.

DISSEMINATED TUBERCULOSISDISSEMINATED TUBERCULOSIS - APPERARS
DURING LYMPHOHEMATOGENOUS DISSEMINATION OF
THE INFECTION AND IS CHARACTERISED BY BILATERAL
SYMETRIC FOCAL LESION, WHICH IS LOCALISED IN
SUPERIOR AND CORTICAL PARTS OF LUNGS.
THERE IS ACUTE, SUBACUTE AND CHRONIC
DISSEMINATED TUBERCULOSIS OF LUNGS.
THIS FORM OF TUBERCULOSIS AFFECTS BONES,
KIDNEYS, GENITAL ORGANS , LARYNX, PLEURA, MORE
FREQUENTLY.

PPATHOGENESISPPATHOGENESISPPATHOGENIC FACTORS AREPPATHOGENIC FACTORS ARE:
1. - Presence of tuberculous infection in the organism.2. - Bacteriemia.
3. - Hypersensibilization and hyperpermeability of pulmonary
vessels. More frequently mycobacteries appear in blood from
affected intrathoracic lymthatic nodes. Through thoracic duct
subvclavian vein in right ventricle and futher in pulmonary
bifurcation and lungs.

Ways of MBT spreading.1 – haematogenous2 – lymphogenous3 - bronchogenous

Miliary tuberculosis

TABLE 1. Organ Involvement in Miliary Organ Involvement in Miliary
Tuberculosis at NecropsyTuberculosis at Necropsy
Organ (% involved):
Spleen 86%
Liver 91
Lungs 100
Bone marrow 24
Kidneys 62
Adrenals 14
Eye —
Thyroid 19


AS TO CLINICAL PROGRESS MILIARY AS TO CLINICAL PROGRESS MILIARY
TUBERCULOSIS IS CONDITIONALLY TUBERCULOSIS IS CONDITIONALLY
DIVIDED INTO:DIVIDED INTO:
-- LUNGLUNG
-- TYPHOIDTYPHOID - - MENINGEALMENINGEAL - - SEPTIC FORMSSEPTIC FORMS..

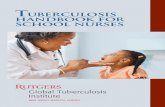
FIGURE 1. Chest radiograph of a patient with miliary tuberculosis. Note the extensive, symmetrical distribution of 2- to 3-mm lesions
throughout both lungs.

FIGURE 2. Close-up view of the chest radiograph in Figure 1. Note the uniform distribution of nodules throughout the lung parenchyma.


Subacute disseminated tuberculosisSubacute disseminated tuberculosis
This form of the tuberculosis develops during decreased resistance of the organism, in senile age, during immunodepression therapy. Pathologic anatomy. Subacute disseminated tuberculosis appears during affection of intralobular veins and intralobular branches of pulmonary artery. It results formulation of great simetric focuses (5-10 mm) in the superior parts of pulmonary fields.

Clinical pictureClinical picture. The start of disseminated tuberculosis can be
acute or gradual. In case of gradual start there are such symptoms:
fatiquabiliti, general weakness, poor apetite, dry couph, then pus-
mucus couph, blood sputum, chest pain, dyspnea.
General state of the patient changes for the worse, develops
circulatory insufficiency, caused by overload of right heart
chambers.
In some cases onset signs can be larynx lesion (painful
swallowing, hoarse voice) or kidneys’ affection.
Objective investigation is characterized by symmetric dull sound
under upper and middle pulmonary parts, auscultation - of harsh or
vesicular-bronchial breathing, moist fine bubbling rales.

LaboratoryLaboratory investigationinvestigation. Hypochromic anemia, leucocytosis (12-17x109), neutrophils elevation (10-15%), lymphopenia, monocytosis, elevation of the erythrocyte sedimentation rate are observed in blood picture. During distruction process mycobacterium in sputum can be observed. Mantu`s test is positive. Negative unergic process appears during progressive of the process. X-ray examinationX-ray examination. It is characterized by large symmetric focal shadows with uneven outlines, total or subtotal affection. These X-ray changes are typical and imitate the picture of “dropping snow”. Then appear lightings with irregular shape situated symmetrically in the upper lung segments.

Disseminated lung tuberculosis (subacute)

Disseminated lung tuberculosis (subacute)

“Stamped cavern” in the apper part of the right lung

Chronic disseminated tuberculosis of lungs.Chronic disseminated tuberculosis of lungs.
Appears in case of not entirely effective therapy of the subacute
disseminated tuberculosis, its observed more frequently as
independent form. Characterized by presence of temporary
remission of a disease and acute condition, which is caused by
bacteriemia, dissemination and infiltrating changes in lungs.
Pathologic anatomy. The process has apica-caudal dissemination
calcific focuses are situated in the upper segments of lungs, but there
are lower fresh focuses. Symmetric cavities are formed in the upper
segments, emphysema prevails in lower segments.

Chronic disseminated lung tuberculosis

X-ray examinationX-ray examination. During hematogenic dissemination on the X-
ray we can observe symmetrically situated focal shadows with weak
intensity and unclear outlines of shadows. Typical X-ray picture of
chronic disseminated tuberculosis formulates during long course:
multishaped focal shadows, with different intensity in superior and
median segments of lungs, deformation of the lung picture. In the
inferior segments we observe particulary clear lung field and poor
lung picture, wich is caused by emphysema.
Old focuses are situated in the superior segments, they are more
intensive with well contured outlines. Fresh focuses are in the
inferior segments, characterized by low intencity. Deformation of the
roots of lungs with superior disposition ("sign of willow branches") is
observed.

Chronic disseminated lung tuberculosis


Differential diagnosis.Differential diagnosis.
More frequently differential diagnosis carries out with:
- bilateral focal pneumonia,
- carcinomatosis
-silicosis
- sarcoidosis
-pulmonary congestion
For the comfirmation of diagnosis of the tuberculosis it is neccessary to pay attention on contact with affected persons, enduring of primary tuberculosis, pleuritis, focuses in the superior and cortical segments.

Bilateral nidus pneumonia

Sarcoidosis of the lungs and intrathorasic limph. nodes

Sarcoidosis of the lungs and intrathorasic limph. nodes

Carcinomatosis

Lung stagnation phenomena

Lung stagnation phenomena. Left-side transsudate

Focal ( Nidus) lung tuberculosis (FLT)Focal ( Nidus) lung tuberculosis (FLT)
In this form of tuberculosis, foci of specific
inflammation are formed in the lungs with a size up to 1cm,
single or multiple, 1-side or 2-side, localized not more 1-2
segment.

FLT is divided into:
1- Soft focal (acute) with fresh foci of exudative or productive
character
2 - Fibrouse focal (chronic) at which foci are surrounded with a
connective tissue capsule, sometimes with elements of
calcination; but places of active inflammative process could be
found. Lung tissue is sclerotized; there is possible bronchial
deformation, and pleural layers. Fibrous-focal tuberculosis
may be the next stage of development of soft-focal
tuberculosis or involution of other forms.

figfig. . 1 1 Focal lung tuberculosisFocal lung tuberculosis

figfig.2.2 R Roentgenogram. Focal lung tuberculosisFocal lung tuberculosis

Determination of activity of Determination of activity of
tuberculosis processtuberculosis process
Active are such tuberculosis
change at which specific process is not
finished and may progress or regress. It
must be treated. For determination of
process activity these criteria are used. .

The most informative criteria of activity of
tuberculosis process:
- Finding of MBT;
- X-ray criteria;
- Involution of the process under the
test treatment.

Infiltrative lung tuberculosis (ILT)Infiltrative lung tuberculosis (ILT)
ILT is a zone of specific
inflammation mostly of exudative
character, with size more than 1 cm, with
ability to progressing and destruction.

fig. 5. Cloudlike infiltrate
variants of infiltrate

figfig. 6.. 6. Round shaped infiltrate

FigFig. 7.. 7. Lobitis.

X-ray examination.X-ray examination. 1. On X-ray there’s seen a shadow, with diameter more than 1 cm that in tuberculosis has some specialties. 2. Localization in 1, 2, 6 segments (on anterior lower X-ray-above, under the clavicle and parahillary). 3. Non-homogenic structure due to more intensitive foci conditioned by old fibrosis formations around which infiltrate developed or by caseoua foci. Areas of lighting also condition non-homogenic of infiltrate during formation of destruction cavities. 4. Focal shadows with unclear borders around the inlitrate and in other parts of this or that lung as a result of lympha- or bronchogenoc dissemination; 5. “Road” to the root often as double stripe of infiltrated walls of bronchus is revealed often at tuberculosis infiltrate in destruction phase.

Infiltrative tuberculosis

fig.3 RRoentgenogram. . Infiltrative lung tuberculosisInfiltrative lung tuberculosisС6 С6 left lung with decayleft lung with decay

fig.4 RRoentgenogram. . Cloudlike infiltrate of left lungof left lung. .

Main signs Infiltrative tuberculosis
Pneumonia Infarct of lung Eosinophilic infiltrate
Cancer of lung
ANAMNESIS
Sometimes contact with tb patients, previous tb
Caught a cold, catharrh of upper respiratory ways, angina
Operation, trauma, trombophlebitis, heart diseases
Allergic diseases, helminths
Patients are men after 40, smoking
COURSE
Beginning often is gradual, acute. At tuberculostatic therapy regress is slow
The beginning is acute, fast regress after antibiotics
The beginning is acute
The beginning is not visible, rare acute
Gradual beginning, progressive worse condition
SYMPTOMS
Moderate toxication, fever, sweating, cough. Few ausculatative changes
High temperature, dyspnea, cough. Full ausculataive picture (wet and dry rhonchi)
Pain in chest, dyspnea. Above the infiltrate zone, there is dullness, bronchial breathing
None complains, sometimes cough, impermanent dry or wet rhonchi
Pain in chest, dyspnea, cough, a big tumor or complicated with atelectasis – dullness, sometimes dry rhonchi above infiltrate
ROENTGENO-LOGIC PICTURE
Not homogenic infiltrate in1, 2 or 6 segment. Road to root, injured places on the background and around infiltrate
Shadow in most cases is homogenic
Triangle homogeny shadow, apex towards the root. Rare shadow is round or oval. High state of diaphragm
Shadow with unclear margins like cotton tampon, often homogeny. Rapid appearance and disappearance of infiltrate.
At peripheral cancer the shadow is homogenic and tuberose. At central one the shadow goes out of root
OTHER METHODS OF INVESTIGATION
Positive Mantu test. At bronchoscopy there is a specific endobronchitis
At bronchiscopy there is unspecific endobronchitis
On ECG there are signs of overloading of right heart
Positive skin tests with specific allergen
Direct and indirect signs of tumor at bronchoscopy
Differential diagnosis at infiltrative tuberculosisDifferential diagnosis at infiltrative tuberculosis (table)

fig.8 RRoentgenogram. . Pneumonia of inferior part of left lungPneumonia of inferior part of left lung..

fig.9 RRoentgenogram. . Eosinophilic pneumoniaEosinophilic pneumonia. .

fig.10 RRoentgenogram. . Central cancer of left lungCentral cancer of left lung..

fig.11 Tomogram of right lungTomogram of right lung. . Infarct of lung ..

Caseous pneumonia
Caseous pneumonia is a clinical
form of tuberculosos with massive
caseous changes in lungs and
severe, progressive clinical course.

fig. 12 Lobar caseous pneumonia..

X-rayX-ray investigation determines massive uneven darkness of entire lung lobe during caseuos pneumonia, there can be separate intensive foci on the background of it. While next progressing of process shadow becomes almost homogenic, than on its background lightening of cavity destruction appears or gigantic caverns form. Lower lobar shadow in other regions of either lung’s broncho-dissemination processes appear.
During lobularlobular caseous pneumonia big processes with irregular margins are defined (if lobular caseous pneumonia appears on the background of disseminative tuberculosis, they are localized symmetrically in both lungs). During the progressing of disease in pneumonic foci appears multiple lightening of cavity destruction, in other lungs there are new bronchogenic injured places, which are united rapidly and destruct.

fig.13 Caseous pneumonia of left lung..Bronchogenic dissemination of right lung.

Caseous pneumonia

Staphylococcal pneumonia

LUNG TUBERCULOMALung tuberculoma is a distinct
by genesis encapsulated caseous formation exceeding 1
cm in diametre and having a chronic torpid course.

Homogenous tuberculoma

Layer-by-layer tuberculoma

Conglomerate tuberculoma

Tuberculoma of the cerebellum

Tuberculoma

FIBROUS-CAVERNOUS LUNG TUBERCULOSIS
Fibrous-cavernous lung tuberculosis is a chronic
destructive process, characterized by the presence of an old fibrous cavern, expressed fibrosis and nidi of bronchogenic dissemination in lung tissue, surrounding the cavern, or in other parts of the lungs; protracted undulant course with aggravations and remissions periods, constant or periodic bacterial secretion. In the social aspect fibrous-cavernous lung tuberculosis patients are invalids, predominantly of the 2-nd group.

Fibrous-cavernous
lung tuberculosis


Fibrous-cavernous lung tuberculosis

Stages of destructive process in lungs.
Fresh elastic cavity fibrous cavity disintegration

elastic cavity

Fibrous-cavernous lung tuberculosis

fibrous-cavernous lung tuberculosis

Possible ways of cicatrization of cavities.
1. scar;
2. hearths;
3. blocked cavity;
4. pseudocysts.



chronic abscess


CIRRHOTIC LUNG TUBERCULOSIS
Cirrhotic lung tuberculosis is a clinical form, that is characterized by the development of connective tissue in lungs and pleura as a result of involution of various clinical forms of lung tuberculosis or specific pleurisy, with the preservation of signs of tuberculous process activity, inclination to periodic aggravations and meagre mycobacterial secretion, but without the presence of an active cavern.
In patients with firstly diagnosed lung tuberculosis cirrhotic tuberculosis is observed very rarely, somewhat more frequently among the contingents of antitu-berculous dispensaries (up to 1 %).

Cirrhotic lung tuberculosis

Cirrhotic lung tuberculosis

Cirrhotic tuberculosis

Pleurogeniccirrhosis of
the leftlung