Scrotal Sonography - event.anobnic.ru · Technical requirements Linear-array transducer 12-18 MHz...
43
Scrotal Sonography Julia Geiger
Transcript of Scrotal Sonography - event.anobnic.ru · Technical requirements Linear-array transducer 12-18 MHz...

ScrotalSonography
Julia Geiger

Learning objectives
Technical basics: how to perform scrotal sonographyin children and adolescents
Most important scrotal pathologies in boys
Recognize and differentiate «acute scrotum»
No scrotal tumors and trauma
2

Technical requirements
Linear-array transducer12-18 MHz (high-frequency)
• use gray-scale ultrasound first• always perform Color doppler and spectral doppler !• adjust settings
3

Scrotal anatomy
4

Standard documentation
Start with transverse-plane image to compare both testiclesSymmetry in location, size and echogenicity?
5

Doppler: PRF (pulse repetition frequence adaption) low!
Standard documentation
6

Standard documentation: sagittal and transversal
Continue withunaffected side,Volumetry of both testicles
7

reliable Doppler evaluation of both testiclesrepeat, try to derive curve in the center!
Standard documentation
8

Standard documentation
Focus on epididymis:compare size, echogenicity and perfusion
9

Standard documentation
Do not forget spermatic cord!10

Acute scrotum
Testicular torsion Epididymitis
Acute idiopathicscrotal edema
Testicular appendagestorsion
11

11 yo boyscrotal pain for 4h, no swelling or redness
No scrotal swelling, symmetric echogenicity12

11 yo boyscrotal pain for 4h, no swelling or redness
symmetric size13

Doppler sonography:Asymmetric perfusion
testicular torsion!
14

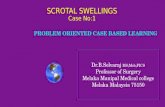
13 yo boyright scrotal pain since yesterday
Asymmetric testicular volume and echogenicity15

Suspicion of epididymitis with associated orchitis
Perfusion of both testicles, almost symmetric flow curves!
Swelling andhyperperfusion ofepididymis
hydrocele
16

Follow-up 4 days later…testicular torsion
Progressive swelling, no perfusion right testicle
17

Follow-up 2 days later after exploration and detorsion
Asymmetric echogenicity, no perfusion,right testicle necrotic
18

Testicular torsion
• ~25% of acute scrotum• Adolescents and newborns
• Acute pain, nausea, vomiting• Absent cremaster reflex, high-riding testicle
• Surgical emergency (testicular infarction)
• If clinically high suspicion, do not waste time with sonography«time is testicle» (max. 6 h for salvage)
19

Testicular torsion
Sonography:
• Testicle may look normal in first hours
• May mimick epididymitis
• Reactive scrotal edema or hydroceles
• May visualize torsed spermatic cord
• Color doppler useful for abnormal/reduced blood flow, but can be false negative (early or partial torsion)!
20

8 yo boyscrotal pain for 3 days, swelling, slight redness
Scrotal thickening, hydrocele
21

Epididymitis, hydrocele and slight orchitis
22

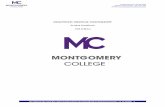
5 yo boyscrotal pain for 3 hours, swelling, flush
23

Epididymitis with hydrocele, scrotal swellingmarked hyperperfusion!
IncreasedDoppler flow!
24

Epididymitis
• ~30% of acute scrotum• Important: clinical history• Infectious inflammation (antibiotics)• In younger boys usually idiopathic,
in adolescents sexually transmitted• If recurrent, rule out urinary tract abnormalities
Sonography:
• Enlarged epididymis with hyperperfusion• Associated orchitis: testicle enlarged, hyperperfusion• Reactive hydrocele, scrotal wall thickening
25

6 yo boyrecurrent pain for 2 days, swelling
thickening of scrotum26

AISE = Acute idiopathic scrotal edema
Normal testicular andepididymal perfusion
Hyperperfusionscrotum
27

10 yo boyscrotal pain for about 18 h, no swelling or redness
thickening of scrotum
28

AISE = Acute idiopathic scrotal edema
thickening and hyperperfusion of scrotum29

Acute idiopathic scrotal edema (AISE)
• <10% of acute scrotum• Scrotal swelling and erythema• 4-7 yo boys• Idiopathic, self-limiting disease
Sonography:
• Scrotal wall thickening• Scrotal hyperemia («fontain sign»)• Normal testicles and epididymides
30

12 yo boyleft scrotal pain
31

Torsion of testicular appendage
Hydrocele, calcified structurefloating in hydrocele
32

Torsion of testicular or epididymal appendage(Hydatid torsion)
• Frequently in prepubertal boys• Torsion/Twisting of testicular appendage more frequent• Focal scrotal pain• Palpable nodule, bluish skin («blue dot sign»)
Sonography:
• Often no finding!• Oval avascular mass/nodule with variable echogenicity• Location frequently between testicle and epididymis• Associated scrotal edema and reactive hydrocele• Color Doppler may show surrounding hyperemia
33

What else to consider?
34

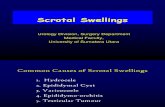
13 yo boyleft scrotal swelling for some years
35

VaricoceleValsalva enforces the dilation
36

Varicocele
symmetric volume?
(shunt or stop type?)
37

13 yo boyright scrotal pain for 3 h
Cyst or spermatocele epididymis38

1 yo boyswelling right inguinal region
Fluid collection in tunica vaginalis = hydrocele
39

2 yo boyswelling in right inguinal region
Funiculocele =Funicular hydrocele
40

6 yo boypainless swelling left scrotum for weeks
Lymphatic malformation
41

6 month old boyCryptorchism right
Retractile testiswith microlithiasis
42

Take home messages
Consider clinical information and history
Standardized sonography and documentation helpsto avoid errors
Side-by-side transverse view important
Recognize acute pathologies: testicular torsion = emergency vs. epididymitis vs. AISE and torsion of testicular appendages
43