Scientific Homeopathy
49
1 FUNDAMENTAL RESEARCH Dr. Girish Gupta* Dr. A. K. Srivastava** In-vitro activity of Thuja occidentalis Linn. against human pathogenic aspergilli INTRODUCTION Aspergilli are wide spread in the environment and are common inhabitants of soil. It is readily recog- nized that very large number of people, both adults and children are potentially exposed to such indoor and outdoor contaminants 1,2,3 . Several studies have provided evidence for the association of cancer in human with inhalation of aflatoxin contaminated dust 4,5,6 . It is now recognized that there are basi- cally three categories of disease involving Aspergilli viz. Allergic aspergillosis, colonizing aspergillosis and invasive aspergillosis 7,8,9 . Treatment of aspergil- losis with an antifungal drug such as amphotericin B is the first step of management but in neutropenic patients it is unsuccessful. Side effects and treat- ment duration may not be overlooked and is sug- gestive of finding a nontoxic safe remedy 9,10 . Thuja occidentalis, a tall tree belongs to the family Cupressaceae. Thuja is considered as antisycotic homoeopathic drug used mainly for wart - like ex- crescences upon mucus and cutaneous surface, vegetative condylomata and spongy tumors. Thuja is known to contain oil of thuja, a thujol, flavone gly- coside thujin and an acid called thujin. Antifungal action of Thuja occidentalis against Candida albi- cans, Trichophyton rubrum, and Trichophyton mentagrophytes is reported 11 . The present paper explores in-vitro antifungal potential of homoeo- pathic drug Thuja occidentalis Q, 30, 200, 1M, 10M and 50M against human pathogenic aspergilli. MATERIALS AND METHODS FUNGAL ISOLATES A) Aspergillus niger: A clinical isolate of patient complaining of chronic ear discharge for several years. Patients registered himself in GCCHR for the management of disease. MIC of ketoconazole for Aspergillus niger was standardized as 0.75 mg/ml by following the method of Jacob et al.12 - 13. B) Aspergillus flavus: Isolated from skin of the patient at GCCHR showing hyperpigmentation with severe itching. MIC of ketoconazole for Aspergillus niger was standardized as 0.50 mg/ml by following the same method as above 12 - 13 . MEDICINES Thuja occidentalis in various potencies like Q, 30, 200, 1M, 10M and 50M was purchased from manufacturer. Quantity of drug was standardised as 0.5 ml. CONTROLS Three controls were taken, one of sterile water, second of vehicle i.e. rectified spirit and third con- trol of Ketoconazole as positive control. Quantity of drug was taken as per their MIC calculated. * B. Sc., G.H.M.S. (Gold Medalist), Chief Consultant Physician ** M. Sc., Ph.D., Medical Mycologist, GAURANG CLINIC AND CENTRE FOR HOMOEO- PATHIC RESEARCH, B-1/41, Sector A, Near Rajshree Talkies, Kapoorthala, Aliganj, Lucknow-226 024 (UP), INDIA ABSTRACT In-vitro antifungal potential of homoeopathic drug Thuja occidentalis Q, 30, 200, 1M, 10M, 50M against Aspergillus flavus causing cutaneous aspergillosis and Aspergillus niger causing oto- mycosis in Human are evaluated by following food poisoning method. Thuja Q, 30, 200 are found highly potent against Aspergillus flavus and 50M against Aspergillus niger. Percent growth inhibition, sporulation and exudation are taken as parameters for assessment. Results are reported for the first time and are discussed in relation to homoeopathic concept "Higher dilu- tion and high energy". Keywords: Antifungal drugs, Thuja occidentalis, Aspergillus flavus, Aspergillus niger, Aspergil- losis This paper has already been published in Vol. 27, No. 1, January 2002 issue of 'The Homoeopathic Heritage' on pg. 5 - 12. The same is being reprinted here with the prior permission of the authors.
-
Upload
prabhat-tandon -
Category
Technology
-
view
5.668 -
download
3
description
Transcript of Scientific Homeopathy

1
FUNDAMENTAL RESEARCH
Dr. Girish Gupta* Dr. A. K. Srivastava**
In-vitro activity of Thuja occidentalis Linn. against human pathogenic aspergilli
INTRODUCTION
Aspergilli are wide spread in the environment andare common inhabitants of soil. It is readily recog-nized that very large number of people, both adultsand children are potentially exposed to such indoorand outdoor contaminants1,2,3. Several studies haveprovided evidence for the association of cancer inhuman with inhalation of aflatoxin contaminateddust4,5,6. It is now recognized that there are basi-cally three categories of disease involving Aspergilliviz. Allergic aspergillosis, colonizing aspergillosisand invasive aspergillosis7,8,9. Treatment of aspergil-losis with an antifungal drug such as amphotericinB is the first step of management but in neutropenicpatients it is unsuccessful. Side effects and treat-ment duration may not be overlooked and is sug-gestive of finding a nontoxic safe remedy9,10.Thuja occidentalis, a tall tree belongs to the familyCupressaceae. Thuja is considered as antisycotichomoeopathic drug used mainly for wart - like ex-crescences upon mucus and cutaneous surface,vegetative condylomata and spongy tumors. Thujais known to contain oil of thuja, a thujol, flavone gly-coside thujin and an acid called thujin. Antifungalaction of Thuja occidentalis against Candida albi-cans, Trichophyton rubrum, and Trichophyton
mentagrophytes is reported11. The present paperexplores in-vitro antifungal potential of homoeo-pathic drug Thuja occidentalis Q, 30, 200, 1M, 10Mand 50M against human pathogenic aspergilli.
MATERIALS AND METHODSFUNGAL ISOLATES
A) Aspergillus niger: A clinical isolate of patientcomplaining of chronic ear discharge for severalyears. Patients registered himself in GCCHR for themanagement of disease. MIC of ketoconazole forAspergillus niger was standardized as 0.75 mg/mlby following the method of Jacob et al.12 - 13.B) Aspergillus flavus: Isolated from skin of thepatient at GCCHR showing hyperpigmentation withsevere itching. MIC of ketoconazole for Aspergillusniger was standardized as 0.50 mg/ml by followingthe same method as above12 - 13.
MEDICINES
Thuja occidentalis in various potencies like Q, 30,200, 1M, 10M and 50M was purchased frommanufacturer. Quantity of drug was standardisedas 0.5 ml.
CONTROLS
Three controls were taken, one of sterile water,second of vehicle i.e. rectified spirit and third con-trol of Ketoconazole as positive control. Quantity ofdrug was taken as per their MIC calculated.
* B. Sc., G.H.M.S. (Gold Medalist), Chief ConsultantPhysician ** M. Sc., Ph.D., Medical Mycologist,GAURANG CLINIC AND CENTRE FOR HOMOEO-PATHIC RESEARCH, B-1/41, Sector A, Near RajshreeTalkies, Kapoorthala, Aliganj, Lucknow-226 024 (UP),INDIA
ABSTRACT
In-vitro antifungal potential of homoeopathic drug Thuja occidentalis Q, 30, 200, 1M, 10M, 50Magainst Aspergillus flavus causing cutaneous aspergillosis and Aspergillus niger causing oto-mycosis in Human are evaluated by following food poisoning method. Thuja Q, 30, 200 arefound highly potent against Aspergillus flavus and 50M against Aspergillus niger. Percent growthinhibition, sporulation and exudation are taken as parameters for assessment. Results arereported for the first time and are discussed in relation to homoeopathic concept "Higher dilu-tion and high energy".
Keywords: Antifungal drugs, Thuja occidentalis, Aspergillus flavus, Aspergillus niger, Aspergil-losis
This paper has already been published in Vol. 27, No. 1, January 2002 issue of 'The Homoeopathic Heritage' onpg. 5 - 12. The same is being reprinted here with the prior permission of the authors.

2
EXPERIMENTAL PROTOCOL
Antimycotic activity of homoeopathic drug Thujaoccidentalis Q, 30, 200, 1M, 10M, 50M prepared inrectified sprit was tested by poison food technique12
- 13 against test fungi Aspergillus niger and Aspergil-lus flavus. 0.5 ml of each drug was mixed with 10ml of Sabouraud's dextrose agar just before solidi-fication in 50 mm diameter petridishes. SDA plateswith 0.5 ml sterile water, 0.5 ml rectified spirit and0.5 ml containing 5 mg ketoconozole (200mg tabletdissolved in 20 ml water) for Aspergillus niger and0.75 ml for Aspergillus flavus were kept as controls.All the plates including controls were inoculatedcentrally with 1.5 mm diameter of disc of test fungiaseptically from 8 to 10 days old SDA plates cul-ture. All the experimental petridishes were used intriplicates and incubated at 37°C. The linear dia-metrical growth of colonies were measured (in cm.)on 3rd, 6th and 9th days of post inoculation. Theresults were presented on an average of three plateson 9th days of post inoculation. Percent growth in-hibition was calculated as per formula.
dc = Colony diameter of controldt = Colony diameter of treated plate
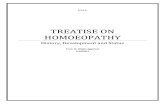
RESULTS
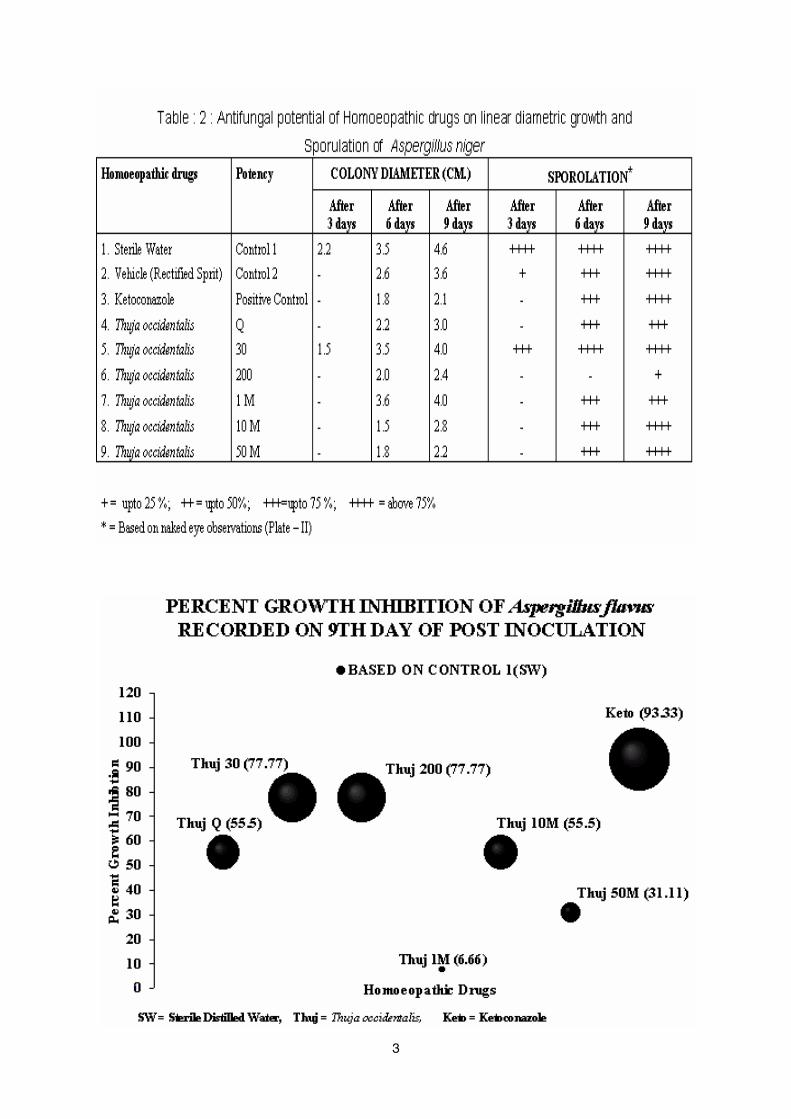
Antifungal efficacy of homoeopathic drug Thujaoccidentalis Q, 30, 200, 1M, 50M have beenpresented in Tables - 1 and 2 against Aspergillusflavus and Aspergillus niger. Thuja 30, 200 are foundto inhibit the linear diametric growth of Aspergillusflavus equally on 9th day of post inoculation. Thuja1M showed no effect, the growth of Aspergillusflavus was almost equal to control I (SW) and morethan control II (RS) (Table - 1). Other potenciesshowed less sporulation in comparison to controlsbut Thuja 30 and 200 showed no sporulation (Plate- I; figs : 5 - 6). Percent growth inhibition ofAspergillus flavus on 9th day of post inoculation arepresented in figs. 10 and 11. Fig. 10 is based oncontrol I (SW) and fig. 11 is based on control II (RS).It is evident from the figs. 10 - 11 that Thuja 30 andThuja 200 showed maximum inhibition i.e. 77.77%in each as compared to control I and 64.28% ineach as compared to control II. Percent growthinhibition of positive control i.e. ketoconazole was93.33 and 89.28 as compared to control I and controlII respectively. Thuja 30 and Thuja 200 was less by15.56 percent in each as compared to ketoconazolebased on control I and 25 percent in each ascompared ketoconazole based on control II.
Thuja 50 M was very effective against Aspergillusniger. Colony diameter observed was 2.2 mm al-
3
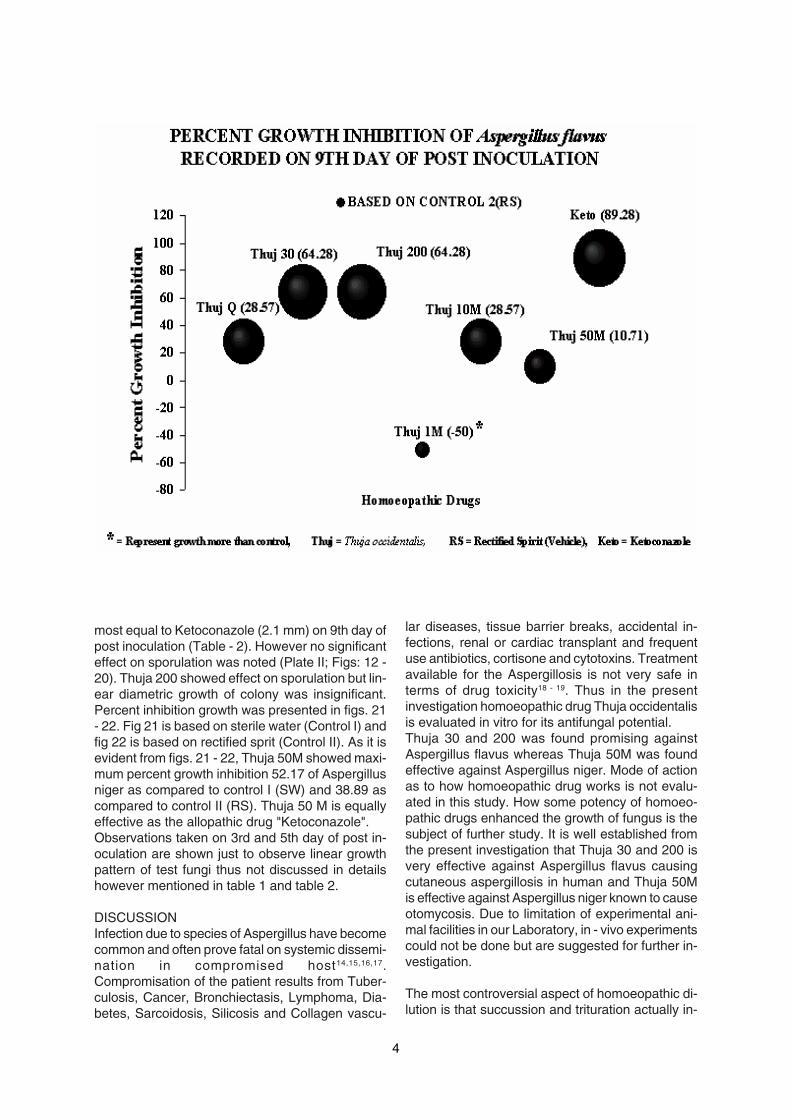
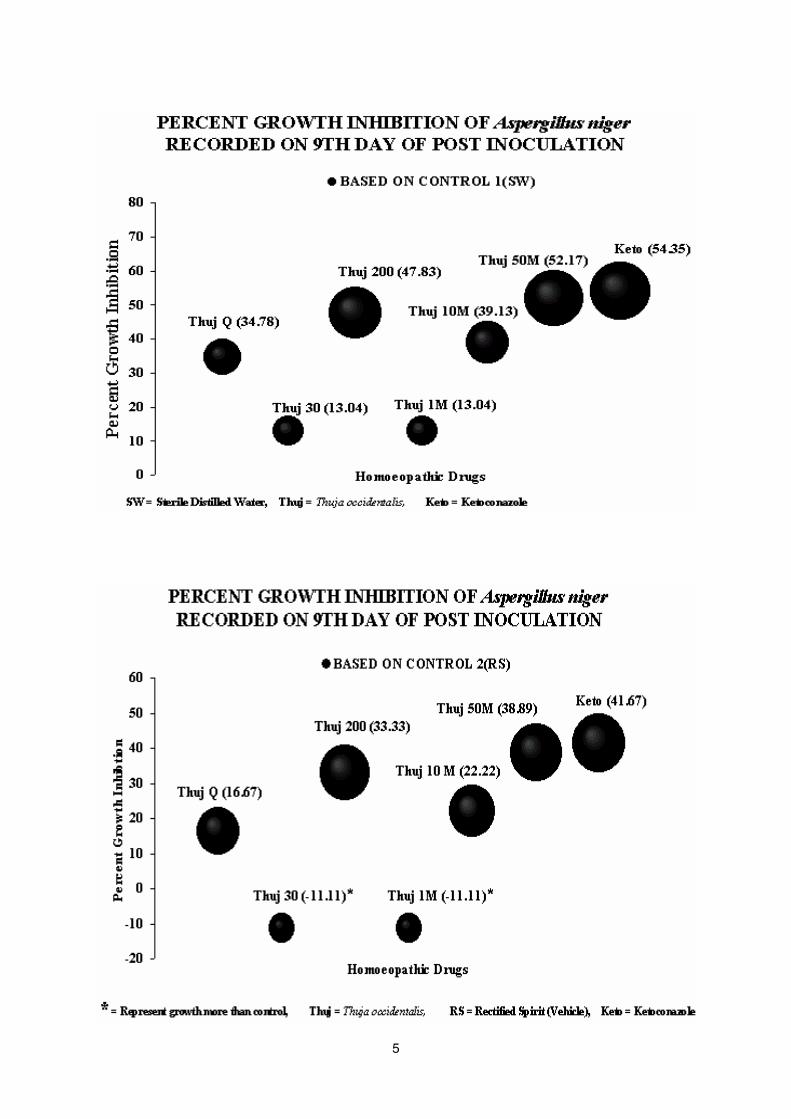
4
most equal to Ketoconazole (2.1 mm) on 9th day ofpost inoculation (Table - 2). However no significanteffect on sporulation was noted (Plate II; Figs: 12 -20). Thuja 200 showed effect on sporulation but lin-ear diametric growth of colony was insignificant.Percent inhibition growth was presented in figs. 21- 22. Fig 21 is based on sterile water (Control I) andfig 22 is based on rectified sprit (Control II). As it isevident from figs. 21 - 22, Thuja 50M showed maxi-mum percent growth inhibition 52.17 of Aspergillusniger as compared to control I (SW) and 38.89 ascompared to control II (RS). Thuja 50 M is equallyeffective as the allopathic drug "Ketoconazole".Observations taken on 3rd and 5th day of post in-oculation are shown just to observe linear growthpattern of test fungi thus not discussed in detailshowever mentioned in table 1 and table 2.
DISCUSSIONInfection due to species of Aspergillus have becomecommon and often prove fatal on systemic dissemi-nation in compromised host14,15,16,17.Compromisation of the patient results from Tuber-culosis, Cancer, Bronchiectasis, Lymphoma, Dia-betes, Sarcoidosis, Silicosis and Collagen vascu-
lar diseases, tissue barrier breaks, accidental in-fections, renal or cardiac transplant and frequentuse antibiotics, cortisone and cytotoxins. Treatmentavailable for the Aspergillosis is not very safe interms of drug toxicity18 - 19. Thus in the presentinvestigation homoeopathic drug Thuja occidentalisis evaluated in vitro for its antifungal potential.Thuja 30 and 200 was found promising againstAspergillus flavus whereas Thuja 50M was foundeffective against Aspergillus niger. Mode of actionas to how homoeopathic drug works is not evalu-ated in this study. How some potency of homoeo-pathic drugs enhanced the growth of fungus is thesubject of further study. It is well established fromthe present investigation that Thuja 30 and 200 isvery effective against Aspergillus flavus causingcutaneous aspergillosis in human and Thuja 50Mis effective against Aspergillus niger known to causeotomycosis. Due to limitation of experimental ani-mal facilities in our Laboratory, in - vivo experimentscould not be done but are suggested for further in-vestigation.
The most controversial aspect of homoeopathic di-lution is that succussion and trituration actually in-
5
6
crease the power of remedy. Clinical efficacy of highdilution is well established in homoeopathic science.But in the present investigation it is proved that thereis no increase in the activity of higher dilution. Thuja30 and 200 is effective against Aspergillus flavushowever higher dilution 1M, 10M and 50M is noteffective which contradicts theory of high dilutionand high energy. The present investigation consti-tute the first report for proving in vitro action of ho-moeopathic drug Thuja occidentalis Q, 30, 200, 1M,10M, 50M against human pathogenic fungi viz. As-pergillus flavus and Aspergillus niger. The findingsalso disqualify the concept of higher energy andhigh dilution in the system of fungi - a eukarolic or-ganism. Similar results were also observed by Singhand Gupta et al.20,21,22 and proved antiviral efficacyof homoeopathic drugs against plant and animalviruses. Sharma 1998 suggested vital force iscertainly a form of Sharmon-composed "basic sub-stance" which mediates the molecular mechanismsunderlying vital functions of health and disease andalso potentization of medicines throughdynamization processes as human cells23. Vitalforce concept requires updation in the term of en-ergy quanta, their measuring parameters and con-stitutional suitability of potency to the patients andtheir disease.
REFERENCES
1. Srivastava A. K., 1991, Air pollution(Biopollutants in air), Ashish Publishing House, NewDelhi, pp. 302.
2. Srivastava A. K., 1992, Mould Allergy - anoverview, Advances in Medical Mycology edited byMukherji et al., Aditya Books, New Delhi, pp. 63 -80.
3. Nair M. V., Gupta S., Srivastava A. K.(eds),1996, Environmental biopollutants and humanhealth, Anmol Publication Pvt. Ltd., New Delhi, pp.199.
4. Dvorackova I, 1976, Aflatoxin inhalation andalveolar cell carcinoma. Br. Med J III : 691
5. Olsen J. H., Dragsted L., Autrup H., 1998,Cancer risk and occupational exposure to aflatoxinsin Denmark. Br. J Cancer 58: 392 - 396.
6. Hayes R. B., Van Nieuwenhuze J. P.,Raatgever J. W., Ten Kate F. J. W. 1984, Aflatoxinexposures in the industrial setting : an epidemio-logical study of morality. Food Chem Toxicol 22: 39- 43.
7. Rippon J. W., 1988, Medical Mycology. Thepathogenic fungi and the pathogenic actinomycetes,W.B. Saunders Company, Philadelphia. pp. 797
8. Emmon's E. W., 1977, Medical Mycology,Lea & Febiger, Philadelphia.
9. Srivastava O. P., Srivastava A. K., ShuklaP. K., 1988, Advances in Medical Mycology Vol. 2,Evoker Research Perfecting Company, Lucknow.pp. 182
10. Gupta G., Srivastava A. K., Gupta N., 1997,Mycoses: An update over clinical cure with Homoeo-pathic drugs. Asian Homoeopathic Journal 7(4) :67-96
11. Akhtar Husain et al. 1992, Directory of IndiaMedicinal plants, Central Institute of Medicinal andaromatic plants, India pp 546.
12. Wahab S., Srivastava. O. P., Singh N. B.,Gupta S. K., 1978, Comparative in vitro and in vivoevaluation of toliciclate, tonaftate, miconazole,clotrimazole and undecylenic acid against Tricho-phyton mentagrophytes. Indian J. Exp. Biol., 16,1200 - 1202.
13. Wahab, S., Tandon, R. N., Jacob, Z., Sagar,P. & Srivastava, O. P., 1981, In vitro activity ofphytochemical alantolactone from Inula racemosaHook f. against some pathogenic and opportunisticfungi. J. Indian Bot. Soc., 60, 278 -281.
14. Srivastava A. K., Garg K. L., Neelima Garg,1992, Health risk associated with fungal agents fromsludge, Advances in Medical Mycology edited byMukherji et. al., Aditya Books, New Delhi, pp. 145 -156.
15. Wadhwani K., Srivastava A. K., 1984, Fungifrom Otitis media of agricultural field workers,Mycopathologia 88 : 155 -159.
16. Wadhwani K., Srivastava A. K., 1985, Somecases of Onchomycosis from North India in differ-ent working environment Mycopathologia 92 : 149- 266.
17. Das Gupta S. N., Shome S. K., 1959, Stud-ies in Medical Mycology I - On the occurrence ofmycotic diseases in Lucknow. Mycopath. & MycolAppl., 10: 177-186.
18. Varma R. S., 1997, Antifungal agents fromnatural products, National seminar on "Emerging

7
trends in the management of fungal (Mycotic) in-fections", Nov. 14 - 16, 1997, at Industrial Toxicol-ogy Research Centre, Lucknow, organized by Na-tional Academy of Chemistry and Biology (India),abstract no. 11.
19. Srivastava A. K., Singh K. P., Ray P. K., 1997,Protein A induced protection against experimentalCandidiasis in mice Mycopathologia 138: 21-28.
20. Singh L. M., Gupta G., 1985, "Antiviral effi-cacy of Homoeopathic drugs against animal vi-ruses", The British Homoeopathic Journal, 74(3):168 - 174.
21. Singh B. P., Gupta G., Srivastava K. M.,1980, "Homoeopathic Drugs as inhibitors of To-bacco Mosaic Virus", (1980), Indian Journal of Ho-moeopathy IV(7) : 301 - 303.
22. Khurana Paul S. M., Gupta G., 1981, "Ho-moeopathy: Promises & Prospects for plant pro-tection", Advancing Homoeopathy 1: 107 - 116.
23. Sharma R. R., 1998, The vital force: An up-date proceedings of 8th National homoeopathicconference 3rd and 4th April 1998, Eds. - Arora et.al., organized by Research Society of homoeopa-thy, Lucknow.
8
DRUG PROVING
A Systematic Review of Homeopathic Pathogenetic Trials from 1945 To 1995
Flávio Dantas! , Peter Fisher, D.P.Rastogi, Dick Koster,Maria Eugenia Pulido Alvarez, José Eizayaga, Frank Wieland,Harald Walach, Hélio Teixeira, Jean Pierre Jansen,Luc Louis Maurice Weckx, Matheus Marim, Philippe Belon
BACKGROUND
Homoeopathic pathogenetic trials (HPTs)are the basic method of homoeopathy. They aredesigned to investigate body and mind effects ofpotentially toxic or pathogenic substances, dilutedand serially agitated according to homoeopathicpharmacopoeias, in non-patient volunteers in goodand relatively stable health conditions. They areclinical trials designed to assess the effects of highlydiluted medicines in healthy volunteers, the resultsare applied in practice on the basis of ‘Similiasimilibus curentur’.
The methodology of HPTs was first proposedby Hahnemann. The controlled investigation of thepathogenetic power of medicines was one yardstickin Hahnemann’s writings. Hahnemann recognizedearly in the Organon1 the main methodologicalproblems of HPTs, namely truthfulness ofvolunteers, to use medicines with different powersand to deal with individual differences. In attemptingto minimize the effects of suggestion on volunteersHahnemann recommended that “in the investigationof these drug-symptoms all suggestion must be asrigidly avoided as in the examination of thesymptoms of disease”. To obtain symptoms asaccurately as possible, every subject had a pocket-size notebook to write down the sensations andchanges immediately after they occurred. Thevolunteers were required to repeat the descriptionof the changes without referring to this notebookduring the personal interview: if the accounts variedhe advised the director of the trial to confront thesubject with both versions and invite him to chooseand confirm the statement which is nearest to thetruth. Prevention of guess-work, imagination andrecording of findings only after close questioningwere continuously stressed in different editions ofthe Organon. For him only reliable symptomsshould be included in the homoeopathic materiamedica.
However a critical analysis of Hahnemann’smethod to conduct HPTs raised many flaws andsystematic errors2, given our current knowledge,which could not be anticipated by Hahnemann atthat time, leading to an over-estimation of medicineeffects. Some of them are described below:
� Absence of control group� Use of well-known friends and lecture
audiences as volunteers (“believers”)� Volunteers informed that they were using
a medicine to observe effects upon them� Recording of all complaints, symptoms
and changes observed during the actionof the medicine even if the person hasnoticed similar symptoms in himself aconsiderable time before
� Absence of masking in volunteers or insupervisors of the trial
� Close supervision and daily (or 2-3 days)interview with subjects + daily recordingin a pocket notebook
� Sudden prohibition of coffee, tea, spicesand alcoholic drinks (or medicinal drugs)
� Vague definition of healthy volunteers==> Inclusion of non-healthy volunteers
� No random assignment of subjects
Taken together these flaws are sufficient to causeserious doubts on the scientific acceptability of thespecific pathogenetic symptoms reported inHahnemann’s writings. This was partially confirmedin a preliminary systematic review of HPTs publishedin the UK from 1945-1995, including 45 studies,which showed a great deal of variability in terms ofthe medicines tested, methodology, volunteers,sample size and outcome. This was reflected in greatvariability in the numbers, incidence and types ofeffects reported. There was also a clear associationbetween the methodological quality of the trial and
!Universidade Federal de Uberlândia / Universidade Federal de São Paulo (Brazil). Former Visiting Research Fellow, The Royal London Homoeopathic Hospital (UK)* Originally published in the transactions of the conference "Improving the Success of Homeopathy 5: A Global Perspective", London 26-27 january 2006.
DRUG PROVING

9
the numbers of effects reported: better trials produceda lower incidence of pathogenetic effects (or none)compared to trials of poorer quality. Overall theanalysis of reports revealed methodologicalshortcomings which could seriously compromise thevalidity, reliability and clinical applicability of theresults3.
To what extent have HPT incorporated newmethods developed in scientific medicine in the fivedecades from 1945 to 1995? Can we rely on theconclusions drawn from HPT done during thisperiod? A systematic review of published studieswas therefore designed to assess the methods andoutcomes of HPTs published in six languages(English, German, Spanish, French, Portugueseand Dutch) in the five decades from 1945 to 1995and to help design and conduct future HPT to getmore valid and reliable information.
METHODS
A criterion-based systematic review of HPTswas done in trials published in six languages from1945 to 1995. The literature was exhaustivelysearched and only published reports of HPTs wereincluded. Information was extracted by twoindependent reviewers, with experience inconducting HPT or clinical research, using aspecially developed form with 87 items. Informationon: medicines, volunteers, ethics, blinding,randomisation, use of placebo, adverse effects,assessments, presentation of data and number ofclaimed findings were recorded.
For each medicine the name , dilution(s),method of dilution, presentation, dose, frequencyper day, repetition of doses, total duration of thetrial, number of active treatment periods andduration per volunteer (in days), source of the drug,mode of preparation and preparation responsibilitywas recorded. Regarding the study population weextracted the initial and final number, ethnic origin,sex, age, occupation, number of control volunteers,percentage of sensitive volunteers, inclusioncriteria, exclusion criteria, assessment of healthstatus prior to admission, training of volunteers,personality traits, physical characteristics, informedconsent, method of recruitment.
The study method was assessed in termsof: approval of protocol by Ethical Committee,direction/coordination, randomization, sequencegeneration of subjects in the trial, allocationconcealment, masking (blindness) of volunteersand of supervisor, use of placebo, pre-trialobservation period with or without placebo, placebo
distinguishable from verum, placebo potentised,comparative group, crossover, washout period(post-treatment observation), management ofadverse effects, rules for stopping medicine,rationale and source of the medicine. Theassessment of each trial was recorded in terms of:use of symptom diary, type of diary, initial interview(case-taking/ collection of previous symptoms),follow-up interview, use of laboratory investigations,use of psychological tests, withdrawal/dropout ofvolunteers, reason for withdrawal, withdrawal dueto severe adverse effects, presence of adverseeffects, pre-defined categories for assessment ofthe attributes of a symptom.
For the presentation of results we extractedinformation on the frequency of symptoms in thesample, description of complete symptoms,analytical presentation, chronology of symptoms,character of symptoms, location of symptoms,duration of symptoms, onset of symptoms, intensityof symptoms, modalities of symptoms, presenceof concomitant symptoms, inclusion of priorsymptoms that improved during the trial, detailedreport of individual volunteers, use of symptomtables and charts.
The interpretation of the results by theauthors was reviewed in terms of : pre-definedcriteria to include medicine effects, use ofdescriptive statistics (measures of central tendencyor dispersion of data), use of statistical tests andpresence and number of significant findingsclaimed.
Finally, each reviewer was invited to makea subjective judgement: ‘after reading and analysingall the points above, and based exclusively on thepublished report’:
- Do you think the symptoms stated asbelonging to the medicine can be trusted ?
- Would you apply the information given in itinto your clinical practice to prescribe thismedicine to a patient? For both questionsthe options were certainly, almost certainly,probably, possibly, with serious reservations,definitely not, can’t answer or none claimed
- From a methodological point of view, youjudge this report of proving as: completelyreliable, very reliable, reliable, unreliable,completely unreliable
- Compared to the other reports you read, youthink this is: below average, average, aboveaverage, much above average, excellent.A final, open question asked about the main
methodological criticisms of the reviewer to eachstudy.
10
The methodological quality of publishedHPTs was assessed by a specially designed index,using mainly traditional indicators of quality inclinical trials, complemented by a personaljudgement of reviewers for each study. Scoreswere organized in 4 methodological classes, where
SCOREVariable 1 2 3 4
Randomization Not Only stated, Incomplete, description Complete, descriptionstated no details of sequence generation of sequence
or allocation concealment generation andallocationconcealment
Blinding Not Single blind Double-blind without Double-blind withstated checking checking after
finishing the studyInclusion and Not One partially One clearly stated or Clearly statedExclusion stated stated both partially statedCriteria
Criteria for Not At least one 2 to 4 defined More than 4 definedSelection of stated stated defined
class I is the worst and class IV is the best qualityHPT. Cutoff points of score for the different classeswere 4,5,6 for Class I, 7,8,9,10 for Class II, 11,12,13for Class III and 14,15,16 for Class IV. TheMethodological Quality Index for homeopathicpathogenetic trials is shown below:
Pathogenetic effects were defined as allclinical events and laboratory findings noted byvolunteers during a HPT and recorded in the finalreport. In other words they are the findings claimedat the end of the trial by authors to be used bypractitioners seeing patients with similar pictures.We counted as one pathogenetic effect a piece ofinformation which could be included in anhomoeopathic repertory as an independentsubheading. For instance “boring headacheameliorated by pressure” was counted as oneclaim.
PRELIMINARY RESULTS AND DISCUSSION
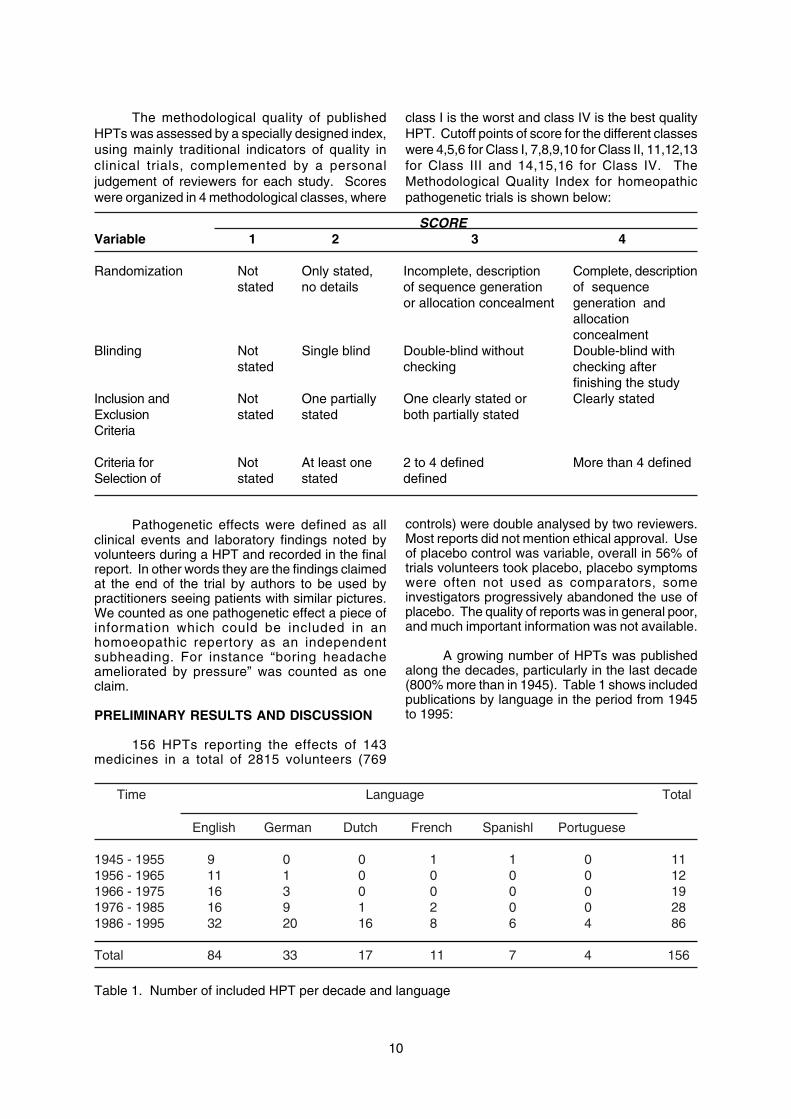
156 HPTs reporting the effects of 143medicines in a total of 2815 volunteers (769
controls) were double analysed by two reviewers.Most reports did not mention ethical approval. Useof placebo control was variable, overall in 56% oftrials volunteers took placebo, placebo symptomswere often not used as comparators, someinvestigators progressively abandoned the use ofplacebo. The quality of reports was in general poor,and much important information was not available.
A growing number of HPTs was publishedalong the decades, particularly in the last decade(800% more than in 1945). Table 1 shows includedpublications by language in the period from 1945to 1995:
Time Language Total
English German Dutch French Spanishl Portuguese
1945 - 1955 9 0 0 1 1 0 111956 - 1965 11 1 0 0 0 0 121966 - 1975 16 3 0 0 0 0 191976 - 1985 16 9 1 2 0 0 281986 - 1995 32 20 16 8 6 4 86
Total 84 33 17 11 7 4 156
Table 1. Number of included HPT per decade and language
11
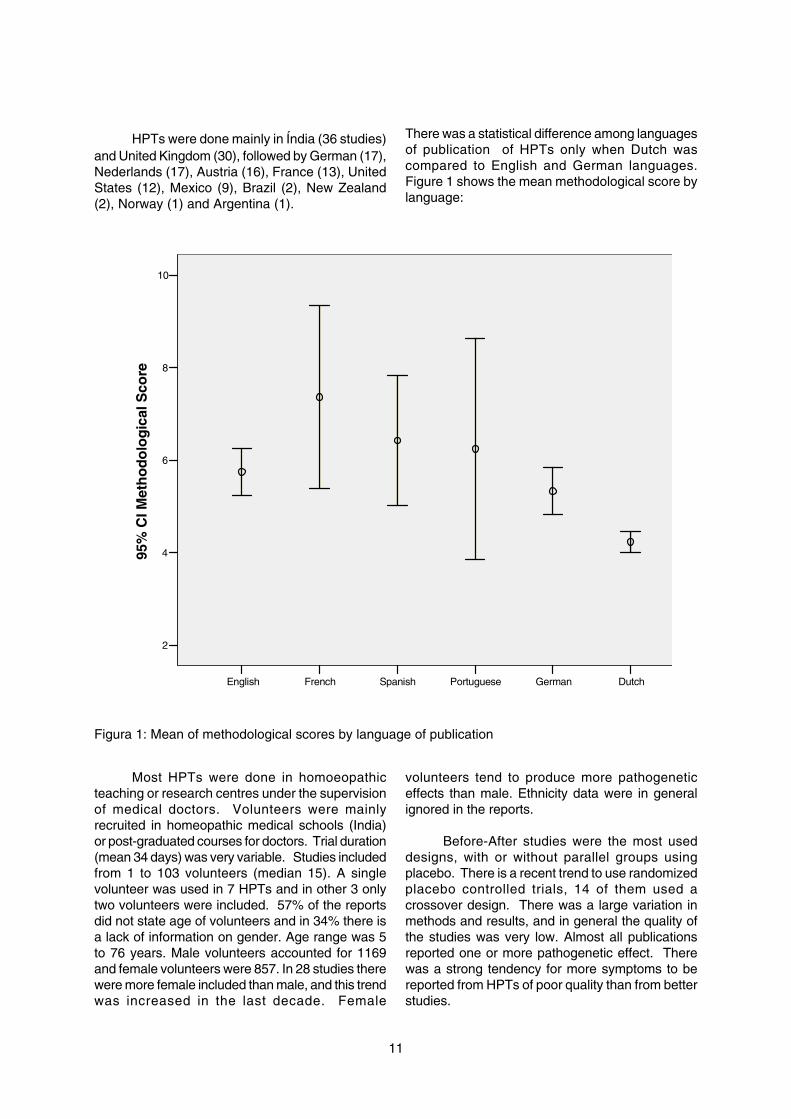
HPTs were done mainly in Índia (36 studies)and United Kingdom (30), followed by German (17),Nederlands (17), Austria (16), France (13), UnitedStates (12), Mexico (9), Brazil (2), New Zealand(2), Norway (1) and Argentina (1).
There was a statistical difference among languagesof publication of HPTs only when Dutch wascompared to English and German languages.Figure 1 shows the mean methodological score bylanguage:
DutchGermanPortugueseSpanishFrenchEnglish
10
8
6
4
2
95%
CI M
eth
od
olo
gic
al S
core
Figura 1: Mean of methodological scores by language of publication
Most HPTs were done in homoeopathicteaching or research centres under the supervisionof medical doctors. Volunteers were mainlyrecruited in homeopathic medical schools (India)or post-graduated courses for doctors. Trial duration(mean 34 days) was very variable. Studies includedfrom 1 to 103 volunteers (median 15). A singlevolunteer was used in 7 HPTs and in other 3 onlytwo volunteers were included. 57% of the reportsdid not state age of volunteers and in 34% there isa lack of information on gender. Age range was 5to 76 years. Male volunteers accounted for 1169and female volunteers were 857. In 28 studies therewere more female included than male, and this trendwas increased in the last decade. Female
volunteers tend to produce more pathogeneticeffects than male. Ethnicity data were in generalignored in the reports.
Before-After studies were the most useddesigns, with or without parallel groups usingplacebo. There is a recent trend to use randomizedplacebo controlled trials, 14 of them used acrossover design. There was a large variation inmethods and results, and in general the quality ofthe studies was very low. Almost all publicationsreported one or more pathogenetic effect. Therewas a strong tendency for more symptoms to bereported from HPTs of poor quality than from betterstudies.
12
65 publications tested medicines in single dilutionsand 91 in different dilutions used by the same ordifferent volunteers. In total 323 dilutions were used,mostly centesimal (192) followed by decimal (129)and fifty millesimal (2). 30c was the most frequentlyused dilution in our sample (66 trials) followed by6c (33) and 6x (32). More than 50% of the testedmedicines were not studied before the study tookplace.
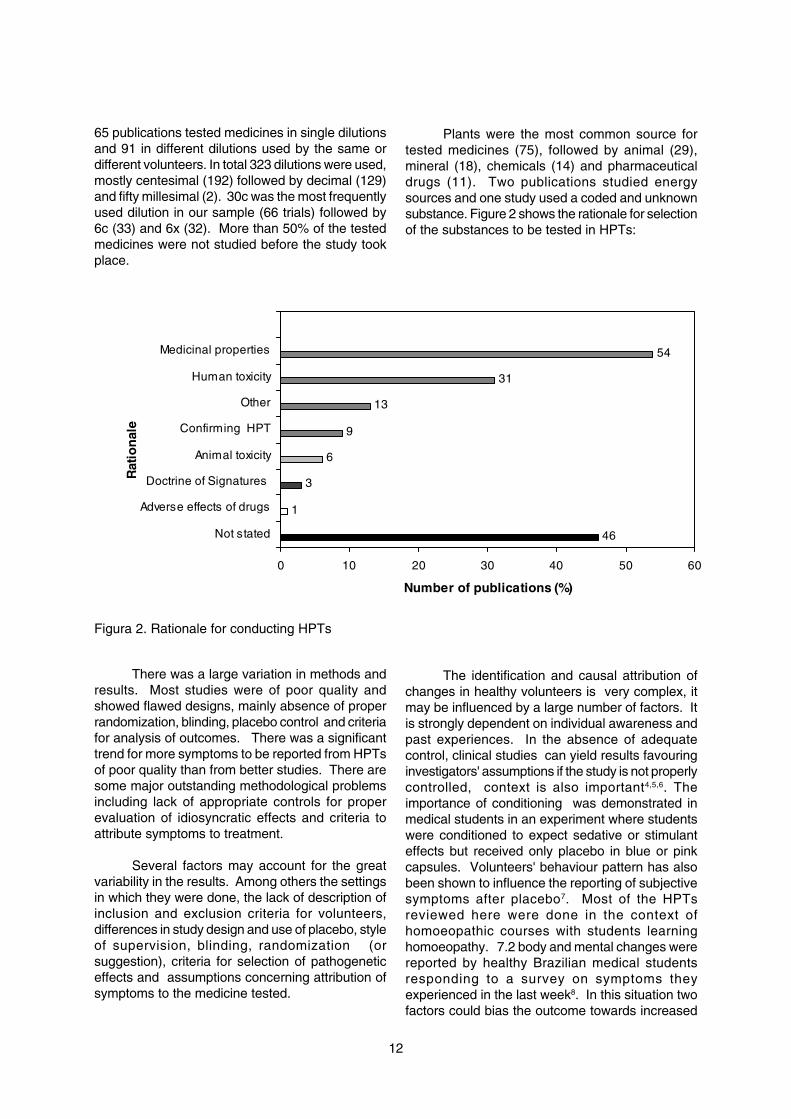
Plants were the most common source fortested medicines (75), followed by animal (29),mineral (18), chemicals (14) and pharmaceuticaldrugs (11). Two publications studied energysources and one study used a coded and unknownsubstance. Figure 2 shows the rationale for selectionof the substances to be tested in HPTs:
46
1
3
6
9
13
31
54
0 10 20 30 40 50 60
Not stated
Adverse effects of drugs
Doctrine of Signatures
Animal toxicity
Confirming HPT
Other
Human toxicity
Medicinal properties
Rat
ion
ale
Number of publications (%)
Figura 2. Rationale for conducting HPTs
There was a large variation in methods andresults. Most studies were of poor quality andshowed flawed designs, mainly absence of properrandomization, blinding, placebo control and criteriafor analysis of outcomes. There was a significanttrend for more symptoms to be reported from HPTsof poor quality than from better studies. There aresome major outstanding methodological problemsincluding lack of appropriate controls for properevaluation of idiosyncratic effects and criteria toattribute symptoms to treatment.
Several factors may account for the greatvariability in the results. Among others the settingsin which they were done, the lack of description ofinclusion and exclusion criteria for volunteers,differences in study design and use of placebo, styleof supervision, blinding, randomization (orsuggestion), criteria for selection of pathogeneticeffects and assumptions concerning attribution ofsymptoms to the medicine tested.
The identification and causal attribution ofchanges in healthy volunteers is very complex, itmay be influenced by a large number of factors. Itis strongly dependent on individual awareness andpast experiences. In the absence of adequatecontrol, clinical studies can yield results favouringinvestigators' assumptions if the study is not properlycontrolled, context is also important4,5,6. Theimportance of conditioning was demonstrated inmedical students in an experiment where studentswere conditioned to expect sedative or stimulanteffects but received only placebo in blue or pinkcapsules. Volunteers' behaviour pattern has alsobeen shown to influence the reporting of subjectivesymptoms after placebo7. Most of the HPTsreviewed here were done in the context ofhomoeopathic courses with students learninghomoeopathy. 7.2 body and mental changes werereported by healthy Brazilian medical studentsresponding to a survey on symptoms theyexperienced in the last week8. In this situation twofactors could bias the outcome towards increased

13
reporting of symptoms: the students, believers inthe system and the production, in the past, of validsymptoms from HPTs; and the coordinatorexpecting the students to give him useful informationafter testing the substance.
The consistency of the effects across trialsis another matter. Many investigators seemed tohave taken for granted that every substance mustelicit symptoms and for this reason felt itunnecessary to use placebo as a control or failedto include symptoms experienced by volunteerstaking placebo. On the other hand the use ofplacebo exclusively for comparative statisticalpurpose excludes from consideration rare,idiosyncratic effects. Attempts by Martini in the1930's to evaluate the occurrence of pathogeneticeffects due to highly diluted substances in HPTswere, on the whole negative, a critical reappraisalof his results shows that no definite conclusion canbe drawn9.
Further methodological improvements fordesigning rigorous HPT are required. In the last
decades several attempts to develop newapproaches to test homeopathic medicines inhealthy volunteers were done, either for testing newsubstances10 or to confirm results11,12. It is urgentto improve the quality of reporting and it is imperativeto have a consensus on minimal requirements forreporting HPT. The central question of whetherhomoeopathic medicines in high dilutions canprovoke effects in healthy volunteers has not yetbeen definitively answered. We need a purehomeopathic materia medica, with valid and reliableinformation from HPT, to get better results in ourclinical practice and research.
Acknowledgements
CNPq (Conselho Nacional de DesenvolvimentoCientífico e Tecnológico do Brasil); Royal LondonHomoeopathic Hospital; Cecília Lomônaco de Paulaand Gleice Margarete de Souza Conceição forstatistical advise; Mary Gooch for help in literaturesearch; David Riley for early cooperation ininforming HPTs done in USA.
REFERENCES
1. Hahnemann S. The Organon of Medicine. Los Angeles; J.P. Tarcher, 1982.2. Dantas F. How can we get more reliable information from homoeopathic pathogenetic trials? A
critique of provings. Br. Hom. J. 1996; 85: 230-236.3. Dantas F, Fisher P. A systematic review of homoeopathic pathogenetic trials ('provings') published
in the United Kingdom from 1945 to 1995. In: Ernst E, Hahn EG. Homoeopathy: a critical appraisal.London: Butterworth-Heinemann; 1998. p. 69-97.
4. Green DM. Pre-existing conditions, placebo reactions and "side effects". Ann Int Med 1964;60:255-265.
5. Reidenberg MM, Lowenthal DT. Adverse nondrug reactions. New Eng J Med 1968; 279:678-9.
6. Meyer FP, Troger U, Rohl FW.Adverse nondrug reactions: an update. Clin Pharmacol Ther.1996;60(3):347-52.
7. Drici M, Raybaud F, De Lunardo C, Iacono P, Gustovic P. Influence of the behaviour pattern onthe nocebo response of healthy volunteers. Br J clin Pharmacol 1995; 39: 204 206.
8. Dantas F. Incidência de efeitos patogenéticos não-farmacológicos e triviais numa amostra deestudantes de medicina. Revista de Homeopatia 2004; 69:5-10.
9. Walach H. Research in Homoeopathy in Germany during the Thirties: Inquiry by theReichsgesundheitsamt 1936-1939 , the remedy proving by Martini. Berlin J Research Hom1991; 1:325-338.
10. Fisher P, Dantas F. Homeopathic pathogenetic trials of Acidum malicum and Acidum ascorbicum.Br Hom J 2001; 90(3): 118-125.
11. McCarney R, Fisher P, Spink F, Flint G, van Haselen R. Can homeopaths detect homeopathicmedicines by dowsing? A randomized, double-blind, placebo-controlled trial. J R Soc Med.2002;95(4):189-91.
12. Signorini A, Lubrano A, Manuele G, Fagone G, Vittorini C, Boso F, Vianello P, Rebuffi A, FrongiaT, Rocco V, Pichler C. Classical and new proving methodology: provings of Plumbum metallicumand Piper methysticum and comparison with a classical proving of Plumbum metallicum.Homeopathy. 2005;94(3):164-74.
14
CLINICAL RESEARCH
Evaluation of Homoeopathic Therapy inOsteoarthritis- A Study conducted by CCRH
Abstract
The prevalence of Osteoarthritis (OA) increases with advancing age, that is 50 years orabove. The change in the chemical characteristics of the ground substance of the joint, heredity,overuse of joints, obesity, hyper mobility, orthopaedic deformities, endocrine diseases are importantin the causation of this disease. This study was undertaken to see the effect of homoeopathicmedicines and their reliable indications, their most useful potencies, frequency of administrationand the same was conducted at Clinical Research Unit, Patiala and Central Research Institute,Kottayam. At Clinical Research Unit, Patiala, 93 cases were studied under Drug RelatedProgramme and 360 cases were studied under Disease Related Programme. At Central ResearchInstitute, Kottayam, 273 cases were studed under Disease Related Programme were studied.The patients of inflammatory, metabolic, suppurative and systemic arthritis were excluded fromthis study. 78 patients were found markedly improved joint pains, with agg. during motion and onbeginning to move.
Introduction
Osteoarthritis (OA, osteoarthrosis) is by farthe most common form of arthritis. It shows a strongassociation with ageing and is a major cause ofpain and disability in the elderly. Pathologically, itmay be defined as a condition of synovial jointscharacterized by:
• Focal loss of articular hyaline cartilage• Simultaneous proliferation of new bone
with remodeling of joint contour
Inflammation is not a prominent feature. OA,however, is not a disease or a single condition. Itis best viewed as the dynamic repair process ofsynovial joints that may be triggered by a variety ofinsults, some but not all of which result insymptomatic ‘joint failure’. Radiographic andautopsy studies show that OA preferentially targetsonly certain small and large joints. There is a steadyrise in overall prevalence from age 30 such that by65, 80% of people have some radiographicevidence of OA, though only 25-30% haveassociated symptoms. The knee and hip are theprincipal large joints affected and the principal sitesof significant disability. Knee OA is more prevalentthan hip OA, but taken together they affect 10-25%of those aged over 65 years. Homoeopathicmedicines have been reported to be effective inOA. CCRH started the work with an objective tosee the effect of Homoeopathic therapy in OA andto determine the reliable indications, potencies orfrequency of administration of the medicines founduseful in relieving OA.
Materials and Method
A total of 726 cases were enrolled in thestudy. Out of these, 93 cases were studied underDrug related programme of Clinical Research inPatiala (2001-2003) and under the Disease relatedproject – 360 cases at Clinical Research Unit,Patiala (1993 to 2003) and 273 cases at CentralResearch Institute, Kottayam (2000 to 2003). Theetiological factors are :
Miasmatic profile of : Psora (33 cases),273 cases Sycosis (68 cases),
Mixed miasm(123 cases),Pseudo psora (49 cases).
Precipitating factors : Over use of joints (263in 545 cases cases),
Cold climate(155 cases),Dampness (127 cases).
Parameters Assessment of intensity of the dis-ease
Mild : Asymptomatic cases but onlyradiological abnormalities
Moderate : Cases with severe pain,stiffness, with or withoutswelling with or without cracking in joints, with orwithout lock knee, with orwithout Heberden's nodes, withor without deformities but nopain at night.
Severe : Cases with night pains
15
Selection of research cases:
General :
• All cases of joint disease which seem to bedegenerative nature and excluding knowncases of inflammatory, metabolic, Suppurativeand systemic arthritis, .
• In relation to age, sex, occupation and physicalconstitution, the patient are registered initiallybefore the inclusion.
Symptoms related to particular system:
• Joint pain• Localized or generalized with or without
swelling• < During rest• < After bodily exertion• < On beginning to move• Relieved by continuous motion
• Morning stiffness• Crepitus/cracking in joints• Locked knee• Limitation of movement• Heberden's nodes• Deformities like genu varus, halux valgus etc.
Assessment of improvement of cases
Cure : Complete disappearance of thesubjective & objective with norecurrence for the next fiveyears.
Mild : Reduction in pain and othersymptoms with recurrenceafter least exertion.
Marked : Complete disappearance ofsubjective and objectivesymptoms (excluding radiologi-cal findings) with no recur-rence during the period underreport.
Moderate : Disappearance of thesymptoms like morningstiffness, cracking, lock knee,limitations of motion etc.but only the mitigation of pains.
Not improved : No improvement even afterconsiderable period oftreatment with similar remedy.
Worse : Aggravation of signs andsymptoms even after thetreatment with well selectedremedies.
Result
Improvement indices
Total Male FemaleImproved
- Mild 12 02 10- Moderate 105 20 85- Marked 78 10 68
Not improved 02 00 02Not reported 37 02 35Dropped out 19 02 17Under observation 20 03 17
Subjective symptoms
Before Aftertreatment treatment
Pain Joints 273 32Pain joints < motion 404 282Pain < beginning to move 207 117Pain < night 114 21Pain < day time 47 24Pain < after movements 91 20Pain < rest 447 282Morning stiffness 669 353Cracking in joints 190 20Lock knee 146 10Bilateral paraesthesia 55 07Symptoms of cord 108 36compression
Objective symptoms
Before Aftertreatment treatment
Swelling of joints 211 31Limitation of motion 228 77Deformities 05 05Heberden's nodes 02 02Flexion contractures 01 00Weakness of lower limbs 83 13
Pathological / radiological findings
Before Aftertreatment treatment
Osteophytes deposition 138 112Reduction of joint space 131 131Sclerosis of subchondral 04 04bonesSubchondral cyst 02 02

16
Drugs found effective
(Before treatment/After treatment)
Ars. Alb. 30,200,1M 05 04Calc. carb. 30,200,1M 29 25Lyco. 30,200,1M 76 67Medorh.30,200,1M 10 8Nat. mur. 30,200,1M,10M 12 9Puls. 30,200,1M,10M 17 12Rhus tox. 30,200,1M,10M 63 55Sulphur 30,200,1M,10M 13 7
Reliable indications of the drugs found useful
Arsenicum albumNocturnal burning pain relieved by warm
application, warm bath. Pain agg. damp coldseason with tingling and numbness of the limbs,pain agg. by cold air, fanning and uncovering.
Bryonia Mild swelling in the knee joints. Stiffness in
the knee joints. Pain in knee joints< by motion > byrest. < night, change of climate from cold to warm,amelioration by absolute rest. Backache agg. whileturning in the bed. Joints pain amel. by lying onback, pressure or wrapping up. Pain in joints,swelling, sitting, pain, agg. night, motion, changeof climate from cold to warm, amel. by absoluterest. Backache agg. while turning in the bed, painjoints amel. by lying on back, pressure or wrappingup, adapted to robust fibre and dark constitution.
Calcarea carb.Found effective in fat, flabby, and flatulent
constitution, liable to affections of weight bearingjoints. Pain knee joints agg, squatting, rising fromsquatting., cold climate, standing in cold basement.Amel. by warm application, cracking in joints onmotion, chilly patient, desires warm food, colddrinks, egg, fish, aversion to milk,. Sharp stickingpains in the knee joints. Pain worse in change ofweather and physical exertion. Pain in knee jointbetter in warm dry climate, worse in cold weather.Tendency to obesity. Burning in soles of feet.
Calcarea phos.Chilly patient, knee joint affected from left to
right, desires salt, meat and fish, cold food anddrinks, , cracking in joints on motion, and on risingfrom seat, stiffness and pain in joints, with coldnessand numbness of limbs. Pain is worse duringascending.
CausticumPain and stiffness in the knee joints. Pain
better by hard pressure and heat. Paralytic feelingin lower limbs. Numbness of limbs at night with
restlessness, amelioration by warm application.pains are worse in fine weather but relieved in rainyseason. Joint pains with tearing and drawing,deformities at the joint, joint affection with weaknessof limbs and tendency to fall, numbness of limbs atnight, pains are aggravated at night withrestlessness and amel. by warm application.cracking of joints especially knee.
GraphitesPain especially in women of climacteric age.
Pain is more at night. < cold air, cold bath, winter.> warm application, chilly patient, desiring warmth.Aversion to sweets and fish. Scanty menses ofshort duration. Habitual constipation.
LycopodiumDrawing and tearing pain in knee joints. Pain
of knee joints worse at night and rest. Pain of kneejoint better with warm application. Swelling on thert, knee joint with numbness. Carbonitrogenoidconstitution, desires warm food and drinks, sweets,desires cold climate, excessive flatulence esp.evening hours and after flatulent food. Eating a littlecauses fullness in abdomen, pain and stiffness ofjoints < at night, first motion, winter, amel. continuedmotion, cold applications, Rt. sided affections,rheumatism of right shoulder < raising the limb.
MedorrhinumWarm patient, burning sensation all over,
desires cold food and drinks. General relief in rainyseason, gen. aggravation in warm and winterseason, pain agg. first motion, winter, summer,daytime, amel. contd. motion, rainy season.
Natrum mur.Constitutional remedy with caving for salt and
salty thing, warm patient, always desires cold, painsin spinal joints which are more during sitting,standing and lying on sides. Pain is better by lyingon back on something hard. Pain in knee jointswith cracking sensation.
Rhus tox.Chilly patient, desires warmth in general, warm
food and drinks, desires milk, rheumatism of left,shoulder joint, left sided affections mainly, painstiffness and swelling of joints, large and small;aggravation at night, morning, beginning to move,first motion, after physical exertion, rest, winterseason, damp season, constantly standing ondamp floor, bathing, cloudy weather, over exertionof joints, after excessive sweating, turning in thebed, amelioration continued motion, day time,warmth, warm bath, warm application, warmseason, rubbing, tight bandage, covering of thepart, restless at night, constantly changes positionin bed, pain in back especially, lumbar region isamel. by lying on back.

17
SulphurRheumatism of left shoulder joint, burning type
of pain, < night, raising the affected limb, drawingand tearing pains at night, pain agg. due to the heatof the bed, pain lumbar region, agg. standing andrising from stooping, has to stoop a while afterrising, warm patient. Desires cold food and drinks,open air, and warm bath, winter season, amel. drywarm weather, burning Sensation of palms andsoles, at night, amel. by cold application, desiressweets, aversian to milk.
PulsatillaWarm patient, desires open air, cold food, cold
drinks, cold climate, gen amel. in cold, sensitiveto pain which rapidly shift from one joint to another,easily weeping, consolation amel., pain agg. atnight, amel. open air, agg. rest, first motion, amel.continued motion, pain agg. from letting the affectedlimb down, pain of drawing or tearing type, withchilliness especially at night, patient is usuallythirstless, with late or protracted menstruation.
Discussion
Osteo arthritis, the most common joint diseaseof the aged is symptomatic three times more oftenin women than men, and is resulting fromdegeneration of the articular cartilage and fibrocartilage in inter vertebral discs. The prevalenceof this disease sharply increases with advancingage, with mean age of onset is 50 years but theother factors notably, heredity, over use of joints,change in the chemical characteristics of the groundsubstance of the joint, pre existing joint disease,
obesity, hper mobility, orthopaedic deformities,endocrine disease like Diabetes mellitus,hypothyroidism, hyperparathyroidism etc. areimportant in the causation of this disease. It isusually primary but may develop secondary to anyjoint disease or joint injuries.
In our study it was observed that no agewas an exempted from this disease because theage of the patients ranged from 15 years to 88years (refer table 2.3.1. and 2.3.2.). However, it isfurther observed that in more than 225 casesincluded in the study, age ranged from 40 to 60years of age. This means that this is a disease ofadvancing age. Among the 273 cases studied, 255belong to primary OA in which heredity, obesity,overuse of joints, hypermobility, etc. were foundresponsible for the onset and/or continuation of thedisease process.
Conclusion
Response to treatment on the basis ofrecurrence of symptoms and signs during and aftertreatment and symptomatic improvement were alsostudied. It has been observed that in 88 cases norecurrence of signs & symptoms was noticed andmajority of the cases in which symptoms recurredonly in less intensity and in short duration. The X-ray examination shows that in a few cases eventhe marginal osteophytes deposition decreased.No increase in osteophytes deposition found duringthe treatment but in other cases no change noticedwas even after repeated x-ray examinations.
18
CLINICAL VERIFICATION
Lac Caninum(Clinically verified Symptoms)
Introduction : The secretion of the mammary glands of a lactatingfemale dog collected at least 15 days after parturition5.The symptoms which are given in literature(1,2,3,4,5), wereclinically verified by CCRH.
Name in Contemporary use : Dog's Milk5 (Bitch's Milk)3
Synonyms : French Lait de chienne5
Preparation of : Solution1/100 in distilled water (Class-B), freshlyHomoeopathic Medicine made5.and Class.
Source of drug : Hahnemann Publishing Company Pvt. Ltd., Kolkata
Period of study : April 1984- March 2003
Potencies used : 6, 30, 200, 1M
Number of cases studied : 4347
Clinical Verification conducted at:-
1. Regional Research Institute (H), New Delhi2. Homoeopathic Research Institute, Lucknow (U.P.)3. Homoeopathic Research Institute. Jaipur (Rajasthan)4. Clinical Verification Unit, Ghaziabad (U.P.)5. Clinical Verification Unit, Patna (Bihar)6. Clinical Verification Unit, Vrindavan (U.P.)7. Clinical Research Unit, Jammu (J&K)
Clinically verified Symptoms observed during the study:
Location Symptom No. of patients No. of patientsprescribed relieved
Mind Anxiety N 2 2Anxiety with palpitation in crowded 1 1placeN
Forgetfulness; in writing, makes 31 23mistakesN
Nervousness3 9 7
Note: i) The symptoms super scribed with a particular number(1,2,3,4) are found in theliterature, as well as clinically verified by CCRH.
ii) Symptoms superscribed with (N) are those reported and relieved by patients but not mentionedin the literature.
iii) The figure 1,2,3 & 4 stand for the source literature referred.
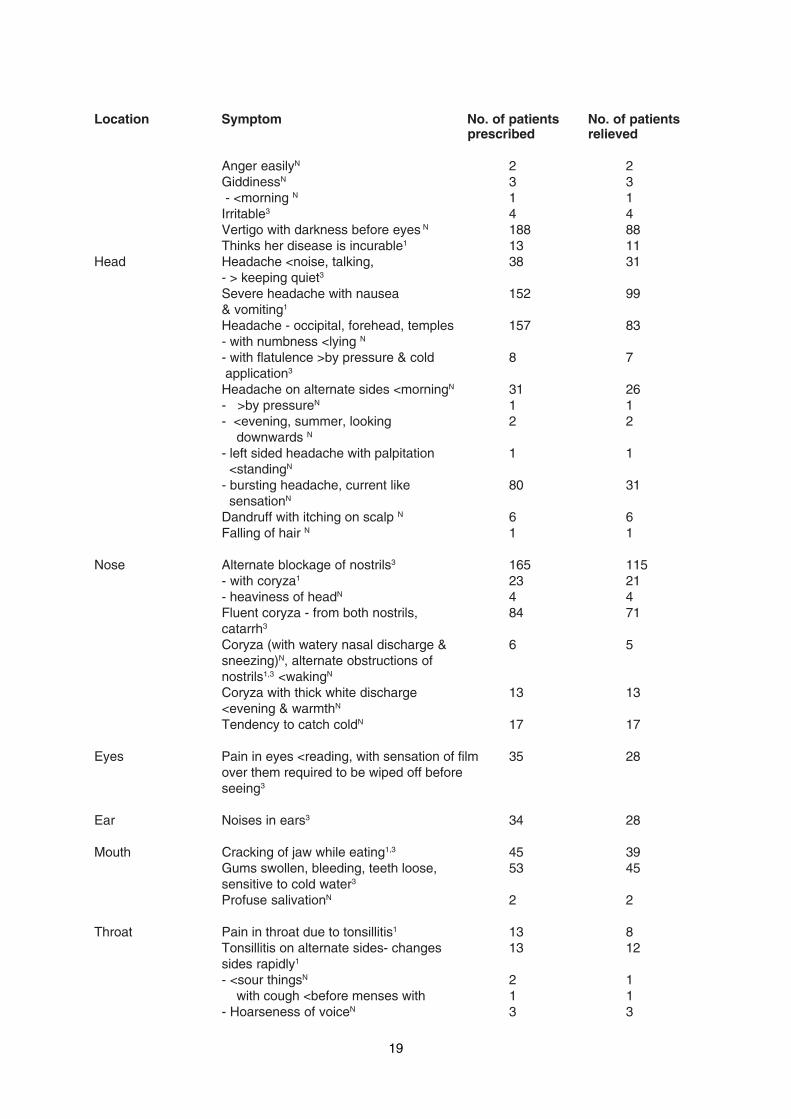
19
Location Symptom No. of patients No. of patientsprescribed relieved
Anger easilyN 2 2GiddinessN 3 3 - <morning N 1 1Irritable3 4 4Vertigo with darkness before eyes N 188 88Thinks her disease is incurable1 13 11
Head Headache <noise, talking, 38 31- > keeping quiet3
Severe headache with nausea 152 99& vomiting1
Headache - occipital, forehead, temples 157 83- with numbness <lying N
- with flatulence >by pressure & cold 8 7 application3
Headache on alternate sides <morningN 31 26- >by pressureN 1 1- <evening, summer, looking 2 2 downwards N
- left sided headache with palpitation 1 1 <standingN
- bursting headache, current like 80 31 sensationN
Dandruff with itching on scalp N 6 6Falling of hair N 1 1
Nose Alternate blockage of nostrils3 165 115- with coryza1 23 21- heaviness of headN 4 4Fluent coryza - from both nostrils, 84 71catarrh3
Coryza (with watery nasal discharge & 6 5sneezing)N, alternate obstructions ofnostrils1,3 <wakingN
Coryza with thick white discharge 13 13<evening & warmthN
Tendency to catch coldN 17 17
Eyes Pain in eyes <reading, with sensation of film 35 28over them required to be wiped off beforeseeing3
Ear Noises in ears3 34 28
Mouth Cracking of jaw while eating1,3 45 39Gums swollen, bleeding, teeth loose, 53 45sensitive to cold water3
Profuse salivationN 2 2
Throat Pain in throat due to tonsillitis1 13 8Tonsillitis on alternate sides- changes 13 12sides rapidly1
- <sour thingsN 2 1 with cough <before menses with 1 1- Hoarseness of voiceN 3 3
20
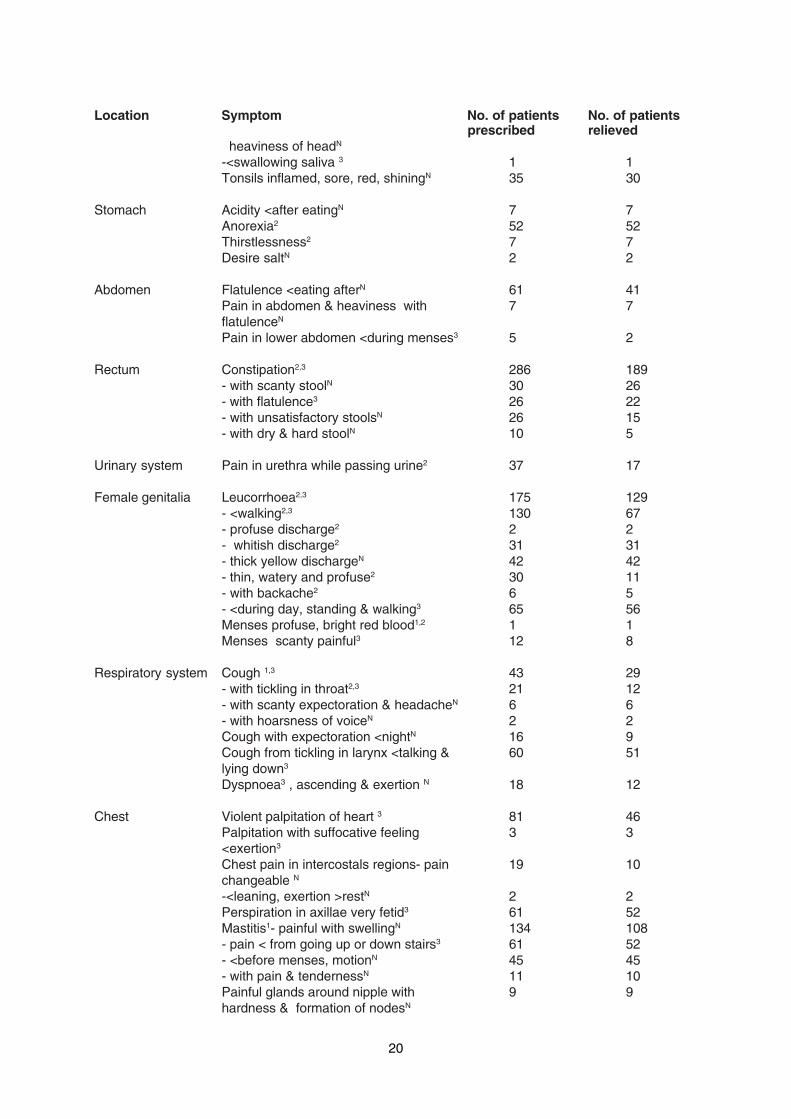
Location Symptom No. of patients No. of patientsprescribed relieved
heaviness of headN
-<swallowing saliva 3 1 1Tonsils inflamed, sore, red, shiningN 35 30
Stomach Acidity <after eatingN 7 7Anorexia2 52 52Thirstlessness2 7 7Desire saltN 2 2
Abdomen Flatulence <eating afterN 61 41Pain in abdomen & heaviness with 7 7flatulenceN
Pain in lower abdomen <during menses3 5 2
Rectum Constipation2,3 286 189- with scanty stoolN 30 26- with flatulence3 26 22- with unsatisfactory stoolsN 26 15- with dry & hard stoolN 10 5
Urinary system Pain in urethra while passing urine2 37 17
Female genitalia Leucorrhoea2,3 175 129- <walking2,3 130 67- profuse discharge2 2 2- whitish discharge2 31 31- thick yellow dischargeN 42 42- thin, watery and profuse2 30 11- with backache2 6 5- <during day, standing & walking3 65 56Menses profuse, bright red blood1,2 1 1Menses scanty painful3 12 8
Respiratory system Cough 1,3 43 29- with tickling in throat2,3 21 12- with scanty expectoration & headacheN 6 6- with hoarsness of voiceN 2 2Cough with expectoration <nightN 16 9Cough from tickling in larynx <talking & 60 51lying down3
Dyspnoea3 , ascending & exertion N 18 12
Chest Violent palpitation of heart 3 81 46Palpitation with suffocative feeling 3 3<exertion3
Chest pain in intercostals regions- pain 19 10changeable N
-<leaning, exertion >restN 2 2Perspiration in axillae very fetid3 61 52Mastitis1- painful with swellingN 134 108- pain < from going up or down stairs3 61 52- <before menses, motionN 45 45- with pain & tendernessN 11 10Painful glands around nipple with 9 9hardness & formation of nodesN
21
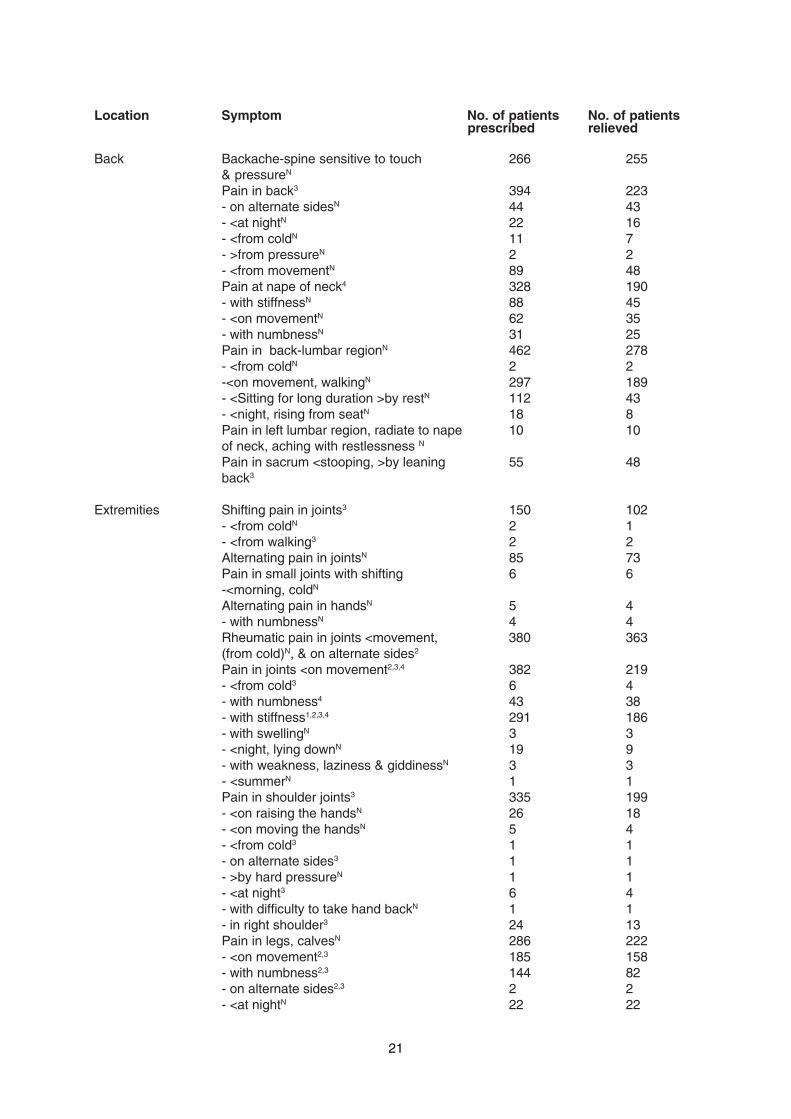
Location Symptom No. of patients No. of patientsprescribed relieved
Back Backache-spine sensitive to touch 266 255& pressureN
Pain in back3 394 223- on alternate sidesN 44 43- <at nightN 22 16- <from coldN 11 7- >from pressureN 2 2- <from movementN 89 48Pain at nape of neck4 328 190- with stiffnessN 88 45- <on movementN 62 35- with numbnessN 31 25Pain in back-lumbar regionN 462 278- <from coldN 2 2-<on movement, walkingN 297 189- <Sitting for long duration >by restN 112 43- <night, rising from seatN 18 8Pain in left lumbar region, radiate to nape 10 10of neck, aching with restlessness N
Pain in sacrum <stooping, >by leaning 55 48back3
Extremities Shifting pain in joints3 150 102- <from coldN 2 1- <from walking3 2 2Alternating pain in jointsN 85 73Pain in small joints with shifting 6 6-<morning, coldN
Alternating pain in handsN 5 4- with numbnessN 4 4Rheumatic pain in joints <movement, 380 363(from cold)N, & on alternate sides2
Pain in joints <on movement2,3,4 382 219- <from cold3 6 4- with numbness4 43 38- with stiffness1,2,3,4 291 186- with swellingN 3 3- <night, lying downN 19 9- with weakness, laziness & giddinessN 3 3- <summerN 1 1Pain in shoulder joints3 335 199- <on raising the handsN 26 18- <on moving the handsN 5 4- <from cold3 1 1- on alternate sides3 1 1- >by hard pressureN 1 1- <at night3 6 4- with difficulty to take hand backN 1 1- in right shoulder3 24 13Pain in legs, calvesN 286 222- <on movement2,3 185 158- with numbness2,3 144 82- on alternate sides2,3 2 2- <at nightN 22 22
22
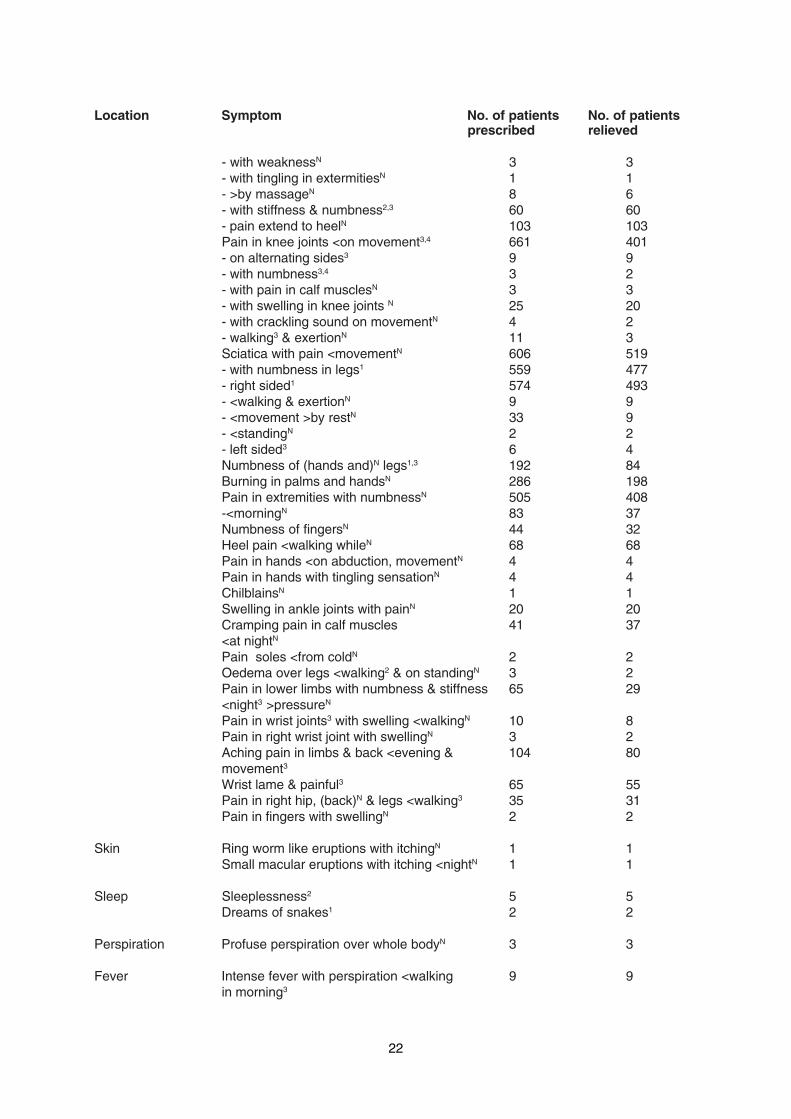
Location Symptom No. of patients No. of patientsprescribed relieved
- with weaknessN 3 3- with tingling in extermitiesN 1 1- >by massageN 8 6- with stiffness & numbness2,3 60 60- pain extend to heelN 103 103Pain in knee joints <on movement3,4 661 401- on alternating sides3 9 9- with numbness3,4 3 2- with pain in calf musclesN 3 3- with swelling in knee joints N 25 20- with crackling sound on movementN 4 2- walking3 & exertionN 11 3Sciatica with pain <movementN 606 519- with numbness in legs1 559 477- right sided1 574 493- <walking & exertionN 9 9- <movement >by restN 33 9- <standingN 2 2- left sided3 6 4Numbness of (hands and)N legs1,3 192 84Burning in palms and handsN 286 198Pain in extremities with numbnessN 505 408-<morningN 83 37Numbness of fingersN 44 32Heel pain <walking whileN 68 68Pain in hands <on abduction, movementN 4 4Pain in hands with tingling sensationN 4 4ChilblainsN 1 1Swelling in ankle joints with painN 20 20Cramping pain in calf muscles 41 37<at nightN
Pain soles <from coldN 2 2Oedema over legs <walking2 & on standingN 3 2Pain in lower limbs with numbness & stiffness 65 29<night3 >pressureN
Pain in wrist joints3 with swelling <walkingN 10 8Pain in right wrist joint with swellingN 3 2Aching pain in limbs & back <evening & 104 80movement3
Wrist lame & painful3 65 55Pain in right hip, (back)N & legs <walking3 35 31Pain in fingers with swellingN 2 2
Skin Ring worm like eruptions with itchingN 1 1Small macular eruptions with itching <nightN 1 1
Sleep Sleeplessness2 5 5Dreams of snakes1 2 2
Perspiration Profuse perspiration over whole bodyN 3 3
Fever Intense fever with perspiration <walking 9 9in morning3
23
Location Symptom No. of patients No. of patientsprescribed relieved
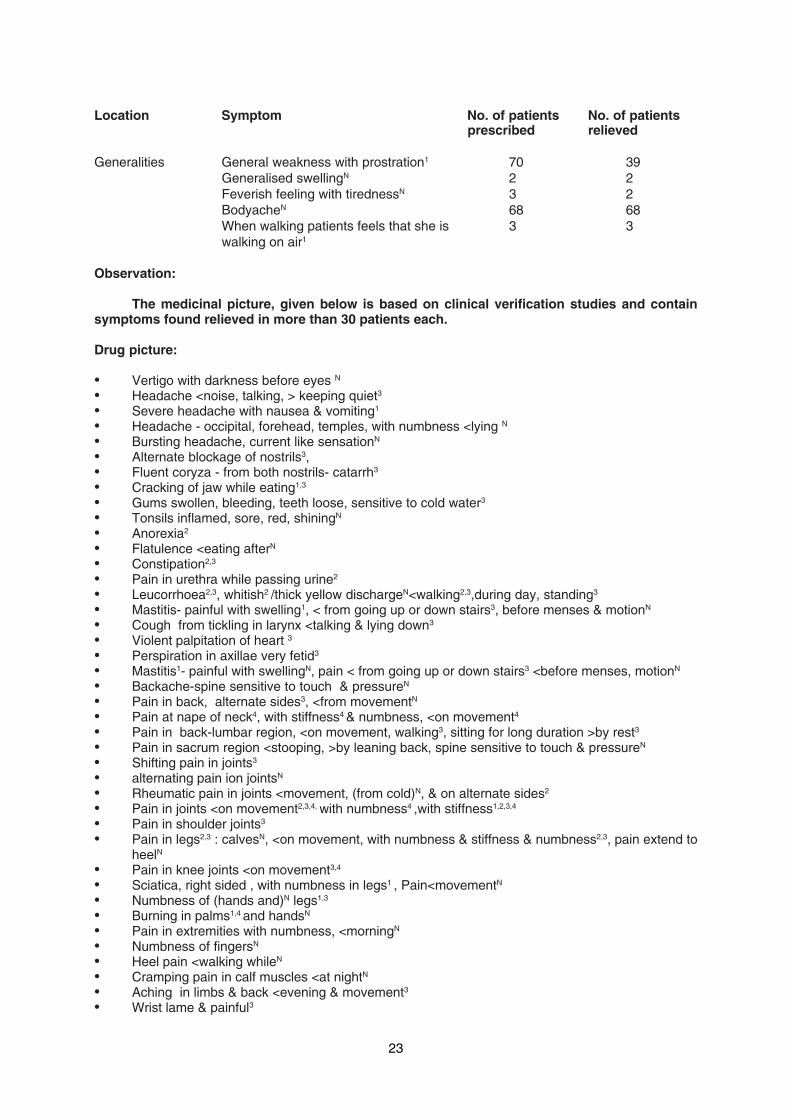
Generalities General weakness with prostration1 70 39Generalised swellingN 2 2Feverish feeling with tirednessN 3 2BodyacheN 68 68When walking patients feels that she is 3 3walking on air1
Observation:
The medicinal picture, given below is based on clinical verification studies and containsymptoms found relieved in more than 30 patients each.
Drug picture:
• Vertigo with darkness before eyes N
• Headache <noise, talking, > keeping quiet3
• Severe headache with nausea & vomiting1
• Headache - occipital, forehead, temples, with numbness <lying N
• Bursting headache, current like sensationN
• Alternate blockage of nostrils3,• Fluent coryza - from both nostrils- catarrh3
• Cracking of jaw while eating1,3
• Gums swollen, bleeding, teeth loose, sensitive to cold water3
• Tonsils inflamed, sore, red, shiningN
• Anorexia2
• Flatulence <eating afterN
• Constipation2,3
• Pain in urethra while passing urine2
• Leucorrhoea2,3, whitish2 /thick yellow dischargeN<walking2,3,during day, standing3
• Mastitis- painful with swelling1, < from going up or down stairs3, before menses & motionN
• Cough from tickling in larynx <talking & lying down3
• Violent palpitation of heart 3
• Perspiration in axillae very fetid3
• Mastitis1- painful with swellingN, pain < from going up or down stairs3 <before menses, motionN
• Backache-spine sensitive to touch & pressureN
• Pain in back, alternate sides3, <from movementN
• Pain at nape of neck4, with stiffness4 & numbness, <on movement4
• Pain in back-lumbar region, <on movement, walking3, sitting for long duration >by rest3
• Pain in sacrum region <stooping, >by leaning back, spine sensitive to touch & pressureN
• Shifting pain in joints3
• alternating pain ion jointsN
• Rheumatic pain in joints <movement, (from cold)N, & on alternate sides2
• Pain in joints <on movement2,3,4, with numbness4 ,with stiffness1,2,3,4
• Pain in shoulder joints3
• Pain in legs2,3 : calvesN, <on movement, with numbness & stiffness & numbness2,3, pain extend toheelN
• Pain in knee joints <on movement3,4
• Sciatica, right sided , with numbness in legs1 , Pain<movementN
• Numbness of (hands and)N legs1,3
• Burning in palms1,4 and handsN
• Pain in extremities with numbness, <morningN
• Numbness of fingersN
• Heel pain <walking whileN
• Cramping pain in calf muscles <at nightN
• Aching in limbs & back <evening & movement3
• Wrist lame & painful3
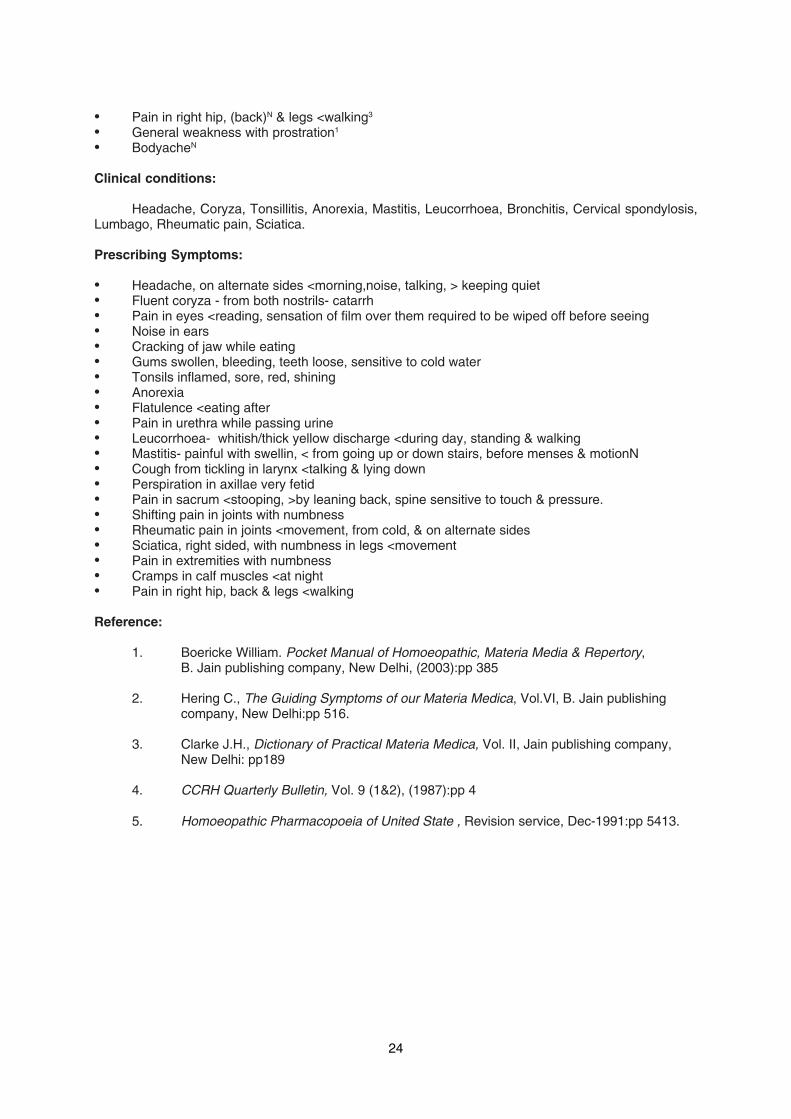
24
• Pain in right hip, (back)N & legs <walking3
• General weakness with prostration1
• BodyacheN
Clinical conditions:
Headache, Coryza, Tonsillitis, Anorexia, Mastitis, Leucorrhoea, Bronchitis, Cervical spondylosis,Lumbago, Rheumatic pain, Sciatica.
Prescribing Symptoms:
• Headache, on alternate sides <morning,noise, talking, > keeping quiet• Fluent coryza - from both nostrils- catarrh• Pain in eyes <reading, sensation of film over them required to be wiped off before seeing• Noise in ears• Cracking of jaw while eating• Gums swollen, bleeding, teeth loose, sensitive to cold water• Tonsils inflamed, sore, red, shining• Anorexia• Flatulence <eating after• Pain in urethra while passing urine• Leucorrhoea- whitish/thick yellow discharge <during day, standing & walking• Mastitis- painful with swellin, < from going up or down stairs, before menses & motionN• Cough from tickling in larynx <talking & lying down• Perspiration in axillae very fetid• Pain in sacrum <stooping, >by leaning back, spine sensitive to touch & pressure.• Shifting pain in joints with numbness• Rheumatic pain in joints <movement, from cold, & on alternate sides• Sciatica, right sided, with numbness in legs <movement• Pain in extremities with numbness• Cramps in calf muscles <at night• Pain in right hip, back & legs <walking
Reference:
1. Boericke William. Pocket Manual of Homoeopathic, Materia Media & Repertory,B. Jain publishing company, New Delhi, (2003):pp 385
2. Hering C., The Guiding Symptoms of our Materia Medica, Vol.VI, B. Jain publishingcompany, New Delhi:pp 516.
3. Clarke J.H., Dictionary of Practical Materia Medica, Vol. II, Jain publishing company,New Delhi: pp189
4. CCRH Quarterly Bulletin, Vol. 9 (1&2), (1987):pp 4
5. Homoeopathic Pharmacopoeia of United State , Revision service, Dec-1991:pp 5413.

25
DRUG RESEARCH
Pharmacognostic & Physico-Chemical Evaluation Of Psidium Guajava L.P. Subramanian*, P. Padma Rao** and M. Prabhakar***
* Research Officer (Chemistry), ** Assistant Research Officer( Pharmacognosy), *** Ex-Project Officer, DrugStandardization Unit (H), O.U.B. 32, Road No. 4, Habsiguda, Hyderabad-500 007.
Abstract
Psidium guajava L. belonging to the family Myrtaceae is known as Guava. It is acommon fruit tree, cultivated and naturalized throughout India. The leaves are used as anapplication in wounds, ulcers and as an astringent to bowels in Unani. Besides, it is also usedas digestive, febrifuge and antispasmodic, in cerebral affections, nephritis, rheumatism,epilepsy and chorea. Leaves contain catechol and pyrogallol tannins besides oil and vitamins.
Due to growing urge for introduction of well known indigenous drugs intoHomoeopathy, the leaves of P. guajava are also being adopted. In the present,pharmacognostic studies of leaf comprising macro- and microscopic characters, organolepticand powder microscopic features, besides physico-chemical constants viz. moisture content,ash and extractive values for raw drugs and parameters such as weight per ml., total solids,alcohol content and chromatographic profiles of TLC, HPTLC, along with UV absorbance formother tincture are detailed.
Introduction
Psidium guajava L. belonging to the familyMyrtaceae is commonly known as guava in Eng-lish, amrud in Hindi, koyya in Tamil and tella jamain Telugu. Guava is also referred to as the apple ofthe tropics. It is a native of tropical America andcultivated and naturalized throughout India1. It isan arborescent shrub or a small tree, upto 8 m high.The guava leaves are used as an application inwounds, ulcers, and as an astringent for bowels(Unani). The young leaves are used as a tonic inthe diseases of the digestive functions. Thedecoction of leaves has been used in Cholera andalso as a febrifuge and antispasmodic. Infusion ofleaves is used in Cerebral affections, Nephritis andCachexia. The pounded leaves are locally appliedin Rheumatism and their extract in Epilepsy andChorea. Though traditionally the medicinal use ofleaves of P. guajava finds mention only in Unanisystem, their folklore utilities have been elaborate5.Leaves are reported to contain catechol and pyro-gallol tannins. A new flavonol glycoside quercetin4' glucuronide was reported4. Oil of leaves is aro-matic and also used as a flavouring agent. Besides,they also contain carotene, vitamins B1, B2 and B6and vitamin C. Antibacterial activity is reported byRabe and Van Staden8.
Presently, there is a growing urge to intro-duce indigenous drugs into Homoeopathic system.
In view of this leaves of P. guajava is one of thedrug also being tried. Review of literature revealsthat there is no reported work on pharmacognosticand physico-chemical aspects of the leaves of P.guajava. Hence a detailed study on these aspectsis presented.
Material and Methods
Leaves of Psidium guajava L. was collectedfrom Botanic garden, Department of Botany,Osmania University, Hyderabad. Fresh leaves werefixed in Carnoy's fixative. Subsequently epidermalpeels of leaf and petiole were prepared followingthe method of Leelavathi and Ramayya6. Micro-tome sections of 10-15 µm thick of leaf and petiolewere prepared following the traditional techniques3.Sections were stained with crystal violet and basicfuchsin. Powder studies were made followingYoungken9 and Johansen3.
The air dried leaves were powdered to ob-tain coarse powder 10/44 (sieve size). It was sub-jected to determination of moisture content (L.O.D.),Ash values and extractive values. The above pa-rameters were determined in accordance with theprocedures given in Homoeopathic Pharmacopoeiaof India2. The mother tincture was prepared by per-colation technique2. Alcohol content for the prepa-ration of mother tincture was fixed as per maximumextractive value (M.E.V.).

26
The alcoholic extract (mother tincture) wassubjected for a) Physico-chemical constants, b)Chromatography (TLC/HPTLC), c) U.V. absorb-ance.
All chemicals and solvents used were of ana-lytical grade. Silica gel G (E Merck) was used forthin layer chromatography (T.L.C.). U.V. spectrawas recorded using spectrophotometer, Shimadzumake (courtesy CFTRI, Hyderabad)
Physico-chemical Constants
Physico-Chemical parameters viz., orga-noleptic characters, weight per ml. total solids, al-cohol content and pH value, were determined asper the guidelines laid down in the HomoeopathicPharmacopoeia of India2.
Chromatography (T.L.C.)
For TLC 25 ml. alcoholic extract was evapo-rated on water bath to remove alcohol. The remain-ing aqueous part was extracted with 25 ml. chloro-form (three times). All the three fractions were com-bined and concentrated to 2ml. 15 µm was appliedon activated silica gel G coated TLC plate. It wasdeveloped using chloroform and benzene with fewdrops of acetic acid (1:1v/v) on mobile phase and10% FeCl3 solution was sprayed for visualization.
UV Absorbance
For UV absorbance, the mother tincture wasdiluted with 99 parts 70% alcohol, scanned in therange of 200-300 nm. The peaks of maximum ab-sorption are given in Table 6.
HPTLC Studies
Precoated high performance TLC plates(silica gel 60 F 254 as stationary phase) were used.For sample application, CAMAG Linomat IV sam-ple applicator was employed. The speed of appli-cation was maintained at 4mm/sec. The solventsystem used for development was chloroform, ace-tic acid, methanol and water (6.2 : 2.1 : 2.0 : 0.8 v/v). Methanolic sulphuric acid and anisaldehydeH
2SO
4 were used for derivatisation. The Rf values
of the various components before and afterderivatisation are provided in Table 5.
OBSERVATIONS
Pharmacognostic Studies
Macroscopy : Leaves 10-15 cm long, oblong or el-
liptic oblong, entire glabrous above, pubescent be-neath, pellucid punctuate; lateral nerves 10-20 pairs,prominent beneath, strongly curved near the edgeand joined by intro marginal veins, petioles 2.5-7.5mm long.
Microscopy: Adaxally epidermal cells polygonalisodiametric or anisodiametric with sides slightlythick, straight to curved; surface striated; contentsscanty or dense in few. Epidermal cells 5,45,000per sq. cm. Stomata are absent on adaxial side.Trichomes 1) Unicellular conical hair, longer, dis-tributed all over surface. 2) Unicellular flagellateconical hair, long, flagellate conical, all over, moreon vens.
Abaxially cells similar as on adaxial, sidesthin with curved or wavy anticlinal walls; contentsscanty but with tannins in few; interspersed by se-cretory cavities. Epidermal cells 10,20,000 per sq.cm. Stomata mostly paracytic, few anisocytic andanomocytic; paracytic subsidiaries longer, distinct.Stomatal pore large, contents dense; Stomatal fre-quency: 2,90,000 per sq. cm. Stomatal Index:22.13; Stomatal size; 19-24 um (21) long and 12-16 um (15) wide. Trichomes are similar to thosedescribed on adaxial side.
Transection (TS):
In T.S. midvein is grooved on adaxial sideand prominently ribbed towards abaxial. Second-ary and tertiary veins ribbed abaxially. Midvein kid-ney-shaped, laterally upto 1.5 mm and vertically1mm thick; Lamina isobilateral, 151-173 um thick.Covered by conical and flagellate hair. Secretorycavities conspicuously present on abaxial.
Epidermis is 1-layered, adaxially large, bar-rel shaped or tabular to polygonal, covered by athick cuticle and often dispersed with conical hairs.Abaxially cells smaller, interrupted by stomata,which are sunken. Mesophyll is characterizedadaxially with a hypoderm, consisting of 3-4 lay-ered tabular to barrel shaped cells often containingtannins, sphaeraphides and resins and interruptedby secretary cavities. Palisade is abaxial, 4-5 lay-ered, cells cylindrical, 11-27 µm (19) long and 5.5-8 µm (7) wide; filled with chloroplasts, tannins andsphaeraphides and interrupted by secretory cavi-ties.
Ground tissue at midvein of collenchyma,parenchyma and sclerenchyma tissues.Collenchyma: abaxially 1-layered and as a groupof cells on adaxial side, 5-19 µm (13) in diameter;angular or lamellar, contents dense. Parenchyma:
27
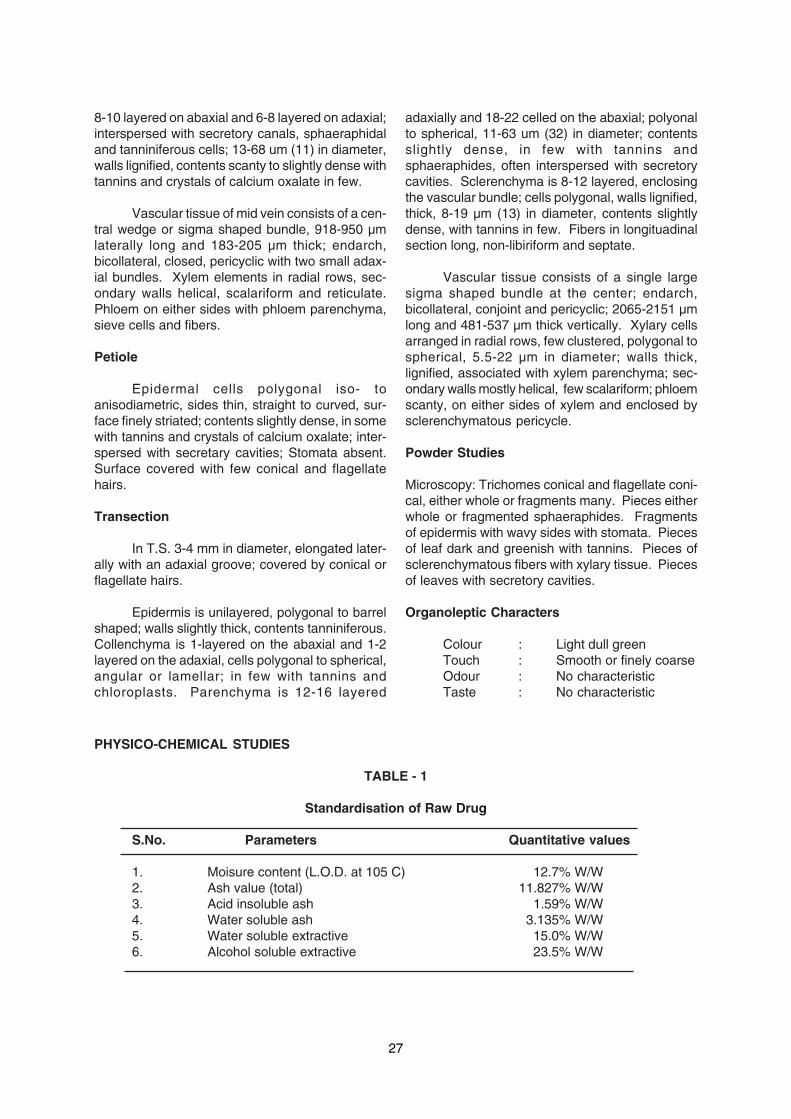
8-10 layered on abaxial and 6-8 layered on adaxial;interspersed with secretory canals, sphaeraphidaland tanniniferous cells; 13-68 um (11) in diameter,walls lignified, contents scanty to slightly dense withtannins and crystals of calcium oxalate in few.
Vascular tissue of mid vein consists of a cen-tral wedge or sigma shaped bundle, 918-950 µmlaterally long and 183-205 µm thick; endarch,bicollateral, closed, pericyclic with two small adax-ial bundles. Xylem elements in radial rows, sec-ondary walls helical, scalariform and reticulate.Phloem on either sides with phloem parenchyma,sieve cells and fibers.
Petiole
Epidermal cells polygonal iso- toanisodiametric, sides thin, straight to curved, sur-face finely striated; contents slightly dense, in somewith tannins and crystals of calcium oxalate; inter-spersed with secretary cavities; Stomata absent.Surface covered with few conical and flagellatehairs.
Transection
In T.S. 3-4 mm in diameter, elongated later-ally with an adaxial groove; covered by conical orflagellate hairs.
Epidermis is unilayered, polygonal to barrelshaped; walls slightly thick, contents tanniniferous.Collenchyma is 1-layered on the abaxial and 1-2layered on the adaxial, cells polygonal to spherical,angular or lamellar; in few with tannins andchloroplasts. Parenchyma is 12-16 layered
adaxially and 18-22 celled on the abaxial; polyonalto spherical, 11-63 um (32) in diameter; contentsslightly dense, in few with tannins andsphaeraphides, often interspersed with secretorycavities. Sclerenchyma is 8-12 layered, enclosingthe vascular bundle; cells polygonal, walls lignified,thick, 8-19 µm (13) in diameter, contents slightlydense, with tannins in few. Fibers in longituadinalsection long, non-libiriform and septate.
Vascular tissue consists of a single largesigma shaped bundle at the center; endarch,bicollateral, conjoint and pericyclic; 2065-2151 µmlong and 481-537 µm thick vertically. Xylary cellsarranged in radial rows, few clustered, polygonal tospherical, 5.5-22 µm in diameter; walls thick,lignified, associated with xylem parenchyma; sec-ondary walls mostly helical, few scalariform; phloemscanty, on either sides of xylem and enclosed bysclerenchymatous pericycle.
Powder Studies
Microscopy: Trichomes conical and flagellate coni-cal, either whole or fragments many. Pieces eitherwhole or fragmented sphaeraphides. Fragmentsof epidermis with wavy sides with stomata. Piecesof leaf dark and greenish with tannins. Pieces ofsclerenchymatous fibers with xylary tissue. Piecesof leaves with secretory cavities.
Organoleptic Characters
Colour : Light dull greenTouch : Smooth or finely coarseOdour : No characteristicTaste : No characteristic
PHYSICO-CHEMICAL STUDIES
TABLE - 1
Standardisation of Raw Drug
S.No. Parameters Quantitative values
1. Moisure content (L.O.D. at 105 C) 12.7% W/W2. Ash value (total) 11.827% W/W3. Acid insoluble ash 1.59% W/W4. Water soluble ash 3.135% W/W5. Water soluble extractive 15.0% W/W6. Alcohol soluble extractive 23.5% W/W
28
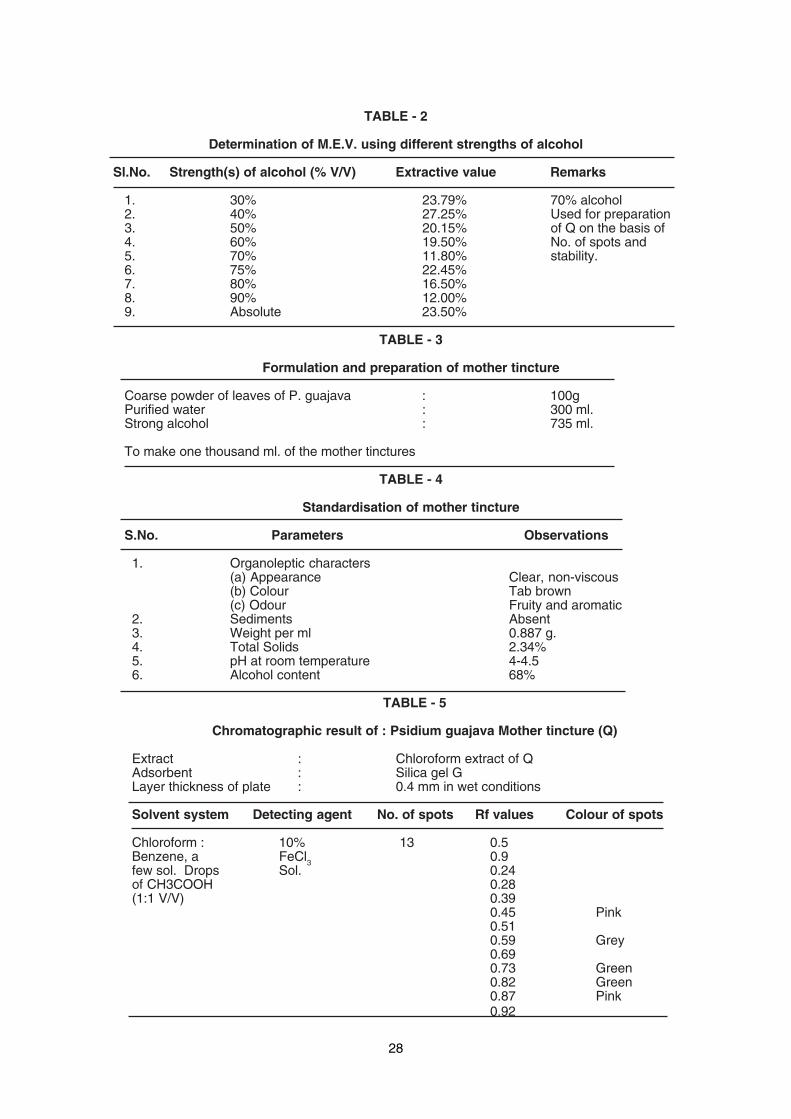
TABLE - 2
Determination of M.E.V. using different strengths of alcohol
Sl.No. Strength(s) of alcohol (% V/V) Extractive value Remarks
1. 30% 23.79% 70% alcohol2. 40% 27.25% Used for preparation3. 50% 20.15% of Q on the basis of4. 60% 19.50% No. of spots and5. 70% 11.80% stability.6. 75% 22.45%7. 80% 16.50%8. 90% 12.00%9. Absolute 23.50%
TABLE - 3
Formulation and preparation of mother tincture
Coarse powder of leaves of P. guajava : 100gPurified water : 300 ml.Strong alcohol : 735 ml.
To make one thousand ml. of the mother tinctures
TABLE - 4
Standardisation of mother tincture
S.No. Parameters Observations
1. Organoleptic characters(a) Appearance Clear, non-viscous(b) Colour Tab brown(c) Odour Fruity and aromatic
2. Sediments Absent3. Weight per ml 0.887 g.4. Total Solids 2.34%5. pH at room temperature 4-4.56. Alcohol content 68%
TABLE - 5
Chromatographic result of : Psidium guajava Mother tincture (Q)
Extract : Chloroform extract of QAdsorbent : Silica gel GLayer thickness of plate : 0.4 mm in wet conditions
Solvent system Detecting agent No. of spots Rf values Colour of spots
Chloroform : 10% 13 0.5Benzene, a FeCl3 0.9few sol. Drops Sol. 0.24of CH3COOH 0.28(1:1 V/V) 0.39
0.45 Pink0.510.59 Grey0.690.73 Green0.82 Green0.87 Pink0.92

29
TABLE - 6
UV Absorbance of alcoholic extract of leaves of P. guajava
Mother tincture No. of peaks UV absorbance
Psidium guajava Q 5 259.5 nm254.3 nm239.4 nm221.5 nm212.5 nm
Discussion
Psidium guajava is also known as the appleof the tropics and grows under a wide variety ofclimatic conditions. Guava is one of the richestnatural sources of vitamin C besides pectin andother nutrients. Leaves are reported to contain cat-echol and pyrogallol types of tannins1. The leavesare popularly used in tanning leathers.
a) Pharmacognostic features :
The leaves are light green, finely pubescentand chartaceous. Epidermal cells in surface showstriations on adaxial side. Stomata occur only onlower surface. Paracytic type being dominant be-sides anisocytic and anomocytic. Unicellular coni-cal and uniseriate flagellate conical hairs occur oneither surfaces. Stomatal index is 22.13.
Transectionally midvein is kidney shapedbeing prominently ribbed towards abaxial andgrooved adaxially. Lamina wing is 151-173 µm inthickneww. Secretary cavities appear conspicu-ously on the abaxial surface. An adaxial hypodermof 3-4 layers is conspicuous and confirms earlierobservations of Metcalfe and Chalk7. Palisade is 4layered and is confined to abaxial side. Secretorycavities interrupt the mesophyll. Cells of mesophylloften contain tannins and sphaeraphides besideschloroplasts.
Ground parenchyma at midvein is inter-spersed with secretory cavities besidessphaeraphidal and tanniniferous idioblasts. Asclerenchymatous cap of 8-10 celled thick enclosesthe midvein bundle.
Central vascular bundle is sigma shaped,918-950 µm laterally long and 183-205 µm verti-cally thick; endarch, and bicollateral. Secondarywalls of xylary elements possess helical andscalariform thickenings.
Petiole
In surface epidermal cells are polygonal withstraight to curved sides. Epidermal cells often pos-sess tannins and prismatic crystals of calciumoxalate. The epidermal surface also is dispersedwith some conical and flagellate hairs.
In transaction 3-4 mm in diameter, laterallyelongated with an adaxial groove. Epidermis is 1-layered and hypodermal collenchyma is 1-2 layered.Ground parenchyma is predominant, interspersedwith cells containing tannins and sphaeraphides. 8-12 layered sclerenchyma encloses the central vas-cular bundle.
Vascular tissue is made of a single largesigma shaped bundle which is bicollateral andpericyclic. Phloem is scanty and present on eithersides of xylem.
b) Physico-chemical
Alcohol extract and mother tincture haveshown positive tests for tannins. The data pertain-ing to physico-chemical studies of raw drugs is pre-sented in table 1. Formulation of mother tincture isgiven in table 2 & 3. Physico-chemical constantsof mother tincture are summarized in Table 4. TLCstudy on Chloroform extract of the mother tincturereveals 3 prominent spots on spraying with 10%Ferric chloride solution and heating at 110 C (Table5). It is evident from the raw drug studies that thevalue of acid insoluble ash falls within the accept-able range.
HPTLC profile shows absorbance in the shortand long wave length of UV light before derivitisationwhile after derivitisation i.e. subsequent to spray-ing with methanolic sulfuric acid and anisaldehydesulfuric acid separately, reveals eight bands withRf values 0.15, 0.19, 0.28, 0.51, 0.57, 0.66, 0.79and 0.94 correspondingly in both.

30
The diluted mother tincture (1 ml Q dilutedwith 99 ml of alcohol) reveals large number of peaksin the UV region. It is clear that 70% alcohol usedfor preparation of mother tincture is the best alco-hol in accordance with Homoeopathy philosophy.However, five major peaks amongst them are re-ported.
Acknowledgements
The authors thank Prof. C. Nayak, Director,Central Council for Research in Homoeopathy, NewDelhi for encouragement and facilities. Thanks arealso due to Anchrom HPTLC applications Labora-tory, Mumbai, for HPTLC profile and scientistincharge, CFTRI, RC, Hyderabad, for UV studies.
References
1. Anonymous, 1969, Wealth of India, Rawmaterial, Vol. 8, Publication and InformationDirectorate, CSIR, New Delhi.
2. Anonymous, 1971, Homoeopathic Pharma-copoeia of India, Vol 1, Ministry of Health andFamily Welfare, Govt. of India, New Delhi.
3. Johnson, D.A. 1940, Plant Microtechnique,Mc Graw Hill Book Col., New York.
4. Kaudil, F.E. et al., 1997. Flavonoids fromPsidium guajava, Asian Journal of Chemis-try, 9(4), 871-872.
5. Kirtikar, K.R. AND b.d. Basu, 1980, IndianMedicinal Plants, Vol. 2, Bishen SinghMahendra Pal Singh, Dehradun.
6. Leelavathi, A. and N. Ramayya, 1975, Rapid,isolation of leaf epidermis by double treat-ment method, Geobios, Vol. 2, 117-119.
7. Metcalf, C.R. and L. Chalk, 1950, Anatomyof the Dicotyledeons, Vol. 1, Oxford Univer-sity Press, London.
8. Rabe, T. and J. Van Staden, 1997, Antibac-terial activity of South African plants used formedicinal purposes, J. Ethnopharmacology,56(1), 81-87.
9. Youngken, H.W., 1951, PharmaceuticalBotany, Rep. Ed. International Book Distribu-tors, Dehradun.

31
Role of Homoeopathy in Migraine in Adolescence
Dr. S. Gopinadhan*
GENERAL ARTICLE
Abstract
The aim of this paper is to show that the treat-ment on the basis of similia similibus curentur is thebest psychosomatic approach for migraine in ado-lescence. 25 cases of adolescent patients suffer-ing from classical migraine were treated as out pa-tients during the period 1997-2002. Homoeopathicmedicines were selected on totality of symptoms.A total of 21 cases were relieved out of 25 cases.Of these 11 cases had no recurrence, 7 hadmoderate improvement and 3 had mildimprovement. 3 cases showed no improvementwhereas one patient reported with aggravation ofsymptoms.
Introduction
Headache is a headache for both physicianand the patient. This is the commonest but themost difficult clinical problem encountered by thephysician. Most often headache is asymptomatic expression of some minor ailments,mental tension or fatigue, but occasionally it is ofsinister significance, indicative of seriousintracranial disease and i.e. why when a person ishaving regular headache, he may be much alarmeddue to anxiety and fear. Among different types ofheadaches, such as referred headache, neuralgicheadache, headache due to meningeal irritation,vascular headaches, traction headache andpsychogenic headache, vascular headache isoften very severe. The commonest form ofvascular headache is MIGRAINE1. The wordMigraine came from another word 'Megrime'meaning Hemi cranial. Migraine is characterizedby epidsodic throbbing, hemi cranial headache be-ginning in childhood, adolescent or early adult lifewhich tends to decrease in intensity and frequencyas age advances. Although migraine may beginat any age the usual onset is adolescene or youngadult life2. Women are slightly more affected andout number men by about 4:1 and in many cases apositive family history is elicitable.
There are two types of migraine:
1.Common migraine
Unilateral throbbing headache lasting a fewhours with nausea and vomiting but there is no pre-ceding neurological symptoms.
2. Classical migraine also known as neurologicmigraine; has hemicranial or generalized throbbingheadache with nausea and vomiting and lasts forone to two days but is preceded by prominentneurological symptoms, known as aura.
Diagnosis in both the varieties is made mainlyfrom history3. The most common aura is visualdisturbances such as dazzling zig zag lines,scintillating scotoma, homonymous hemianopia,field defects and rarely total blindness. The auralasts for 15-30 minutes and usually is merged withhemicranial or generalized headache. There aremany aggravating or precipitating factors but themost common factors are anxiety, emotional stress,menstruation (pre menstrual tension), relaxation ofstress, alcohol, overwork and change of weather4.As this is one of the important types of headache,psychological factors play a major role in itsprecipitation and maintenance5.
According to modern medicine the treatmentof migraine falls into three groups such as (i) avoid-ance of aggravating or precipitating factors (ii) con-trol of acute attacks and (iii) prophylaxis. To avoidthese precipitating factors, physician used to givefull explanation to the patient about the nature andphenomena of migraine. But this is not always ef-fective because the persons affected with migrainehave peculiar personality. They have excessive selfdemands, they are over ambitious, perfectionist,meticulous and scruplous. Failure to attainperfection and ambition leads to mental stress andstrain. Therefore, all known precipitating factors es-pecially the anxiety and emotional stress cannotbe avoided by the patient. Another important
*Assistant Research Officer(Homoeo.), Central Research Institute(Homoeo.), Kottayam

32
precipitating factor, say, pre menstrual tension, alsois very difficult to avoid by mere explanation orcounseling. Since these patients are over ambi-tious they are liable to more physical strain which isone of the important aggravating factors and it isvery difficult for such persons to refrain from overwork. Therefore, instead of asking them to avoidanxiety, overwork or mental stress, their personalattitudes are to be changed and this is possible onlythrough the homoeopathic treatment becausethe personality of a person is a manifestation of theunderlying chronic miasm.
This short scientific paper is based on stud-ies conducted in O.P.D. at CRI(H) Kottayam on 25adolescent patients suffering from classical migrainewith homoeopathic medicine in the period 1997-2002. All these cases were treated only withhomoeopathic medicines, i.e. without any psycho-logical advice. Since psychological factors play amajor role in the causation or precipitation of mi-graine a complete psychosomatic approach withsimilimum is necessary. As mentioned in the Or-ganon of Medicine by Dr. Samuel Hahnemann, ‘afterthe control of acute attacks these patients shouldbe treated with deep acting anti miasmatic remediesin order to prevent further attacks’.
Materials and Methods
The materials for the study consisted of 25cases of classical migraine in adolescence treatedduring the period between 1997-2000 as outpatients. These 25 patients included 9 males and16 females (refer Table-I) between the age of 13years - 18 years (refer Table-II). All of them hadaura before the onset of headache and the majorityhad visual disturbances like dazzling, zig zag lines,dimness of vision, lachrimation, pain in eyes andphotophobia (refer Table-III). The duration of thecomplaints ranged from 8 months to 5 years but inmajority it was between 2 & 5 years (refer Table-IV). These patients had different aggravating andprecipitating factors (refer Table-V), but all of themhad one or other types of emotional stress as pre-cipitating factors. But in many cases more thanone precipitating factors were present. Similarlymajority of the patients studied had positive familyhistory of migraine (refer Table-VI). A detailed studyon the episodes of migraine reveals that the majoritysuffered from moderate to severe headache, theduration of the episodes ranged from less than 5hours to 15 hours and frequency of attack rangedfrom more than once a month to once in threemonths. But in majority, the frequency of episodeswas once in a month (refer Table-VIII-X).
The method of study was purely clinical innature. These 25 cases of migraine were includedfor the study on the basis of the following criteria:
1. Only adolescent migraine cases wereselected
2. Only classical migraine was included3. Both males and females were included4. Patients with other systemic diseases were
excluded5. Patients with emotional and psychological
stress as precipitating factors forheadache only were included
6. Before inclusion all related investigationswere done to exclude other causes ofheadache.
In each case a detailed case history wastaken with special stress given to aggravating andprecipitating factors, personal history and mentaldisposition of the patient and in all cases a mias-matic analysis was also done in order to find outwhich miasm was predominant and later on it helpedfor the selection of remedies for follow-up studies.All these patients were given medicines after strictindividualization, in minimum dose, along withplacebo. They were advised to repeat the dose onthe occurrence of the next episode only. They werealso advised to avoid coffee, tea, coco and otherdrugs used externally or internally during the wholecourse of the treatment. Each and every case wasfollowed up for two years and final assessment wasdone after that. In many cases after the relief of theacute attacks with short acting remedies, deep act-ing anti-miasmatic remedies were found necessaryto prevent further episodes of headache. But incertain cases drugs found effective to control theacute attacks were also found effective for the pre-vention of the episodes.
To test the significance of the result ob-tained the data collected from the study especiallythe frequency of paroxysms before and after thetreatment was statistically analysed with the helpof Paired T test. The null hypothesis H0 in this studyis that the treatment is not effective and the alter-nate hypothesis H1 is that the treatment is effec-tive. For the statistical analysis, disease intensityscores were given on the basis of frequency of epi-sodes before and after treatment (refer Table-XVI).
Observation
All the results obtained were given in tabu-lar form from Table I-XVI. The results obtained wereconfined to those 25 cases only. It showed that 11out of 25 cases had marked improvement with norecurrence after one or two initial attacks, 07 cases
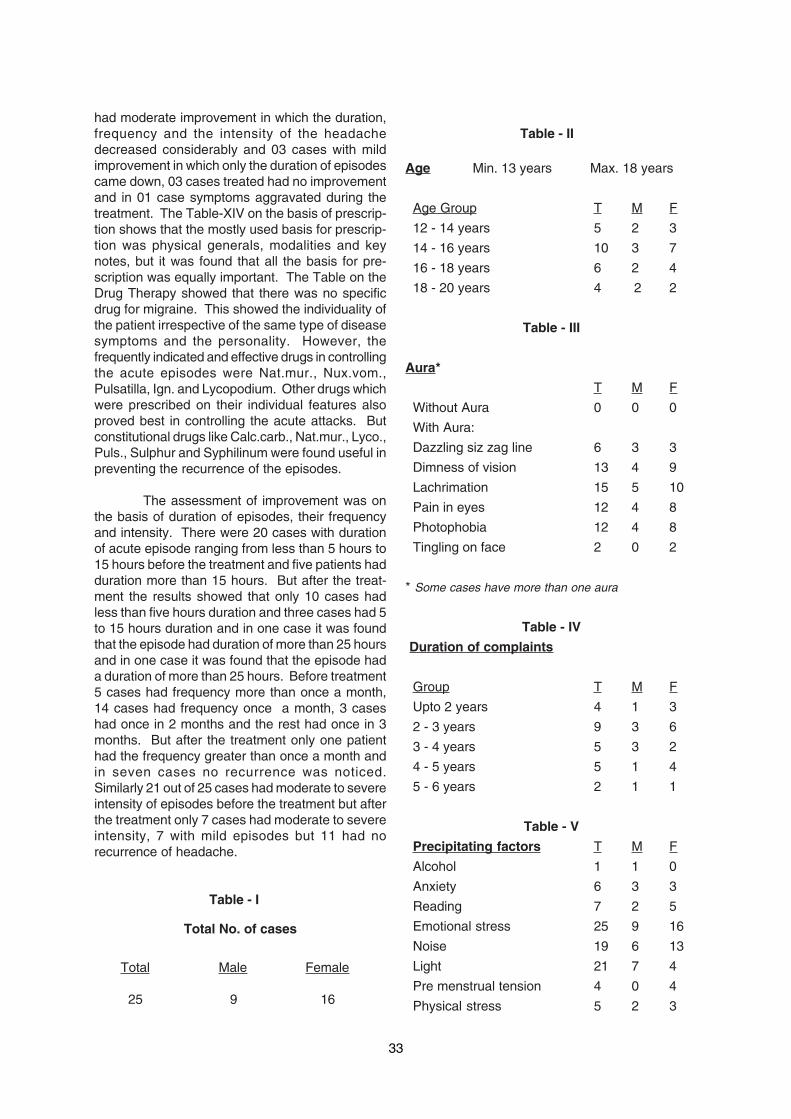
33
had moderate improvement in which the duration,frequency and the intensity of the headachedecreased considerably and 03 cases with mildimprovement in which only the duration of episodescame down, 03 cases treated had no improvementand in 01 case symptoms aggravated during thetreatment. The Table-XIV on the basis of prescrip-tion shows that the mostly used basis for prescrip-tion was physical generals, modalities and keynotes, but it was found that all the basis for pre-scription was equally important. The Table on theDrug Therapy showed that there was no specificdrug for migraine. This showed the individuality ofthe patient irrespective of the same type of diseasesymptoms and the personality. However, thefrequently indicated and effective drugs in controllingthe acute episodes were Nat.mur., Nux.vom.,Pulsatilla, Ign. and Lycopodium. Other drugs whichwere prescribed on their individual features alsoproved best in controlling the acute attacks. Butconstitutional drugs like Calc.carb., Nat.mur., Lyco.,Puls., Sulphur and Syphilinum were found useful inpreventing the recurrence of the episodes.
The assessment of improvement was onthe basis of duration of episodes, their frequencyand intensity. There were 20 cases with durationof acute episode ranging from less than 5 hours to15 hours before the treatment and five patients hadduration more than 15 hours. But after the treat-ment the results showed that only 10 cases hadless than five hours duration and three cases had 5to 15 hours duration and in one case it was foundthat the episode had duration of more than 25 hoursand in one case it was found that the episode hada duration of more than 25 hours. Before treatment5 cases had frequency more than once a month,14 cases had frequency once a month, 3 caseshad once in 2 months and the rest had once in 3months. But after the treatment only one patienthad the frequency greater than once a month andin seven cases no recurrence was noticed.Similarly 21 out of 25 cases had moderate to severeintensity of episodes before the treatment but afterthe treatment only 7 cases had moderate to severeintensity, 7 with mild episodes but 11 had norecurrence of headache.
Table - I
Total No. of cases
Total Male Female
25 9 16
Table - II
Age Min. 13 years Max. 18 years
Age Group T M F
12 - 14 years 5 2 3
14 - 16 years 10 3 7
16 - 18 years 6 2 4
18 - 20 years 4 2 2
Table - III
Aura*
T M F
Without Aura 0 0 0
With Aura:
Dazzling siz zag line 6 3 3
Dimness of vision 13 4 9
Lachrimation 15 5 10
Pain in eyes 12 4 8
Photophobia 12 4 8
Tingling on face 2 0 2
* Some cases have more than one aura
Table - IV
Duration of complaints
Group T M F
Upto 2 years 4 1 3
2 - 3 years 9 3 6
3 - 4 years 5 3 2
4 - 5 years 5 1 4
5 - 6 years 2 1 1
Table - V
Precipitating factors T M F
Alcohol 1 1 0
Anxiety 6 3 3
Reading 7 2 5
Emotional stress 25 9 16
Noise 19 6 13
Light 21 7 4
Pre menstrual tension 4 0 4
Physical stress 5 2 3
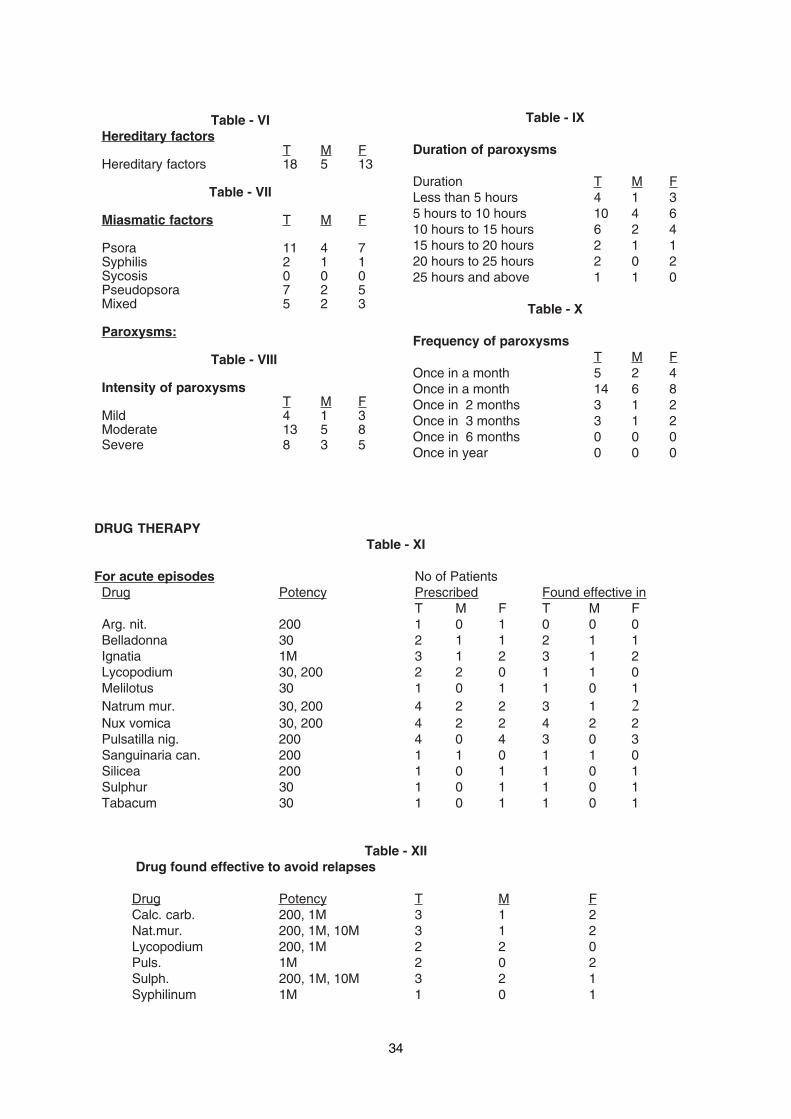
34
Table - VIHereditary factors
T M FHereditary factors 18 5 13
Table - VII
Miasmatic factors T M F
Psora 11 4 7Syphilis 2 1 1Sycosis 0 0 0Pseudopsora 7 2 5Mixed 5 2 3
Paroxysms:
Table - VIII
Intensity of paroxysmsT M F
Mild 4 1 3Moderate 13 5 8Severe 8 3 5
Table - IX
Duration of paroxysms
Duration T M FLess than 5 hours 4 1 35 hours to 10 hours 10 4 610 hours to 15 hours 6 2 415 hours to 20 hours 2 1 120 hours to 25 hours 2 0 225 hours and above 1 1 0
Table - X
Frequency of paroxysmsT M F
Once in a month 5 2 4Once in a month 14 6 8Once in 2 months 3 1 2Once in 3 months 3 1 2Once in 6 months 0 0 0Once in year 0 0 0
DRUG THERAPYTable - XI
For acute episodes No of PatientsDrug Potency Prescribed Found effective in
T M F T M FArg. nit. 200 1 0 1 0 0 0Belladonna 30 2 1 1 2 1 1Ignatia 1M 3 1 2 3 1 2Lycopodium 30, 200 2 2 0 1 1 0Melilotus 30 1 0 1 1 0 1Natrum mur. 30, 200 4 2 2 3 1 2Nux vomica 30, 200 4 2 2 4 2 2Pulsatilla nig. 200 4 0 4 3 0 3Sanguinaria can. 200 1 1 0 1 1 0Silicea 200 1 0 1 1 0 1Sulphur 30 1 0 1 1 0 1Tabacum 30 1 0 1 1 0 1
Table - XII Drug found effective to avoid relapses
Drug Potency T M FCalc. carb. 200, 1M 3 1 2Nat.mur. 200, 1M, 10M 3 1 2Lycopodium 200, 1M 2 2 0Puls. 1M 2 0 2Sulph. 200, 1M, 10M 3 2 1Syphilinum 1M 1 0 1
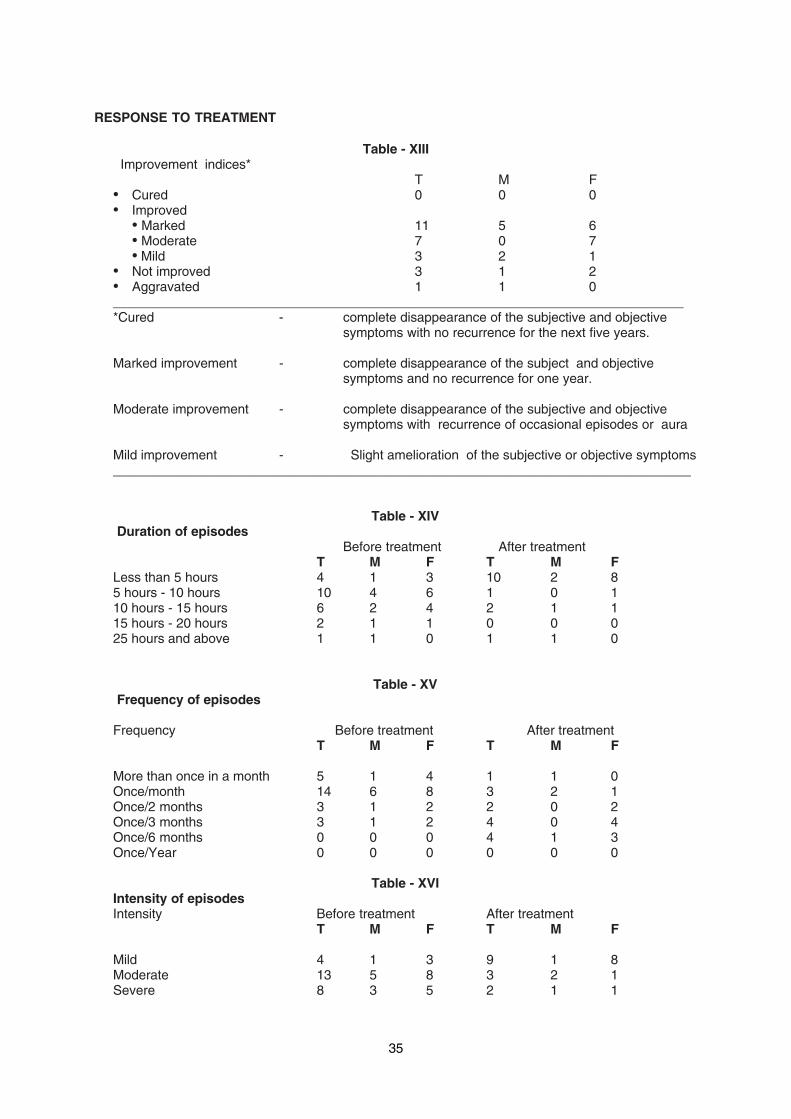
35
RESPONSE TO TREATMENT
Table - XIII Improvement indices*
T M F• Cured 0 0 0• Improved
• Marked 11 5 6• Moderate 7 0 7• Mild 3 2 1
• Not improved 3 1 2• Aggravated 1 1 0______________________________________________________________________________*Cured - complete disappearance of the subjective and objective
symptoms with no recurrence for the next five years.
Marked improvement - complete disappearance of the subject and objectivesymptoms and no recurrence for one year.
Moderate improvement - complete disappearance of the subjective and objectivesymptoms with recurrence of occasional episodes or aura
Mild improvement - Slight amelioration of the subjective or objective symptoms_______________________________________________________________________________
Table - XIV Duration of episodes
Before treatment After treatmentT M F T M F
Less than 5 hours 4 1 3 10 2 85 hours - 10 hours 10 4 6 1 0 110 hours - 15 hours 6 2 4 2 1 115 hours - 20 hours 2 1 1 0 0 025 hours and above 1 1 0 1 1 0
Table - XV Frequency of episodes
Frequency Before treatment After treatmentT M F T M F
More than once in a month 5 1 4 1 1 0Once/month 14 6 8 3 2 1Once/2 months 3 1 2 2 0 2Once/3 months 3 1 2 4 0 4Once/6 months 0 0 0 4 1 3Once/Year 0 0 0 0 0 0
Table - XVIIntensity of episodesIntensity Before treatment After treatment
T M F T M F
Mild 4 1 3 9 1 8Moderate 13 5 8 3 2 1Severe 8 3 5 2 1 1

36
Discussion
The study of 25 cases of adolescent migraineshows that all are having one or the other type ofpsychological stress and anxiety which play the roleof exciting and maintaining cause for the headache.In this study group females are more affected thanmales which is in conforming with what is said intext books. The miasmatic study shows that themajority of the group falls under Psora andPseudopsora while the rest belongs to mixed group.This may be the reason that in majority of the pa-tients multi miasmatic remedies are found useful tocontrol acute episodes and to prevent further at-tacks.
The drug therapy part shows that many drugsare found useful to control the acute paroxysmsand to prevent the recurrence (13 drugs in 25cases). This reveals that there is no specific rem-edies for migraine but only specifics for individualpatients.
The table on improvement indices shows that21 out of 25 cases improved in various degreesout of which 11 cases had no recurrence of head-ache for the next two years and 7 had moderateimprovement in which there was considerable re-duction in the duration, frequency and intensity ofattacks. Three cases studied shows no responseafter the treatment, but in one patient the headacheaggravated after the treatment. More than 80%improvement obtained in this study is a greatachievement and this shows the efficacy of Ho-moeopathic medicine given on the basis of indi-vidualization. This is more evident when we gothrough the tables on response to treatment relatedto the duration, frequency and intensity of head-ache (refer XV-XVII). After a month the 14 cases,which had relapse of migraine, 9 cases had head-ache in mild intensity only with occasional aura whilethe rest had moderate to severe headache butthe duration and frequency were reduced exceptin 1 case.
Conclusions
1. The most common age group which isprone to migraine of psychosomatic originis adolescence because this age group isvulnerable to great emotional, psychologicaland physical stress as they are passingthrough a new phase of life which is differentfrom infancy and childhood.
2. The predominant miasms found out in thisstudy which are responsible for migraineare psora and pseudopsora.
3. There is no specific remedy for adolescentmigraine but drugs selected on strictindividualization only are found useful.
4. In adolescent migraine the true psychoso-matic approach is the homoeopathic way oftreatment because the drugs prescribed onthe basis of the totality of the symptomswere able to give relief in 21 out of 25cases.
Acknowledgement
I acknowledge the constant help and encour-agement received from the Director, CCRH with-out which such research work could not be done. Ialso acknowledge with thanks those who helpedme in this study and the preparation of thisscientific paper.
References
1. Churchil's Pocket Book of Medicine p-28.
2. Lance J.W., Mechanism and Managementof Headache Edition IV, Butterworth,Stoneham M.A. 1982.
3. C. Houston, L. Joiner, R. Trounce, A ShortText Book of Medicine, ELBS 7th EditionP-370.
4. Harold I. Kaplan; Benjamin J. Sadock,Comprehensive Text Book of PsychiatryVol. I Vth Edition p-232.

37
WEB INFORMATION
Avian Influenza (Bird Flu) & Homoeopathy: Search On InternetO.P.Verma*
"Given the high level of global traffic, the pandemic virus may spread rapidly, leaving little or notime to prepare."
- World Health Organization
Avian influenza (AI) is a disease of viraletiology that ranges from a mild or evenasymptomatic infection to an acute, fatal diseaseof chickens, turkeys, guinea fowls, and other avianspecies, especially migratory waterfowl.
Most avian species appear to besusceptible to at least some of the AI viruses. Aparticular isolate may produce severe disease inturkeys but not in chickens or any other avianspecies. Therefore, it would be impossible togeneralize on the host range for HPAI, for it willlikely vary with the isolate. This assumption issupported by reports of farm outbreaks where onlya single avian species of several species presenton the farm became infected. Swine appear to beimportant in the epidemiology of infection of turkeyswith swine influenza virus when they are in closeproximity. Other mammals do not appear to beinvolved in the epidemiology of HPAI. The infectionof humans with an H5 avian influenza virus in HongKong in 1997 has resulted in a reconsideration ofthe role of the avian species in the epidemiology ofhuman influenza.
Highly pathogenic avian influenza viruseshave periodically occurred in recent years inAustralia (H7), England (H7), South Africa (H5),Scotland (H5), Ireland (H5), Mexico (H5), Pakistan(H7), and the United States (H5). Becauselaboratory facilities are not readily available in someparts of the world to differentiate Newcastle diseaseand HPAI, the actual incidence of HPAI in the world'spoultry flocks is difficult to define. It can occur inany country, regardless of disease controlmeasures, probably because of its prevalence inwild migratory waterfowl, sea birds and shore birds.
Highly pathogenic avian influenza issuspected with any flock where sudden deathsfollow severe depression, inappetence, and a drasticdecline in egg production. The presence of facialedema, swollen and cyanotic combs and wattles,and petechial hemorrhages on internal membranesurfaces increases the likelihood that the disease
* Librarian, Central Council for Research in Homoeopathy, New Delhi
is HPAI. However, an absolute diagnosis isdependent upon the isolation and identification ofthe causative virus. Commercially available type Ainfluenza antigen-capture enzyme linkedimmunosorbent assay kits designed for use inhuman influenza have recently shown promise asa possible rapid diagnostic test for poultry.
This article is intended for busyscientists engaged in research work in the fieldof Avian Flu to help them reap the benefits ofthe Internet without surfing too much forlocating the resources.
• http://www.pandemicflu.gov/
One stop access to U.S. Government avianand pandemic flu information. Managed by theDepartment of Health and Human Services. Therisk from avian influenza is generally low to mostpeople, because the viruses do not usually infecthumans. However, confirmed cases of humaninfection from several subtypes of avian influenzainfection, including H5N1, have been reported since1997. Most cases of avian influenza infection inhumans have resulted from contact with infectedpoultry (e.g., domesticated chicken, ducks, andturkeys) or surfaces contaminated with secretion/excretions from infected birds.
• http://www.cdc.gov/flu/avian/
The Centres for Disease Control andPrevention stated how are avian, pandemic, andseasonal flu different?Avian flu is caused by avian influenza viruses, whichoccur naturally among birds.Pandemic flu is flu that causes a global outbreak,or pandemic, of serious illness that spreads easilyfrom person to person. Currently there is nopandemic flu.Seasonal flu is a contagious respiratory illnesscaused by influenza viruses.

38
• w w w . w h o . i n t / c s r / d i s e a s e /avian_influenza/en/
WHO is coordinating the global responseto human cases of H5N1 avian influenza andmonitoring the corresponding threat of an influenzapandemic. Information on this page tracks theevolving situation and provides access to bothtechnical guidelines and information useful for thegeneral public.
• www.homeopathy.boiron.com/en/htm/service/actualites.htm
The first WORLD MEDICALCONFERENCE on the theme 'Homeopathy andAvian Influenza' took place in Paris on Saturday 19November 2005. Homeopathy is routinely used andprescribed for the prevention and as treatment for"ordinary" influenza with an effectiveness that hasbeen recorded in several scientific publications*.This explains why homeopathic physicians andpharmacists are being increasingly consulted aboutavian influenza: what can homeopathy do? On apreventive or curative level?
• w w w . h o m e o w e b . c o m / c l i n i c /bird_flu.htm
Homeopathy offers a much effectivetreatment against viral infections in general. Also itoffers complete cure in almost all infectious illnessif there is not much destruction of tissues that is incases other than advanced pathological changes.It is of greater importance that as homeopathy canstart effective treatment based on symptomatologyone can start the damage control much earlierbefore actual diagnosis of bird flu. The only problembeing many a cases of possible bird flue (or anyother grave or answerless illness) will be completelycured without there is a chance for proper diagnosisand recording the credit to the account ofhomeopathy. But no good homeopath needs creditbut relief to suffering human
• w w w . u s e n a t u r e . c o m /article_bird_flu.htm
Its not difficult to find someone these days who isconcerned about the possibility of an influenzapandemic throughout the world. Equally commonare the theories that abound from a plethora of'experts' and medical/scientific institutions about itslikelihood, the form it might take and the possiblelevels of devestation that it might reap throughoutthe animal and human populations.
• http://www.wisegeek.com/what-is-bird-flu.htm
Most health experts researching andfighting the incidence of human bird flu do not have
an optimistic outlook. They point out that thepathogen has not appeared to evolve such thathuman-to-human contact is contagious, yet itremains that people working with fowl, swimming ininfected rivers, playing in an area where carcasseswere buried, or breathing air near a poultryprocessing plant, can lead to infection.
• w w w . h o m e o w e b . c o m /bird_flu_more.htm
There has been much discussion about themerits or otherwise of Avian Flu anti-viral medicinesin the media but no discussion of the effectivenessof homeopathy in the treatment of influenza. Historyshows us that homeopathy was used byhomeopathic physicians in USA to treat patientsduring 1918-1919 influenza epidemic. Frominformation recorded by these doctors, homeopathictreatment was highly successful. In most cases oneor two homeopathic medicines were needed. Theseare known as the "Genus epidemicus" in anepidemic and become known through the carefulobservation of a number of influenza cases. It isdifficult to speculate exactly what homeopathicremedies will work best in the possible Avian fluepidemic. However there are a number of known'flu remedies that may be useful eg Gelsemium,Bryonia, Arnica, Eupatorium perfoliatum, Arsenicumetc . In the 1918 epidemic Gelsemium and Bryoniawere most commonly indicated according to thefollowing extracts
• w w w . a c a c i a a n i m a l c a r e . c o m /influenza.htm
Many viruses and bacteria travel betweenspecies. Usually they do not cause overt diseasein humans , people for example catch Fowlpoxwithout even knowing they have had it, as it maynot replicate in the cells.
• www.goldbamboo.com/topic-t7926.html
Influenza, or flu, is a respiratory infection causedby a variety of flu viruses. The most familiar aspectof the flu is the way it can "knock you off your feet"as it sweeps through entire communities. Studiessuggest that the prescription medicines approvedfor human flu viruses would work in preventing birdflu infection in humans. However, flu viruses canbecome resistant to these drugs, so thesemedications may not always work. The risk frombird flu is generally low to most people because theviruses occur mainly among birds and do not usuallyinfect humans. However, during an outbreak of birdflu among poultry (domesticated chicken, ducks,turkeys), there is a possible risk to people who havecontact with infected birds or surfaces that havebeen contaminated with excretions from infectedbirds.

39
• www.bird-flu-facts.info/date/2005/11
What type of vaccines has been developedfor bird flu - This website publishes bird fluinformation and resources. The H5N1 strain of birdflu has killed at least 62 people in Asia so far. It is aflu carried by birds that can be contracted byhumans. There are growing fears that a pandemiccould start soon as a result of this bird flu. There iscurrently no vaccine for the bird flu, but if anpandemic occurs with a hybrid form, researcherswill be quick to engineer one.
• www.appleseek.com/6885.php
AS BIRD flu, or Avian Influenza, ragedthrough Asia, countries such as Vietnam, China,Thailand, Indonesia, Cambodia, Laos, Japan, Koreaand Taiwan are stepping up on massive culling oftheir poultry as they are seized by a realisation thatthe animal virus could eventually threaten humanlives.www.information-homeopath.com/Bird-flu.htmlAccording to CDCP (the US Centre for DiseaseControl and Prevention), symptoms of bird flu inhumans have ranged from typical flu-like symptoms(fever, cough, sore throat and muscle aches) to eyeinfections, pneumonia, severe respiratory diseases(such as acute respiratory distress), and othersevere and life-threatening complications. (Thesymptoms of bird flu may depend on which viruscaused the infection.) This sounds like bad news.However!...Bird flu is hard to catch Judging from reports so far,catching bird flu is quite difficult. You have to livewith the chickens, literally in the same room as them,and be handling them or in physical contact withthem for quite some time. This explains why fewpeople have caught it so far.
• www.cochrane .o rg / rev iews /en /ab001957.html
Homoeopathic Oscillococcinum does notprevent influenza, but probably shortens the lengthof the illness .Influenza (the flu) is a highly infectiousdisease caused by viruses. Other than treatmentsfor complications (such as pneumonia),conventional medical treatment is bed rest.Homeopathy is a system based on "curing like withlike", often using highly diluted substances.Oscillococcinum is a homoeopathic preparationmanufactured from wild duck heart and liver(common sources of influenza). It is claimed thatOscillococcinum (or similar homeopathic medicines)can be taken regularly over the winter months toprevent flu, or as a treatment. The review found that
trials do not show that it can prevent flu. Taking itonce you have flu probably shortens the illness, butmore research is needed.
• www.shrtn.info/users/surveillance-avian-flu
This Day Online - Federal Government andthe 36 state governments at the weekend called oninternational agencies and other developmentpartners to come to its aid in tackling the avianinfluenza which has spread to 10 states of thecountry so far.
• www.netplo.com/pworldsflu.html
This is a planet wave resource area in thefield of study of Avian Flu. Access to the latest newsregarding outbreaks of disease. Page also providesaccess to disease outbreak news archives, (by year,disease or country). A RSS feed for notification ofupdates is also available from this page.
• www.avianflutests.com/list/2/avian-flu-homeopathic-remedy.html
Welcome to the information page aboutavian flu homeopathic remedy.They have compiled a list of avian flu homeopathicremedy websites at: avian flu homeopathic remedySite Map. This list of avian flu homeopathic remedywebsites will be updated regularly.
• http://www.911-bird-flu.com/
This is a specialized news site for Bird Flu. Oneminute the US government is stockpiling Tamiflu,the main drug used to treat flu symptoms in Asianhospitals; the next, researchers say that H5N1 virusis already mutating and building resistance to thedrug. So, what's a fairly-conscious, always-prepared, not-ready-to-die-of-blasted-flu health nutsupposed to do? Get some antivirals in your naturalremedies cabinet. Olive leaf extract is a good one.So is LarreaX, made from a plant in the Southwestdesert. Others rely on colloidal silver.
• www.birdfluweb.com
We have put this web site together foranyone interested in bird flu symptom so we inviteyou to take a tour. We hope you find what you arelooking for. But if you don't please do not hesitateto email us at the address shown at the bottom ofthis web site. It is your feedback that helps us tomake sure that this site eventually becomes one ofthe best bird flu symptom resources on the web.

40
MEDI NEWS
1. Carbon Monoxide Helps Shut Down theIntestinal Inflammation that Causes UlcerativeColitis
Doctors have long known that smokersrarely suffer from a common form of inflammatorybowel disease (IBD) called ulcerative colitis, but theydidn't know why. A new study in the December 19issue of The Journal of Experimental Medicine mighthelp explain this apparent resistance. Scott Plevyand his colleagues at the University of Pittsburghnow show that carbon monoxide (CO), a componentof cigarette smoke, helps shut down the intestinalinflammation that causes ulcerative colitis.
CO is best known as a toxic air pollutant,but small amounts of this gas are also produced inthe human body as a normal by-product ofmetabolism, suggesting that the effects of CO mustnot be all bad. High dose CO gas is lethal, becauseit robs the body of life-sustaining oxygen. It is thisasphyxiant property of CO that has earned it a badreputation. But recent scientific studies have shownthat CO -- at least at low concentrations -- has aredeeming quality: it acts as an anti-inflammatoryagent.
It is this quality, according to Plevy andcolleagues, that allowed CO to ease the symptomsof IBD in mice. The group traced the action of inhaledCO to a protein that is produced by immune cellscalled interleukin (IL)-12. IL-12 is normally producedduring infection and helps activate the immune cellsthat fight off the invading pathogens. But chronicproduction of IL-12 in the gut also drives theinflammation that causes ulcerative colitis. InhaledCO inhibited the production of IL-12, short-circuitingthe disease-causing inflammation.
The researchers are now trying to unravelthe specific cellular components that are requiredfor CO to inhibit IL-12. In the meantime, Plevy thinksthat inhaled CO might provide some relief forpatients with ulcerative colitis. But non-smokers withIBD shouldn't necessarily break out the Marlboros,as cigarette smoking is a risk factor not only forheart disease and cancer but also for Crohn'sdisease, another form of IBD.
(Source: Medical News Today, Category: Irritable-BowelSyndrome News, dated 20 Dec. 2005)
2. Passive Smoking Almost Doubles Risk OfDegenerative Eye Disease
Passive smoking doubles the risk of thedegenerative eye disease, macular degeneration,shows research in the British Journal ofOphthalmology.
The macula lies at the centre of retina atthe back of the eye. It's crucial for fine central vision,which is essential for tasks, such as reading anddriving.
The risk of macular degeneration increasesat the age of 60. It is a leading cause of partialsightedness and blindness in many Europeancountries and the USA.
The researchers base their findings on 435people with end stage macular degeneration and280 partners who lived with them.
They found that the more a person smoked,the greater were their chances of developing agerelated macular degeneration.
Regularly smoking a pack or more a dayfor 40 years almost tripled the risk of age relatedmacular degeneration compared with non-smokers.
The risks were also increased for partnerswho were non-smokers, and had lived with a smokerfor five years or more. Their risk nearly doubled.
(Source: Medical News Today, Category: Smoking News,dated 20 Dec. 2005)
3. Fish Oil Prevents Potentially Deadly HeartRate Variability
A two-gram fish oil supplement given dailyto elderly persons prevented a decline in heart ratevariability caused by tiny, dangerous airbornepollutant particles. Heart rate variability, a measureof the autonomic nervous system's regulation of theheart, is an independent risk factor for cardiacarrhythmias, heart attack or sudden death.
These findings appeared in the secondissue of the December 2005 American Journal of

41
Respiratory and Critical Care Medicine, publishedby the American Thoracic Society.
Fernando Holguin, M.D., of the Centers forDisease Control and Prevention in Atlanta, Georgia,and eight associates provided fish oil supplementsto 26 residents of a nursing home in Mexico City. Acontrol group of 24 residents was given soy oilsupplements. The participants' average age rangedfrom 81 to 83 years old.
"In this randomized controlled trial, fish oilsupplementation prevented the reduction in heartrate variability associated with the same-dayexposure to indoor particulate matter," said Dr.Holguin. "In contrast, soy oil, was associated with amarginal protection on heart rate variability."
"Fish oil as a source of omega-3polyunsaturated fatty acids could be considered asa potential form of preventive measure to reducethe risk of arrhythmia and sudden death in elderlysubjects exposed to ambient air pollution," said Dr.Holguin.
In the study, the residents were exposedto tiny indoor air pollutant particles that had adimension of 2.5 micrograms or less. All participantsspent 92 percent of their time indoors.
The supplement study was conducted oversix months. None of the patients suffered fromcardiac arrhythmias, had a pacemaker or werebeing treated with oral anticoagulants.
(Source: Medical News Today, Category: Seniors/AgingNews, dated 20 Dec. 2005)
4. Women Are More Likely To Be Treated ForSleep Problems After An Induced Abortion
Results of a study show that women aremore likely to be treated for sleep disorders ordisturbances following an induced abortioncompared to a birth. The observed risk was highestin the first 180 days after pregnancy outcome butwas not significant after the third year.
The authors examined the records of15,345 women who had an induced abortion and41,479 women who gave birth. Women with ahistory of treatment for sleep disorders beforepregnancy were excluded.
Compared to women who carry unintendedpregnancies to term, research shows that women
who have abortions are more susceptible togeneralized anxiety disorder and depression andare more likely to receive psychiatric treatment.Sleep disorders are often linked to a mood disorderand posttraumatic stress disorder.
(Source: Medical News Today, Category: Abortion News,dated 04 Jan 2006)
5. Smoking While Pregnant Causes Finger, ToeDeformities
Women have yet another reason to stopsmoking while pregnant. In the largest study of itskind, plastic surgeons found smoking duringpregnancy significantly elevates the risk of havinga child with excess, webbed or missing fingers andtoes, according to the January issue of Plastic andReconstructive Surgery®, the journal of theAmerican Society of Plastic Surgeons (ASPS). Infact. Smoking just half a pack per day increasesthe risk of having a child born with a toe or fingerdefect by 29 percent.
Researchers examined the records of morethan 6.8 million live births in the United States during2001 and 2002, finding 5,171 children born with adigital anomaly where the mother smoked duringpregnancy but did not suffer from other medicalcomplications, such as heart disease, diabetes orhigh blood pressure.
The more a woman smoked, the higher therisk became. Women who smoked 11 to 20cigarettes a day raised the risk 38 percent, andwomen who smoked 21 or more cigarettes per dayraised the risk 78 percent.
Webbed fingers or toes occur one in every2,000 to 2,500 live births and excess fingers or toesoccur one in every 600 live births.
Nevertheless, the majority of these defectsoccur without any family history and most causesare unknown which has lead researchers toinvestigate environmental causes, such as smoking,for these anomalies.
"Smoking is so addictive that pregnantwomen often can't stop the habit, no matter whatthe consequences. Our hope is this study will showexpectant mothers another danger of lighting up."
(Source: Medical News Today, Category: SmokingNews, dated : 07 Jan 2006)
42
6. Treatment Of Gum Disease May Reduce TheRisk Of Cardiovascular Disease
The Journal of Dental Research has justpublished the results of a study showing thattreatment of gum disease may reduce the risk ofcardiovascular disease.
Researchers from Australia (Sydney DentalHospital and Royal North Shore Hospital) andNorway (University of Oslo) collaborated in thePERICAR clinical trial, providing strong evidencelinking periodontal (gum) disease to an increasedrisk of developing blood clots, which could lead tothe onset of heart attack and stroke.
In recent years, many studies throughoutthe world have linked periodontal disease toincreased cardiovascular risk, although the reasonsfor this link have not been fully explained, nor has itbeen proven that the link is a direct causal one.One explanation is that inflammation and infectionhave also been related to increased atherosclerosisand cardiovascular risk. Periodontal disease is themost common chronic infection in humans, andsymptoms include bleeding, swollen or recedinggums, and bad breath. In severe cases, the teethbecome loose and may eventually fall out.
Individual participants who were involvedin the trial had blood tests before and after treatment
of gum disease that was so severe that all their teethhad to be extracted. The blood tests were for blood-clot risk factors and signs of inflammation.
The average level of factors fell when thegum infection was eradicated, suggesting that therisk of heart attacks and clots in the future hadreduced. This also indicates that inflammation inthe mouth has a measurable effect in thebloodstream, and therefore the rest of the body.
The researchers are currently studying therelationship between gum and heart disease inpeople with less severe periodontal disease whodo not need to have all their teeth extracted.
Dental disease impacts on people's generalhealth and well-being. Periodontal disease iscommon, preventable, and treatable. This studysuggests that improving periodontal health couldsignificantly reduce the risk of cardiovasculardisease.
The Journal of Dental Research is theflagship publication of the International andAmerican Associations for Dental Research(www.dentalresearch.org) and is the top dentaljournal in the world.
(Source: Medical News Today, Category: DentistryNews, dated 05 Jan 2006)
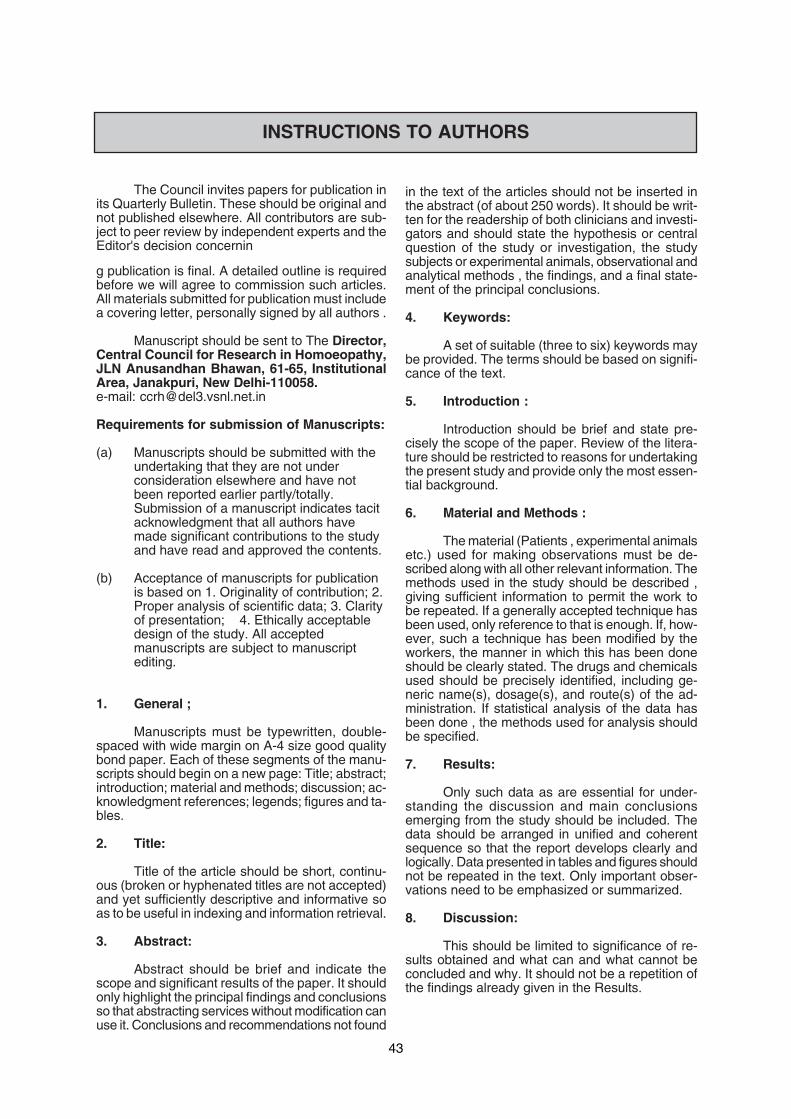
43
The Council invites papers for publication inits Quarterly Bulletin. These should be original andnot published elsewhere. All contributors are sub-ject to peer review by independent experts and theEditor's decision concernin
g publication is final. A detailed outline is requiredbefore we will agree to commission such articles.All materials submitted for publication must includea covering letter, personally signed by all authors .
Manuscript should be sent to The Director,Central Council for Research in Homoeopathy,JLN Anusandhan Bhawan, 61-65, InstitutionalArea, Janakpuri, New Delhi-110058.e-mail: [email protected]
Requirements for submission of Manuscripts:
(a) Manuscripts should be submitted with theundertaking that they are not underconsideration elsewhere and have notbeen reported earlier partly/totally.Submission of a manuscript indicates tacitacknowledgment that all authors havemade significant contributions to the studyand have read and approved the contents.
(b) Acceptance of manuscripts for publicationis based on 1. Originality of contribution; 2.Proper analysis of scientific data; 3. Clarityof presentation; 4. Ethically acceptabledesign of the study. All acceptedmanuscripts are subject to manuscriptediting.
1. General ;
Manuscripts must be typewritten, double-spaced with wide margin on A-4 size good qualitybond paper. Each of these segments of the manu-scripts should begin on a new page: Title; abstract;introduction; material and methods; discussion; ac-knowledgment references; legends; figures and ta-bles.
2. Title:
Title of the article should be short, continu-ous (broken or hyphenated titles are not accepted)and yet sufficiently descriptive and informative soas to be useful in indexing and information retrieval.
3. Abstract:
Abstract should be brief and indicate thescope and significant results of the paper. It shouldonly highlight the principal findings and conclusionsso that abstracting services without modification canuse it. Conclusions and recommendations not found
in the text of the articles should not be inserted inthe abstract (of about 250 words). It should be writ-ten for the readership of both clinicians and investi-gators and should state the hypothesis or centralquestion of the study or investigation, the studysubjects or experimental animals, observational andanalytical methods , the findings, and a final state-ment of the principal conclusions.
4. Keywords:
A set of suitable (three to six) keywords maybe provided. The terms should be based on signifi-cance of the text.
5. Introduction :
Introduction should be brief and state pre-cisely the scope of the paper. Review of the litera-ture should be restricted to reasons for undertakingthe present study and provide only the most essen-tial background.
6. Material and Methods :
The material (Patients , experimental animalsetc.) used for making observations must be de-scribed along with all other relevant information. Themethods used in the study should be described ,giving sufficient information to permit the work tobe repeated. If a generally accepted technique hasbeen used, only reference to that is enough. If, how-ever, such a technique has been modified by theworkers, the manner in which this has been doneshould be clearly stated. The drugs and chemicalsused should be precisely identified, including ge-neric name(s), dosage(s), and route(s) of the ad-ministration. If statistical analysis of the data hasbeen done , the methods used for analysis shouldbe specified.
7. Results:
Only such data as are essential for under-standing the discussion and main conclusionsemerging from the study should be included. Thedata should be arranged in unified and coherentsequence so that the report develops clearly andlogically. Data presented in tables and figures shouldnot be repeated in the text. Only important obser-vations need to be emphasized or summarized.
8. Discussion:
This should be limited to significance of re-sults obtained and what can and what cannot beconcluded and why. It should not be a repetition ofthe findings already given in the Results.
INSTRUCTIONS TO AUTHORS
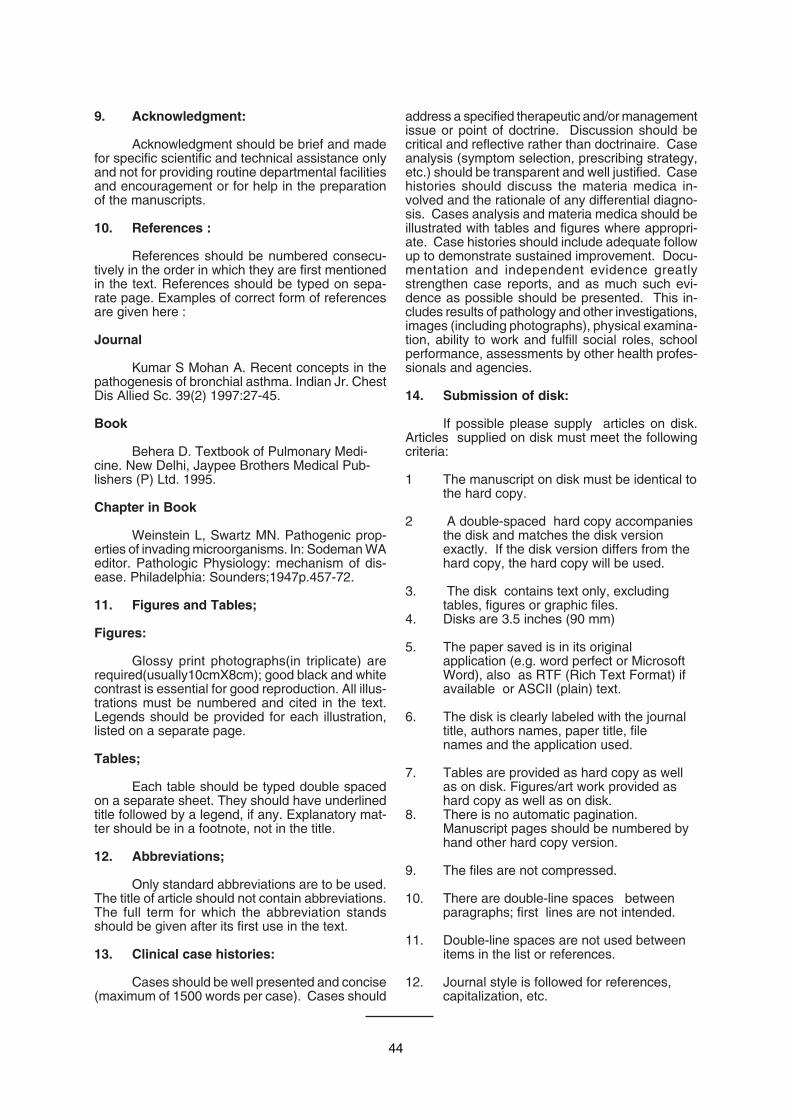
44
9. Acknowledgment:
Acknowledgment should be brief and madefor specific scientific and technical assistance onlyand not for providing routine departmental facilitiesand encouragement or for help in the preparationof the manuscripts.
10. References :
References should be numbered consecu-tively in the order in which they are first mentionedin the text. References should be typed on sepa-rate page. Examples of correct form of referencesare given here :
Journal
Kumar S Mohan A. Recent concepts in thepathogenesis of bronchial asthma. Indian Jr. ChestDis Allied Sc. 39(2) 1997:27-45.
Book
Behera D. Textbook of Pulmonary Medi-cine. New Delhi, Jaypee Brothers Medical Pub-lishers (P) Ltd. 1995.
Chapter in Book
Weinstein L, Swartz MN. Pathogenic prop-erties of invading microorganisms. In: Sodeman WAeditor. Pathologic Physiology: mechanism of dis-ease. Philadelphia: Sounders;1947p.457-72.
11. Figures and Tables;
Figures:
Glossy print photographs(in triplicate) arerequired(usually10cmX8cm); good black and whitecontrast is essential for good reproduction. All illus-trations must be numbered and cited in the text.Legends should be provided for each illustration,listed on a separate page.
Tables;
Each table should be typed double spacedon a separate sheet. They should have underlinedtitle followed by a legend, if any. Explanatory mat-ter should be in a footnote, not in the title.
12. Abbreviations;
Only standard abbreviations are to be used.The title of article should not contain abbreviations.The full term for which the abbreviation standsshould be given after its first use in the text.
13. Clinical case histories:
Cases should be well presented and concise(maximum of 1500 words per case). Cases should
address a specified therapeutic and/or managementissue or point of doctrine. Discussion should becritical and reflective rather than doctrinaire. Caseanalysis (symptom selection, prescribing strategy,etc.) should be transparent and well justified. Casehistories should discuss the materia medica in-volved and the rationale of any differential diagno-sis. Cases analysis and materia medica should beillustrated with tables and figures where appropri-ate. Case histories should include adequate followup to demonstrate sustained improvement. Docu-mentation and independent evidence greatlystrengthen case reports, and as much such evi-dence as possible should be presented. This in-cludes results of pathology and other investigations,images (including photographs), physical examina-tion, ability to work and fulfill social roles, schoolperformance, assessments by other health profes-sionals and agencies.
14. Submission of disk:
If possible please supply articles on disk.Articles supplied on disk must meet the followingcriteria:
1 The manuscript on disk must be identical tothe hard copy.
2 A double-spaced hard copy accompaniesthe disk and matches the disk versionexactly. If the disk version differs from thehard copy, the hard copy will be used.
3. The disk contains text only, excludingtables, figures or graphic files.
4. Disks are 3.5 inches (90 mm)
5. The paper saved is in its originalapplication (e.g. word perfect or MicrosoftWord), also as RTF (Rich Text Format) ifavailable or ASCII (plain) text.
6. The disk is clearly labeled with the journaltitle, authors names, paper title, filenames and the application used.
7. Tables are provided as hard copy as wellas on disk. Figures/art work provided ashard copy as well as on disk.
8. There is no automatic pagination.Manuscript pages should be numbered byhand other hard copy version.
9. The files are not compressed.
10. There are double-line spaces betweenparagraphs; first lines are not intended.
11. Double-line spaces are not used betweenitems in the list or references.
12. Journal style is followed for references,capitalization, etc.
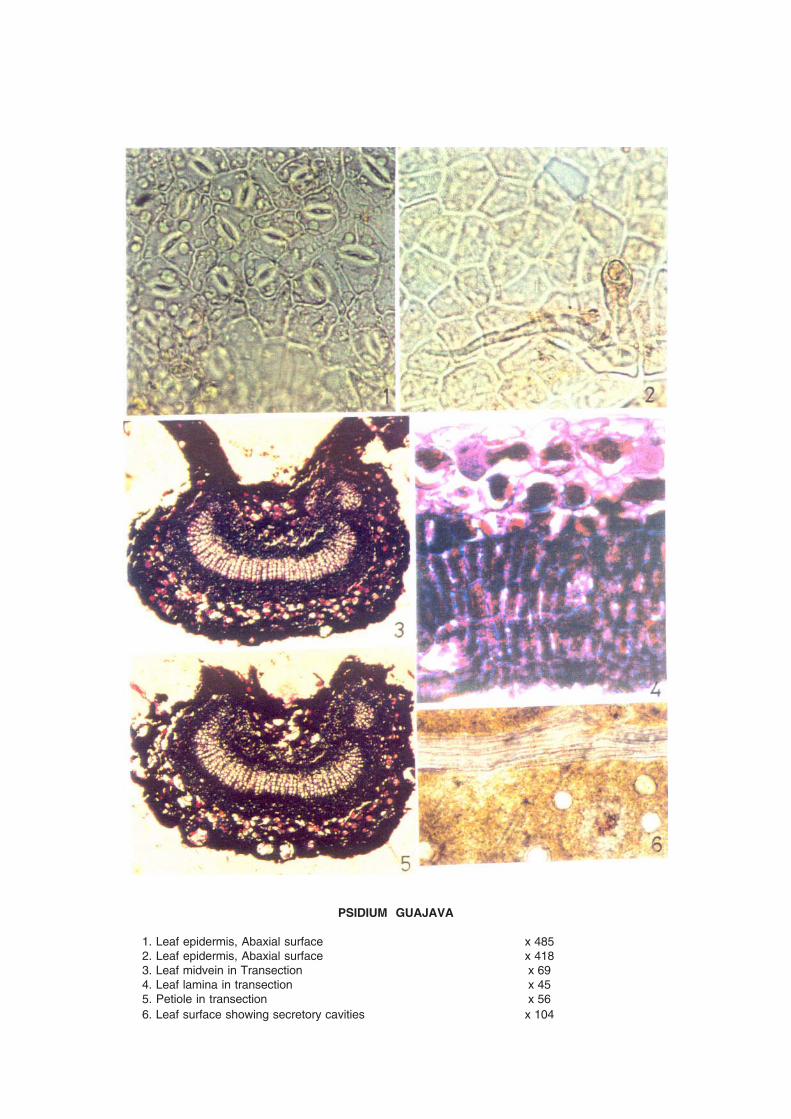
PSIDIUM GUAJAVA
1. Leaf epidermis, Abaxial surface x 4852. Leaf epidermis, Abaxial surface x 4183. Leaf midvein in Transection x 694. Leaf lamina in transection x 455. Petiole in transection x 566. Leaf surface showing secretory cavities x 104
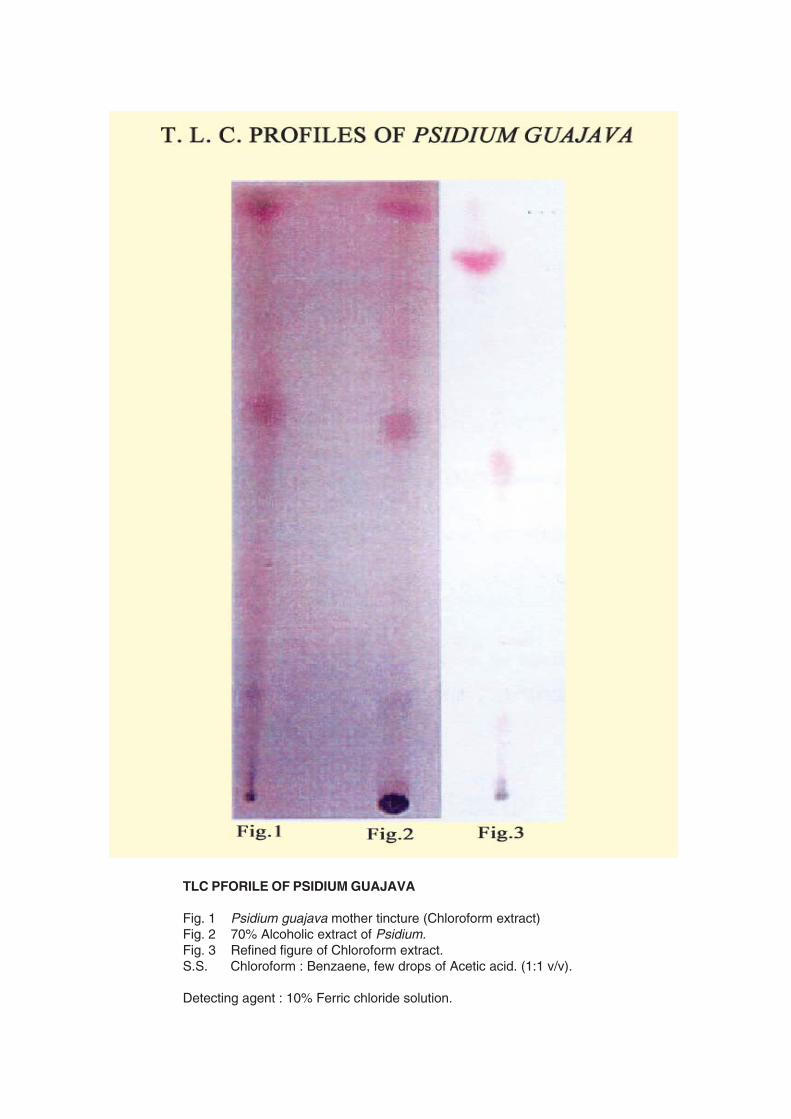
TLC PFORILE OF PSIDIUM GUAJAVA
Fig. 1 Psidium guajava mother tincture (Chloroform extract)Fig. 2 70% Alcoholic extract of Psidium.Fig. 3 Refined figure of Chloroform extract.S.S. Chloroform : Benzaene, few drops of Acetic acid. (1:1 v/v).
Detecting agent : 10% Ferric chloride solution.
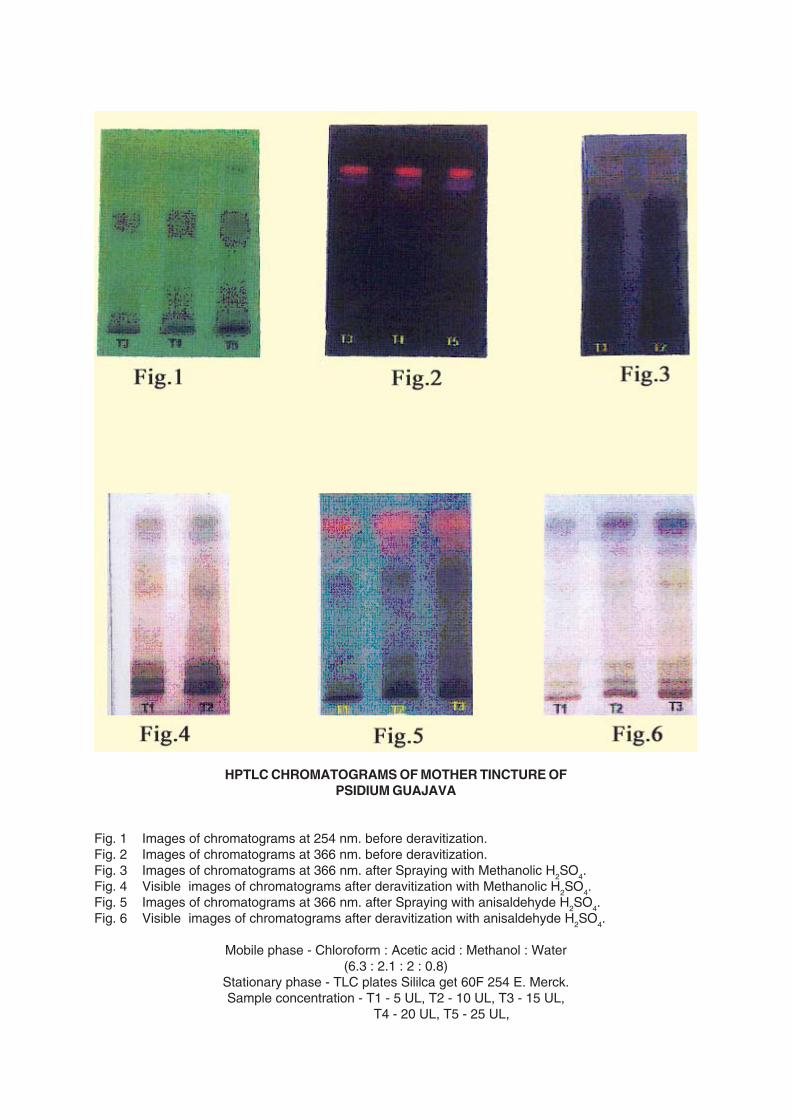
HPTLC CHROMATOGRAMS OF MOTHER TINCTURE OFPSIDIUM GUAJAVA
Fig. 1 Images of chromatograms at 254 nm. before deravitization.Fig. 2 Images of chromatograms at 366 nm. before deravitization.Fig. 3 Images of chromatograms at 366 nm. after Spraying with Methanolic H2SO4.Fig. 4 Visible images of chromatograms after deravitization with Methanolic H2SO4.Fig. 5 Images of chromatograms at 366 nm. after Spraying with anisaldehyde H2SO4.Fig. 6 Visible images of chromatograms after deravitization with anisaldehyde H2SO4.
Mobile phase - Chloroform : Acetic acid : Methanol : Water(6.3 : 2.1 : 2 : 0.8)
Stationary phase - TLC plates Sililca get 60F 254 E. Merck.Sample concentration - T1 - 5 UL, T2 - 10 UL, T3 - 15 UL,
T4 - 20 UL, T5 - 25 UL,