SARCOIDOSIS · 2014. 1. 29. · THE EPIDEMIOLOGY OF SARCOIDOSIS TABLE II Sarcoidosis attack rates...
18
STUDIES ON THE EPIDEMIOLOGY OF SARCOIDOSIS IN THE UNITED STATES: THE RELATIONSHIP TO SOIL AREAS AND TO URBAN-RURAL RESIDENCE By JOHN T. GENTRY,' HAROLD M. NITOWSKY,2 AND MAX MICHAEL, JR.3 (From the Communicable Disease Center, Public Health Service, U. S. Department of Health, Education, and Welfare, Atlanta, Georgia; the Medical Service, Veterans Administration Hospital, Atlanta, Georgia; and The Department of Medicine, Emory University School of Medicine, Atlanta, Ga.) (Submitted for publication October 16, 1953; accepted August 3, 1955) During World War II, there were 350 recog- nized cases of sarcoidosis among American Armed Forces personnel. These cases, chosen in a rela- tively unselected manner, afford an admirable op- portunity for investigation into some of the aspects of the epidemiology of this disease. Preliminary studies of this group have demonstrated a striking concentration of patients' birthplaces in the South- eastern United States (1, 2). Although cases in negroes predominated, the observed geographic localization could not be accounted for solely by the distribution of the negro population in the United States. The present investigation, which was concerned with factors which might have in- fluenced this unusual case distribution, revealed an association between the distribution of the cases and certain soil areas. Furthermore, a higher incidence of the disease was found among servicemen from the more rural areas of the Southeast. These correlations may serve as ad- ditional localizing factors for further studies on the epidemiology of sarcoidosis. MATERIAL AND METHODS Of the 350 cases of sarcoidosis diagnosed in World War II servicemen, there were 334 living at the time of this study. Only these were investigated since the compilation of epidemiologic data would be incomplete in those deceased. In many patients the disease was discovered accidentally by routine x-ray examination taken during the course of hospitalization or upon sepa- ration from service. The diagnoses of sarcoidosis were made in American military hospitals scattered over the 1 Present address: District State Health Officer, Dis- trict Office, 400 Foote Bldg., 316 So. Warren St., Syra- cuse, New York. 2 Present address: Sinai Hospital of Baltimore, Balti- more, Maryland. 3 Present address: Maimonides Hospital of Brooklyn, 4802 Tenth Avenue, Brooklyn 19, New York. world. In all instances the biopsy specimens were re- viewed and confirmed by the Armed Forces Institute of Pathology. A record of the induction chest film and physical examination was available on all patients. The complete records of all hospitalizations on each patient were studied and an analysis of the clinical data is in preparation. The standards for verification of the diag- nosis have been previously reported (1, 2). The pres- ent analysis has been restricted to 297 of these cases, 37 were excluded because of the lack of availability of data to clearly establish locale of residence or diagnosis. The minimum information on these cases consisted of identifying data including race, birthplace, residence at the time of entry into the military service, i.e., "induc- tion residence", and clinical and pathological reports wvhich conformed to the criteria for the diagnosis of the disease, as proposed by the National Research Council (1). Additional consideration was given to those cases whose birthplace and induction residence were in the same or adjacent counties. For convenience, these cases have been arbitrarily designated "lifetime residents". Figures giving the total number of persons serving in all the military services from the beginning of con- scription to December 2, 1946, were obtained through the courtesy of the National Selective Service. These data, available by county and state of indt-ction and race, were used as a basis for calculating race specific attack rates. Since the numerator consists of servicemen, a denominator representing the source of this group would be needed for calculation, hence the use of this Selec- tive Service data. While certain factors of bias, such as omission of females, older persons and those rejected from military duty, are recognized in these rates, this military service information represented the most ap- propriate denominator that was available. The rates by induction residence, in turn, were selected because fac- tors of migration, particularly the movement of Ne- groes from the Southeast to the northern industrial cen- ters, prolonged the determination of accurate rates by birthplace. The soil classification data which were used in this study were obtained through the courtesy of the Division of Soil Survey, United States Department of Agricul- ture. By the use of a recent map, showing the soil re- gions of the South, the various counties in Alabama, 1839
Transcript of SARCOIDOSIS · 2014. 1. 29. · THE EPIDEMIOLOGY OF SARCOIDOSIS TABLE II Sarcoidosis attack rates...

STUDIES ON THE EPIDEMIOLOGYOF SARCOIDOSIS IN THEUNITED STATES: THE RELATIONSHIP TO SOIL AREAS
ANDTO URBAN-RURALRESIDENCE
By JOHNT. GENTRY,' HAROLDM. NITOWSKY,2 AND MAXMICHAEL, JR.3
(From the Communicable Disease Center, Public Health Service, U. S. Department of Health,Education, and Welfare, Atlanta, Georgia; the Medical Service, Veterans Administration
Hospital, Atlanta, Georgia; and The Department of Medicine, Emory UniversitySchool of Medicine, Atlanta, Ga.)
(Submitted for publication October 16, 1953; accepted August 3, 1955)
During World War II, there were 350 recog-nized cases of sarcoidosis among American ArmedForces personnel. These cases, chosen in a rela-tively unselected manner, afford an admirable op-portunity for investigation into some of the aspectsof the epidemiology of this disease. Preliminarystudies of this group have demonstrated a strikingconcentration of patients' birthplaces in the South-eastern United States (1, 2). Although cases innegroes predominated, the observed geographiclocalization could not be accounted for solely bythe distribution of the negro population in theUnited States. The present investigation, whichwas concerned with factors which might have in-fluenced this unusual case distribution, revealedan association between the distribution of thecases and certain soil areas. Furthermore, ahigher incidence of the disease was found amongservicemen from the more rural areas of theSoutheast. These correlations may serve as ad-ditional localizing factors for further studies onthe epidemiology of sarcoidosis.
MATERIAL AND METHODS
Of the 350 cases of sarcoidosis diagnosed in WorldWar II servicemen, there were 334 living at the timeof this study. Only these were investigated since thecompilation of epidemiologic data would be incompletein those deceased. In many patients the disease wasdiscovered accidentally by routine x-ray examinationtaken during the course of hospitalization or upon sepa-ration from service. The diagnoses of sarcoidosis weremade in American military hospitals scattered over the
1 Present address: District State Health Officer, Dis-trict Office, 400 Foote Bldg., 316 So. Warren St., Syra-cuse, New York.
2 Present address: Sinai Hospital of Baltimore, Balti-more, Maryland.
3 Present address: Maimonides Hospital of Brooklyn,4802 Tenth Avenue, Brooklyn 19, New York.
world. In all instances the biopsy specimens were re-viewed and confirmed by the Armed Forces Institute ofPathology. A record of the induction chest film andphysical examination was available on all patients. Thecomplete records of all hospitalizations on each patientwere studied and an analysis of the clinical data is inpreparation. The standards for verification of the diag-nosis have been previously reported (1, 2). The pres-ent analysis has been restricted to 297 of these cases, 37were excluded because of the lack of availability of datato clearly establish locale of residence or diagnosis.
The minimum information on these cases consisted ofidentifying data including race, birthplace, residence atthe time of entry into the military service, i.e., "induc-tion residence", and clinical and pathological reportswvhich conformed to the criteria for the diagnosis of thedisease, as proposed by the National Research Council(1). Additional consideration was given to those caseswhose birthplace and induction residence were in thesame or adjacent counties. For convenience, these caseshave been arbitrarily designated "lifetime residents".
Figures giving the total number of persons servingin all the military services from the beginning of con-scription to December 2, 1946, were obtained through thecourtesy of the National Selective Service. These data,available by county and state of indt-ction and race,were used as a basis for calculating race specific attackrates. Since the numerator consists of servicemen, adenominator representing the source of this group wouldbe needed for calculation, hence the use of this Selec-tive Service data. While certain factors of bias, suchas omission of females, older persons and those rejectedfrom military duty, are recognized in these rates, thismilitary service information represented the most ap-propriate denominator that was available. The rates byinduction residence, in turn, were selected because fac-tors of migration, particularly the movement of Ne-groes from the Southeast to the northern industrial cen-ters, prolonged the determination of accurate rates bybirthplace.
The soil classification data which were used in thisstudy were obtained through the courtesy of the Divisionof Soil Survey, United States Department of Agricul-ture. By the use of a recent map, showing the soil re-gions of the South, the various counties in Alabama,
1839

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
Arkansas, Florida, Georgia, Louisiana, Mississippi, NorthCarolina, South Carolina, and Texas were placed in oneof 91 categories, depending upon the predominant soilseries charted for each county. The soil series, in turn,were combined into larger groups on the basis of simi-larities in topography, profile, and parent materials, to
form the soil areas characteristic of the Piedmont Pla-teau, Middle and Lower Coastal Plain, and other physio-graphic divisions of the Southeast. These soils are con-tained for the greater part in 8 of the 36 great soilgroups thus far recognized in the United States, namely,the Red-Yellow Podzolic soils, Rendzinas, Alluivial soils,
TABLE I
Cases of sarcoidosis in the Armed Forces during World lW"ar II, according to states, by race,birthplace, and induction residence
Number of cases
Birthplace Induction residence
State Total White Negro Total White Negro
Region I (South Atlantic Gulf Coast)AlabamaArkansasFloridaGeorgiaLouisianiaMississippiNorth CarolinaSouth CarolinaTexasVirginia
Total
Region II (Middle Atlantic and B3order)DelawareDistrict of ColtumbiaJIarylandNew JerseyNew YorkOklahomaPennsylvaniaTennesseeWest Virginia
Total
Region III (Rest of Cotuntry)*ArizonaCaliforniaConnecticti tIllinoisIndianaIowaKansasKentuckvMassachusettsMichiganMiSSOLII'iMontanaNebraskaNorth DakotaOhioUtahWashingtonWisconsin
TotalU. S. Total
31 513 411 126 313 222 336 430 223 418 2
223 30
1
32
133383
36
j53214221l3
21
31290t
269
1023111932281916
193
27 5 2214 3 1115 1520 3 1712 2 1019 2 1729 4 2515 2 1320 6 1414 2 12
185 29 1 56
1
2 -12 1
2 134 42 1
25 11
1
3 ?32
_ 1141 11 1lI11 2121
23 878 212
647
183
1482
63
64
1 615 3
1 24 103 51 1
25 38
1 16 4 21 1 -8 5 34 3 1
2 1 11 14 4 -8 3 ;3 2 11 11 1
6 2 41 1 -2 2
49 31 18297 84 212
New Hampshire, Oregon,* No cases were recognized from 11 states: Colorado, Idaho, Maine, 'Minnesota, Neyada,Rhode Island, South Dakota, Vermont, WVyoming.
t Seven white cases were foreigni born.
1840

THE EPIDEMIOLOGY OF SARCOIDOSIS
TABLE II
Sarcoidosis attack rates among World War II servicemen, by race and induction residence,according to regions of the United States
Sarcoidosis cases by Attack ratesSelective service population induction residence per 100,000
RatioTotal White Negro Total White Negro Total White Negro N/W
Region I 2,955,135 2,291,056 664,079 185 29 156 6.3 1.3 23.5 18/1
(South Atlantic Gulf Coast)Region II 4,238,992 3,953,837 285,155 63 25 38 1.5 0.6 13.3 22/1
(Middle Atlantic Border)Region III 7,037,448 6,820,041 217,407 49 31 18 0.7 0.5 8.3 17/1
(Rest of U. S.)Total 14,231,575 13,064,934 1,166,641 297 85 212 2.1 0.7 18.2 26/1
Ratio of Rates: Region I/Region III 9/1 3/1 3/1Region I/Region II 4/1 2/1 2/1
Reddish-Chestnut soils, Ground-Water Podzolic soils,and Lithosols.4
The urban-rural distribution data which were usedin this study were obtained from the 1940 census report.The population characteristics utilized in the urban-ruralclassification included population density, as defined bypopulation per square mile, and total population. In re-lation to the negro cases, the population of negro in-habitants of a county classified as rural by the Bureau ofCensus was used. For this part of the study a total of185 cases was studied. Each of these patients had en-tered military service from one of the ten Southeasternstates, the area in which the highest incidence of thedisease was found. An attempt was made to character-ize the county areas of residence as predominantly ruralor urban on a relative basis and to consider attack ratesamong servicemen from county areas of varying urban-rural composition.
RESULTS
Geographic distribution
The breakdown of cases by states is shown inTable I. The states have been divided into threegeographic areas on the basis of the relative inci-dence of the disease. Region I, which had thehighest incidence of sarcoidosis, was composed ofthe nine South Atlantic and Gulf Coast states ofAlabama, Florida, Georgia, Louisiana, Mississippi,North Carolina, South Carolina, Texas, and Vir-ginia plus Arkansas. In these states there was atotal of 223 cases by birthplace, 30 whites and 193
4The classification and nomenclature of soils used inthis study is that of Soils and Men, U. S. Dept. of Agr.Yearbook of Agriculture, 1938, Part IV, pp. 861-1161,with some modifications outlined in the issue of SoilScience and Soil Classification, Vol. 67, No. 2, 1949.
negroes; and 185 by induction, 29 whites and 156negroes. The difference of 37 negroes indicatesthe migration of this group out of the section.Region II which had the next highest incidencewas contiguous to Region I and comprised theDistrict of Columbia, the five Middle AtlanticStates of Delaware, Maryland, New Jersey, NewYork and Pennsylvania, plus Tennessee, WestVirginia and Oklahoma. In these states therewas a total of 36 cases by birthplace, 25 whites and11 negroes; and 63 by induction, 25 whites and 38negroes. The difference of 27 negroes representsthe migration into this industrial region. In theremainder of the country, Region III, there were31 cases by birthplace, 23 whites and 8 negroes;and 49 by induction, 31 whites and 18 negroes.
Attack rates for sarcoidosis, specific for raceand induction residence, are summarized in TableII for the three regions. In the South AtlanticGulf Coast States, Region I, the overall attackrates are 1.3 and 23.5 for whites and negroes, re-spectively. The overall rate in the Middle At-lantic and Border States, Region II, was 1.5 per100,000, 0.6 for whites and 13.3 for negroes. InRegion III, the remainder of the country, theoverall rate was 0.7 per 100,000, 0.5 among whitesand 8.3 among negroes. It is apparent from theseattack rates that a marked predominance of thedisease exists among negro inductees of all re-gions, with the remarkably consistent negro-to-white ratios of 18 to 1, 22 to 1, and 17 to 1 forRegions I, II, and III, respectively. It is possible,however, that the disproportionately larger num-
1841

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
TABLE III
Sarcoidosis attack rates among World War II servicemen, by race and induction residence, according tothe states of the South Atlantic Gulf Coast region
State
AlabamaArkansasFloridaGeorgiaLouisianaMississippiNorth CarolinaSouth CarolinaTexasVirginia
Total
Selective service population
Total White Negro
272,843 202,648 70,195189,327 156,550 32,777208,787 157,599 51,188292,172 220,912 71,260242,943 170,620 72,323211,667 125,592 86,075349,809 276,260 73,549179,664 125,201 54,463716,250 626,258 89,992291,673 229,416 62,257
2,955,135 2,291,056 664,079
Attack rates per 100,000
Total White Negro
9.9 2.5 31.37.4 1.9 33.67.2 0 29.36.8 1.4 23.94.9 1.2 13.89.0 1.6 19.88.9 1.4 34.08.3 1.6 23.92.8 1.0 15.64.8 0.9 19.3
6.3 1.3 23.5
(O-E)2_ E
(for Negro cases)
* 1.831.410.750.012.880.513.430.002.390.46
X2= 13.670.20>p> 0.10
ber of negro, as compared to white, emigrantsfrom the Southeast may have altered the negro-to-white attack rate ratios for Regions II and III.
In comparing rates between the regions, it canbe seen that the overall rate for Region I, 6.3 per
100,000, is nine times as great as that for RegionIII, 0.7 per 100,000. However, a large part ofthis difference is due to the disproportionaterates between the two races, since a ratio of lessthan 3 to 1 is observed between the respective
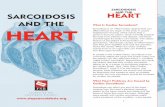
DISTRIBUTION OF CASES OF SARCOIDOSIS AMONGAMERICANARMEDFORCESPERSONNELBY BIRTHPLACE
FIG. 1. THE DISTRIBUTION, BY BIRTHPLACE, OF 290 CASES OF SARCOIDOsIs RECOGNIZEDAMONGWORLDWARIISERVICEMEN
Each dot represents the birthplace of a single case. Seven additional cases were foreign-born.
1842

THE EPIDEMIOLOGY OF SARCOIDOSIS
DISTRIBUTION OF CASES OF SARCOIDOSIS AMONGAMERICANARMEDFORCESPERSONNEL
BY INDUCTION RESIDENCE
FIG. 2. THE DISTRIBUTION, BY RESIDENCE AT THE TIME OF INDUCTION INTO THE ARMEDFORCES, OF 297 CASES OFSARcoIDoSIS RECOGNIZEDAMONGWORLDWARII SERVICEMEN
Each dot represents the induction residence of a single case.
negro and white rates for these regions. Simi-larly, the 4 to 1 ratio between the overall rates ofRegions I and II, 6.3 and 1.5, respectively, alsoreflects the disproportionate rates between the ne-groes and whites.
It is evident, therefore, that the higher attackrate for sarcoidosis in the negro and the largenegro population in Region I account, in part, forthe concentration of cases in this area. How-ever, the 3 to 1 ratio of rates in negroes for Re-gions I and III clearly indicates the presence ofsome localizing factor, aside from race, which in-fluences the distribution of the cases.
In attempting to disclose what this factor (orfactors) might be, subsequent considerations werefocused on the ten states of Region I. Attackrates specific for race and induction residencewere first determined for each of these states, asshown in Table III. Because of the small numberof white cases, comparisons were made betweenthe negroes only. In the table, the observed inci-
dence of the disease among negro inductees foreach state has been compared with the expectedincidence on the basis of the overall rates for thearea. It is evident that the variations obtainedare not great. Although the negro attack rate forNorth Carolina, 34.0 per 100,000, is somewhatgreater than that for the rest of the area, 22.2per 100,000, this difference is only of questionablestatistical significance. Thus, when comparingindividual states as units in this manner, it is ap-parent that no definite concentration of the casesby induction residence exists in any one state.
Relation of the disease to the fall line
Reference to Figures 1 and 2 will reveal cer-tain peculiarities in the distribution of the casesin the Southeast, both by birthplace and inductionresidence. Within the Carolinas, a greater num-ber of residences appear in the eastern portion ofthe states. Concentrations also appear in Southern
1843

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
DISTRIBUTION OF SARCOIDOSIS IN 10 SOUTHEASTERNSTATESBY INDUCTION RESIDENCE
IN RELATION TO THE "MODIFIED" FALL LINE AREA
\
LEGEND
o WHITE CASE
* NEGROCASE
FIG. 3. THE DISTRIBUTION, BY INDUCTION RESIDENCE, OF 185 CASES OF SARCOIDOSIS IN THE 10 SOUTH ATLANTICGULF COASTSTATES OF REGION I IN RELATION TO THE FALL LINE AND "BORDERCOUNTIES"
Each dot represents the induction residence of a single case. The heavy line represents the approximate locationof the fall line and the shaded area indicates the "border" counties.
Georgia and in the area where Texas, Louisiana,and Arkansas are contiguous. This distributioncorresponds very closely with the physiographicarea known as the Atlantic and Gulf CoastalPlain. Until relatively recent geologic times, thisarea was covered by the sea and was delineatedalong its westernmost and northernmost extent bythe former coast line, which is now known as thefall line (3). The approximate position of thisformer coast line is shown by the heavy line onFigure 3.
Comparisons were next made of the race specificattack rates by induction residence for the areaswithin the Southeastern states in relation to thisgeologic landmark. In arriving at these rates,counties- were assigned to the "above" or "be-low fall line" category, depending upon their lo-calization. Since the former coast line transectsmany contemporary county borders, and since the
determination of its exact location in any regionmay be difficult, the counties traversed by andadjacent to the fall line, which have been desig-nated as border counties, were considered sepa-rately. The term "modified" fall line was intro-duced to represent the composite area of theseborder counties and is depicted in Figure 3 by thestippled area.
Table IV indicates negro attack rates by induc-tion residence for the areas of the ten states ofRegion I in relation to the "modified" fall line.It can be seen that for each state a greater numberof cases in negroes occurs in the "below fallline" area. Similarly, the attack rate is greaterfor this area in each of the states, with the ex-ception of Texas. The overall rate for the "be-low fall line" area in four of the states, Alabama,Georgia, North Carolina, and South Carolina, is49.0 per 100,000 or five times greater than the
1844
.Is
iI

THE EPIDEMIOLOGY OF SARCOIDOSIS
,overall "above fall line" rate of 10.0 per 100,000for these states. In three other states, Arkansas,Texas, and Virginia, the differences in attackrates between the "above" and "below fall line"areas are not statistically significant. However,in two of these, Arkansas and Virginia, the trendof the rates is the same as that observed in thefour states where the differences are significant.Thus, we have a distinct intrastate concentrationof the cases in the coastal plain area which ap-
pears to be unaccountable for by population dis-tribution within these states.
Relation to other geographic factors
A number of ecological factors were exploredfor a possible explanation of this unusual localiza-tion. Among these were meteorologic conditions(4), the distribution of plant and animal life (5,6), agricultural practices (7), and overall popu-lation densities (8). It was found that none ofthese factors was overtly associated with the dis-tribution of the cases.
Since the fall line delineates, among otherthings, the boundaries of geologic formations (9)and major soil groups in the Southeast, attentionwas directed to a consideration, in a qualitativefashion, of surface materials. A close associationappeared to exist between the residences of thecases and some of the soils of the coastal plains.This correlation was strengthened by several ad-ditional observations. In the Mississippi Valley,relatively few cases were noted although this isan area with a large negro population. The Al-luvial soils, which are found there, differ signifi-cantly in character from the other soils of theSoutheast. Furthermore, in the area whereTexas, Louisiana, and Arkansas are contiguous,there is a reappearance of some of the soils whichare present along the eastern portion of the coastalplain. The concentration of cases in this generalregion appeared to strengthen the preliminary cor-
relation of the cases with these soils. Therefore, a
more detailed and quantitative study was made ofthis relationship.
TABLE IV
Sarcoidosis attack rates among World War II Negro servicemen, by induction residence, according to areas in relationto the "modified" fall line in the South Atlantic Gulf Coast states
State
Alabama
Arkansas
Florida
Georgia
Louisiana
Mississippi
North Carolina
South Carolina
Texas
Virginia
Area inrelation to"modified"
fall line
AboveBelow
AboveBelow
Below
AboveBelow
Below
Below
AboveBelow
AboveBelow
AboveBelow
AboveBelow
Negroselectiveservice
population
28,75125,760
2,14223,543
51,188
30,72126,636
72,323
86,075
33,49821,745
17,23726,214
5,31874,301
22,10124,767
Negrocases byinductionresidences
415
8
15
311
10
17
312
11
212
46
Attackrates
per100,000
13.958.2
34.0
29.3
9.8l41.3)
13.8
19.8
9.0l55.2J
42.0)
37.616.21
18.1/24.2
X2 ofdifferences
betweenNegro rates
7.66
0.46*
5.81
10.38
5.67*
1.30
0.21
Total Above 139,768 16 11.4 11.07Below 432,552 117 27.01Border 91,759 23 25.1
* Corrected for continuity.
1845

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
SOIL REGIONS OF THE SOUTH
v~~~~.-.-
El]to
LEGEND
RED-YELLOW PODZOLIC SOILS OFTHE MIDDLE COASTAL PLAIN
RED-YELLOWPODZOLIC SOILS OFTHE PIEDMONT PLATEAU
OTHER RED-YELLOW PODZOLIC SOILS
ALLUVIAL SOILS OF THE MISSISSIPPI DELTA
GROUNDWATER PODZOLIC AND HUMIC-GLEYSOILS OF THE LOWER COASTAL PLAINAND GULF COAST FLATWOODS
OTHER SOILS (RENDZINAS, LITHOSOLS, PLANOSOLSREDDISH CHESTNUT, REDDISH PRAIRIE AND RED DEkERT)
FIG. 4. THE GENERALPATTERN OF THE GREAT SOIL GROUPSIN THE SOUTHEASTLocal details have been submerged in order to present a general view of the significant features on a small map.
Soils of the southeast
The general pattern of the soil areas in theSouitheast is shown in Figure 4.5 These soils canbe differentiated on the basis of well-definedmorphological and other characteristics, such aschemical composition, geologic precursors, na-tive vegetation, and topographhy (10, 11).
The Red-Yellow Podzolic soils formii the domi-nant group in this region, extending from Virginiato Texas. These have light-colored sandy sur-faces overlying firm, red to yellow subsoils. Theyare generally well drained, strongly leached, andlow in organic and mineral plant nutrients.
On the basis of variations in one or more oftheir characteristics, these leached soils can befurther classified among a number of subgroups.
5 Since identical soil classification data were not avail-able for Virginia, the subsequent analysis has been re-stricted to nine of the states in Regioni I. Older soilclassification schemes (10) indicated that the inclusionof Virginia did not significantly alter the correlationsobtained between race specific attack rates for sarcoidosisand residence in certain soil areas.
In Figure 4 are outlined The Red-Yellow Pod-zolic soils of the Middle Atlantic Coastal Plain,subgroup "la," those of the Piedmont Plateau,subgroup "lb," and a miscellaneous subgroup,
1lc."The Alluvial soils occupy the flood plains in
the Southeast and form the dominant soils of theMississippi Valley. They are soils in early stagesof profile development, having been affected verylittle by processes of soil formation. In general,the Alluvial soils in this region are relatively highin organic miiatter, poorly drained, and neutral inreaction. These have been designated as group"2" in Figure 4.
The Humic-Grey and Ground-Water Podzolsare poorly drained soils which occur extensivelyalong the Atlantic and Gulf Coasts. These soils,group "3" in Figure 4, generally have light-greysandy leached layers and usually contain littleorganic matter. Most of these have been derivedfrom beds of unconsolidated sands and sandyclays of relatively recent geological origin.
The remaining soils in the Southeast are com-
1846
' S

THE EPIDEMIOLOGY OF SARCOIDOSIS
TABLE V
Sarcoidosis attack rates among World WVar II Negro servicemen, by induction residence, according tosoil areas of the South Atlantic Gulf Coast states *
Negro Negro Attack (O-E)2selective cases by rates Eservice induction per (for Negro
Soil group population residence 100,000 cases)
Red-Yellow Podzolic soils of the MiddleCoastal Plain (la) 188,049 82 43.6 30.65
Red-Yellow Podzolic soils of the Pied-mont Plateau (lb) 92,542 6 6.5 11.72
Other Red-Yellow Podzolic soils (1c) 63,995 11 17.2 1.21Alluvial soils of the Mississippi Delta (2) 55,881 6 10.7 4.09Ground-Water Podzolic and Humic-Clav
soils of the Lower Coastal Plain (3) 116,376 23 19.8 0.83Other soilst (4) 84,979 16 18.8 0.91
X2= 49.41p < 0.001
Totals 601,882 144 23.9
$ Includes Alabama, Arkansas, Florida, Georgia, Louisiana, Mississippi, North Carolina, South Carolina, Texas.t Includes Rendzinas, Lithosols, Plenosols, Reddish Chestnut, Reddish Prairie and Red Desert soils.
posed of a heterogeneous group of shallow, stonysoils (Lithosols), clay pan soils (Planosols),black soils (Rendzinas), and subhumid and semi-arid soils (Reddish-Prairie and Reddish-Chest-nut), all of which have been combined into group
"4" in Figure 4.
Negro attack rates by soils
Race specific attack rates for negroes by induc-tion residence were determined for the varioussoil areas in the Southeast, as shown in Table V.Although the number of white cases in relationto each soil group was too small to make validcomparisons of the attack rates between thegroups, the trends observed were similar to thoseamong the negro patients.
The negro attack rates range from 6.5 per
100,000 for the soils of the Piedmont Plateauabove the fall line to 43.6 per 100,000 for the soilsof the Middle Coastal Plain below the fall line.The attack rate for the Alluvial soil area is some-
what low, 10.7, but the remaining rates appear
to be quite uniform. Thus, rates of 17.2, 19.8, and18.8 per 100,000 were noted for the group "ic,"
group "3," and group "4" soil areas, respectively.It is apparent that the greatest differences in
attack rates exist between the soils of the MiddleCoastal Plain and those of the Piedmont Plateau,where a ratio of almost 7 to 1 in these rates is ob-served. This ratio should be contrasted to themuch smaller 3 to 1 ratio which was found be-
tween the negro attack rates for Regions I andIII.
No significant localization of the cases by in-duction residence appeared to exist within theRed-Yellow Podzolic soils of the Middle CoastalPlain itself. Thus, negro attack rates in relationto this particular soil group for each of the nineSoutheastern states, as shown in Table VI, areessentially equivalent. The one exception, per-haps, is North Carolina, where the rate of 71.3 per100,000 is somewhat higher than those for theother states. Even with this elevated rate, how-ever, the total chi square of the differences, 10.48,is not statistically significant.
TABLE VI
Sarcoidosis attack rates among World War II Negroservicemen from the "la" soil area,
according to states
Negro Negro Attack (O-E)'selective cases by rates Eservice induction per (for Negro
State population residence 100,000 cases)
Alabama 27,175 13 47.8 0.12Arkansas 10,464 7 66.9 1.25Florida 10,001 6 60.0 0.58Georgia 27,059 13 48.0 0.12Louisiana 18,574 5 26.9 1.19Mississippi 20,898 8 38.3 0.13North Carolina 22,449 16 71.3 3.92South Carolina 19,374 5 25.8 1.38Texas 32,055 9 28.1 1.79
X2 10.480.20 <p <0.30
Totals 188,049 82 43.6
1847

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
Race specific attack rates were determined foreach of the seventeen minor soil series which com-pose the leached soils of the Middle Coastal Plain.Because of the generally small number of cases, itwas difficult to compare the rates, which werefound to be quite variable. However, no signifi-cant concentration of induction residences was ob-served in relation to any of these soil series, ascan be observed from Figure 5. There, the ap-proximate locations of the individual soil seriesare indicated by the alphabetical characters. Thus,the factor (or factors) which influence the con-centration of cases by induction residence in theMiddle Coastal Plain area appears to be dis-tributed with some uniformity.
Factors of migrationAdmittedly, these efforts to quantitate the as-
sociation of the cases of sarcoidosis with certain
soil groups are crude. However, the previously-mentioned influence of migration, particularly for-the negroes, seems to mlinimize the observed dif-ferences. For example, of the 52 negroes in-ducted from Regions II and III. only- 17 wereborn in this area; 35 had been born in the South-east. Of these 35 migrants, 22, or 63 per centwere born in the area of the Middle Coastal Plainsoils. Since it is reasonable to assumnle that themajority of these individuials had nmigrated tonorthern areas as recentl) as the pre-war period ofnational mobilization, exposure to the soils mayhave been of considerable duration.
The tincertainties introduced by migration canbe minimized by considering only those caseswhose birthplace and induction residence werelocated in the same or adjacent counties, the so-called "lifetime residents." It would seem rea-sonable to assume that these individuials had a pro--
DISTRIBUTION OF SARCOIDOSIS IN 9 SOUTHEASTERNSTATESBY INDUCTION RESIDENCE
IN RELATION TO CERTAIN OF THE RED-YELLOWPODZOLIC SOILS
I VrJ
'K S .*1 */. \' Ii .
N.1 -I
. 2) _ _
LEGENDc WHITE CASEo NEGROCASE
FIG. 5. THE INDUCTION RESIDENCES OF A GROUPOF 171 CASES OF SARCOIDOSIS IN NINE OF THE SOUTH ATLANTIC-GULF COAST STATES
The residences are shown in relation to the 17 minor soil series, indicated by the alphabetical characters which,compose the "la" Red-Yellow Podzolic soils.
1848

THE EPIDEMIOLOGY OF SARCOIDOSIS
longed contact with the soils in and about theircounty of induction, whereas a similar assumptionwould be less likely to apply in the case of themigrants. Of the 113 negroes with sarcoidosisinducted from Region I who could be classifiedas "lifetime residents," 73 came from the MiddleCoastal Plain soil area and 4 from the leachedsoil area of the Piedmont Plateau. The total negro
selective service populations for these areas, in-clusive of immigrants and permanent residents,were approximately 188,000 and 93,000, respec-
tively. While these figures are not deemed suf-ficiently comparable to calculate valid attack rates,the crude rates which may be derived are 39 per
100,000 and 4 per 100,000 indicating differences of10 to 1 or greater. As noted previously, the at-tack rates based on the total number of cases in-ducted from these areas were 43.6 per 100,000 and6.5 per 100,000, respectively, representing a differ-ence of slightly less than 7 to 1.
Unfortunately, chronological residence data are
not available for all the cases from Region I. Ifsuch were at hand, it would be feasible to deter-mine man-years of experience for all the soilareas. The significant correlations obtained byuse of "lifetime residents" suggest that such a
method of analysis would strengthen the relation-ship between sarcoidosis and the soils of theMiddle Atlantic Coastal Plain.
Urban-rural occurrence of the disease
By grouping the counties of the ten Southeast-ern states according to population density, sar-
coidosis attack rates can be calculated for whiteand negro servicemen from these compositecounty areas. In Table VII the rates for negromilitary personnel are shown. It can be seen
that an inverse relationship exists between theserates and county population density. For thecounties with 19 or fewer inhabitants per squaremile, presumably those which are most rural incharacter, the rate of 48.7 per 100,000 is highest.On the other hand, a much lower rate, 15.2 per100,000, is found among the servicemen from thecounties with population densities of 100 or more
people per square mile, areas which presumablyare most urbanized. The attack rates amongnegro servicemen from counties with intermediatepopulation densities lie in between these extremes.
TABLE VI I
Sarcoidosis attack rates among World War II Negro service-menfrom 10 South Atlantic Gulf Coast states *
according to population density ofcounty of induction
Populationdensityt ofcounty ofinduction
Less than 2020-4950-99100 and over
Total
Negroselectiveservice
population
20,560219,332187,434236,753
664,079
Negrocases by
inductionresidence
10713936
156
Attackrates (O-E)2
100,000 E
48.6 5.6332.4 7.3820.8 0.5715.2 6.91
23.5 X2=20.49p< 0.001
* Includes Alabama, Arkansas, Florida, Georgia, Louisi-ana, Mississippi, North Carolina, South Carolina, Texas,and Virginia.
t Population per square mile (1940), from County DataBook, U. S. Bureau of the Census, 1947.
The overall differences between these rates are
statistically highly significant (X2 = 20.49, p <.001). The small number of white cases in rela-tion to each county group made it difficult toevaluate the differences between the attack ratesobserved. However, the overall trend of theserates was the same as that found among negro
servicemen.
Figure 6 illustrates the population density dis-tribution for the counties of the ten-state region.In comparing this with Figure 3, which illustratesthe distribution of the cases of sarcoidosis in re-
lation to the modified fall line, it appears that themore densely populated counties are located inthe area of the Piedmont Plateau (above the fallline) whereas the distribution of the less denselypopulated counties appears to conform to that ofthe Atlantic Coastal Plain (below the Fall line).
In view of the previously demonstrated cor-
relation between race specific attack rates forsarcoidosis and residence in certain soil areas inthe Southeast, it was deemed desirable to deter-mine whether urban-rural localizing factors were
acting independently of these soil associations.Therefore, attack rates were computed for serv-
icemen from the various soil areas of the South-east according to the population density distri-bution of the various counties.
These rates for negro servicemen from theRed-Yellow Podzolic soil area of the Middle At-lantic Coastal Plain in nine of the Southeasternstates having identical soil classification data are
1849

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
POPULATION DENSITY DISTRIBUTION BY COUNTIES10 SOUTHEASTERNSTATES
,
V\4
LEGENDPOPULATION DENSITY
0-19C777 20-49 i* /
EM 50-99
_ 100 AND OVER
FIG. 6. THE POPULATIONDENSITY DISTRIBUTION BY COUNTIES IN TEN SOUTHEASTERNSTATESPopulation density is expressed as number of inhabitants per square mile and refers to Bureau of the Census data
from the 1940 census.
shown in Table VIII. This "la" soil area, asdesignated previously, represents the site of maxi-mal intraregional concentration of the cases, both
TABLE VIII
Sarcoidosis attack rates among World War II Negro service-men from the Middle Coastal Plain soil area,* by
induction residence, according to populationdensity of county of induction
Populationdensityt ofcounty ofinduction
Less than 2020-4950-99100 and over
Total
Negroselectiveservice
population
7,63993,61256,00030,798
188,049
Negrocases by
inductionresidence
7372513
82
Attackrates
per100,000
91.639.544.642.2
43.6
by birthplace and induction residence. The rateof 91.8 per 100,000 among the servicemen fromthe counties with lowest population densities, 19or fewer inhabitants per square mile, is more thantwice as great as the overall rate of 41.7 per 100,-000 among servicemen from the more denselypopulated counties. Although the number ofcases in the former category is small, the differ-ence between these rates is statistically significant(p < 0.04). The remaining attack rates amongservicemen from counties with population densi-ties of 20-49, 50-99, and 100 or more inhabitantsper square mile, show no consistent downwardtrend, in contrast to the findings for the whole ofthe ten-state region.
On the other hand, the attack rates amongnegro servicemen from the remaining soil areasof the nine-state region exclusive of the "la" Mid-dle Coastal Plain area are shoNwn in Table IX.
* Middle Coastal Plain Soil area in 9 states, includingAlabama, Arkansas, Florida, Georgia, Louisiana, Missis-sippi, North Carolina, South Carolina, and Texas.
t Population per square mile (1940), from County DataBook, U. S. Bureau of the Census, 1947.
1850

THE EPIDEMIOLOGY OF SARCOIDOSIS
TABLE IX
Sarcoidosis attack rates among World War II servicemenfrom nine South Atlantic Gulf Coast states,* exclusive
of the Middle Coastal Plain soil area,according to population density
of county of induction
Population Negro Negro Attackdensityt of selective cases by ratescounty of service induction perinduction population residence 100,000
Less than 20 12,640 3 25.720-49 108,294 27 24.950-99 114,060 11 9.6100 and over 178,779 21 11.7
Total 413,773 62 15.0
* Includes Alabama, Arkansas, Florida, Georgia, Louisi-ana, Mississippi, North Carolina, South Carolina, andTexas.
t Population per square mile (1940) from County DataBook, U. S. Bureau of the Census (1947).
Rates of 23.7 and 24.9 per 100,000 were obtainedfor servicemen from counties with population den-sities of 19 or fewer, and 20 to 49 inhabitants persquare mile, respectively. The overall rate forthese composite county areas, 24.9 per 100,000,is statistically significantly higher (p < 0.001)than the overall rate of 10.9 per 100,000 observedamong servicemen from counties with greaterpopulation densities, 50 to 99, and 100 or moreinhabitants per square mile, respectively. Again,there is no consistent downward trend in therates as shown in Table VII for the entire ten-state region, but the qualitative relationshipsremain unchanged, i.e., higher attack rates pre-vail among servicemen from counties with low pop-ulation densities, which presumably are most ruralin character. These findings suggest the presenceof a rural localizing factor in the occurrence ofsarcoidosis which may be independent of any pri-mary soil relationship.
By grouping the counties of the "la" MiddleCoastal Plain soil area according to populationsize, a similar correlation can be demonstrated,as shown in Table X. Here, a threefold differenceis evident between the attack rate of 124.4 per 100,-000 among negro servicemen from counties withthe smallest total populations, less than 10,000inhabitants, and the overall rate of 41.1 per 100,-000 among servicemen from counties with thesmallest total populations, less than 10,000 in-habitants, and the overall rate of 41.1 per 100,000among servicemen from counties with more than10,000 inhabitants. Although the former rate is
based on only seven cases, the difference betweenthese rates is statistically significant (p < 0.01).Again, no consistent downward trend in the ratesis apparent among the more populous counties;however, the rate among servicemen from countieswith populations of 100,000 or more, is only 25.7per 100,000, a somewhat lower value than theothers.
A further suggestion of the rural localization ofsarcoidosis is provided by other Bureau of theCensus data. Table XI presents the attack ratesamong negro servicemen from the Middle At-lantic Coastal Plain soil area according to the pro-portion of inhabitants classified as "rural," i.e.,those residents in communities with less than 2500people, among the negro population of eachcounty. A direct correlation exists between theserates and the percentage of "rural" negro inhabi-tants. Thus, among negro servicemen fromcounties where 90 to 100 per cent of the negroesare in the "rural" category, the attack rate of 54.7per 100,000 is highest. This declines to a rateof 29.0 per 100,000 for the servicemen from coun-ties with less than 49 per cent "rural" negro in-habitants. Although the differences between theserates are only of borderline statistical significance,the trend is in conformity with previous findings.
Admittedly, these attempts to demonstrate arural localization of sarcoidosis among World WarII servicemen are also crude. The factor of mi-gration, among others, again introduces some un-certainty in the interpretation of the findings andthe unavailability of residence data pertaining to
TABLE X
Sarcoidosis attack rates among World War II Negro service-men from the AMiddle Coastal Plain soil area,* by
induction residence, according to popula-tion size of county of induction
Negro Negro AttackPopulation sizet selective cases by rates
of county of service induction perinduction population residence 100,000
Less than 10,000 5,622 7 124.510,000-19,999 30,502 14 45.920,000-49,999 95,854 39 40.750,000-99,999 40,514 18 44.4100,000 and over 15,557 4 25.7
Total 188,049 82 43.6
* Middle Coastal Plain soil area in nine states, includingAlabama, Arkansas, Florida, Georgia, Louisiana, Missis-sippi, North Carolina, South Carolina, and Texas.
t 1940 population, from County Data Book, U. S.Bureau of the Census, 1947.
1851

JOHN T. GENTRY, HAROLD M. NITOWSKY, AND MAX MICHAEL, JR.
TABLE XI
Sarcoidosis attack rates among World War II Negro service-men from the Middle Coastal Plain soil area,* by
induction residence, according to per cent ofrural inhabitants among Negro popui-
lation of county of induction
Per cent of ruralinhabitants amongNegro population
of county ofinductiont
90-10070-8950-69Less than 50
Total
Negroselecti,veservice
population
58,54663,36731,69734,439
188,049
Negrocases by
inductionresidence
32261410
82
Attackrates
per100,000
57.741.044.229.0
43.6
* Middle Coastal Plain soil area in Alabama, Arkanisas,Florida, Georgia, Louisiana, Mississippi, North Carolina,South Carolina, and Texas.
t From 1940 Btureau Census Data.
the pre-induction period precludes any attemlpt tocorrect for this variable. The importance of thelatter is evident from the findings on the follow-upstudies of 40 cases in the ten-state Southeasternregion. Sixteen, or 40 per cent of these patients,lived in a community with a population of 2500 or
greater at the time of their induction into thearmed forces, and by the criteria of the Bureau ofthe Census, could be termed '"urban' inhabitants.However, chronological residence histories fromthese sixteen individuals revealed that eleven hadspent more than half their lives on farms or hadengaged in farming as an occupation prior to mili-tary service, and therefore must have had pro-
longed contact with rural environments. It wouldseem likely that similar residence information frommore intensive follow-up studies of all the cases
would serve to strengthen the relationship betweenthe disease and previous rural residence.
DISCUSSION
An analysis of the residence data from thisgroup of 297 military cases of sarcoidosis revealeda distinct concentration of their birthplaces andinduction residence in the Southeast. Within thisregion, a significant correlation was observed be-tween race specific attack rates and residence inareas defined by the distribution of certain specificsoil groups. In addition, significantly higher at-tack rates were noted among military personnelfrom the Southeast whose residences at the time ofentry into the armed forces were located in therelatively rural counties, as evidenced by low popu-
lation density and small population size of theseareas.
Since sarcoidosis is not a reportable disease,there is a paucity of morbidity data from whichany comparison might be made with the caseswhich occur in the general population. Israel andSones (12) have recently described their experi-ences with cases of sarcoidosis seen in Philadel-phia. Of the 74 negroes in their group, 64 wereborn in the South, a distribution greatly dispropor-tionate to the estimated percentage of southern-born negroes in that city.
Some (lata from a group of civilian cases ofsarcoidosis in North Carolina (13) and SouthCarolina (14) provided an opportunity to com-pare the geographic localization of these cases withthat observed among the military group. Of atotal of 14 individuals suspected of having tu-berculosis but later diagnosed as sarcoidosis, dur-ing 1949 and 1950 in South Carolina, 12 residedin the "below fall line" area. Nine of these re-sided within counties containing the leached soilsof the Middle Coastal Plain as the predominantsoil types. In North Carolina, 17 deaths werereported from Boeck's sarcoid from 1949 to 1951.Of the total, four resided in counties above thefall line, six lived in "border" counties and sevenresided in the "below fall line" area. Of the 13deaths in "border" and "below fall line" counties,nine had lived where the leached Middle CoastalPlain soils abounded. Thus, these data, while in-appropriate for the computation of sarcoidosis at-tack rates for different areas, would appear to beconsistent with the observations on the militarycases inducted from these states.
On the other hand, in analyzing the birthplacesof 177 patients with sarcoidosis diagnosed at theMIayo Clinic from 1940 through 1951, Carr andGage (15) did not find that the disease was morecommon in patients who came from the South-eastern part of the United States than in those whocame from other areas. Apparently, such factorsas age, sex, race, and severity of disease could notexplain the difference in distribution from thatwhich had been reported for the group of militarycases (2). It should be pointed out, however,that the comparison between the geographic dis-tribution of cases and the total population at theMIayo Clinic does not provide any precise infor-mation as to the relative incidence of the disease
1852

THE EPIDEMIOLOGY OF SARCOIDOSIS
:among an unselected population in a given area.The series of Carr and Gage therefore is notstrictly comparable to the military group.
The evidence that Boeck's sarcoid occurs withgreater frequency among inhabitants of rural areasis in accord with the suggestion that soils may bedeterminants in the occurrence of the disease.Longcope and Freiman (16) in confirming anearlier observation of Lomholt (17), noted thatsarcoidosis often affected farm laborers and thosewho live in country districts. Whitehead (18)and Cone (19) refer to similar observations. Inrelating calcareous crystalline material in soils tothe pathogenesis of lesions characteristic of sar-coidosis, Refvem (20) noted ". . . that peopleliving in the country are preferably attacked byBoeck's disease, especially farmers, gardners, etc."Israel and Sones (12) reported that of ten cases ofsarcoidosis in white persons seen in Philadelphiaonly one had been a life-long resident of that city.They noted that "Sarcoidosis would appear to beextremely rare among what is the largest groupin this country, the native-born urban white."
The higher attack rates of sarcoidosis amongthe rural inhabitants of the Southeastern UnitedStates, its apparent predilection for negroes andfor those living in certain soil areas presents achallenging and perplexing problem. If sarcoido-sis is a manifestation of a single etiologic agent,the widespread occurrence of cases in this countrywould indicate that such an agent is not confinedto the Southeast. However, the distinct aggre-gation of military cases in this area and the sug-gestion of a similar distribution among civiliancases leads to speculations which may point tofurther investigation.
It is conceivable that the observed geographiclocalization of the disease is the result of a) thepresence of a highly favorable environment inareas within the Southeast for the growth, propa-gation, or transmission of an etiologic agent oragents, or b) an alteration in the susceptibility ofthe population of these areas which predisposesthem to the action of some agent which elsewheremight possess a very low grade or altered patho-genecity.
The role of possible host factors in the localiza-tion of sarcoidosis is suggested by experienceswith pellagra in this country. The concentrationof the latter disease in the Southeast could be re-
lated largely to the socio-economic status andconsequent dietary habits of the affected popula-tion, with contributory or secondary factors, suchas infectious diseases, influencing its incidence ata particular time or place (21). Similarly, dietarypeculiarities and the socio-economic status of thepopulation in certain areas of the Southeast mayenhance their resistance to the inciting factor ofsarcoidosis; however, little information is avail-able on this point.
The data pertaining to the unusually high inci-dence of sarcoidosis among negroes in this coun-try also suggest an influence of host susceptibility.Of the total of 523 cases reported in the Americanliterature up to 1952, 385, or 73.4 per cent, wereof this race (16). The 26 to 1 ratio between theoverall negro and white attack rates in the pres-ent series of cases emphasizes this racial predilec-tion. In contrast are the reports from Europe andelsewhere which indicate a high frequency ofsarcoidosis in the white race (22). Schonholzerfound 67 cases of sarcoidosis among 516,879Swiss army recruits subjected to mass radio-graphic examinations, an incidence of 13 per 100,-000 (23). This rate compares much better withthe overall attack rate in negroes of 18 per 100,000,than the white rate of 0.7 per 100,000 amongAmerican servicemen. Although these two seriesare not strictly comparable, the results suggestthat factors other than inherent racial suscepti-bility may be influencing the higher prevalence ofsarcoidosis among negroes in this country. Thus,sociologic and environmental factors, such as thosesuggested to account for the significantly higherincidence of venereal diseases among this group(24), may similarly contribute to a susceptibilityfor Boeck's sarcoid.
The possible concentration of an etiologic agentin some of the soils of the Southeast is brought tomind by the somewhat similar distribution of hook-worm disease in the sandy areas of this region(25), and the greater prevalence of this parasiticinfection among rural inhabitants (26). Further-more. recent epidemiologic studies of variousmycotic diseases, particularly histoplasmosis andcoccidioidomycosis, indicate that their distributionis restricted to regions containing soils favorablefor the growth and dissemination of the causativefungi (27-29). By analogy, it can be postulatedthat some helminth, bacterium, fungus. or virus
1853

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
giving rise to sarcoidosis may find certain of theRed-Yellow Podzolic soils of the Southeast thebest. natural media in which to thrive and thusresult in the described localization of the disease.
Other factors, such as the role of intermediatevectors, may account for the circumscribed dis-tribution of Boeck's sarcoid. The Southeasternlocalization of typhus and malaria can be cor-related with the distribution of the tropical ratflea (Xenopsylla cheopis) and certain species ofmosquitoes (Anopheles quadrimaculatus) (30,31). In these instances the concentration and mi-gration of the rat, as well as climatic conditions(32, 33), and the presence of impounded waterand other suitable breeding places (34), ratherthan any specific soil characteristics, appear to bethe factors which confine these respective arthro-pods to this region. However, certain insects arerestricted to specific soil areas, thereby localizingdisease agents for which they are the natural vec-tor. Acute conjunctivitis in the South and thedistribution of the sand gnat, (Hippelates pusio),may be such a case in point (35, 36). Again byanalogy, it is possible that some intermediatearthropod vector, in close association with certainsoils, serves as an effective transmitter of the etio-logic agent of sarcoidosis. However, the lack ofany evidence to incriminate an intermediate vectorin the transmission of the disease and the lack ofany knowledge concerning an arthropod distribu-tion which conforms to that observed for the mili-tary cases casts some doubt upon such an hy-pothesis.
The plant and animal life of the soil areas inwhich cases of sarcoidosis are concentrated bearscrutiny for a possible etiologic relationship to thedisease. In addition, the chemical differences be-tween the various soils of the Southeast mighthave some relation to the localization of Boeck'ssarcoid.
In regard to the latter, the Red-Yellow Pod-zolic soils of the Piedmont Plateau (where rela-tively few cases of sarcoidosis resided) contain astrikingly lower percentage of silica and higherpercentages of alumina and potash than do thesoils of the middle Atlantic Coastal Plain (10).These differences and the resemblance of thepulmonary forms of sarcoidosis to some of thepneumoconioses suggest the possibility that soilsmay be directly implicated in the pathogenesis of
Boeck's sarcoid. In support of this are the ob-servations of Refvem, who demonstrated crystal-line material, which he assumed to be derivedfrom calcareous spars in the soil, in biopsy speci-mens of 4 of 100 patients with sarcoidosis (20).Ayres, Ober, and Hamilton are of the opinion thatmany of the strictly localized sarcoid lesions ofthe skin, following trauma, are actually a form ofsilicosis (37), and similar contentions have beenmade by other workers (38, 39). Experimentally,Gardner was able to reproduce in rabbits, guineapigs, and rats, granulomatous lesions resemblingthose of sarcoidosis, following the administrationof particles of silicon dioxide (40).
Suggestions have been made of a relationshipbetween sarcoidosis and the chronic form ofberyllium poisoning (41 ). Although there aremany similarities in clinical features between thetwo, certain differences have been found (42).Furthermore, as Freiman has noted (43), therelatively recent industrial use of beryllium com-pounds makes these agents unlikely causes forany great numbers of cases of sarcoidosis. How-ever, the inability of Dutra, Cholak, and Hubbard(44) to recover abnormal quantities of berylliumfrom some lesions of chronic berylliosis, illustratesthe difficulty of evaluating possible relationships.
The possibility does exist that exposure to un-usual amounts of naturally-occurring beryllium inthe soils of the Southeast might have accountedfor the aggregation of cases in the middle AtlanticCoastal Plain. Soils in this area were derivedfrom the granitic rocks of the Appalachian Moun-tains which represent the major concentration ofberyllium containing surface ore in the UnitedStates. Similarly, such beryllium containingrocks have their greatest concentration in Europein the Scandinavian countries where sarcoidosisis quite prevalent. Analysis of soil samples ob-tained in close proximity to the lifetime residenceof several of the military cases revealed, by thespecific gravity flotation method, the presence ofoccasional small fragments of beryllium containingrock (44). Chemical and spectrographic analysescarried out by Hodge, Toribara, Steadman, Cho-lak, and Hubbard, confirmed the presence ofberyllium in these samples, although not in anyunusual concentrations (45, 46). However, theneed for caution in relating sarcoidosis to beryl-liosis and other forms of pneumoconioses which
1854

THE EPIDEMIOLOGY OF SARCOIDOSIS
might result from any association with soils mustbe stressed, in view of the diversity of agents thatcan induce tissue reactions closely simulating thesarcoid granuloma.
Many hypotheses relating to factors of hostsusceptibility or to characteristics necessary forthe propagation and transmission of an etiologicagent may be invoked to account for the observedconcentration of cases in certain areas of theSoutheast. Undoubtedly, other possibilities existwhich have not been mentioned. Any workinghypothesis should be in accord with the availableepidemiologic knowledge of sarcoidosis in thiscountry; namely, its apparent predilection for ne-
groes, its concentration in certain soil areas, andits apparent greater relative frequency among
rural inhabitants. The newly defined hyper-en-demic sarcoidosis area in the Southeast wouldappear to warrant more intensive study in an ef-fort to elucidate the many obscurities still sur-
rounding the etiology and pathogenesis of thisdisease.
SUMMARY
An epidemiologic study of 350 cases of sar-
coidosis in military personnel during World WarII has indicated the occurrence of this disease witha significantly greater frequency among thosewhose birthplace is in the Southeastern UnitedStates. Residence in a rural area further favorsdevelopment of the disease.
The ratio of negro to white cases of 18 to 1accounts in part only for this geographic distribu-tion. The occurrence of sarcoidosis is greater inpatients living within certain regions of this en-
demic area. A close association between the distri-bution of certain soil types with these regions was
noted. Thus, residence in rural areas of theSoutheast, particularly of negroes, within regionsof a fine sandy soil type appears to favor the de-velopment of sarcoidosis. The possible implica-tions of these findings are discussed.
ACKNOWLEDGMENT
The authors gratefully acknowledge the selective serv-
ice data provided by Mr. Kenneth H. McGill, Researchand Statistics Chief, National Selective Service; the soilclassification data provided by Dr. Roy W. Simonson,Assistant Chief, Division of Soil Survey, U. S. Depart-ment of Agriculture; and the statistical assistance ofMrs. Bricelyn Cantey, and Mr. David Sack, Communi-
cable Disease Center. Appreciation is also extended toDr. Alexander D. Langmuir, Chief, Epidemiology Branch,Communicable Disease Center, for his invaluable as-sistance and advice during the course of this study. MissJewell Schaeffer gave invaluable assistance in compilingand analyzing clinical records of all patients.
REFERENCES1. Ricker, W., and Clark, M., Sarcoidosis. A clinico-
pathologic review of three hundred cases, includingtwenty-two autopsies. Am. J. Clin. Path., 1949,19, 725.
2. Michael, M., Jr., Cole, R. M., Beeson, P. B., andOlson, B. J., Sarcoidosis. Preliminary report on astudy of 350 cases with special reference to epi-demiology. Am. Rev. Tuberc., 1950, 62, 403.
3. Fenneman, N. M., Physiography of Eastern UnitedStates. New York, McGraw-Hill Book Com-pany, Inc., 1938.
4. Thornthwaite, C: W., Atlas of Climatic Types in theUnited States, 1900-1939. Washington, D. C.,U. S. Department of Agriculture, 1941, Miscel-laneous Publication 421.
5. Society of American Foresters, Committee on For-est Types, Forest Cover Types of the EasternUnited States. 3rd. ed. rev., Washington, D. C.,1940.
6. Schantz, H. L., and Zon, R., Natural vegetation inAtlas of American Agriculture, Washington, D. C.,U. S. Dept. of Agriculture, 1936.
7. Klages, K. H. W., Ecological Crop Geography. NewYork, The Macmillan Company, 1942.
8. U. S. Bureau of the Census, County Data Book. Asupplement to the Statistical Abstract of theUnited States. Washington, D. C., 1947.
9. Longwell, C. R., Knopf, A., and Flint, R. F., Text-book of Geology. Part I. Physical Geology. NewYork, John Wiley and Sons, Inc., 1932.
10. Marbut, C. F., Soils of the United States in Atlas ofAmerican Agriculture, Washington, D. C., U. S.Department of Agriculture, 1936.
11. Baldwin, M., Kellog, C. E., and Thorp, J., Soil clas-sification in Yearbook of Agriculture: Soils andMen, Washington, D. C., U. S. Department ofAgriculture, 1938, pp. 979-1001.
12. Israel, H. L., and Sones, M., Sarcoidosis. Am.Pract. & Digest Treatment, 1952, 3, 18.
13. Hamilton, J., Personal communication.14. Rakich, J. H., Personal communication.15. Carr, D. T., and Gage, R. P., The geographic dis-
tribution of sarcoidosis. Am. Rev. Tuberc., 1954,70, 899.
16. Longcope, W. T., and Freiman, D. G., A study ofsarcoidosis: Based on a combined investigation of160 cases including 30 autopsies from The JohnsHopkins Hospital and Massachusetts GeneralHospital. Medicine, 1952, 31, 1.
17. Lomholt, S., Douze cas de Sarcoides de Boeck Traitesa l'antileprol. Bull. Soc. Franc. de dermat. etsyph., 1934, 41. 1354.
1855

JOHN T. GENTRY, HAROLDM. NITOWSKY, AND MAX MICHAEL, JR.
18. Whitehead, H. G., Sarcoidosis: Manifestations oftuberculosis without allergy; studies on possibleetiological relationship of acid-fast chromogen iso-lated from two cases. Bull. Am. Acad. Tuberc.Physicians, 1940, 4, 117.
19. Cone, R. B., A review of Boeck's sarcoid with analy-sis of twelve cases occurring in children. J. Pediat.,1948, 32, 629.
20. Refvem, O., I. Chronic granulomas in the alimentarytract caused by minute mineral particles. II."Boeck's Disease" and occurrence of minute min-eral particles (Preliminary Report). Acta Patho-logica, 1948, XXV, 107.
21. Love, A. G., and Davenport, C. B., Immunity of city-bred recruits. Arch. Int. Med., 1919, 24, 129.
22. Leitner, S. I., Der Morbus Besnier-Boeck-Schaumann;Chronische Epitheloidzellige Reticuloendothelioseoder Granulomatose. 2. Erweiterte Aufl., Basel,Benno Schwabe & Co., 1949.
23. Schonholzer, G., Morbus Besnier-Boeck-Schaumannund Armeedurch-Leuchtung. Schweiz. med.Wchnschr., 1947, 77, 585.
24. Lewis, J. H., The Biology of the Negro. Chicago,Univ. of Chicago Press, 1942.
25. Augustine, D. L., and Smillie, W. G., The relationof the type of soils of Alabama to the distributionof hookworm disease. Am. J. Hyg., 1926, 6,March Suppl., 36.
26. Chandler, A. C., Hookworm Disease; Its Distribu-tion, Biology, Epidemiology, Pathology, Diagnosis,Treatment and Control. New York, The Mac-millan Co., 1929.
27. Grayston, J. T., and Furcolow, M. L., The occurrenceof histoplasmosis in epidemics-epidemiologicalstudies. Am. J. Pub. Health, 1953 43, 665.
28. Smith, C. E., Epidemiology of acute coccidioidomy-cosis with erythema nodosum. ("San Joaquin" or"Valley Fever"). Am. J. Pub. Health, 1940, 30,600.
29. Smith, C. E., Beard, R. R., Rosenberger, H. G., andWhiting, E. G., Effect of season and dust controlon coccidioidomycosis. J. A. M. A., 1946, 132,833.
30. Dyer, R. E., Rumreich, A., and Badger, L. F.,Typhus fever. A virus of the typhus type de-rived from fleas collected from wild rats. Pub.Health Rep., 1931, 46, 334.
31. Barber, M. A., Komp, W. H. W., and Hayne, T. B.,The susceptibility to malaria parasites and the re-lation to the transmission of malaria of the speciesof Anopheles common in the Southern UnitedStates. Pub. Health Rep., 1927, 42, 2487.
32. Dyer, R. E., The control of typhus fever. Am. 3.Trop. Med., 1941, 21, 163.
33. Eskey, C. R., Relation of reported cases of typhusfever to location, temperature, and precipitation.Pub. Health Rep., 1948, 63, 941.
34. Malaria Control on Impounded Water. Federal Se-curity Agency, U. S. Public Health Service, andTennessee Valley Authority, Health and SafetyDepartment, Washington, D. C., U. S. Govern-ment Printing Office, 1947.
35. Davis, D. J., and Pittman, M., Acute conjunctivitisin the South. CDCBulletin, 1950 (April), 9, 18.
36. Dow, R. P., The eye gnat problem. CDC Bulletin,1950 (April), 9, 20.
37. Ayres, W. W., Ober, W. B., and Hamilton, P. K,Post-traumatic subcutaneous granuloma associ-ated with a crystalline material. Am. J. Path.,1951, 27, 303.
38. German, W. M., Lupoid-sarcoid reaction induced byforeign body (Silica). Am. J. Clin. Path., 1940,10, 245.
39. King, C. O., Posttraumatic sarcoid-like lesions.South. M. J., 1946, 39, 122.
40. Gardner, L. U., The similarity of the lesions pro-duced by silica and by the tubercle bacillus. Am.J. Path., 1937, 13, 13.
41. Hardy, H. L., and Tabershaw, I. R., Delayed chemi-cal pneumonitis occurring in workers exposed toberyllium compounds. J. Indust. Hyg. & Toxicol.,1946, 28, 197.
42. Vorwald, A. J., Pneumoconiosis; Beryllium, BauxiteFumes, Compensation. NewYork, Paul B. Hoeber,Inc., 1950.
43. Freiman, D. G., Sarcoidosis. New England J. Med.,1948, 239, 664-671, 709-716, 743-749.
44. Dutra, F. R., Cholak, J., and Hubbard, D. M., Thevalue of beryllium determinations in the diagnosisof berylliosis. Am. J. Clin. Path., 1949, 19, 229.
45. Hodge, H. C., Toribara, T. Y., and Steadman, L. T.,Personal communication.
46. Cholak, I., and Hubbard, D. M., Personal communi-cation.
1856